 Paolo Del Fiore1*†
Paolo Del Fiore1*† Irene Russo1,2†
Irene Russo1,2† Beatrice Ferrazzi3Alessandro Dal Monico4
Beatrice Ferrazzi3Alessandro Dal Monico4 Francesco Cavallin5Angela Filoni1
Francesco Cavallin5Angela Filoni1 Saveria Tropea1Francesco Russano1Claudia Di Prata1
Saveria Tropea1Francesco Russano1Claudia Di Prata1 Alessandra Buja6Alessandra Collodetto1
Alessandra Buja6Alessandra Collodetto1 Romina Spina1Sabrina Carraro1Rocco Cappellesso7
Romina Spina1Sabrina Carraro1Rocco Cappellesso7 Lorenzo Nicolè8,9Vanna Chiarion-Sileni10Jacopo Pigozzo10
Lorenzo Nicolè8,9Vanna Chiarion-Sileni10Jacopo Pigozzo10 Luigi Dall’Olmo1,11
Luigi Dall’Olmo1,11 Marco Rastrelli1,11Antonella Vecchiato1
Marco Rastrelli1,11Antonella Vecchiato1 Clara Benna11
Clara Benna11 Chiara Menin12Daniela Di Carlo13Gianni Bisogno13
Chiara Menin12Daniela Di Carlo13Gianni Bisogno13 Angelo Paolo Dei Tos7
Angelo Paolo Dei Tos7 Mauro Alaibac2‡Simone Mocellin1,11‡
Mauro Alaibac2‡Simone Mocellin1,11‡- 1Soft-Tissue, Peritoneum and Melanoma Surgical Oncology Unit, Veneto Institute of Oncology - IOV IRCCS, Padua, Italy
- 2Division of Dermatology, Department of Medicine (DIMED), University of Padua, Padua, Italy
- 3Postgraduate School of Occupational Medicine, University of Verona, Verona, Italy
- 4Department of Medicine, University of Padua School of Medicine and Surgery, Padua, Italy
- 5Independent Statistician, Solagna, Italy
- 6Department of Cardiological, Thoracic, Vascular Sciences and Public Health, University of Padua, Padua, Italy
- 7Pathological Anatomy Unit, University Hospital of Padua, Padua, Italy
- 8Department of Medicine (DIMED), Unit of Pathology & Cytopathology, University of Padua, Padua, Italy
- 9Unit of Surgical Pathology & Cytopathology, Ospedale dell’Angelo, Mestre, Italy
- 10Melanoma Oncology Unit, Veneto Institute of Oncology IOV-IRCCS, Padua, Italy
- 11Department of Surgery, Oncology and Gastroenterology (DISCOG), University of Padua, Padua, Italy
- 12Immunology and Diagnostic Molecular Oncology Unit, Veneto Institute of Oncology IOV-IRCCS, Padua, Italy
- 13Hematology/Oncology Division, Department of Women’s and Children’s Health, University of Padua, Padua, Italy
The “Veneto Cancer Registry” records melanoma as the most common cancer diagnosed in males and the third common cancer in females under 50 years of age in the Veneto Region (Italy). While melanoma is rare in children, it has greater incidence in adolescents and young adults (AYA), but literature offers only few studies specifically focused on AYA melanoma. The aim of this study was to describe the characteristics, surgical treatment, and prognosis of a cohort of AYA melanoma in order to contribute to the investigation of this malignancy and provide better patient care. This retrospective cohort study included 2,752 Caucasian patients (702 AYA and 2,050 non-AYA patients) from the Veneto Region who were over 15 years of age at diagnosis, and who received diagnosis and/or treatment from our institutions between 1998 and 2014. Patients were divided in adolescents and youth (15-25 years), young adults (26-39 years) and adults (more than 39 years) for the analysis. We found statistically significant differences in gender, primary site, Breslow thickness, ulceration, pathologic TNM classification (pTNM) stage and tumor subtype among the age groups. Disease-specific survival and disease-free survival were also different among the age groups. Our findings suggest that the biological behavior of melanoma in young people is different to that in adults, but not such as to represent a distinct pathological entity. Additional and larger prospective studies should be performed to better evaluate potential biological and cancer-specific differences between AYAs and the adult melanoma population.
1 Introduction
The incidence of melanoma is continuously increasing in both adult and pediatric population around the world (1, 2). Although melanoma is rare in pediatric patients, the risk of developing melanoma grows significantly in adolescents and young adults, and represents the second most common type of cancer in this age group (3–5). The literature on melanoma offers very few studies specifically addressing adolescents and young adults (AYA). Of note, previous studies presented clinical and prognostic differences between melanoma diagnosed in adolescents, young adults and adults (6, 7). Specific clinical practice guidelines for the treatment of melanoma in AYA do not exist, and current management is similar to melanoma in adults.
This study compared characteristics, surgical treatment, and prognosis in a cohort of melanoma patients according to the age at diagnosis, with the purpose of underling potential differences in terms of tumor characteristics and prognosis between melanoma in AYA and melanoma in adults (non-AYA).
