 Nicolò Bizzarri1
Nicolò Bizzarri1 Nazario Foschi2
Nazario Foschi2 Matteo Loverro1
Matteo Loverro1 Lucia Tortorella1
Lucia Tortorella1 Francesco Santullo3
Francesco Santullo3 Andrea Rosati1
Andrea Rosati1 Salvatore Gueli Alletti1Barbara Costantini1Valerio Gallotta1Gabriella Ferrandina1,4Anna Fagotti1,4Francesco Fanfani1,4
Salvatore Gueli Alletti1Barbara Costantini1Valerio Gallotta1Gabriella Ferrandina1,4Anna Fagotti1,4Francesco Fanfani1,4 Alfredo Ercoli5
Alfredo Ercoli5 Vito Chiantera6
Vito Chiantera6 Giovanni Scambia1,4
Giovanni Scambia1,4 Giuseppe Vizzielli1,7*
Giuseppe Vizzielli1,7*- 1Unità Operativa Complessa (UOC) Ginecologia Oncologica, Dipartimento per la salute della Donna e del Bambino e della Salute Pubblica, Fondazione Policlinico Universitario A. Gemelli, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy
- 2UOC Clinica Urologica, Dipartimento Scienze Mediche e Chirurgiche, Fondazione Policlinico Universitario A. Gemelli, IRCCS, Rome, Italy
- 3UOC Chirurgia Peritoneo e Retroperitoneo, Dipartimento Scienze Mediche e Chirurgiche, Fondazione Policlinico Universitario A. Gemelli, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS), Rome, Italy
- 4Università Cattolica del Sacro Cuore, Rome, Italy
- 5Department of Gynecologic Oncology and Minimally-Invasive Gynecologic Surgery, Università Degli Studi di Messina, Policlinico G. Martino, Messina, Italy
- 6ARNAS Ospedali Civico Di Cristina Benfratelli, Department of Gynecologic Oncology, University of Palermo, Palermo, Italy
- 7Obstetrics and Gynecology Department, Academic Hospital of Udine, Department of Medicine, University of Udine, Udine, Italy
Introduction: Pelvic exenteration performed for recurrent/persistent gynecological malignancies has been associated with urological short- and long-term morbidity due to altered vascularization of tissues for previous radiotherapy. The aims of the present study were to describe the use of intravenous indocyanine green (ICG) to assess vascularity of urinary diversion (UD) after pelvic exenteration for gynecologic cancers, to evaluate the feasibility and safety of this technique, and to assess the postoperative complications.
Methods: Prospective, observational, single-center, pilot study including consecutive patients undergoing anterior or total pelvic exenteration due to persistent/recurrent gynecologic cancers between August 2020 and March 2021 at Fondazione Policlinico Gemelli IRCCS, Rome, Italy. All patients underwent intravenous injection of 3–6 ml of ICG (1.25 mg/ml) once the UD was completed. A near-infrared camera was used to evaluate ICG perfusion of anastomoses (ileum–ileum, right and left ureter with small bowel, and colostomy or colorectal sides of anastomosis) a few seconds after ICG injection.
Results: Fifteen patients were included in the study. No patient reported adverse reactions to ICG injection. Only 3/15 patients (20.0%) had an optimal ICG perfusion in all anastomoses. The remaining 12 (80.0%) patients had at least one ICG deficit; the most common ICG deficit was on the left ureter: 3 (20.0%) vs. 1 (6.7%) patient had no ICG perfusion on the left vs. right ureter, respectively (p = 0.598). 8/15 (53.3%) and 6/15 (40.0%) patients experienced grade ≥3 30-day early and late postoperative complications, respectively. Of these, two patients had early and one had late postoperative complications directly related to poor perfusion of anastomosis (UD leak, ileum–ileum leak, and benign ureteric stricture); all these cases had a suboptimal intraoperative ICG perfusion.
Conclusion: The use of ICG to intraoperatively assess the anastomosis perfusion at time of pelvic exenteration for gynecologic malignancy is a feasible and safe technique. The different vascularization of anastomotic stumps may be related to anatomical sites and to previous radiation treatment. This approach could be in support of selecting patients at higher risk of complications who may need personalized follow-up.
Introduction
Pelvic exenteration is a major radical operation that represents the last curative option in recurrent/persistent gynecologic cancers previously treated with radiotherapy (1, 2). In selected patients in whom this surgical procedure is performed with curative intent, overall survival ranges from 20% to 73% at 5 years (2–4). In view of the promising oncological outcomes, gynecologic oncologists have recently pushed the boundaries and stretched the indication of such surgery to patients with pelvic sidewall involvement (5, 6), previously deemed inoperable.
Different studies have reported the perioperative morbidity associated with pelvic exenteration (7). In particular, postoperative complications range from 51% to 82%, of which 22%–32% are major complications (1, 7). The anterior part of pelvic exenteration contemplates the reconstruction by urinary diversion (UD) that can be performed with different techniques (8). UD options (orthotopic neobladder, continent and incontinent diversions) require anastomosis of the ureters with selected bowel segments; among UD, ileal conduit continues to be the most widely UD used after pelvic exenteration for gynecologic malignancies (8–10). A wide range of complications are not only related to the pelvic exenteration but specifically to UD: 45% of patients experience functional complications after 5 years, 50% at 10 years, and 94% at 15 years (11). Despite the multiple variations in uretero-enteric anastomosis, ureteric fistula and benign ureteric stricture represent short- and long-term complications associated with ileal conduit urinary diversion in 5%–22% and 3%–27% of cases, respectively (8, 12).
