 Stine Elleberg Petersen*
Stine Elleberg Petersen* Morten Høyer
Morten Høyer- Danish Centre for Particle Therapy, Aarhus University Hospital, Aarhus, Denmark
Purpose: There is high-level evidence for addition of androgen deprivation therapy to photon-based radiotherapy of the prostate in intermediate- and high-risk prostate cancer. Little is known about the value of ADT in particle therapy of prostate cancer. We are conducting a systematic review on biochemical disease-free survival, overall survival, and morbidity after combined particle therapy and ADT for prostate cancer.
Methods: A thorough search in PubMed, Embase, Scopus, and Web of Science databases were conducted, searching for relevant studies. Clinical studies on prostate cancer and the treatment combination of particle therapy and androgen deprivation therapy were included. The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and registered on PROSPERO (CRD42021230801).
Results: A total of 298 papers were identified. Fifteen papers reporting on 7,202 patients after proton or carbon-ion therapy for localized prostate cancer where a fraction or all patients received ADT were selected for analysis. Three thousand five hundred and nineteen (49%) of the patients had received combined ADT and particle therapy. Primarily high-risk (87%), to a lesser extent intermediate-risk (34%) and low-risk patients (12%) received ADT. There were no comparative studies on the effect of ADT in patients treated with particles and no studies identified ADT as an independent prognostic factor related to survival outcomes.
Conclusions: The review found no evidence to support that the effects on biochemical disease-free survival and morbidity of combining ADT to particle therapy differs from the ADT effects in conventional photon based radiotherapy. The available data on the topic is limited.
Introduction
Prostate cancer (PC) is the second most common cancer among men worldwide, however with a relatively high survival rate (1). The efficacy of radiotherapy (RT) of PC was demonstrated in the randomized Scandinavian Prostatic Cancer Group 7 (SPCG-7) trial where intermediate- and high-risk patients receiving 70 Gy to the prostate had superior survival outcomes compared to patients who did not receive RT (2). In the SPCG-7 study, patients in both randomization arms received 3 months of neoadjuvant androgen deprivation therapy (ADT) and life-long antiandrogen. The European Organization for Research and Treatment of Cancer (EORTC) 62863 Study randomized high-risk patients who all received pelvic RT to either long-term (3 years) ADT or no ADT showed that concomitant/adjuvant ADT improved 10-years overall survival (OS) from 40% (95% CI 32–48%) to 58% (95% CI 49–66%) in high-risk PC patients (3). Short-term ADT (6 months), however, provides inferior OS as compared with 3-years of ADT as demonstrated in the EORTC 22961 Study (4). In intermediate-risk PC patient, the EORTC 22991 Study showed that combined RT plus short-term ADT (6 months) increased biochemical disease-free survival (bDFS) (5).
In most studies on the efficacy of concomitant/adjuvant ADT, the patients received conventional RT doses (60–70 Gy) that are now considered inadequate. Dose-escalation studies randomizing between 70 Gy or 74–78 Gy with long-term follow-up have shown improved bDFS with high dose (6–10) and a very recent study on simultaneous integrated boost with up to 95 Gy to focal intraprostatic lesions further improved bDFS (11). Studies of escalated proton boost to the prostate from the Massachusetts General Hospital revealed improved bDFS in patients receiving the escalated dose (12). The escalated radiation dose to the prostate may to some extent neutralize the effect of concomitant/adjuvant ADT, but guidelines still recommend the same concomitant/adjuvant ADT combined with high-dose radiation therapy (13).
Particle therapy is used to optimize the therapeutic ration in treatment of PC, improving disease control and minimizing treatment related morbidities. However, little is known about the interaction between particle therapy and ADT and the outcomes regarding bDFS, overall survival, and morbidity for PC patients. We conducted a review on the efficacy of the combination of particle therapy and ADT and the morbidity following this combined treatment.
Methods
Literature Search Strategy and Data Sources
The systematic review process was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (14, 15); the protocol is registered in the PROSPERO database (registration number CRD42021230801). On January 11, 2021 a thorough database literature search was performed on PubMed, Embase, Web of Science, and Scopus to identify relevant publications. The following keywords were used: prostate neoplasms, prostate cancer, prostate carcinoma, prostate tumor, proton, proton therapy, carbon ion therapy, androgen antagonists, androgen depravation therapy, and antiandrogen.
Study Selection
To identify relevant studies, the following inclusion criteria were used: original study, clinical study, ADT combined with particle therapy in primary therapy for prostate cancer, and reporting of treatment outcomes (see below). The following exclusion criteria were used: language other than English, Danish, Swedish, or Norwegian, reviews, meta-analyses, guidelines, editorials, comments, case reports, letters to and communications without original data, and conference abstracts. If publications of identical patient cohorts were found, the most complete study was chosen.
Interventions
The interventions were particle therapy and ADT to patients with PC in a curative setting. Neoadjuvant, adjuvant, and the combination of neoadjuvant plus adjuvant ADT were considered.
