
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 24 January 2022
Sec. Head and Neck Cancer
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.747520
This article is part of the Research Topic Women in Head and Neck Cancer: 2021 View all 18 articles
 Virginia Arrazubi1†
Virginia Arrazubi1† Gerardo Cajaraville2†David Cantero3†
Gerardo Cajaraville2†David Cantero3† Jordi Giralt4†
Jordi Giralt4† Ricard Mesia5†Florencio Monje6†Antonio Rueda7†
Ricard Mesia5†Florencio Monje6†Antonio Rueda7† Alexander Sistiaga8†Jorge Suarez9
Alexander Sistiaga8†Jorge Suarez9 Alejandro Mut9
Alejandro Mut9 Marta Comellas10
Marta Comellas10 Luis Lizán10,11*
Luis Lizán10,11*Purpose: A systematic, standardized collection of health outcomes during patient treatment and follow-up, relevant from the perspective of all stakeholders, is a crucial step toward effective and efficient disease management. This project aimed to define a standard set of health outcomes for patients with squamous cell carcinoma of the head and neck (SCCHN).
Methods: The project was led and coordinated by a scientific committee (SC). It comprised: (1) a literature review (to identify variables used during SCCHN management); (2) 1st-SC meeting (to select the variables for presentation during nominal groups-NG); (3) five NG (n=42 experts) and four interviews with patients (to reach consensus on the variables for inclusion); and (4) final-SC meeting (to review the results of NG ensuring consensus on the variables where consensus was not reached).
Results: Experts agreed to include the following variables in the standard set: treatment-related (treatment intent and type, response to treatment, treatment toxicity/complication, treatment completion), degree of health (performance status, patient-reported health status, pain, dysphonia, feeding and speech limitations, body image alteration, tracheotomy), survival (overall and progression-free survival, cause of death), nutritional (weight, nutritional intervention), other variables (smoking status, alcohol consumption, patient satisfaction with aftermath care, employment status), and case-mix variables (demographic, tumor-related, clinical and nutritional factors).
Conclusions: This project may pave the way to standardizing the collection of health outcomes in SCCHN and promote the incorporation of patients’ perspective in its management. The information provided through the systematic compilation of this standard set may define strategies to achieve high-quality, patient-centered care.
Head and neck cancer includes a group of neoplasms of various anatomical sites that differ in terms of etiology, diagnostic and treatment approaches (1). It was the seventh most common cancer worldwide in 2020 accounting for 932,000 new cases and 466,500 deaths (2). In Spain, it was estimated that 14,200 new cases of head and neck cancer would be diagnosed in 2020 (3). More than 90% of cases are squamous cell carcinomas of the head and neck (SCCHN) (4) and more than 60% of patients with SCCHN present with stage III or IV disease (5). SCCHN is typically diagnosed in older patients, with smoking and alcohol consumption being two of the main risk factors for its development (1). Moreover, human papilloma virus (HPV) infection has emerged as a new risk factor, especially in oropharyngeal cancer (6).
Treatment for SCCHN is complex and requires a multidisciplinary approach since it differs according to the stage of the disease, anatomical site, and surgical accessibility. It may require intricate surgery, radiation, chemotherapy, and/or targeted therapy, and/or immunotherapy (7, 8). Some of these treatment options involve changes to critical structures for speaking, eating and breathing, which can lead to functionality problems. Therefore, as a result of treatment, patients with SCCHN face long-term challenges beyond surveillance for recurrent or secondary cancer, including adapting to disfigurement, managing dysphagia and developing alternative speech (9, 10).
In addition to curative intention, structural and functional preservation, amelioration of morbidities when feasible, and long-term maintenance of health-related quality of life (HRQoL) are the principal treatment objectives. Therefore, treatment selection based on a multidisciplinary tumor board decision is essential (11, 12). There is growing evidence supporting the routine collection of patient-reported outcomes (PROs) to enable improved, patient-centered care. The systematic collection of PROs in oncology has a positive effect on patient-physician communication, improves the monitoring of disease progression and response to therapy, helps identify unrecognized problems (physical, emotional and/or social problems), contributes to detecting adverse effects of treatment, and enhances patients’ experience and satisfaction (13). Despite the collection of PROs being considered the cornerstone for achieving the best results and preserving patients’ HRQoL, their systematic collection using standardized and validated instruments is mostly limited to clinical research environment, with scarce use in clinical practice.
To move toward an effective and efficient patient-centered system, a holistic approach is required, integrating evidence from clinical outcomes and PROs. Experience gained from other fields shows that the systematic and standardized collection of outcomes is the sine qua non to improve the quality of any process (14). During the last few years, pioneer initiatives such as the one performed by the International Consortium for Health Outcomes Measurements (ICHOM) (15) have focused on the development of standard sets of health outcomes for various diseases, among which SCCHN is not included. The long-term goal of these initiatives is to promote consistency in data collection between different institutions within the same country or among different countries. A systematic, standardized compilation of health outcomes, relevant from the perspective of all stakeholders, during patient treatment and follow-up, is a key step toward effective and efficient disease management. This project aimed to define a standard set of health outcomes and the most appropriate instruments to measure them for managing patients diagnosed with SCCHN. This is the first step to ensure to standardize the collection of health outcomes in SCCHN.
The project comprised four phases: (1) a literature review; (2) first scientific committee meeting; (3) five nominal groups (described in greater detail below) and four semi-structured interviews with patients, and; (4) final scientific committee meeting (Figure 1). The scientific committee and nominal group meetings were conducted between June 2019 and December 2020. The project was led and coordinated by a scientific committee consisting of healthcare professionals who are experts in the management of SCCHN, and/or have experience in implementing strategies to standardize health outcomes (three specialists in medical oncology [VA, RM, AR], one specialist in radiation oncology [JG], one specialist in otolaryngology [AS], one specialist in oral and maxillofacial surgery [FM], one specialist in quality and innovation [DC], one hospital pharmacist [GC]) and one representative of a Spanish patient advocacy group (Grupo Español de Pacientes con Cancer, GEPAC).
