
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 07 July 2021
Sec. Cancer Epidemiology and Prevention
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.690390
This article is part of the Research TopicDisparities in Cancer Prevention and EpidemiologyView all 15 articles
 Michael S. Simon1,2*†
Michael S. Simon1,2*† Sreejata Raychaudhuri3†
Sreejata Raychaudhuri3† Lauren M. Hamel1,2Louis A. Penner1,2Kendra L. Schwartz2,4Felicity W. K. Harper1,2Hayley S. Thompson1,2Jason C. Booza4,5
Lauren M. Hamel1,2Louis A. Penner1,2Kendra L. Schwartz2,4Felicity W. K. Harper1,2Hayley S. Thompson1,2Jason C. Booza4,5 Michele Cote1,2Ann G. Schwartz1,2
Michele Cote1,2Ann G. Schwartz1,2 Susan Eggly1,2
Susan Eggly1,2Racial disparities in cancer incidence and outcomes are well-documented in the US, with Black people having higher incidence rates and worse outcomes than White people. In this review, we present a summary of almost 30 years of research conducted by investigators at the Karmanos Cancer Institute’s (KCI’s) Population Studies and Disparities Research (PSDR) Program focusing on Black-White disparities in cancer incidence, care, and outcomes. The studies in the review focus on individuals diagnosed with cancer from the Detroit Metropolitan area, but also includes individuals included in national databases. Using an organizational framework of three generations of studies on racial disparities, this review describes racial disparities by primary cancer site, disparities associated with the presence or absence of comorbid medical conditions, disparities in treatment, and disparities in physician-patient communication, all of which contribute to poorer outcomes for Black cancer patients. While socio-demographic and clinical differences account for some of the noted disparities, further work is needed to unravel the influence of systemic effects of racism against Black people, which is argued to be the major contributor to disparate outcomes between Black and White patients with cancer. This review highlights evidence-based strategies that have the potential to help mitigate disparities, improve care for vulnerable populations, and build an equitable healthcare system. Lessons learned can also inform a more equitable response to other health conditions and crises.
An understanding of race-related factors underlying and maintaining health disparate outcomes is essential for developing interventions and initiatives that could reduce current inequalities in cancer care. Knowledge gained from research on racial health disparities can also help to eradicate disparities in the future.
In the United States, there are significant racial disparities in cancer incidence and outcomes with higher incidence rates and worse outcomes occurring in Black compared to White populations across multiple primary cancer sites (1). Evidence suggests that these disparities result in large measure from inequitable social, economic, political, behavioral, and psychological processes, which disproportionately negatively impact outcomes among Black individuals with cancer (2). Numerous studies have evaluated the extent to which levels of socioeconomic status (SES), access to care, cancer treatment, and clinical communication contribute to racial health and healthcare disparities (3). While multiple causal pathways might explain in part why Black cancer patients have worse outcomes than their White counterparts, the major underlying force is arguably the legacy of various forms of racism against Black people in the US (4).
Systemic racism in the US began with the legal enslavement primarily of people from Africa and has pervaded medical practice over the last 300 years. Examples of racism in the US medical system range from unethical experimentation on coerced Black people to institutional practices in medical care that either exclude Black people entirely or systematically provide them with poorer treatment than White people (5–10). In an effort to understand and address Black-White health disparities, researchers in the Karmanos Cancer Institute’s (KCI’s) Population Studies and Disparities Research (PSDR) Program have conducted research over the past 30 years ranging from descriptive to evaluative and interventional. Our efforts to explore and better understand racial disparities in cancer incidence, care, and outcomes, along with efforts of our collaborators, are particularly relevant to our institution given our location in Detroit Michigan, a city with a majority of Black people.
In 2019, it was estimated that 69.6% of Michigan’s 1,350,329 non-Hispanic Black population resided within the tri-county Detroit area with the largest proportion of the population (N=518,305) living in the city of Detroit, and the remainder (N=421,799) living in the suburban environs surrounding Detroit. According to Surveillance Epidemiology and End Results (SEER) data, between 2013 and 2017, Black compared with White individuals in Detroit had a disproportionate share of the burden of cancer, with incidence and death rates per 100,000 of 491.92 vs 489.01 and 195.25 vs 164.68 respectively (11). Our research on disparities has largely focused on populations in Detroit and the surrounding tri-county area. Further, given that KCI is one of the founding sites of the National Cancer Institute’s SEER program, many of our studies and those of our collaborators include populations outside of the Detroit area.
In this review, we present a selection of research studies published on cancer disparities conducted by investigators in the KCI’s PSDR program together with collaborators from several different institutions. After a thorough PubMed search of publications by PSDR investigators on racial disparities, we selected studies which focused on Black-White disparities in clinical presentation at diagnosis, treatment, and outcomes, as well as those that evaluated interventions designed to reduce or eliminate Black-White disparities. Given the critical juncture in race relations and health care equity in the US, the goal of this review is to summarize and critique published research and to provide a framework to shape future research that can lead to elimination of health disparities.
The sections of the review generally follow the framework of Thomas et al. (12), which describes three generations of cancer disparities research ranging from descriptive, to analytical and interventional. First generation studies are those that both identify and document the existence of health disparities. Second-generation studies are analytic or evaluative, and attempt to assess variables that could potentially explain the noted disparities. Lastly, third generation studies have the goal of testing interventions that could serve as solutions to mitigate disparate outcomes. While the order of this review generally follows this overall framework, many of the studies cited span both first and second generations, and the section focused on physician-patient communication includes studies spanning all three generations of disparities research. We will conclude with a discussion of fourth generation research, the goal of which is to ultimately take action to eliminate disparities.
Table 1 lists studies by PSDR investigators and their collaborators that identify and document disparities stratified by primary cancer type and show first-generation evidence that Black patients as compared with White patients present with more advanced and aggressive disease at diagnosis across cancer sites evaluated. In a survival analysis of 10,502 women with breast cancer using data from the Detroit Metropolitan Area (DMA)-SEER database, Black women were more likely to present with regional or distant stage disease (44.5%) compared to White women (36.5%) (p <0.00001) (13). In another analysis of 1,700 women with early-stage breast cancer, using data from the Detroit and Los Angeles SEER registries, 16.1% of patients with stage 0 + 1 disease were Black and 75% were White, compared to stage II + III disease where 21.2% were Black and 62.4% were White (14). Similar results were reported for other primary cancer sites including a Detroit Metropolitan Area–SEER analysis of colorectal cancer (CRC) (15) and a study of young-onset CRC identified at 18-SEER sites, which showed that Black compared to White patients were less likely to be diagnosed with early-stage disease (16).
