 Xue Yang1,2
Xue Yang1,2 Yao Xie
Yao Xie
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol. , 20 August 2021
Sec. Hematologic Malignancies
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.717678
Background: Anti-thymocyte globulin (ATG) prophylaxis reduces graft-versus-host disease (GVHD) incidence. This meta-analysis aimed to explore the long-term efficacy of ATG and the influencing factors in patients undergoing allogeneic hematopoietic stem cell transplantation (allo-HSCT).
Methods: PubMed, Embase, and Cochrane databases were searched for the relevant studies published up to August 2020. Data from randomized controlled trials (RCTs) on ATG prophylaxis for GVHD prevention in allo-HSCT patients were extracted.
Results: A total of eight relevant RCTs (1,348 patients) were included. ATG significantly reduced the incidence of grade III–IV aGVHD (P = 0.001) and cGVHD (P < 0.001). ATG significantly improved the GVHD relapse-free survival (GRFS) (P < 0.001). The immunosuppressive regimen (number and dose of immunosuppressants) was significantly reduced when using ATG (P = 0.005). Epstein-Barr virus (EBV) reactivation was high in patients receiving ATG (P = 0.003). No significant differences were detected in relapses, overall survival (OS), relapse-free survival (RFS), and non-relapse mortality (NRM) between the ATG and no ATG groups. Subgroup analyses revealed that the donor type and ATG formulation might be the possible sources of heterogeneity among the included studies. Meta-regression analysis showed that the cumulative dose of ATG did not affect GVHD, OS, relapse, RFS, and NRM.
Conclusion: Although ATG had no significant effect on relapse, RFS, and NRM, it significantly reduced the occurrence and severity of GVHD, improved the GRFS, and reduced the number and dose of immunosuppressants in patients undergoing allo-HSCT.
Hematopoietic stem cell transplantation (HSCTs) is a major treatment option for patients with malignant blood diseases, but the clinical management of post-transplantation complications can be challenging (1, 2). Graft-versus-host disease (GVHD) is the major life-threatening complication following allo-HSCT (3, 4). Drug-related toxicity; infections by viruses bacteria, and fungi; immune-mediated disorders; and disease recurrence can also lead to potentially lethal complications (5, 6). Still, the acute GVHD (aGvHD) rates have significantly improved in recent years (7).
Different anti-thymocyte globulin (ATG) formulations can be used for T-cell depletion, thereby reducing the risk of rejection in allo-HSCTs (8). The addition of ATG to standard cyclosporine A and methotrexate prophylaxis is widely applied for GVHD prevention prior to allo-HSCT (9). Still, the long-term efficacy of ATG for allo-HSCT is yet to be elucidated. Several studies evaluated the efficacy of ATG plus standard GVHD prophylaxis in patients with hematological malignancies who received myeloablative conditioning (MAC) or reduced-intensity conditioning (RIC) regimen from related and unrelated donors prior to allo-HSCT (10–12). A meta-analysis suggested that ATG significantly reduces the risk of acute and chronic GVHD, whereas the impact of ATG on disease relapse and the survival of patients was unsure (13). The effect of ATG on long-term prognosis has not been analyzed in previous meta-analyses (8, 13–15). The composite endpoints of GVHD relapse-free survival (GRFS) and free of immunosuppressive therapy (i.e., immunosuppressants are no longer necessary) are considered indicators of allo-HSCT completion (10, 16, 17). In addition, there was a lack of in-depth analysis to identify factors that affect the efficacy of ATG. Recently, three additional randomized controlled trials (RCTs) assessing long-term outcomes have been published. Walker et al. showed that the addition of ATG resulted in improved 2-year survival and decreased use of immunosuppressive therapy after unrelated donor transplantation (16). Chang et al. found an improved 3-year GRFS in patients undergoing sibling donor transplantation (10). Bonifazi et al. reported that patients receiving sibling donor transplantation showed improved 5-year GRFS and short immunosuppressive treatment, whereas the overall survival (OS) did not differ significantly (17).
This updated meta-analysis aimed to assess the impact of ATG therapy on acute and chronic GVHD, OS, GRFS, free of immunosuppressant therapy, relapse, RFS, non-relapse mortality (NRM), and infections, the effect of the optimal donor source, and the formulation of ATG in allo-HSCT.
This meta-analysis was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (18). A systematic search was performed from databases including PubMed, Embase, the Cochrane Library, and Clinical Trials Registry for potentially eligible studies published up to August 2020. The key terms “hematopoietic stem cell,” “allogeneic hematopoietic cell transplantation,” and “anti-thymocyte globulin” were used to identify the relevant publications. The reference lists from the retrieved studies were reviewed to identify any additional eligible studies.
The inclusion criteria were as follows: (1) population: stem cell transplantation for a hematological malignancy; there were no restrictions on matching during this screening process as long as the patients were undergoing allo-HSCT; (2) intervention: ATG and standard GVHD prophylaxis; (3) control: standard GVHD prophylaxis; (4) outcomes: III–IV aGVHD, cGVHD, OS, GRFS, free immunosuppressant therapy (no longer needing immunosuppressant therapy), the incidence of relapse, RFS, NRM, and infections; (5) study design: RCTs; and (6) language was limited to English. All steps of the study were conducted independently by two investigators (XY and DL).
The study characteristics, including the first author’s name, NCT register ID, sample size, age and sex of the patients, donor source, intervention arms, ATG formulation and dose, follow-up, and outcomes, were extracted by two authors (XY and DL) independently. If a study reported hazard ratio (HR), the data of HR and 95% confidence interval (CI) were extracted. Otherwise, the risk ratio (RR) and 95% CI with events in two arms were calculated. The level of evidence of all articles was assessed independently by two authors (XY and DL) according to the Cochrane Handbook. Any discrepancy was resolved by discussion.
