
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 27 October 2021
Sec. Gastrointestinal Cancers
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.712053
 Alessandro Parisi1,2*
Alessandro Parisi1,2* Alessio Cortellini3,4
Alessio Cortellini3,4 Olga Venditti1
Olga Venditti1 Roberto Filippi5,6,7Lisa Salvatore8,9Giampaolo Tortora8,9
Roberto Filippi5,6,7Lisa Salvatore8,9Giampaolo Tortora8,9 Michele Ghidini10Olga Nigro11Fabio Gelsomino12
Michele Ghidini10Olga Nigro11Fabio Gelsomino12 Ina Valeria Zurlo13
Ina Valeria Zurlo13 Claudia Fulgenzi14
Claudia Fulgenzi14 Pasquale Lombardi6Susana Roselló Keränen15,16Ilaria Depetris17
Pasquale Lombardi6Susana Roselló Keränen15,16Ilaria Depetris17 Riccardo Giampieri18
Riccardo Giampieri18 Cristina Morelli19Pietro Di Marino20,21
Cristina Morelli19Pietro Di Marino20,21 Francesca Romana Di Pietro22
Francesca Romana Di Pietro22 Nicoletta Zanaletti23Pasquale Vitale24
Nicoletta Zanaletti23Pasquale Vitale24 Ingrid Garajova25
Ingrid Garajova25 Gian Paolo Spinelli26Federica Zoratto27
Gian Paolo Spinelli26Federica Zoratto27 Michela Roberto28
Michela Roberto28 Angelica Petrillo29Giacomo Aimar5,6Leonardo Patruno1,3
Angelica Petrillo29Giacomo Aimar5,6Leonardo Patruno1,3 Carla D’Orazio1,3Corrado Ficorella1,3Claudio Ferri2Giampiero Porzio1,3
Carla D’Orazio1,3Corrado Ficorella1,3Claudio Ferri2Giampiero Porzio1,3Background: Few data regarding post-induction management following first-line anti-epidermal growth factor receptor (EGFR)-based doublet regimens in patients with left-sided RAS/BRAF wild-type metastatic colorectal cancer (mCRC) are available.
Methods: This multicenter, retrospective study aimed at evaluating clinicians’ attitude, and the safety and effectiveness of post-induction strategies in consecutive patients affected by left-sided RAS/BRAF wild-type mCRC treated with doublet chemotherapy plus anti-EGFR as first-line regimen, who did not experience disease progression within 6 months from induction initiation, at 21 Italian and 1 Spanish Institutions. The measured clinical outcomes were: progression-free survival (PFS), overall survival (OS), adverse events, and objective response rate (ORR).
Results: At the data cutoff, among 686 consecutive patients with left-sided RAS/BRAF wild-type mCRC treated with doublet plus anti-EGFR as first-line regimen from March 2012 to October 2020, 355 eligible patients have been included in the present analysis. Among these, 118 (33.2%), 66 (18.6%), and 11 (3.1%) received a maintenance with 5-fluorouracil/leucovorin (5FU/LV)+anti-EGFR, anti-EGFR, and 5FU/LV, respectively, while 160 (45.1%) patients continued induction treatment (non-maintenance) until disease progression, unacceptable toxicity, patient decision, or completion of planned treatment. The median period of follow-up for the overall population was 33.7 months (95%CI = 28.9–35.6). The median PFS values of the 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance cohorts were 16.0 (95%CI = 14.3–17.7, 86 events), 13.0 (95%CI = 11.4–14.5, 56 events), 14.0 (95%CI = 8.1–20.0, 8 events), and 10.1 months (95%CI = 9.0–11.2, 136 events), respectively (p < 0.001). The median OS values were 39.6 (95%CI = 31.5–47.7, 43 events), 36.1 (95%CI = 31.6–40.7, 36 events), 39.5 (95%CI = 28.2–50.8, 4 events), and 25.1 months (95%CI = 22.6–27.6, 99 events), respectively (p < 0.001). After adjusting for key covariates, a statistically significant improvement in PFS in favor of 5FU/LV+anti-EGFR (HR = 0.59, 95%CI = 0.44–0.77, p < 0.001) and anti-EGFR (HR = 0.71, 95%CI = 0.51–0.98, p = 0.039) compared to the non-maintenance cohort was found. Compared to the non-maintenance cohort, OS was improved by 5FU/LV+anti-EGFR (HR = 0.55, 95%CI = 0.38–0.81, p = 0.002) and, with marginal significance, by anti-EGFR (HR = 0.67, 95%CI = 0.51–0.98, p = 0.051). No difference was found in ORR. Any grade non-hematological and hematological events were generally higher in the non-maintenance compared to the maintenance cohorts.
Conclusion: Among the treatment strategies following an anti-EGFR-based doublet first-line induction regimen in patients affected by left-sided RAS/BRAF wild-type mCRC treated in a “real-life” setting, 5FU/LV+anti-EGFR resulted the most adopted, effective, and relatively safe regimen.
The introduction of biological agents and the development of continuum of care strategies profoundly changed the treatment landscape for patients with unresectable metastatic colorectal cancer (mCRC). As the maximum benefit is achieved during the first-line treatment, strategies to consolidate the obtained response, maintaining the disease control while keeping a good safety profile, are essential. This applies even more with oxaliplatin-based regimens, as peripheral neuropathy could strongly worsen the long-term quality of life of patients (1). The landmark randomized, phase 3 OPTIMOX1 study found no difference in progression-free survival (PFS), overall survival (OS), and objective response rate (ORR) between a maintenance strategy with fluorouracil/leucovorin (5FU/LV) and full chemotherapy continuation after six induction cycles of 5FU/LV and oxaliplatin (FOLFOX). The better safety profile of the de-escalated arm, including a lower incidence of grade 3–4 cumulative peripheral sensory neuropathy, led to a progressive change in clinical practice by adopting maintenance strategies with 5FU/LV in association with a targeted agent (1).
Multiple phase 3 studies have investigated the role of maintenance anti-vascular endothelial growth factor (VEGF) blockade with bevacizumab/fluoropyrimidine following induction chemotherapy in the first-line setting, with variable benefits in terms of PFS and a good safety profile compared to no de-escalation and treatment holidays (2–5). According to these results and current guidelines, bevacizumab plus a fluoropyrimidine is regarded as the optimal maintenance regimen after a 4- to 6-month induction treatment with bevacizumab plus doublet or triplet regimens (6).
An anti-epidermal growth factor receptor (EGFR) agent (i.e., cetuximab or panitumumab) added to doublet chemotherapy is currently recommended as the first-line treatment option, particularly in left-sided RAS/BRAF wild-type mCRC (6–8). However, only few phase 2 studies investigating the role of maintenance (9–12) or intermittent (13, 14) strategies following anti-EGFR-based induction are available. The aim of this study was to retrospectively assess clinicians’ attitude and the safety and effectiveness of anti-EGFR post-induction strategies in a “real-life” population of patients affected by unresectable left-sided RAS/BRAF wild-type mCRC.
This retrospective analysis evaluated consecutive unresectable RAS and BRAF wild-type left-sided mCRC patients treated with first-line doublet chemotherapy plus an anti-EGFR agent outside of a clinical trial setting at 21 Italian and 1 Spanish institutions (Supplementary File 1) from March 2012 to October 2020.