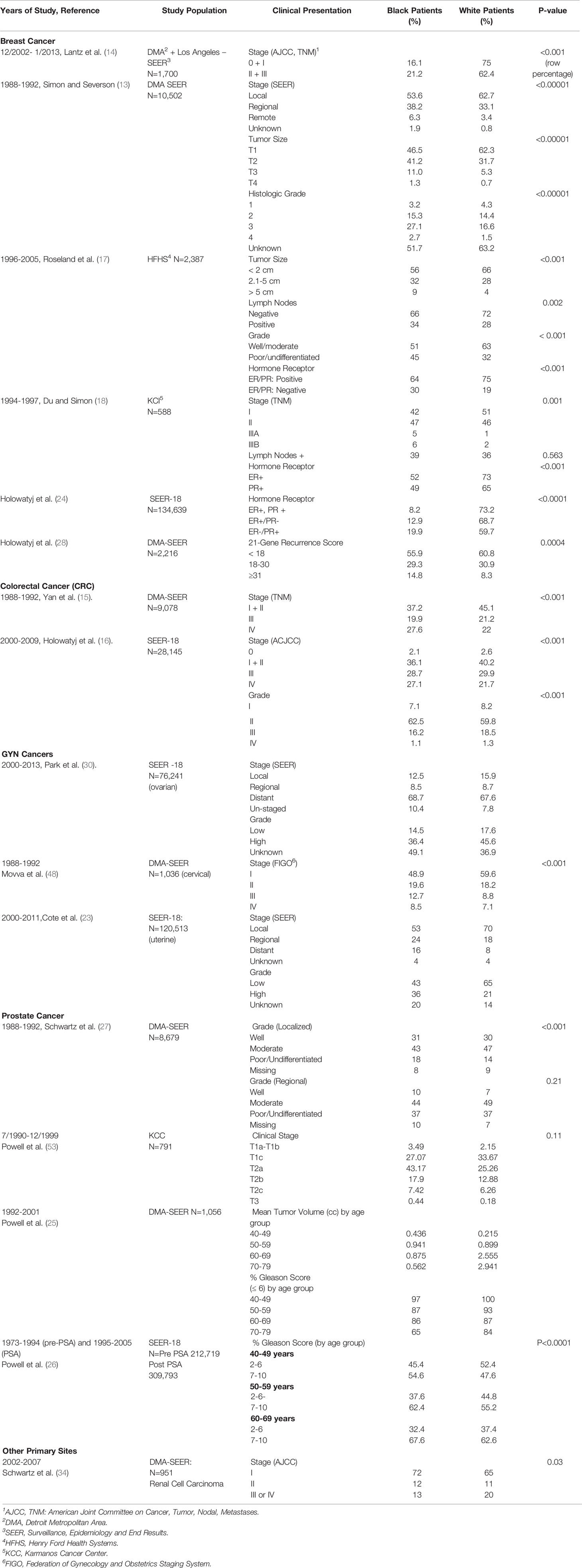
Table 1 First-Generation Evidence of Black-White Disparities at Diagnosis.
Data from single institutions in the Detroit Metropolitan area also showed disparities in stage at diagnosis. Together with their collaborators, researchers from the PSDR conducted studies using data from Henry Ford Health System (HFHS), a large integrated health center in Detroit, and the Karmanos Cancer Center (KCC), one of 54 National Cancer Institute designated Comprehensive Cancer Centers in the US.
In a study of Black-White differences in breast cancer survival among women diagnosed and treated at HFHS, the distribution of tumor size by race demonstrated that 66% of White women had tumors ≤ 2cm and 4% had tumors > 5 cm; however, the tumor size distribution for Black women was 56% and 9% respectively (p< 0.001) (17). Using data from the KCI, PSDR investigators demonstrated that Black women were also more likely to present with advanced disease at diagnosis (18).
Other first-generation evidence includes studies that describe Black-White disparities in tumor phenotypic characteristics in both SEER-based and single institution studies. Black compared to White cancer patients across multiple tumor types were more likely to present with higher-grade, and more aggressive disease (16, 19–22), and among individuals with endometrial cancer, Black patients were more likely to present with histologic subtypes associated with worse outcomes (20–23). In three hospital-based studies, Black women were more likely to present with triple-negative breast cancer (17, 18, 24), and in studies of prostate cancer, Black men were more likely to present with aggressive disease associated with higher Gleason grade and greater prostate gland volume (25–27). Similar patterns were seen in a study evaluating tumor genomic profiling in a Detroit Metropolitan Area-SEER analysis of women with early-stage hormone-sensitive breast cancer. The results from this analysis demonstrated higher recurrence scores in Black compared to White women, signifying a greater need for adjuvant chemotherapy (28).
These racial disparities in stage and tumor phenotype have been exemplified in reported racial disparities in overall survival over time. In an analysis of 25,997 women with breast cancer diagnosed through the Detroit Metropolitan Area–SEER registry between 1975-2001, successive historical cohorts (1975-1980 and 1990-1995) demonstrated a widening survival gap between Black and White women with breast cancer over time. This disparity pertained specifically to younger women who were not yet Medicare-eligible. In addition, disadvantages in access to radiation, chemotherapy, and hormonal therapy continued over time, particularly among Black women with lymph node-positive disease (data not shown in Table) (29). This information serves in a sense as a “natural experiment” in which it can be hypothesized whether changes in policy and interventions over time could have an influence on cancer survival and treatment. Lastly, in a SEER-18 study of ovarian cancer, Black compared to White women experienced poorer 5-year overall survival for each stage of disease (30).
In this section, we include studies of racial disparities in comorbidities among patients with cancer in order to identify factors that may place Black cancer patients at greater risk for poorer outcomes. In studies using data from both single institutions to multiple sites, PSDR investigators and collaborators found that Black compared to White cancer patients across multiple tumor types were more likely to be diagnosed with co-morbid medical conditions including hypertension (HTN) (18, 21, 22, 31, 32), diabetes (18, 32), heart disease (18), obesity (22, 33, 34), and chronic renal failure (34).
Table 2 lists studies suggesting that co-morbid medical conditions have a differential impact on cancer outcomes for Black and White patients with cancer. In a case-control study from the HFHS, metabolic syndrome was associated with prostate cancer risk in Black men with organ confined disease but not in White men (OR 1.82, 95% CI 1.02-3.23). Data from this study also suggested a possible protective influence of obesity for White but not Black men (OR 0.51, 95% CI 0.33-0.8) (32). Another analysis of Black ovarian cancer survivors from a large multi-site epidemiological study, showed that BMI ≥ 40 and weight gain since age 18 were associated with higher odds of ovarian cancer (OR 1.72, 95% CI 1.12-2.66 for BMI; and OR 1.52, 95% CI 1.07-2.16 for weight gain) (35).
