 Yichu Yuan
Yichu Yuan Yiqiu Wang
Yiqiu Wang Nan Zhang
Nan Zhang Xiawa Mao1
Xiawa Mao1 Jiwei Huang
Jiwei Huang Na Ji
Na Ji
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
HYPOTHESIS AND THEORY article
Front. Oncol. , 04 October 2021
Sec. Genitourinary Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.723669
This article is part of the Research Topic Therapies and Influences in Urothelial Carcinoma View all 8 articles
Introduction: As a research team of urologists and an anesthetist, we sought to investigate the prognostic significance of American Society of Anesthesiologists (ASA) score in patients with upper tract urothelial cancer (UTUC) after radical nephroureterectomy (RNU). ASA physical status (ASA-PS) classification not only was found to be associated with increased comorbidities but also independently factors for predicting morbidity and mortality. Accurate risk assessment was being particularly important for patients being considered for surgery.
Methods: Records for 958 patients with UTUC who underwent RNU were reviewed. Clinicopathologic variables, including ASA-PS, were assessed at two institutions. Overall survival (OS), cancer-specific survival (CSS), intravesical recurrence-free survival (IRFS), and metastasis-free survival (MFS) were estimated using the Kaplan–Meier method and Cox regression analyses. We measured the independent predictive value of ASA-PS for mortality by multivariate regression. Association of ASA-PS and clinicopathologic variables was assessed.
Results: The group of patients with ASA = 2/3 had a shorter 5-year OS (67.6% and 49.9%), CSS (72.9% and 58.1%), and MFS (75.1% and 58.5%). The median follow-up time was 39 months. Kaplan–Meier curves showed that the group with ASA = 2/3 had significantly poorer OS, CSS, and MFS. Adjusting for multiple potential confounding factors, multivariate analyses suggested that ASA score was an independent predictor of OS, CSS, and MFS (p = 0.004, p = 0.005, p < 0.001).
Conclusion: Higher ASA scores were independently associated with lower survival rate. This capability, along with its simplicity, makes it a valuable prognostic metric. It should be seriously referenced in UTUC patients being considered for RNU.
Although radical nephroureterectomy (RNU) with bladder cuff excision is considered the gold standard for the treatment of upper tract urothelial cancer (UTUC), distant relapses are common for locally advanced high-grade disease. UTUC is the most aggressive malignant tumor of the urinary system (1); 30% of patients demonstrate invasive and/or locally advanced disease, 30%–40% have regional lymph node (LN) involvement, and 20% have metastatic disease (2, 3). The 5-year cancer-specific survival (CSS) ranging from 50% to 80% is for UTUC patients who underwent RNU (4, 5). It is of great significance to establish effective prediction methods to assist clinicians in making treatment decisions and follow-up strategies. For UTUC patients, pathological stage, tumor grade, lymph node metastasis, and tumor multifocality are known to be well-established prognostic factors (6–8). Potential prognostic preoperative factors would benefit outcome prediction and individual patient treatment choices.
American Society of Anesthesiologists physical status (ASA-PS) classification, as a standardized way for anesthesiologists to convey information about the patient’s overall health status, allows outcomes to be stratified by a global assessment. It was first introduced in 1940 and has been updated. Nowadays, ASA-PS classification includes a 6-point scale (Table 1). It has been demonstrated as a significant prognostic factor for the treatment outcome of bladder cancer (9), hepatocellular cancer (10), and endometrial cancer (11). Given the positive effects of the RNU on clinical benefits, it is reasonable to speculate that the magnitude and the impact of established morbidity predictors may be altered in UTUC patients undergoing RNU.
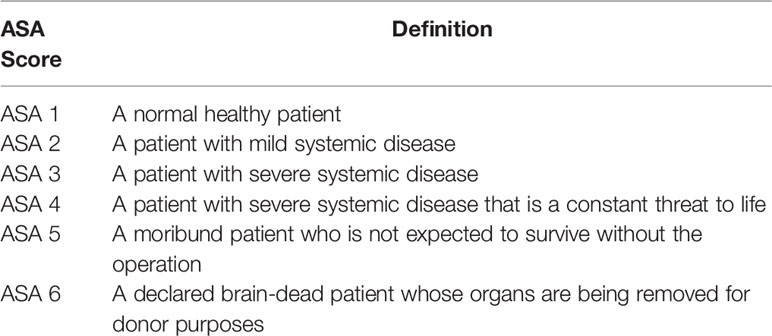
Table 1 American Society of Anesthesiologists (ASA) physical status classification.
For the purpose of investigating the influence of ASA scores on the long-term oncologic outcomes in patients diagnosed with UTUC, we set up several endpoints including overall survival (OS), CSS, intravesical recurrence-free survival (IRFS), and metastasis-free survival (MFS) and utilized the clinical data of 958 UTUC patients who underwent RNU in two Chinese institutions.
Patients with one of the following conditions were excluded: (1) incomplete clinical or pathological data; (2) underwent neoadjuvant chemotherapy or radiotherapy; (3) non-primary UTUC; (4) preoperative distant metastasis; (5) presence of other tumor types. Additionally, when computed tomography urography or other imaging examinations could not provide enough information to help clinicians make a definite diagnosis, diagnostic ureteroscopy with or without biopsy was used. In our study, 518 patients underwent diagnostic ureteroscopy. Information on 958 patients’ clinical and pathological features, including ASA score, gender, age, tumor location and size, smoking history, hydronephrosis, concomitant non-muscle invasive bladder cancer (NMIBC) or history of NMIBC, surgical methods, tumor grade and pathological stage, lymph node metastasis, tumor architecture and differentiation, lymphovascular invasion (LVI), multifocality and history of adjuvant chemotherapy (AC), was collected from Renji Hospital and Second Affiliated Hospital, Zhejiang University School of Medicine. This study was approved by the institutional review board, and approval number was 2020-369. Pathological stage was uniformly adjusted with reference to the 2017 TNM classification system (12). The histological grade was assessed according to the 2016 WHO consensus classification (13). Tumor multifocality was defined as the synchronous presence of multiple tumors in the renal pelvis or ureter. ASA score was used to assess the physical status of patients before RNU. Patients after surgery were followed up by telephone and outpatient.
The study endpoints were OS, CSS, IRFS, and MFS. According to the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines, patients were assessed by computed tomography and/or magnetic resonance imaging to detect any findings suspected of disease progression every 3–4 months in the first year after surgery, every 6 months from the second through fifth year, and annually thereafter. In addition, history taking, physical examination, routine blood and serum chemistry lab work, urinary cytology, chest radiography, and cystoscopy were also included. OS was defined as the period from the date of surgery to patient death from any cause. CSS was defined as the time in months from date of surgery to cancer-related death. The cause of death was determined by the treating physicians and institutional cancer registries, by chart review corroborated by death certificates, or by death certificates alone. IRFS was defined as the time in months from the date of surgery to bladder recurrence. MFS was defined as the time in months from date of surgery to tumor metastasis.
Statistical tests were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Proportions of the variables were analyzed using the chi-square test. Variables that had a univariate association with OS, CSS, IRFS, and MFS (p < 0.05) were included in the multiple Cox regression model. Hazard ratio (HR) and 95% CI were presented for selected items. Kaplan–Meier method with the log-rank test was used to assess OS, CSS, IRFS, and MFS. Multivariate analysis was conducted using Cox regression model to evaluate ASA-PS as an independent predictor of survival. All statistical tests were two-sided, and p < 0.05 was considered statistically significant.
Clinical and pathologic characteristics of 958 patients are shown in Table 2. There were 630 males (65.8%) and 328 females (34.2%), aged 30–89 years, with a median age of 67 years. Among them, 489 patients (51.1%) had UTUC located in the renal pelvis, 394 (41.1%) in the ureter, and 75 (7.8%) in both sites. A total of 252 patients (26.3%) had a history of smoking. Hydronephrosis was present in 499 patients (52.1%). In addition, 119 patients (12.4%) had synchronous presence or with a history of NMIBC. Open RNU and laparoscopic RNU were performed in 415 (43.3%) and 543 patients (56.7%), respectively. Here, 543 patients (51.6%) had a tumor ≤3 cm, and 415 (48.4%) had a tumor >3 cm. Low and high pathological grade was diagnosed in 275 (28.7%) and 683 patients (71.3%), respectively. The distribution of pathological stage was pTa-1 in 441 patients (46.0%), pT2 in 180 (18.8%), pT3 in 308 (32.2%), and pT4 in 29 (3.0%). Lymphadenectomy was performed in 227 patients (23.7%), and 62 (6.5%) were pathologically confirmed lymph node metastasis. Here, 516 patients (53.9%) showed papillary architecture, and 442 (46.1%) showed sessile architecture. Squamous or glandular differentiation and LVI were detected in 48 (5.0%) and 150 patients (15.7%), respectively. Moreover, 134 patients (14.0%) were multifocality. Of all patients, 196 patients received AC, including 53 pTa-1 patients and 143 pT2–4 patients. As to these 53 pTa-1 patients, we found most of them had the presence of risk factors, including positive lymph node, high tumor grade, tumor size >3 cm, and flat architecture.