The eligibility criteria were: age ≥18 years; histologically confirmed diagnosis of CRC originating from the splenic flexure, descending colon, sigma, and rectum; confirmed KRAS (exons 2–4), NRAS (exons 2–4), and BRAF (V600E) wild-type genotype; and having received a first-line treatment with an anti-EGFR-based doublet [FOLFOX or irinotecan/5-fluorouracil/leucovorin (FOLFIRI)]. The exclusion criteria were: surgery after an induction treatment; early (within 4 months) discontinuation of the induction due to death, toxicity, or patient’s decision; induction treatment ongoing (defined as less than 4 months treatment completed) at the time of data cutoff analysis; or fast progressors (i.e., patients who experienced disease progression within 6 months from the beginning of the induction treatment). The CONSORT flow diagram with patient selection is presented in Figure 1.
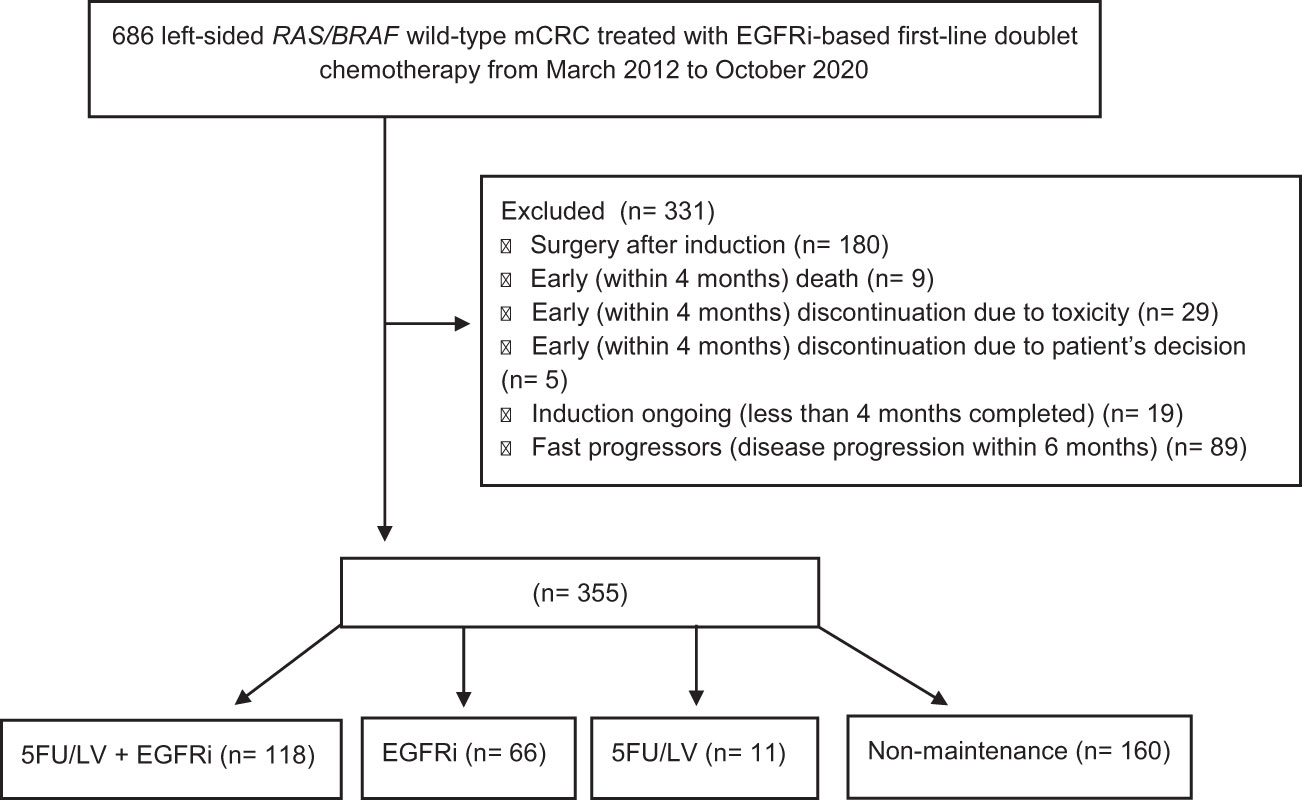
Figure 1 CONSORT flowchart of patient selection and disposition.
All patients alive at the time of data collection provided informed consent to participate in this retrospective, observational, non-interventional study. The procedures followed were in accordance with the precepts of Good Clinical Practice and the Declaration of Helsinki. The study was approved by the respective local ethical committees on human experimentation of each institution, after previous approval by the coordinating center (Comitato Etico delle Province di L’Aquila e Teramo, protocol no, 21, approved on July 16, 2020).
The measured effectiveness, safety, and antitumor activity clinical outcomes were PFS, OS, ORR, and treatment-related adverse events (AEs). Disease responses were evaluated with the RECIST (Response Evaluation Criteria in Solid Tumors) (version 1.1) (15). Only patients with measurable disease at the time of first radiological assessment were included in the activity analysis. ORR was defined as the portion of patients experiencing an objective response (complete response or partial response) as best response. PFS was defined as the length of time from the beginning of first-line treatment to disease progression or death from any cause; OS, as the length of time between the beginning of first-line treatment to death from any cause. Data cutoff period was October 2020. For the study purpose, we grouped patients according to the type of maintenance treatment, if received, regardless of the duration of the induction period: 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance (i.e., induction continuation). The baseline characteristics of patients were compared across the four cohorts.
Fixed regression models were used for the multivariable analyses of PFS and OS. Covariates were chosen with a clinical prioritization approach and on the basis of their availability (16–18). The chosen key covariates were: age (<70 vs. ≥70 years) (19), gender (male vs. female) (20), Eastern Cooperative Oncology Group—Performance Status (ECOG-PS) (0 vs. 1–2), number of metastatic sites (one vs. two or more), baseline alkaline phosphatase (ALP; normal vs. high), and white blood cell (WBC) count (normal vs. high) (21).
AEs experienced during induction and maintenance treatments were clustered as: hematological (leukopenia, anemia, and thrombocytopenia); non-hematological (nausea, vomiting, mucositis, hand–foot syndrome, asthenia, anorexia, and others); and anti-EGFR class-specific AEs (skin rash/acneiform dermatitis, paronychia/nail disorders, and others). Because of their clinical relevance, diarrhea, peripheral neuropathy, and neutropenia were evaluated individually. AEs were reported for the overall population, registered according to National Cancer Institute Common Terminology Criteria (NCI-CTC) for AEs (version 4 up to January 2018 and version 5 from January 2018), and grouped according to severity (G1–2 and G3–4). In the non-maintenance cohort, AEs have been collected throughout the entire duration of treatment.
Chi-square and Fisher’s exact tests, as appropriate, were used to compare the baseline characteristics of patients, reported with descriptive statistics, and treatment outcomes across the cohorts. Survival analysis employed the Kaplan–Meier method, in which patients without events were censored at the last follow-up available, and log-rank test for inter-cohort comparisons. The Cox proportional hazard model was used for the univariate and multivariate analyses and for calculating hazard ratios (HRs) with 95% confidence intervals (CIs). The median period of follow-up was calculated through the reverse Kaplan–Meier method. The threshold for statistical significance was set to p = 0.05. All statistical analyses were performed using IBM SPSS Statistics, version 26.0 (released 2019, IBM SPSS Statistics for Macintosh, version 26.0; IBM Corp., Armonk, NY, USA).
All the molecular analyses were performed according to the local clinical practice of the participating centers. KRAS, NRAS, and BRAF mutational status was assessed with Sanger sequencing, real-time PCR techniques, and next-generation sequencing (NGS) (such as OncoGenBasic-S1 kit, Seqplexing; Pyromark Q96 ID System, Qiagen; EasyPGX and Myriapod Colon Status, Diatech Pharmacogenetics; Idylla KRAS and NRAS-BRAF Mutation Test, Biocartis; and Ion AmpliSeq Colon and Lung Cancer Panel, Ion Torrent).
