
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol., 16 September 2021
Sec. Gastrointestinal Cancers
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.706331
This article is part of the Research TopicCurrent Innovations in GI-Oncology: Where do we stand?View all 7 articles
 Byeongsang Oh1,2,3,4*
Byeongsang Oh1,2,3,4* Frances Boyle2,3Nick Pavlakis1,3
Frances Boyle2,3Nick Pavlakis1,3 Stephen Clarke1,3Alex Guminski1,2,3Thomas Eade1,2,3Gillian Lamoury1,2,3Susan Carroll1,2,3Marita Morgia1,2Andrew Kneebone1,2,3George Hruby1,2,3
Stephen Clarke1,3Alex Guminski1,2,3Thomas Eade1,2,3Gillian Lamoury1,2,3Susan Carroll1,2,3Marita Morgia1,2Andrew Kneebone1,2,3George Hruby1,2,3 Mark Stevens1,2
Mark Stevens1,2 Wen Liu4
Wen Liu4 Brian Corless1
Brian Corless1 Mark Molloy5
Mark Molloy5 Towia Libermann6,7David Rosenthal7Michael Back1,2,3
Towia Libermann6,7David Rosenthal7Michael Back1,2,3Increasing evidence suggests that the gut microbiome is associated with both cancer chemotherapy (CTX) outcomes and adverse events (AEs). This review examines the relationship between the gut microbiome and CTX as well as the impact of CTX on the gut microbiome. A literature search was conducted in electronic databases Medline, PubMed and ScienceDirect, with searches for “cancer” and “chemotherapy” and “microbiome/microbiota”. The relevant literature was selected for use in this article. Seventeen studies were selected on participants with colorectal cancer (CRC; n=5), Acute Myeloid Leukemia (AML; n=3), Non-Hodgkin’s lymphoma (n=2), breast cancer (BCa; n=1), lung cancer (n=1), ovarian cancer (n=1), liver cancer (n=1), and various other types of cancers (n=3). Seven studies assessed the relationship between the gut microbiome and CTX with faecal samples collected prior to (n=3) and following CTX (n=4) showing that the gut microbiome is associated with both CTX efficacy and toxicity. Ten other prospective studies assessed the impact of CTX during treatment and found that CTX modulates the gut microbiome of people with cancer and that dysbiosis induced by the CTX is related to AEs. CTX adversely impacts the gut microbiome, inducing dysbiosis and is associated with CTX outcomes and AEs. Current evidence provides insights into the gut microbiome for clinicians, cancer survivors and the general public. More research is required to better understand and modify the impact of CTX on the gut microbiome.
Chemotherapy (CTX), systemic cancer treatment involving cytotoxic drugs, has significantly improved the overall survival of people with cancer (1). However, the main drawback of CTX are adverse events (AEs) related to treatment, which impact on both the physical and psychological well-being of patients. Up to 87% of people experienced at least one AE during and after CTX (2, 3), although recent advancements in CTX have achieved more tolerable and safer outcomes. Common AEs are nausea and vomiting, bloating, diarrhea, constipation, mucositis, CTX-induced peripheral neuropathy (CIPN), fatigue, hot flushes, anxiety and depression, insomnia and cognitive impairment. CTX also has the effect of suppressing immune responses and increasing the incidence of infection and subsequent morbidity and mortality (4).
Despite clinical practice guidelines that summarise evidence of effective strategies for preventing and managing AE’s (5–7), implementation has proven challenging. A further challenge for managing AEs, is to minimise health service costs (8–10), and also minimise the financial burden for patients and their families arising from cancer treatment (4, 11, 12). Furthermore, there are few effective biomarkers that have been developed to predict and/or proactively manage CTX-induced AEs (13, 14).
In the past decade, numerous studies have reported that the gut microbiome, defined as the collection of genomes from all micro-organisms in a given environment (15), is associated with the pathogenesis of cancer, including breast, colorectal (CRC), ovarian, and prostate (PCa) cancers (16). For example, an exploratory study in breast tissue in women with breast cancer examined the microbiota, defined as all the micro-organisms found in the environment and a term that is often used interchangeably with the microbiome (15), and found that malignancy was related to the enrichment in taxa of lower abundance, including the genera Fusobacterium, Atopobium, Gluconacetobacter, Hydrogenophaga and Lactobacillus (17). Another study compared differences in the gut microbiome of patients with CRC and healthy populations and found that the relative abundances of Prevotella, Collinsella and Peptostreptococcus were significantly higher in CRC patients, whereas the relative abundance of Escherichia-Shigella was significantly lower (16).
Previous reviews included preclinical and clinical trials (18) with systematic therapies (19), suggesting that the gut microbiome is not only associated with the development of cancer but also with CTX-induced toxicities. Studies in melanoma patients have identified that response to immunotherapy may be modified by the gut microbiome (20, 21). Other studies have proposed that the modulation of the gut microbiome in cancer patients before and during CTX might reduce the incidence of AEs and improve the efficacy of CTX (18, 22).
To date, few studies have examined the impact of CTX on the gut microbiome of cancer survivors in relation to CTX-induced AEs. Most of the previous reviews have included both preclinical and clinical studies and attempted to elucidate the underlying mechanisms of dysbiosis of gut microbiota in cancer pathogenesis but did not examine relationships between CTX-related AEs and the gut microbiome during and after treatment. Hence, our current review assesses the impact of CTX on the gut microbiome and CTX-related AEs in cancer patients and provides meaningful information for clinicians, patients, caregivers and the general public.
A literature search was conducted using the electronic databases Medline, PubMed and ScienceDirect, with the main search terms including “cancer” and “chemotherapy” and “microbiome/microbiota”. Inclusion criteria in the searches were: clinical trials conducted with adults (> 18 years) and published in English. References contained in the included studies were carefully reviewed for relevant papers that may have been missed by electronic searches. The search strategy was performed for studies published up to November 2020.