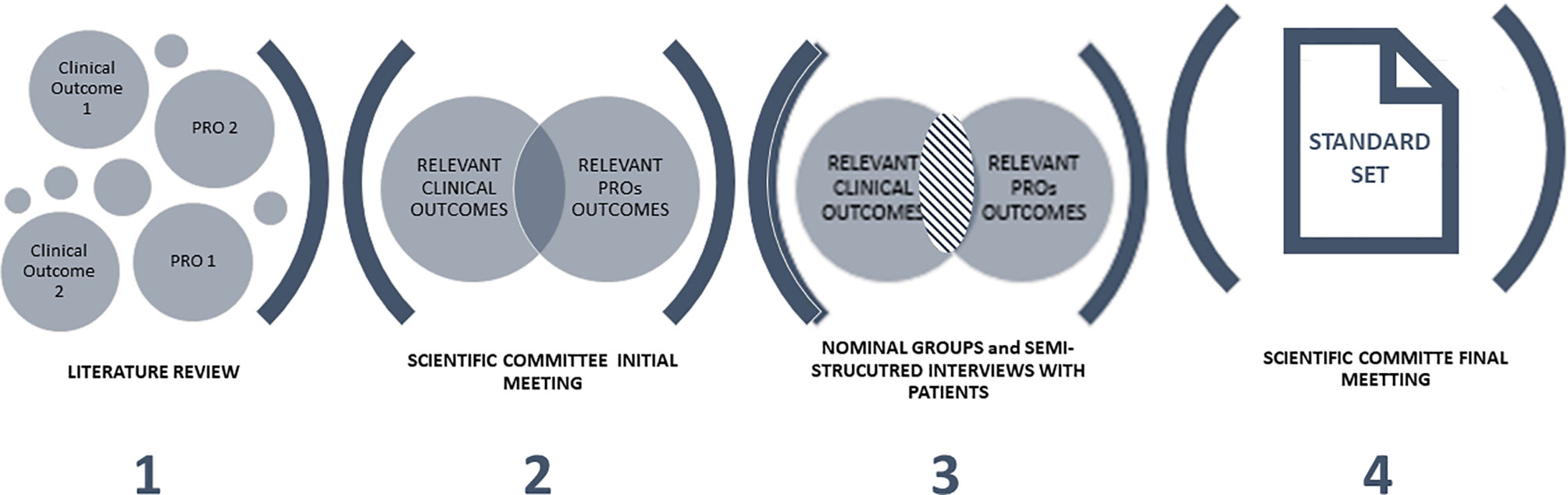
Figure 1 Project phases.
To identify health outcomes [clinical and patient-reported outcomes (PROs)], instruments, and frequency of measurement to be used during SCCHN patient follow-up, a systematic literature review according to the Cochrane Handbook for Systematic Reviews of Interventions (16) (Supplementary Table S1), was carried out in Medline/PubMed. Clinical trials or systematic reviews that include clinical trials in SCCHN, published in English and/or Spanish between 01/01/2016 and 03/31/2019 were reviewed.
The first meeting with the members of the scientific committee aimed to present the project, define the target population and, based on the results of the literature review, select the health outcomes for presenting during the nominal groups.
During the discussion group, the scientific committee screened health outcomes (variable/instrument/frequency of measurement) identified in the literature review and selected them according to their relevance for patient follow-up and availability in the Spanish setting. Moreover, the scientific committee proposed new health outcomes not previously identified in the literature review, but relevant from their perspective.
Five nominal multidisciplinary groups were conducted to reach a consensus on the health outcomes for inclusion in the standard set. Nominal group meetings took place either face-to-face (n=4 meetings) or online (n=1 meeting), depending on participants’ availability to meet.
A nominal group is a qualitative methodology that allows reaching a consensus and ensuring balanced participation among group members, giving them equal opportunities to share their opinions (17). Following the methodological recommendation (18), nominal groups involved five main steps: 1) Introduction and explanation: welcome and description of the purpose and procedure of the meeting; 2) Silent generation of ideas: each participant individually (without consulting or discussing with others) evaluated the health outcomes proposed; 3) Sharing ideas: separately, participants shared the health outcomes they had selected; 4) Group discussion: participants could seek a verbal explanation or further details about any of the health outcomes that other participants had proposed; 5) Voting and ranking: during this phase, participants were asked to prioritize the health outcomes proposed. Health outcomes were included if ≥ 75% of participants agreed on their inclusion. The five nominal groups worked on the same standard set (based on scientific committee proposal). An individual consensus on specific standard set was reached in each of the nominal group.
The participation in each nominal group was limited to a maximum of 12 experts. Nominal groups consisted of experts from different geographic areas of Spain, including medical oncologists, radiation oncologists, otolaryngologists, oral and maxillofacial surgeons, a phoniatrician, primary care specialists, hospital pharmacists, hospital managers, psycho-oncologists, nutritionists, speech therapists, and dentists. Members of the nominal groups were identified by the scientific committee, in collaboration with the study coordinator. They were selected based on their experience in SCCHN management, PRO measurement, implementing strategies to standardize health outcomes, as well as their availability and interest in the project.
To gain patients’ perspectives on the impact of the disease and its treatment on their day-to-day lives, semi-structured telephone interviews (Supplementary Table S2) were conducted with four patient representatives.
The main objective of the last meeting of the scientific committee was to define the final standard set for SCCHN. For this purpose, the agreed health outcomes (clinical and PROs) in each nominal group were presented to the scientific committee. The scientific committee reviewed the individual results of the five nominal groups, ensuring consensus on the health outcomes for which no agreement was reached among the nominal groups. Therefore, if a health outcome did not reach the consensus of inclusion in the five nominal groups, the scientific committee members assessed its inclusion or exclusion from the final standard set. The consensus was reached if ≥ 75% of the members of the scientific committee agreed on the inclusion/exclusion of the health outcome.
Additionally, results from semi-structured interviews with patients were also presented to confirm that the most relevant health outcomes from the patients’ perspective were included in the standard set.