At the data cutoff, the clinical histories of 686 consecutive patients with left-sided RAS and BRAF wild-type mCRC treated with doublet plus anti-EGFR as first-line regimen were entered. After the exclusion of 331 patients, 355 eligible patients have been included in the present analysis (Figure 1). Among these, 118 (33.2%), 66 (18.6%), and 11 (3.1%) received a maintenance regimen with 5FU/LV+anti-EGFR, anti-EGFR, and 5FU/LV, respectively; meanwhile, 160 (45.1%) patients continued induction treatment (non-maintenance) until completion of 4–6 months of planned treatment (i.e., “stop-and-go” or intermittent approach), disease progression, unacceptable toxicity, or patient decision. Patients’ features are summarized in Table 1. The median age was 64 years (range = 29–84). A statistically significant difference was found between the four cohorts with respect to disease burden, as a higher number of metastatic sites was found in the 5FU/LV+anti-EGFR (52.5%), anti-EGFR (55.4%), and non-maintenance (60.3%) cohorts compared to that in the 5FU/LV (18.2%) cohort. Moreover, statistically significant differences were found with regard to the chemotherapy induction backbone and the anti-EGFR used. Within the non-maintenance cohort, 90 (56.2%) patients were treated up to disease progression, unacceptable toxicity, or drug holiday/patient decision. Among these, 31 (34.4%) and 51 (65.6%) patients were treated with FOLFOX or FOLFIRI, respectively, in association with panitumumab (39, 43.3%) or cetuximab (51, 56.7%). Within the non-maintenance cohort, 70 (43.7%) patients were treated with a “stop-and-go” strategy with FOLFOX (39, 55.7%) or FOLFIRI (31, 44.3%) in association with panitumumab (41, 58.6%) or cetuximab (29, 41.4%).
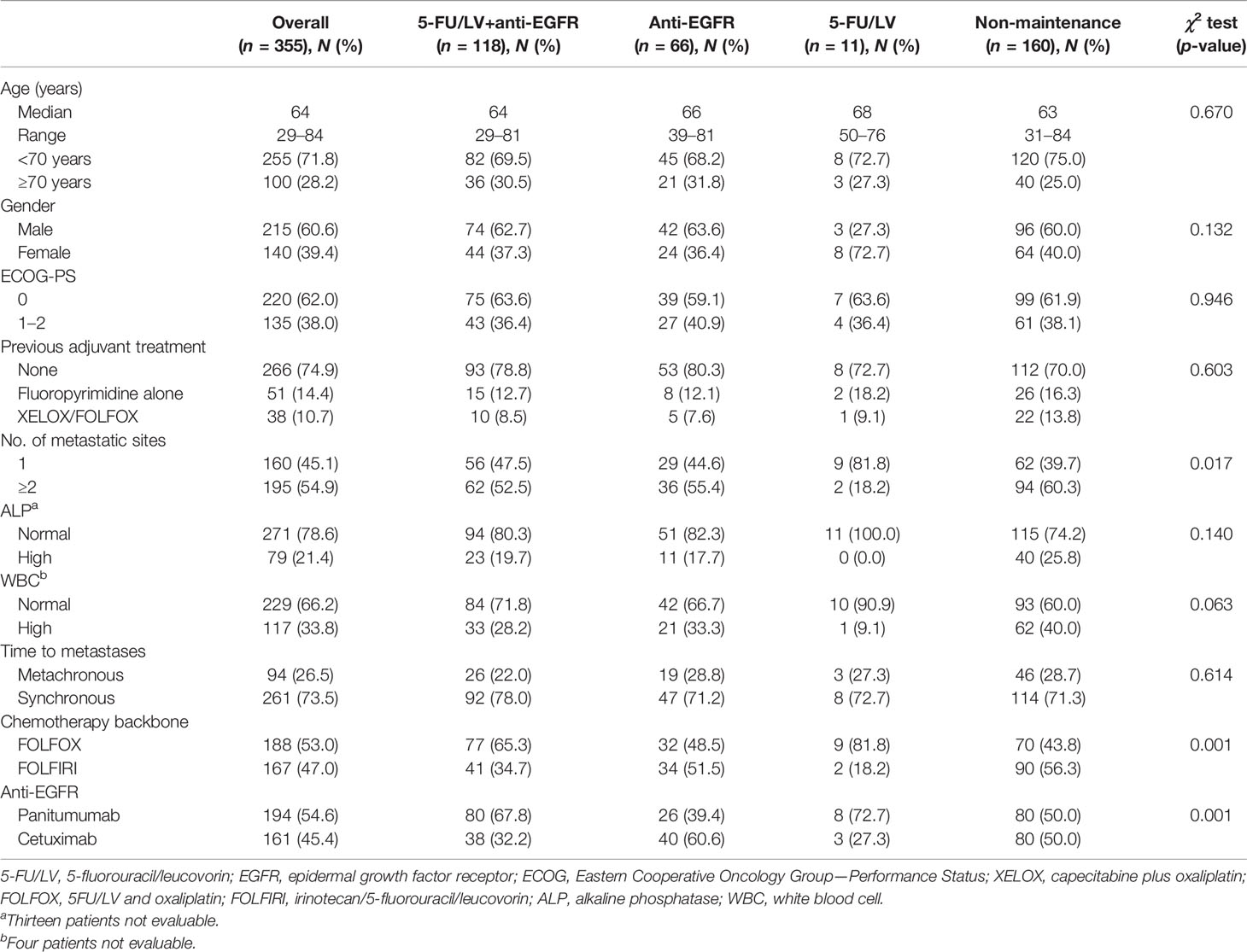
Table 1 Baseline demographic and disease characteristics.
The median period of follow-up for the overall population was 33.7 months (95%CI = 28.9–35.6), while those among the 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance cohorts were 26.4 (95%CI = 18.1–34.7), 42.0 (95%CI = 33.6–50.4), 30.0 (95%CI = 13.7–46.3), and 38.3 months (95%CI = 27.6–49.0), respectively.
The median PFS of the overall population was 12.6 months (95%CI = 11.8–13.4, 286 events), while the median PFS values of the 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance cohorts were 16.0 (95%CI = 14.3–17.7, 86 events), 13.0 (95%CI = 11.4–14.5, 56 events), 14.0 (95%CI = 8.1–20.0, 8 events), and 10.1 months (95%CI = 9.0–11.2, 136 events), respectively, with a statistically significant heterogeneity at the univariate analysis (p < 0.001). The median OS of the overall population was 32.3 months (95%CI = 27.7–36.7, 182 events), while median OS values of the 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance cohorts were 39.6 (95%CI = 31.5–47.7, 43 events), 36.1 (95%CI = 31.6–40.7, 36 events), 39.5 (95%CI = 28.2–50.8, 4 events), and 25.1 months (95%CI = 22.6–27.6, 99 events), respectively, with a statistically significant heterogeneity at the univariate analysis (p < 0.001) (Table 2 and Figure 2). After adjusting for the key covariates, a statistically significant improvement in PFS was found in the multivariate analysis in favor of 5FU/LV+anti-EGFR (HR = 0.59, 95%CI = 0.44–0.77, p < 0.001) and anti-EGFR (HR = 0.71, 95%CI = 0.51–0.98, p = 0.039) compared to the non-maintenance cohort. Moreover, a statistically significant improvement in OS was found at the multivariate analysis in favor of 5FU/LV+anti-EGFR (HR = 0.55, 95%CI = 0.38–0.81, p = 0.002), while a trend toward better OS was found for anti-EGFR (HR = 0.67, 95%CI = 0.51–0.98, p = 0.051) compared to the non-maintenance cohort (Table 3).