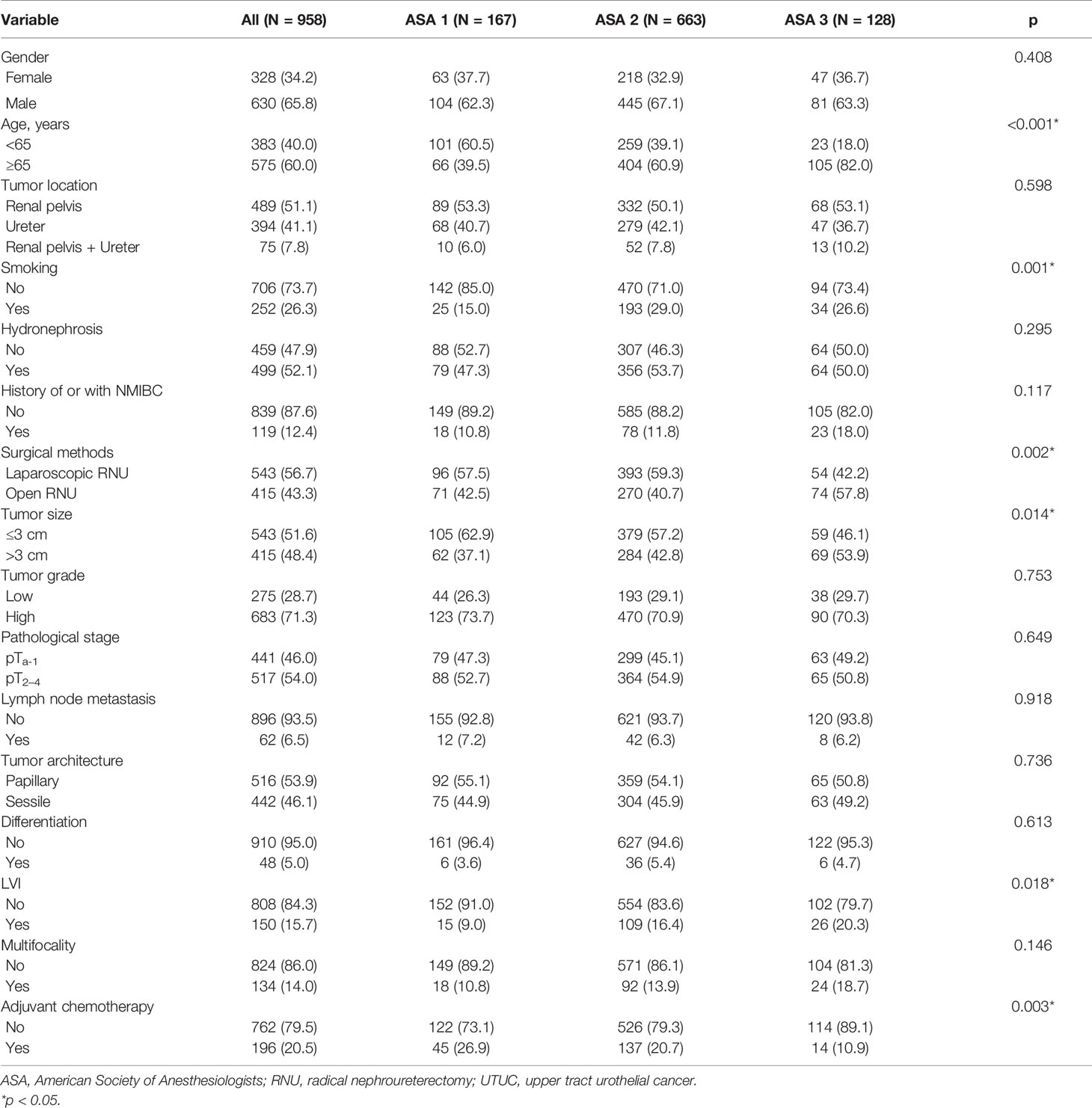
Table 2 Clinicopathological characteristics of UTUC patients stratified by ASA scores.
A total of 167 patients (17.4%) were classified as ASA score = 1, 663 (69.2%) as ASA score = 2, and 128 (13.4%) as ASA score = 3. There was no significant difference with regard to gender, hydronephrosis, tumor location, history of or with NMIBC, pathological stage, lymph node metastasis, tumor architecture, tumor grade, differentiation, and multifocality between different ASA scores (all p > 0.05). However, the distribution of characteristics was significantly varied in age (p < 0.001), smoking (p = 0.001), surgical methods (p = 0.002), tumor size (p = 0.014), LVI (p = 0.018), and AC (p = 0.003).
The median follow-up time was 39 months (ranged from 2 to 206 months). During the follow-up, a total of 304 patients (31.7%) died and 236 patients (24.6%) died from UTUC. A total of 225 patients (23.2%) had metastasis, including 96 (42.7%) with lung metastases, 52 (23.1%) with bone metastases, 42 (18.7%) with liver metastases, 15 (6.7%) with lymph node metastasis, nine (4.0%) with lumbar muscle metastases, seven (3.1%) with posterior peritoneal metastasis, and four (1.7%) in other sites (Figure S1).
Intravesical recurrence and distant metastasis occurred in 192 (20.0%) and 225 patients (23.5%), respectively. To explore the prognostic significance of ASA scores in UTUC, Kaplan–Meier survival curves were generated, and groups were compared using the log-rank test. Patients with low ASA score (ASA = 1) had a significantly reduced rate of survival than those with high ASA score (ASA = 2/3) with regard to OS (Figure 1; p < 0.001), CSS (Figure 2; p < 0.001), and MFS (Figure 3; p < 0.001), but not IRFS (Figure 4; p = 0.586). The 5-year OS rates after RNU were 75.2% for the ASA = 1 group, 67.6% for the ASA = 2 group, and 49.9% for the ASA = 3 group. The 5-year CSS rate was 80.5% in patients with ASA = 1, 72.9% in patients with ASA = 2, and 58.1% in patients with ASA = 3. As to 5-year MFS rate, ASA = 1/2/3 group had 81.3%, 75.1%, and 58.5%, respectively. However, no significant differences in IRFS were observed among the different ASA scores.