RRs and corresponding 95% CIs were used to summarize the data. Statistical heterogeneity among studies was calculated using Cochran’s Q test and the I2 index (19). Since the population originated from different countries and there was heterogeneity in the interventions, the random-effects model was used. Subgroup analyses according to donor source (related vs. unrelated donors) and ATG formulation (ATG thymoglobulin vs. anti-T lymphocyte globulin (ATLG)) were conducted. Meta-regression analysis was used to evaluate the correlation between the cumulative dose of ATG and post-transplantation outcomes. Nonetheless, we did not assess the possible publication bias by funnel plots and Egger’s test since the number of studies included in each quantitative analysis was <10 (20). All analyses were performed using STATA SE 14.0 (StataCorp, College Station, TX, USA).
The initial literature search retrieved 531 relevant articles. Subsequently, eight RCTs that fulfilled the criteria were included in the final meta-analysis (10–12, 16, 17, 21–27). The search and selection process is illustrated in Supplementary Figure 1.
The characteristics of the included studies are summarized in Table 1. The eight studies encompassed 1,348 patients, including 683 cases in the ATG group and 665 cases in the control group. The median follow-up was 2 (range, 1–5) years. Five trials used rabbit ATG (Sanofi Genzyme, Cambridge, MA, USA) derived from human thymocytes, while three trials used rabbit ATLG (Neovii, Rapperswil, Switzerland) derived from the human Jurkat T cell line. Related donors were used in four studies, and the others used unrelated donors. The dose varied from 4.5 to 15 mg/kg for ATG and 10 to 60 mg/kg for ATLG. The overall methodological quality of included studies ranged from moderate to very low.
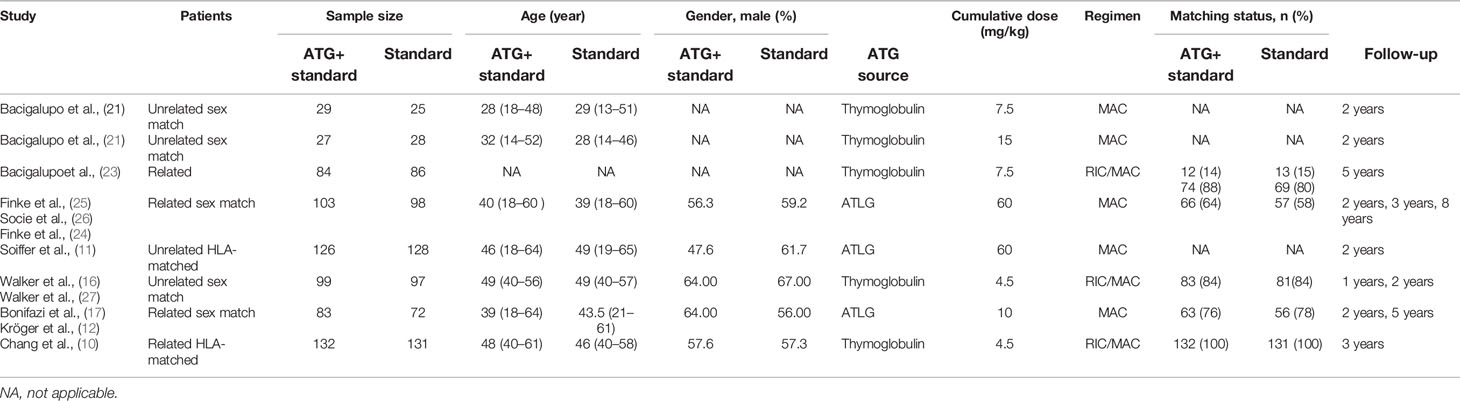
Table 1 Characteristics of studies included in the meta-analysis.
The overall pooled analysis of the eight studies showed that adding ATG to GVHD prophylaxis reduced the incidence of grade III–IV aGVHD (RR = 0.558, 95% CI = 0.400–0.779, P = 0.001; I2 = 37.4%; Pheterogeneity = 0.131; Figure 1A). The prevention of severe aGVHD was also observed in related (RR = 0.518, 95% CI = 0.343–0.782, P = 0.002), ATG (RR = 0.589, 95% CI = 0.378–0.917, P=0.019), and ATLG (RR = 0.457, 95% CI = 0.299–0.699, P < 0.001) subgroup analysis after prophylactic treatment with ATG. Moreover, ATG treatment significantly reduced cGVHD (RR = 0.446, 95% CI = 0.336–0.592, P < 0.001; I2 = 52.5%; Pheterogeneity = 0.049; Figure 1B) in all patients, and all subgroup analyses revealed similar benefits (Table 2). Meta-regression analysis showed that the cumulative dose of ATG did not affect both grade III–IV aGVHD and cGVHD (Supplementary Figures 2A, B).

Table 2 Summary of subgroup results.