Seventeen studies were identified from the three electronic databases (Medline, PubMed and ScienceDirect) and included in this review (Table 1).
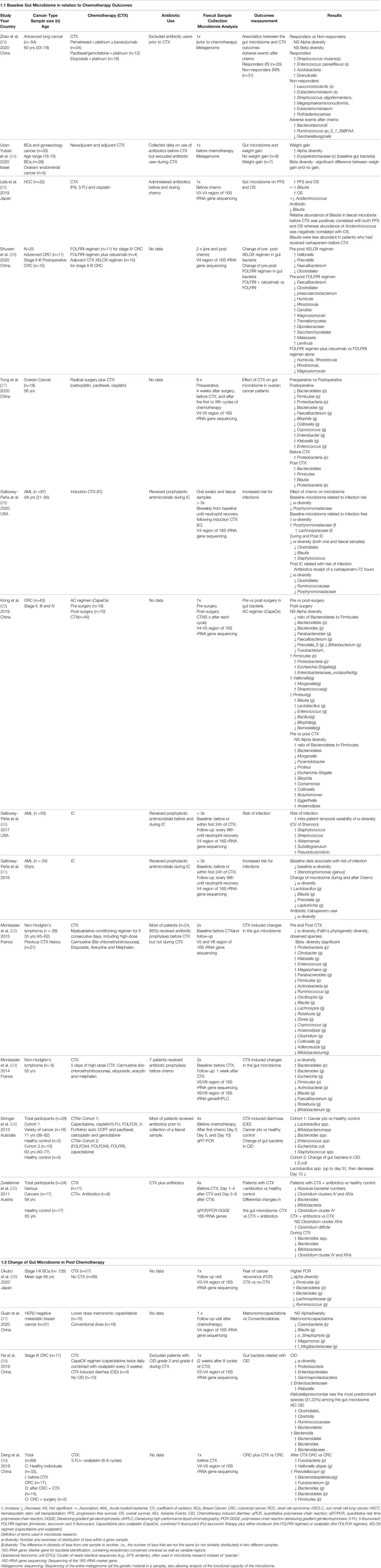
Table 1 The gut microbiome in chemotherapy outcomes.
The seventeen selected studies included a total of 742 patients with a range of 8 – 126 participants in each of the studies. Cancers studied included CRC (n=5) (26, 29, 38, 39), AML (n=3) (28, 30, 31), BCa (n=2) (24, 36), Non-Hodgkin’s lymphoma (n=2) (32, 33), lung cancer (n=1) (23), ovarian cancer (n=1) (27), liver cancer (n=1) (25), and various other types of cancers (n=3) (24, 34, 35). Six studies were conducted in China (23, 26, 27, 29, 38, 39), three in the USA (28, 30, 31), two in France (32, 33), two in Japan (25, 36), and one each in Austria (35), Australia (34) and Israel (24). Total CTX dosage, type of CTX drugs and periods of CTX interventions varied across studies. Study designs and the primary outcomes of individual studies included in this review were diverse.
Three studies assessed the relationship between the gut microbiome and CTX outcomes [response to CTX and AEs (23), weight gain (24), PFS and OS (25)] with faecal samples collected prior to CTX.
Eleven studies collected faecal samples multiple times (before, during and/or after CTX) and assessed the impact of CTX on the gut microbiome and the relationship between the gut microbiome and CTX-related AEs, including risk of infection, diarrhea and the effects of antibiotics (27, 28, 30–35).
In studies conducted with cancer survivors who had undergone chemoradiotherapy (CRT), two studies assessed the relationship between the gut microbiome and CTX-related AEs [fear of recurrence (36), diarrhea (38)], whereas two studies assessed the impact of CTX on the gut microbiome [low vs high dosage CTX (37), surgery vs surgery plus CTX (39)] with faecal samples collected after CTX.
Fifteen studies analysed the gut microbiome profile with the 16S ribosomal RNA (16S-rRNA) gene sequencing method, two with metagenomic sequencing (23, 24), one study with quantitative real time polymerase chain reaction (qRT/PCR) (34) and another study with qPCR and Denaturing gradient gel electrophoresis (DGGE) (35). Interestingly, analysis of gene sequencing regions of 16S rRNA varied across studies: V3-V4 (n=3) (25, 36, 38), V4 (n=4) (26, 28, 30, 31), V4-V5 (n=5) (27–29, 32, 39), V5-V6 (n=1) (33), qRT/PRC (n=1) (34), and qPCR/PCR-DGGE (n=1) (35).
Three studies assessed the relationship between baseline composition and diversity of the gut microbiome and CTX outcomes (23–25). Two studies reported that the composition and diversity of the gut microbiome was related to the efficacy of CTX (23, 25) and one study found that the composition and diversity of the gut microbiome was related to weight gain (24).
A recent study examined the relationship between the baseline gut microbiome in lung cancer patients (n=63) and CTX outcomes and found that the baseline gut microbiome was associated with both response to CTX and AEs (23). The relative abundance of Streptococcus mutans and Enterococcus casseliflavus were higher in responders (n=33) (p < 0.05), whereas 11 gut bacteria including Leuconostoc lactis and Eubacterium siraeum were enriched in non-responders (n=31) (p < 0.05). In addition, the relative abundance of Bacteroides nordii, Ruminococcus sp_5_1_39BFAA and Gardnerella vaginalis were associated with severe AEs of CTX.
A recent study of patients with BCa and gynaecological cancers (n=35) assessed the relationship between the gut microbiome and weight gain in those treated with adjuvant CTX (24). The study found that higher alpha diversity and enriched composition of the microbiome in pretreatment faecal samples was associated with weight gain following CTX (24).