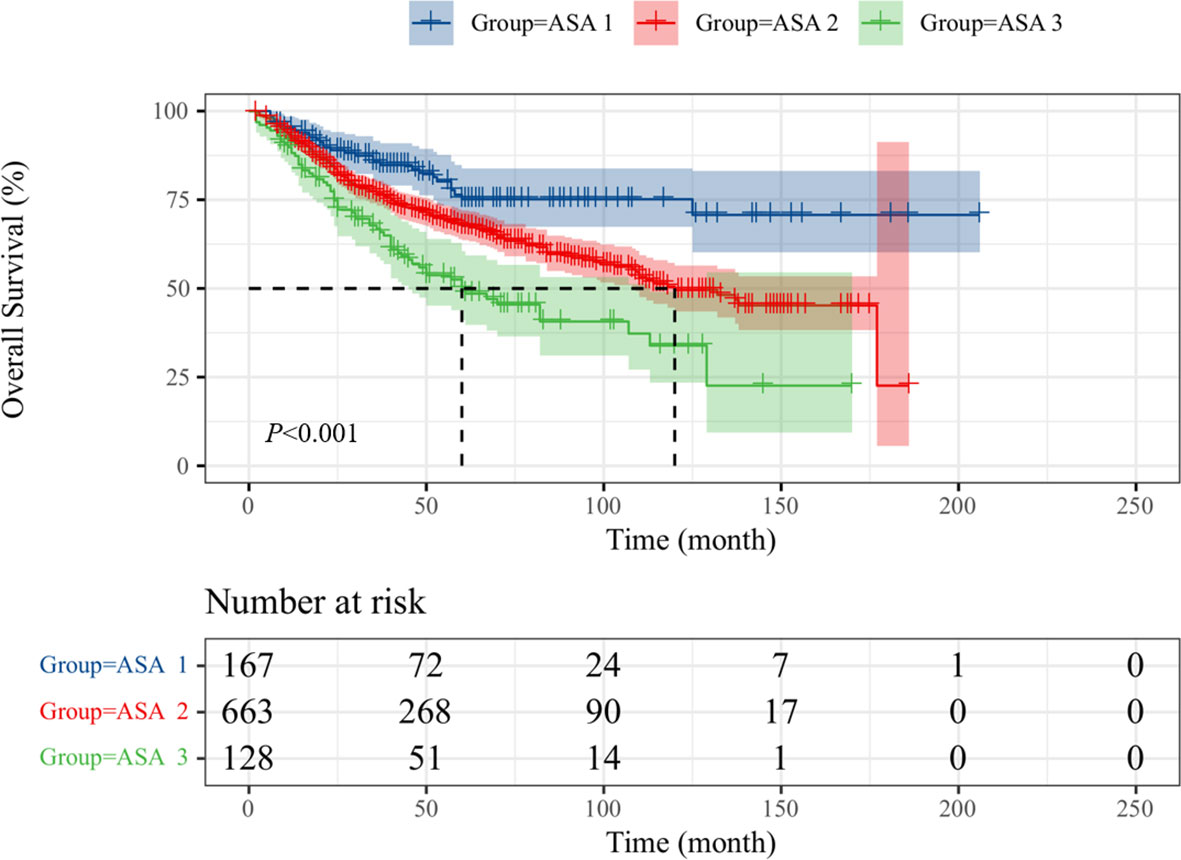
Figure 1 Kaplan-Meier curves for OS stratified according to ASA scores.
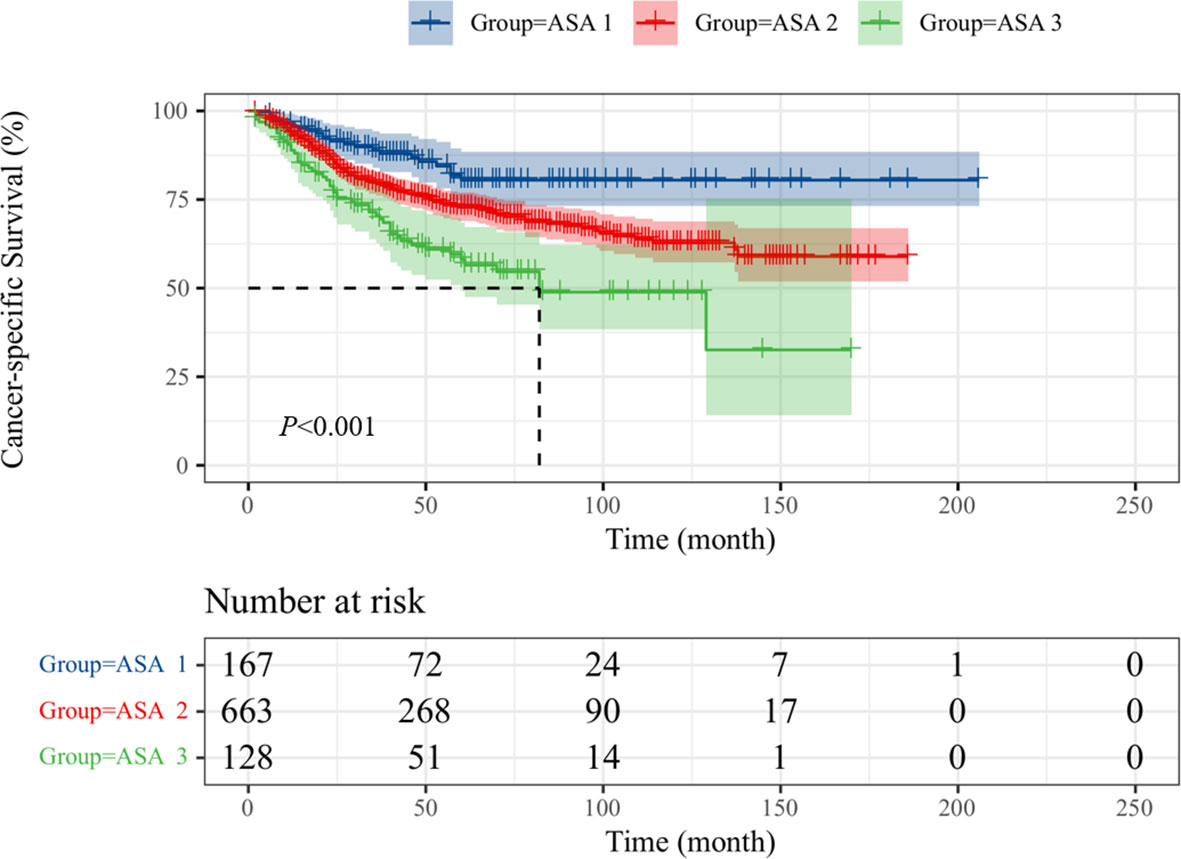
Figure 2 Kaplan-Meier curves for CSS stratified according to ASA scores.
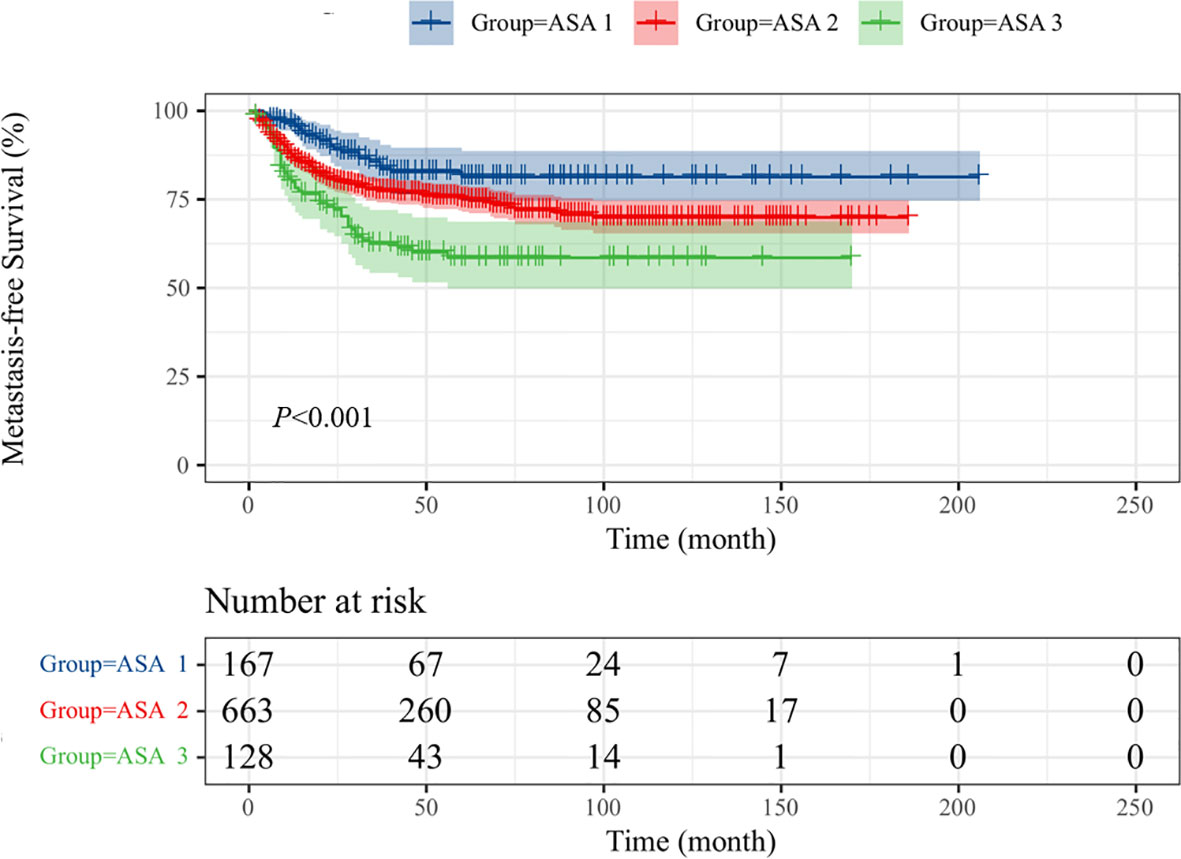
Figure 3 Kaplan-Meier curves for MFS stratified according to ASA scores.