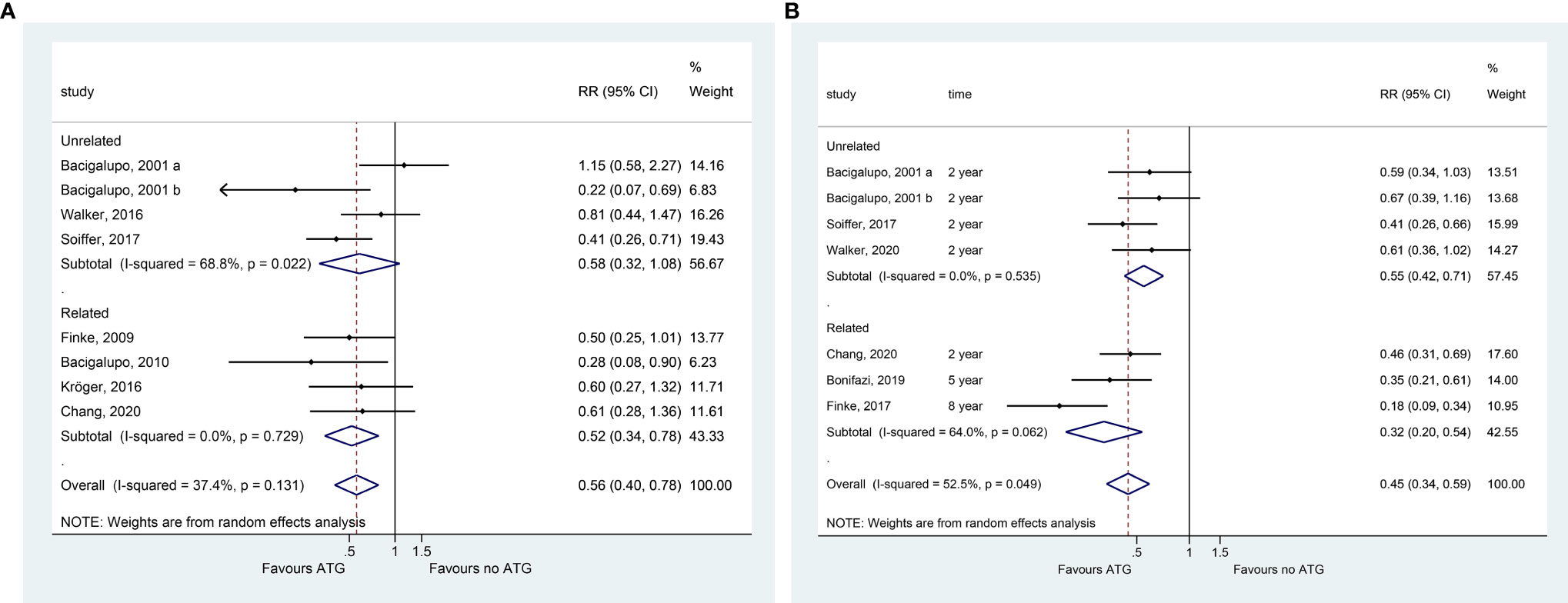
Figure 1 Forest plot for III–IV acute GVHD (A) and chronic GVHD (B).
All eight studies presented OS data. Typically, patients treated with ATG did not benefit in terms of OS (RR = 0.922, 95% CI = 0.736, P = 0.48; I2 = 46.8%; Pheterogeneity = 0.068). In the subgroup analyses, no significant differences were detected in OS in the unrelated donors, related donors, ATG, and ATLG groups (Figure 2 and Table 2). The meta-regression analysis showed that the cumulative dose of ATG did not affect the OS (Supplementary Figure 2C).
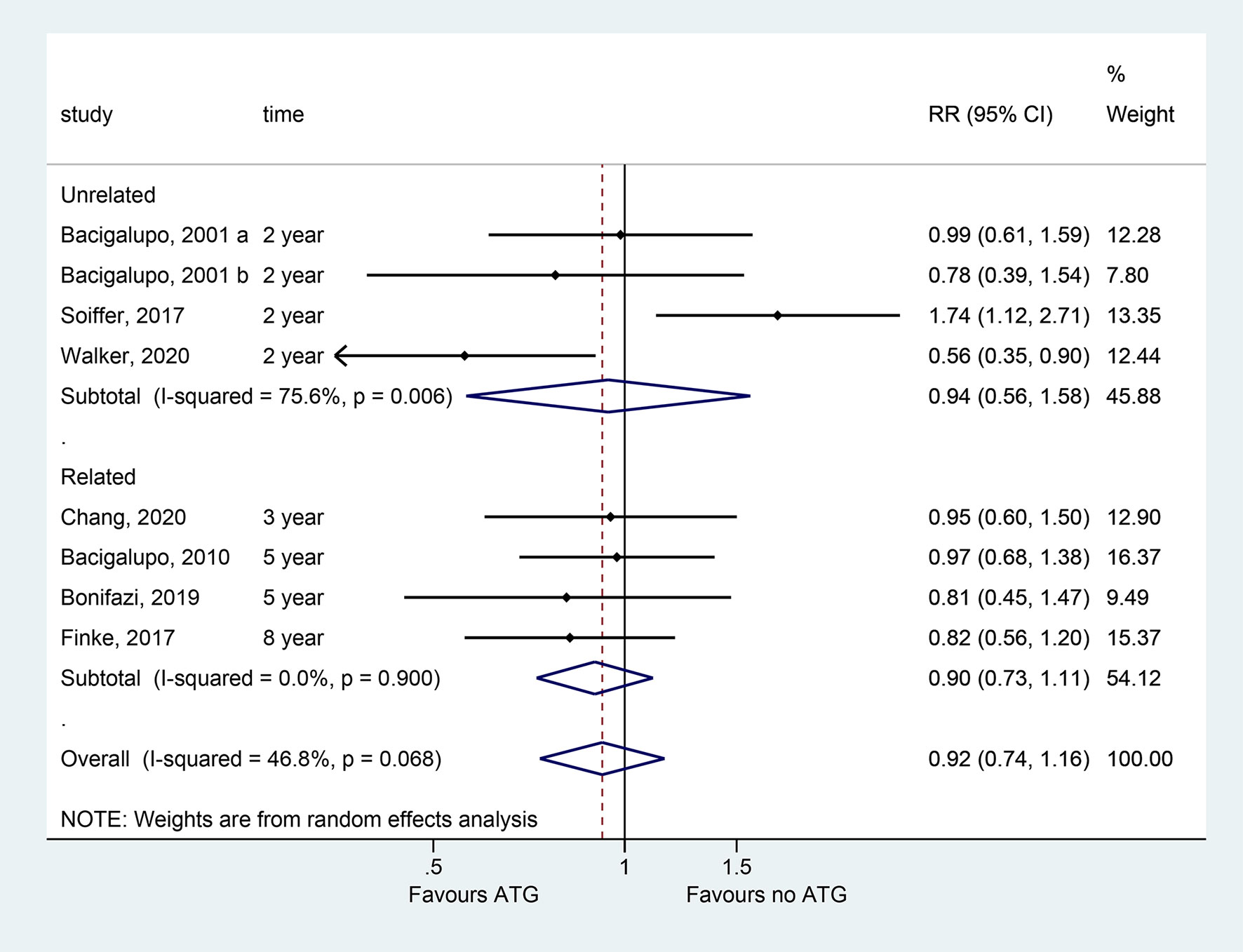
Figure 2 Forest plots of OS.