Furthermore, faecal microbiota transplantation (FMT) from pre-treatment samples of those patients’ who gained weight post-treatment induces, glucose intolerance, adverse lipid changes and inflammatory changes in germ-free Swiss Webster mice (24). These results suggest that the gut microbiome is mediating metabolic changes in women who undertake CTX, as an adjuvant treatment, however further examination in a larger patient cohort is warranted.
An innovative study examined the effect of antibiotic use in patients with hepatocellular carcinoma (n=32) during CTX and found that the use of antibiotics (carbapenem) before and during CTX was associated with poor PFS and OS (carbapenem + vs. −; median PFS, 78 days vs. 154 days, p = 0.0053; median OS, 177 days vs. 475 days, p = 0.0003) (25). Notably, in this study it was reported that the relative abundance of Blautia in faecal samples before CTX was positively correlated with both PFS and OS, whereas abundance of Acidaminococcus was negatively correlated with OS. It also found that Blautia were less abundant in patients who had received carbapenem before CTX.
Another study compared the composition of gut bacteria in four groups, viz. healthy controls (n=33) vs patients diagnosed with CRC (n=17) vs patients with CRC plus surgery (n=5) vs patients with CRC plus CTX (n=14) (39). This study reported that, at the genus level, Veillonella and species Veillonella dispar were observed in CRC patients treated with CTX, but not in the other three groups. In addition, although not detected at the genus level, two other species, Prevotella copri and Bacteroides plebeius, were enriched in CRC patients treated with CTX (39), whereas alpha diversity of the gut microbiome was lower in CRC patients who received surgery, compared to the other three groups.
Ten studies examined the effect of CTX on the gut microbiome in patients receiving CTX; three with AML, two each with CRC, Non-Hodgkin’s lymphoma, a mixed group of cancers, and one with ovarian cancer patients.
Two studies conducted in CRC patients reported changes in the gut microbiome pre and post CTX (26, 29). One study examined the effects of three palliative CTX regimens (FOLFIRI (n=11) vs FOLFIRI regimen plus cetuximab (n=4) vs XELOX regimen (n=15)) on the gut microbiome and found that impacts on the gut microbiome varied according to the CTX regime administered (26). Namely, this study reported that the relative proportions of Faecalibacterium, Clostridiales, phascolarctobacterium, Humicola and Rhodotorula were decreased, and the abundances of Candida, Magnusiomyces, Tremellomycetes, Dipodascaceae, Saccharomycetales, Malassezia and Lentinula were increased in advanced CRC patients treated with the FOLFIRI regimen. In comparison with those treated with the FOLFIRI regimen alone the proportion of Humicola, Rhodotorula, and Magnusiomyces were decreased in advanced CRC patients treated with the FOLFIRI regimen combined with cetuximab, whilst those of Candida, Tremellomycetes, Dipodascaceae, Saccharomycetales, Malassezia and Lentinula were increased. The abundances of Veillonella, Humicola, Tremellomycetes and Malassezia were increased in postoperative CRC patients treated with the XELOX regimen. Another study conducted with CRC patients in stage II-IV (n=43) collected faecal sample five times after each treatment cycle and reported an increased ratio of Bacteroidetes to Firmicutes, Bacteroidetes, Bilophila Comamonas, Collinsella, Butyricimonas, Eggerthella and Anaerostipes, and decreased Morganella, Pyramidobacter, Proteus, and Escherichia-Shigella after CTX (29).
Three studies assessed the predictive value of the gut microbiome and its relationship to infection risk in patients with AML (28, 30, 31). Although these studies were conducted by the same research team, it was reported that the associations between the relative abundance of the gut microbiome and risk of infection varied across studies, while associations between risk of infection and alpha diversity of the gut microbiome was consistent in two studies (28, 31). One study (n=34) reported that lower alpha diversity and enriched Stenotrophomonas prior to CTX was associated with risk of infection in patients with AML (31). They also reported decreased alpha-diversity and decreased Blautia, Prevotella, Leptotrichia of the microbiome but increased Lactobacillus at the genus level during and after CTX. A subsequent study conducted with AML patients (n= 55) reported that increased intra-patient temporal variability of alpha-diversity and enriched Staphylococcus, Streptococcus, Akkermansia, Subdilogranulum, and Pseudobutyrivibrio were associated with risk of infection (30). The third study conducted with a large sample size (n=97) reported that, at baseline, higher alpha-diversity (hazard ratio [HR], 0.36; 95% confidence interval [CI],.18–.74) and relative abundance of Porphyromonadaceae (HR, 0.36; 95% CI,.18–.73) were associated with an increased probability of remaining infection-free during neutropenia (28). This study reported that the use of antibiotics (carbapenem >72 hours) increased the risk of infection in addition to lowering alpha-diversity and a relative low abundance of Clostridiales, Ruminococcaceae and Porphyromonadaceae.
Two studies examined the impact of CTX on the gut microbiome in patients undergoing one course of bone marrow transplantation (BMT) conditioning CTX and found that CTX changed the diversity and composition of the gut microbiome (32, 33).
An earlier study conducted with a small sample size (n=8) reported a significant reduction in alpha diversity and alterations in the composition of the gut microbiome associated with GI toxicities, viz. decreased Faecalibacterium, Bifidobacterium and increased Bacteroides, Proteobacteria and Escherichia (33). A subsequent study by the same researchers compared the diversity and composition of the gut microbiome with faecal samples from patients (n=28) before and after CTX (32). They reported, at genus level, significant decreases in the abundance of Ruminococcus, Oscillospira, Blautia, Lachnospira, Roseburia, Dorea, Coprococcus, Anaerostipes, Clostridium, Collin- sella, Adlercreutzia and Bifidobacterium.
One study assessed changes in the gut microbiome of ovarian cancer patients pre and post-surgery compared with surgery plus CTX (27). This study found significant decreases in the abundance of Bacteroidetes and Firmicutes and increases in the abundance of Proteobacteria after surgery. Interestingly, a comparison of pre and post CTX following surgery found the abundance of Bacteroidetes and Firmicutes increased, and the abundance of Proteobacteria decreased after CTX.
