
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 26 July 2021
Sec. Cancer Genetics
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.695038
 Eloisa Jantus-Lewintre1*
Eloisa Jantus-Lewintre1* Bartomeu Massutí Sureda2
Bartomeu Massutí Sureda2 José Luis González Larriba3
José Luis González Larriba3 Delvys Rodríguez-Abreu4
Delvys Rodríguez-Abreu4 Oscar Juan5
Oscar Juan5 Ana Blasco6
Ana Blasco6 Manuel Dómine7
Manuel Dómine7 Mariano Provencio Pulla8Javier Garde9
Mariano Provencio Pulla8Javier Garde9 Rosa Álvarez10Inmaculada Maestu11Ramón Pérez de Carrión12Ángel Artal13Christian Rolfo14Javier de Castro15
Rosa Álvarez10Inmaculada Maestu11Ramón Pérez de Carrión12Ángel Artal13Christian Rolfo14Javier de Castro15 Mónica Guillot16Juana Oramas17Ramón de las Peñas18
Mónica Guillot16Juana Oramas17Ramón de las Peñas18 Lioba Ferrera19
Lioba Ferrera19 Natividad Martínez20Òlbia Serra21
Natividad Martínez20Òlbia Serra21 Rafael Rosell22Carlos Camps23* on behalf of Grupo Español de Cáncer de Pulmón (GECP)
Rafael Rosell22Carlos Camps23* on behalf of Grupo Español de Cáncer de Pulmón (GECP)Finding angiogenic prognostic markers in advanced non-small-cell lung cancer is still an unmet medical need. We explored a set of genetic variants in the VEGF-pathway as potential biomarkers to predict clinical outcomes of patients with non-small-cell lung cancer treated with chemotherapy plus bevacizumab. We prospectively analyzed the relationship between VEGF-pathway components with both pathological and prognostic variables in response to chemotherapy plus bevacizumab in 168 patients with non-squamous non-small-cell lung cancer. Circulating levels of VEGF and VEGFR2 and expression of specific endothelial surface markers and single-nucleotide polymorphisms in VEGF-pathway genes were analyzed. The primary clinical endpoint was progression-free survival. Secondary endpoints included overall survival and objective tumor response. VEGFR-1 rs9582036 variants AA/AC were associated with increased progression-free survival (p = 0.012 and p = 0.035, respectively), and with improved overall survival (p = 0.019) with respect to CC allele. Patients with VEGF-A rs3025039 harboring allele TT had also reduced mortality risk (p = 0.049) compared with the CC allele. The VEGF-A rs833061 variant was found to be related with response to treatment, with 61.1% of patients harboring the CC allele achieving partial treatment response. High pre-treatment circulating levels of VEGF-A were associated with shorter progression-free survival (p = 0.036). In conclusion, in this prospective study, genetic variants in VEGFR-1 and VEGF-A and plasma levels of VEGF-A were associated with clinical benefit, progression-free survival, or overall survival in a cohort of advanced non-squamous non-small-cell lung cancer patients receiving chemotherapy plus antiangiogenic therapy.
Lung cancer is one of the most frequent malignancies, and presently the leading cause of cancer-related deaths in Europe (1). Approximately 85% of lung cancer cases are non-small-cell lung cancer (NSCLC), and most NSCLC patients (70%) are diagnosed with advanced-stage disease (i.e., stages IIIB/IV) at presentation (2). A crucial aspect for solid tumor growth is vascularization, and various tumors have been found to produce angiogenic factors themselves or benefit from vascularization induced by inflammatory mediators (3). The major regulator of angiogenesis is vascular endothelial growth factor (VEGF) (4), whose overexpression seems to play a most relevant role in malignant phenotype of solid tumors, including NSCLC (5). Carboplatin-based chemotherapy with bevacizumab has become a standard therapy for eligible NSCLC patients after the results obtained in trials (6–9) and observational studies (10–12). However, careful consideration of the results within the study populations points to the need of determining prognostic markers to select those patients that might achieve greater benefit of treatment with these schemes.
Serum levels of VEGF isoforms and their receptors have been used as prognostic markers and to monitor response to chemotherapy or anti-angiogenic agents (5, 13). In fact, their levels before therapy initiation correlate to prognosis in NSCLC (14–17), but clinical biomarkers and these characteristics alone have been insufficient to predict the course of the disease and response to therapy (16, 17). Variants within VEGF-related genes seem to regulate their transcription (18, 19), and several single-nucleotide polymorphisms (SNPs) have been identified, some of them influencing levels of VEGF isoforms or of their receptors in plasma (18, 20–24). Genotype variants in proteins of the VEGF pathway have been shown to impact patient outcomes, however with inconsistent results (25–32), and SNPs are therefore still subject of study as potential prognostic biomarkers. The possible role as biomarkers in NSCLC has also been widely studied in specific endothelial surface proteins CD31, CD34, CD133, and CD146 (33, 34).
Kristen Rat Sarcoma viral oncogene (KRAS) is a well-known driver of NSCLC for which no targeted therapy has been developed yet. KRAS mutations have been classically defined as a negative prognostic factor in terms of progression-free survival (PFS) and overall survival (OS), but results are heterogenous and the clinical significance remains controversial, also in patients that receive platinum-based chemotherapy (35). However, SNPs in KRAS have been related to relapse-free survival in NSCLC (36) and PFS in colorectal cancer (37), and results suggest further research in their potential as biomarkers in NSCLC.
Therefore, the main objective of this clinical study was to increase insight in the correlation between selected molecular biomarkers in genes coding for VEGF-A, VEGF receptors 1 and 2 (VEGF-R1 and VEGFR-2), and KRAS, circulating levels of angiogenic mediators and expression of endothelial markers, and the clinical response to the combined treatment of carboplatin, paclitaxel, and bevacizumab in advanced NSCLC patients.
The authors present the following article in accordance with the STROBE reporting checklist.
ANGIOMET (NCT01814163) was a case-only observational exploratory, post-authorization study. The study has a prospective and multicenter scheme in advanced NSCLC of non-squamous histology, treated in first line with carboplatin-paclitaxel-bevacizumab conducted between February 2011 and February 2013. It was designed to investigate the relationship between genotypes and circulating levels of selected angiogenic mediators and the clinical outcomes and response to this treatment scheme. Twenty hospitals of the public healthcare system across Spain participated.
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The trial was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The protocol was approved by the Ethics Committee of Hospital General Universitario de Alicante and was accepted by each participating center. All patients provided written consent for inclusion.
Patients aged over 18 years with advanced non-resectable NSCLC, metastatic or recurrent, and not previously treated with chemotherapy were invited to participate if the treating specialist considered the study therapy as the most appropriate. Those with squamous or non-measurable tumors [according to RECIST 1.1 criteria (38)] or in whom peripheral blood samples could not be obtained were excluded. Detailed inclusion and exclusion criteria are provided in the Supplementary Appendix. Recruitment period was 12 months, and the patients were followed for 24 months. These patients received standard therapy of a combination of carboplatin (AUC 6), paclitaxel (200 mg/m2), and bevacizumab (15 mg/kg) every 21 days for a total of six cycles unless there was evidence of disease progression or intolerance to treatment.
Peripheral blood samples were collected before the first chemotherapy cycle and after three treatment cycles in tubes containing EDTA as anticoagulant (BD Vacutainer®, USA) and Blood RNA tubes (PAXgene®, USA). Samples were stored at 4°C until DNA, RNA, or plasma extraction was performed.
Blood samples were sent to a reference laboratory within 24 h of blood collection and subject to RNA or plasma extraction. Two centrifugation steps were performed to obtain plasma (10 min at 1,100 g at room temperature and a second centrifugation of the supernatants for 10 min at 2,000 g at RT to eliminate any possible cell fragments). Plasma aliquots were immediately stored at −80°C until further analysis. Circulating levels of VEGF-A and VEGFR-2 in plasma were assayed as previously described (39); double sandwich ELISA (Duo Set, R&D Systems) was used, in which the lower limit of detection for VEGF-A was 31.2 pg/ml, and 15.6 pg/ml for VEGFR-2.