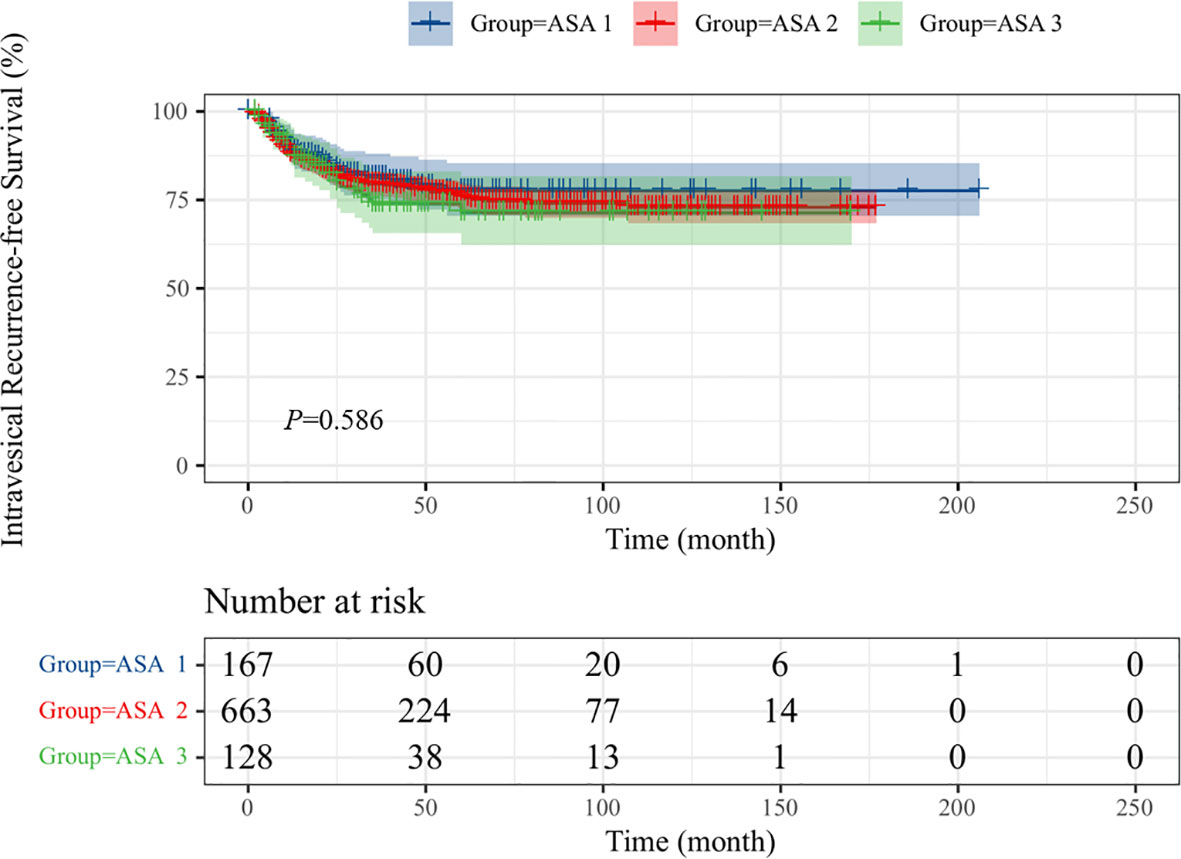
Figure 4 Kaplan-Meier curves for IRFS stratified according to ASA scores.
Cox regression analyses were performed with ASA-PS score as reference. All-cause mortality and cancer-related mortality were increased in patients whose score was 3 or 2.
The univariate analysis also revealed that age ≥65 years, tumor location, hydronephrosis, history of or with NMIBC, tumor size, higher tumor grade and pathological stage, sessile tumor, lymph node metastasis, differentiation, LVI, and multifocality were significantly associated with OS, CSS, and MFS. Besides, AC was significantly associated with CSS/MFS but not OS.
A multivariate model was constructed to identify the factors associated with OS (Table 3) and CSS (Table 4). In multivariate analysis, ASA = 2 and ASA = 3 [hazard ratio (HR) = 1.535, p = 0.030; HR = 2.133, p = 0.001] were independent predictors of OS, along with age ≥65 years (HR = 1.869, p < 0.001), history of or with NMIBC (HR = 1.740, p < 0.001), high grade (HR = 1.665, p = 0.001), pT2–4 (HR = 1.585, p = 0.001), lymph node metastasis (HR = 1.898, p = 0.001), sessile tumor (HR = 1.360, p = 0.027), and differentiation (HR = 1.728, p = 0.009).
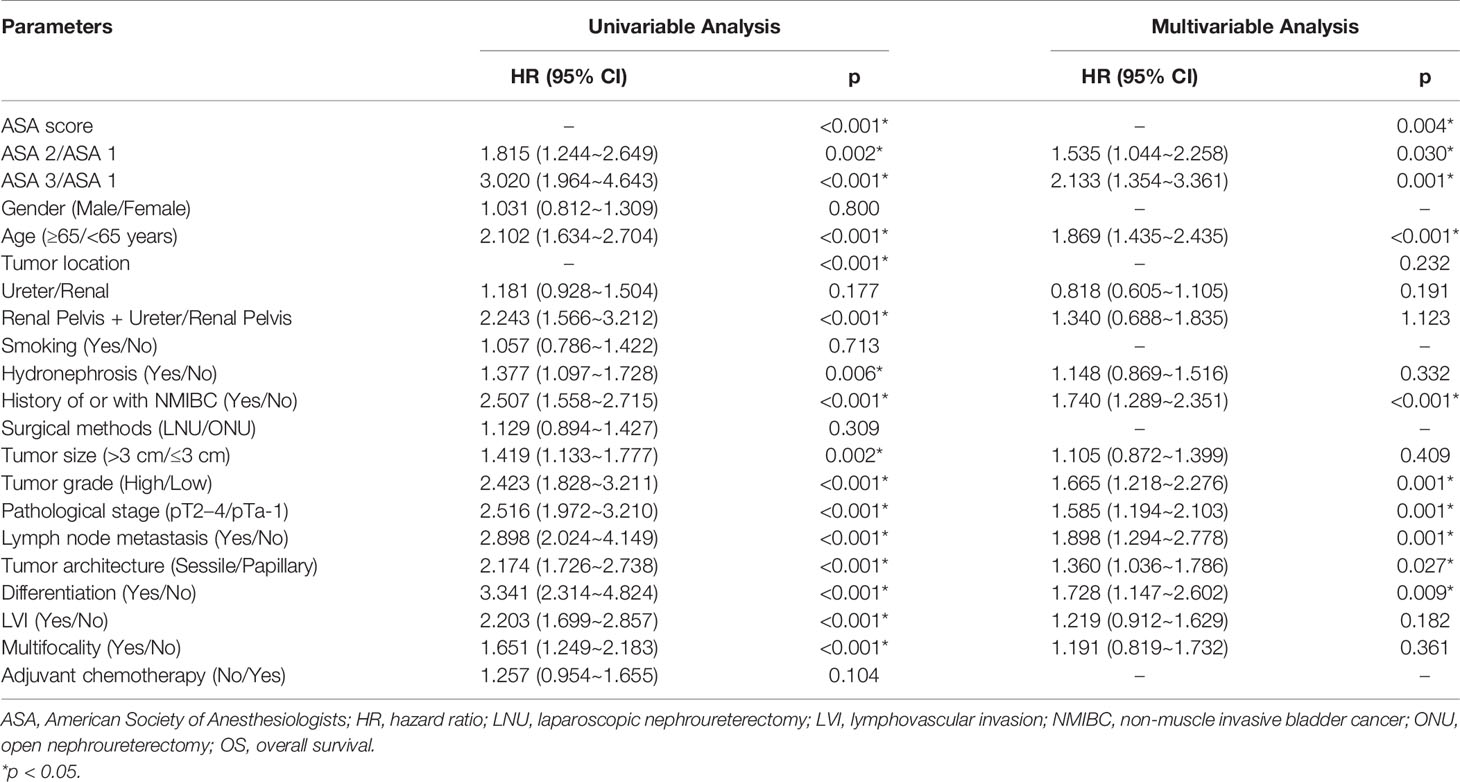
Table 3 Univariable and multivariable Cox regression models to predict OS.