Benign ureteric strictures are mainly related to ischemic-inflammatory mechanisms or surgical technique (poor preservation of ureteral vascular supply, ureteral handling and mobilization, tension of anastomosis, tightness of suture, etc.) (13, 14), and they are associated with urinary tract infections and potential detrimental effects on renal function.
Ischemia has been considered a key factor associated with anastomosis complications, leading to prolonged hospitalization, septic complications, hospital readmission, need for invasive interventions, and finally loss of the renal unit (15, 16).
Very recently, indocyanine green (ICG) fluorescence has been proposed as a tool to assess tissue perfusion. ICG becomes fluorescent when excited with near-infrared light, allowing for its detection within tissue with specially designed cameras. ICG has gained wide applicability in different fields of surgery, including the assessment of anastomosis and flap perfusion (17, 18). In particular, intravenously administered ICG is used to identify vessel perfusion and differentiate tissue density (19). Very few studies have assessed the use of intravenous ICG to check vascularity of ileal conduit UD, showing that ICG was useful to reduce the incidence of benign ureteric strictures (20, 21). However, no study was performed in patients with gynecologic cancers, particularly after treatment with pelvic radiotherapy.
The aims of the present study were to describe the use of ICG to assess vascularity of UD after pelvic exenteration for gynecologic cancers to evaluate the feasibility and safety of this technique and to assess the postoperative complications.
Methods
This is a prospective, observational, pilot study. The present study was approved by the institutional review board (number DIPUSVSP-27-07-20108). Consecutive patients undergoing anterior or total pelvic exenteration due to persistent or recurrent gynecologic cancers between August 2020 and March 2021 at Fondazione Policlinico Gemelli IRCCS, Rome, Italy, were included. Women older than 18 years with histological diagnosis of cervical, vulvar, vaginal, or endometrial cancer previously treated with (chemo)radiotherapy or with chemotherapy only were included; patients with allergy to iodine, who underwent posterior exenteration only, and who underwent ureterostomy were excluded. Pelvic exenteration was performed with the attempt to remove pelvic organs in one single specimen and with the aim of achieving tumor-free surgical margins. The surgical approach was open or minimally invasive according to the patient’s body mass index (BMI) and to the tumor’s maximum diameter at preoperative imaging (22). All patients underwent intravenous injection of 3–6 ml of ICG (1.25 mg/ml) once the UD was completed. All ileal conduits were performed by the same urologist (NF), and the decision to perform Bricker–Nelaton vs. Wallace type I (medial-posterior wall continuous suture) (8) uretero-enteric anastomosis technique was taken according to the appearance, availability, and mobility of the distal ureters after the oncological resection and previous radiotherapy. A near-infrared laparoscopic camera (Olympus, Tokyo, Japan) or the SPY Portable Handheld Imager (SPY-PHI) (Stryker, Kalamazoo, MI, USA) was used to evaluate ICG perfusion a few seconds after intravenous ICG injection (Figure 1A). Contrast fluorescence mode demonstrated ICG fluorescence in perfused tissues as white against a black/gray background (Figure 1B). Color-segmented fluorescence was used to show different levels of ICG uptake demonstrating higher levels of perfusion (Figure 1C). After ICG injection, a four-tier (+++ vs. ++- vs. + - - vs. - - -) classification was used to assess the vascularity (ICG perfusion) of each anastomosis: ileum–ileum, right and left ureter with small bowel, and colostomy or colorectal sides of anastomosis (in case of total pelvic exenteration). Ureter perfusion was analyzed separately even in case of Wallace type I anastomosis. The classification of ICG perfusion of anastomoses was performed by two independent assessors: the urologist and the gynecologic oncologist. In case of conflict, a third opinion from a gynecologic oncologist was requested to solve the conflict. In view of the observational nature of the present study, no surgical action was taken in case of poor ICG perfusion of the anastomoses.
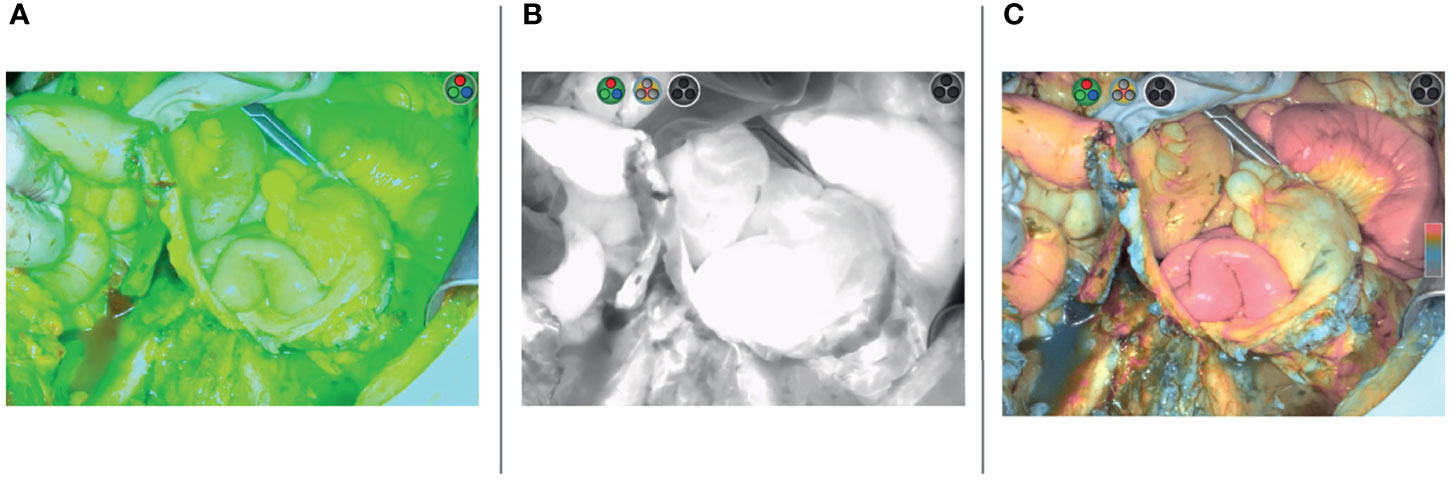
Figure 1 Wallace ileal conduit uretero-enteric anastomoses indocyanine green (ICG) perfusion demonstrated with three different modalities: overlay fluorescence mode (A), contrast fluorescence mode (B), color segmented fluorescence mode (C).