RNA was isolated using the PreAnalytiX blood RNA kit (Qiagen, Valencia, CA, USA) and quantified by spectrophotometry in a NanoDrop2000c device (ThermoScientific, USA). Retrotranscription was performed with 500 ng of RNA using the High-Capacity cDNA Reverse Transcription Kit (Applied Biosystems, USA). Expression of CD31, CD34, CD133, and CD146 markers was determined by real-time quantitative PCR using primers and probes designed with Taqman® technology (Gene Expression Assays, Applied Biosystems). Expression of target genes was normalized against endogenous expression of a combination of two genes, GAPDH and CDKN1B, as a reference. cDNA sample from a known cell line was used as a calibrator to minimize inter-trial variability.
To analyze differences between baseline and post-treatment samples, the circulating levels of VEGF-A and VEGFR-2 and the expression of endothelial markers (CD31, CD34, CD133, and CD146) were showed as ratios, calculated as the fraction between baseline and post-treatment measurements. Results were dichotomized in “high” and “low.” To evaluate the association with survival times and response to treatment, Chi-square test or Fisher’s Exact test were used as appropriate.
Molecular analysis of 10 SNPs in the genes coding for VEGFR-1, VEGFR-2, VEGF-A, and KRAS was performed by means of real-time PCR. The SNPs analyzed were VEGFR-1 rs7996030, VEGFR-1 rs9582036, VEGF-A rs3025039, VEGF-A rs833061, VEGF-A rs2010963, VEGFR-2 rs2071559, VEGFR-2 rs1870377, KRAS rs10842513, KRAS rs12813551, and KRAS rs10505980. Details and rationale for their inclusion in molecular analysis are provided in the supplementary material (Table S1).
Genomic DNA was extracted from the buffy coat fraction (EDTA tubes) using QIAamp DNA blood Mini Kit (Qiagen, Valencia, CA, USA). Real-time PCR reactions were carried out on 20 ng of DNA using predesigned assays (TaqMan® SNP Genotyping Assay, Applied Biosystems) and master mix containing DNA polymerase, dNTPs, and buffer (TaqMan® genotyping master mix, Applied Biosystems®) in a final volume of 5 µl. A positive and a negative control were included for each SNP analyzed and each reaction plate. All samples were tested in duplicate. The PCR conditions were as follows: 95°C for 1 min, 40 cycles of 95°C for 10 s, 60°C for 1 min. Genotypes were discriminated using probes labeled with FAM and VIC fluorophores in a single multiplex reaction. Fluorescence intensity readings of the probes were measured by the ABI 7900 instrument, and the genotypes were assigned using the SDS 2.4 Software (ABI). All blood samples were centrally analyzed at the Research Institute of Hospital General Universitario de Valencia (Valencia, Spain).
Correlation between angiogenic markers and PFS was the primary clinical endpoint (defined as the time from treatment initiation until disease progression or death, whichever occurred first). OS (defined as the time from diagnosis until death from any cause or last clinical follow-up) at 12 and 24 months and response to treatment (classified using the RECIST 1.1. criteria in complete response, partial response, stable disease, and disease progression) were among the secondary endpoints. The absolute and variable frequencies of the responses according to the treatment are presented through contingency tables.
Sample size was estimated considering feasibility in the 20 participating hospitals, given the recruitment period, and set in 200 patients. Descriptive analysis was performed with all variables, which were summarized as mean and standard deviation (SD), median and interquartile range (IQR), or frequency and proportion as appropriate. OS and PFS curves were plotted according to the Kaplan–Meier method, and differences between groups were assessed using the log-rank test. Association of SNPs, circulating levels of angiogenic mediators, and expression of endothelial markers with PFS and OS was analyzed by means of univariate Cox regression models. Multivariate Cox analysis was performed including all statistically significant variables from the univariate analyses. Clinical response to treatment was evaluated by the Chi-square test or Fisher’s Exact test when appropriate. The tests were analyzed using Stata v16.1. software (College Station, TX: StataCorp LLC). The level of significance was set to a = 0.05.
Of the 201 patients initially included in the study, two of them did not start treatment (consent was withdrawn in one case, and another experienced rapid deterioration); therefore, 199 received the planned combination of carboplatin, paclitaxel, and bevacizumab (CPB). Median age was 62 years (range 54–67), and 139 (70%) were male. Performance status at baseline was ECOG 0 or 1 in the majority (96.2%), and most of them were current smokers or ex-smokers (85.3%). The most frequent histological type was adenocarcinoma (89.1%). Regarding tumor characteristics (Table 1), all patients presented a median of two target lesions of mean size 8.41 ± 5.63 cm, and 91.5% presented also non-target lesions. One hundred and seventy-four patients presented two or more metastases, of which pulmonary lymph nodes (65.2%) and lung metastases (50.2%) were the most common (Table S2).

Table 1 Demographic and clinical characteristics of the study cohort.
One hundred and sixty-eight patients had baseline valid blood samples and complete data for the variables of interest and outcomes analyzed. The median OS for these patients was 14.6 months (range 11.7–16.2) (Figure 1A), and the median PFS was 7.1 months (range 6.1–7.9) (Figure 1B). The OS was 80% at 6 months and 58% at 1 year. Regarding PFS, it was 59% at 6 months, and 18% after 1 year. One patient achieved complete response, 86 achieved partial response (43.2% of the overall sample and 51.2% among those that received at least three cycles), and 20 (10.1%) progressed during initial therapy (Figure 2). All patients were followed up until death, abandonment, or end of study. Of the 199 treated patients, 11 (5.5%) died during initial therapy and 142 (71.3%) during the follow-up period. Adverse events and other safety outcomes are shown in Supplementary Appendix and Tables S3–S5.
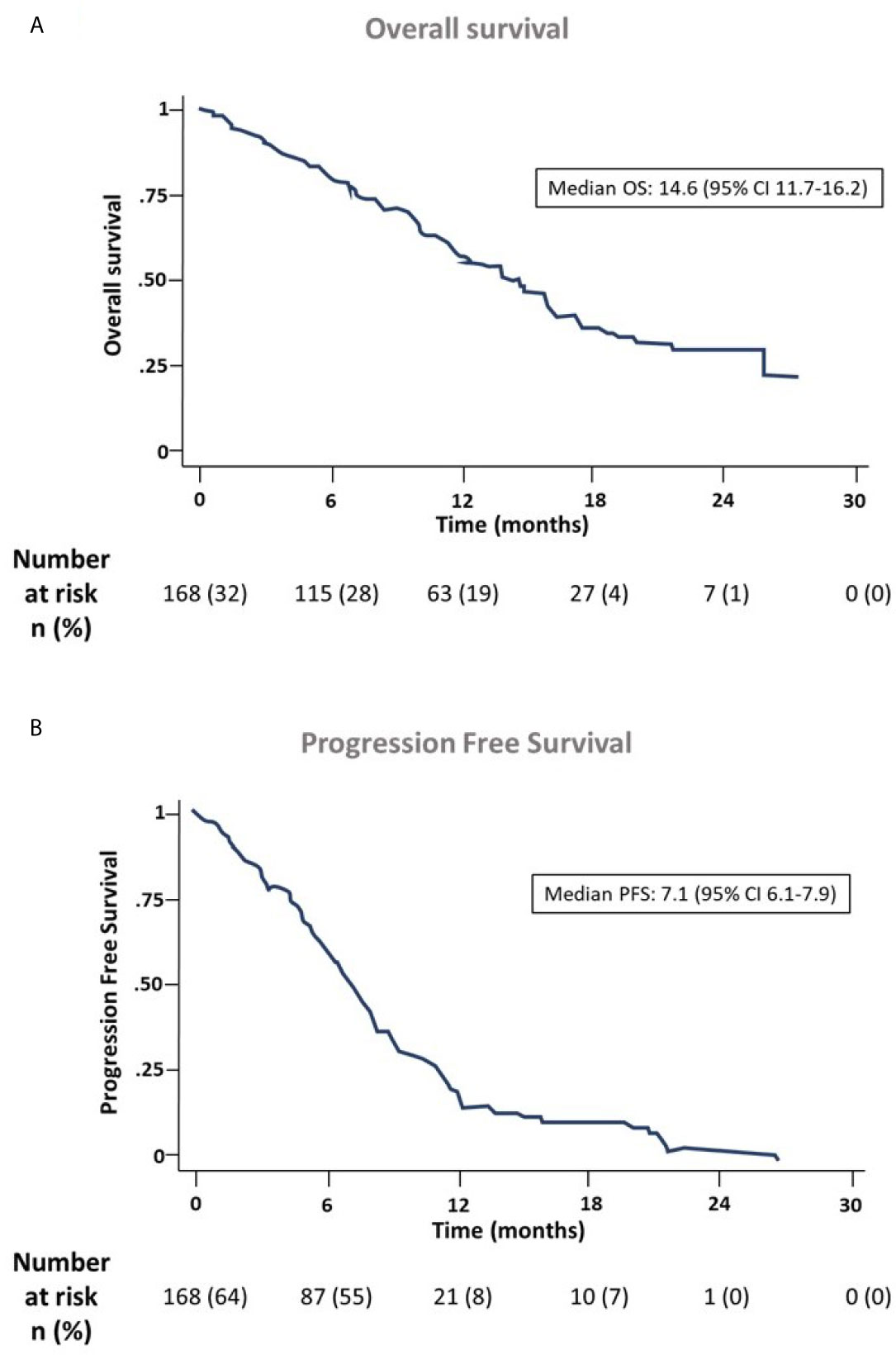
Figure 1 Overall survival (A) and progression-free survival (B) of the ANGIOMET cohort.