Furthermore, some forms of anaerobic bacteria, such as Bacteroides, Collinsella and Blautia significantly increased after CTX.
Two earlier studies explored the effects of CTX on gut bacteria in people diagnosed with various cancers (34, 35). One study examined the effect of gut bacteria related to CTX-induced diarrhea (CID) (34). They compared the gut bacteria of cancer patients with CID and a healthy control group and found decreased Lactobacillus spp., Bifidobacterium spp., Bacteroides spp. and Enterococcus spp. and increased Escherichia coli and Staphylococcus spp. in patients with CID (34).
Another similar study compared differences between patients after CTX and a healthy group, and found decreased diversity and Clostridium clusters IV and XIVa, Bacteroides, Bifidobacteria, Clostridium cluster IV in patients after CTX (35). In addition, this study investigated the differences in gut bacteria between patients who received CTX with antibiotics and those without and found an abundance of Clostridium difficile in patients treated with antibiotics. In these two studies, faecal samples were analysed using conventional culture techniques and qRT-PCR, while other studies included in this review were analysed using next generation sequencing (NGS), and advanced technology including 16S rRNA sequencing and metagenomics.
Four studies examined the relationship between the gut microbiome and cancer survivorship in patients who had received CTX (36–39). Faecal samples were collected at the follow-up visit after CTX and examined the relationship between the gut microbiome and post CTX-related AEs. Two studies examined the effects of CTX on the gut microbiome (low dose vs traditional dose of CTX and PFS (37), surgery vs surgery plus CTX) (39), and two other studies assessed the relationship between CID (38) and fear of recurrence (36) after CTX.
An earlier study explored the association between the gut microbiome and CID (completed 8 cycles of the CapeOX regimen: capecitabine (1000 mg/m2 twice daily) combined with oxaliplatin (130 mg/m2 every 3 weeks) in patients diagnosed with stage III CRC. This study found that the gut microbial community richness and diversity were lower after CTX in CID (p < 0.05) compared to a control group (38). It also reported that, at the species level, there were significant differences in 75 micro-organisms between the CRC with and without CID and identified that Klebsiella pneumoniae was the most predominant species among the gut microbiome in patients with CID.
A recent study examined the effect of CTX (low doses of metronomic capecitabine (n=15) vs conventional doses (n=16)) on the gut microbiome in women diagnosed with HER2-negative metastatic breast cancer and found that beta diversity (unweighted-unifrac index) was significantly lower in the metronomic group compared to the group who received conventional doses (p=0.025) (37). Furthermore, they found that the median PFS was significantly shorter in patients with the gut bacteria composition of Slackia (9.2 vs. 32.7 months, P = 0.004), while the patients with Blautia obeum had a significantly prolonged PFS compared to those without (32.7 vs. 12.9 months, P = 0.013). At the phylum level, the main composition of Cyanobacteria was significantly lower in the metronomic group, while the phyla of Bacteroidetes, Firmicutes, Proteobacteria, and Actinobacteria were similar between the groups. In addition, at the genus level, Megamonas and f_Mogibacteriaceae were significantly enriched and Blautia and o_Streptophyta were depleted in the metronomic group.
A recent study examined the relationship between the gut microbiota and FCR in women diagnosed with invasive breast cancer with a history of CTX (n=57) and those with no history of CTX (n=60) (36). Interestingly, this study found that in women with a history of CTX and FCR, lower alpha diversity, lower relative abundance of the Firmicutes (p=0.03) and higher relative abundance of Bacteroidetes (p=0.04) at the phylum level, and higher relative abundance of Bacteroides (p<0.01) and lower relative abundance of Lachinospitaceae (p=0.03) and Ruminococcus (p=0.02) at the genus level, were associated with FCR while there was no significant association in women diagnosed with invasive breast cancer with no history of CTX.
One study compared the composition of gut bacteria in four groups, viz., healthy controls (n=33) vs patients diagnosed with CRC (n=17) vs patients with CRC plus surgery (n=5) vs patients with CRC plus CTX (n=14) (39). This study reported that, at the genus level, Veillonella and species Veillonella dispar were only found in CRC patients treated with CTX but not in the other three groups. In addition, although not detected at the genus level, two other species, Prevotella copri and Bacteroides plebeius, were enriched in CRC patients treated with CTX, whereas alpha diversity of the gut microbiome was lower in CRC patients who received surgery compared to the other three groups.
Often prospective studies, seven studies collected data about use of antibiotics in participants. Three studies conducted with AML (28, 30, 31) and two studies with Non-Hodgkin’s lymphoma (32, 33) received antibiotics as prophylaxis prior and during CTX, one study each received antibiotics before chemotherapy and during CTX (34, 35). One study examined the difference between CTX with antibiotics versus CTX with no antibiotics and showed decreased diversity of Clostridium cluster IV and XIVa in response to CTX with cluster IV diversity being particularly affected by antibiotics (35).
Of the seven studies that examined the relationship, two studies excluded antibiotic users during recruitment (23, 38), one study included participants using antibiotics before but not during CTX (24), whereas, another study included participants using antibiotics before and during CTX (25).