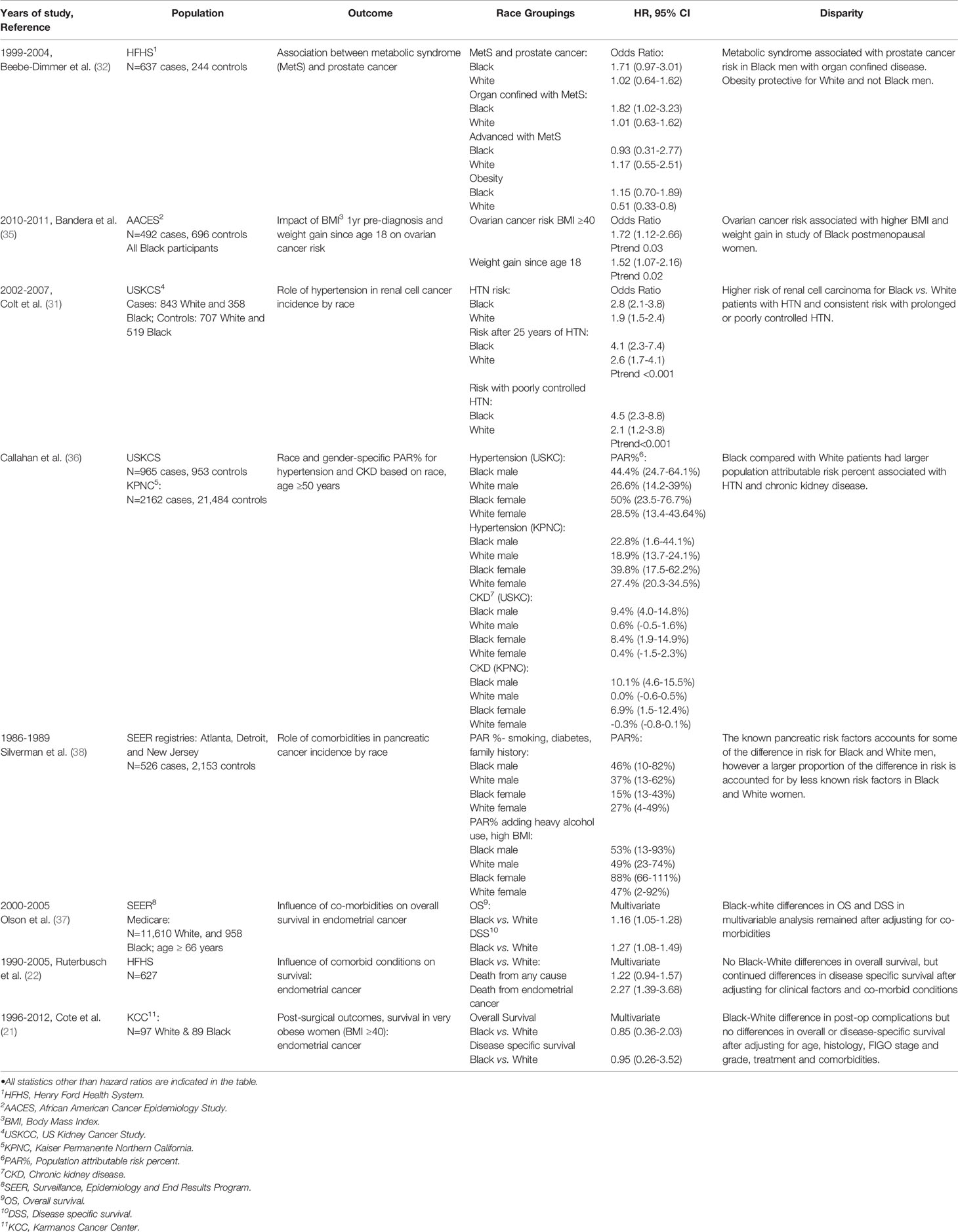
Table 2 The Impact of Co-Morbid Medical Conditions.
A study from the US Kidney Cancer Study (USKCS), which included Detroit as one of two sites, compared risk of renal cell carcinoma (RCC) among Black compared to White patients. Findings demonstrated a higher risk of RCC associated with history of HTN among Black compared to White patients (OR 2.8, 95% CI 2.1-3.8) (31). In an expansion of the USKCS analysis, which also used data from the Kaiser Permanente Northern California (KPNC) registry, the population-attributable risk percentages (PAR%) for HTN and RCC were highest among Black women followed by Black men, White women, and White men. The PAR% for RCC for chronic kidney disease for Black men and women was 7-10 times greater than for White women and men (36).
An analysis of the impact of co-morbid medical conditions on disparities in survival among Black and White women with endometrial cancer at the HFHS, found that Black women continued to have worse overall survival outcomes despite adjustment for co-morbid medical conditions (22). These findings were replicated in a similar analysis of SEER-Medicare linked data (37). In comparison, however, in a study of morbidly obese women with endometrial cancer from the KCC, there were no Black-White disparities in overall or disease specific survival, suggesting the possibility of more equal provision of care once women are part of a single medical care system (21).
Lastly, in a collaborative population-based case-control study of pancreatic cancer including patients from Detroit, Atlanta, and New Jersey, established risk factors (cigarette smoking, long-term diabetes mellitus, family history of pancreatic cancer) accounted for 46% of the risk of disease in Black men and 37% in White men, potentially explaining all but 6% of the excess risk among Black patients. Among women, when less accepted risk factors such as moderate/heavy alcohol consumption (>7 drinks per week) and elevated BMI (above the first quartile) were combined with established risk factors, 88% of the risk of disease in Black women and 47% in White women was explained, potentially accounting for all of the excess risk among Black women (38).
The studies included in this section identify explanatory variables that might at least in part explain Black-White disparities as outlined below. PSDR investigators and collaborators assessed disparities using different outcome measures such as disparities in receipt of cancer-directed treatment, disparities in stage at diagnosis, disparities in rate of relapse, and disparities in survival including overall and disease-specific survival. The majority of studies utilized multivariable methods in order to determine the contribution of multiple potential confounders on racial disparities in outcomes.
Table 3 includes studies that evaluate racial disparities in cancer treatment and show mixed results across type of treatment, tumor type and institution. In an analysis of data on treatment for breast cancer from the KCC, no differences or disparities were found related to surgery or radiation, but Black women with regional stage disease were more likely to receive tamoxifen (OR 4.59, 95% CI 1.52-13.9) or chemotherapy (OR 3.10, 95% CI 1.09-8.81), suggesting the presence of other factors related to the need for more aggressive treatment among Black patients. In the same analysis, women with Medicare or Medicaid were more likely to have mastectomy compared to breast conserving surgery, suggesting that older women and women with lower income were less likely to take, or less likely to be offered, the more favored surgical option (39). In another analysis of early stage breast cancer at the HFHS, there were no racial differences in the receipt of adjuvant chemotherapy (OR 1.01, 95% CI 0.72-1.42) or in the timing of receipt of chemotherapy (OR 1.18, 95% CI 0.8-1.74) (40). Lastly, in an analysis of Black-White differences in breast cancer survival at the KCC, there were no racial differences in treatment received or the cost of care, suggesting similar provision of care despite race at a single institution (18).