Figure 2 Rate of responses to chemotherapy with carboplatin and paclitaxel combined with bevacizumab.
Molecular analysis of genetic variants was performed in DNA samples obtained from peripheral blood, and the frequencies obtained are detailed in Table 2. Table 3 shows the results on the association between SNPs in VEGFA, VEGFR1, VEGFR2, and KRAS genes and treatment response. Among the multiple variants analyzed, only VEGF-A rs833061 was significantly related with a clinical response to CPB (p = 0.036). Patients with the CT genotype had a higher percentage of partial response to treatment compared with patients with CC and TT alleles (61.1 vs. 38.9 and 40.5% respectively).
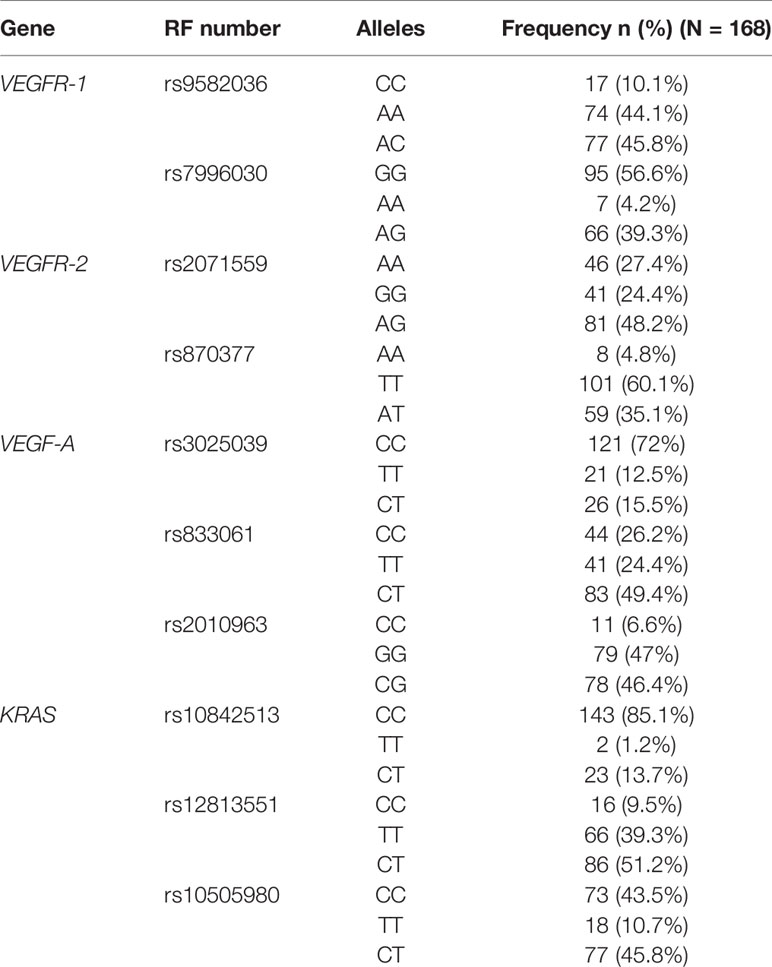
Table 2 Genotype data and SNPs frequency.
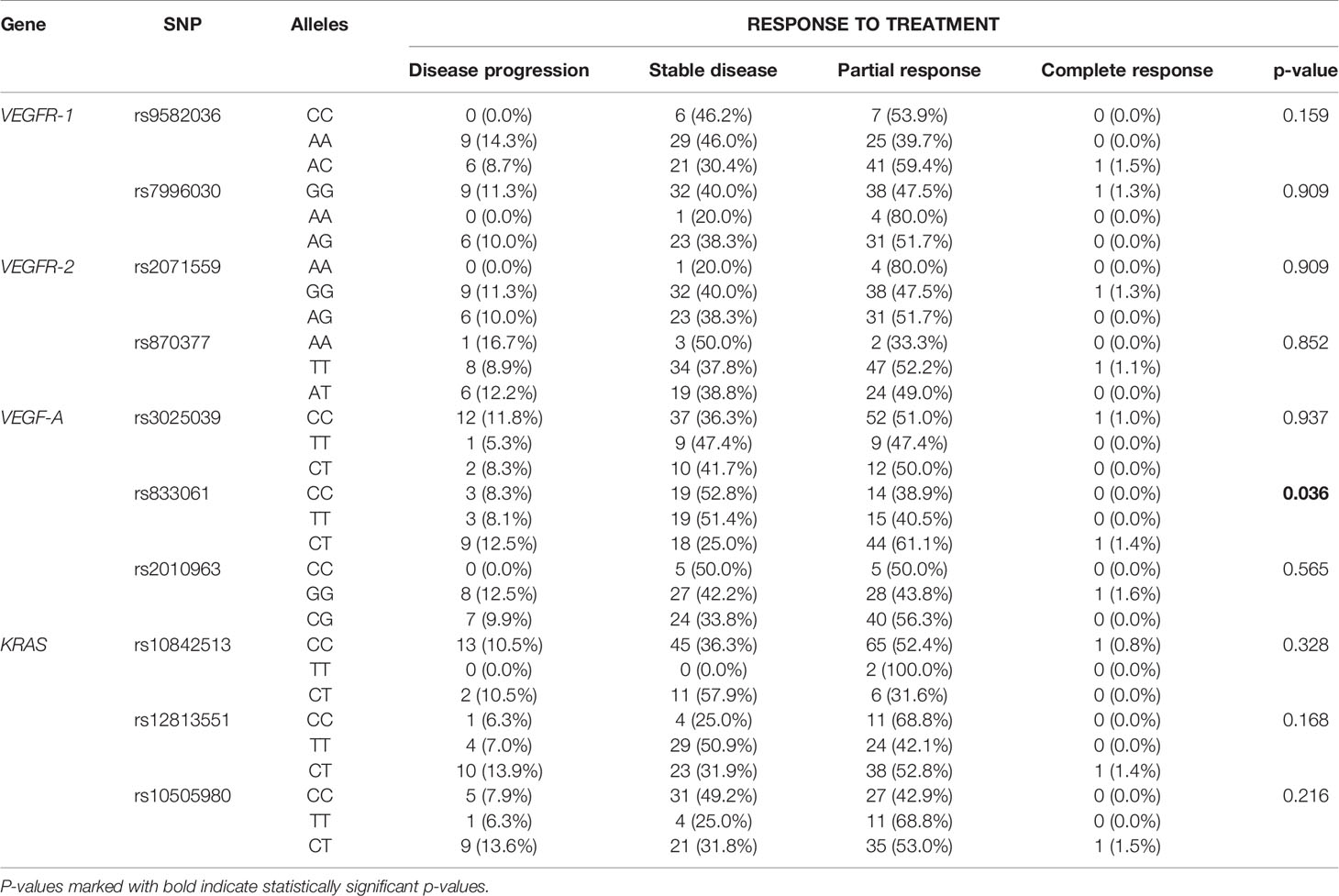
Table 3 Association of SNPs in VEGFA, VEGFR1, VEGFR2, and KRAS genes with response to BCP therapy.