2 Materials and Methods
2.1 Study Design
This is a retrospective cohort study of patients who were diagnosed and/or treated for Melanoma of the skin between 1998-2014 at the Veneto Institute of Oncology (IOV) and at the University Hospital of Padua (UHP).
2.2 Material
The study included all 2,752 patients aged ≥15 years and living in the Veneto Region, who were diagnosed and/or treated for Primary Melanoma of the skin between 1998-2014 at the Veneto Institute of Oncology (IOV) and at the University Hospital of Padua (UHP). IOV and UHP are level III referral centers which are located in Northeastern Italy. Most patients are referred for diagnosis and/or first-line treatment, while some patients are referred for disease progression after being treated at local level II centers.
2.3 Diagnosis and Treatment
Melanoma was diagnosed according to the histopathology and immunohistochemistry of the lesion biopsy. Tumor stage was defined according to the eighth version of the American Joint Committee on Cancer (AJCC) staging system (8), effective from January 2018. All diagnoses before January 2018 were re-staged according to the last version of the staging system.
The surgical treatment included wide excision (WE) of the primary lesion, sentinel lymph node biopsy (SNB) and/or regional lymph node dissection. Patients with locoregional primary melanoma underwent WE, followed by complete lymph node dissection (LND) in clinical node-positive patients. Sentinel node biopsy was performed concurrently with WE in patients with primary lesions.
Follow-up visits were performed every three to four months for the first three years, every six months for up to five years, and every year thereafter.
Disease progression included regional recurrences, in-transit metastases, lymph node metastases, and distant metastases.
2.4 Data Collection
All data were extracted from a local database. Demographics included age at diagnosis, sex and family history, while tumor information included subtype of melanoma (such as acral lentiginous melanoma, lentigo maligna melanoma, nodular melanoma, superficial spreading melanoma, spitzoid melanoma, nevoid melanoma, pagetoid melanoma, polypoid melanoma, desmoplastic melanoma, minimal deviation melanoma and neurotropic melanoma) primary site, Breslow thickness, ulceration, mitotic rate, and pTNM stage.
Follow-up information was extracted from scheduled visits. Follow‐up was calculated from the date of diagnosis to December 31, 2019. Disease-specific survival was calculated from date of diagnosis to date of disease-related death, or date of last visit/disease-unrelated death. Disease-free survival was calculated in patients with primary melanoma from date of diagnosis to date of recurrence, or date of last visit/death. Recurrence was defined as regional recurrences, in-transit metastases, lymph node metastases or distant metastases.
2.5 Statistical Analysis
Continuous data were summarized as median and interquartile range (IQR). The patient cohort was divided into three age groups: adolescents and youth (15-25 years), young adults (26-39 years) and adults (more than 39 years). Categorical data were compared between age groups using the Fisher’s exact test, while the Kruskal-Wallis test was used for continuous data. Survival estimates were calculated using the Kaplan-Meier method and compared among age groups using log-rank test (unadjusted analysis) and Cox regression models with pTNM stage as additional independent variable (adjusted analysis). Effect sizes were reported as hazard ratio (HR) with 95% confidence interval (CI). The limited sample size and availability of immunohistochemistry data did not allow any meaningful multivariable analyses. All tests were two-sided and a p-value of less than 0.05 was considered statistically significant. Statistical analyses were performed using R software version 4.1 (R Foundation for Statistical Computing, Vienna, Austria) (9).
2.6 Ethics Considerations
The study was approved by the local Ethics Committee (number 2/2020). The study was conducted according to Helsinki Declaration principles, and all patients gave their consent to have their anonymized data used for scientific purpose.
3 Results
3.1 Patients
This analysis included 2,752 Caucasian patients aged ≥15 years, involving 76 (2.8%) adolescents and youth (median 22 years, IQR 20-24), 626 (22.7%) young adults (median 34 years, IQR 31-37) and 2,050 (74.5%) adults (median 54 years, IQR 48-68). Patient characteristics according to age classes are outlined in Table 1. Sex, primary tumor site, Breslow thickness, ulceration, number of mitoses, tumor stage and sub-type differed among the age classes.