Outcomes
Biochemical disease-free survival, OS, acute and late morbidity, and patient reported outcome measures (PROs) were outcomes of interest. Biochemical disease-free survival was defined by the Phoenix criteria (16) and OS was defined in the individual papers. Morbidity and PROs were any morbidity described in the papers regarding grade and timing (acute or late).
Data Extraction and Quality Assessment
For initial inclusion in the study, the two authors (MH and SP) independently screened titles and abstract, in case of disagreement, consensus was reached. Full text screening and data extraction was performed by one of the authors (SP) and checked by the other author (MH). Endnote (17) was used to manage study selection and Covidence (18) was used in the process of inclusion and exclusion of papers.
Results
Study Selection and Patients’ Characteristics
The literature search revealed a total of 298 papers. After removal of duplicates, 192 papers were eligible for review. Titles and abstracts were screened for eligibility based on the intervention and outcomes, 40 papers were eligible for full-text screening. Of the 40 papers, 15 papers met the selection criteria for analysis (Figure 1). Of the 15 studies, nine had a prospective design, four had a retrospective design, and one study was a match-pair analysis. The number of included patients ranged from 58 to 2,021 and follow-up time varied from 1 year to 7 years. Seven studies reported on bDFS and OS. All studies reported on morbidity in terms of one or more of the following: toxicity scoring, PROs, and QoL.
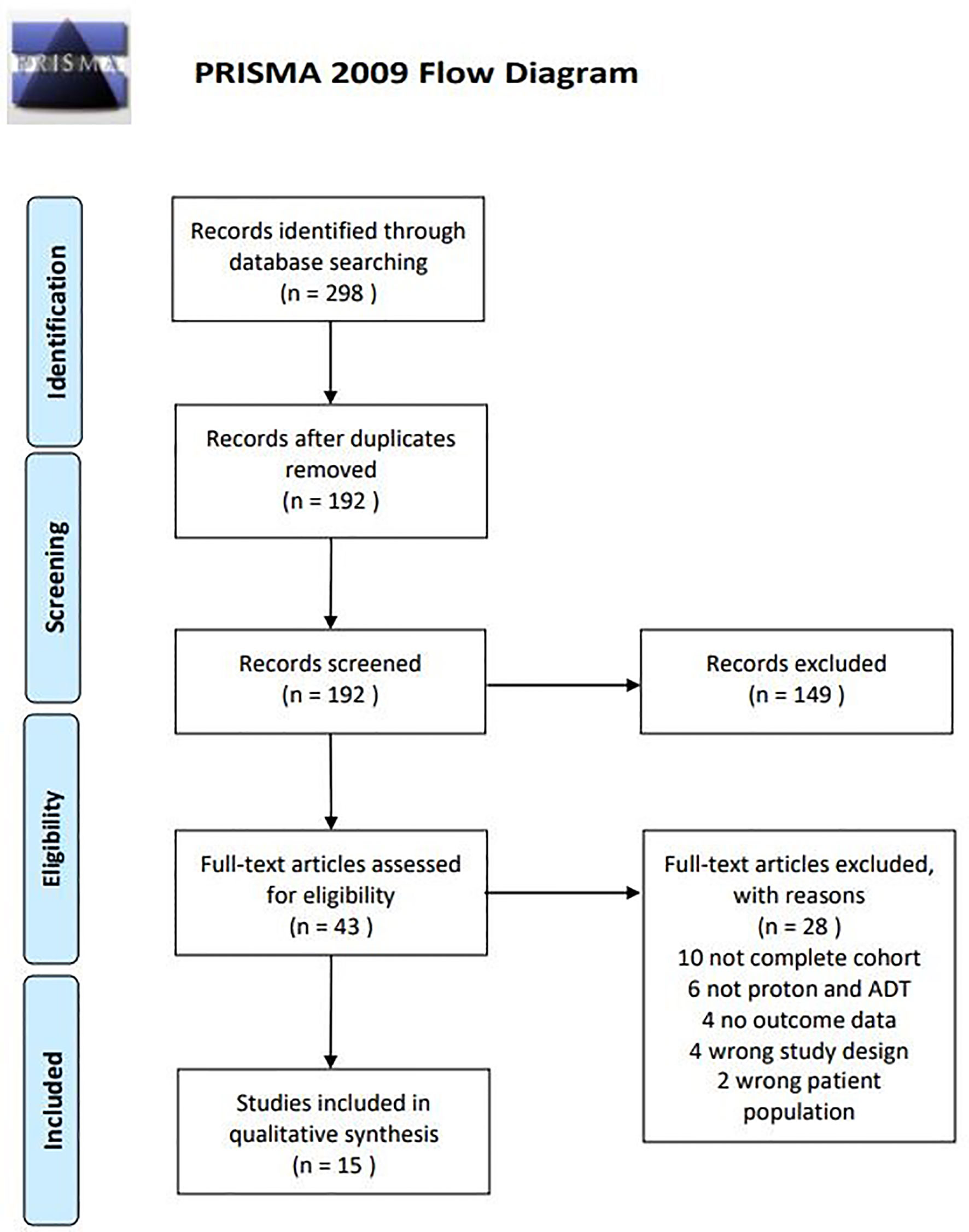
Figure 1 Flow chart of inclusion and exclusion procedure.