All eight studies presented relapse data. The incidence of relapse did not change with ATG in the whole sample (RR = 1.201, 95% CI = 0.970–1.488, P = 0.093; Figure 3A), as well as in the related, unrelated, and ATG subgroups. Adding ATLG in the conditioning regimen significantly reduced the risk of disease relapse according to the pooled analysis of four studies (RR = 1.495, 95% CI = 1.045–2.140, P = 0.028) (Figure 3A and Table 2). The meta-regression analysis showed that the cumulative dose of ATG did not affect relapse (Supplementary Figure 2D).
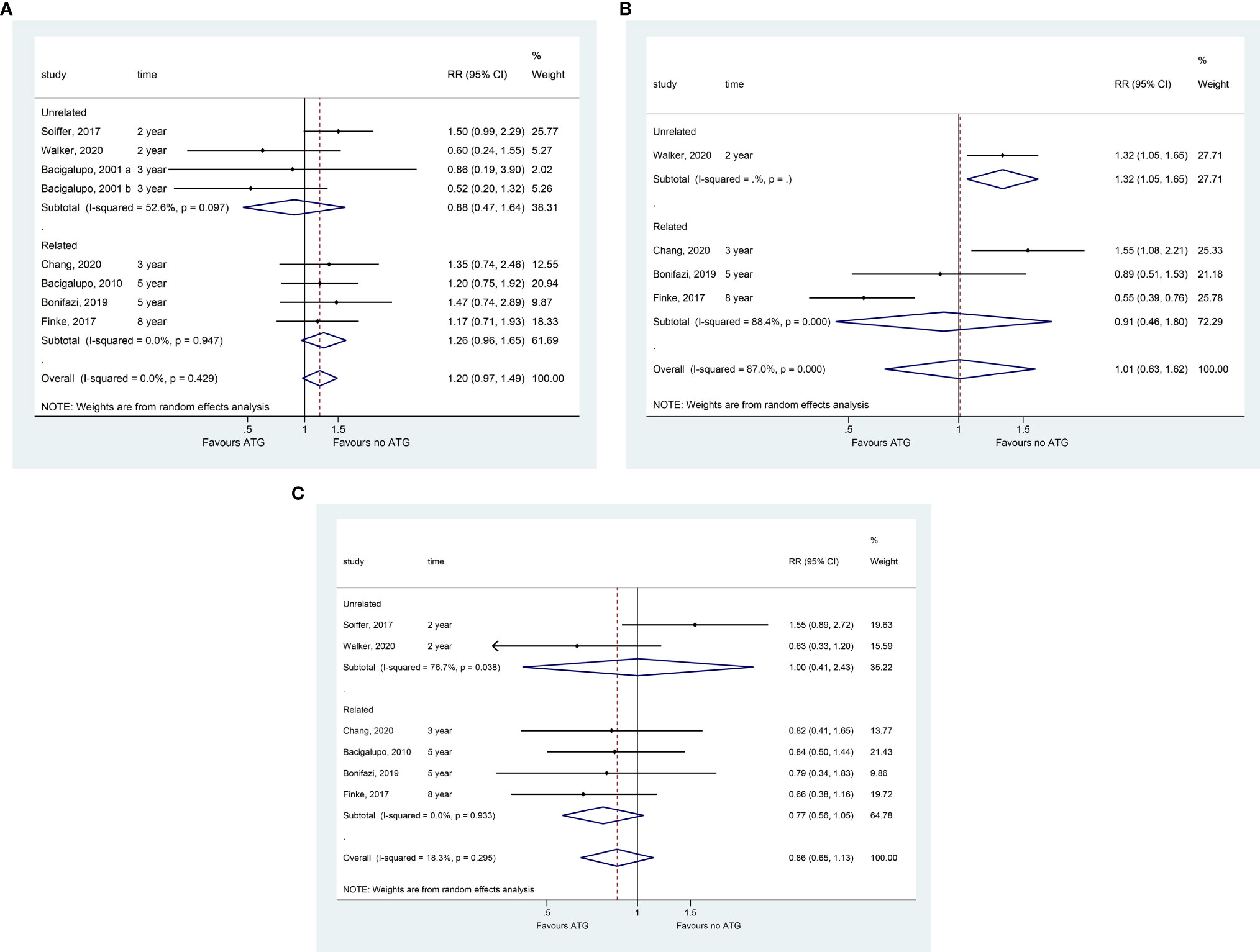
Figure 3 Forest plot for the incidence of relapse (A), RFS (B), and NRM (C).
Only one study suggested that ATG significantly reduced the RFS in patients undergoing transplantation from unrelated donors (RR = 1.319, 95% CI = 1.054–1.651, P = 0.016; Figure 3B). No significant decline was observed in RFS reduction in the overall and other subgroup pooled analyses (Table 2). The meta-regression analysis showed that the cumulative dose of ATG did not affect the OS (Supplementary Figure 2E).
Adding ATG, but not ATLG, significantly improved NRM (RR = 0.734, 95% CI = 0.545–0.989, P = 0.042; Figure 3C). Compared to the no ATG group, ATG did not cause any significant difference in NRM based on the overall pooled analysis and related and unrelated subgroups analyses (Table 2).
Three studies assessing GRFS suggested that ATG with GVHD prophylaxis improved the GRFS (RR = 0.551, 95% CI = 0.432–0.703, P < 0.001) (Figure 4A).