Postoperative complications were graded according to Clavien–Dindo classification system (23), and they were divided into early (between date of pelvic exenteration and 30th postoperative day) and late (from 31st to 180th postoperative day).
All patients underwent radiologic assessment of the abdomen 3 months after the pelvic exenteration (CT scan, MRI scan, or ultrasound scan) to check for any sign of hydronephrosis.
Statistical Analysis
A sample of at least 12 patients was considered adequate for a descriptive pilot study (24).
Standard descriptive statistics was used: median with range and incidence with percentage were used to report continuous and categorical variables, respectively. Student’s t-test and chi-square test were used to compare continuous and categorical variables, respectively. ICG perfusion was assessed in two ways: comparing poor (- - -/+ - -) vs. good (++-/+++) (Figure 2) ICG perfusion and comparing any ICG deficit vs. optimal ICG vascularization (optimal vascularization was defined as such, if all anastomoses had maximum ICG perfusion +++). Logistic regression analysis was performed to estimate variables related to negative perioperative outcomes.
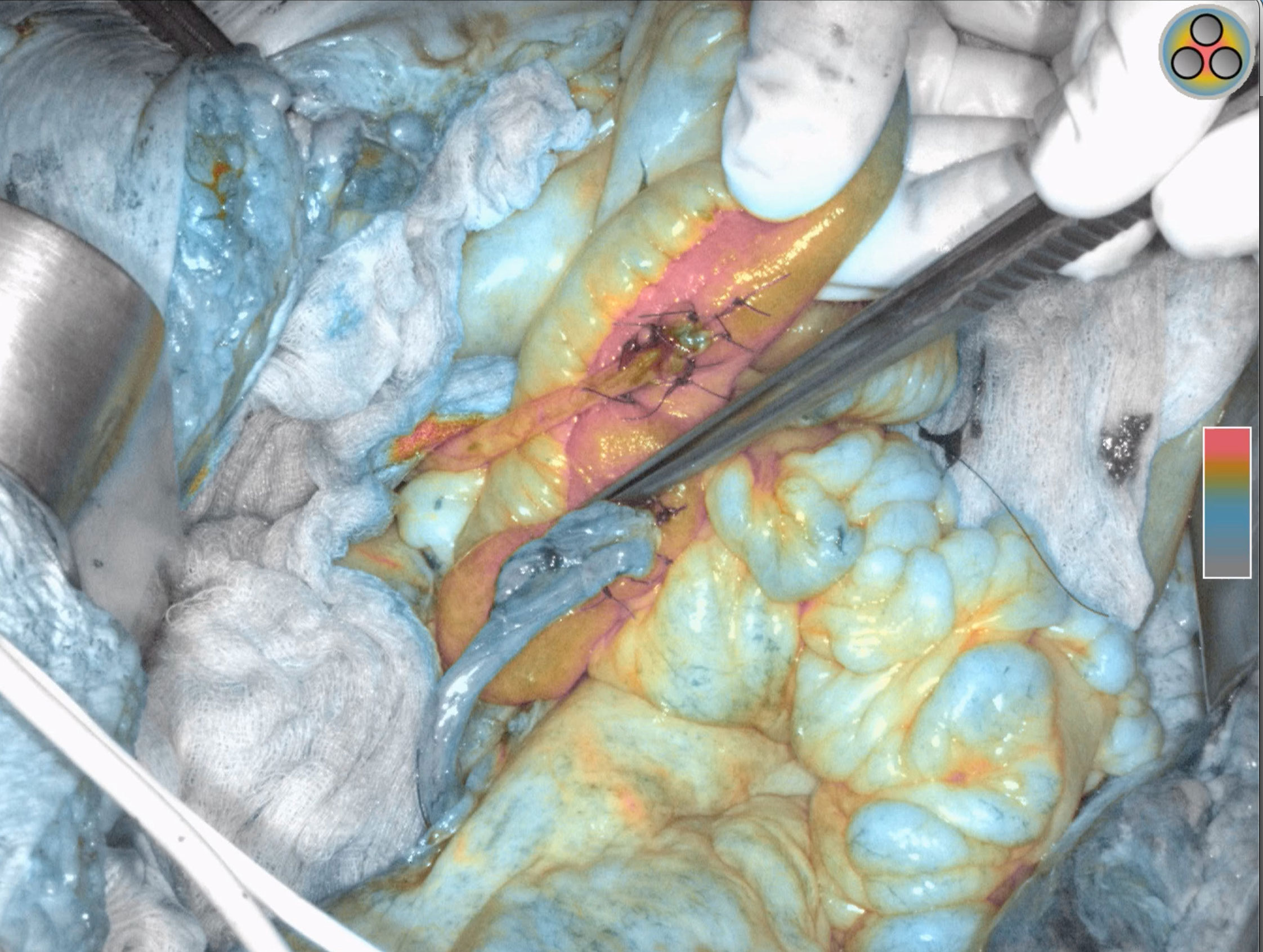
Figure 2 Bricker ileal conduit uretero-enteric anastomoses demonstrating right ureter with optimal indocyanine green (ICG) perfusion (+++) vs. left ureter with poor ICG perfusion (- - -).