Based on the meeting results, the health outcomes for inclusion in the standard set for SCCHN were defined.
The database search yielded 66 references of which 30 were excluded as their title and abstract contained detailed reviews that did not report health outcomes for patient follow-up. The remaining 36 publications were assessed for eligibility. All of them were selected to be reviewed for qualitative synthesis and identification of health outcomes, measuring instrument, and frequency (Figure 2).
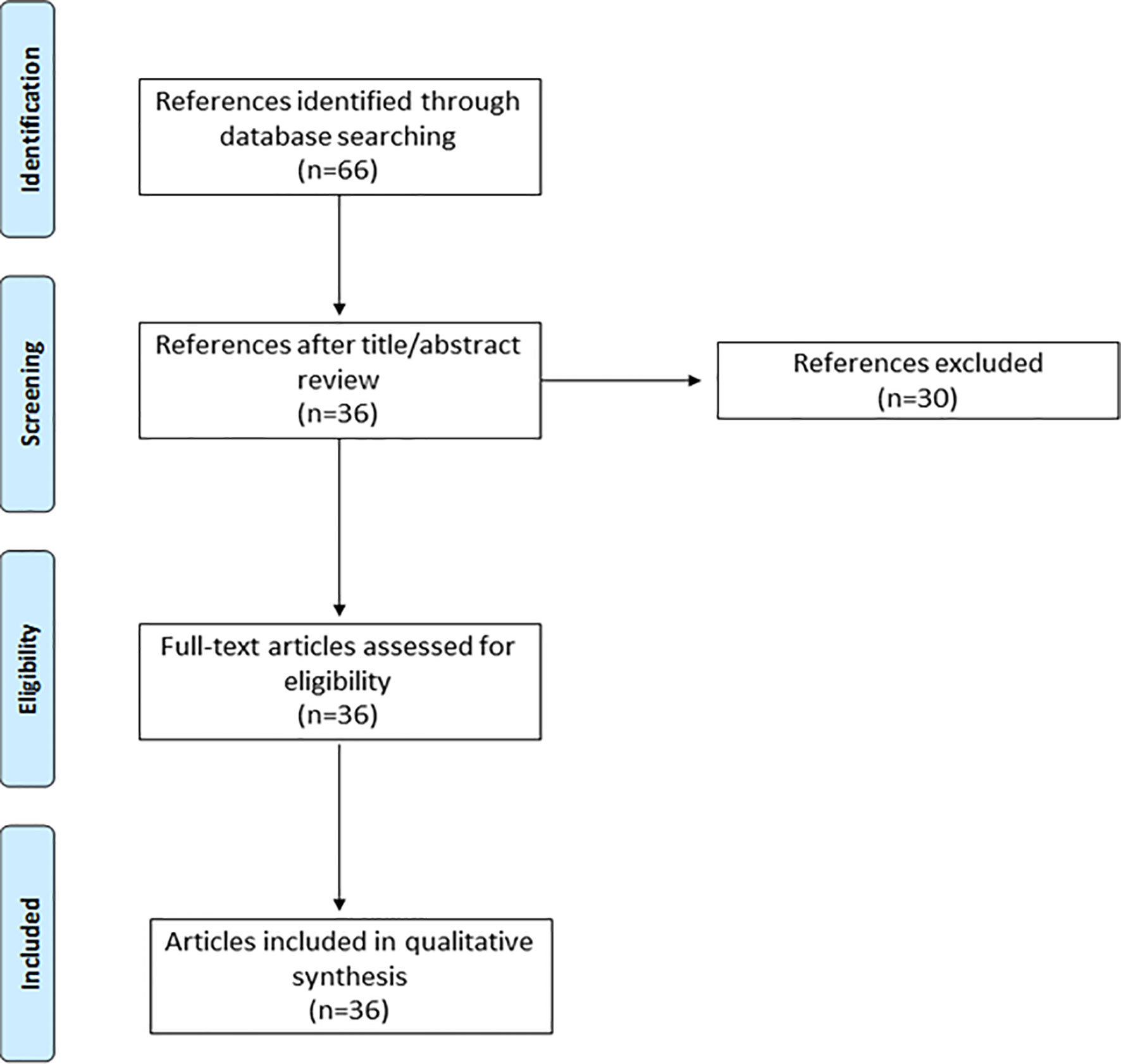
Figure 2 PRISMA flow diagram.
A total of 47 health outcomes were identified in the literature review. They were categorized into case-mix variables (baseline factors that may affect the health outcomes but cannot be controlled as part of the management of the condition and enable patient characterization) (n=27) and 20 outcomes variables (variables for patient follow-up) (n=20) (Supplementary Table S3).
The scientific committee considered 18 out of 27 case-mix and 11 out of 20 outcomes variables previously identified in the literature as being relevant. Moreover, two additional case-mix and nine outcomes variables were proposed. Thus, 20 case-mix and 20 outcomes variables were selected by the scientific committee for presentation and evaluation during the nominal groups (Supplementary Table S4).
The target population of the standard set was also defined. The scientific committee agreed to include all patients with newly-diagnosed SCCHN originating from the oral cavity, oropharynx, hypopharynx and larynx. Head and neck cancers originating from salivary glands, nasopharynx, paranasal sinuses and nasal cavity, and those with a histological type other than squamous, have special characteristics and are subject to specific recommendations and were therefore not included in the target population of this standard set.
A total of 42 experts on SCCHN from different specialties (n=12 medical oncologists, n=4 radiation oncologists, n=6 otolaryngologists, n=2 oral and maxillofacial surgeons, n=1 phoniatrician, n=1 primary care specialist, n=10 hospital pharmacists, n=1 hospital manager, n=2 psycho-oncologists, n=1 nutritionist, n=1 speech therapist, and n=1 dentist) and geographical areas of Spain participated in four nominal group meetings.
The experts agreed to include twelve case-mix and thirteen outcomes variables proposed by the scientific committee in the standard set. Additionally, thirteen new case-mix and thirteen outcomes variables were proposed during the nominal groups (Supplementary Table S5).