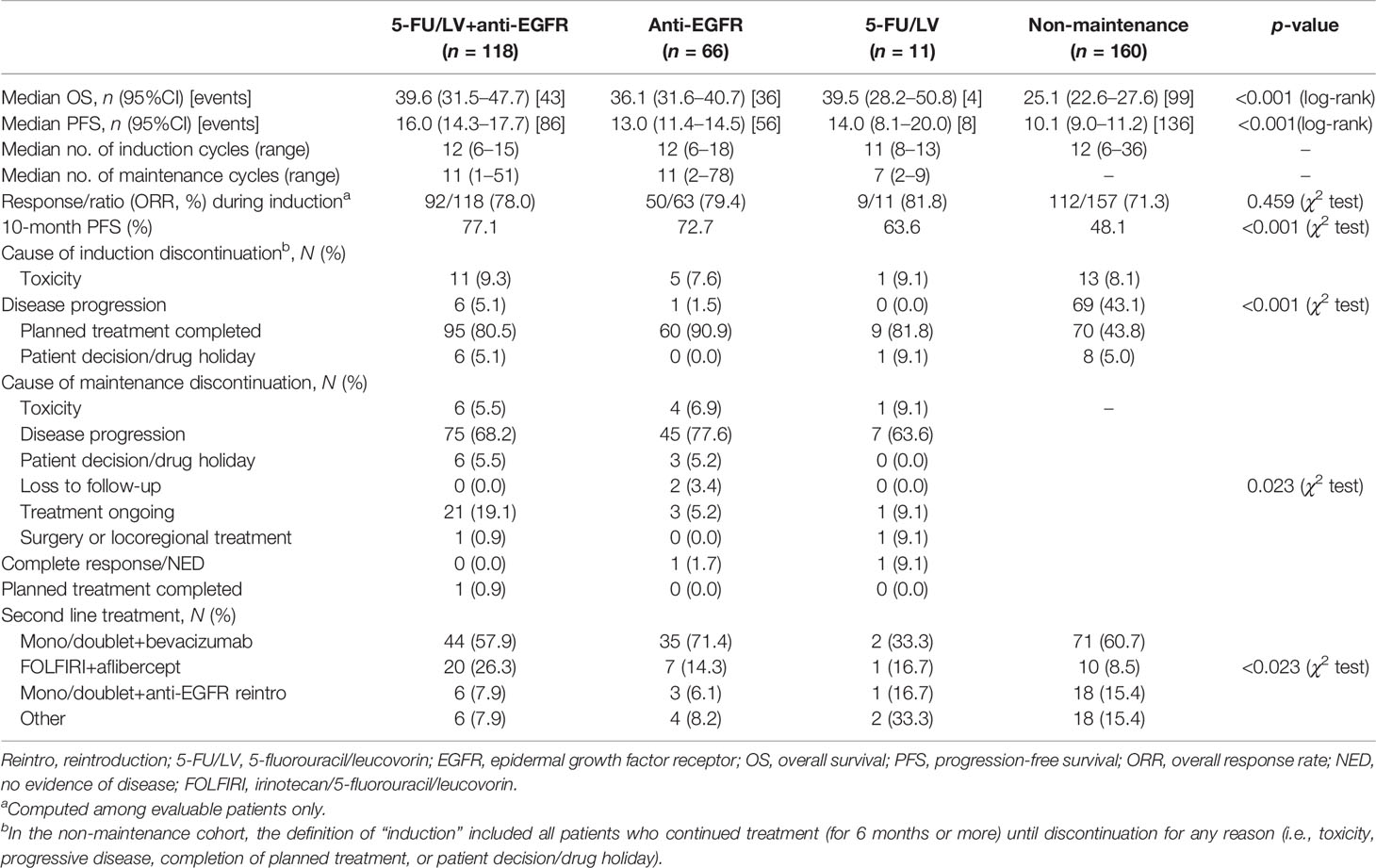
Table 2 Treatment outcomes during first-line treatment.
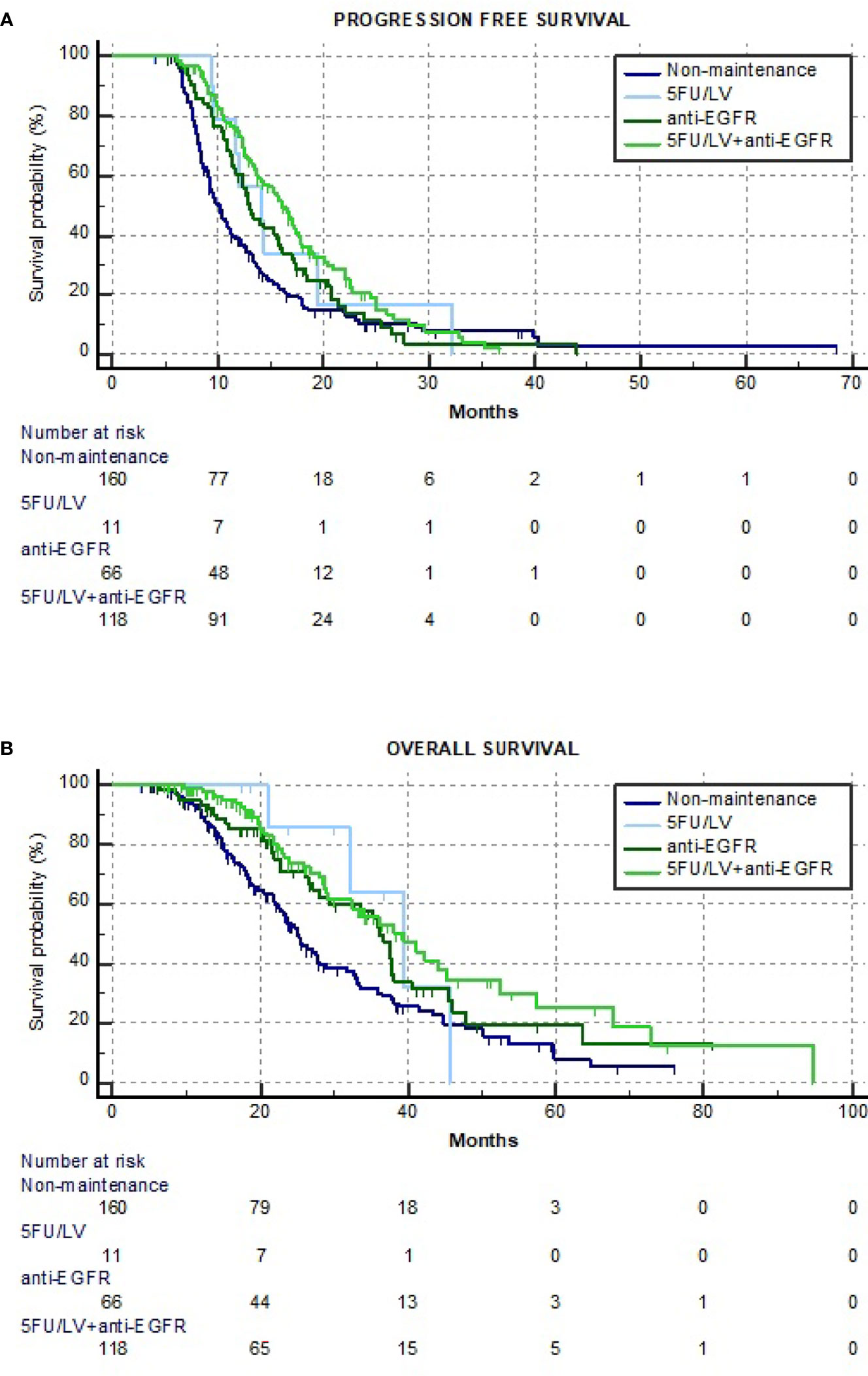
Figure 2 Kaplan–Meier estimate curves of progression-free survival (PFS) (A) and overall survival (OS) (B).