Results
Fifteen patients were included in the study. Clinical characteristics of the entire cohort are demonstrated in Table 1. All but one patient (93.3%) underwent previous treatment with radiotherapy or chemoradiotherapy. Seven (46.7%) patients were operated on for persistent disease and eight (53.3%) for recurrent disease. The most common site of primary cancer was the cervix (12, 80.0%), and most patients underwent total pelvic exenteration (10, 66.7%). One (6.7%) patient underwent minimally invasive pelvic exenteration, while the remaining underwent open approach.
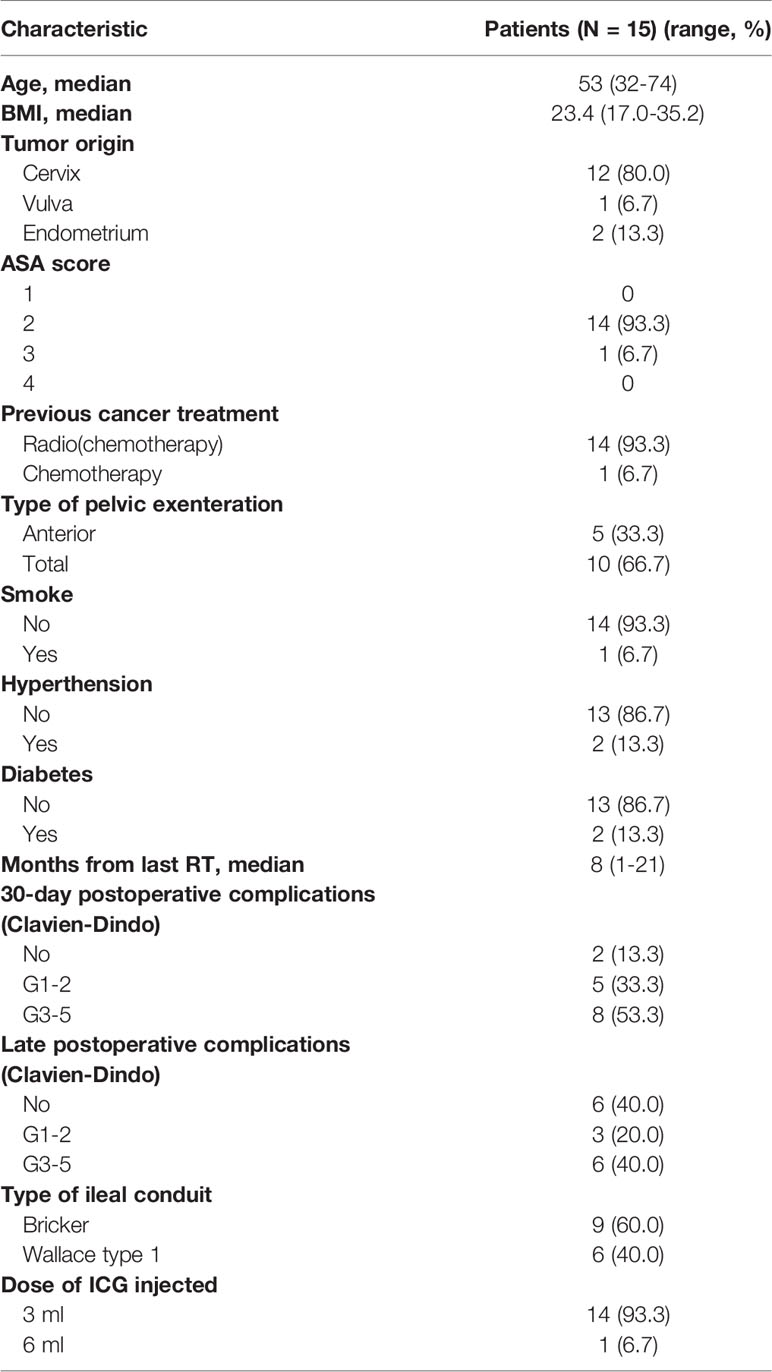
Table 1 Patients’ characteristics.
No patient reported adverse reactions to ICG injection. Only 3/15 patients (20.0%) had an optimal ICG perfusion (+++) in all anastomoses. The remaining 12 (80.0%) patients had at least one ICG deficit; the most common ICG deficit was on the left ureter: 3 (20.0%) vs. 1 (6.7%) patient had no ICG perfusion (- - -) on the left vs. right ureter, respectively (p = 0.598). Out of 30 ureters analyzed separately, 20 (66.7%) had good (++-/+++) while 10 (33.3%) had poor (- - -/+ - -) ICG perfusion. Table 2 shows the grading of ICG perfusion in different anastomoses. No difference was seen when comparing poor (- - -/+ - -) vs. good (++-/+++) ICG perfusion between right vs. left ureter (p = 0.700). Moreover, both types of cameras were used and no differences were noted between them (data not shown).