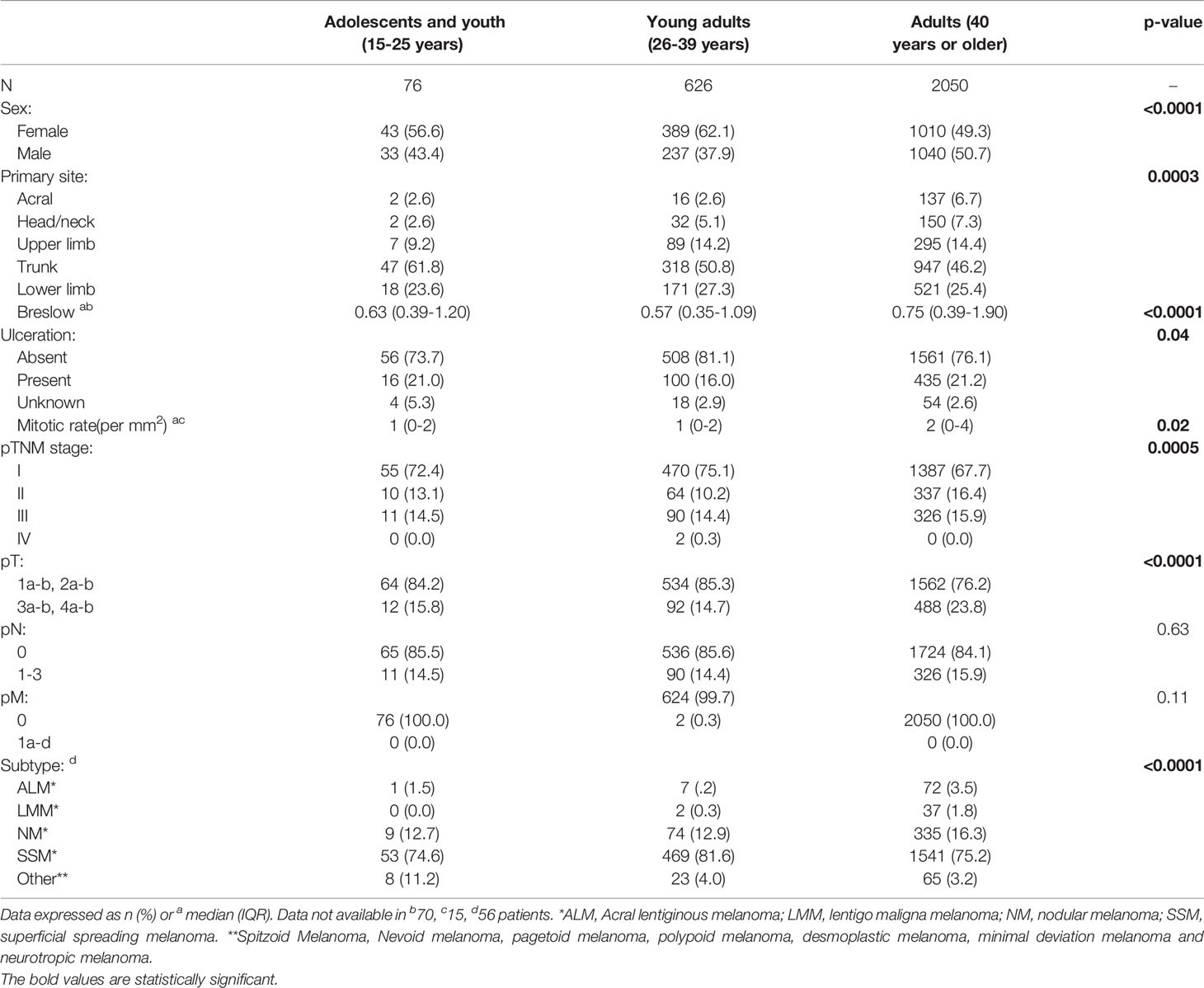
Table 1 Patient and tumor characteristics in 2,752 patients aged ≥15 years and living in the Veneto Region who were diagnosed and/or treated for Melanoma of the skin between 1998-2014 at the Veneto Institute of Oncology and at the University Hospital of Padua (Italy): comparison between age classes (15-25 years, 26-39 years, 40 years or older).
3.2 Treatment of Primary Melanoma
All patients underwent WE, while SNB was performed in 1,412 patients and LND in 394. Treatment according to age classes is shown in Table 2. The number of excised sentinel lymph nodes (SLNs) differed among age classes, while the number of positive sentinel lymph nodes and the number of positive dissected lymph nodes were the same.
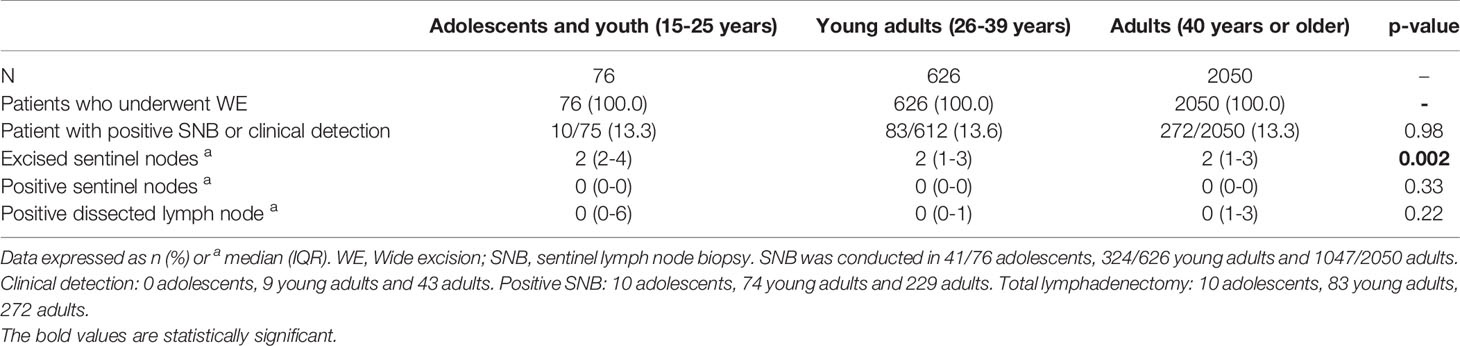
Table 2 Treatment of primary Melanoma of the skin in 2,752 patients aged ≥15 years and living in the Veneto Region who were diagnosed and/or treated for Melanoma between 1998-2014 at the Veneto Institute of Oncology and at the University Hospital of Padua (Italy): comparison between age classes (15-25 years, 26-39 years, 40 years or older).