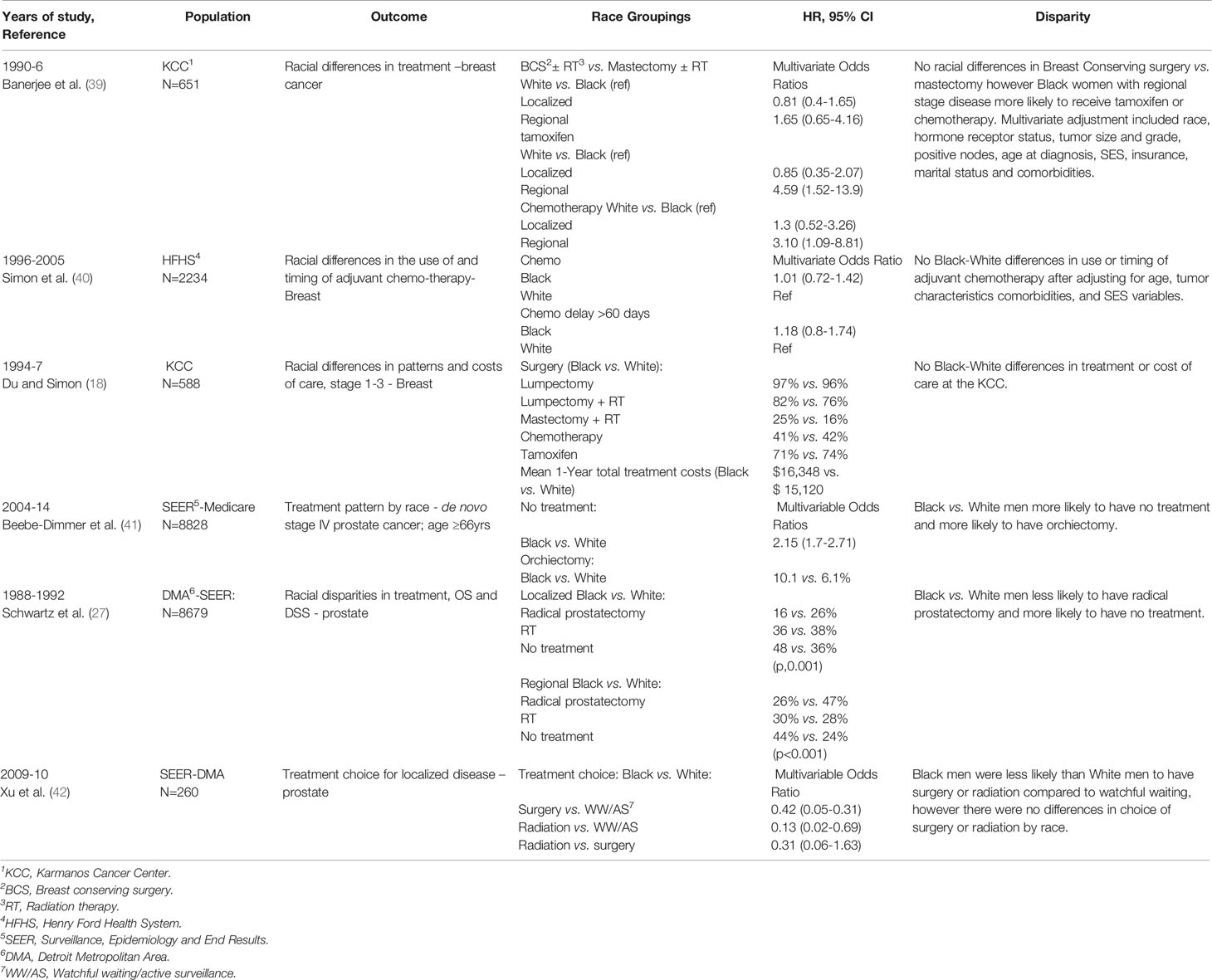
Table 3 Studies focusing on Black-White differences in cancer-directed therapy.
In contrast however, racial disparities in treatment were consistently noted in studies of men with prostate cancer. In three SEER-based collaborative studies, Black compared to White men with prostate cancer were less likely to receive treatment for their cancer. In one study, Black men were less likely to receive any treatment for de-novo stage IV disease (41), or if they received treatment, more likely to have orchiectomy. In another study, Black men were less likely to receive treatment for local or regional stage disease and had worse survival (27). In the third study, Black men were more likely to choose observation only instead of active treatment (42).
In the HFHS study cited earlier, on the influence of co-morbidities on racial differences in outcome for women with endometrial cancer (Table 2), Black women were more likely to have no surgery (17% vs. 4%, p<0.001), and also more likely to need chemotherapy after surgery (27% vs. 20%, p=0.041), again potentially reflecting the more advanced stage and aggressive disease seen in Black women (data not shown in the table) (22). In summary, the studies cited in this section suggest that based on primary site, Black compared to White patients with comparable disease and stage may either be under-treated (less surgical intervention) or receive less desirable treatment (more mastectomy or orchiectomy). Other studies from single institutions show more comparable receipt of treatment across racial groups.
It is generally acknowledged that there are strong associations between variables that include patient social and economic characteristics, neighborhood characteristics, and cancer outcomes (43). Since individual measures of SES such as income, education and insurance are generally not available in larger population-based studies, PSDR investigators in collaboration with other researchers assessed SES through linkage of geocoded residential addresses to sources of data for larger groups residing in standard geographic regions such as census tract (44) county, or census block, noting the potential for ecological fallacy (43, 45).
To account for differences in SES and other neighborhood characteristics, PSDR investigators used the deprivation index, which provides an estimate of the quality of living conditions at census tract levels. The deprivation index is based on the proportion of households without a vehicle; households without a telephone; population over the age of 16 that are unemployed; population living in a residence with more than 1 person per room; and population living below the poverty line (46). A composite index is calculated by adding the value of each of the variables divided by 5 to produce a single index value ranging from 0 to 1, with 0 representing no deprivation and 1 maximal deprivation (17). It should be noted that this method, while providing a broader context for individual SES, is not perfectly valid in that high-deprivation areas can include people of varying economic background (47).
Across a range of studies using data from single institutions or from the SEER registry, Black compared to White patients were more likely to have a primary residence in census tract areas documented as low SES or in areas where a lower proportion of the population had received higher education or had access to medical insurance (15, 17, 19, 40, 48, 49), or to reside in areas with higher measures of deprivation (17, 40, 49). In addition, as reported in one Detroit Metropolitan area-SEER study, Black breast cancer patients were more likely to reside in an area where hospitals provided more care for Medicare and Medicaid patients (13).
In studies using data from the KCC (18), pooled data from case-control studies (50), or from a large US study of postmenopausal women (51), Black compared to White patients had lower levels of educational achievement. In a Detroit Metropolitan Area-SEER analysis of colorectal cancer (CRC), Black compared to White patients were less likely to reside in a census tract area categorized as “professional” (16.5% vs. 42.5%, p<0.001) (15). In a study of women with estrogen and progesterone receptor negative breast cancer at the HFHS, Black compared to White women were ten times more likely to reside in an area with the highest level of deprivation (45.9% vs 4.4%, respectively p< 0.001) (49).
Table 4 lists studies that include SES as part of a multivariable model. In a Detroit Metropolitan Area -SEER study of racial differences in breast cancer survival, after adjustment for SES (based on census tract level data), and other predictors of survival including socio-demographic and clinical factors, White women with local- and regional-stage disease had better overall survival rates than Black women (p<0.00001); however, for women with distant-stage disease, there were no significant survival differences by race (p=0.3). In this analysis, racial differences in survival were only apparent up to 4 years after diagnosis, but not after 4 years (p=0.6). It is of note that the difference in survival for Black and White women in this analysis was more apparent among women at a younger age at diagnosis with a relative risk (RR) for women < 50 years at diagnosis (RR,1.68, 95% CI 1.27-2.23), that was greater than the RR for women 51 and older at diagnosis (RR, 1.33, 95% CI, 1.13-1.56) (13). In other Detroit Metropolitan Area-SEER studies however, adjustment for SES at the census tract level accounted for all of the racial disparities in overall and disease specific survival for Black and White individuals with CRC (15), and overall survival for women with cervical cancer (48).