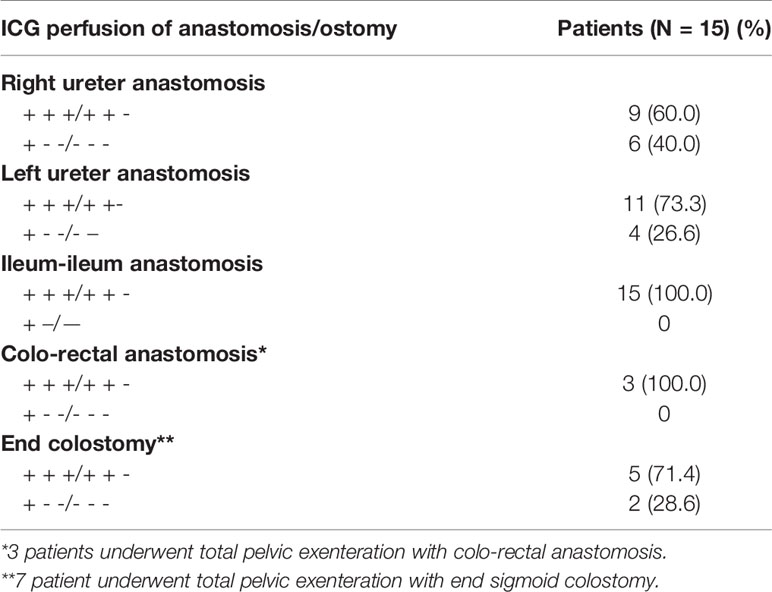
Table 2 Indocyanine green (ICG) perfusion according to different anastomoses.
Two (13.3%) patients did not experience early postoperative complications. Among the remaining patients, five (33.3%) had grade 2, three (20.0%) had grade 3a, three (20.0%) had grade 3b, and two (13.3%) had grade 4 early postoperative complications. Two (13.3%) patients had early postoperative complications that can be directly attributed to an impaired vascularization of the anastomosis. One patient had a leak of uretero-enteric anastomosis in the Bricker ileal conduit: this patient had an intraoperative perfusion of the left ureter that was classified as - - -; the second patient had a leak of ileo-ileal anastomosis: this anastomosis was intraoperatively classified as ++-. No patient developed necrotic ischemia of the ileal conduit.
The median time of follow-up was 4.5 months (range, 1–7). Six (40.0%) patients did not experience late postoperative complications; three (20.0%) patients had grade 2, three (20.0%) patients had grade 3a, and one (6.7%) patient had grade 3b. Two patients (13.3%) died of late complications: one had a fistula between external iliac artery and small bowel with following sepsis, and the other had a sepsis of pulmonary origin. Regarding anastomosis vascularity complications, one patient (6.7%) had left benign ureteric stricture at 47th postoperative day. The left ureter in this patient was intraoperatively judged with a - - - ICG perfusion.
Table 3 demonstrates the correlation between ICG perfusion of all anastomoses and clinical outcomes. None of the analyzed outcomes was significantly related to a poor or a better ICG perfusion of all anastomoses.
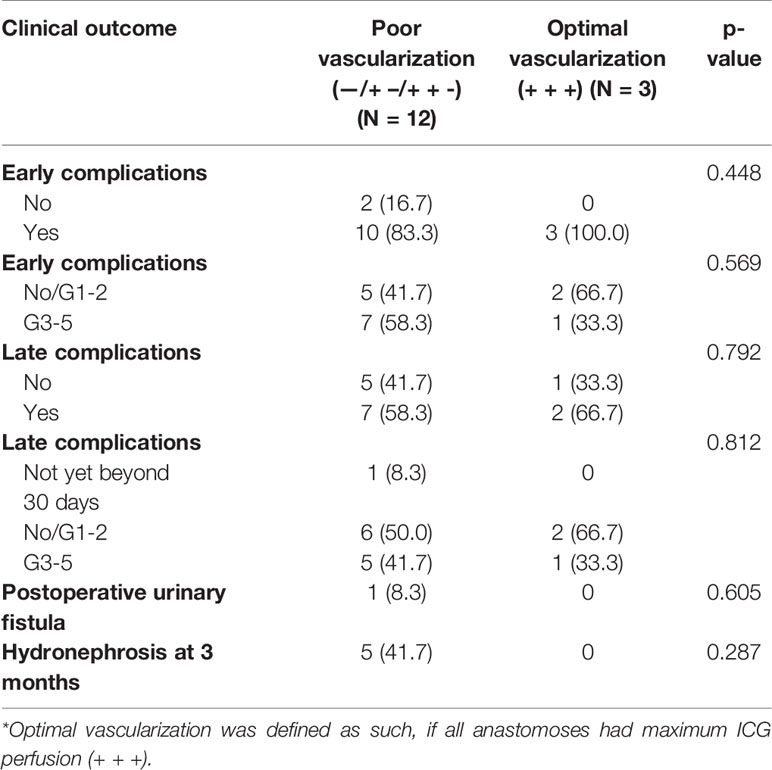
Table 3 Correlation between indocyanine green (ICG) perfusion of all anastomoses* and clinical outcomes.