3.2.1 Disease-Specific Survival
Median follow-up was 96 months (IQR 60-132). Overall, 312 patients died from the disease, and 211 patients died due to other causes (18 patients were lost to follow-up). 5-year disease-specific survival was 95% in patients aged 15-25 years, 95% in patients aged 26-39 years, and 90% in patients over 39 years (p<0.0001) (Figure 1). Adjusting for pTNM stage, patients aged 26-39 years had better disease-specific survival compared to patients over 39 years (HR 0.52, 95% CI 0.37 to 0.70; p<0.0001), while the difference between patients aged 15-25 years and patients over 39 years was not statistically significant (HR 0.46, 95% CI 0.19 to 1.12; p=0.09).
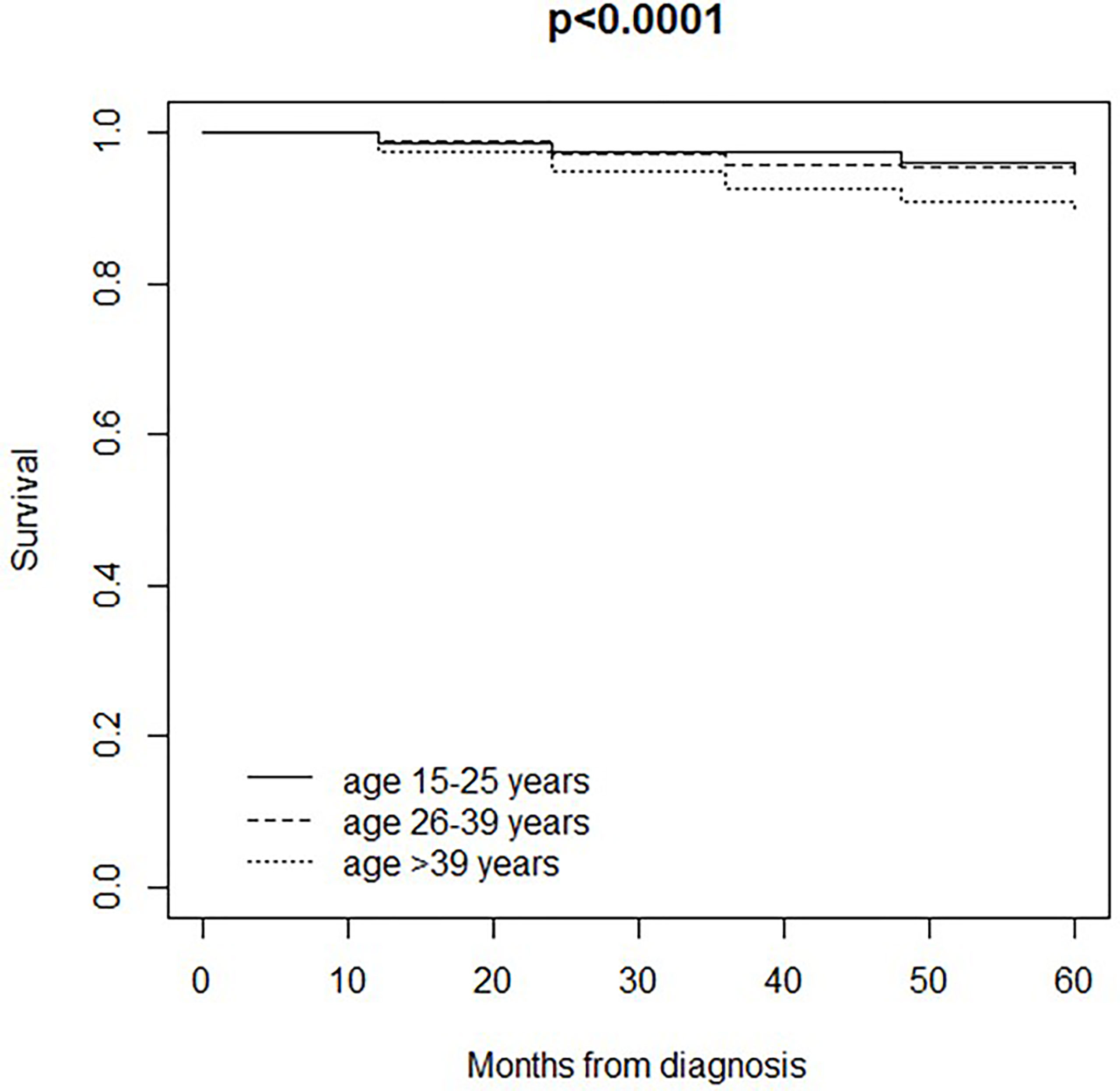
Figure 1 Disease-specific survival in 2,734 patients (18 patients were lost to follow-up) aged ≥15 years and living in the Veneto Region who were diagnosed and/or treated for Melanoma between 1998-2014 at the Veneto Institute of Oncology and at the University Hospital of Padua (Italy): comparison between age classes (15-25 years, 26-39 years, 40 years or older).