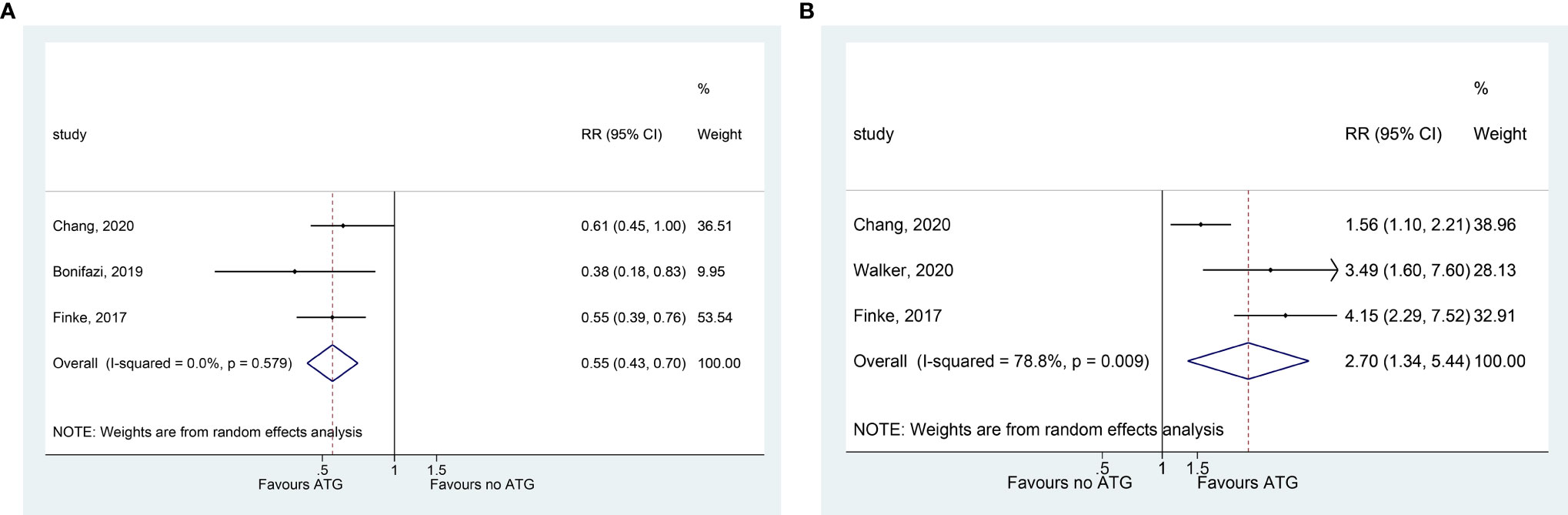
Figure 4 Forest plot for GRFS (A) and free of immunosuppressant therapy (B).
Compared with GVHD prophylaxis without ATG, a shorter immunosuppressive treatment was needed after the addition of ATG (RR = 2.700, 95% CI = 1.340–5.440, P = 0.005; three studies) (Figure 4B).
Epstein-Barr virus (EBV) reactivation (based on viremia monitoring) was common in patients who received ATG (RR = 3.882, 95% CI = 1.576–9.564, P = 0.003; three studies) (Figure 4B). However, GVHD prophylaxis with ATG did not significantly increase the total infection events, CMV reactivation, and fungal infections (Figure 5 and Table 2).
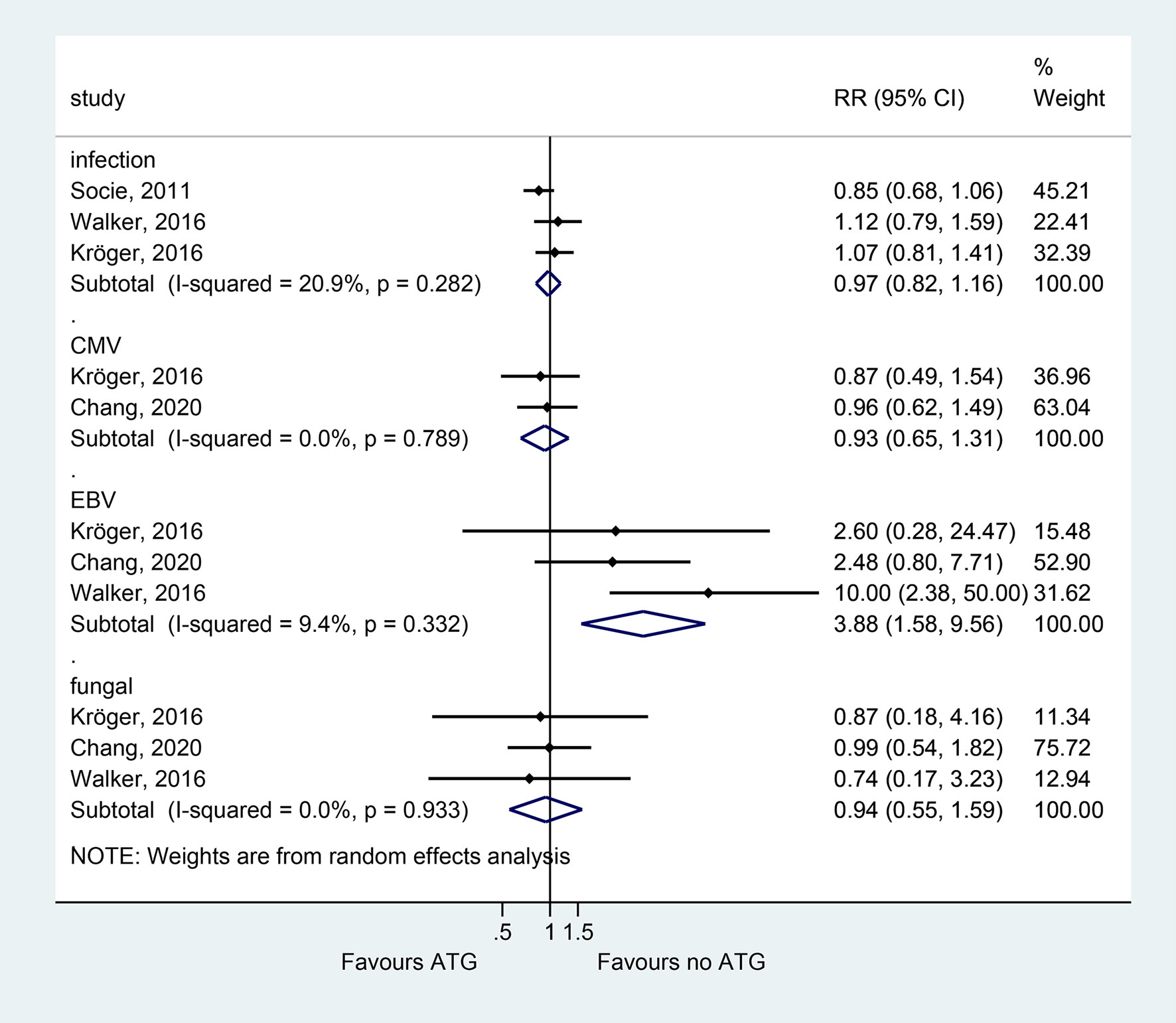
Figure 5 Forest plot for infection complications.