The significance of the current review is that we not only assessed literature examining the relationship between the gut microbiome and CTX outcomes and AEs, but also the impact of CTX on the gut microbiome during treatment. Previous reviews examined the association between the gut microbiome and cancer survivors using limited clinical trials and attempted to elucidate the mechanisms of pathogenesis of cancer with preclinical studies (40, 41). Of seventeen studies reviewed, we found that three studies assessed the relationship between the gut microbiome and CTX outcomes (respondent vs non respondent, PFS, OS and weight gain) with faecal samples collected prior to CTX (23–25), whereas four other studies assessed the relationship between the gut microbiome and CTX outcomes (diarrhea, FCR, low dosage vs conventional dosage, surgery vs surgery plus CTX) with faecal samples collected either after CTX or in patients with a history of CTX (36) (37–39). In addition to evaluating these relationships, in ten other prospective studies, faecal samples were collected multiple times during CTX, and examined the impact of CTX on the gut microbiome which provided valuable insight into the importance of the gut microbiome in cancer survivors (26–35). The findings of the current review regarding the association between the gut microbiome and CTX-related AEs and treatment outcomes are consistent with previous reviews (19, 40, 41). Several studies reported consistent relationships between dysbiosis of the microbiome and CTX-related AEs and suggested that the gut microbiome has the potential to be applied as a biomarker to predict CTX outcomes and related AEs (40, 41). However, associations do not represent causation and further well-designed studies are required, such as a recent high quality clinical trial that is being undertaken in Canada exploring the effect of CTX on the gut microbiome (42). In recognition of weaknesses in the evidence from cohort studies, we examined causal links between the gut microbiome and CTX in ten prospective studies. A review of these ten studies assessed the impact of CTX on the gut microbiome during CTX and indicated that CTX modulated the gut microbiome, and that this modulatory effect is associated with an increased risk of infection and impacts on the efficacy of CTX. The ten prospective studies demonstrated the vital role of the gut microbiome in CTX and suggests that the modulation of the gut microbiome during CTX may reduce the risk of AEs and increase the efficacy of CTX. This hypothesis was partially supported by previous studies conducted with lifestyle interventions including prebiotics and exercise although there were some discrepancies among the studies (43–45).
Furthermore, several recent studies evaluated the effects of antibiotic exposure on cancer risk and reported that antibiotics tend to increase cancer risk (46–48) and reduce the efficacy of various forms of cancer therapy, including CTX, radiotherapy and immunotherapy (46, 49). Along the lines of these studies, we also assessed the use of antibiotics in this review. Of seventeen studies, nine studies (prospective studies (n=7) and cohort studies (n=2)) reported the use of antibiotics in their study design. In the prospective studies, three studies were conducted with AML (28, 30, 31) and two studies with Non-Hodgkin’s lymphoma (32, 33) where patients received antibiotics as prophylaxis prior to, and during CTX, and in one study each patient received antibiotics before CTX and during CTX (34, 35).
This study finding the association between the use of antibiotic and poor efficacy is comparable to an earlier study performed with patients with advanced non-small cell lung cancer (NSCLC) treated with nivolumab and with antibiotic (50). Previously, only one study had examined the difference in outcomes between CTX with antibiotics versus CTX with no antibiotics and reported a decreased diversity of Clostridium cluster IV and XIVa in response to CTX, with cluster IV diversity being particularly affected by antibiotics (35). However, a major limitation of this finding was that faecal samples were analysed using conventional culture techniques and qRT-PCR, whereas in most of the recent studies included in this review, samples were analysed using next generation sequencing (NGS) advanced technology including 16S rRNA sequencing and metagenomics.
Consequently, in future studies, a comparison of the effects of CTX on the gut microbiome of patients, with and without antibiotics, utilizing modern NGS technology will be worthwhile.
This review has several limitations. Firstly, while the main strength of the review is its assessment of causal effects of CTX on the gut microbiome, in addition to the relationships between the gut microbiome and CTX outcome and AEs, we found that a number of studies (n=10) were conducted with heterogeneous cancer populations; AML (n=3), CRC (n=2), Non-Hodgkin’s lymphoma (n=2), ovarian cancer (n=1) and mixed cancer groups (n=2). Hence, in order to identify specific gut bacteria related to certain cancer types, more studies are required with matching diagnoses for types of cancers. Also, most of the studies reviewed (n=8) were conducted with very small sample sizes ranging from 8 to 43 participants. Although two studies were conducted with moderate sample sizes of 55 and 97 participants, neither study described any power calculation in their methodologies leading to concerns about the validity of the results. Moreover, interpretations of causal effects in the outcomes of several studies are complex because of a range of potentially confounding variables. For example, administering various CTX drugs among studies instead of standard CXT drug interventions, the use of groups of multiple cancer survivors, a lack of standardization in the microbiome analysis of faecal samples, varied outcome measures and varied study design complicated the conclusions drawn. Although having studies conducted across several countries [China (n=6) (23, 26, 27, 29, 38, 39), USA (n=3) (28, 30, 31), France (n=2) (32, 33), Japan (n=2) (25, 36), Austria (n=1) (35), Australia (n=1) (34), and Israel (n=1) (24)] increases the generalizability of results, it also makes for a more complex interpretation of the data as several studies have demonstrated that the gut microbiome is associated with ethnicity, diet, physical activities and environment (51–53). Hence, future international multicentre trials will need to be conducted to provide comprehensive and reliable data that controls for confounding patient variables including age, ethnicity, gender, co-morbidities, drug use, geography, and lifestyle factors, including diet and physical activities.
Considering these limitations, future studies with larger sample sizes and robust study designs are required to provide evidence that can readily translate into the clinical setting. To our knowledge, the current comprehensive literature review is the first to examine causal relationships of the gut microbiome on CTX outcomes and AEs with prospective clinical trials, and to assess the relationship between the gut microbiome and CTX outcomes and CTX-related AEs with observational studies. In conclusion, although there is a lack of high quality clinical trials on this topic, our results from a comprehensive review provides further insight into the complex relationships between the gut microbiome and CTX and shows the potential for future research to improve patient care. The current evidence suggests the potential implications for the gut microbiome to predict CTX outcome and prevent AEs in patients undergoing CTX, however, several challenges remain and need to be resolved before recommending microbiome therapy in oncology.
All authors cooperated on developing the concept design and preparing the manuscript. Drafting of the manuscript: BO, BC, FB, TL, GH and NP. All authors contributed to the article and approved the submitted version.