3.2.2 Disease-Free Survival
393 patients experienced a clinical event during follow-up: local recurrence in 56 patients, regional lymph node metastasis in 128, regional skin/in-transit in 130, and distant metastasis in 167.
5-year disease-free survival (i.e. survival until the occurrence of a clinical event or death/last visit) was 95% in patients aged 15-25 years, 91% in patients aged 26-39 years, and 87% in patients over 39 years (p=0.003) (Figure 2). Adjusting for pTNM stage, disease-free survival was better in patients aged 15-25 years (HR 0.42, 95% CI 0.19 to 0.95; p=0.04) and patients aged 26-39 years (HR 0.74, 95% CI 0.57 to 0.95; p=0.02) compared to patients over 39 years.
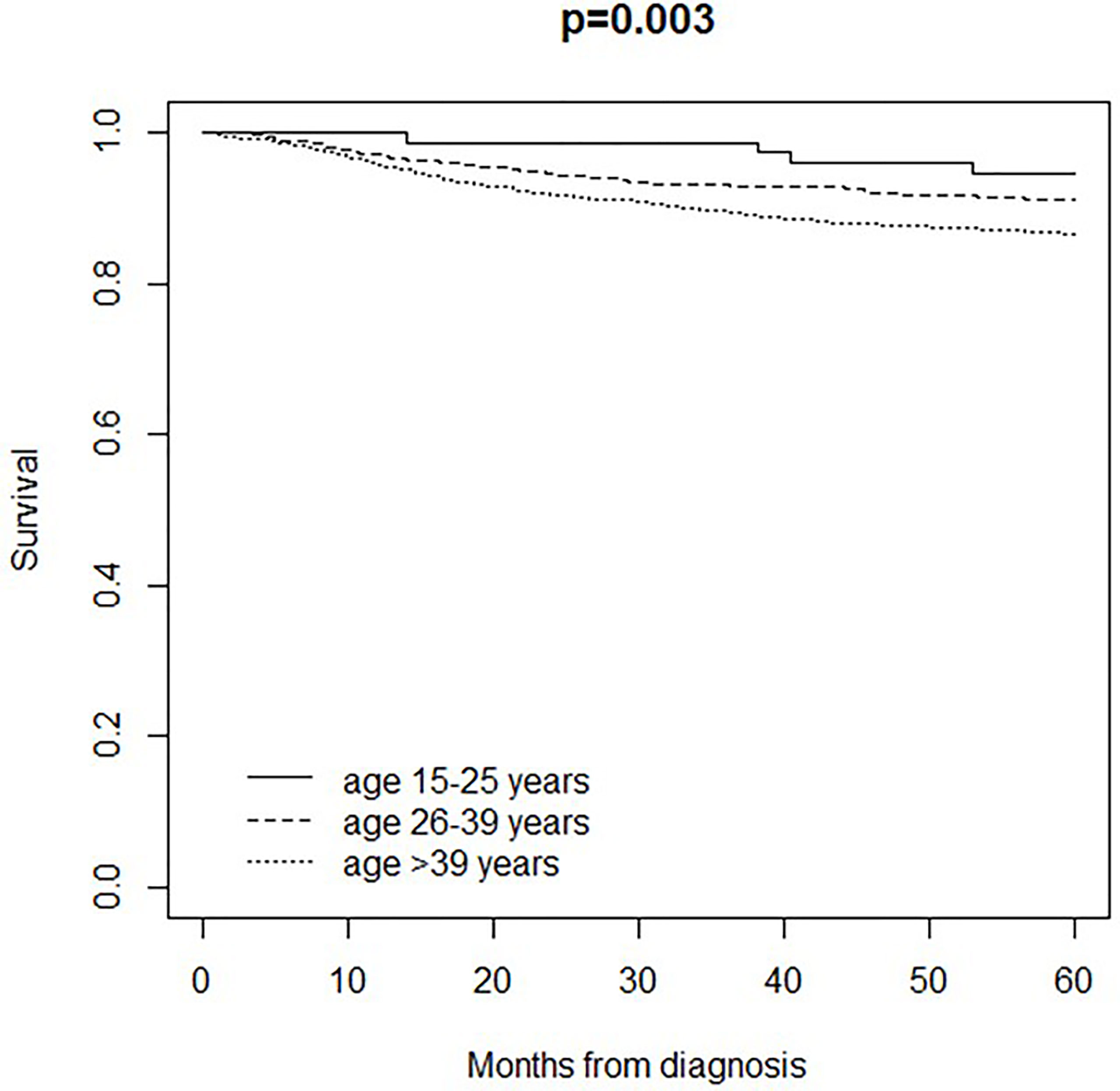
Figure 2 Disease-free survival in 2,734 patients (18 patients were lost to follow-up) aged ≥15 years and living in the Veneto Region who were diagnosed and/or treated for Melanoma between 1998-2014 at the Veneto Institute of Oncology and at the University Hospital of Padua (Italy): comparison between age classes (15-25 years, 26-39 years, 40 years or older).