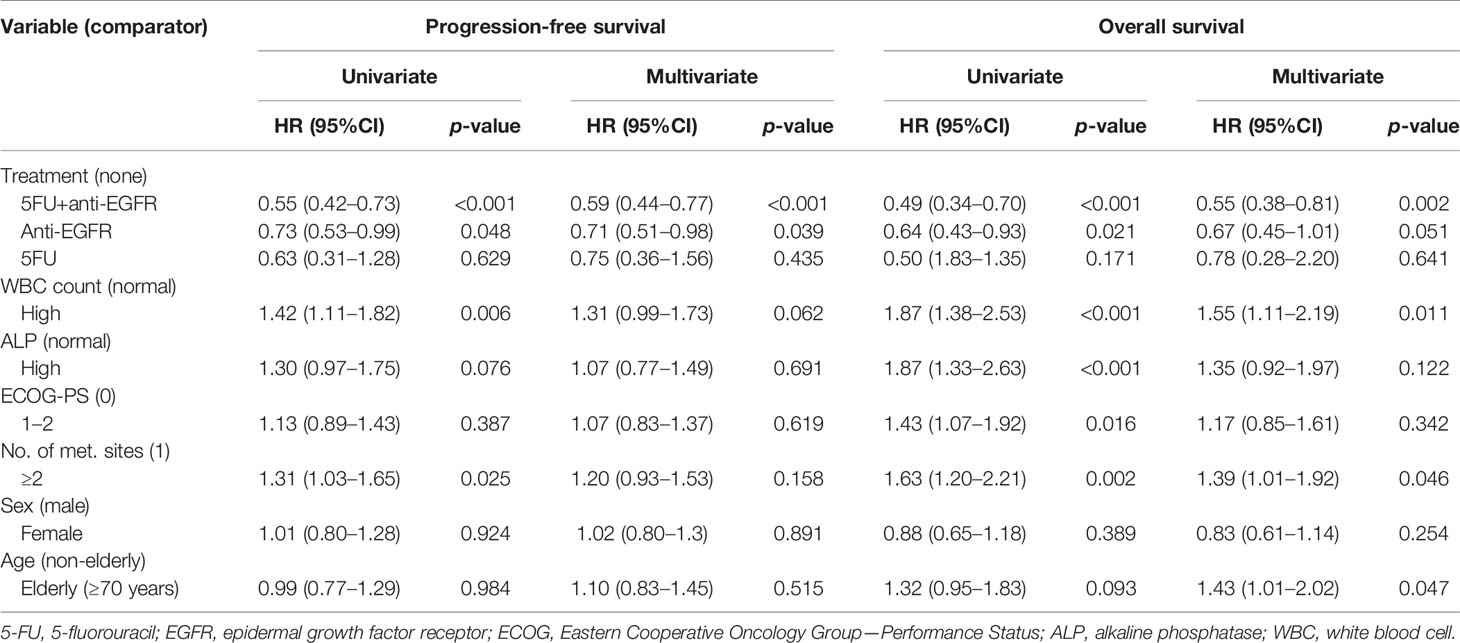
Table 3 Univariate and multivariate analyses for progression-free survival and overall survival.
The ORRs were 78% (95%CI = 69.9–84.7), 79.4% (95%CI = 68.2-87.9), 81.8% (95%CI = 53.3–96), and 71.3% (95%CI = 63.9–78.0) in the 5FU/LV+anti-EGFR, anti-EGFR, 5FU/LV, and non-maintenance (p = 0.459) cohorts, respectively (Table 2).
The toxicity profiles are summarized in Table 4. The AEs that occurred most commonly during maintenance treatment with 5FU/LV+anti-EGFR, anti-EGFR, and 5FU/LV were any grade non-hematological (24.6%, 9.1%, and 27.3%, respectively), hematological (22.9%, 7.6%, and 27.3%, respectively), neutropenia (20.3%, 7.6%, and 9.1%, respectively), skin rash (65.3%, 68.2%, and 9.1%, respectively), and paronychia/nail disorders (33.1%, 19.7%, and 0.0%, respectively). Among the G3–G4 AEs, diarrhea was more frequent in the 5FU/LV cohort (9.1%), while skin rash was more frequent in the 5FU/LV+anti-EGFR and anti-EGFR cohorts (8.5% and 9.1%, respectively). In general, the non-maintenance cohort had higher incidence rates of any grade non-hematological and hematological AEs, diarrhea, and neutropenia compared to those of the 5FU/LV+anti-EGFR and anti-EGFR cohorts.
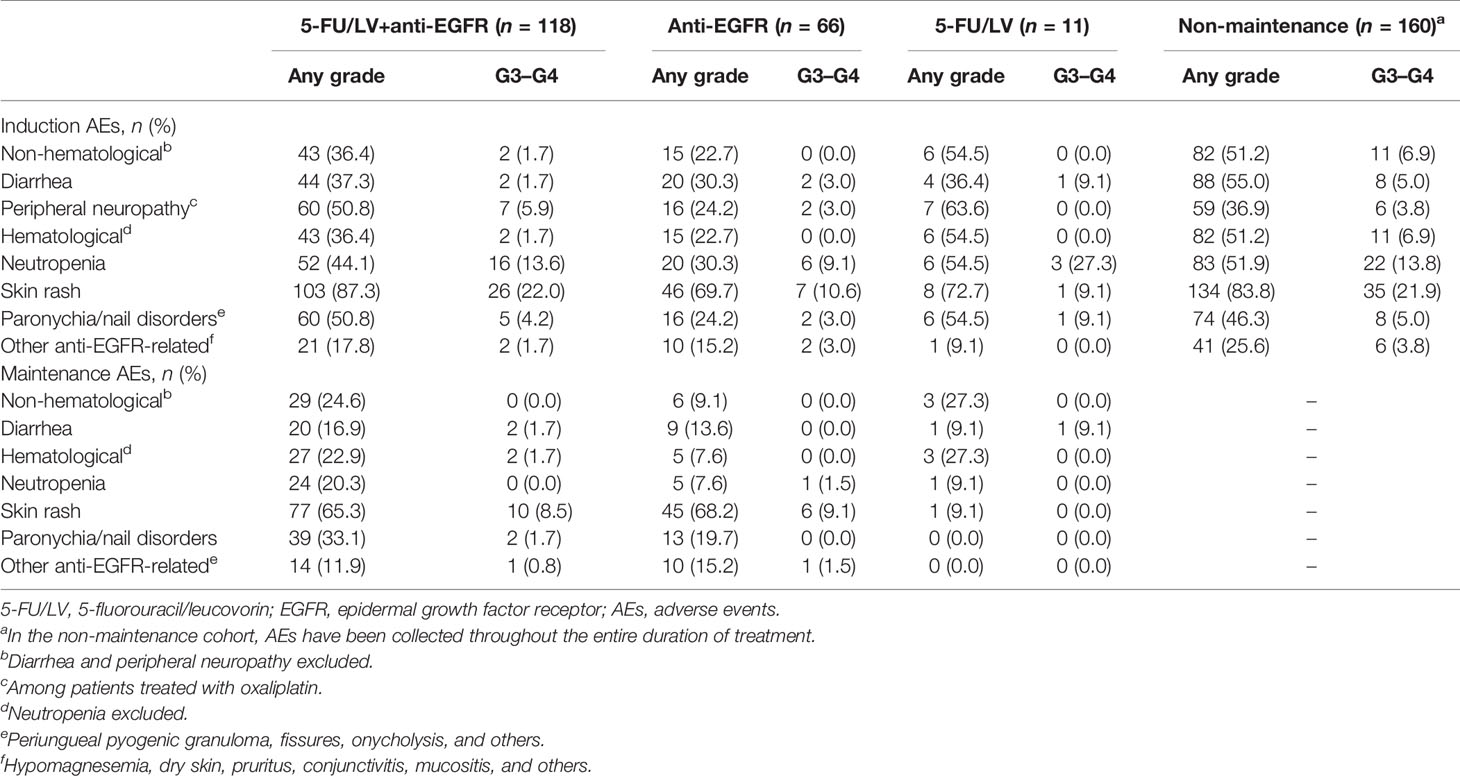
Table 4 Induction and maintenance of treatment-related adverse events (AEs).