The 15 papers reported on a total of 7,202 patients. Of these, 1,411 (20%) had low-risk, 2,837 (41%) intermediate-risk, and 2,639 (39%) high-risk disease. Patients received proton only in seven studies, carbon ions in four studies, combined protons and photons in three of the studies, and protons or carbon ions in one study. Total dose and dose per fraction fractionation ranged 51.6–82 Gy (RBE) and 1.8–5 Gy (RBE), respectively (Table 1). The majority of patients received treatment on prostate only, in two of the studies 34 (3%) and 5 (6.6%) of the patients received prophylactic pelvic irradiation (Table 1). Across all included studies, 3,519 (49%) patients received ADT. In studies reporting D’Amico risk-group, 12% (range between studies: 0–22%) of the low-risk, 34% (0–67%) of the intermediate-risk, and 87% (66–100%) of the high-risk patients received ADT (Table 2). The median duration of ADT was only reported in six studies, ranging from 6 to 30.2 months.
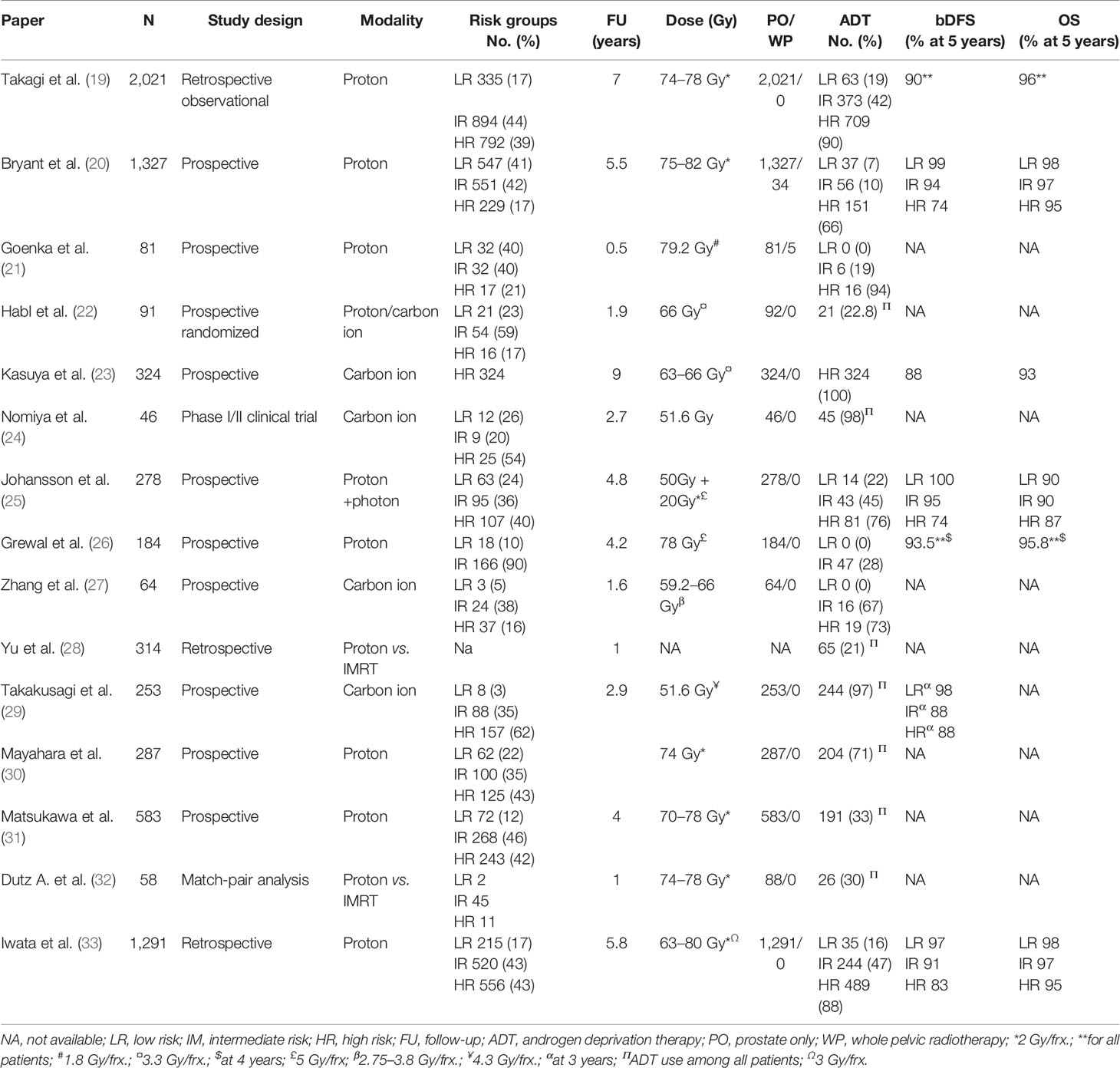
Table 1 Biochemical disease-free survival and overall survival.