“Local recurrence”-free survival did not differ among age classes (p=0.20)
“Regional lymph node metastasis”- free survival differed among age classes (5-year survival: 98% in patients aged 15-25 years, 97% in patients aged 26-39 years, and 95% in patients aged over 39 years; p=0.02). Adjusting for pTNM stage, patients aged 26-39 years had better “regional lymph node metastasis”- free survival compared to patients over 39 years (HR 0.58, 95% CI 0.36 to 0.95; p=0.03), while the difference between patients aged 15-25 years and patients over 39 years was not statistically significant (HR 0.46, 95% CI 0.11 to 1.85; p=0.27).”Regional skin/in-transit” - free survival differed among age classes (5-year survival: 98% in patients aged 15-25 years, 98% in patients aged 26-39 years, 95% in patients aged over 39 years; p=0.003). Adjusting for pTNM stage, patients aged 26-39 years had better “regional skin/in-transit”- free survival compared to patients over 39 years (HR 0.44, 95% CI 0.26 to 0.75; p=0.002), while the difference between patients aged 15-25 years and patients over 39 years was not statistically significant (HR 0.42, 95% CI 0.10 to 1.72; p=0.23). “Distant metastasis” - free survival did not differ among age classes (p=0.06).
4 Discussion
There is currently a lack of data with regard to melanoma features and outcomes in AYA. A distinction should be made between AYA and older adult cancer in disease biology, treatment efficacy, and psychosocial barriers to care for patients. Moreover, patients aged 15-25 are a sub-category of AYA which is trapped in a medical gray area and may receive cancer treatment from pediatric or adult oncologists. Although this may not be perceived as an important aspect, treatment regimens for pediatric and adult cancer can lead to significant survival differences (10).
Overall, we found some differences in epidemiological, clinical, histopathological and prognostic features between AYA and non-AYA melanoma patients. Furthermore, some differences between adolescents and young adults also emerged.
We found more female patients in the AYA group than in the non-AYA. Females represented 56.6% of adolescents and youth (15-25 years old) and 62.1% of young adults (26-39 years old), while the proportion of males and females was similar among older adults. This finding is consistent with available literature (3), and could be explained by both biological and behavioral gender differences between young male and female patients (11). A strong endogenous estrogen exposure, due to early menarche associated with UV exposure during childhood, seems to play a crucial role in cutaneous melanoma development, and may explain the higher occurrence of melanoma in young females than in males (11).
AYA melanoma presented higher involvement of the trunk, while non-AYA melanoma were more common in the acral region, head/neck and upper limbs. On the other hand, the occurrence in lower limbs was similar among the age groups. Adolescent subjects, compared to young adults, had less involvement of the head/neck and upper limbs, while the trunk was the main affected site. These data mirror what is already known in the literature, namely, that the most affected sites are the trunk and lower limbs in young people and the head/neck and upper limbs increases among adults (3). However, the involvement of the trunk, upper limbs and head/neck in young adults was more similar to older adults than adolescents.
We found a different distribution of histological subtypes of melanoma between AYAs and older adults. Superficial spreading melanoma (SSM) was more common in young adults than in adults, but less common in adolescents than in adults. Nodular melanoma (NM), lentigo maligna melanoma (LMM) and acral lentiginous melanoma (ALM) were more common in adults. There was a considerable fraction of rare melanomas in adolescents these findings largely reflect what is known in the literature, namely, the greater presence of NM in older age, the presence of ALM almost exclusively in the elderly and rare melanomas in adolescent and young patients (12).
Moreover, we found that older adults were the subgroup with the worst pathological characteristics at the time of diagnosis. 21.2% of older adults presented ulceration, 32.3% had pTNM stage above the first, and the median Breslow thickness was 0.75 mm. At the time of diagnosis, melanoma in our cohort of patients was generally less advanced in AYAs than in adults. However, we found important differences between adolescents and young adults. Median Breslow thickness was 0.63 mm in adolescents and 0.57 mm in young adults; ulceration was found 21% in adolescents and 16% in young adults; a pTNM stage above the first was described in 27.6% of adolescents and in 24.9% of young adults. AYAs had lower Breslow thickness and lower pTNM stage at the time of diagnosis compared to adults, while there was no difference in regional lymph node involvement among age groups. Of note, adolescents had slightly worse stage characteristics than young adults.
It is important to emphasize that regional lymph node invasion (detected through positivity of the SNB or clinical positivity) was almost the same in the three age groups. Most pediatric melanoma studies suggested that the clinical history of melanoma in children and adolescents resembled that of adult disease (3, 4, 6, 7). As in adults, features such as ulceration, tumor thickness, and node involvement seemed to affect prognosis. Hence, in the absence of specific treatment guidelines, AYA melanoma is currently managed in the same way as non-AYA melanoma, though it is unclear whether it actually may have the same biological features as adult melanoma.