When we compared the type of uretero-enteric anastomosis technique in UD performed, we noted that patients who underwent Bricker anastomosis technique had a higher chance to have any deficit in ICG perfusion compared to Wallace type I anastomosis technique (9, 100.0% in Bricker vs. 3, 50.0% in Wallace type I; p = 0.044). When we analyzed the 30 ureters separately, we noted that there was no difference in the ICG perfusion between the two anastomosis techniques (good perfusion ++-/+++ in 10/18, 55.6% vs. 10/12, 83.3% patients, respectively; p = 0.235).
Similarly, there was no statistically significant relation between the type of early postoperative complication (no complications/G1–2 vs. G3–4) and the ICG perfusion to any anastomosis (p = 0.569). Moreover, no difference between no/G1–2 vs. G3–4 late complications according to ICG perfusion was noted (p = 0.812) (Table 3).
Table 4 represents a logistic regression analysis of variables associated with 30-day grade 3–4 postoperative complications. None of the analyzed variables was significantly associated with early postoperative complications.
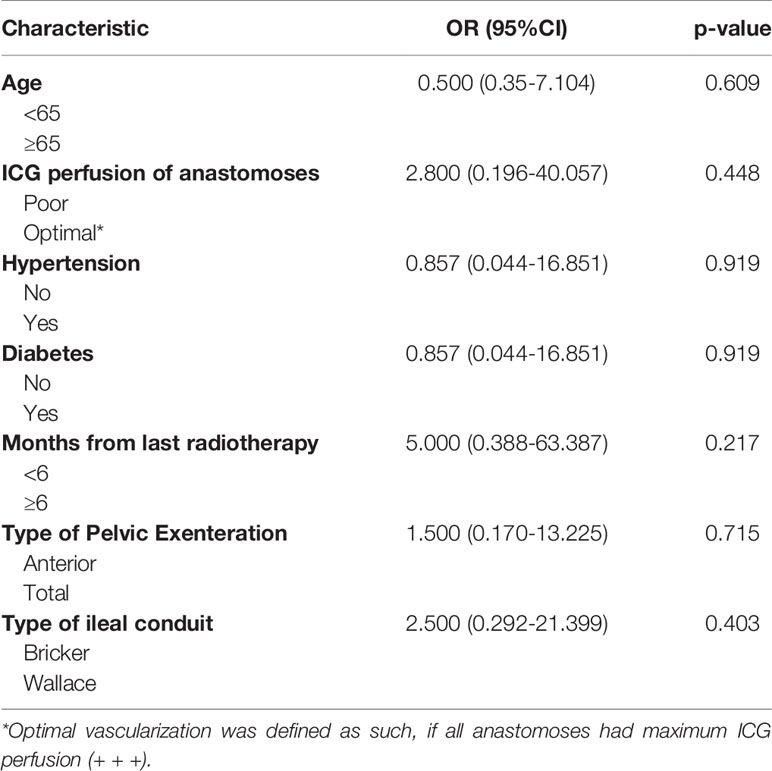
Table 4 Logistic regression analysis of variables associated with 30-day grade 3–4 postoperative complications.
Discussion
With the present study, we aimed to describe the use of ICG to assess vascularity of ileal conduit UD, uretero-enteric anastomosis, and intestinal anastomosis after pelvic exenteration for gynecologic cancers and to assess postoperative complications. With the power of a pilot study, therefore with a limited number of patients, we showed that only 20.0% of patients had optimal ICG perfusion in all anastomoses; this is most likely due to the fact that almost all included patients (93.3%) underwent previous treatment with radio(chemo)therapy. To the best of our knowledge, this is the first report to describe the use of ICG to assess vascularity of UD, uretero-enteric anastomosis, and ileo-ileal anastomosis in patients who previously underwent radiotherapy; moreover, it is the first study that assess ileal conduit perfusion with ICG in patients with gynecologic malignancies.
The main objective of intraoperative assessment of anastomosis vascularization is to reduce the incidence of postoperative complications that may be directly related to poor perfusion, such as leak/fistula and benign strictures. In our series, we documented one leak of uretero-enteric anastomosis and one benign ureteric stricture; in both cases, there was a poor vascularization of the ureteric stump (- - -). Interestingly, this happened in the left ureter; even though not statistically significant, the left ureter was more frequently impacted by a poor vascularization. This may be due to the mobilization of the left ureter during the formation of the ileal conduit with consequent perfusion impairment (15). Moreover, when looking at the vascularization of patients with Bricker vs. Wallace type I uretero-enteric anastomosis, we noted that Bricker conduit was less likely to have both ureters with optimal vascularization; nevertheless, there is large evidence in literature showing no difference in short- and long-term outcomes when Bricker is compared to Wallace techniques (25).
Few urology studies have reported the use of ICG to intraoperatively assess vascularization of uretero-enteric anastomosis after radical cystectomy (13, 14). The main result reported by these Authors was the reduced incidence of benign ureteric strictures when perfusion was analyzed with ICG. Particularly, poor distal perfusion required further ureter re-excision, leading to a significant per-ureter reduction of ureteric strictures [from 7.5% to 0% in one study (13) and from 6.6% to 0% in the other study (14)]. The present study was designed as a prospective observational study to assess the feasibility and safety of ICG use after radiation therapy in patients undergoing pelvic exenteration and to evaluate the outcomes of different ICG perfusions; therefore, the surgery was not modified according to intraoperative findings. Further interventional studies with re-excision of poorly perfused stumps may be necessary to better understand the potential role of ICG to reduce short- and long-term postoperative complications.