Four patient representatives participated in the semi-structured interviews (100% men, age range: 54-82 years).
Patients described the impact of the disease and its treatment on HRQoL, mainly due to disease aftermath. The most common symptoms and side effects reported by patients included dry mouth, oral pain, fatigue and loss of taste and smell. Moreover, several dysfunctions such as speech or voice and swallowing problems were also pointed out.
The disease also harmed patients’ working lives, as most of the patients who were active at the time of diagnosis were unable to return to work.
Based on the consensus reached among nominal groups, the scientific committee assessed the inclusion or exclusion of the new health outcomes proposed and those for which the nominal groups did not reach a consensus.
Case-mix variables are defined as factors that may affect the health outcomes but cannot be controlled as part of the management of the condition. The experts agree to collect at baseline the main sociodemographic factors (age, gender, and social/familiar support), tumor-related factors (tumor localization and sublocalization, cancer staging based on TNM status, and date of diagnosis), clinical factors (alcohol consumption; smoking status, performance status, comorbidities, global patient health status, pain, dysphagia, dysphonia, p16 expression, PD-L1 expression, fragility, and referral to dentistry), and nutritional factors (unintentional weight loss, and dental problem) at the time of diagnosis, before initiating treatment (baseline visits) (Table 1).
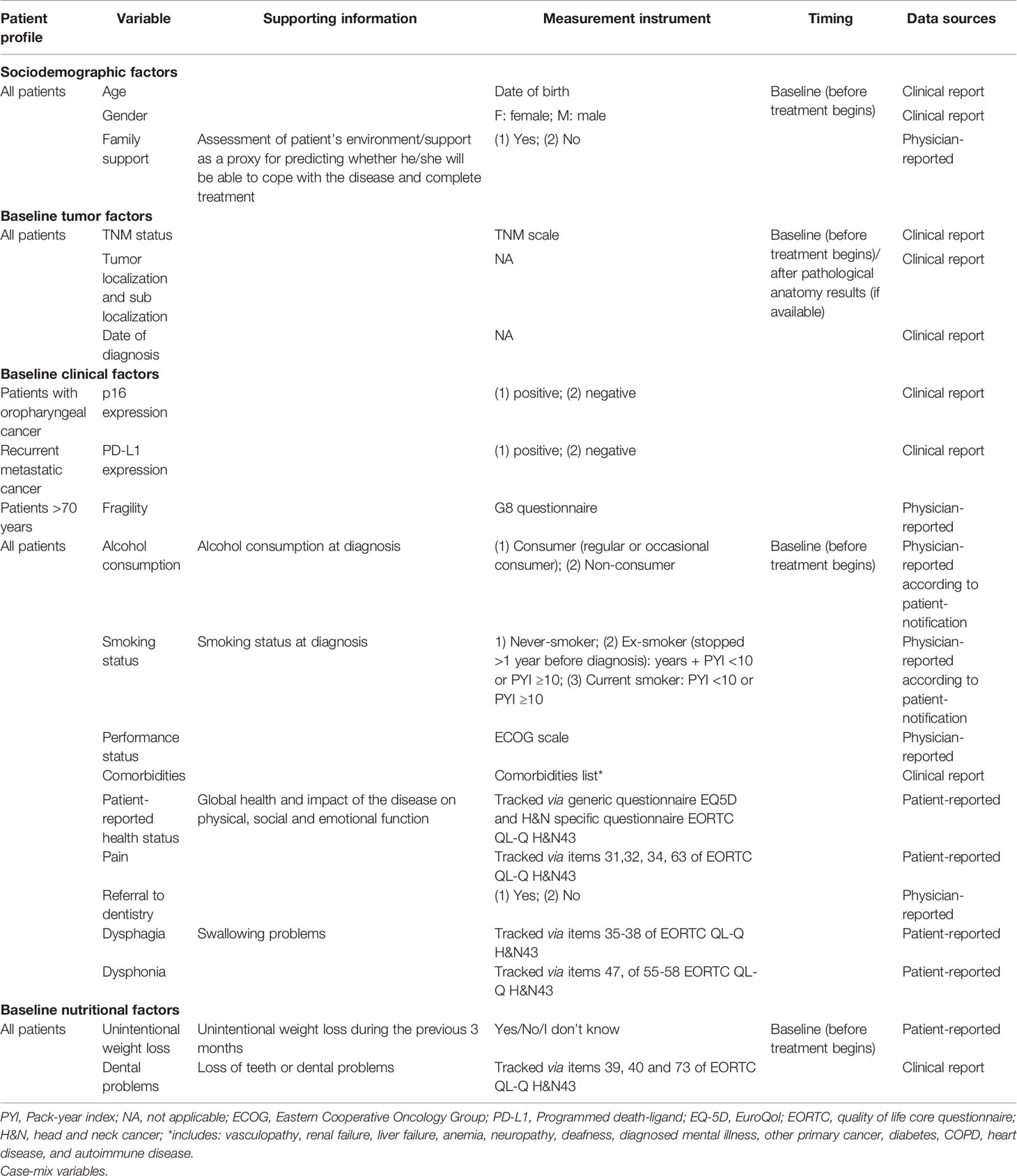
Table 1 Spanish standard set of patient-centered outcomes in SCCHN.
Social/familial support was defined as a proxy for predicting whether the patient would be able to cope with the disease and complete treatment from the physician’s perspective (yes/no).
To standardize the assessment of alcohol consumption, a consensus was reached to classify patients as consumers (regular or occasional) or non-consumers from the patient’s perspective. Similarly, to collect smoking status at diagnosis in a standardized way, the experts agreed to report if the patient was a never-smoker, an ex-smoker (defined as a patient who has stopped at least one year before diagnosis), or a current smoker. For ex-smoker and current smoker patients, it was agreed to record whether the patient’s pack-year index (calculated by multiplying the number of packs of cigarettes smoked per day by the number of years the person has smoked) was < or ≥10.