Publication fee is supported by the Department of Radiation Oncology, Royal North Shore Hospital.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Noonan KL, Ho C, Laskin J, Murray N. The Influence of the Evolution of First-Line Chemotherapy on Steadily Improving Survival in Advanced Non-Small-Cell Lung Cancer Clinical Trials. J Thorac Oncol (2015) 10:1523–31. doi: 10.1097/JTO.0000000000000667
2. Montemurro F, Mittica G, Cagnazzo C, Longo V, Berchialla P, Solinas G, et al. Self-Evaluation of Adjuvant Chemotherapy-Related Adverse Effects by Patients With Breast Cancer. JAMA Oncol (2016) 2:445–52. doi: 10.1001/jamaoncol.2015.4720
3. Pearce A, Haas M, Viney R, Pearson S-A, Haywood P, Brown C, et al. Incidence and Severity of Self-Reported Chemotherapy Side Effects in Routine Care: A Prospective Cohort Study. PloS One (2017) 12:e0184360–e0184360. doi: 10.1371/journal.pone.0184360
4. Stokes ME, Muehlenbein CE, Marciniak MD, Faries DE, Motabar S, Gillespie TW, et al. Neutropenia-Related Costs in Patients Treated With First-Line Chemotherapy for Advanced Non-Small Cell Lung Cancer. J Manag Care Pharm (2009) 15:669–82. doi: 10.18553/jmcp.2009.15.8.669
5. Sharma R, Tobin P, Clarke SJ. Management of Chemotherapy-Induced Nausea, Vomiting, Oral Mucositis, and Diarrhoea. Lancet Oncol (2005) 6:93–102. doi: 10.1016/S1470-2045(05)01735-3
6. Raji MA. Management of Chemotherapy-Induced Side-Effects. Lancet Oncol (2005) 6:357. doi: 10.1016/S1470-2045(05)70182-0
7. Maroun JA, Anthony LB, Blais N, Burkes R, Dowden SD, Dranitsaris G, et al. Prevention and Management of Chemotherapy-Induced Diarrhea in Patients With Colorectal Cancer: A Consensus Statement by the Canadian Working Group on Chemotherapy-Induced Diarrhea. Curr Oncol (Toronto Ont) (2007) 14:13–20. doi: 10.3747/co.2007.96
8. Ward RL, Laaksonen MA, van Gool K, Pearson S-A, Daniels B, Bastick P, et al. Cost of Cancer Care for Patients Undergoing Chemotherapy: The Elements of Cancer Care Study. Asia Pac J Clin Oncol (2015) 11:178–86. doi: 10.1111/ajco.12354
9. Rashid N, Koh HA, Baca HC, Lin KJ, Malecha SE, Masaquel A. Economic Burden Related to Chemotherapy-Related Adverse Events in Patients With Metastatic Breast Cancer in an Integrated Health Care System. Breast Cancer (Dove Med Press) (2016) 8:173–81. doi: 10.2147/BCTT.S105618
10. Irwin DE, Masaquel A, Johnston S, Barnett B. Adverse Event-Related Costs for Systemic Metastatic Breast Cancer Treatment Among Female Medicaid Beneficiaries. J Med Economics (2016) 19:1027–33. doi: 10.1080/13696998.2016.1192548
11. Liou SY, Stephens JM, Carpiuc KT, Feng W, Botteman MF, Hay JW. Economic Burden of Haematological Adverse Effects in Cancer Patients: A Systematic Review. Clin Drug Investig (2007) 27:381–96. doi: 10.2165/00044011-200727060-00002
12. Hurvitz S, Guerin A, Brammer M, Guardino E, Zhou Z-Y, Latremouille Viau D, et al. Investigation of Adverse-Event-Related Costs for Patients With Metastatic Breast Cancer in a Real-World Setting. Oncol (2014) 19:901–8. doi: 10.1634/theoncologist.2014-0059
13. Timmins HC, Li T, Goldstein D, Trinh T, Mizrahi D, Harrison M, et al. The Impact of Obesity on Neuropathy Outcomes for Paclitaxel- and Oxaliplatin-Treated Cancer Survivors. J Cancer Surviv (2021). doi: 10.1007/s11764-021-01012-y
14. Wigle TJ, Tsvetkova EV, Welch SA, Kim RB. DPYD and Fluorouracil-Based Chemotherapy: Mini Review and Case Report. Pharmaceutics (2019) 11:199. doi: 10.3390/pharmaceutics11050199
15. Quigley EMM, Gajula P. Recent Advances in Modulating the Microbiome. F1000Research (2020) 9:F1000 Faculty Rev–46. doi: 10.12688/f1000research.20204.1
16. Sheng Q, Du H, Cheng X, Cheng X, Tang Y, Pan L, et al. Characteristics of Fecal Gut Microbiota in Patients With Colorectal Cancer at Different Stages and Different Sites. Oncol Lett (2019) 18:4834–44. doi: 10.3892/ol.2019.10841
17. Hieken TJ, Chen J, Hoskin TL, Walther-Antonio M, Johnson S, Ramaker S, et al. The Microbiome of Aseptically Collected Human Breast Tissue in Benign and Malignant Disease. Sci Rep (2016) 6:30751. doi: 10.1038/srep30751
18. Chen J, Douglass J, Prasath V, Neace M, Atrchian S, Manjili MH, et al. The Microbiome and Breast Cancer: A Review. Breast Cancer Res Treat (2019) 178:493–6. doi: 10.1007/s10549-019-05407-5
19. Aarnoutse R, Ziemons J, Penders J, Rensen SS, de Vos-Geelen J, Smidt ML. The Clinical Link Between Human Intestinal Microbiota and Systemic Cancer Therapy. Int J Mol Sci (2019) 20(17):4145. doi: 10.3390/ijms20174145