The main limitations of the present study are represented by the small sample size and the short follow-up period that prevent to draw solid conclusions. Selection bias to choose UD anastomosis technique may also be considered as a potential limitation such as the subjectivity of the evaluation. However, since the introduction of artificial intelligence is revolutionizing surgery, the combination of endoscopy with fluorescence imaging with ICG read by bioinformatics software could be in the future a forward-looking modality to enhance surgical precision and reduce postoperative complications while improving oncologic and functional outcomes with a better quality of life.
Other potential biases of the perfusion of the ileal conduit such as BMI or concomitant cardiovascular diseases were not investigated in this paper due to its small sample size. Nevertheless, this is the first report on the use of ICG to assess ileal conduit perfusion in the setting of pelvic exenteration in gynecologic malignancy after pelvic radiotherapy and reports a graduated scale of stump perfusion.
Conclusion
The use of ICG to intraoperatively assess anastomosis perfusion at the time of pelvic exenteration for gynecologic malignancy is a feasible and safe technique. The different vascularization of anastomotic stumps may be related to anatomical sites and to previous radiation treatment. This approach could be in support of selecting patients at higher risk of complications who may need personalized follow-up. In this context, further studies are required to better understand whether ICG may be able to improve morbidity outcomes in this setting.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the institutional review board of Fondazione Policlinico Gemelli IRCCS (number DIPUSVSP-27-07-20108). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors fulfilled the conditions required for authorship and approved the submission, in particular: GV and NB provided a substantial contribution to the design of the project and drafted the article. NF, ML, LT, FS, AR, SGA BC, and VG collected the data giving an important contribution to critical aspects of the research. GF, AF, and FF revised the paper for important intellectual content. GS approved the final version to be published. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor and reviewers AG and GC declared a shared affiliation with several of the authors, NB, NF, ML, FS, AR, SG, BC, VG, GF, AF, FF, GS, and GV, at time of review.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kaur M, Joniau S, D'Hoore A, Vergote I. Indications, Techniques and Outcomes for Pelvic Exenteration in Gynecological Malignancy. Curr Opin Oncol (2014) 26(5):514–20. doi: 10.1097/CCO.0000000000000109
2. Khoury-Collado F, Einstein MH, Bochner BH, Alektiar KM, Sonoda Y, Abu-Rustum NR, et al. Pelvic Exenteration With Curative Intent for Recurrent Uterine Malignancies. Gynecol Oncol (2012) 124:42–7. doi: 10.1016/j.ygyno.2011.09.031
3. Schmidt AM, Imesch P, Egger H. Indications and Long-Term Clinical Outcomes in 282 Patients With Pelvic Exenteration for Advanced or Recurrent Cervical Cancer. Gynecol Oncol (2012) 125:604–9. doi: 10.1016/j.ygyno.2012.03.001
4. Chiantera V, Rossi M, De laco P, Koehler C, Marnitz S, Ferrandina G, et al. Survival After Curative Pelvic Exenteration for Primary or Recurrent Cervical Cancer: A Retrospective Multicentric Study of 167 Patients. Int J Gynecol Cancer (2014) 24:916–22. doi: 10.1097/IGC.0b013e3182a80aec
5. Höckel M, Horn LC, Einenkel J. (Laterally) Extended Endopelvic Resection: Surgical Treatment of Locally Advanced and Recurrent Cancer of the Uterine Cervix and Vagina Based on Ontogenetic Anatomy. Gynecol Oncol (2012) 127(2):297–302. doi: 10.1016/j.ygyno.2012.07.120
6. Vizzielli G, Naik R, Dostalek L, Bizzarri N, Kucukmetin A, Tinelli G, et al. Laterally Extended Pelvic Resection for Gynaecological Malignancies: A Multicentric Experience With Out-Of-the-Box Surgery. Ann Surg Oncol (2019) 26(2):523–30. doi: 10.1245/s10434-018-07088-8
7. Chiantera V, Rossi M, De Iaco P, Koehler C, Marnitz S, Fagotti A, et al. Morbidity After Pelvic Exenteration for Gynecological Malignancies: A Retrospective Multicentric Study of 230 Patients. Int J Gynecol Cancer (2014) 24:156–64. doi: 10.1097/IGC.0000000000000011
8. Martínez-Gómez C, Angeles MA, Martinez A, Malavaud B, Ferron G. Urinary Diversion After Pelvic Exenteration for Gynecologic Malignancies. Int J Gynecol Cancer (2021) 31(1):1–10. doi: 10.1136/ijgc-2020-002015
9. Lee RK, Abol-Enein H, Artibani W, Bochner B, Dalbagni G, Daneshmand S, et al. Urinary Diversion After Radical Cystectomy for Bladder Cancer: Options, Patient Selection, and Outcomes. BJU Int (2014) 113(1):11–23. doi: 10.1111/bju.12121