To systematically report patients’ comorbidities, a list of diseases that can influence treatment and/or clinical practice was developed to select patient comorbidities. The list includes: vasculopathy, renal failure, liver failure, anemia, neuropathy, deafness, diagnosed mental illness, other primary cancer, diabetes, COPD, heart disease, and autoimmune disease.
The experts agreed to use validated questionnaires to assess and collect some of these case-mix variables. To describe patients’ performance status, experts agreed on the use of the Eastern Cooperative Oncology Group (ECOG) scale, which assesses patients’ level of functioning in terms of self-care, carrying out daily activities, and physical ability (19). A generic HRQoL questionnaire (EQ-5D) (20, 21) and head and neck cancer-specific HRQoL questionnaire [EORTC QL-Q H&N43 (22)] were proposed to assess patients’ global health status and the impact of the disease on their social, working and personal function. The use of EORTC QL-Q H&N43 also allows gathering information about patients’ perspective of pain, dysphagia, and dysphonia. And finally, to evaluate patients’ fragility, the experts agreed to complete the G8 questionnaire (23) in patients over 70 years of age.
Outcomes variables establish the evolution of patients’ health status and determine the response (success) in managing the medical condition (Table 2). They are collected during patient follow-up.
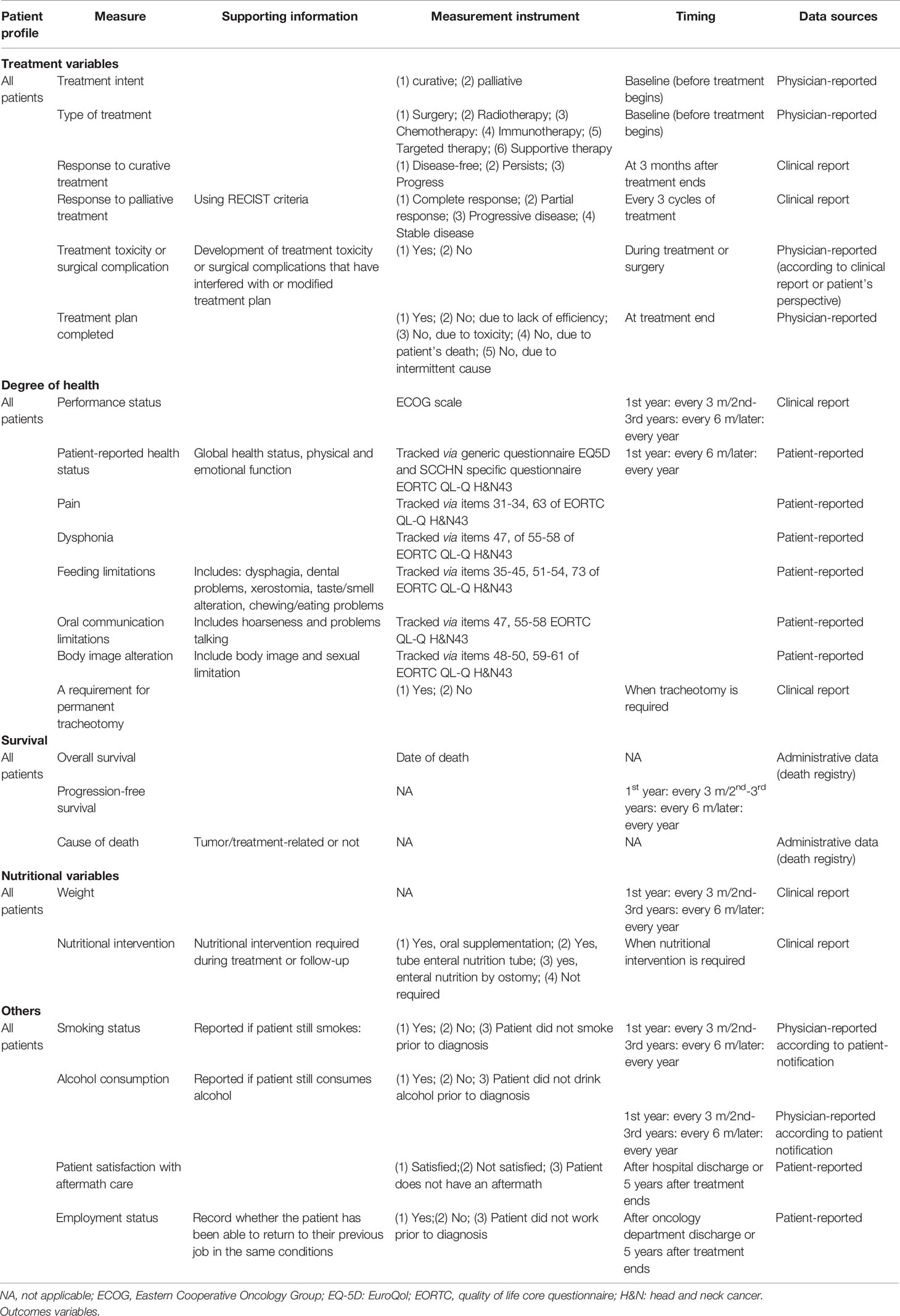
Table 2 Spanish standard set of patient-centered outcomes in SCCHN.
It was agreed to collect, prior to initiating treatment, data on treatment intention and type. For patients that receive curative treatment, the experts reached a consensus on the inclusion of treatment response at three months after end of treatment. For patients receiving palliative treatment, it was agreed to assess response to treatment using RECIST criteria every three cycles of treatment.
The experts agreed to report if the patient had developed treatment toxicity or any surgical complication interfering with or modifying the treatment plan. Finally, the experts considered it relevant to indicate if the patient had completed the treatment plan and, when applicable, record the reason for not doing so.
SCCHN has a negative impact on patients’ performance and health status. Therefore, it was agreed to collect both sets of variables during patient follow-up. As previously indicated, the ECOG scale (19) was selected to assess patients’ performance status, while the EQ-5D (20, 21) and EORTC QL-Q H&N43 (22) were chosen for the assessment of patients’ HRQoL. The use of EORTC QL-Q H&N43 annually during patient follow-up allows the evaluation of the impact of the disease on patients’ lives, including pain, dysphonia, feeding limitations, oral communication limitations, and body image alterations.