20. Gopalakrishnan V, Spencer CN, Nezi L, Reuben A, Andrews MC, Karpinets TV, et al. Gut Microbiome Modulates Response to Anti-PD-1 Immunotherapy in Melanoma Patients. Science (2018) 359:97–103. doi: 10.1126/science.aan4236
21. Peters BA, Wilson M, Moran U, Pavlick A, Izsak A, Wechter T, et al. Relating the Gut Metagenome and Metatranscriptome to Immunotherapy Responses in Melanoma Patients. Genome Med (2019) 11:61. doi: 10.1186/s13073-019-0672-4
22. Villéger R, Lopès A, Carrier G, Veziant J, Billard E, Barnich N, et al. Intestinal Microbiota: A Novel Target to Improve Anti-Tumor Treatment? Int J Mol Sci (2019) 20(18):4548. doi: 10.3390/ijms20184584
23. Zhao Z, Fei K, Bai H, Wang Z, Duan J, Wang J. Metagenome Association Study of the Gut Microbiome Revealed Biomarkers Linked to Chemotherapy Outcomes in Locally Advanced and Advanced Lung Cancer. Thorac Cancer n/a (2020) 12(1):66–78. doi: 10.21203/rs.3.rs-48380/v1
24. Uzan-Yulzari A, Morr M, Tareef-Nabwani H, Ziv O, Magid-Neriya D, Armoni R, et al. The Intestinal Microbiome, Weight, and Metabolic Changes in Women Treated by Adjuvant Chemotherapy for Breast and Gynecological Malignancies. BMC Med (2020) 18:281. doi: 10.1186/s12916-020-01751-2
25. Iida N, Mizukoshi E, Yamashita T, Terashima T, Arai K, Seishima J, et al. Overuse of Antianaerobic Drug Is Associated With Poor Postchemotherapy Prognosis of Patients With Hepatocellular Carcinoma. Int J Cancer (2019) 145:2701–11. doi: 10.1002/ijc.32339
26. Shuwen H, Xi Y, Yuefen P, Jiamin X, Quan Q, Haihong L, et al. Effects of Postoperative Adjuvant Chemotherapy and Palliative Chemotherapy on the Gut Microbiome in Colorectal Cancer. Microb Pathog (2020) 149:104343. doi: 10.1016/j.micpath.2020.104343
27. Tong J, Zhang X, Fan Y, Chen L, Ma X, Yu H, et al. Changes of Intestinal Microbiota in Ovarian Cancer Patients Treated With Surgery and Chemotherapy. Cancer Manag Res (2020) 12:8125–35. doi: 10.2147/CMAR.S265205
28. Galloway-Peña JR, Shi Y, Peterson CB, Sahasrabhojane P, Gopalakrishnan V, Brumlow CE, et al. Gut Microbiome Signatures Are Predictive of Infectious Risk Following Induction Therapy for Acute Myeloid Leukemia. Clin Infect Dis (2020) 71:63–71. doi: 10.1093/cid/ciz777
29. Kong C, Gao R, Yan X, Huang L, He J, Li H, et al. Alterations in Intestinal Microbiota of Colorectal Cancer Patients Receiving Radical Surgery Combined With Adjuvant CapeOx Therapy. Sci China Life Sci (2019) 62:1178–93. doi: 10.1007/s11427-018-9456-x
30. Galloway-Peña JR, Smith DP, Sahasrabhojane P, Wadsworth WD, Fellman BM, Ajami NJ, et al. Characterization of Oral and Gut Microbiome Temporal Variability in Hospitalized Cancer Patients. Genome Med (2017) 9:21–1. doi: 10.1186/s13073-017-0409-1
31. Galloway-Peña JR, Smith DP, Sahasrabhojane P, Ajami NJ, Wadsworth WD, Daver NG, et al. The Role of the Gastrointestinal Microbiome in Infectious Complications During Induction Chemotherapy for Acute Myeloid Leukemia. Cancer (2016) 122:2186–96. doi: 10.1002/cncr.30039
32. Montassier E, Gastinne T, Vangay P, Al-Ghalith GA, Bruley des Varannes S, Massart S, et al. Chemotherapy-Driven Dysbiosis in the Intestinal Microbiome. Aliment Pharmacol Ther (2015) 42:515–28. doi: 10.1111/apt.13302
33. Montassier E, Batard E, Massart S, Gastinne T, Carton T, Caillon J, et al. 16s rRNA Gene Pyrosequencing Reveals Shift in Patient Faecal Microbiota During High-Dose Chemotherapy as Conditioning Regimen for Bone Marrow Transplantation. Microb Ecol (2014) 67:690–9. doi: 10.1007/s00248-013-0355-4
34. Stringer AM, Al-Dasooqi N, Bowen JM, Tan TH, Radzuan M, Logan RM, et al. Biomarkers of Chemotherapy-Induced Diarrhoea: A Clinical Study of Intestinal Microbiome Alterations, Inflammation and Circulating Matrix Metalloproteinases. Support Care Cancer (2013) 21:1843–52. doi: 10.1007/s00520-013-1741-7
35. Zwielehner J, Lassl C, Hippe B, Pointner A, Switzeny OJ, Remely M, et al. Changes in Human Fecal Microbiota Due to Chemotherapy Analyzed by TaqMan-PCR, 454 Sequencing and PCR-DGGE Fingerprinting. PloS One (2011) 6:e28654. doi: 10.1371/journal.pone.0028654
36. Okubo R, Kinoshita T, Katsumata N, Uezono Y, Xiao J, Matsuoka YJ. Impact of Chemotherapy on the Association Between Fear of Cancer Recurrence and the Gut Microbiota in Breast Cancer Survivors. Brain Behav Immun (2020) 85:186–91. doi: 10.1016/j.bbi.2019.02.025
37. Guan X, Ma F, Sun X, Li C, Li L, Liang F, et al. Gut Microbiota Profiling in Patients With HER2-Negative Metastatic Breast Cancer Receiving Metronomic Chemotherapy of Capecitabine Compared to Those Under Conventional Dosage. Front Oncol (2020) 10:902. doi: 10.3389/fonc.2020.00902