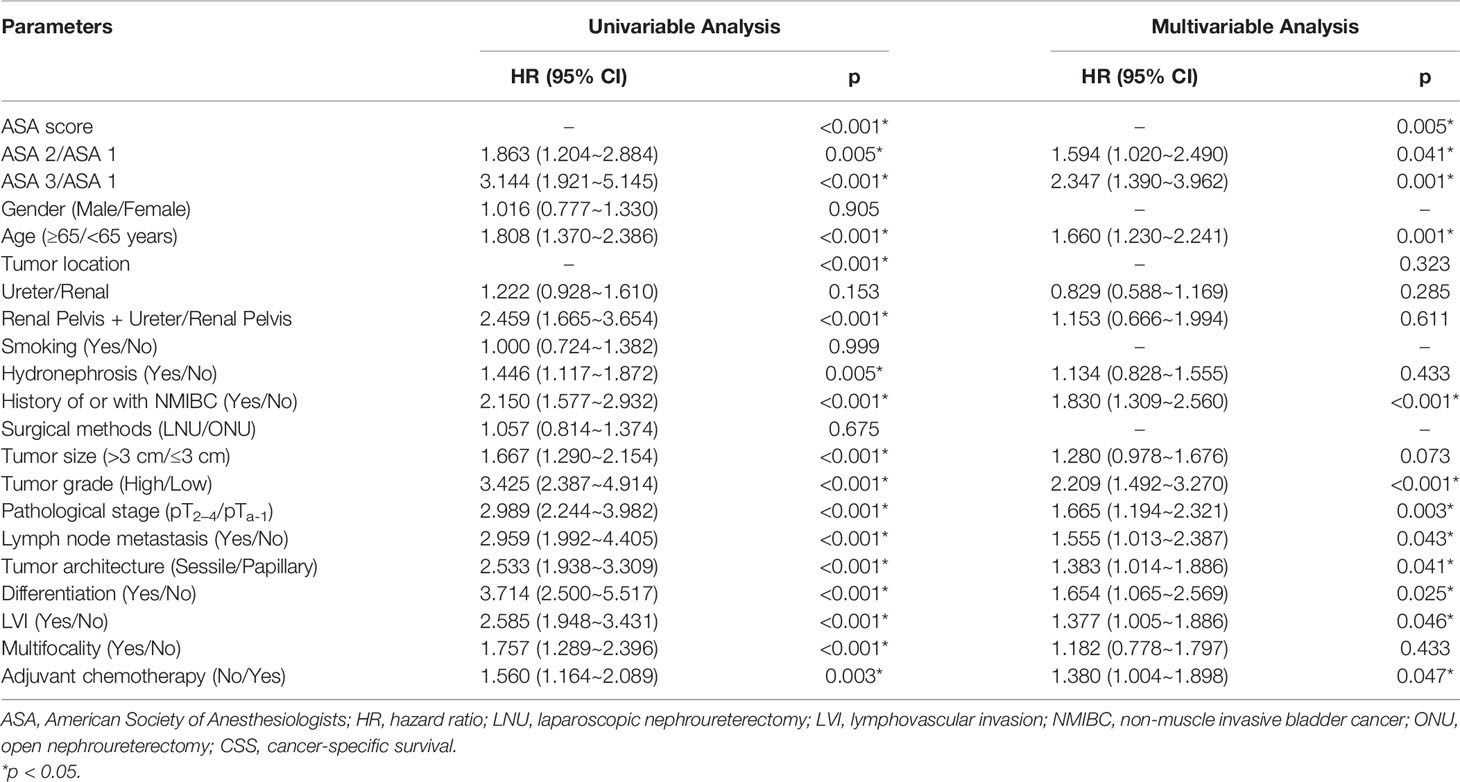
Table 4 Univariable and multivariable Cox regression models to predict CSS.
As to CSS, multivariable analysis also demonstrated that ASA = 2 and ASA = 3 (HR = 1.594, p = 0.041; HR = 2.347, p = 0.001) were independent predictors, along with age ≥65 years (HR = 1.660, p = 0.001), history of or with NMIBC (HR = 1.830, p < 0.001), high grade (HR = 2.209, p < 0.001), pT2–4 (HR = 1.665, p = 0.003), lymph node metastasis (HR = 1.555, p = 0.043), sessile tumor (HR = 1.383, p = 0.041), differentiation (HR = 1.654, p = 0.025), LVI (HR = 1.377, p = 0.046), and AC (HR = 1.380, p = 0.047).
Adjusting for multiple potential confounding factors, ASA = 2 (HR = 1.706, p = 0.017) and ASA = 3 (HR = 2.859, p < 0.001) remained independently associated with decreased MFS (Table 5). In addition, history of or with NMIBC (HR = 1.566, p = 0.013), high tumor grade (HR = 2.523, p < 0.001), pT2–4 (HR = 2.158, p < 0.001), lymph node metastasis (HR = 1.730, p = 0.009), and AC (HR = 1.651, p = 0.001) were independent prognostic factors.
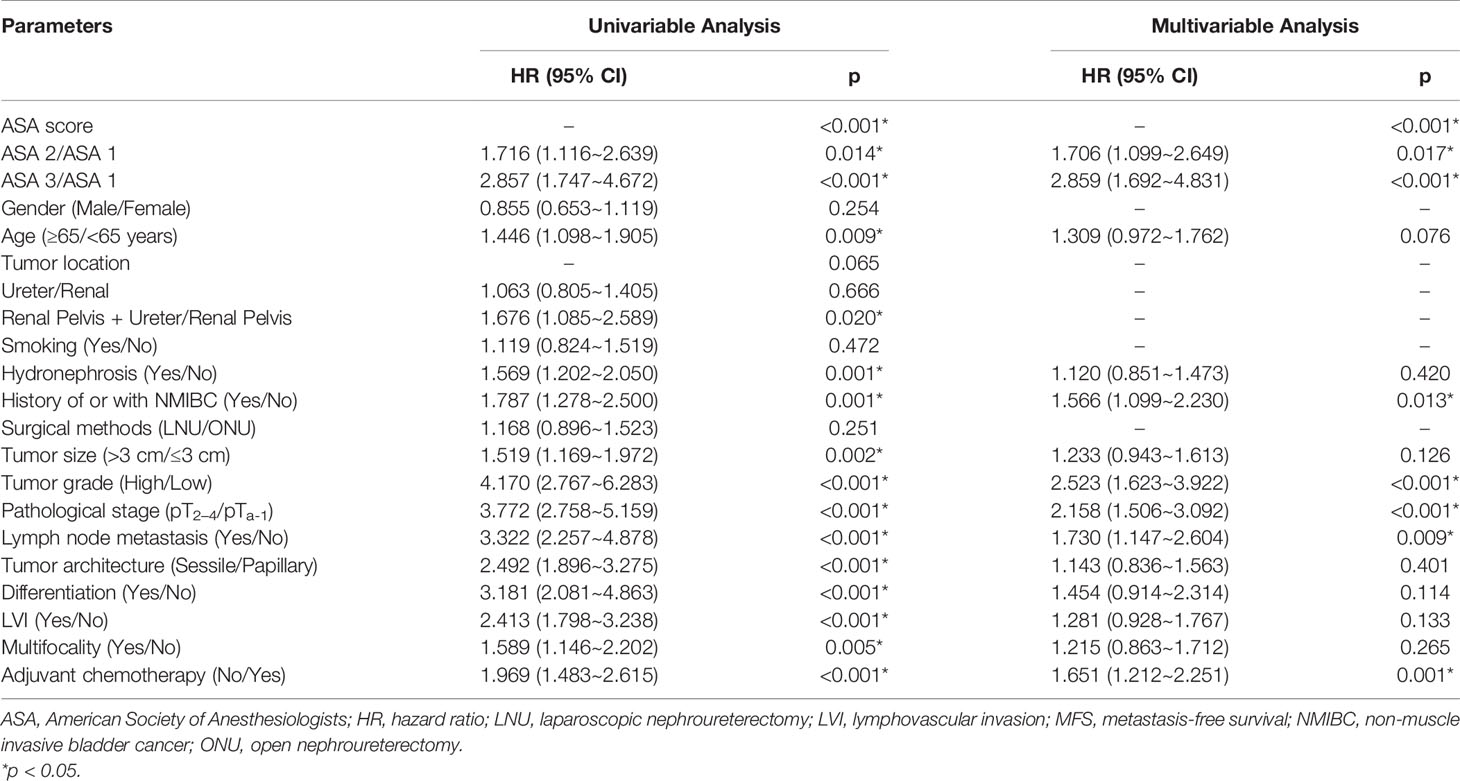
Table 5 Univariable and multivariable Cox regression models to predict MFS.