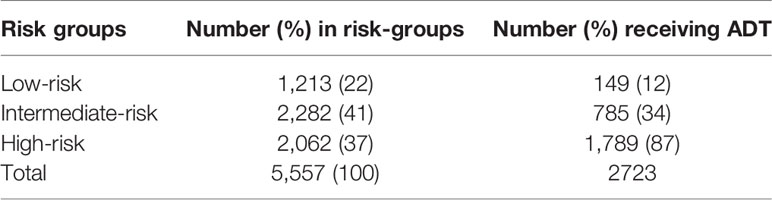
Table 2 Use of ADT across studies (only eight studies reporting ADT included).
Disease Free Biochemical Survival and Overall Survival
Of the seven publications reporting bDFS and OS, five stratified patients into low-, intermediate-, or high-risk groups according to D’Amico (34) and reported bDFS and OS for the three risk groups. The bDFS reported at 3–5 years ranged 87–100, 88–95, and 74–88% for the low-, intermediate-, and high-risk group, respectively. Overall survival rates at 5 years ranged from 90–98.4, 90–97, and 87–95.2% for the three risk groups (Table 1). The prognostic value of long-term (>24 months) ADT on bDFS was tested in a study on carbon-ion therapy for high-risk PC where long-term was not superior to short-term (<12 months) ADT (23). Androgen deprivation therapy was not tested as an independent prognostic factor in any of the studies included in the analysis.
Morbidity Scores, Patient-Reported Outcomes, and Quality of Life
Seven of the publications reported acute toxicity and nine of the studies reported late morbidities according to the Common Terminology Criteria for Adverse Events (CTCAE) (19, 20, 22, 24, 26, 27, 29, 30, 32, 33). Incidences of grade ≥2 acute GI and GU morbidities ranged from 0–17 to 5–40%, respectively, and late grade ≥2 morbidities ranged from 0–14 to 0–32% for GI and GU morbidities, respectively (Table 3). In one study using the Radiation Therapy Oncology Group (RTOG) toxicity scale, the incidence of grade ≥2 late GI and GU morbidities after 5 years were 0 and 3–30% (25). With few exceptions, there were no significant changes in PROs and QoL endpoints from before to after RT in the seven publications reporting on these items. In one study sexual summary score declined significantly from baseline to 5 years follow-up (67 to 53) in patients not receiving ADT (20) and remained low and stable in patients receiving ADT. Another study revealed a significantly poorer urinary obstruction/irritation score at the end of treatment compared to baseline, but recovering afterwards (27), the same pattern was seen in one of the other publications using EPIC-26 for PROs (31).

Table 3 Acute and late morbidity and patient reported outcomes.
Discussion
The present review provides an overview of the available literature on combined particle therapy and ADT in therapy for PC. It included 15 reports on combined particle therapy and ADT. Across the studies, 48% of the patients received particle therapy in combination with ADT with a higher percentage (87%) of the patients in the high-risk group receiving ADT and with lower frequencies for intermediate- (34%) and low-risk groups (12%). The bDFS of 87–100, 88–95, and 74–88% and OS of for 90–98.4, 90–97, and 87–95.2% at 3–5 years for the low-, intermediate-, and high-risk group in the present review are comparable with outcomes of similar risk groups treated with photons in randomized clinical trials (3, 5, 41–43).
To a large extent, high-risk PC patients received ADT according to international guidelines that recommend long-term ADT (13). The use of ADT in intermediate-risk patients was less compliant to guidelines as only 34% of patients in this risk-group received ADT and the use of ADT in 7% of low-risk patients is not in accordance with guidelines. The reason for the non-compliance may be due to waiting lists, doctors’ or patients’ preferences.
Due to the quality of reporting, heterogeneity of study design, study cohorts, treatments, and dose-fractionation schedules, it was not possible to perform statistical metaanalysis of the effect of ADT on bDSF and OS. Review of the selected studies did not reveal evidence on the efficacy of combining ADT to particle therapy in PC. No randomized study addressed this issue and no study found that ADT was an independent prognostic factor related to survival outcomes. A study by Kasuya et al. on hypofractioned carbon ion therapy for high-risk PC tested the effect of length of ADT and it found no difference in bDSF in patients treated with short- and long-term ADT (23). However, in a previous publication from the same group on an overlapping patient population, long-term ADT resulted in improved bDFS compared to short-term ADT in very-high-risk patients (44). Due to the overlapping study populations, this study was not included in the present review.