38. Fei Z, Lijuan Y, Xi Y, Wei W, Jing Z, Miao D, et al. Gut Microbiome Associated With Chemotherapy-Induced Diarrhea From the CapeOX Regimen as Adjuvant Chemotherapy in Resected Stage III Colorectal Cancer. Gut Pathog (2019) 11:18. doi: 10.1186/s13099-019-0299-4
39. Deng X, Li Z, Li G, Li B, Jin X, Lyu G. Comparison of Microbiota in Patients Treated by Surgery or Chemotherapy by 16S rRNA Sequencing Reveals Potential Biomarkers for Colorectal Cancer Therapy. Front Microbiol (2018) 9:1607. doi: 10.3389/fmicb.2018.01607
40. Ervin SM, Ramanan SV, Bhatt AP. Relationship Between the Gut Microbiome and Systemic Chemotherapy. Dig Dis Sci (2020) 65:874–84. doi: 10.1007/s10620-020-06119-3
41. Secombe KR, Coller JK, Gibson RJ, Wardill HR, Bowen JM. The Bidirectional Interaction of the Gut Microbiome and the Innate Immune System: Implications for Chemotherapy-Induced Gastrointestinal Toxicity. Int J Cancer (2019) 144:2365–76. doi: 10.1002/ijc.31836
42. Deleemans JM, Chleilat F, Reimer RA, Henning J-W, Baydoun M, Piedalue K-A, et al. The Chemo-Gut Study: Investigating the Long-Term Effects of Chemotherapy on Gut Microbiota, Metabolic, Immune, Psychological and Cognitive Parameters in Young Adult Cancer Survivors; Study Protocol. BMC Cancer (2019) 19:1243. doi: 10.1186/s12885-019-6473-8
43. Mailing LJ, Allen JM, Buford TW, Fields CJ, Woods JA. Exercise and the Gut Microbiome: A Review of the Evidence, Potential Mechanisms, and Implications for Human Health. Exercise Sport Sci Rev (2019) 47:75–85. doi: 10.1249/JES.0000000000000183
44. Górska A, Przystupski D, Niemczura MJ, Kulbacka J. Probiotic Bacteria: A Promising Tool in Cancer Prevention and Therapy. Curr Microbiol (2019) 76:939–49. doi: 10.1007/s00284-019-01679-8
45. Hendler R, Zhang Y. Probiotics in the Treatment of Colorectal Cancer. Medicines (Basel) (2018) 5:101. doi: 10.3390/medicines5030101
46. Amadei SS, Notario V. A Significant Question in Cancer Risk and Therapy: Are Antibiotics Positive or Negative Effectors? Current Answers and Possible Alternatives. Antibiotics (Basel) (2020) 9(9):580. doi: 10.3390/antibiotics9090580
47. Velicer CM, Heckbert SR, Lampe JW, Potter JD, Robertson CA, Taplin SH. Antibiotic Use in Relation to the Risk of Breast Cancer. Jama (2004) 291:827–35. doi: 10.1001/jama.291.7.827
48. Cao Y, Wu K, Mehta R, Drew DA, Song M, Lochhead P, et al. Long-Term Use of Antibiotics and Risk of Colorectal Adenoma. Gut (2018) 67:672–8. doi: 10.1136/gutjnl-2016-313413
49. Pinato DJ, Gramenitskaya D, Altmann DM, Boyton RJ, Mullish BH, Marchesi JR, et al. Antibiotic Therapy and Outcome From Immune-Checkpoint Inhibitors. J Immunother Cancer (2019) 7:287. doi: 10.1186/s40425-019-0775-x
50. Ouaknine Krief J, Helly de Tauriers P, Dumenil C, Neveux N, Dumoulin J, Giraud V, et al. Role of Antibiotic Use, Plasma Citrulline and Blood Microbiome in Advanced Non-Small Cell Lung Cancer Patients Treated With Nivolumab. J Immunother Cancer (2019) 7:176. doi: 10.1186/s40425-019-0658-1
51. Senghor B, Sokhna C, Ruimy R, Lagier J-C. Gut Microbiota Diversity According to Dietary Habits and Geographical Provenance. Hum Microb J (2018) 7-8:1–9. doi: 10.1016/j.humic.2018.01.001
52. Deschasaux M, Bouter KE, Prodan A, Levin E, Groen AK, Herrema H, et al. Depicting the Composition of Gut Microbiota in a Population With Varied Ethnic Origins But Shared Geography. Nat Med (2018) 24:1526–31. doi: 10.1038/s41591-018-0160-1
Keywords: gut microbiome, chemotherapy, cancer, biomarker, adverse events
Citation: Oh B, Boyle F, Pavlakis N, Clarke S, Guminski A, Eade T, Lamoury G, Carroll S, Morgia M, Kneebone A, Hruby G, Stevens M, Liu W, Corless B, Molloy M, Libermann T, Rosenthal D and Back M (2021) Emerging Evidence of the Gut Microbiome in Chemotherapy: A Clinical Review. Front. Oncol. 11:706331. doi: 10.3389/fonc.2021.706331
Received: 07 May 2021; Accepted: 25 August 2021;
Published: 16 September 2021.
Edited by:
Holger Rumpold, Ordensklinikum Linz, AustriaReviewed by:
Mohammad Raghibul Hasan, Shaqra University, Saudi ArabiaCopyright © 2021 Oh, Boyle, Pavlakis, Clarke, Guminski, Eade, Lamoury, Carroll, Morgia, Kneebone, Hruby, Stevens, Liu, Corless, Molloy, Libermann, Rosenthal and Back. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Byeongsang Oh, Ynllb25nLm9oQHN5ZG5leS5lZHUuYXU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.