However, no significant difference was found in patients with different ASA scores in IRFS (Table 6). History of or with NMIBC (HR = 1.576, p = 0.022) and tumor size (HR = 1.379, p = 0.03) showed a significant effect on patients in the multivariate analysis.
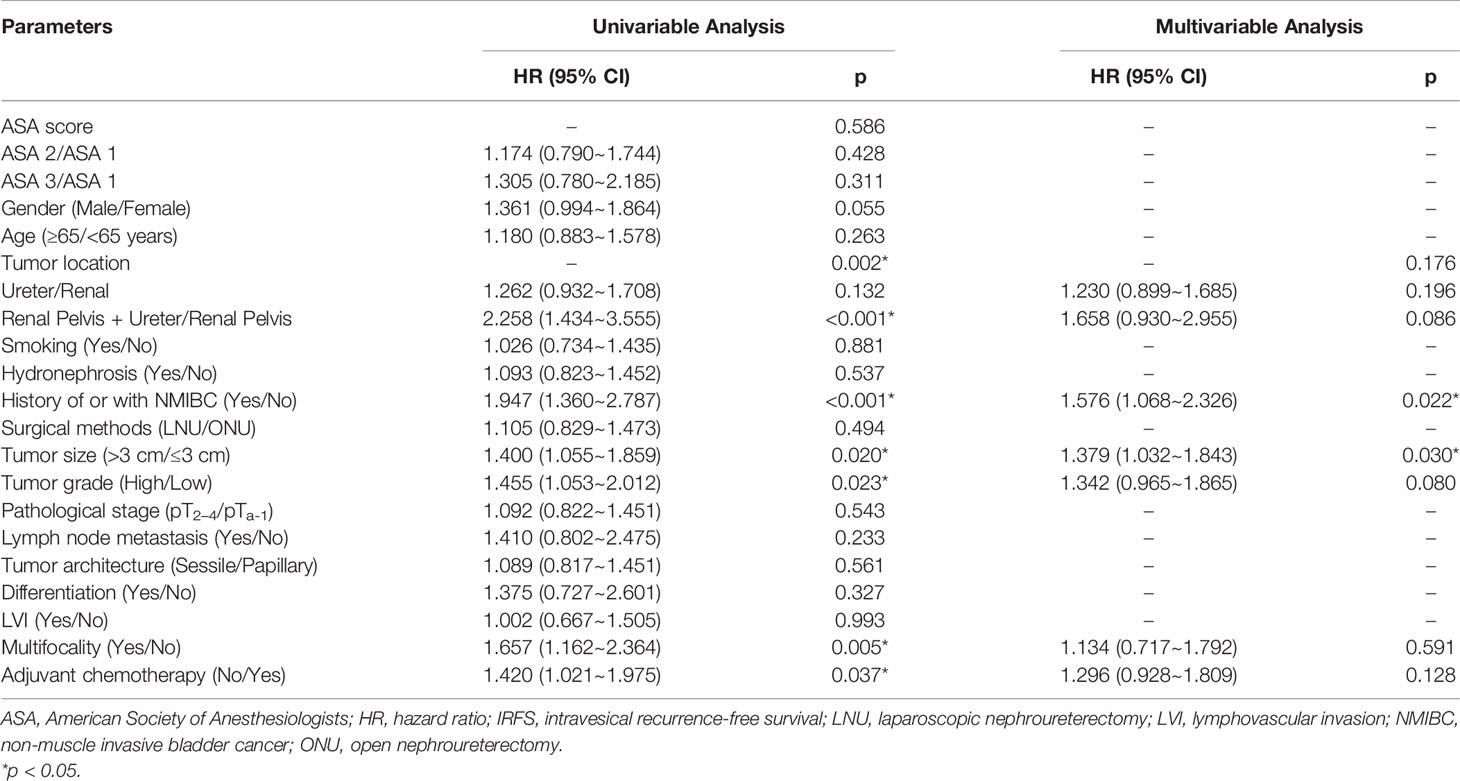
Table 6 Univariable and multivariable Cox regression models to predict IRFS.
Together with Adult Comorbidity Evaluation-27 (ACE-27), Charlson Comorbidity Index (CCI), and Eastern Cooperative Oncology Group (ECOG) performance status, the ASA-PS was one of the most commonly used comorbidity indices in the literature (14, 15).
In contrast to the ASA score, however, an anesthetist does not need to complete the CCI in practice schedule. Recently, some researchers aimed to quantify the relationship between the CCI and the ASA grade; the former was determined from documented International Classification of Diseases (ICD) codes, and the latter was assigned by the anesthetist. They have found that the addition of the demographic variables made for a much better predictive model and helped to explain considerably more of the variance in ASA grade than did CCI alone (16). That means in the real life of assigning an ASA grade, anesthetists would take full factors into account, not only the medical condition but also factors that may adversely influence a patient’s tolerance to an operative procedure. Such characteristics as well-documented data, such as age, body mass index (BMI), and lifestyle factors like smoking history, but perhaps also alcohol consumption and sometimes even the complexity of the planned surgery (17). ASA score was much more comprehensive than we might expect. It is also reported that the ASA score is superior to other notable scoring systems including the Charlson score (18) in predicting surgical outcomes. Admittedly, for UTUC, two systems ought to be further compared in randomized controlled trials. Unlike the results of our study, the 2021 European Association of Urology (EAU) Guidelines of muscle-invasive and metastatic bladder cancer (19) strongly recommend to “Assess comorbidity by a validated score, such as the Charlson Comorbidity Index. The American Society of Anesthesiologists score should not be used in this setting”.
ASA-PS has been demonstrated as a strong independent factor associated with postoperative morbidity and mortality (11, 20). Based on a large cohort of 6,301 patients who received surgery, Wolters et al. (21) have reported similar findings and found that high ASA score reflected delayed wound repair. Several studies have revealed that high ASA score was associated with prognosis in several urologic malignancies (9, 18, 22); limited evidence has shown that high ASA score was related to unfavorable prognosis in UTUC patients. Our results suggested that ASA score ≥2 was independently associated with poorer OS, CSS, and MFS, adjusting for a number of potential confounding variables. However, there was no significant difference with regard to IRFS between low and high ASA score groups in UTUC patients. This might indicate that ASA scores, as a general systemic status indicator, could not reflect localized disease completely. Additionally, we demonstrated the distinct relationship between ASA score and some clinicopathological characteristics, such as age, tumor size, LVI, and AC. Most of these indicators certainly had significant impact on the prognosis of UTUC patients (23–26).
Our results also showed that advanced age, high tumor grade and pathological stage, lymph node metastasis, sessile architecture, and differentiation were associated with worse OS and CSS, which was consistent with the results reported by Margulis et al. (27). Although previous studies have reported the prognostic value of ASA scores in UTUC patients (28, 29), our study is unique for several reasons. Primarily, in the present study, a total of 17 clinicopathological characteristics were analyzed, while a strong predictor of lymph node metastasis was not included in the study by Ho et al. (28) and only seven characteristics were collected in the study by Alexis et al. (29). Nearly twice as many in previous studies, a larger cohort had longer follow-up, and approximately 1,000 patients were retrospectively analyzed. Furthermore, given that survival is a heterogeneous endpoint, overall, cancer-specific, intravesical recurrence-free, and metastasis-free survival have all been involved.