The various rates of acute and late morbidity scores between the selected studies reflects the heterogeneous scoring schemes, administration by physicians or patients, patient groups, etc. The lack of detailed reporting of the studies did not allow assessment of the morbidity specifically related to ADT. Previous studies comparing morbidity of particle therapy to intensity modulated radiation therapy (IMRT) in PC patients revealed less GI morbidity in patients treated with particle therapy. The differences in morbidity in these studies were detected by the use of PROs (45, 46). However, in the present review we do not find data to support that ADT interacts with particles on development of radiation damage in a way that differs from photons. It is more likely that the observed toxicities are directly related to the radiation exposure of the organs at risk. However, in particle therapy, ADT may also contribute with specific hormonal related morbidity such as sexual dysfunction, hot flashes, fatigue, osteoporosis, metabolic syndrome, and potentially increased risk of cardiovascular disease (47).
Seven of the studies delivered particle therapy on moderate or ultra-hypofraction schedules. The heterogeneity of the data does not allow analysis of the effect of fractionation on the interaction between particle therapy and ADT. Follow-up in hypofractionated studies was short and does therefore not allow comparison of disease control and survival outcomes and there was no obvious difference in toxicity rates between studies with normo- and hypofraction. In randomized studies on photons, hypofractionation did not result in worse outcome compared to normofractioned RT (41, 42, 48, 49). It has been suggested that ADT is not needed in ultra-hypofractionation of PC. A study by King et al. on SBRT treating localized PC with 36.25 Gy in four to five fractions showed that there was no benefit of short-course ADT (50). In addition, ADT has never proven effective in high dose-rate (HDR) brachytherapy (51). There is so far no data suggesting a similar effect for particle therapy.
The current review has several limitations. The lack of comparative studies in particle therapy together with the heterogeneity of the included studies regarding design, particle therapy dose-fraction, toxicity scoring scales, and use of ADT represent major limitations of the present review. Furthermore, the quality on reporting on the use of ADT in specific risk groups, the duration of treatment, etc. are sparsely reported.
Conclusions
Based on currently available literature, there is no evidence to support different use of ADT in particle therapy compared to standard of care in conventional photon RT of PC. Patients receiving particle therapy for PC should therefore receive ADT according to international guidelines, which implies use of short-term ADT for intermediate-risk and long-term for high-risk PC.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Widmark A, Klepp O, Solberg A, Damber JE, Angelsen A, Fransson P, et al. Endocrine Treatment, With or Without Radiotherapy, in Locally Advanced Prostate Cancer (SPCG-7/SFUO-3): An Open Randomised Phase III Trial. Lancet (2009) 373(9660):301–8. doi: 10.1016/s0140-6736(08)61815-2
3. Bolla M, Van Tienhoven G, Warde P, Dubois JB, Mirimanoff RO, Storme G, et al. External Irradiation With or Without Long-Term Androgen Suppression for Prostate Cancer With High Metastatic Risk: 10-Year Results of an EORTC Randomised Study. Lancet Oncol (2010) 11(11):1066–73. doi: 10.1016/s1470-2045(10)70223-0
4. Bolla M, de Reijke TM, Van Tienhoven G, Van den Bergh AC, Oddens J, Poortmans PM, et al. Duration of Androgen Suppression in the Treatment of Prostate Cancer. N Engl J Med (2009) 360(24):2516–27. doi: 10.1056/NEJMoa0810095
5. Bolla M, Maingon P, Carrie C, Villa S, Kitsios P, Poortmans PM, et al. Short Androgen Suppression and Radiation Dose Escalation for Intermediate- and High-Risk Localized Prostate Cancer: Results of EORTC Trial 22991. J Clin Oncol (2016) 34(15):1748–56. doi: 10.1200/jco.2015.64.8055