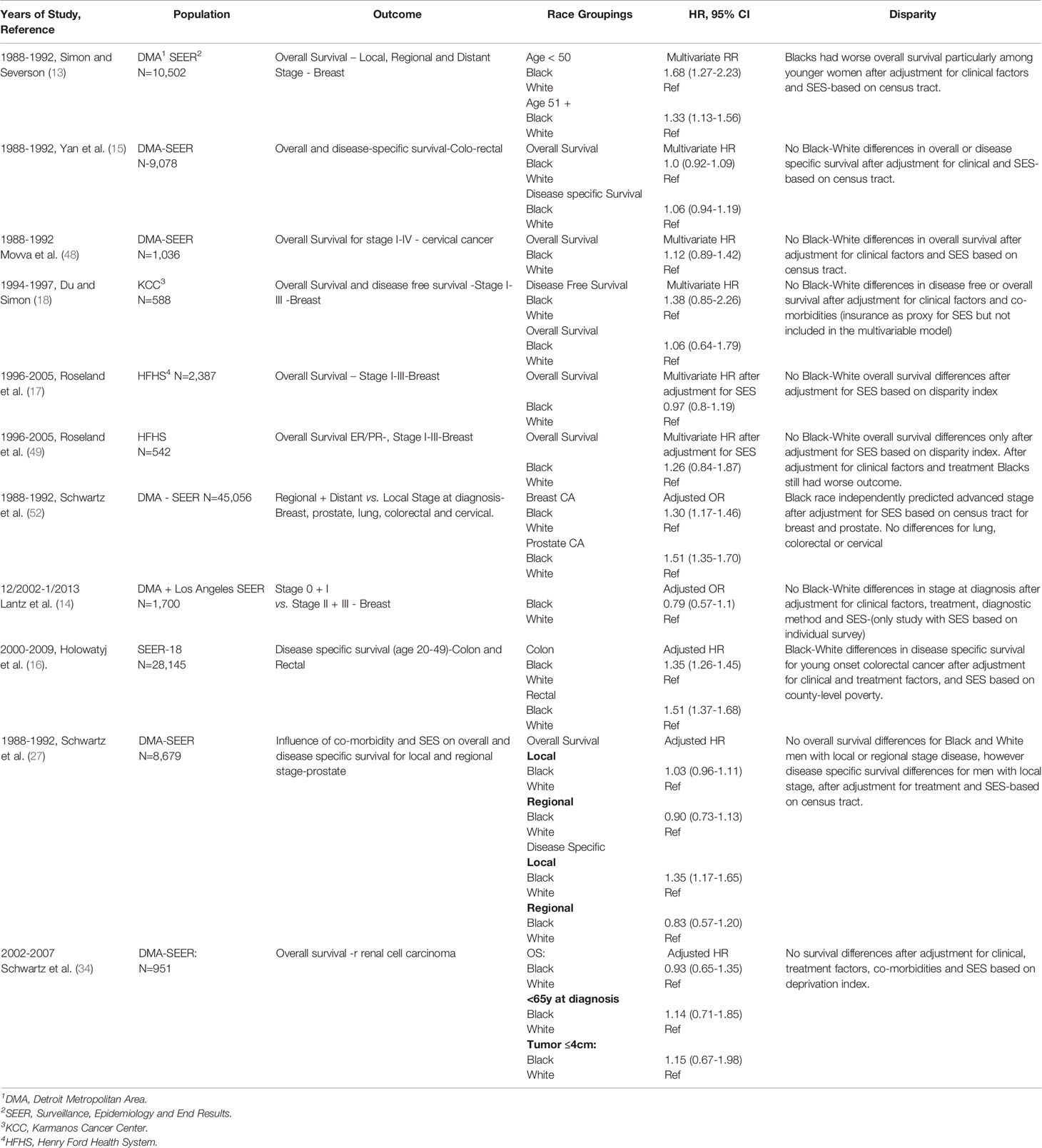
Table 4 Racial Disparities Studies Which Include Socioeconomic Status as Part of Multivariable Model.
Similarly, results from single-institution studies showed no racial differences in survival after accounting for SES. These included a KCC study which showed no Black-White differences in breast cancer disease-free survival (HR 1.38, 95% CI 0.85-2.26) or overall survival (HR 1.06, 95% CI 0.64-1.75) (18), and in the HFHS analysis that showed no breast cancer survival differences after adjustment for neighborhood deprivation index (HR 0.97, 95% CI 0.8-1.9) (17). In a sub-analysis of Black and White women with estrogen and progesterone receptor negative breast cancer at the HFHS, there was also no overall survival disparity after adjustment for deprivation index (HR 1.26, 95% CI 0.84-1.87) (49).
However, other studies showed racial disparities even after controlling for economic and social factors. In a Detroit Metropolitan Area-SEER study after adjusting for SES based on census block, Black patients still had more advanced stage at diagnosis (regional or distant vs. local) among women with breast cancer (OR 1.30, 95% CI 1.17-1.46) and men with prostate cancer (OR 1.51, 95% CI 1.35-1.70) (52). However, differences in stage at presentation were not seen in an analysis of women with stage 0 to III breast cancer using the Detroit and Los Angeles SEER registries where after adjusting for SES based on individual questionnaire, and method of detection, there were no significant differences between Black and White women in diagnosis of stage 0+I disease vs. II+III (14).
In a SEER-18 site study of early onset CRC, after adjusting for SES based on the proportion of individuals below 200% of the poverty level at the county level as well as clinical and treatment factors, Black compared to White patients continued to have worse disease specific survival for both colon (HR 1.35, 95% CI 1.26-1.45) and rectal cancers (HR 1.51, 95% CI 1.37-1.68) (16). A Detroit Metropolitan Area–SEER prostate cancer study showed that after adjustment for SES based on census block data, there were no significant differences for Black and White men for overall survival; however, Black men with localized disease continued to have worse disease specific survival (HR 1.35, 95% CI 1.17-1.65) (27). Lastly, in a Detroit Metropolitan Area-SEER case-control study of RCC that adjusted for SES based on deprivation index and also adjusted for clinical factors and co-morbidity, there were no racial differences in overall survival (HR 0.93, 95% CI 0.65-1.35) (34).
Other studies that did not take into account SES showed varying results (not shown in Table). In a KCC analysis of men who had radical prostatectomy for clinically localized disease, after multivariable adjustment, Black men continued to have worse progression-free survival than White men (HR 2.35, 95% CI 1.63-3.4), p<0.0001 (53). Another study comparing the pre- to post-prostate screening era (PSA testing), another “natural experiment” over time, showed that Black men diagnosed in the pre-PSA era (1973–1994) had higher mortality than White men for all age groups; however this difference in survival disappeared in the post-PSA era (26).