Considering the underlying systemic disease with predisposition to poor recovery, infectious and cardiorespiratory complications were more common in patients with a high ASA score than in those with a low score. General condition and systemic illness were absolute barriers for systemic chemotherapy and also significant determinants of survival, as for ASA-PS, ranging from a healthy person (class 1) to one with a bad/severe systemic disorder that is a constant threat to life (30). When the cardiopulmonary system is not strong and working inefficiently, oxygen will not circulate all around the body helping to feed and renew our body tissues and vital organs (liver, kidney, et al.). Especially, there is additional task for tumor-host’s body to activate the antitumor effect, such as immunological function response. Different from other tumor types, renal insufficiency was an unavoidable problem for UTUC patients who underwent RNU. Renal insufficiency often constrains the choice of nephrotoxic chemotherapy regimen, which seems to be a challenge preventing the effective delivery of cisplatin-based chemotherapy (30–32). In this study, similarly, as ASA score increased, the proportion of AC has also risen (10.9%, 20.7%, and 26.9%, respectively, p = 0.003*; Table 2). It turns out that higher ASA score results in damage to the tumor-bearing host and tolerance to systemic therapy. In other words, disorder of the immune function will decrease the antitumor ability and simultaneously increase tumor burden (33).
Additionally, preoperative hydronephrosis and multifocality were considered to be correlated with adverse prognosis (8, 34); in contrast, our results found that these two indicators were not independent predictors. Our study reveals that hydronephrosis and multifocality do not appear to have a significant influence on survival outcome; this result has also been confirmed by previous studies (8, 35). We need to acknowledge a selection bias for exclusion of patients receiving AC. Given their impaired renal function, patients with hydronephrosis are more likely to miss the opportunity to receive AC after radical nephroureterectomy (36). The prognostic impact of multifocal UTUC has also been poorly understood. The ability of chemotherapy of eradicating micrometastasis has been widely recognized (37). Thomas et al. (8) have reported that tumor multifocality was not an independent predictor of both disease progression (HR = 1.43, p = 0.019) and CSS (HR = 1.46, p = 0.027) in advanced UTUC (stratified by non-confined type, the confounding effect of AC cannot be adequately adjusted).
There were several limitations associated with this study. Firstly, a retrospective analysis may cause a selection bias. Secondly, potential predictors including BMI, history of aristolochic acid, and preoperative renal function were not available. Thirdly, lymphadenectomy was not routinely performed and the extent of lymph node dissection was not standardized because the pattern and benefits of lymphadenectomy were still controversial. Moreover, as widely acknowledged, surgical patients with higher ASA score developed substantially higher rates of perioperative medical complications (20). Unfortunately, we do not know the detailed information of patients who have suffered perioperative complications. It was really a huge effort for researchers from two institutions to collect undocumented clinical data for almost a thousand patients. This aspect was an unavoidable limitation in the current study but could be improved by further study. Based on a large number of cases, the detailed clinical and pathological data with long-term follow-up of UTUC patients from two institutions in China, this study was able to provide more convincing information to clinicians.
We suggest that RNU is safe for selected patients with UTUC. However, higher ASA score predicts poor clinical outcomes, and it was a significant prognostic factor for OS, CSS, and MFS. This prognostic factor may be a useful variable to include into future risk prediction and contribute to clinical decision-making. Long-term and larger-scale studies may produce more reliable results.
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
This study was approved by institutional review board, and approval number was 2020-369.
YY and YW contributed to the conceptualization, methodology, validation, visualization, formal analysis, investigation, and writing the original draft. NZ contributed to the conceptualization, resources, and funding acquisition. XM contributed to the methodology, visualization, software, and validation. YH contributed to the methodology, visualization, and software. JH and NJ contributed to the methodology, data curation, validation, investigation, resources, and writing–review and editing. All authors contributed to the article and approved the submitted version.
This work was supported financially by Zhejiang Provincial Natural Science and Technology Department Public Welfare Projects (grant number LGC21H050001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.723669/full#supplementary-material
1. Alva AS, Matin SF, Lerner SP, Siefker-Radtke AO. Perioperative Chemotherapy for Upper Tract Urothelial Cancer. Nat Rev Urol (2012) 9(5):266–73. doi: 10.1038/nrurol.2012.57
2. Gayed BA, Thoreson GR, Margulis V. The Role of Systemic Chemotherapy in Management of Upper Tract Urothelial Cancer. Curr Urol Rep (2013) 14(2):94–101. doi: 10.1007/s11934-013-0307-z
3. Kang HW, Jung HD, Ha YS, Kim TH, Kwon TG, Byun SS, et al. Preoperative Underweight Patients With Upper Tract Urothelial Carcinoma Survive Less After Radical Nephroureterectomy. J Korean Med Sci (2015) 30(10):1483–9. doi: 10.3346/jkms.2015.30.10.1483
4. Fairey AS, Kassouf W, Estey E, Tanguay S, Rendon R, Bell D, et al. Comparison of Oncological Outcomes for Open and Laparoscopic Radical Nephroureterectomy: Results From the Canadian Upper Tract Collaboration. BJU Int (2013) 112(6):791–7. doi: 10.1111/j.1464-410X.2012.11474.x
5. Pichler M, Dalpiaz O, Ehrlich GC, Stojakovic T, Martín Hernández JM, Mannweiler S, et al. Validation of the Preoperative Plasma Fibrinogen Level as a Prognostic Factor in a European Cohort of Patients With Localized Upper Tract Urothelial Carcinoma. J Urol (2014) 191(4):920–5. doi: 10.1016/j.juro.2013.10.073
6. Yates DR, Hupertan V, Colin P, Ouzzane A, Descazeaud A, Long JA, et al. French Collaborative National Database on UUT-UC: Cancer-Specific Survival After Radical Nephroureterectomy for Upper Urinary Tract Urothelial Carcinoma: Proposal and Multi-Institutional Validation of a Post-Operative Nomogram. Br J Cancer (2012) 106(6):1083–6. doi: 10.1038/bjc.2012.64
7. Ku JH, Byun SS, Jeong H, Kwak C, Kim HH, Lee SE. Lymphovas-Cular Invasion as a Prognostic Factor in the Upper Urinary Tract Urothelial Carcinoma: A Systematic Review and Meta-Analysis. Eur J Cancer (2013) 49(12):2665–80. doi: 10.1016/j.ejca.2013.04.016
8. Chromecki TF, Cha EK, Fajkovic H, Margulis V, Novara G, Scherr DS, et al. the Impact of Tumor Multifocality on Outcomes in Patients Treated With Radical Nephroureterectomy. Eur Urol (2012) 61(2):245–53. doi: 10.1016/j.eururo.2011.09.017
9. Djaladat H, Bruins HM, Miranda G, Cai J, Skinner EC, Daneshmand S. The Association of Preoperative Serum Albumin Level and American Society of Anesthesiologists (ASA) Score on Early Complications and Survival of Patients Undergoing Radical Cystectomy for Urothelial Bladder Cancer. BJU Int (2014) 113(6):887–93. doi: 10.1111/bju.12240
10. Takagi K, Yagi T, Yoshida R, Shinoura S, Umeda Y, Nobuoka D, et al. Sarcopenia and American Society of Anesthesiologists Physical Status in the Assessment of Outcomes of Hepatocellular Carcinoma Patients Undergoing Hepatectomy. Acta Med Okayama (2016) 70(5):363–70. doi: 10.18926/AMO/54594
11. Kolehmainen AM, Pasanen A, Tuomi T, Koivisto-Korander R, Butzow R, Loukovaara M. American Society of Anesthesiologists Physical Status Score as a Predictor of Long-Term Outcome in Women With Endometrial Cancer. Int J Gynecol Cancer (2019). 29:879–85. doi: 10.1136/ijgc-2018-000118
12. Compérat E, Varinot J, Eymerit C, Paner GP, Hansel DE, Amin MB, et al. Comparison of UICC and AJCC 8th Edition TNM Classifications in Uropathology Ann Pathol (2019) 39(2):158–66. doi: 10.1016/j.annpat.2018.12.005
13. Moch H, Cubilla AL, Humprey PA, Reuter VE, Ulbright TM. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur Urol (2016) 70(1)77–98.