10. Hautmann RE, Abol-Enein H, Lee CT, Mansson W, Mills RD, Penson DF, et al. Urinary Diversion: How Experts Divert. Urology (2015) 85(1):233–8. doi: 10.1016/j.urology.2014.06.075
11. Madersbacher S, Schmidt J, Eberle JM, Thoeny HC, Burkhard F, Hochreiter W, et al. Long-Term Outcome of Ileal Conduit Diversion. J Urol (2003) 169(3):985–90. doi: 10.1097/01.ju.0000051462.45388.14
12. Urh A, Soliman PT, Schmeler KM, Westin S, Frumovitz M, Nick AM, et al. Postoperative Outcomes After Continent Versus Incontinent Urinary Diversion at the Time of Pelvic Exenteration for Gynecologic Malignancies. Gynecol Oncol (2013) 129(3):580–5. doi: 10.1016/j.ygyno.2013.02.024
13. Shah SH, Movassaghi K, Skinner D, Dalag L, Miranda G, Cai J, et al. Ureteroenteric Strictures After Open Radical Cystectomy and Urinary Diversion: The University of Southern California Experience. Urology (2015) 86(1):87–91. doi: 10.1016/j.urology.2015.03.014
14. Anderson CB, Morgan TM, Kappa S, Moore D, Clark PE, Davis R, et al. Ureteroenteric Anastomotic Strictures After Radical Cystectomy-Does Operative Approach Matter? J Urol (2013) 189(2):541–7. doi: 10.1016/j.juro.2012.09.034
15. Lobo N, Dupré S, Sahai A, Thurairaja R, Khan MS. Getting Out of a Tight Spot: An Overview of Ureteroenteric Anastomotic Strictures. Nat Rev Urol (2016) 13(8):447–55. doi: 10.1038/nrurol.2016.104
16. Hautmann RE, de Petriconi RC, Volkmer BG. 25 Years of Experience With 1,000 Neobladders: Long-Term Complications. J Urol (2011) 185(6):2207–12. doi: 10.1016/j.juro.2011.02.006
17. Watanabe J, Ishibe A, Suwa Y, Suwa H, Ota M. Indocyanine Green Fluorescence Imaging to Reduce the Risk of Anastomotic Leakage in Laparoscopic Low Anterior Resection for Rectal Cancer: A Propensity Score-Matched Cohort Study. Surg Endosc (2020) 34(1):202–8. doi: 10.1007/s00464-019-06751-9
18. Phillips BT, Lanier ST, Conkling N, Wang ED, Dagum AB, et al. Intraoperative Perfusion Techniques can Accurately Predict Mastectomy Skin Flap Necrosis in Breast Reconstruction: Results of a Prospective Trial. Plast Reconstr Surg (2012) 129:778e–88e. doi: 10.1097/PRS.0b013e31824a2ae8
19. Ris F, Hompes R, Cunningham C, Lindsey I, Guy R, et al. Near-Infrared (NIR) Perfusion Angiography in Minimally Invasive Colorectal Surgery. Surg Endosc (2014) 28(7):2221–6. doi: 10.1007/s00464-014-3432-y
20. Shen JK, Jamnagerwalla J, Yuh BE, Bassett MR, Chenam A, et al. Real-Time Indocyanine Green Angiography With the SPY Fluorescence Imaging Platform Decreases Benign Ureteroenteric Strictures in Urinary Diversions Performed During Radical Cystectomy. Ther Adv Urol (2019) 11:1756287219839631. doi: 10.1177/1756287219839631
21. Ahmadi N, Ashrafi AN, Hartman N, Shakir A, Cacciamani GE, et al. Use of Indocyanine Green to Minimise Uretero-Enteric Strictures After Robotic Radical Cystectomy. BJU Int (2019) 124(2):302–7. doi: 10.1111/bju.14733
22. Bizzarri N, Chiantera V, Ercoli A, Fagotti A, Tortorella L, et al. Minimally Invasive Pelvic Exenteration for Gynecologic Malignancies: A Multi-Institutional Case Series and Review of the Literature. J Minim Invasive Gynecol (2019) 26(7):1316–26. doi: 10.1016/j.jmig.2018.12.019
23. Dindo D, Demartines N, Clavien PA. Classification of Surgical Complications: A New Proposal With Evaluation in a Cohort of 6336 Patients and Results of a Survey. Ann Surg (2004) 240(2):205–13. doi: 10.1097/01.sla.0000133083.54934.ae
24. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations for Planning Pilot Studies in Clinical and Translational Research. Clin Transl Sci (2011) 4(5):332–7. doi: 10.1111/j.1752-8062.2011.00347.x
Keywords: indocyanine green (ICG), pelvic exenteration (PE), ileal conduit diversion, major postoperative complications, anastomosis, gynecological cancer
Citation: Bizzarri N, Foschi N, Loverro M, Tortorella L, Santullo F, Rosati A, Gueli Alletti S, Costantini B, Gallotta V, Ferrandina G, Fagotti A, Fanfani F, Ercoli A, Chiantera V, Scambia G and Vizzielli G (2021) Indocyanine Green to Assess Vascularity of Ileal Conduit Anastomosis During Pelvic Exenteration for Recurrent/Persistent Gynecological Cancer: A Pilot Study. Front. Oncol. 11:727725. doi: 10.3389/fonc.2021.727725
Received: 19 June 2021; Accepted: 01 November 2021;
Published: 07 December 2021.
Edited by:
Francesco Giovinazzo, Catholic University of the Sacred Heart, ItalyReviewed by:
Alessandro Gioè, Catholic University of the Sacred Heart, ItalyGiacomo Corrado, Agostino Gemelli University Polyclinic, Italy
Giuseppe Giaccone, Cornell University, United States
Copyright © 2021 Bizzarri, Foschi, Loverro, Tortorella, Santullo, Rosati, Gueli Alletti, Costantini, Gallotta, Ferrandina, Fagotti, Fanfani, Ercoli, Chiantera, Scambia and Vizzielli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Giuseppe Vizzielli, Z2l1c2VwcGV2aXp6aWVsbGlAeWFob28uaXQ=