Correlation between analyzed polymorphisms and PFS or OS in our cohort is shown in Table 4. The genetic variant in VEGFR-1 rs9582036 was significantly associated to OS and PFS and VEGF-A rs3025039 was significantly associated to OS (Figure 3). Patients harboring the AA/AC alleles in VEGFR-1 rs9582036 had increased OS compared with those with CC allele, with median OS of 17.4, 13.7 and 10.0 months, respectively. Similarly, patients with the VEGF-A rs3025039 SNPs, TT and CT presented half the risk of death than those patients with the CC allele (HRTT: 0.45, p = 0.049; HRCT: 0.54, p = 0.068). On the other hand, the PFS was significatively increased in patients with VEGFR-1 rs9582036 AA/AC alleles (HRAA: 0.47, p = 0.012; HRAC: 0.54, p = 0.035). No association was found in any of the SNPs studied in KRAS and OS or PFS (Table 4).
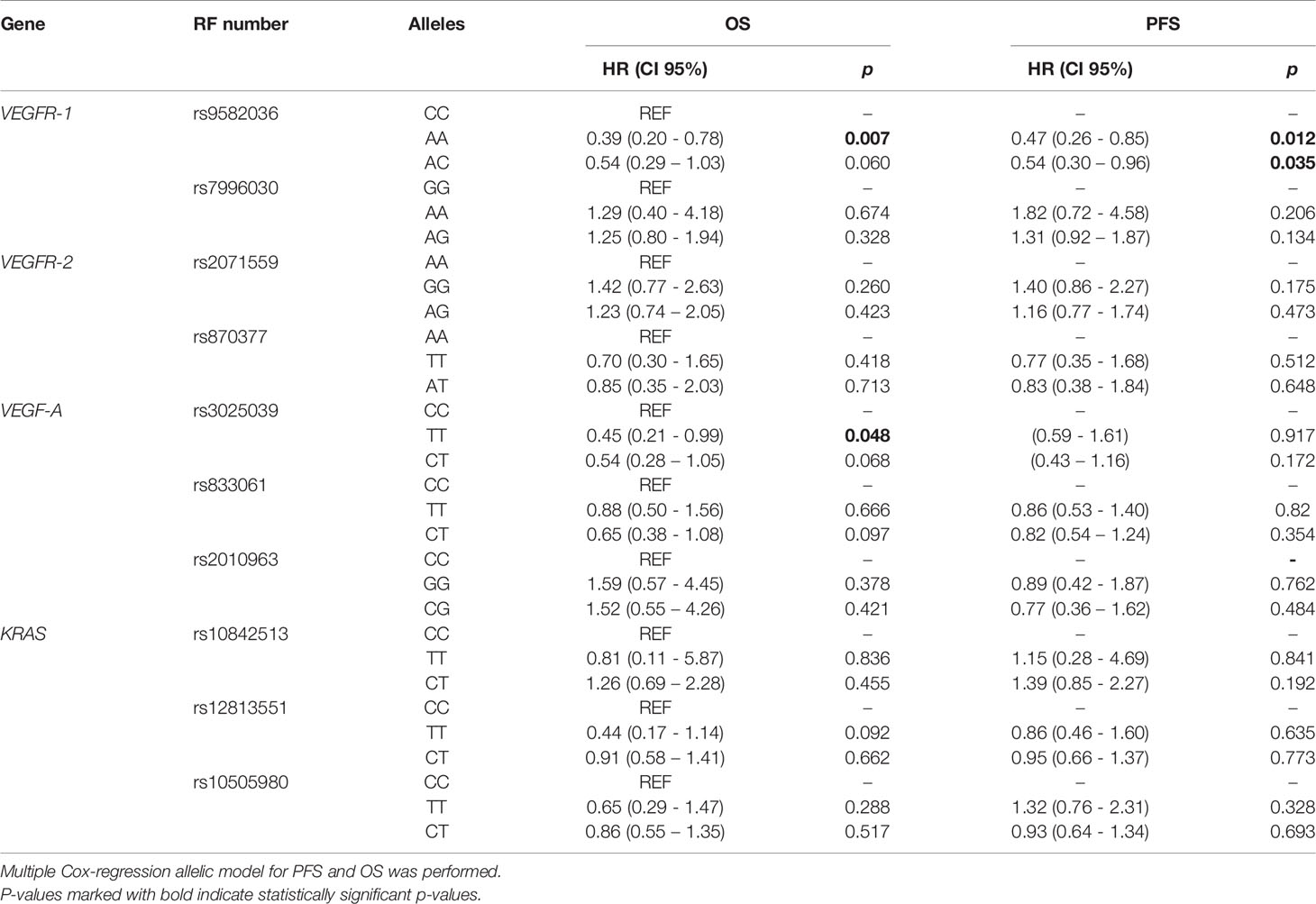
Table 4 Association of SNPs in VEGFA, VEGFR1, VEGFR2, and KRAS genes with OS and PFS.