Given the significant impact that it can have on patients, it was also agreed to collect information on whether or not the patient requires a permanent tracheotomy.
Overall survival and progression-free survival were considered key variables for inclusion in the standard set for patient follow-up. Moreover, participants agreed on gathering information regarding cause of death, indicating whether it was tumor- or treatment-related.
The disease and its treatment have a negative impact on patients’ nutritional status. For this reason, it was agreed to collect patients’ weight at each visit, and record whether the patient had required nutritional intervention during treatment or follow-up.
It is important to note that the use of EORTC QL-Q H&N43 allows the physician to assess dysphagia, dental problems, xerostomia, taste/smell alterations, and chewing/eating problems that may impact patients’ nutritional status.
Alcohol and tobacco consumption are the main risk factors for SCCHN development, and their maintenance during and/or after treatment is related with recurrence, second neoplasms and tobacco/alcohol-related death. Consequently, it was agreed to record whether the patient continued smoking or consuming alcohol after diagnosis.
SCCHN may also affect patients’ employment status; therefore, the experts agreed to report whether patients can return to their previous job under similar conditions after discharge from the oncology department or five years after end of treatment.
Most patients with SCCHN reported difficulty in access to aftermath care. Therefore, it was agreed to record whether patients were satisfied with the aftermath care received after being discharged from the oncology department and five years after treatment end.
A systematic and standardized collection of health outcomes during follow-up of patients with SCCHN is a crucial step toward a more effective and efficient healthcare system. A holistic approach, integrating all stakeholders’ perspectives, is necessary to ensure the best quality care. To this end, a standard set that includes relevant health outcomes from the perspective of both patients and healthcare professionals is required. The SCCHN standard set defined herein is an excellent opportunity to promote patient-centered care and optimize SCCHN management.
The SCCHN standard set includes 21 outcomes variables. In addition to traditional variables regarding survival or treatment, eight are included related to patients’ degree of health (performance status, patient-reported health status, pain, dysphonia, feeding limitations, oral communication limitations, body image alteration, and need for permanent tracheostomy). Six of them are proposed for tracking via HRQoL questionnaires, EQ-5D-3L and EORTC QL-Q H&N43. SCCHN and its treatment can compromise vital functions, such as breathing, swallowing, and speech. Therefore, the disease can lead to significant physical, emotional, and social problems, reducing patients’ HRQL. Although the collection of HRQoL and other PROs is scarce in clinical practice, the inclusion of these variables in the standard set was considered key to establishing the impact of the disease from the patients’ perspective (24, 25). Due to the lack of resources and the limited knowledge of these questionnaires in clinical practice (26), it was proposed to complete these questionnaires every six months during the first year and then annually. Moreover, by using the EORTC QL-Q H&N43 questionnaire, information about the impact of the disease and its treatment on nutritional status, such as dysphagia, dental problems, dry mouth, sensory problems, taste/smell alterations, problems with chewing, and weight loss, can also be gathered.
Although some healthcare professionals perceive the use of PROs in clinical practice as time-consuming, a one-year pilot study conducted in the Netherlands demonstrated that the ICHOM standard set could be implemented during routine SCCHN treatment without significantly disturbing the everyday workflow (27, 28). The authors concluded that the collection of PROs is not overly time-consuming; however, it requires ad hoc tools and dedicated staff (27, 28).
Providing patient-centered care is essential to move toward high-quality integrated care. Therefore, the inclusion of PROs in the standard set is crucial. Other initiatives have been conducted to promote the use of PROs and patient-reported experiences (PREs) to measure the quality of care, showing that PROs and PREs are promising for measuring and improving the quality and personalization of healthcare in patients with SCCHN (29, 30).
In addition to defining the essential variables for patient follow-up, the experts agreed on those necessary to characterize the patient, the case-mix. The inclusion of these variables is beneficial for benchmarking purposes and for comparing results based on patient profiles.
Data from the implementation of other standard sets in clinical practice has shown benefits from patients’ and clinicians’ perspectives. On the one hand, the inclusion of PROs in the standard set will allow clinicians to focus on the aspects of the disease that most matter to the patient, and therefore encourage better patient engagement in disease management. Moreover, clinicians can learn from the outcomes data they gather, and from the experience of other healthcare professionals in different settings, the standard set thus becoming a valuable tool for benchmarking (31–34).
This project presents several limitations. This standard set reflects the opinion of a group of 50 experts on the management of SCCHN, four patient representatives (all men) and one patient advocacy group representative. Although no significant differences are expected, different groups of experts and patients, including women, could have agreed on various other recommendations. To minimize this potential bias and ensure national representativeness, participants from four broad geographic areas were involved in the project. Secondly, some health outcomes, for instead data regarding surgical details are finally excluded from the standard set. In this regard, it is important to bear in mind that we aim to achieve a minimum, standard set to ensure that at a minimum these health outcomes are collected. In third place, some relevant variables, such as biomarkers may not have been considered when elaborating on the standard set. To minimize this limitation, and due to the continuing advances in both the knowledge and treatment of this disease, we recommend periodically updating the list of biomarkers for evaluation during patient follow-up. We also suggest that the present standard set be regularly updated.
Although this standard set for SCCHN marks a starting point, several barriers need to be overcome on the road to its successful implementation in the Spanish setting. Namely, the time required for the collection of the health outcomes proposed, the lack of digital tools allowing systematic and automatic PRO measurements (PROMs) compilation, together with limited education and information of patients and clinicians about PROs, have been identified as the main barriers to the implementation of the present standard set (35). Newer platforms for data collection, based on information and communication technologies, may reduce the burden on both patient and clinician, as well as data processing time, thus facilitating the use of PROs in clinical practice (36). It is important to notice that, regardless of the platform used to collect the health outcomes of the standard set, they will be included in the patient’s medical record; therefore, the protection of personal data will be guaranteed and will follow the same procedure as the rest of the data in the medical record. Other barriers that must be overcome to ensure the widespread use of this standard set are inherent to the structure of the Spanish national healthcare system (SNHS). Indeed, one of the main characteristics of the SNHS is its heterogeneity: healthcare processes, organizational models as well as information systems differ widely both among and within regions.