In summary, PSDR investigators in collaboration with others have conducted a wide range of studies using data from either single centers in Detroit or across multiple sites using SEER or other larger data bases to better understand and explain racial health disparities. In general, the studies cited demonstrate that Black compared to White patients with cancer present with more advanced and biologically aggressive disease, are more likely to live in economically and socially deprived areas and are more likely to be diagnosed with co-morbid medical conditions which has the potential to hamper accessibility to optimal cancer-directed treatment. It is also possible that Black patients with co-morbid medical conditions are less likely to be offered treatment as a White person with the same co-morbidity.
While a number of studies have sought to evaluate factors such as differences in treatment or SES that might explain some of the disparities in cancer outcomes noted, these types of first- and second-generation disparities studies are largely descriptive and serve only to document the extent of the problem or identify potential factors underlying the disparities. Further, while controlling for SES is an accepted practice in studies of treatment disparities, two important caveats should be taken into consideration. First of all, SES disparities can be easily traced to legacies of institutional and structural racism and therefore controlling for SES is an attempt to control for one of the consequences of racism which remains unresolved. Secondly, in the process of controlling for disparities, researchers in a sense are creating a world where Black and White people have the same SES, which does not reflect reality.
In order to identify potential ways to address and intervene to reduce racial disparities, investigators in the PSDR in collaboration with other researchers, have conducted studies evaluating differences in clinical communication during patient-physician interactions with Black compared to White patients. In this section, we will present first-generation evidence of disparities in patient-physician communication and then second-generation studies looking at potential factors explaining these disparities and the impact of disparities on cancer outcomes. We will then describe third-generational interventional studies designed to mitigate these disparities in communication.
Clinical communication involving patients, their companions, and their providers plays a critical role in patient-centered care and outcomes (54, 55). Racial disparities in patient-physician communication are well-documented and have been associated with racial disparities in cancer treatment and mortality (56, 57). In research that used video-recordings of patient-physician treatment discussions (after written consent) (58), PSDR researchers have investigated disparities in clinical communication during interactions between non-Black oncologists and their Black patients (59–62). They have also studied the influence of race-based attitudes (e.g., oncologist implicit racial bias, patient suspicion of medical care) on those interactions (61, 62).
As part of this research, PSDR researchers conducted a mixed-methods analysis of 109 video recordings to investigate patient and companion question-asking during interactions with oncologists. Findings showed that compared to White patients, Black patients asked fewer total questions, fewer direct questions, and were less likely to have a companion with them to contribute to question-asking and information-exchange. Findings from this research suggest that these differences in question asking may diminish the quality of information exchange during interactions with Black patients and that Black patients may receive less information from their oncologists (63).
A more recent study of video-recorded interactions between 114 Black patients and non-Black oncologists found that having a companion(s) during the interaction had a positive impact on patient-oncologist interactions. These included oncologists spending more time with the patient and using more patient-centered communication with patients who brought a companion (64). Given documented racial disparities in communication, the presence of companions may be especially beneficial to Black patients. Findings from these studies suggest that provider-level and system-level interventions may be used to encourage patients to participate actively in clinical interactions and to bring supportive companions to assist them in exchanging information with physicians. For example, oncologists could be trained to elicit patient questions and answer them directly and compassionately, and hospitals could encourage companion participation by facilitating video conferencing with companions who may not be able to attend visits.
Another study used linguistic discourse analysis to better understand communication about clinical trials in video-recorded interactions with Black and White patients and their medical oncologists. Findings showed that interactions with Black patients were shorter; the topic of clinical trials was less frequently mentioned; and, when clinical trials were mentioned, less time was spent discussing them (65). Differences were also observed in the discussion of some aspects of consent to clinical trials. Specifically, oncologists and Black patients spent less time discussing the purpose of the trial, risks and benefits, and alternatives to participating in the trial; however, they spent more time discussing the voluntary nature of trials (65). These findings are particularly problematic if this type of communication about clinical trials is the norm for Black patients with cancer (66) because it suggests that Black patients are not receiving adequate information to make an informed decision about participating in a clinical trial. These and similar findings led to intervention studies, described below, to improve the quality of communication during interactions in which clinical trials may be discussed.
Several investigations have focused on the influence of patient and physician race-based attitudes. With regard to physician race-based attitudes, PSDR investigators showed that oncologists with higher implicit bias (i.e. favoring White people) were more likely to have shorter interactions with Black patients than oncologists with lower implicit bias. Further, their communication was perceived by patients as less patient-centered and by patients and independent observers as less supportive with their Black patients. This in turn led to less patient confidence in treatment recommendations and greater perceived difficulty in completing treatment (61). With regard to patient race-based attitudes, using the Group-Based Medical Mistrust scale developed by a PSDR investigator (67), relationships were found between Black patients’ group-based medical suspicion (67) and their attitudes about adherence and decisional control (62). Other work found that high levels of group-based medical suspicion among Black patients was associated with more negative evaluations of physicians and recommended treatment (68). Patient mistrust of medical care and lack of trust in physicians were also associated with not only how much Black patients spoke during medical interactions but also the valence of the words they used. High levels of patient mistrust was also associated with less favorable physician perceptions of Black patients, which, in turn, affected physician perceptions of how well these patients would tolerate treatments (68). A more recent study found that Black men with prostate cancer had higher levels of group-based medical suspicion than White men, and this race-based attitude was associated with less willingness to discuss clinical trials with their physicians (69). More current research is examining how patient and oncologist nonverbal communication may be associated with these race-based attitudes (70, 71).
In an attempt to mitigate these disparities in communication and the influence of race-based attitudes, PSDR investigators have developed and tested communication interventions. One type of low-cost and effective intervention tested has been question prompt lists (QPL). QPLs are simple communication tools designed to promote active participation in clinical interactions. QPLs are provided to patients before a clinical interaction and include a list of questions patients can consider asking their physician in a specific clinical context (72–75). Using a community engagement process to aid in its development, PSDR investigators created and tested a QPL for patients considering chemotherapy (76, 77). In a trial with 114 Black patients randomized to receive standard of care, a QPL brochure, or a QPL brochure and the assistance of a coach, video recordings of patient-physician interactions and post-interaction, patient surveys demonstrated that the QPL was feasible and acceptable. The QPL also increased observer coded patient active participation and information exchange in treatment discussions with their medical oncologist (78). In ongoing studies, researchers are currently testing the effectiveness of a QPL designed to improve clinical trials discussions along with a companion intervention for oncologists (78), and an app-based QPL focused on cancer treatment costs (79).
The current paper has framed KCI research in the context of first-, second,- and third -generation disparities research. We are now laying the foundation for fourth-generation research, which is rooted in justice and action to eliminate disparities. Fourth generation research may be guided by public health critical race praxis (PHCR): “…a semi-structured process for conducting research that remains attentive to issues of both racial equity and methodologic rigor” (80). At the core of PHCR is race consciousness, which requires attention to racial dynamics within the research context as well as the outer world, and the role of racism in cancer health inequity (80).