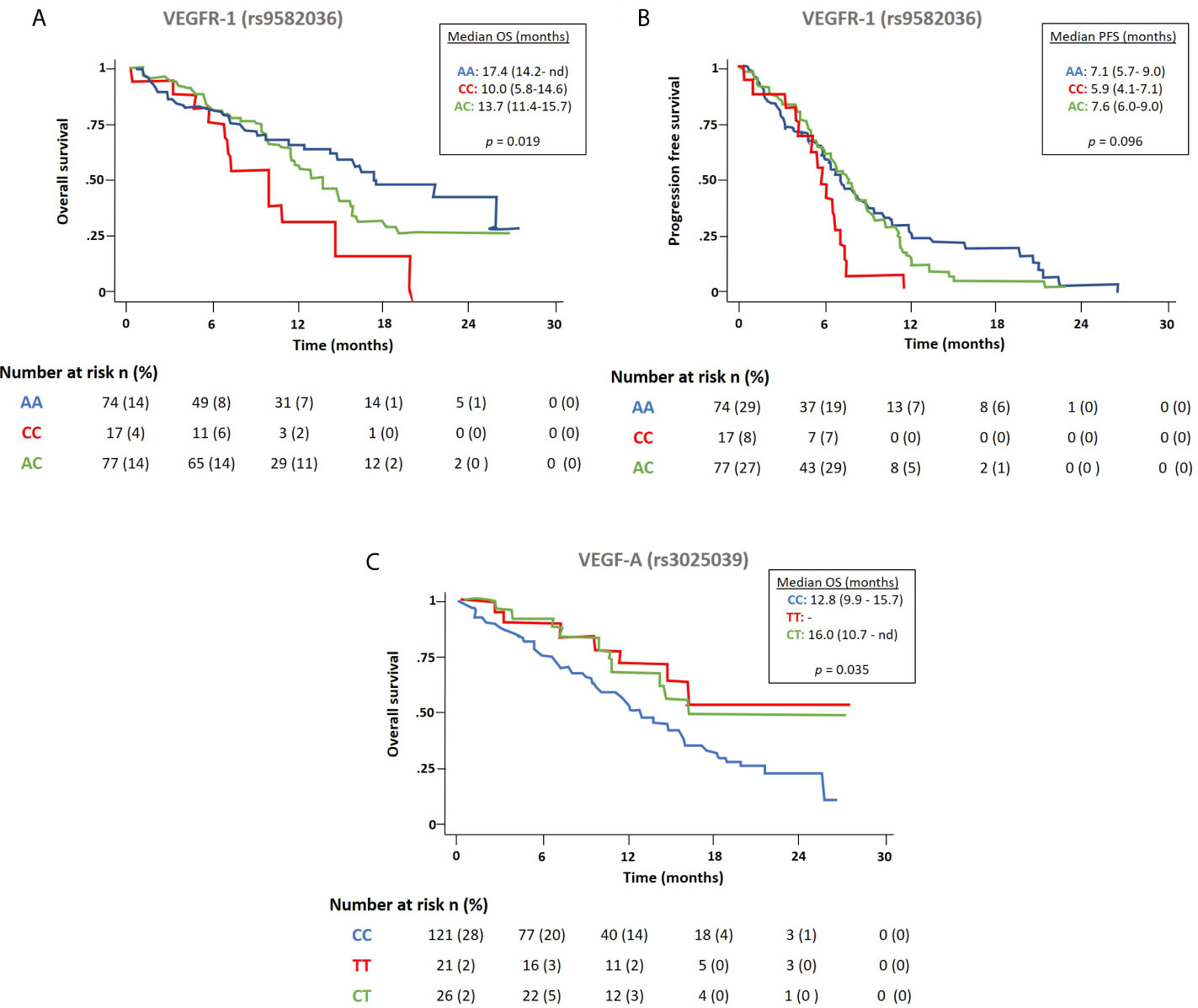
Figure 3 Effect of the polymorphism in VEGFR-1 rs9582036 in estimated OS (A) and PFS (B), and in VEGFA rs3025039 in estimated OS (C).
We evaluated baseline VEGF-A and VEGFR-2 circulating levels as possible biomarkers of clinical outcomes such as PFS, OS, or treatment response to CPB (Table S6). By using the median of each soluble marker as a cutoff, continuous variables were dichotomized as “high” (values above the median) and “low” (values equal or less than the median). Our results showed that patients within the “high” VEGF-A group had significantly shorter PFS [5.9 vs. 8.4 months, p = 0.036] than patients within the “low” VEGF-A group. A similar trend (non-statistically significant) was observed in OS (12.0 vs. 16.0 months, p = 0.095). Survival analysis was performed also for VEGFR-2, and in this case, no significant association was found between basal levels of this biomarker and PFS or OS.
When we analyzed the possible changes in circulating levels of VEGF-A and VEGFR-2 between pre- and post-treatment values (expressed as a ratio and using a cutoff value = 1), we found no significant association with risk of death, progression, or response to treatment either in the group with a ratio below 1 or in the group with a ratio above 1 (data not shown).
No correlations were found between expression levels of CD31, CD34, CD146, or CD133 at baseline, post treatment, or when ratios baseline/post-treatment (cutoff value = median) were analyzed and correlated with PFS, OS, or response to treatment in this study (Table S6 and data not shown).
A multivariate Cox regression model for PFS and OS was built using clinical variables (PS-ECOG, gender, histology, smoking habit) and the analytical variables that were found significant in the univariate analysis. Regarding PFS, this analysis revealed that only the VEGFR-1 rs9582036 and baseline circulating levels of VEGF-A were independent prognostic variables (p = 0.012 and p = 0.042, respectively) in our patient population. Moreover, ECOG-PS, VEGFR-1 rs9582036, and VEGF-A rs3025039 were found as independent markers for OS (p = 0.004, p = 0.018 and p = 0.007, respectively) in our study.
There is a strong unmet need for new biomarkers that can predict clinical responses to various therapies in patients with NSCLC, facilitating a more individualized treatment. During the last years, several studies have evaluated different molecules related to VEGF pathway in relation to clinical outcomes in patients with NSCLC treated with CPB regimen, but until now, there are no validated predictive biomarkers in the clinical setting (40). This prospective study contributes to the body of evidence demonstrating the potential of some biomarkers, including SNPs in angiogenic genes and circulating levels of VEGF, as prognostic factors in NSCLC. Our results show that both VEGFR-1 rs9582036 and VEGF-A rs3025039 were independent prognostic markers for OS. Moreover, shorter PFS correlates with higher baseline plasma levels of VEGF-A and the presence of the CC allele in VEGFR-1 rs9582036. Then, we propose the analysis of variants in VEGFR-1 and VEGF-A as potential biomarkers in patients with NSCLC treated with CPB.
Several studies have linked rs9582036 VEGFR-1 polymorphism and clinical outcomes in bevacizumab-treated patients with different kinds of cancer (36, 41, 42). The CC allele of rs9582036 variant was predictive of shorter survival in pancreatic and colorectal cancer (41, 42). Regarding NSCLC patients, the study performed by Glubb et al. (36) in 2015 showed that AA variants of rs9582036 were associated with longer relapse-free survival independent of the treatment, and were proposed as a prognostic biomarker in stage I-III NSCLC (36). Our results found that the CC rs9582036 allele has a negative predictive effect in patients with advanced NSCLC treated with chemotherapy plus bevacizumab, while the AA and AC variants are associated with an increase in PFS and OS. Taken together, these data suggest that carriers of the CC allele of the VEGFR-1 variant rs9582036 may be less responsive to angiogenesis inhibition having a detrimental effect on survival. However, one should consider that the VEGFR-1 variants found in our study were detected in peripheral blood, while the SNPs reported in the study by Glubb et al. (36) were found in somatic tumor cells. Considering all these pieces of evidence supporting the role of the rs9582036 polymorphism in VEGFR-1 in treatment response and outcome in NSCLC, more studies are needed to understand the molecular mechanism of VEGFR-1 genetic variation in response to VEGF blockage.
Additionally, we found that patients harboring both the TT and CT alleles in rs3025039 VEGF-A had reduced their risk of death by approximately half compared to CC. Again, there is some controversy in the literature regarding the effect of this SNP in lung cancer clinical outcomes. While patients with advance NSCLC treated with chemoradiotherapy showed no significant association with survival (43), a trend toward improved survival was observed in early-stage NSCLC patients treated with surgical resection, in concordance with our findings (30). In line with these results, Chen et al. reported that patients with the TT allele treated with chemotherapy presented lower risk of death from all causes (44).
Only VEGF-A rs833061 polymorphism was found to be significantly associated with response to treatment in our study. Previous reports have already demonstrated a potential role of this particular SNP in the metastatic capacity of many tumors, including NSCLC (26, 30, 45–47). Regarding its impact on the therapeutic efficiency of bevacizumab plus chemotherapy, our analysis showed that more than 60% of the rs833061 CT carriers had a clinical benefit of the treatment. That agrees with the exploratory study performed by Pallaud et al. in 2014 (27), showing increased best overall response to first-line bevacizumab plus chemotherapy treatment in patients harboring this allele. These data provide strong evidence of the predictive value of rs833061 SNP as potential biomarker for response to anti-VEGF therapy.