6. Zietman AL, DeSilvio ML, Slater JD, Rossi CJ Jr., Miller DW, Adams JA, et al. Comparison of Conventional-Dose vs High-Dose Conformal Radiation Therapy in Clinically Localized Adenocarcinoma of the Prostate: A Randomized Controlled Trial. JAMA (2005) 294(10):1233–9. doi: 10.1001/jama.294.10.1233
7. Pasalic D, Kuban DA, Allen PK, Tang C, Mesko SM, Grant SR, et al. Dose Escalation for Prostate Adenocarcinoma: A Long-Term Update on the Outcomes of a Phase 3, Single Institution Randomized Clinical Trial. Int J Radiat Oncol Biol Phys (2019) 104(4):790–7. doi: 10.1016/j.ijrobp.2019.02.045
8. Beckendorf V, Guerif S, Le Prisé E, Cosset JM, Bougnoux A, Chauvet B, et al. 70 Gy Versus 80 Gy in Localized Prostate Cancer: 5-Year Results of GETUG 06 Randomized Trial. Int J Radiat Oncol Biol Phys (2011) 80(4):1056–63. doi: 10.1016/j.ijrobp.2010.03.049
9. Dearnaley DP, Jovic G, Syndikus I, Khoo V, Cowan RA, Graham JD, et al. Escalated-Dose Versus Control-Dose Conformal Radiotherapy for Prostate Cancer: Long-Term Results From the MRC RT01 Randomised Controlled Trial. Lancet Oncol (2014) 15(4):464–73. doi: 10.1016/s1470-2045(14)70040-3
10. Al-Mamgani A, van Putten WL, Heemsbergen WD, van Leenders GJ, Slot A, Dielwart MF, et al. Update of Dutch Multicenter Dose-Escalation Trial of Radiotherapy for Localized Prostate Cancer. Int J Radiat Oncol Biol Phys (2008) 72(4):980–8. doi: 10.1016/j.ijrobp.2008.02.073
11. Kerkmeijer LGW, Groen VH, Pos FJ, Haustermans K, Monninkhof EM, Smeenk RJ, et al. Focal Boost to the Intraprostatic Tumor in External Beam Radiotherapy for Patients With Localized Prostate Cancer: Results From the FLAME Randomized Phase III Trial. J Clin Oncol (2021) 39(7):787–96. doi: 10.1200/jco.20.02873
12. Zietman AL, Bae K, Slater JD, Shipley WU, Efstathiou JA, Coen JJ, et al. Randomized Trial Comparing Conventional-Dose With High-Dose Conformal Radiation Therapy in Early-Stage Adenocarcinoma of the Prostate: Long-Term Results From Proton Radiation Oncology Group/American College of Radiology 95-09. J Clin Oncol (2010) 28(7):1106–11. doi: 10.1200/JCO.2009.25.8475
13. Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. Eau-Eanm-Estro-Esur-Siog Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment With Curative Intent. Eur Urol (2021) 79(2):243–62. doi: 10.1016/j.eururo.2020.09.042
14. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA Statement For Reporting Systematic Reviews And Meta-Analyses Of Studies That Evaluate Health Care Interventions: Explanation And Elaboration. J Clin Epidemiol (2009) 62(10):e1–34. doi: 10.1016/j.jclinepi.2009.06.006
15. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items For Systematic Reviews And Meta-Analyses: The PRISMA Statement. Ann Intern Med (2009) 151(4):264–9. doi: 10.7326/0003-4819-151-4-200908180-00135
16. Roach M 3rd, Hanks G, Thames H Jr., Schellhammer P, Shipley WU, Sokol GH, et al. Defining Biochemical Failure Following Radiotherapy With or Without Hormonal Therapy in Men With Clinically Localized Prostate Cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys (2006) 65(4):965–74. doi: 10.1016/j.ijrobp.2006.04.029
18. Covidence. Available at: www.covidence.org.
19. Takagi M, Demizu Y, Fujii O, Terashima K, Niwa Y, Daimon T, et al. Proton Therapy for Localized Prostate Cancer: Long-Term Results From a Single-Center Experience. Int J Radiat Oncol Biol Phys (2021) 109(4):964–74. doi: 10.1016/j.ijrobp.2020.11.007
20. Bryant C, Smith TL, Henderson RH, Hoppe BS, Mendenhall WM, Nichols RC, et al. Five-Year Biochemical Results, Toxicity, and Patient-Reported Quality of Life After Delivery of Dose-Escalated Image Guided Proton Therapy for Prostate Cancer. Int J Radiat Oncol Biol Phys (2016) 95(1):422–34. doi: 10.1016/j.ijrobp.2016.02.038
21. Goenka A, Newman NB, Fontanilla H, Cahlon O, Chon B, Tsai H, et al. Patient-Reported Quality of Life After Proton Beam Therapy for Prostate Cancer: The Effect of Prostate Size. Clin Genitourinary Cancer (2017) 15(6):704–10. doi: 10.1016/j.clgc.2017.03.005
22. Habl G, Uhl M, Katayama S, Kessel KA, Hatiboglu G, Hadaschik B, et al. Acute Toxicity and Quality of Life in Patients With Prostate Cancer Treated With Protons or Carbon Ions in a Prospective Randomized Phase II Study - The IPI Trial. Int J Radiat Oncol Biol Phys (2016) 95(1):435–43. doi: 10.1016/j.ijrobp.2016.02.025