Thomas et al. (12) assert: “In fourth-generation research, guided by PHCR, it is essential to remember that the goal is ultimately to take action to eliminate health disparities. In that context, the voice of community members is an absolute necessity. Fourth-generation research is deeply rooted in community and the racialized context of the populations who reside within them.” The need for community voice in research guides KCI’s Office of Cancer Health Equity and Community Engagement and its Michigan Cancer HealthLink program, which engages diverse populations throughout the state to build public interest, involvement, and community capacity to collaborate in cancer-related research. Michigan Cancer HealthLink is an academic-community partnership that uses a participatory research approach to facilitate collaboration between community members and researchers through an iterative process of problem definition, problem solving, and evaluation. Partnership activities also focus on skill development, resource mobilization, and relationship building. HealthLink is based on a network of Cancer Action Councils or CACs: groups of cancer survivors, caregivers, and advocates who use their local knowledge and expertise to reduce the burden of cancer in underserved communities. There are currently 9 CACs with over 100 members in six cities across four counties in Michigan, representing Black American, Arab American, young survivor, and LGBT+ communities (81).
Through Michigan Cancer HealthLink, we are setting the stage for fourth generation research to eliminate the disparities that disadvantage Black Americans. These efforts are informed by the principle of voice: the privileging of marginalized persons’ contributions to discourses (81). The CACs are a key way to amplify the voices of Black Americans in our work. Using semi-structured methods, CACs identify and develop research priorities that they feel are most relevant to their specific communities. CACs also receive training in research methods to prepare them to actively partner with our researchers and contribute to development of research ideas, design, and implementation. In short, HealthLink is an infrastructure that supports action-oriented disparities research by building research capacity in Black American communities and soliciting different perspectives that can challenge, supplement, and even replace the traditional, academic perspectives that tend to dominate disparities work. As Ford et al. (80) assert, “[Voice] helps to illuminate disciplinary blind spots that are otherwise imperceptible from within a discipline’s mainstream. It increases understandings of minorities’ lived experiences, which improves operationalization of constructs, development of effective interventions and creation of an equitable society.” As we apply a PHCR approach, we increasingly distance ourselves from the perspective that Black American communities are mainly environments that drive racial disparities in cancer risk, care, and outcomes. When viewed through the PHCR lens, these communities are vital hubs for resources, opportunities, partners, and solutions to achieve equity.
Researchers in KCI’s PSDR, along with their collaborators, have spent the past three decades investigating racial disparities in cancer incidence, treatment, and outcomes among Black and White patients in Southeast Michigan, with a specific focus on the Detroit area, a city with a majority Black population. The studies document the pattern of more aggressive disease seen in Black compared to White cancer patients, as well as higher rates of co-morbid medical conditions and differences in treatment and communication, which have additional adverse effects on cancer outcomes. These findings suggest that in order to reduce or eliminate racial disparities in cancer outcomes, it is also of utmost importance to address larger questions of inequality inherent in the legacy of structural racism in the US, along with disparities across the spectrum of chronic comorbid and medical conditions, which have an disproportionately negative impact on Black people (4).
To date, abundant research on cancer disparities and inequities in health outcomes has been published, as exemplified by the recent review by Zevala et al. (82). This review includes a detailed description of disparities in cancer incidence, mortality, health care screening, treatment and tumor biology experienced by almost every racial and ethnic minority group in the United States, and across both common and uncommon cancers. Consistent with the research reported here, Zevala et al. provided explicit information on potential causative factors and steps needed to mitigate racial and ethnic disparities. Given the demographics of Detroit, our review focused on studies inclusive of Black and White cancer survivors outlining disparities similar to that experienced by other groups (82). Future work in the Detroit area should focus on structural racism and disparities in cancer care experienced by additional marginalized and minority groups in the region including the large Mexican and Arab American populations. One prime example of structural racism is the status of residential housing in the US (4, 83). Black cancer patients are more likely to live in geographic areas with lower levels of aggregate SES, and consequently are faced with less access to high-quality medical care, resulting in lower quality of care. While structural racism may be difficult to address in the short term, providing transportation and easier access to care may be a first step with longer-term goals of equitable housing and insurance coverage. Recent efforts on the part of academic health centers including WSU and the KCI to better understand the underlying influence of social determinants on health care outcomes can provide new structures and options in which to train health care professionals to provide more equitable health care for all racial and ethnic groups (84, 85).
Other underlying reasons for Black-White health disparities include the legacy of fewer and lower quality medical services being available in the areas where many Black people live (5–7, 86); poor employment opportunities; and inadequate and unhealthy housing and inadequate or substandard education opportunities that have historically disadvantaged the Black community and have both directly and indirectly contributed to poor health care outcomes (86). Similarly, a historic loss of population for socioeconomic reasons or excess mortality from chronic health conditions has disproportionately burdened the Black population over time (87). Our research has demonstrated a few examples of “natural experiments” documenting the widening gaps in survival and treatment options for Black and White women with breast cancer over several birth cohorts (29), and a diminution in the prostate cancer mortality gap marked by the institution of PSA screening (26). Future work in Detroit should take advantage of other natural experiments such as new health care policies such as the Affordable Care Act, or other interventions that may shed light on how structural factors impact racial and ethnic differences in outcomes. In order to reduce Black-White disparities in cancer outcomes, we propose multi-level interventions such as community engagement, recruiting more diverse clinical staff (88), and conducting system-wide anti-racism training (85). Our research points to the benefit of interventions that are relatively easy to implement and could have an immediate impact on the quality of and better access to care, including Question Prompt lists, brief language-appropriate educational videos and the inclusion of Lay Health Advisors (89) and patient navigators as essential components of the health delivery system. Such efforts would also be easily adaptable to additional underserved populations.
At the KCI, the Detroit Research on Cancer Survivorship (ROCS) study is the only National Cancer Institute-funded survivorship cohort of Black cancer survivors in the US (90). Studies of this cohort (enrollment goal 5,000) are seeking to elucidate the specific influence of systematic and structural racism at the community and individual levels on the emotional and physical health, health and screening behaviors, and quality of life of Black cancer survivors (91–93) An understanding of race-related factors underlying and maintaining health-disparate outcomes is essential for developing interventions and initiatives that could reduce current inequalities in diagnosis, treatment, and survival, and improve the quality of cancer survivorship in Black men and women with cancer. Knowledge gained from research on racial health disparities among cancer patients and those with other medical conditions can also help to eradicate disparities in additional groups in the future.