We also investigated whether expression profiles of circulating VEGF-A and VEGFR-2 could be of clinical interest for finding predictors of clinical outcomes to CPB in NSCLC. We found that high pre-treatment VEGF-A plasma levels were associated with less favorable prognosis, increasing the risk of progression. In recent years, some studies have also explored the usefulness of measuring the levels of angiogenic factors as prognostic or predictive markers in NSCLC (25–28, 30, 31, 36, 48). Sanmartín et al. identified a signature of angiogenic factors related with NSCLC outcome (48). Particularly, patients with high levels of VEGF-A and low expression of VEGF-B and VEGF-D had worse OS and lower relapse-free survival. A metanalysis including 74 studies and 7,631 patients found that VEGF-A overexpression was an independent prognostic factor in early-stage NSCLC (49). Regarding the role of circulating levels of VEGF-A, there are evidences showing an association between higher levels of this angiogenic mediator and worse clinical outcomes in NSCLC (49, 50). All together, these results suggest that high levels of VEGF-A could be associated with negative outcomes in NSCLC. Since VEGF-A is a target of bevacizumab treatment, one possible explanation of the effects of higher concentrations of VEGF-A in peripheral blood is directly related to a lower therapeutic effect of this drug. Evaluation of VEGF levels in lung cancer development and in response to therapy might suppose an important tool to better understand its prognostic impact.
The limitations of this study include its exploratory nature, since the sample size followed the feasibility criteria and is limited. Also, the SNP panel used is limited, and it should be extended in order to test other SNPs, specifically in VEGF-A, that have shown an association with clinical outcomes in other cancers. On the other hand, this is one of the few studies that prospectively evaluated the effect of different angiogenesis biomarkers in liquid biopsies in the NSCLC setting, accurately collecting information and eliminating any recall bias.
The results of this prospective study support previous findings regarding the influence of SNPs on angiogenic VEGF genes, and the circulating levels of VEGF on the clinical outcomes of patients with non-squamous NSCLC receiving antiangiogenic treatment such as bevacizumab. In most cases, consistent results across studies are lacking, warranting further research on the subject before molecular biomarkers can be useful in selecting patients with NSCLC and being included in treatment algorithms for antiangiogenic agents. However, important advances are being made in other cancer types, including breast cancer, in which a recent study has found an association of independent prognostic factors with specific treatments and has weighted them by the outcome category (51).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Hospital General Universitario de Alicante. The patients/participants provided their written informed consent to participate in this study.
Conception and design: CC, BM, JC, and EJ-L. Administrative support: CC, BM, and RR. Provision of study materials or patients: JGL, DR-A, OJ, AB, MD, MP, JG, RÁ, IM, RPC, AA, CR, JC, MG, JO, RP, LF, NM, and ÒS. Collection and assembly of data: EJ-L, JGL, DR-A, OJ, AB, MD, MP, JG, RÁ, IM, RPC, AA, CR, JC, MG, JO, RP, LF, NM, and ÒS. Data analysis and interpretation: EJ-L, CC, BM, and RR. Manuscript writing: all authors. All authors contributed to the article and approved the submitted version.
DR-A declares having received honoraria for lectures and advisory boards from Bristol-Myers-Squibb, Merck Sharp & Dohme, Hoffmann-La Roche, Pierre-Fabre, Novartis, Boehringer, Pfizer, Lilly, and AstraZeneca. OJ declares that he has received payment for advisory services from Boehringer Ingelheim, Bristol-Myers Squibb, Merck Sharp & Dohme, Roche/Genetech, AstraZeneca, Pfizer, Eli Lilly, Abbvie, and Takeda. MP reports having received payments from Bristol-Myers Squibb, AstraZeneca, Takeda, Merck Sharp & Dohme, Hoffmann-La Roche, and Novartis for advisory services. JC received fees for advisory services from Hoffman-La Roche. CR declares having received lecture fees from Merck Sharp & Dohme and AstraZeneca, advisory board payments from Archer, Iceivafa, Merck Sharp & Dohme and Laboratorios Serono, and honoraria for consultancy roles from Mylan and Oncompass.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors thank Drs. Blanca Piedrafita and Vanessa Marfil at Medical Statistics Consulting for medial writing services. RR also wish to acknowledge the support by the Asociación Española Contra el Cáncer (AECC).
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.695038/full#supplementary-material
CPB, Carboplatin, paclitaxel, and bevacizumab; IQR, Interquartile range; KRAS, Kristen Rat Sarcoma viral oncogene; NSCLC, Non-small-cell lung cancer; OS, Overall survival; PFS, Progression-free survival; SD, Standard deviation; SNP, Single-nucleotide polymorphism.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, et al. The IASLC Lung Cancer Staging Project: Proposals for the Revision of the TNM Stage Groupings in the Forthcoming (Seventh) Edition of the TNM Classification of Malignant Tumours. J Thoracic Oncol: Off Publ Int Assoc Study Lung Cancer (2007) 2(8):706–14. doi: 10.1097/JTO.0b013e31812f3c1a
3. Roviello G, Bachelot T, Hudis CA, Curigliano G, Reynolds AR, Petrioli R, et al. The Role of Bevacizumab in Solid Tumours: A Literature Based Meta-Analysis of Randomised Trials. Eur J Cancer (Oxford England: 1990) (2017) 75:245–58. doi: 10.1016/j.ejca.2017.01.026
4. Ferrara N, Gerber HP, LeCouter J. The Biology of VEGF and its Receptors. Nat Med (2003) 9(6):669–76. doi: 10.1038/nm0603-669
5. Bremnes RM, Camps C, Sirera R. Angiogenesis in Non-Small Cell Lung Cancer: The Prognostic Impact of Neoangiogenesis and the Cytokines VEGF and bFGF in Tumours and Blood. Lung Cancer (Amsterdam Netherlands) (2006) 51(2):143–58. doi: 10.1016/j.lungcan.2005.09.005
6. Reck M, von Pawel J, Zatloukal P, Ramlau R, Gorbounova V, Hirsh V, et al. Phase III Trial of Cisplatin Plus Gemcitabine With Either Placebo or Bevacizumab as First-Line Therapy for Nonsquamous Non-Small-Cell Lung Cancer: AVAil. J Clin Oncol: Off J Am Soc Clin Oncol (2009) 27(8):1227–34. doi: 10.1200/JCO.2007.14.5466
7. Reck M, von Pawel J, Zatloukal P, Ramlau R, Gorbounova V, Hirsh V, et al. Overall Survival With Cisplatin-Gemcitabine and Bevacizumab or Placebo as First-Line Therapy for Nonsquamous Non-Small-Cell Lung Cancer: Results From a Randomised Phase III Trial (AVAiL). Ann Oncol: Off J Eur Soc Med Oncol (2010) 21(9):1804–9. doi: 10.1093/annonc/mdq020