Besides addressing these barriers, a further step to promote the integration of the defined standard set into the Spanish healthcare model may involve conducting a pilot implementation study. A pilot study may help establish the feasibility of introducing the standard set in the routine clinical practice, providing insights into the leading resource requirements and organizational challenges to be tackled during implementation.
The standard set defined may pave the way to standardizing the collection of variables in SCCHN and contribute to promoting the incorporation of patient perspective in SCCHN management. In turn, the information provided through the systematic compilation of this set of health outcomes may allow both clinicians and health policymakers to define strategies aimed at achieving high-quality, patient-centered care.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
VA, GC, DC, JG, RM, FM, AR, and AS: contributed equally to this work with data acquisition and data interpretation. JS, AM, and LL contributed to the conceptualization and design of the study. JS and AM did not participate either as members of Scientific Committee or on the selection of members of the Scientific Committee. MC contributed to the conceptualization and design of the study, data acquisition, data analysis, data interpretation and wrote the first draft of the manuscript. All authors contributed to manuscript revision, read and approved the submitted version.
The project was sponsored by Bristol Myers Squibb. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
JS and AM are employees of Bristol Myers Squibb. MC and LL work for an independent research entity that received funding from Bristol Myers Squibb to coordinate and conduct the study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank to all participants in the nominal groups and to the following Spanish Scientific Societies for endorsing the Project: Sociedad Española de Oncología Médica (SEOM), Sociedad Española de Oncología Radioterápica (SEOR), Grupo Español de oncología Radioterápica de Cabeza y Cuello (GEORCC), Sociedad Española de Cabeza y Cuello (SECyC), Sociedad Española de Cirugía Oral y Maxilofacial de Cabeza y Cuello (SECOM-CyC), Sociedad Española de Otorrinolaringología y Cirugía de Cabeza y Cuello (SEORL-CCC), Grupo Español de Tratamiento de Tumores de Cabeza y cuello (TTCC), Fundación para la Excelencia y la Calidad de la Oncología (ECO), Sociedad Española de Medicina Oral (SEMO), Sociedad Española de Farmacia Hospitalaria (SEFH)] and to Spanish patient advocacy group Grupo Español de Pacientes con Cáncer (GEPAC)].
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.747520/full#supplementary-material
1. Orlandi E, Alfieri S, Simon C, Trama A, Licitra L, Group RW. Treatment Challenges in and Outside a Network Setting: Head and Neck Cancers. Eur J Surg Oncol (2019) 45:40–5. doi: 10.1016/j.ejso.2018.02.007
2. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2021) 71:209–49. doi: 10.3322/caac.21660
3. Sociedad Española de Oncología Médica. Las Cifras del Cáncer en España 2020. Soc Española Oncol Médica (2020) 36.
4. Vigneswaran N MDW. Epidemiological Trends in Head and Neck Cancer and Aids in Diagnosis. Oral Maxillofac Surg Clin North Am (2014) 26:123–41. doi: 10.1016/j.coms.2014.01.001
6. Hayes DN, Van Waes C, Seiwert TY. Genetic Landscape of Human Papillomavirus-Associated Head and Neck Cancer and Comparison to Tobacco-Related Tumors. J Clin Oncol (2015) 33:3227–34. doi: 10.1200/JCO.2015.62.1086
7. Iglesias Docampo L, Arrazubi Arrula V, Baste Rotllan N, Carral Maseda A, Cirauqui Cirauqui B, Escobar Y, et al. SEOM Clinical Guidelines for the Treatment of Head and Neck Cancer (2017). Clin Transl Oncol (2017) 20:75–83. doi: 10.1007/s12094-017-1776-1
8. Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy Plus Cetuximab for Squamous-Cell Carcinoma of the Head and Neck. N Engl J Med (2006) 354:567–78. doi: 10.1056/NEJMoa053422
9. Roman B, Goldenberg D, Givi B. AHNS. Adult Height and Head and Neck Cancer: A Pooled Analysis Within the INHANCE Consortium. Head Neck (2016) 38:168–74. doi: 10.1002/hed.24100
10. Nelke KH, Pawlak W, Gerber H, Leszczyszyn J. Head and Neck Cancer Patients’ Quality of Life. Adv Clin Exp Med (2014) 23:1019–27. doi: 10.17219/acem/37361
11. Mañós M, Giralt J, Rueda A, Cabrera J, Martinez-Trufero J, Marruecos J, et al. Multidisciplinary Management of Head and Neck Cancer: First Expert Consensus Using Delphi Methodology From the Spanish Society for Head and Neck Cancer (Part 1). Oral Oncol (2017) 70:58–64. doi: 10.1016/j.oraloncology.2017.04.004
12. Rueda A, Giralt J, Mañós M, Lozano A, Sistiaga A, García-Miragall E, et al. Multidisciplinary Management of Head and Neck Cancer: First Expert Consensus Using Delphi Methodology From the Spanish Society for Head and Neck Cancer (Part 2). Oral Oncol (2017) 70:65–72. doi: 10.1016/j.oraloncology.2017.04.005
13. Chen J, Ou L, Hollis SJ. A Systematic Review of the Impact of Routine Collection of Patient Reported Outcome Measures on Patients, Providers and Health Organisations in an Oncologic Setting. BMC Health Serv Res (2013) 13:211. doi: 10.1186/1472-6963-13-211
14. Porter M, Larsson S, Lee T. Standardizing Patient Outcomes Measurement Michael. N Engl Med (2016) 374:504–6. doi: 10.1056/NEJMp1511701
16. Higgins J, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration (2011). Available from handbook.cochrane.org.
17. Gallagher M, Hares T, Spencer J, Bradshaw C, Webb I. The Nominal Group Technique: A Research Tool for General Practice? Fam Pract (1993) 10:76–81. doi: 10.1093/fampra/10.1.76
18. Potter M, Gordon S, Hamer P. The Nominal Group Technique: A Useful Consensus Methodology in Physiotherapy Research. New Zeal J Physiother (2004) 32:126–30.