Completion of the planned induction treatment was achieved by 80.5%, 90.9%, and 81.8% of patients in the 5FU/LV+anti-EGFR, anti-EGFR, and 5FU/LV cohorts, respectively. Among them, 68.2%, 77.6%, and 63.6%, respectively, discontinued the maintenance treatment due to disease progression. On the other hand, 43.1% and 43.8% of patients in the non-maintenance cohort discontinued the induction treatment due to disease progression and completion of planned treatment, respectively.
As expected, most of the patients underwent an antiangiogenic-containing second-line regimen with bevacizumab or aflibercept, while a lower rate of patients was treated with the anti-EGFR reintroduction in association with a mono- or doublet chemotherapy (Table 2).
Compared to bevacizumab-based strategies, anti-EGFR-based post-induction treatment options are less codified and no phase 3 data are available.
According to the results of phase 2 trials, anti-EGFR-based maintenance therapy is feasible in mCRC patients after oxaliplatin-based induction regimens.
The randomized, phase 2 MACRO-2 study compared continued treatment with FOLFOX–cetuximab vs. maintenance cetuximab after induction with eight cycles of FOLFOX–cetuximab in KRAS wild-type mCRC Western patients. No difference was found between the continued oxaliplatin and maintenance groups in terms of PFS (9.8 vs. 8.7 months, respectively), with reduced incidence of peripheral neuropathy (15% vs. 2%, respectively) and acneiform rash (24% vs. 15%, respectively) (11).
The randomized, phase 2 SAPPHIRE study compared continued treatment with FOLFOX+panitumumab vs. 5FU/LV+panitumumab after induction with six cycles of FOLFOX+panitumumab in RAS wild-type mCRC Eastern patients. The median PFS was comparable between the continued oxaliplatin group and the de-escalated group (9.1 and 9.3 months, respectively), with slightly improved outcomes in left-sided patients (10.5 vs. 11.5 months, respectively) and a reduced incidence of peripheral neuropathy (13.5% vs. 1.9%, respectively) (12).
In the non-comparative phase 2 COIN-B study, KRAS exon 2 wild-type mCRC patients were randomized to receive FOLFOX–cetuximab for 12 weeks followed by cetuximab maintenance vs. observation and reintroduced FOLFOX–cetuximab at disease progression. No difference was noted among the maintenance and intermittent strategies in 10-month failure-free survival (52% vs. 50%, respectively), even if a trend toward better post-induction PFS (5.8 vs. 3.1 months, respectively) and OS (22.2 vs. 16.8 months, respectively) was observed in favor of the maintenance treatment, particularly in the RAS wild-type population (13).
In the randomized phase 2 VALENTINO study, RAS wild-type mCRC patients were randomized to receive induction with FOLFOX–panitumumab for eight cycles, followed by either 5FU/LV+panitumumab or panitumumab alone as maintenance. A clinically relevant benefit in favor of 5FU/LV+panitumumab in terms of 10-month PFS (59% vs. 49%) and median PFS (12 vs. 9.9 months) was observed. As expected, a higher incidence of AEs, particularly diarrhea and stomatitis (42% vs. 20%), as well as of anti-EGFR-related AEs (76% vs. 42%), was found with 5FU/LV+panitumumab compared to that with panitumumab alone (9).
Drawing from this puzzling evidence, the present study retrospectively assessed the effectiveness and safety outcomes of the different post-induction strategies adopted in clinical practice in a selected population of patients with left-sided RAS and BRAF wild-type mCRC.
The first result to be discussed is the relatively low rate of patients undergoing a chemotherapy-only maintenance treatment, particularly with 5FU/LV alone, as compared to patients treated with 5FU/LV+anti-EGFR and anti-EGFR alone. This is in line with the scarce evidence previously discussed, as, to date, no evidence supports the use of 5FU/LV alone as maintenance after an anti-EGFR-based induction regimen. In this respect, in the randomized phase 2 PanaMa trial comparing 5FU/LV+panitumumab vs. 5FU/LV alone as maintenance strategies in RAS wild-type mCRC, the PFS of maintenance therapy was significantly improved with 5FU/LV+panitumumab (8.8 vs. 5.7 months), with a trend toward better OS (28.7 vs. 25.7 months) (10).
With the exception of a higher tumor burden and a more extensive use of FOLFIRI and cetuximab in the non-maintenance cohort compared to the maintenance cohorts, no significant differences were found regarding the baseline characteristics and prognostic factors, which were fairly balanced among the numerically larger cohorts (i.e., 5FU/LV+anti-EGFR, anti-EGFR, and non-maintenance). The higher tumor burden might have negatively affected the clinical histories and steered the clinicians’ choice toward not de-escalating the treatment. The median number of induction cycles was also balanced between the cohorts. These results are consistent with previously summarized literature data, as the maintenance (10–12) or intermittent (13, 14) strategies have been mainly investigated in patients treated with an oxaliplatin-based chemotherapy backbone following a 6- to 12-cycle (i.e., about 3–6 months) induction in order to reduce the incidence of peripheral neuropathy. The higher proportion of patients treated with a FOLFIRI chemotherapy backbone up to disease progression, unacceptable toxicity, or patient decision in the non-maintenance compared to the maintenance cohorts, together with the higher incidence of non-hematological and hematological AEs, including diarrhea and neutropenia, emphasized the issue of dealing with irinotecan-related cumulative toxicities and the need for comparative trials of post-induction management in this setting. In this respect, the results of the ongoing phase 2 IMPROVE trial (NCT04425239), aimed at comparing intermittent first-line FOLFIRI-panitumumab vs. the same regimen given continuously, and those of the ongoing randomized phase 3 ERMES trial (22), aimed at comparing FOLFIRI–cetuximab vs. maintenance cetuximab following FOLFIRI–cetuximab, both in a population of patients with unresectable RAS/BRAF wild-type mCRC, are awaited.
In our study, a clinically relevant and statistically significant benefit was observed for patients treated with 5FU/LV+anti-EGFR maintenance over the non-maintenance strategy, while maintenance treatment with anti-EGFR alone achieved less clear results. This differential advantage is confirmed by the progressive reduction in the relative risk of disease progression or death. This survival benefit was associated with a higher incidence of hematological and non-hematological AEs, other than paronychia/nail disorders, which usually occur after several weeks of treatment with anti-EGFR, particularly in association with fluoropyrimidines (23). These results are consistent with the existing literature, corroborating the hypothesis that patients gain more in terms of PFS and OS from a maintenance approach than from a “stop-and-go” strategy (13), with an even greater benefit for FU/LV+anti-EGFR compared to anti-EGFR alone, particularly in patients affected by left-sided RAS/BRAF wild-type mCRC, at the price of a slightly higher incidence of manageable toxic effects (9, 10).