23. Kasuya G, Ishikawa H, Tsuji H, Nomiya T, Makishima H, Kamada T, et al. Significant Impact of Biochemical Recurrence on Overall Mortality in Patients With High-Risk Prostate Cancer After Carbon-Ion Radiotherapy Combined With Androgen Deprivation Therapy. Cancer (2016) 122(20):3225–31. doi: 10.1002/cncr.30050
24. Nomiya T, Tsuji H, Maruyama K, Toyama S, Suzuki H, Akakura K, et al. Phase I/II Trial of Definitive Carbon Ion Radiotherapy for Prostate Cancer: Evaluation of Shortening of Treatment Period to 3 Weeks. Br J Cancer (2014) 110(10):2389–95. doi: 10.1038/bjc.2014.191
25. Johansson S, Aström L, Sandin F, Isacsson U, Montelius A, Turesson I. Hypofractionated Proton Boost Combined With External Beam Radiotherapy for Treatment of Localized Prostate Cancer. Prostate Cancer (2012) 2012:654861. doi: 10.1155/2012/654861
26. Grewal AS, Schonewolf C, Min EJ, Chao HH, Both S, Lam S, et al. Four-Year Outcomes From a Prospective Phase II Clinical Trial of Moderately Hypofractionated Proton Therapy for Localized Prostate Cancer. Int J Radiat Oncol Biol Phys (2019) 105(4):713–22. doi: 10.1016/j.ijrobp.2019.05.069
27. Zhang YF, Li P, Yu Q, Wu S, Chen X, Zhang Q, et al. Preliminary Exploration of Clinical Factors Affecting Acute Toxicity and Quality of Life After Carbon Ion Therapy for Prostate Cancer. Radiat Oncol (2019) 14(1):94. doi: 10.1186/s13014-019-1303-3
28. Yu JB, Soulos PR, Herrin J, Cramer LD, Potosky AL, Roberts KB, et al. Proton Versus Intensity-Modulated Radiotherapy for Prostate Cancer: Patterns of Care and Early Toxicity. J Natl Cancer Institute (2013) 105(1):25–32. doi: 10.1093/jnci/djs463
29. Takakusagi Y, Katoh H, Kano K, Anno W, Tsuchida K, Mizoguchi N, et al. Preliminary Result of Carbon-Ion Radiotherapy Using the Spot Scanning Method for Prostate Cancer. Radiat Oncol (2020) 15(1):127. doi: 10.1186/s13014-020-01575-7
30. Mayahara H, Murakami M, Kagawa K, Kawaguchi A, Oda Y, Miyawaki D, et al. Acute Morbidity of Proton Therapy for Prostate Cancer: The Hyogo Ion Beam Medical Center Experience. Int J Radiat Oncol Biol Phys (2007) 69(2):434–43. doi: 10.1016/j.ijrobp.2007.03.009
31. Matsukawa K, Arimura T, Orita M, Kondo H, Chuman I, Ogino T, et al. Health-Related Quality of Life in Japanese Patients With Prostate Cancer Following Proton Beam Therapy: An Institutional Cohort Study. Jpn J Clin Oncol (2020) 50(5):519–27. doi: 10.1093/jjco/hyaa027
32. Dutz A, Agolli L, Baumann M, Troost EGC, Krause M, Hölscher T, et al. Early and Late Side Effects, Dosimetric Parameters and Quality of Life After Proton Beam Therapy and IMRT for Prostate Cancer: A Matched-Pair Analysis. Acta Oncol (2019) 58(6):916–25. doi: 10.1080/0284186X.2019.1581373
33. Iwata H, Ishikawa H, Takagi M, Okimoto T, Murayama S, Akimoto T, et al. Long-Term Outcomes of Proton Therapy for Prostate Cancer in Japan: A Multi-Institutional Survey of the Japanese Radiation Oncology Study Group. Cancer Med (2018) 7(3):677–89. doi: 10.1002/cam4.1350
34. D’Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, Broderick GA, et al. Biochemical Outcome After Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA (1998) 280(11):969–74. doi: 10.1001/jama.280.11.969
35. Cox JD, Stetz J, Pajak TF. Toxicity Criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (Eortc). Int J Radiat Oncol Biol Phys (1995) 31(5):1341–6. doi: 10.1016/0360-3016(95)00060-c
36. Szymanski KM, Wei JT, Dunn RL, Sanda MG. Development and Validation of an Abbreviated Version of the Expanded Prostate Cancer Index Composite Instrument for Measuring Health-Related Quality of Life Among Prostate Cancer Survivors. Urology (2010) 76(5):1245–50. doi: 10.1016/j.urology.2010.01.027
37. Barry MJ, Fowler FJ Jr., O’Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American Urological Association Symptom Index for Benign Prostatic Hyperplasia. The Measurement Committee of the American Urological Association. J Urol (1992) 148(5):1549–57. doi: 10.1016/s0022-5347(17)36966-5
38. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer Qlq-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J Natl Cancer Inst (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