8. Zhou C, Wu YL, Chen G, Liu X, Zhu Y, Lu S, et al. BEYOND: A Randomized, Double-Blind, Placebo-Controlled, Multicenter, Phase III Study of First-Line Carboplatin/Paclitaxel Plus Bevacizumab or Placebo in Chinese Patients With Advanced or Recurrent Nonsquamous Non-Small-Cell Lung Cancer. J Clin Oncol: Off J Am Soc Clin Oncol (2015) 33(19):2197–204. doi: 10.1200/JCO.2014.59.4424
9. Soria JC, Mauguen A, Reck M, Sandler AB, Saijo N, Johnson DH, et al. Systematic Review and Meta-Analysis of Randomised, Phase II/III Trials Adding Bevacizumab to Platinum-Based Chemotherapy as First-Line Treatment in Patients With Advanced Non-Small-Cell Lung Cancer. Ann Oncol: Off J Eur Soc Med Oncol (2013) 24(1):20–30. doi: 10.1093/annonc/mds590
10. Lopez-Chavez A, Young T, Fages S, Leon L, Schiller JH, Dowlati A, et al. Bevacizumab Maintenance in Patients With Advanced Non-Small-Cell Lung Cancer, Clinical Patterns, and Outcomes in the Eastern Cooperative Oncology Group 4599 Study: Results of an Exploratory Analysis. J Thoracic Oncol: Off Publ Int Assoc Study Lung Cancer (2012) 7(11):1707–12. doi: 10.1097/JTO.0b013e318265b500
11. Lynch TJ Jr, Spigel DR, Brahmer J, Fischbach N, Garst J, Jahanzeb M, et al. Safety and Effectiveness of Bevacizumab-Containing Treatment for Non–Small-Cell Lung Cancer: Final Results of the ARIES Observational Cohort Study. J Thoracic Oncol (2014) 9(9):1332–9. doi: 10.1097/JTO.0000000000000257
12. Zahn MO, Linck D, Losem C, Gessner C, Metze H, Gaillard VE, et al. AVAiLABLE NIS - AVASTIN(R) in Lung Cancer Treatment in Routine Oncology Practice in Germany. BMC Cancer (2019) 19(1):433. doi: 10.1186/s12885-019-5618-0
13. Brattstrom D, Bergqvist M, Hesselius P, Larsson A, Wagenius G, Brodin O. Serum VEGF and bFGF Adds Prognostic Information in Patients With Normal Platelet Counts When Sampled Before, During and After Treatment for Locally Advanced Non-Small Cell Lung Cancer. Lung Cancer (Amsterdam Netherlands) (2004) 43(1):55–62. doi: 10.1016/j.lungcan.2003.07.007
14. Sanmartin E, Jantus Lewintre E, Sirera R, Miñana M, Navarro A, Cabrera A, et al. Soluble Vascular Endothelial Growth Factor Receptor 2 (VEGFR2): New Biomarker in Advanced Non-Small Cell Lung Cancer (NSCLC)? J Clin Oncol (2009) 27(15S):e22108–e. doi: 10.1200/jco.2009.27.15_suppl.e22108
15. Bocci G, Man S, Green SK, Francia G, Ebos JM, du Manoir JM, et al. Increased Plasma Vascular Endothelial Growth Factor (VEGF) as a Surrogate Marker for Optimal Therapeutic Dosing of VEGF Receptor-2 Monoclonal Antibodies. Cancer Res (2004) 64(18):6616–25. doi: 10.1158/0008-5472.CAN-04-0401
16. Zhan P, Wang J, Lv XJ, Wang Q, Qiu LX, Lin XQ, et al. Prognostic Value of Vascular Endothelial Growth Factor Expression in Patients With Lung Cancer: A Systematic Review With Meta-Analysis. J Thoracic Oncol: Off Publ Int Assoc Study Lung Cancer (2009) 4(9):1094–103. doi: 10.1097/JTO.0b013e3181a97e31
17. Mok T, Gorbunova V, Juhasz E, Szima B, Burdaeva O, Orlov S, et al. A Correlative Biomarker Analysis of the Combination of Bevacizumab and Carboplatin-Based Chemotherapy for Advanced Nonsquamous Non–Small-Cell Lung Cancer: Results of the Phase II Randomized ABIGAIL Study (Bo21015). J Thoracic Oncol (2014) 9(6):848–55. doi: 10.1097/JTO.0000000000000160
18. Stevens A, Soden J, Brenchley PE, Ralph S, Ray DW. Haplotype Analysis of the Polymorphic Human Vascular Endothelial Growth Factor Gene Promoter. Cancer Res (2003) 63(4):812–6.
19. Koukourakis MI, Papazoglou D, Giatromanolaki A, Bougioukas G, Maltezos E, Sivridis E. VEGF Gene Sequence Variation Defines VEGF Gene Expression Status and Angiogenic Activity in Non-Small Cell Lung Cancer. Lung Cancer (Amsterdam Netherlands) (2004) 46(3):293–8. doi: 10.1016/j.lungcan.2004.04.037
20. Bieniasz M, Oszajca K, Eusebio M, Kordiak J, Bartkowiak J, Szemraj J. The Positive Correlation Between Gene Expression of the Two Angiogenic Factors: VEGF and BMP-2 in Lung Cancer Patients. Lung Cancer (Amsterdam Netherlands) (2009) 66(3):319–26. doi: 10.1016/j.lungcan.2009.02.020
21. Zhai R, Liu G, Asomaning K, Su L, Kulke MH, Heist RS, et al. Genetic Polymorphisms of VEGF, Interactions With Cigarette Smoking Exposure and Esophageal Adenocarcinoma Risk. Carcinogenesis (2008) 29(12):2330–4. doi: 10.1093/carcin/bgn210
22. Zhai R, Gong MN, Zhou W, Thompson TB, Kraft P, Su L, et al. Genotypes and Haplotypes of the VEGF Gene Are Associated With Higher Mortality and Lower VEGF Plasma Levels in Patients With ARDS. Thorax (2007) 62(8):718–22. doi: 10.1136/thx.2006.069393
23. Renner W, Kotschan S, Hoffmann C, Obermayer-Pietsch B, Pilger E. A Common 936 C/T Mutation in the Gene for Vascular Endothelial Growth Factor Is Associated With Vascular Endothelial Growth Factor Plasma Levels. J Vasc Res (2000) 37(6):443–8. doi: 10.1159/000054076
24. Watson CJ, Webb NJ, Bottomley MJ, Brenchley PE. Identification of Polymorphisms Within the Vascular Endothelial Growth Factor (VEGF) Gene: Correlation With Variation in VEGF Protein Production. Cytokine (2000) 12(8):1232–5. doi: 10.1006/cyto.2000.0692
25. Glubb DM, Cerri E, Giese A, Zhang W, Mirza O, Thompson EE, et al. Novel Functional Germline Variants in the VEGF Receptor 2 Gene and Their Effect on Gene Expression and Microvessel Density in Lung Cancer. Clin Cancer Res: Off J Am Assoc Cancer Res (2011) 17(16):5257–67. doi: 10.1158/1078-0432.CCR-11-0379
26. Maeda A, Nakata M, Yasuda K, Yukawa T, Saisho S, Okita R, et al. Influence of Vascular Endothelial Growth Factor Single Nucleotide Polymorphisms on Non-Small Cell Lung Cancer Tumor Angiogenesis. Oncol Rep (2013) 29(1):39–44. doi: 10.3892/or.2012.2075
27. Pallaud C, Reck M, Juhasz E, Szima B, Yu CJ, Burdaeva O, et al. Clinical Genotyping and Efficacy Outcomes: Exploratory Biomarker Data From the Phase II ABIGAIL Study of First-Line Bevacizumab Plus Chemotherapy in Non-Squamous Non-Small-Cell Lung Cancer. Lung Cancer (Amsterdam Netherlands) (2014) 86(1):67–72. doi: 10.1016/j.lungcan.2014.07.019
28. Sullivan I, Riera P, Andres M, Altes A, Majem M, Blanco R, et al. Prognostic Effect of VEGF Gene Variants in Metastatic Non-Small-Cell Lung Cancer Patients. Angiogenesis (2019) 22(3):433–40. doi: 10.1007/s10456-019-09668-y
29. Eng L, Liu G. VEGF Pathway Polymorphisms as Prognostic and Pharmacogenetic Factors in Cancer: A 2013 Update. Pharmacogenomics (2013) 14(13):1659–67. doi: 10.2217/pgs.13.165