As expected, the majority of patients with disease progression underwent an antiangiogenic-based second-line treatment, according to recommendations from national and international guidelines (24, 25) and retrospective experiences (26). The small number of patients who were reintroduced to an anti-EGFR-based regimen at disease progression, particularly in the non-maintenance cohort, limited further assessment of the value of a “stop-and-go” strategy, which might be effective in patients with rapid and deep tumor responses, with low tumor burden, especially, but not only, if converted to radical surgery following an anti-EGFR-containing first-line induction, or in those patients who experienced severe or disabling skin toxicity (27). In the PaNama trial, reinduction therapy was more active and effective in patients who had received FU/LV compared to those who received FU/LV+anti-EGFR (ORR = 34.7% vs. 8.9%, PFS = 6.3 vs. 3.8 months, respectively). On the other hand, preclinical and clinical evidence suggests a potential role of anti-EGFR reintroduction beyond the second-line, particularly in patients selected with liquid biopsy (28–31).
The retrospective nature of the study, with its inherent selection bias and not-on-purpose data collection, and the small sample size of the cohorts are some of the limitations that might have affected the results of this study. As mentioned, confounding by indication could have played a role in the observed inter-cohort differences. Although we may not draw definitive conclusions from our study, its interesting findings can be considered as preliminary and hypothesis-generating. Moreover, the study provided a snapshot of the real-life attitude of clinicians toward the post-induction strategy for patients with unresectable left-sided RAS/BRAF wild-type mCRC treated with anti-EGFR-based doublet first-line induction and contextualized it within the relative scantiness of literature data. In this respect, prospective observational studies, with more homogeneous inclusion criteria and patient characteristics, addressing the reasons leading to maintenance strategies in a real-life setting are certainly desirable.
The ideal maintenance strategy should preserve the obtained response over time by administering an appropriate less toxic regimen, preserving the quality of life of patients without compromising treatment efficacy. In our real-life cohort, maintenance with 5FU/LV+anti-EGFR seems to be the most widely adopted, as well as a safe and effective regimen in patients with unresectable left-sided RAS/BRAF wild-type mCRC treated with an anti-EGFR-based doublet first-line induction regimen. However, intermittent or continuous treatment strategies might still be options in a case-by-case evaluation based on both patient and disease characteristics and response and safety to induction treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comitato Etico delle Province di L’Aquila e Teramo. The patients/participants provided written informed consent to participate in this study.
All authors contributed to the publication according to the ICMJE guidelines for authorship. All authors read and approved the manuscript and agree to be accountable for all aspects of the research in ensuring that the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors contributed to the article and approved the submitted version.
AlP reported receiving advisory board fees from GSK. AC reported receiving consulting/advisory board fees from AstraZeneca, MSD, Roche, and BMS and speakers’ fee from Novartis, Astellas, MSD, and AstraZeneca. AnP reported receiving fees from Eli-Lilly, MSD, and Servier. RG reported receiving fees from Amgen and Servier and advisory board fees from Amgen, Servier, Bayer, and Merck-Serono.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.712053/full#supplementary-material
1. Tournigand C, Cervantes A, Figer A, Lledo G, Flesch M, Buyse M, et al. OPTIMOX1: A Randomized Study of FOLFOX4 or FOLFOX7 With Oxaliplatin in a Stop-and-Go Fashion in Advanced Colorectal Cancer—A GERCOR Study. J Clin Oncol (2006) 24(3):394–400. doi: 10.1200/JCO.2005.03.0106
2. Chibaudel B, Maindrault-Goebel F, Lledo G, Mineur L, André T, Bennamoun M, et al. Can Chemotherapy be Discontinued in Unresectable Metastatic Colorectal Cancer? The GERCOR OPTIMOX2 Study. J Clin Oncol (2009) 27(34):5727–33. doi: 10.1200/JCO.2009.23.4344
3. Hegewisch-Becker S, Graeven U, Lerchenm̈ller CA, Killing B, Depenbusch R, Steffens CC, et al. Maintenance Strategies After First-Line Oxaliplatin Plus Fluoropyrimidine Plus Bevacizumab for Patients With Metastatic Colorectal Cancer (AIO 0207): A Randomised, Non-Inferiority, Open-Label, Phase 3 Trial. Lancet Oncol (2015) 16(13):1355–69. doi: 10.1016/S1470-2045(15)00042-X
4. Koeberle D, Betticher DC, von Moos R, Dietrich D, Brauchli P, Baertschi D, et al. Bevacizumab Continuation Versus No Continuation After First-Line Chemotherapy Plus Bevacizumab in Patients With Metastatic Colorectal Cancer: A Randomized Phase III Non-Inferiority Trial (SAKK 41/06). Ann Oncol (2015) 26(4):709–14. doi: 10.1093/annonc/mdv011
5. Simkens LH, van Tinteren H, May A, ten Tije AJ, Creemers GJ, Loosveld OJ, et al. Maintenance Treatment With Capecitabine and Bevacizumab in Metastatic Colorectal Cancer (CAIRO3): A Phase 3 Randomised Controlled Trial of the Dutch Colorectal Cancer Group. Lancet (2015) 385(9980):1843–52. doi: 10.1016/S0140-6736(14)62004-3
6. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO Consensus Guidelines for the Management of Patients With Metastatic Colorectal Cancer. Ann Oncol (2016) 27(8):1386–422. doi: 10.1093/annonc/mdw235
7. Arnold D, Lueza B, Douillard JY, Peeters M, Lenz HJ, Venook A, et al. Prognostic and Predictive Value of Primary Tumour Side in Patients With RAS Wild-Type Metastatic Colorectal Cancer Treated With Chemotherapy and EGFR Directed Antibodies in Six Randomized Trials. Ann Oncol (2017) 28(8):1713–29. doi: 10.1093/annonc/mdx175
8. Parisi A, Porzio G, Cannita K, Venditti O, Avallone A, Filippi R, et al. Clinicians' Attitude to Doublet Plus Anti-EGFR Versus Triplet Plus Bevacizumab as First-Line Treatment in Left-Sided RAS and BRAF Wild-Type Metastatic Colorectal Cancer Patients: A Multicenter, "Real-Life", Case-Control Study. Clin Colorectal Cancer (2021) S1533-0028(21):00068–2. doi: 10.1016/j.clcc.2021.07.003. S1533-0028(21)00068-2.