19. Oken MM, Creech R, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and Response Criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol (1982) 5:649–55. doi: 10.1097/00000421-198212000-00014
20. Tsang HHL, Cheung JPY, Wong CKH, Cheung PWH, Lau CS, Chung HY. Psychometric Validation of the EuroQoL 5-Dimension (EQ-5D) Questionnaire in Patients With Spondyloarthritis. Arthritis Res Ther (2019) 21:41. doi: 10.1186/s13075-019-1826-x
21. Badia X, Roset M, Montserrat S, Herdman M, Segura A. The Spanish Version of EuroQol: A Description and Its Applications. European Quality of Life Scale. Med Clin (Barc) (1999) 112 Suppl:79–85.
22. Singer S, Amdal CD, Hammerlid E, Tomaszewska IM, Castro Silva J, Mehanna H, et al. International Validation of the Revised European Organisation for Research and Treatment of Cancer Head and Neck Cancer Module, the EORTC QLQ-HN43: Phase Iv. Head Neck (2019) 41:1725–37. doi: 10.1002/hed.25609
23. Bellera CA, Rainfray M, Mathoulin-Pélissier S, Mertens C, Delva F, Fonck M, et al. Screening Older Cancer Patients: First Evaluation of the G-8 Geriatric Screening Tool. Ann Oncol (2012) 23:2166–72. doi: 10.1093/annonc/mdr587
24. Silveira A, Monteiro E, Sequeira T. Head and Neck Cancer: Improving Patient-Reported Outcome Measures for Clinical Practice. Curr Treat Options Oncol (2018) 19(11):59. doi: 10.1007/s11864-018-0578-1
25. Porter I, Gonçalves-Bradley D, Ricci-Cabello I, Gibbons C, Gangannagaripalli J, Fitzpatrick R, et al. Framework and Guidance for Implementing Patient-Reported Outcomes in Clinical Practice: Evidence, Challenges and Opportunities. J Comp Eff Res (2016) 5:507–19. doi: 10.2217/cer-2015-0014
26. McHorney CA, Earl Bricker D. A Qualitative Study of Patients’ and Physicians’ Views About Practice-Based Functional Health Assessment. Med Care (2002) 40:1113–25. doi: 10.1097/00005650-200211000-00012
27. van Meerbeeck J, De Backer L, Hiddinga B, Janssens A. Pilot Trial of the ICHOM Lung Cancer Standard Set, European Respiratory Society (ERS). (2017) 50:PA4234. doi: 10.1183/1393003.congress-2017.PA4234
28. Van Meerbeeck J, De Backer L, Janssens A, Hiddinga B, Vanhoutte G. P1.04-028 Collection of ICHOM-Defined Patient-Reported Outcome Measures (PROMs) During Routine Lung Cancer Treatment: A Pilot Study. J Thorac Oncol (2017) 12:S612. doi: 10.1016/j.jtho.2016.11.784
29. Van Overveld LFJ, Takes RP, Braspenning JCC, Smeele LE, Merkx MAW, Hermens RPM. Quality of Dutch Integrated Head and Neck Cancer Care: Measurements and Evaluation. J Clin Oncol (2017) 35:209–9. doi: 10.1200/JCO.2017.35.8_suppl.209
30. Head and Neck Audit (HANA Project). Available at: https://HanaKillermultimediaCom/n.d.
31. Arora J, Haj M. Implementing Ichom’S Standard Sets of Outcomes: Cleft Lip and Palate at Erasmus University Medical Centre in the Netherlands. London, UK: International Consortium for Health Outcomes Measurement (ICHOM) (2016). Available at: www.ichom.org.
32. Arora J, Tavella R. Implementing Ichom’s Standard Sets of Outcomes: Coronary Artery Disease in the Coronary Angiogram Database of South Australia (CADOSA). London, UK: International Consortium for Health Outcomes Measurement (ICHOM) (2017). Available at: www.ichom.org.
33. Arora J, Lewis S, Cahill MA, Arora J. Implementing Ichom’s Standard Set of Outcomes: Parkinson’s Disease at Aneurin Bevan University Health Board in South Walles, Uk. London, UK: International Consortium for Health Outcomes Measurement (ICHOM) (2017). Available at: www.ichom.org.
34. Ackerman IN, Cavka B, Lippa J, Bucknill A. The Feasibility of Implementing the ICHOM Standard Set for Hip and Knee Osteoarthritis: A Mixed-Methods Evaluation in Public and Private Hospital Settings. J Patient Rep Outcomes (2018) 2:32. doi: 10.1186/s41687-018-0062-5
35. Alonso-Caballero J, Ferrer-Fores M. Monografías de Política Y Gestión. Resultados Reportados Por Los Pacientes (PROs). 1a ed. Madrid: Ergon (2017).
Keywords: head and neck cancer, patient-centered care, outcome measurement, patient-reported outcomes, patient centricity, quality of life
Citation: Arrazubi V, Cajaraville G, Cantero D, Giralt J, Mesia R, Monje F, Rueda A, Sistiaga A, Suarez J, Mut A, Comellas M and Lizán L (2022) Defining a Standard Set of Health Outcomes for Patients With Squamous Cell Carcinoma of the Head and Neck in Spain. Front. Oncol. 11:747520. doi: 10.3389/fonc.2021.747520
Received: 26 July 2021; Accepted: 24 December 2021;
Published: 24 January 2022.
Edited by:
Gyorgy B. Halmos, University Medical Center Groningen, NetherlandsReviewed by:
Oliver Riesterer, Aarau Cantonal Hospital, SwitzerlandCopyright © 2022 Arrazubi, Cajaraville, Cantero, Giralt, Mesia, Monje, Rueda, Sistiaga, Suarez, Mut, Comellas and Lizán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Lizán, bGl6YW5Ab3V0Y29tZXMxMC5jb20=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.