14. Aziz A, Fritsche HM, Gakis G, Kluth LA, Fa H, Engel O, et al. Comparative Analysis of Comorbidity and Performance Indices for Prediction of Oncological Outcomes in Patients With Upper Tract Urothelial Carcinoma Who Were Treated With Radical Nephroureterectomy. Urol Oncol (2014) 32(8):1141–50. doi: 10.1016/j.urolonc.2014.04.008
15. Mayr R, May M, Martini T, Lodde M, Comploj E, Pycha A, et al. Comorbidity and Performance Indices as Predictors of Cancer-Independent Mortality But Not of Cancer-Specific Mortality After Radical Cystectomy for Urothelial Carcinoma of the Bladder. Eur Urol (2012) 62(4):662–70. doi: 10.1016/j.eururo.2012.03.057
16. Mannion AF, Bianchi G, Mariaux F, Fekete TF, Reitmeir R, Moser B, et al. Can the Charlson Comorbidity Index be Used to Predict the ASA Grade in Patients Undergoing Spine Surgery? Eur Spine J (2020) 29:2941–52. doi: 10.1007/s00586-020-06595-1
17. Fitz J. The ASA Classifcation and Peri-Operative Risk. Ann R Coll Surg Engl (2011) 93:185–7. doi: 10.1308/rcsann.2011.93.3.185a
18. Froehner M, Koch R, Litz R. Comparison of the American Society of Anesthesiologists Physical Status Classification With the Charlson Score as Predictors of Survival After Radical Prostatectomy. Urology (2003) 62):698 – 701. doi: 10.1016/S0090-4295(03)00570-3
19. Witjes JA, Bruins H, Cathomas R, Compérat EM, Cowan NC, Gakis G, et al. European Association of Urology Guidelines on Muscle-Invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur Urol (2021) 79(1):82–104. doi: 10.1016/j.eururo.2020.03.055
20. Hackett NJ, Oliveira GSD, Jain UK, Kim JY. ASA Class is a Reliable Independent Predictor of Medical Complications and Mortality Following Surgery. Int J Surg (2015) 18:184–90. doi: 10.1016/j.ijsu.2015.04.079
21. Wolters U, Wolf T, Stutzer H, Schroder T. ASA Classification and Perioperative Variables as Predictors of Postoperative Outcomes. Br J Anaesth (1996) 77(2):217–22. doi: 10.1093/bja/77.2.217
22. Zequi S, Campos E, Guimaraes G, Bachega W, Fonseca F, Lopes A. The Use of the American Society of Anesthesiology Classification as a Prognostic Factor in Patients With Renal Cell Carcinoma. Urol Int (2010) 84(1):67–72. doi: 10.1159/000273469
23. Liu W, Sun L, Guan F, Wang F, Zhang G. Prognostic Value of Lymphovascular Invasion in Upper Urinary Tract Urothelial Carcinoma After Radical Nephroureterectomy: A Systematic Review and Meta-Analysis. Dis Markers (2019) 7386140:1–15. doi: 10.1155/2019/7386140
24. Song SH, Ye CH, Lee S, Hong SK, Byun SS, Lee SE, et al. Association Between Lymphovascular Invasion and Oncologic Outcomes Among Upper Urinary Tract Urothelial Carcinoma Patients Who Underwent Radical Nephroureterectomy. J Cancer Res Clin Oncol (2019) 145(11):2863–70. doi: 10.1007/s00432-019-03020-z
25. Jan HC, Hu CY, Yang WH, Ou CH. Combination of Platelet-Lymphocyte Ratio and Monocyte-Lymphocyte Ratio as a New Promising Prognostic Factor in Upper Tract Urothelial Carcinoma With Large Tumor Sizes >3 Cm. Clin Genitourin Cancer (2019) 18(4):e484–500. doi: 10.1016/j.clgc.2019.12.008
26. Leow JJ, Liu Z, Tan TW, Lee YM, Yeo EK, Chong YL. Optimal Management of Upper Tract Urothelial Carcinoma: Current Perspectives. Onco Targets Ther (2020) 13:1–15. doi: 10.2147/OTT.S225301
27. Margulis V, Shariat SF, Martin SF, Kamat AM, Zigeuner R, Kikuchi E, et al. Outcomes of Radical Nephroureterectomy: A Series From the Upper Tract Urothelial Carcinoma Collaboration. Cancer (2009) 115(6):1224–33. doi: 10.1002/cncr.24135
28. Ho WK, Sung PS, Won TK, Yong JK, Seok JY, Sang CL, et al. Impact of the ASA Physical Status Score on Adjuvant Chemotherapy Eligibility and Survival of Upper Tract Urothelial Carcinoma Patients a Multicenter Study. J Korean Med Sci (2017) 32(2):335–42. doi: 10.3346/jkms.2017.32.2.335
29. Alexis AB, Pierre C, David RY, Adil O, Marie A, Emilie A, et al. The Role of American Society of Anesthesiologists Scores in Predicting Urothelial Carcinoma of the Upper Urinary Tract Outcome After Radical Nephroureterectomy: Results From a National Multi-Institutional Collaborative Study. BJU Int (2012) 110(11 Pt C):E1035–40. doi: 10.1111/j.1464-410X.2012.11195.x
30. Kawai K, Ichioka D, Inai H, Miyazaki J, Nishiyama H. Assessment and Management of Renal Impairment in Chemotherapy for Urogenital Cancer. Jpn J Clin Oncol (2013) 43:1055–63. doi: 10.1093/jjco/hyt132
31. Fang D, Zhang Q, Li X, Qian C, Xiong G, Zhang L, et al. Nomogram Predicting Renal Insufficiency After Nephroureterectomy for Upper Tract Urothelial Carcinoma in the Chinese Population: Exclusion of Ineligible Candidates for Adjuvant Chemotherapy. BioMed Res Int (2014) 2014:529186. doi: 10.1155/2014/529186
32. Xylinas E, Rink M, Margulis V, Clozel T, Lee RK, Comploj E, et al. Impact of Renal Function on Eligibility for Chemotherapy and Survival in Patients Who Have Undergone Radical Nephro-Ureterectomy. BJU Int (2013) 112:453–61. doi: 10.1111/j.1464-410X.2012.11649.x
33. Schirrmacher V. From Chemotherapy to Biological Therapy: A Review of Novel Concepts to Reduce the Side Effects of Systemic Cancer Treatment. Int J Oncol (2019) 54(2):407–19. doi: 10.3892/ijo.2018.4661
34. Fukui T, Kanno T, Kobori G, Moroi S, Yamada H. Preoperative Hydronephrosis as a Predictor of Postnephroureterectomy Survival in Patients With Upper Tract Urothelial Carcinoma: A Two-Center Study in Japan. Int J Clin Oncol (2020) 25(3):456–63. doi: 10.1007/s10147-019-01535-6
35. Haleblian GE, Skinner EC, Dickinson MG, Lieskovsky G, Boyd SD, Skinner DG. Hydronephrosis as a Prognostic Indicator in Bladder Cancer Patients. J Urol (1998) 160:2011–4. doi: 10.1016/S0022-5347(01)62228-6
36. Hoshino K, Kikuchi E, Tanaka N, Akita H, Ito Y, Miyajima A, et al. Preoperative Hydronephrosis: Independent Predictor for Changes in Renal Function Following Nephroureterectomy. Jpn J Clin Oncol (2012) 42(1):202–7. doi: 10.1093/jjco/hyr199
Keywords: radical nephroureterectomy, upper tract urothelial cancer, prognosis, survival, American Society of Anesthesiologists (ASA) score
Citation: Yuan Y, Wang Y, Zhang N, Mao X, Huang Y, Huang J and Ji N (2021) Influence of American Society of Anesthesiologists Score on Oncologic Outcomes in Patients With Upper Tract Urothelial Carcinoma After Radical Nephroureterectomy: A Large-Sample Study in Two Institutions. Front. Oncol. 11:723669. doi: 10.3389/fonc.2021.723669
Received: 11 June 2021; Accepted: 09 September 2021;
Published: 04 October 2021.
Edited by:
Takahiro Osawa, Hokkaido University Hospital, JapanReviewed by:
Hsiang Ying Lee, Kaohsiung Medical University Hospital, TaiwanCopyright © 2021 Yuan, Wang, Zhang, Mao, Huang, Huang and Ji. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiwei Huang, aHVhbmdqaXdlaUByZW5qaS5jb20=; Na Ji, MjMxMjA3MUB6anUuZWR1LmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.