39. van Andel G, Bottomley A, Fosså SD, Efficace F, Coens C, Guerif S, et al. An International Field Study of the EORTC Qlq-PR25: A Questionnaire for Assessing the Health-Related Quality of Life of Patients With Prostate Cancer. Eur J Cancer (2008) 44(16):2418–24. doi: 10.1016/j.ejca.2008.07.030
40. Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The International Index of Erectile Function (IIEF): A Multidimensional Scale for Assessment of Erectile Dysfunction. Urology (1997) 49(6):822–30. doi: 10.1016/s0090-4295(97)00238-0
41. Dearnaley D, Syndikus I, Mossop H, Khoo V, Birtle A, Bloomfield D, et al. Conventional Versus Hypofractionated High-Dose Intensity-Modulated Radiotherapy for Prostate Cancer: 5-Year Outcomes of the Randomised, non-Inferiority, Phase 3 CHHiP Trial. Lancet Oncol (2016) 17(8):1047–60. doi: 10.1016/s1470-2045(16)30102-4
42. Widmark A, Gunnlaugsson A, Beckman L, Thellenberg-Karlsson C, Hoyer M, Lagerlund M, et al. Ultra-Hypofractionated Versus Conventionally Fractionated Radiotherapy for Prostate Cancer: 5-Year Outcomes of the HYPO-RT-PC Randomised, Non-Inferiority, Phase 3 Trial. Lancet (2019) 394(10196):385–95. doi: 10.1016/s0140-6736(19)31131-6
43. Hallemeier CL, Zhang P, Pisansky TM, Hanks GE, McGowan DG, Roach M, et al. 3rd Prostate-Specific Antigen After Neoadjuvant Androgen Suppression in Prostate Cancer Patients Receiving Short-Term Androgen Suppression and External Beam Radiation Therapy: Pooled Analysis of Four Nrg Oncology Radiation Therapy Oncology Group Randomized Clinical Trials. Int J Radiat Oncol Biol Phys (2019) 104(5):1057–65. doi: 10.1016/j.ijrobp.2019.03.049
44. Ishikawa H, Tsuji H, Kamada T, Yanagi T, Mizoe JE, Kanai T, et al. Carbon Ion Radiation Therapy for Prostate Cancer: Results of a Prospective Phase II Study. Radiother Oncol (2006) 81(1):57–64. doi: 10.1016/j.radonc.2006.08.015
45. Hoppe BS, Michalski JM, Mendenhall NP, Morris CG, Henderson RH, Nichols RC, et al. Comparative Effectiveness Study of Patient-Reported Outcomes After Proton Therapy or Intensity-Modulated Radiotherapy for Prostate Cancer. Cancer (2014) 120(7):1076–82. doi: 10.1002/cncr.28536
46. Gray PJ, Paly JJ, Yeap BY, Sanda MG, Sandler HM, Michalski JM, et al. Patient-Reported Outcomes After 3-Dimensional Conformal, Intensity-Modulated, or Proton Beam Radiotherapy for Localized Prostate Cancer. Cancer (2013) 119(9):1729–35. doi: 10.1002/cncr.27956
47. Mohiuddin JJ, Baker BR, Chen RC. Radiotherapy for High-Risk Prostate Cancer. Nat Rev Urol (2015) 12(3):145–54. doi: 10.1038/nrurol.2015.25
48. Lee WR, Dignam JJ, Amin MB, Bruner DW, Low D, Swanson GP, et al. Randomized Phase III Noninferiority Study Comparing Two Radiotherapy Fractionation Schedules in Patients With Low-Risk Prostate Cancer. J Clin Oncol (2016) 34(20):2325–32. doi: 10.1200/jco.2016.67.0448
49. Incrocci L, Wortel RC, Alemayehu WG, Aluwini S, Schimmel E, Krol S, et al. Hypofractionated Versus Conventionally Fractionated Radiotherapy for Patients With Localised Prostate Cancer (HYPRO): Final Efficacy Results From a Randomised, Multicentre, Open-Label, Phase 3 Trial. Lancet Oncol (2016) 17(8):1061–9. doi: 10.1016/s1470-2045(16)30070-5
50. King CR, Freeman D, Kaplan I, Fuller D, Bolzicco G, Collins S, et al. Stereotactic Body Radiotherapy for Localized Prostate Cancer: Pooled Analysis From a Multi-Institutional Consortium of Prospective Phase II Trials. Radiother Oncol (2013) 109(2):217–21. doi: 10.1016/j.radonc.2013.08.030
Keywords: prostate cancer, androgen deprivation therapy, biochemical disease-free survival, overall survival, acute morbidity, late morbidity, proton therapy, carbon ion therapy
Citation: Petersen SE and Høyer M (2021) Androgen Deprivation Therapy Combined With Particle Therapy for Prostate Cancer: A Systematic Review. Front. Oncol. 11:695647. doi: 10.3389/fonc.2021.695647
Received: 15 April 2021; Accepted: 31 May 2021;
Published: 23 June 2021.
Edited by:
Andrea Lancia, Fondazione Ospedale San Matteo (IRCCS), ItalyReviewed by:
Nora Sundahl, Ghent University Hospital, BelgiumCiro Franzese, Humanitas University, Italy
Copyright © 2021 Petersen and Høyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stine Elleberg Petersen, c3RpbnBldGVAcm0uZGs=