This meta-analysis showed that the addition of ATG to GVHD prophylaxis in patients undergoing allo-HSCT resulted in a significantly lower risk of grade III–IV aGVHD and cGVHD and improved the GRFS of patients and subsequent freedom from immunosuppressants. Moreover, ATG treatment was correlated with a high incidence of EBV reactivation. No significant differences were noted regarding disease relapse and patients’ survival, including OS, RFS, and NRM.
In this study, some results were consistent with those of the meta-analysis by Kumar et al. (13), suggesting that ATG reduced grade II/III and grade III/IV aGVHD and cGVHD without affecting the OS and NRM. Still, the previous study showed an increased risk of relapse following the use of ATG, contradicting the present study results. The present updated meta-analysis included RCTs with extended follow-up, and further additional long-term survival benefits of better GRFS, improved OS, and decreased use of immunosuppressive therapy were revealed for GVHD prophylaxis with ATG (16, 17). Interestingly, a short immunosuppressive treatment regimen might reduce the hazards associated with long-term immunosuppression without increasing the disease relapse and infections. The significantly improved probability of survival without disease relapse and cGVHD might prove the long-term efficacy of the ATG plus standard conditioning regimen after allogeneic stem cell transplantation.
We also performed subgroup analyses according to the source of donors and the formulations of ATG to explore their impact on major transplantation outcomes. Although the overall analysis did not reveal any difference, subgroup analyses substantially altered some outcomes. The factors that could affect the transplantation outcomes included disease status at transplantation, different doses of ATG, and the types of donors and grafts; all those factors varied among the included studies. The pooled analyses of four RCTs suggested that ATLG plus GVHD prophylaxis significantly reduced the risk of disease relapse, whereas the addition of ATG significantly improved NRM based on one study. Thus, the type of ATG might be a related factor for relapse and NRM, but additional studies are necessary to confirm these results. In addition, RFS was significantly improved in patients undergoing transplantation from unrelated donors, suggesting that the type of donor also played a role in survival benefit. The overall analysis revealed that ATG treatment significantly decreased grade III/IV aGVHD. Still, the unrelated subgroup did not show a decreased risk of severe aGVHD. For the OS and cGVHD outcomes, the type of donor and ATG did not affect the overall conclusions.
The present study demonstrated that the reduced risk of severe aGVHD and aGVHD was not accompanied by improved relapse, OS, and NRM, which might be explained by other significant complications following prophylactic treatment. The systemic immunosuppressive conditioning regimens plus ATG might delay immune reconstitution and thus increase the risk of infectious complications. Thus, EBV was associated with the post-transplantation lymphoproliferative disorder (28, 29). Our pooled analysis showed that ATG increased subsequent EBV reactivation, while the incidence of general infection complications, CMV reactivation, and fungal infection did not change significantly. Previous reports had conflicting conclusions about whether ATG increased the incidence of infection. The meta-analysis by Yuan et al. found that the risk of infections was similar in the ATG and non-ATG groups and suggested that the anti-pathogenic immune defense was not completely compromised after inhibiting the T-cell pool (14).
Both dosage and timing of ATG have been shown to correlate with the outcomes after HSCT. We conducted a meta-regression analysis based on ATG cumulative dosage. The cumulative dose of ATG was not associated with post-HSCT OS, aGVHD, cGVHD, relapse, RFS, and NRM. Herein, we observed heterogeneity among the included studies. Therefore, subgroup analysis was carried out to identify the source, and the findings revealed that the heterogeneity in cGVHD was significantly decreased in the unrelated and ATLG subgroups, while for OS, the heterogeneity was significantly reduced in the related and ATG subgroups. Therefore, the ATG sources and patients’ correlation with donors could be deemed putative sources of heterogeneity.
The present meta-analysis also had limitations. The included studies were highly heterogeneous, which might be caused by different diseases, donor sources, formulations, and doses of drugs. Thus, meta-regression and subgroup analyses were performed to discuss the effect of heterogeneity on these results. In addition, only the RR could be extracted from some studies, not the HR, which might affect the accuracy of the results. Furthermore, the sample size of the included studies was relatively small, especially for the analysis of the outcome of GRFS and free of immunosuppressant therapy. Finally, the forest plots for GVHD, OS, and relapse took into consideration all eight papers, while all the other outcome parameters considered only one to six studies, limiting the conclusions. Thus, large-scale RCTs are required in the future to validate our findings.