9. Pietrantonio F, Morano F, Corallo S, Miceli R, Lonardi S, Raimondi A, et al. Maintenance Therapy With Panitumumab Alone vs Panitumumab Plus Fluorouracil-Leucovorin in Patients With RAS Wild-Type Metastatic Colorectal Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol (2019) 5(9):1268–75. doi: 10.1001/jamaoncol.2019.1467
10. Modest DP, Karthaus M, Fruehauf S, Graeven U, Müller L, König AO, et al. Panitumumab Plus Fluorouracil and Folinic Acid Versus Fluorouracil and Folinic Acid Alone as Maintenance Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Randomized PANAMA Trial (AIO KRK 0212). J Clin Oncol (2021), JCO2101332. doi: 10.1200/JCO.21.01332
11. Aranda E, García-Alfonso P, Benavides M, Sánchez Ruiz A, Guillén-Ponce C, Safont MJ, et al. Spanish Cooperative Group for the Treatment of Digestive Tumours (TTD). First-Line mFOLFOX Plus Cetuximab Followed by mFOLFOX Plus Cetuximab or Single-Agent Cetuximab as Maintenance Therapy in Patients With Metastatic Colorectal Cancer: Phase II Randomised MACRO2 TTD Study. Eur J Cancer (2018) 101:263–72. doi: 10.1016/j.ejca.2018.06.024
12. Munemoto Y, Nakamura M, Takahashi M, Kotaka M, Kuroda H, Kato T, et al. SAPPHIRE: A Randomised Phase II Study of Planned Discontinuation or Continuous Treatment of Oxaliplatin After Six Cycles of Modified FOLFOX6 Plus Panitumumab in Patients With Colorectal Cancer. Eur J Cancer (2019) 119:158–67. doi: 10.1016/j.ejca.2019.07.006
13. Wasan H, Meade AM, Adams R, Wilson R, Pugh C, Fisher D, et al. COIN-B Investigators. Intermittent Chemotherapy Plus Either Intermittent or Continuous Cetuximab for First-Line Treatment of Patients With KRAS Wild-Type Advanced Colorectal Cancer (COIN-B): A Randomized Phase 2 Trial. Lancet Oncol (2014) 15(6):631–9. doi: 10.1016/S1470-2045(14)70106-8
14. Pfeiffer P, Sorbye H, Qvortrup C, Karlberg M, Kersten C, Vistisen K, et al. Maintenance Therapy With Cetuximab Every Second Week in the First-Line Treatment of Metastatic Colorectal Cancer: The NORDIC-7.5 Study by the Nordic Colorectal Cancer Biomodulation Group. Clin Colorectal Cancer (2015) 14(3):170–6. doi: 10.1016/j.clcc.2015.03.002
15. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur J Cancer (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
16. Woolley KK. How Variables Uncorrelated With the Dependent Variable Can Actually Make Excellent Predictors: The Important Suppressor Variable Case. Southwest Educational Research Association Annual Meeting Proceedings (1997). Available at: https://eric.ed.gov/?id=ED407420.
17. Thompson FT, Levine DU. Examples of Easily Explainable Suppressor Variables in Multiple Regression Research. Multiple Linear Regression Viewpoints (1997) 24:11–3.
18. “Stopping Stepwise: Why Stepwise Selection is Bad and What You Should Use Instead”. Available at: https://towardsdatascience.com/stopping-stepwise-why-stepwise-selection-is-bad-and-what-you-should-use-instead90818b3f52df.
19. Köhne CH, Grothey A, Bokemeyer C, Bontke M, Aapro M. Chemotherapy in Elderly Patients With Colorectal Cancer. Ann Oncol (2001) 12(4):435–42. doi: 10.1023/A:1011170808734
20. Yang Y, Wang G, He J, Ren J, Wu J, Zhang J, et al. Gender Differences in Colorectal Cancer Survival: A Meta-Analysis. Int J Cancer (2017) 141:1942–9. doi: 10.1002/ijc.30827
21. Köhne CH, Cunningham D, Di Costanzo F, Glimelius B, Blijham G, Aranda E, et al. Clinical Determinants of Survival in Patients With 5-Fluorouracil-Based Treatment for Metastatic Colorectal Cancer: Results of a Multivariate Analysis of 3825 Patients. Ann Oncol (2002) 13(2):308–17. doi: 10.1093/annonc/mdf034
22. Pinto C, Normanno N, Orlandi A, Fenizia F, Damato A, Maiello E, et al. Phase III Study With FOLFIRI + Cetuximab Versus FOLFIRI + Cetuximab Followed by Cetuximab Alone in RAS and BRAF WT mCRC. Future Oncol (2018) 14(14):1339–46. doi: 10.2217/fon-2017-0592
23. Lacouture ME, Sibaud V, Gerber PA, van den Hurk C, Fernández-Peñas P, Santini D, et al. Prevention and Management of Dermatological Toxicities Related to Anticancer Agents: ESMO Clinical Practice Guidelines. Ann Oncol (2021) 32(2):157–70. doi: 10.1016/j.annonc.2020.11.005
24. Linee Guida AIOM TUMORI DEL COLON. Available at: https://www.aiom.it/wp-content/uploads/2020/10/2020_LG_AIOM_Colon.pdf.
25. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO Consensus Guidelines for the Management of Patients With Metastatic Colorectal Cancer. Ann Oncol (2016) 27(8):1386–422. doi: 10.1093/annonc/mdw235
26. Parisi A, Cortellini A, Cannita K, Venditti O, Camarda F, Calegari MA, et al. Evaluation of Second-Line Anti-VEGF After First-Line Anti-EGFR Based Therapy in RAS Wild-Type Metastatic Colorectal Cancer: The Multicenter "SLAVE" Study. Cancers (Basel) (2020) 12(5):1259. doi: 10.3390/cancers12051259
27. Petrelli F, Pietrantonio F, Cremolini C, Di Bartolomeo M, Coinu A, Lonati V, et al. Early Tumour Shrinkage as a Prognostic Factor and Surrogate End-Point in Colorectal Cancer: A Systematic Review and Pooled-Analysis. Eur J Cancer (2015) 51(7):800–7. doi: 10.1016/j.ejca.2015.02.011
28. Ciardiello F, Normanno N, Martinelli E, Troiani T, Pisconti S, Cardone C, et al. Cetuximab Continuation After First Progression in Metastatic Colorectal Cancer (CAPRI-GOIM): A Randomized Phase II Trial of FOLFOX Plus Cetuximab Versus FOLFOX. Ann Oncol (2016) 27(6):1055–61. doi: 10.1093/annonc/mdw136
29. Parseghian C, Loree J, Morris V, Liu X, Clifton K, Napolitano S, et al. Anti-EGFR-Resistant Clones Decay Exponentially After Progression: Implications for Anti-EGFR Re-Challenge. Ann Oncol (2019) 30:243–9. doi: 10.1093/annonc/mdy509
30. Parisi A, Porzio G, Pulcini F, Cannita K, Ficorella C, Mattei V, et al. What Is Known About Theragnostic Strategies in Colorectal Cancer. Biomedicines (2021) 9(2):140. doi: 10.3390/biomedicines9020140
Keywords: MCRC, FOLFOX, FOLFIRI, cetuximab, panitumumab, maintenance, observation, de-escalation
Citation: Parisi A, Cortellini A, Venditti O, Filippi R, Salvatore L, Tortora G, Ghidini M, Nigro O, Gelsomino F, Zurlo IV, Fulgenzi C, Lombardi P, Roselló Keränen S, Depetris I, Giampieri R, Morelli C, Di Marino P, Di Pietro FR, Zanaletti N, Vitale P, Garajova I, Spinelli GP, Zoratto F, Roberto M, Petrillo A, Aimar G, Patruno L, D’Orazio C, Ficorella C, Ferri C and Porzio G (2021) Post-Induction Management in Patients With Left-Sided RAS and BRAF Wild-Type Metastatic Colorectal Cancer Treated With First-Line Anti-EGFR-Based Doublet Regimens: A Multicentre Study. Front. Oncol. 11:712053. doi: 10.3389/fonc.2021.712053
Received: 19 May 2021; Accepted: 28 September 2021;
Published: 27 October 2021.
Edited by:
Alessandro Passardi, Romagnolo Scientific Institute for the Study and Treatment of Tumors (IRCCS), ItalyReviewed by:
David Akhavan, University of Kansas Medical Center, United StatesCopyright © 2021 Parisi, Cortellini, Venditti, Filippi, Salvatore, Tortora, Ghidini, Nigro, Gelsomino, Zurlo, Fulgenzi, Lombardi, Roselló Keränen, Depetris, Giampieri, Morelli, Di Marino, Di Pietro, Zanaletti, Vitale, Garajova, Spinelli, Zoratto, Roberto, Petrillo, Aimar, Patruno, D’Orazio, Ficorella, Ferri and Porzio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandro Parisi, YWxleHBhcmlzQGhvdG1haWwuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.