Data concerning the aggressiveness and prognosis of melanoma in AYAs are discordant in literature. Some studies reported that melanomas diagnosed in children and adolescents had higher Breslow thickness, greater tendency to regional lymph node invasion and, generally, a more advanced stage at the time of diagnosis compared to adults (13–17). On the other hand, it was also reported that young patients tended to have a better overall disease-specific survival than older adults (4, 15, 18).
In our study, disease-specific survival and disease-free survival were worse in older adults than in AYAs. Of note, most survival differences between younger and older age classes persisted after adjusting for tumor stage. This can be attributed to a diminished immune response with increased age, changes in host immune biology, and undertreatment due to medical comorbidities that may limit therapy with antineoplastic and biologic agents. The immune surveillance mechanism is one of the main factors which are hypothesized to account for better melanoma survival in the adolescents (19). Nonetheless, promoting skin cancer screening and public education (such as skin protection and self-examination awareness) is of utmost importance in patients of any age.
Regional lymph node metastasis-free survival and regional skin/in transit-free survival were different among age classes, with improved survival in young adults over adults, while the difference between adolescents and adults did not achieved statistical significance (likely due to the small number of adolescents in the study). Regional lymph node metastasis-free survival and regional skin/in transit-free survival have a substantial difference in survival regardless of patient’s age and involve a different therapeutic strategy.
The findings of this study should be interpreted considering his strengths and limitations. The strengths involve the completeness of information regarding epidemiological, clinical, histopathological and prognostic features, and the follow-up duration (at least 5 years for all patients). The limitations include the retrospective nature of the study and the absence of data regarding the analysis of mutational profiles and medical treatments for advanced melanoma. Furthermore, the small number of adolescents (which reflects melanoma epidemiology) may limit the generalizability of the findings for this subgroup.
Nonetheless, our study highlighted a sub-category of AYA aged 15-25 which may receive cancer treatment from pediatric or adult oncologists, with potential difference in survival outcome (10). The proportion of stage II-III melanoma among such patients suggest the need for adequate communication about prevention and awareness. Future research may confirm our results and explore the most appropriate and effective ways of implementing educational interventions among AYA aged 15-25.
5 Conclusion
Our findings show that AYA melanoma does not represent a distinct pathological entity and however there are differences they do not require a different therapeutic strategy because AYA melanoma has a clinical outcome comparable or better than melanoma in adults.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://doi.org/10.5281/zenodo.4736486, 10.5281/zenodo.4736486.
Ethics Statement
The studies involving human participants were reviewed and approved by Il Comitato Etico per la Sperimentazione Clinica (CESC) IOV. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
Author Contributions
Study concepts: PF, BF, AF, MA, and AV. Study design: PF, BF, CP, RS, and AC. Data acquisition: PF, VC, AB, AM, and JP. Quality control of data and algorithms: AM and FC. Data analysis and interpretation: PF, FC, AM, ST, FR, CB and MR. Statistical analysis: FC. Manuscript preparation: BF and PF. Manuscript editing: BF, PF, and IR. Manuscript review: FC, MA, SM, AB, VC-S, DC, GB, CM, and AD. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank “Piccoli Punti ONLUS” and “Fondazione Lucia Valentini Terrani” for their long-lasting support, as well as the Marco Possia family and Mr. Fabio Crivellaro for raising awareness on melanoma and skin cancer in young people.
References
1. Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA eds. SEER Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute (2020). Available at: https://seer.cancer.gov/csr/1975_2017/. based on November 2019 SEER data submission, posted to the SEER web site, April 2020.
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries [Published Correction Appears in CA Cancer J Clin. 2020 Jul;70(4):313]. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
3. Miller KD, Fidler-Benaoudia M, Keegan TH, Hipp HS, Jemal A, Siegel RL. Cancer Statistics for Adolescents and Young Adults, 2020. CA Cancer J Clin (2020) 70(6):443–59. doi: 10.3322/caac.216379.x
4. Bagnoni G, Fidanzi C, D’Erme AM, Viacava P, Leoni M, Strambi S, et al. Melanoma in Children, Adolescents and Young Adults: Anatomo-Clinical Features and Prognostic Study on 426 Cases. Pediatr Surg Int (2019) 35(1):159–65. doi: 10.1007/s00383-018-4388-0
5. AIRTUM Working Group. CCM; AIEOP Working Group. Italian Cancer Figures, Report 2012: Cancer in Children and Adolescents. Epidemiol Prev (2013) 37(1 Suppl 1):1–225.