In conclusion, adding ATG to GVHD prophylaxis prevents severe aGVHD and cGVHD, improves long-term survival endpoint GRFS, and reduces the use of immunosuppressive therapy without impact on disease relapse and patient survival. Moreover, ATG treatment increases the EBV reactivation, but it can be clinically non-significant. Thus, large sample studies are necessary to confirm these findings and to compare ATG and ATLG.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
XY carried out the studies, participated in collecting data, and drafted the manuscript. DL performed the statistical analysis and participated in its design. YX participated in the acquisition, analysis, or interpretation of data and drafted the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the Fund of Science and Technology of Sichuan Province (No. 2020YFS0253).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank all study participants who were enrolled in this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.717678/full#supplementary-material
Supplementary Figure 1 | Flow diagram of the study selection.
Supplementary Figure 2 | Meta-regression plots for III–IV acute GVHD (A), chronic GVHD (B), OS (C), incidence of relapse (D), and NRM (E).
1. Sureda A, Bader P, Cesaro S, Dreger P, Duarte RF, Dufour C, et al. Indications for Allo- and Auto-SCT for Haematological Diseases, Solid Tumours and Immune Disorders: Current Practice in Europe, 2015. Bone Marrow Transplant (2015) 50:1037–56. doi: 10.1038/bmt.2015.6
2. Passweg JR, Baldomero H, Chabannon C, Basak GW, de la Camara R, Corbacioglu S, et al. Hematopoietic Cell Transplantation and Cellular Therapy Survey of the EBMT: Monitoring of Activities and Trends Over 30 Years. Bone Marrow Transplant (2021). doi: 10.1038/s41409-021-01227-8
3. Ziakas PD, Zervou FN, Zacharioudakis IM, Mylonakis E. Graft-Versus-Host Disease Prophylaxis After Transplantation: A Network Meta-Analysis. PloS One (2014) 9:e114735. doi: 10.1371/journal.pone.0114735
4. Zeiser R. Advances in Understanding the Pathogenesis of Graft-Versus-Host Disease. Br J Haematol (2019) 187:563–72. doi: 10.1111/bjh.16190
5. Maffini E, Festuccia M, Brunello L, Boccadoro M, Giaccone L, Bruno B. Neurologic Complications After Allogeneic Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant (2017) 23:388–97. doi: 10.1016/j.bbmt.2016.12.632
6. Sahin U, Toprak SK, Atilla PA, Atilla E, Demirer T. An Overview of Infectious Complications After Allogeneic Hematopoietic Stem Cell Transplantation. J Infection Chemotherapy Off J Japan Soc Chemotherapy (2016) 22:505–14. doi: 10.1016/j.jiac.2016.05.006
7. Greinix HT, Eikema DJ, Koster L, Penack O, Yakoub-Agha I, Montoto S, et al. Improved Outcome of Patients With Graft-Versus-Host Disease After Allogeneic Hematopoietic Cell Transplantation for Hematologic Malignancies Over Time: An EBMT Mega-File Study. Haematologica (2021). doi: 10.3324/haematol.2020.265769
8. Gagelmann N, Ayuk F, Wolschke C, Kröger N. Comparison of Different Rabbit Anti-Thymocyte Globulin Formulations in Allogeneic Stem Cell Transplantation: Systematic Literature Review and Network Meta-Analysis. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant (2017) 23:2184–91. doi: 10.1016/j.bbmt.2017.08.027
9. Bonifazi F, Rubio MT, Bacigalupo A, Boelens JJ, Finke J, Greinix H, et al. Rabbit ATG/ATLG in Preventing Graft-Versus-Host Disease After Allogeneic Stem Cell Transplantation: Consensus-Based Recommendations by an International Expert Panel. Bone Marrow Transplant (2020) 55:1093–102. doi: 10.1038/s41409-020-0792-x
10. Chang YJ, Wu DP, Lai YR, Liu QF, Sun YQ, Hu J, et al. Antithymocyte Globulin for Matched Sibling Donor Transplantation in Patients With Hematologic Malignancies: A Multicenter, Open-Label, Randomized Controlled Study. J Clin Oncol Off J Am Soc Clin Oncol (2020) 38:3367–76. doi: 10.1200/jco.20.00150
11. Soiffer RJ, Kim HT, McGuirk J, Horwitz ME, Johnston L, Patnaik MM, et al. Prospective, Randomized, Double-Blind, Phase III Clinical Trial of Anti-T-Lymphocyte Globulin to Assess Impact on Chronic Graft-Versus-Host Disease-Free Survival in Patients Undergoing HLA-Matched Unrelated Myeloablative Hematopoietic Cell Transplantation. J Clin Oncol Off J Am Soc Clin Oncol (2017) 35:4003–11. doi: 10.1200/jco.2017.75.8177
12. Kröger N, Solano C, Wolschke C, Bandini G, Patriarca F, Pini M, et al. Antilymphocyte Globulin for Prevention of Chronic Graft-Versus-Host Disease. New Engl J Med (2016) 374:43–53. doi: 10.1056/NEJMoa1506002
13. Kumar A, Reljic T, Hamadani M, Mohty M, Kharfan-Dabaja MA. Antithymocyte Globulin for Graft-Versus-Host Disease Prophylaxis: An Updated Systematic Review and Meta-Analysis. Bone Marrow Transplant (2019) 54:1094–106. doi: 10.1038/s41409-018-0393-0
14. Yuan J, Pei R, Su W, Cao J, Lu Y. Meta-Analysis of the Actions of Antithymocyte Globulin in Patients Undergoing Allogeneic Hematopoietic Cell Transplantation. Oncotarget (2017) 8:10871–82. doi: 10.18632/oncotarget.14719