30. Masago K, Fujita S, Kim YH, Hatachi Y, Fukuhara A, Nagai H, et al. Effect of Vascular Endothelial Growth Factor Polymorphisms on Survival in Advanced-Stage Non-Small-Cell Lung Cancer. Cancer Sci (2009) 100(10):1917–22. doi: 10.1111/j.1349-7006.2009.01253.x
31. Dong J, Dai J, Shu Y, Pan S, Xu L, Chen W, et al. Polymorphisms in EGFR and VEGF Contribute to Non-Small-Cell Lung Cancer Survival in a Chinese Population. Carcinogenesis (2010) 31(6):1080–6. doi: 10.1093/carcin/bgq079
32. de Mello RA, Ferreira M, Soares-Pires F, Costa S, Cunha J, Oliveira P, et al. The Impact of Polymorphic Variations in the 5p15, 6p12, 6p21 and 15q25 Loci on the Risk and Prognosis of Portuguese Patients With Non-Small Cell Lung Cancer. PloS One (2013) 8(9):e72373. doi: 10.1371/journal.pone.0072373
33. Duda DG, Cohen KS, di Tomaso E, Au P, Klein RJ, Scadden DT, et al. Differential CD146 Expression on Circulating Versus Tissue Endothelial Cells in Rectal Cancer Patients: Implications for Circulating Endothelial and Progenitor Cells as Biomarkers for Antiangiogenic Therapy. J Clin Oncol: Off J Am Soc Clin Oncol (2006) 24(9):1449–53. doi: 10.1200/JCO.2005.04.2861
34. Hager G, Holnthoner W, Wolbank S, Husa AM, Godthardt K, Redl H, et al. Three Specific Antigens to Isolate Endothelial Progenitor Cells From Human Liposuction Material. Cytotherapy (2013) 15(11):1426–35. doi: 10.1016/j.jcyt.2013.06.018
35. Román M, Baraibar I, López I, Nadal E, Rolfo C, Vicent S, et al. KRAS Oncogene in Non-Small Cell Lung Cancer: Clinical Perspectives on the Treatment of an Old Target. Mol Cancer (2018) 17(1):33–. doi: 10.1186/s12943-018-0789-x
36. Glubb DM, Pare-Brunet L, Jantus-Lewintre E, Jiang C, Crona D, Etheridge AS, et al. Functional FLT1 Genetic Variation Is a Prognostic Factor for Recurrence in Stage I-III Non-Small-Cell Lung Cancer. J Thoracic Oncol: Off Publ Int Assoc Study Lung Cancer (2015) 10(7):1067–75. doi: 10.1097/JTO.0000000000000549
37. Pare-Brunet L, Sebio A, Salazar J, Berenguer-Llergo A, Rio E, Barnadas A, et al. Genetic Variations in the VEGF Pathway as Prognostic Factors in Metastatic Colorectal Cancer Patients Treated With Oxaliplatin-Based Chemotherapy. Pharmacogenom J (2015) 15(5):397–404. doi: 10.1038/tpj.2015.1
38. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur J Cancer (Oxford England: 1990) (2009) 45(2):228–47. doi: 10.1016/j.ejca.2008.10.026
39. Jantus-Lewintre E, Sanmartin E, Sirera R, Blasco A, Sanchez JJ, Taron M, et al. Combined VEGF-A and VEGFR-2 Concentrations in Plasma: Diagnostic and Prognostic Implications in Patients With Advanced NSCLC. Lung Cancer (Amsterdam Netherlands) (2011) 74(2):326–31. doi: 10.1016/j.lungcan.2011.02.016
40. Olaussen KA, Postel-Vinay S. Predictors of Chemotherapy Efficacy in Non-Small-Cell Lung Cancer: A Challenging Landscape. Ann Oncol: Off J Eur Soc Med Oncol (2016) 27(11):2004–16. doi: 10.1093/annonc/mdw321
41. Lambrechts D, Claes B, Delmar P, Reumers J, Mazzone M, Yesilyurt BT, et al. VEGF Pathway Genetic Variants as Biomarkers of Treatment Outcome With Bevacizumab: An Analysis of Data From the AViTA and AVOREN Randomised Trials. Lancet Oncol (2012) 13(7):724–33. doi: 10.1016/S1470-2045(12)70231-0
42. Hansen TF, Christensen R, Andersen RF, Garm Spindler KL, Johnsson A, Jakobsen A. The Predictive Value of Single Nucleotide Polymorphisms in the VEGF System to the Efficacy of First-Line Treatment With Bevacizumab Plus Chemotherapy in Patients With Metastatic Colorectal Cancer: Results From the Nordic ACT Trial. Int J Colorectal Dis (2012) 27(6):715–20. doi: 10.1007/s00384-011-1382-6
43. Guan X, Yin M, Wei Q, Zhao H, Liu Z, Wang LE, et al. Genotypes and Haplotypes of the VEGF Gene and Survival in Locally Advanced Non-Small Cell Lung Cancer Patients Treated With Chemoradiotherapy. BMC Cancer (2010) 10:431. doi: 10.1186/1471-2407-10-431
44. Chen N, Ma CN, Zhao M, Zhang YJ. Role of VEGF Gene Polymorphisms in the Clinical Outcome of Non-Small Cell Lung Cancer. Genet Mol Res (2015) 14(4):16006–11. doi: 10.4238/2015.December.7.13
45. Bayhan Z, Simsek T, Ergul E, Utkan NZ, Canturk NZ, Cekmen M. Serum Cytokine Levels in Patients With Colorectal Cancers According to Tumor Stages and VEGF Gene Polymorphism. Hepatogastroenterology (2014) 61(135):1889–94.
46. Cui W, Li F, Yuan Q, Chen G, Chen C, Yu B. Role of VEGFA Gene Polymorphisms in Colorectal Cancer Patients Who Treated With Bevacizumab. Oncotarget (2017) 8(62):105472–8. doi: 10.18632/oncotarget.22295
47. Jacobs EJ, Feigelson HS, Bain EB, Brady KA, Rodriguez C, Stevens VL, et al. Polymorphisms in the Vascular Endothelial Growth Factor Gene and Breast Cancer in the Cancer Prevention Study II Cohort. Breast Cancer Res (2006) 8(2):R22. doi: 10.1186/bcr1400
48. Sanmartin E, Sirera R, Uso M, Blasco A, Gallach S, Figueroa S, et al. A Gene Signature Combining the Tissue Expression of Three Angiogenic Factors Is a Prognostic Marker in Early-Stage Non-Small Cell Lung Cancer. Ann Surg Oncol (2014) 21(2):612–20. doi: 10.1245/s10434-013-3330-x
49. Zheng CL, Qiu C, Shen MX, Qu X, Zhang TH, Zhang JH, et al. Prognostic Impact of Elevation of Vascular Endothelial Growth Factor Family Expression in Patients With Non-Small Cell Lung Cancer: An Updated Meta-Analysis. Asian Pac J Cancer Prev (2015) 16(5):1881–95. doi: 10.7314/APJCP.2015.16.5.1881
50. Qin S, Yi M, Jiao D, Li A, Wu K. Distinct Roles of VEGFA and ANGPT2 in Lung Adenocarcinoma and Squamous Cell Carcinoma. J Cancer (2020) 11(1):153–67. doi: 10.7150/jca.34693
Keywords: liquid biopsy, biomarkers, NSCLC, angiogenesis, VEGF
Citation: Jantus-Lewintre E, Massutí Sureda B, González Larriba JL, Rodríguez-Abreu D, Juan O, Blasco A, Dómine M, Provencio Pulla M, Garde J, Álvarez R, Maestu I, Pérez de Carrión R, Artal Á, Rolfo C, de Castro J, Guillot M, Oramas J, de las Peñas R, Ferrera L, Martínez N, Serra Ò, Rosell R and Camps C (2021) Prospective Exploratory Analysis of Angiogenic Biomarkers in Peripheral Blood in Advanced NSCLC Patients Treated With Bevacizumab Plus Chemotherapy: The ANGIOMET Study. Front. Oncol. 11:695038. doi: 10.3389/fonc.2021.695038
Received: 14 April 2021; Accepted: 21 June 2021;
Published: 26 July 2021.
Edited by:
Tzu Pin Lu, National Taiwan University, TaiwanReviewed by:
Sherry Yang, National Cancer Institute, (NIH), United StatesCopyright © 2021 Jantus-Lewintre, Massutí Sureda, González Larriba, Rodríguez-Abreu, Juan, Blasco, Dómine, Provencio Pulla, Garde, Álvarez, Maestu, Pérez de Carrión, Artal, Rolfo, de Castro, Guillot, Oramas, de las Peñas, Ferrera, Martínez, Serra, Rosell and Camps. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eloisa Jantus-Lewintre, amFudHVzX2Vsb0BndmEuZXM=; Carlos Camps, Y2FtcHNfY2FyQGd2YS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.