6. Indini A, Brecht I, Del Vecchio M, Sultan I, Signoroni S, Ferrari A, et al. Cutaneous Melanoma in Adolescents and Young Adults. Pediatr Blood Cancer (2018) 65(11):e27292. doi: 10.1002/pbc.27292
7. van der Kooij MK, Wetzels M, Aarts M, van den Berkmortel F, Blank CU, Boers-Sonderen MJ, et al. Age Does Matter in Adolescents and Young Adults Versus Older Adults With Advanced Melanoma; A National Cohort Study Comparing Tumor Characteristics, Treatment Pattern, Toxicity and Response. Cancers (Basel) (2020) 12(8):2072. doi: 10.3390/cancers12082072
8. Gershenwald JE, Scolyer RA. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond [Published Correction Appears in Ann Surg Oncol. 2018 Dec;25(Suppl 3):993-994]. Ann Surg Oncol (2018) 25(8):2105–10. doi: 10.1245/s10434-018-6513-7
9. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing (2021).
10. Rizzari C, Putti MC, Colombini A, Casagranda S, Ferrari GM, Papayannidis C, et al. Rationale for a Pediatric-Inspired Approach in the Adolescent and Young Adult Population With Acute Lymphoblastic Leukemia, With a Focus on Asparaginase Treatment. Hematol Rep (2014) 6(3):5554. doi: 10.4081/hr.2014.5554
11. Caroppo F, Tadiotto Cicogna G, Messina F, Alaibac M. Association Between Melanoma and Exposure to Sex Hormones in Puberty: A Possible Window of Susceptibility (Review). Mol Clin Oncol (2021) 14(4):66. doi: 10.3892/mco.2021.2228
12. Réguerre Y, Vittaz M, Orbach D, Robert C, Bodemer C, Mateus C, et al. Cutaneous Malignant Melanoma in Children and Adolescents Treated in Pediatric Oncology Units. Pediatr Blood Cancer (2016) 63(11):1922–7. doi: 10.1002/pbc.26113
13. Paradela S, Fonseca E, Pita-Fernández S, Kantrow SM, Diwan AH, Herzog C, et al. Prognostic Factors for Melanoma in Children and Adolescents: A Clinicopathologic, Single-Center Study of 137 Patients. Cancer (2010) 116(18):4334–44. doi: 10.1002/cncr.25222
14. Mu E, Lange JR, Strouse JJ. Comparison of the Use and Results of Sentinel Lymph Node Biopsy in Children and Young Adults With Melanoma. Cancer (2012) 118(10):2700–7. doi: 10.1002/cncr.26578
15. Livestro DP, Kaine EM, Michaelson JS, Mihm MC, Haluska FG, Muzikansky A, et al. Melanoma in the Young: Differences and Similarities With Adult Melanoma: A Case-Matched Controlled Analysis. Cancer (2007) 110(3):614–24. doi: 10.1002/cncr.22818
16. Berg P, Lindelöf B. Differences in Malignant Melanoma Between Children and Adolescents. A 35-Year Epidemiological Study. Arch Dermatol (1997) 133(3):295–7.
17. Howman-Giles R, Shaw HM, Scolyer RA, Murali R, Wilmott J, McCarthy SW, et al. Sentinel Lymph Node Biopsy in Pediatric and Adolescent Cutaneous Melanoma Patients. Ann Surg Oncol (2010) 17(1):138–43. doi: 10.1245/s10434-009-0657-4
18. Aldrink JH, Selim MA, Diesen DL, Johnson J, Pruitt SK, Tyler DS, et al. Pediatric Melanoma: A Single-Institution Experience of 150 Patients. J Pediatr Surg (2009) 44(8):1514–21. doi: 10.1016/j.jpedsurg.2008.12.003
Keywords: melanoma, skin cancer, AYA, adolescent and young adult oncology, adolescent and young adult melanoma, survival, incidence, melanoma surgical treatment
Citation: Del Fiore P, Russo I, Ferrazzi B, Monico AD, Cavallin F, Filoni A, Tropea S, Russano F, Di Prata C, Buja A, Collodetto A, Spina R, Carraro S, Cappellesso R, Nicolè L, Chiarion-Sileni V, Pigozzo J, Dall’Olmo L, Rastrelli M, Vecchiato A, Benna C, Menin C, Di Carlo D, Bisogno G, Dei Tos AP, Alaibac M and Mocellin S (2021) Melanoma in Adolescents and Young Adults: Evaluation of the Characteristics, Treatment Strategies, and Prognostic Factors in a Monocentric Retrospective Study. Front. Oncol. 11:725523. doi: 10.3389/fonc.2021.725523
Received: 15 June 2021; Accepted: 01 September 2021;
Published: 16 September 2021.
Edited by:
Suzie Chen, Rutgers, The State University of New Jersey, United StatesReviewed by:
Maciej Kaczorowski, Wroclaw Medical University, PolandChandra K. Singh, University of Wisconsin-Madison, United States
Copyright © 2021 Del Fiore, Russo, Ferrazzi, Monico, Cavallin, Filoni, Tropea, Russano, Di Prata, Buja, Collodetto, Spina, Carraro, Cappellesso, Nicolè, Chiarion-Sileni, Pigozzo, Dall’Olmo, Rastrelli, Vecchiato, Benna, Menin, Di Carlo, Bisogno, Dei Tos, Alaibac and Mocellin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paolo Del Fiore, cGFvbG8uZGVsZmlvcmVAaW92LnZlbmV0by5pdA==
†These authors have contributed equally to this work
‡These authors share last authorship