15. Sheng Z, Ma H, Pang W, Niu S, Xu J. In Vivo T-Cell Depletion With Antithymocyte Globulins Improves Overall Survival After Myeloablative Allogeneic Stem Cell Transplantation in Patients With Hematologic Disorders. Acta haematologica (2013) 129:146–53. doi: 10.1159/000343604
16. Walker I, Panzarella T, Couban S, Couture F, Devins G, Elemary M, et al. Addition of Anti-Thymocyte Globulin to Standard Graft-Versus-Host Disease Prophylaxis Versus Standard Treatment Alone in Patients With Haematological Malignancies Undergoing Transplantation From Unrelated Donors: Final Analysis of a Randomised, Open-Label, Multicentre, Phase 3 Trial. Lancet Haematol (2020) 7:e100–e11. doi: 10.1016/s2352-3026(19)30220-0
17. Bonifazi F, Solano C, Wolschke C, Sessa M, Patriarca F, Zallio F, et al. Acute GVHD Prophylaxis Plus ATLG After Myeloablative Allogeneic Haemopoietic Peripheral Blood Stem-Cell Transplantation From HLA-Identical Siblings in Patients With Acute Myeloid Leukaemia in Remission: Final Results of Quality of Life and Long-Term Outcome Analysis of a Phase 3 Randomised Study. Lancet Haematol (2019) 6:e89–99. doi: 10.1016/s2352-3026(18)30214-x
18. Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ (Clinical Res ed) (2015) 350:g7647. doi: 10.1136/bmj.g7647
19. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring Inconsistency in Meta-Analyses. BMJ (Clinical Res ed) (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
20. Waikittipong S. Mitral Valve Repair for Rheumatic Mitral Regurgitation: Mid-Term Results. Asian Cardiovasc Thoracic Ann (2015) 23:658–64. doi: 10.1177/0218492315576282
21. Bacigalupo A, Lamparelli T, Bruzzi P, Guidi S, Alessandrino PE, di Bartolomeo P, et al. Antithymocyte Globulin for Graft-Versus-Host Disease Prophylaxis in Transplants From Unrelated Donors: 2 Randomized Studies From Gruppo Italiano Trapianti Midollo Osseo (GITMO). Blood (2001) 98:2942–7. doi: 10.1182/blood.v98.10.2942
22. Bacigalupo A, Lamparelli T, Barisione G, Bruzzi P, Guidi S, Alessandrino PE, et al. Thymoglobulin Prevents Chronic Graft-Versus-Host Disease, Chronic Lung Dysfunction, and Late Transplant-Related Mortality: Long-Term Follow-Up of a Randomized Trial in Patients Undergoing Unrelated Donor Transplantation. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant (2006) 12:560–5. doi: 10.1016/j.bbmt.2005.12.034
23. Bacigalupo A, Lamparelli T, Milone G, Sormani MP, Ciceri F, Peccatori J, et al. Pre-Emptive Treatment of Acute GVHD: A Randomized Multicenter Trial of Rabbit Anti-Thymocyte Globulin, Given on Day+7 After Alternative Donor Transplants. Bone Marrow Transplant (2010) 45:385–91. doi: 10.1038/bmt.2009.151
24. Finke J, Bethge WA, Schmoor C, Ottinger HD, Stelljes M, Zander AR, et al. Standard Graft-Versus-Host Disease Prophylaxis With or Without Anti-T-Cell Globulin in Haematopoietic Cell Transplantation From Matched Unrelated Donors: A Randomised, Open-Label, Multicentre Phase 3 Trial. Lancet Oncol (2009) 10:855–64. doi: 10.1016/s1470-2045(09)70225-6
25. Finke J, Schmoor C, Bethge WA, Ottinger H, Stelljes M, Volin L, et al. Long-Term Outcomes After Standard Graft-Versus-Host Disease Prophylaxis With or Without Anti-Human-T-Lymphocyte Immunoglobulin in Haemopoietic Cell Transplantation From Matched Unrelated Donors: Final Results of a Randomised Controlled Trial. Lancet Haematol (2017) 4:e293–301. doi: 10.1016/s2352-3026(17)30081-9
26. Socié G, Schmoor C, Bethge WA, Ottinger HD, Stelljes M, Zander AR, et al. Chronic Graft-Versus-Host Disease: Long-Term Results From a Randomized Trial on Graft-Versus-Host Disease Prophylaxis With or Without Anti-T-Cell Globulin ATG-Fresenius. Blood (2011) 117:6375–82. doi: 10.1182/blood-2011-01-329821
27. Walker I, Panzarella T, Couban S, Couture F, Devins G, Elemary M, et al. Pretreatment With Anti-Thymocyte Globulin Versus No Anti-Thymocyte Globulin in Patients With Haematological Malignancies Undergoing Haemopoietic Cell Transplantation From Unrelated Donors: A Randomised, Controlled, Open-Label, Phase 3, Multicentre Trial. Lancet Oncol (2016) 17:164–73. doi: 10.1016/s1470-2045(15)00462-3
28. Liu L, Zhang X, Feng S. Epstein-Barr Virus-Related Post-Transplantation Lymphoproliferative Disorders After Allogeneic Hematopoietic Stem Cell Transplantation. Biol Blood Marrow Transplant J Am Soc Blood Marrow Transplant (2018) 24:1341–9. doi: 10.1016/j.bbmt.2018.02.026
Keywords: anti-thymocyte globulin, hematological malignancies, allogeneic hematopoietic stem cell transplantation, overall survival, meta-analysis
Citation: Yang X, Li D and Xie Y (2021) Anti-Thymocyte Globulin Prophylaxis in Patients With Hematological Malignancies Undergoing Allogeneic Hematopoietic Stem Cell Transplantation: An Updated Meta-Analysis. Front. Oncol. 11:717678. doi: 10.3389/fonc.2021.717678
Received: 31 May 2021; Accepted: 29 July 2021;
Published: 20 August 2021.
Edited by:
Michele Malagola, University of Brescia, ItalyReviewed by:
Raffaella Greco, San Raffaele Hospital (IRCCS), ItalyCopyright © 2021 Yang, Li and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yao Xie, eGlleWFvMTI2MkBzaW5hLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.