SR: She conducted the pub med review of all of the articles included in the review, constructed the tables and helped edit and write the manuscript. LH: She wrote and organized the section on physician communication. She also was responsible for extensive editing. LP: Extensive editing with a focus on racial disparities and the physician communications section. KS: Extensive editing with a focus on the epidemiologic studies. FH: Extensive editing with a focus on the physician communications section. HT: She wrote the section on fourth generation research and edited the rest of the manuscript. JB: Editing with a focus on area based measures of SES. MC: Editing. AS: Editing and advise as to formatting and structure. SE: Extensive editing. Focused on the physician communication section. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Cronin KA, Lake AJ, Scott S, Sherman RL, Noone AM, Howlader N, et al. Annual Report to the Nation on the Status of Cancer, Part I: National Cancer Statistics. Cancer (2018) 124:2785–800. doi: 10.1002/cncr.31551
2. Braveman P. What are Health Disparities and Health Equity? We Need to be Clear. Public Health Rep (2014) 129(Suppl 2):5–8. doi: 10.1177/00333549141291S203
3. Polite BN, Adams-Campbell LL, Brawley OW, Bickell N, Carethers JM, Flowers CR, et al. Charting the Future of Cancer Health Disparities Research: A Position Statement From the American Association for Cancer Research, the American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute. Cancer Res (2017) 77:4548–55. doi: 10.1158/0008-5472.CAN-17-2932
4. Bailey ZD, Feldman JM, Bassett MT. How Structural Racism Works - Racist Policies as a Root Cause of U.S. Racial Health Inequities. N Engl J Med (2021) 384:768–73. doi: 10.1056/NEJMms2025396
5. Washington HA. Medical Apartheid. The DArk History of Medical Experimentation on Black Americans From Colonial Times to the Present, Anchor Books. (2006).
6. Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington (DC): National Acadamies Press, 3 A.D. (2003)
7. Doubeni CA, Simon M, Krist AH. Addressing Systemic Racism Through Clinical Preventive Service Recommendations From the US Preventive Services Task Force. JAMA (2021) 325(7):627–28. doi: 10.1001/jama.2020.26188
8. National Healthcare Quality and Disparities Reports. Rockville MD: Agency for Healthcare Research and Quality (2021).
9. Williams DR, Lawrence JA, Davis BA. Racism and Health: Evidence and Needed Research. In: Annual Review of Public Health. Annual Review of Public Health (2019). p. 105–25. doi: 10.1146/annurev-publhealth-040218-043750
10. Vyas DA, Eisenstein LG, Jones DS. Hidden in Plain Sight - Reconsidering the Use of Race Correction in Clinical Algorithms. N Engl J Med (2020) 383:874–82. doi: 10.1056/NEJMms2004740
11. Howlader N, Noone AM, Krapcho M, Miller D, Brest A, Yu M, et al eds. Seer Cancer Statistics Review, 1975-2017. Bethesda, MD: National Cancer Institute (2020).
12. Thomas SB, Quinn SC, Butler J, Fryer CS, Garza MA. Toward a Fourth Generation of Disparities Research to Achieve Health Equity. Annu Rev Public Health (2011) 32:399–416. doi: 10.1146/annurev-publhealth-031210-101136
13. Simon MS, Severson RK. Racial Differences in Survival of Female Breast Cancer in the Detroit Metropolitan Area. Cancer (1996) 77:308–14. doi: 10.1002/(SICI)1097-0142(19960115)77:2<308::AID-CNCR13>3.0.CO;2-5
14. Lantz PM, Mujahid M, Schwartz K, Janz NK, Fagerlin A, Salem B, et al. The Influence of Race, Ethnicity, and Individual Socioeconomic Factors on Breast Cancer Stage at Diagnosis. Am J Public Health (2006) 96:2173–8. doi: 10.2105/AJPH.2005.072132
15. Yan B, Noone AM, Yee C, Banerjee M, Schwartz K, Simon MS. Racial Differences in Colorectal Cancer Survival in the Detroit Metropolitan Area. Cancer (2009) 115:3791–800. doi: 10.1002/cncr.24408
16. Holowatyj AN, Ruterbusch JJ, Rozek LS, Cote ML, Stoffel EM. Racial/Ethnic Disparities in Survival Among Patients With Young-Onset Colorectal Cancer. J Clin Oncol (2016) 34:2148–56. doi: 10.1200/JCO.2015.65.0994
17. Roseland ME, Pressler ME, Lamerato E, Krajenta R, Ruterbusch JJ, Booza JC, et al. Racial Differences in Breast Cancer Survival in a Large Urban Integrated Health System. Cancer (2015). doi: 10.1002/cncr.29523
18. Du W, Simon MS. Racial Disparities in Treatment and Survival of Women With Stage I-III Breast Cancer at a Large Academic Medical Center in Metropolitan Detroit. Breast Cancer Res Treat (2005) 91:243–8. doi: 10.1007/s10549-005-0324-9
19. Simon MS, Banerjee M, Crossley-May H, Vigneau FD, Noone AM, Schwartz K. Racial Differences in Breast Cancer Survival in the Detroit Metropolitan Area. Breast Cancer Res Treat (2006) 97:149–55. doi: 10.1007/s10549-005-9103-x
20. Cote ML, Alhajj T, Ruterbusch JJ, Bernstein L, Brinton LA, Blot WJ, et al. Risk Factors for Endometrial Cancer in Black and White Women: A Pooled Analysis From the Epidemiology of Endometrial Cancer Consortium (E2c2). Cancer Causes Control (2015) 26:287–96. doi: 10.1007/s10552-014-0510-3
21. Cote ML, Ruterbusch JJ, Ahmed Q, Bandyopadhyay S, Alosh B, Abdulfatah E, et al. Endometrial Cancer in Morbidly Obese Women: Do Racial Disparities Affect Surgical or Survival Outcomes? Gynecol Oncol (2014) 133:38–42. doi: 10.1016/j.ygyno.2014.01.013
22. Ruterbusch JJ, Ali-Fehmi R, Olson SH, Sealy-Jefferson S, Rybicki BA, Hensley-Alford S, et al. The Influence of Comorbid Conditions on Racial Disparities in Endometrial Cancer Survival. Am J Obstet Gynecol (2014) 211:627–9. doi: 10.1016/j.ajog.2014.06.036
23. Cote ML, Ruterbusch JJ, Olson SH, Lu K, Ali-Fehmi R. The Growing Burden of Endometrial Cancer: A Major Racial Disparity Affecting Black Women. Cancer Epidemiol Biomarkers Prev (2015) 24:1407–15. doi: 10.1158/1055-9965.EPI-15-0316
24. Holowatyj AN, Ruterbusch JJ, Ratnam M, Gorski DH, Cote ML. HER2 Status and Disparities in Luminal Breast Cancers. Cancer Med (2016) 5:2109–16. doi: 10.1002/cam4.757
25. Powell IJ, Bock CH, Ruterbusch JJ, Sakr W. Evidence Supports a Faster Growth Rate and/or Earlier Transformation to Clinically Significant Prostate Cancer in Black Than in White American Men, and Influences Racial Progression and Mortality Disparity. J Urol (2010) 183:1792–6. doi: 10.1016/j.juro.2010.01.015
26. Powell IJ, Vigneau FD, Bock CH, Ruterbusch J, Heilbrun LK. Reducing Prostate Cancer Racial Disparity: Evidence for Aggressive Early Prostate Cancer PSA Testing of African American Men. Cancer Epidemiol Biomarkers Prev (2014) 23:1505–11. doi: 10.1158/1055-9965.EPI-13-1328
27. Schwartz K, Powell IJ, Underwood W, George III, J., Yee C, Banerjee M. Interplay of Race, Socioeconomic Status, and Treatment on Survival of Patients With Prostate Cancer. Urology (2009) 74:1296–302. doi: 10.1016/j.urology.2009.02.058
28. Holowatyj AN, Cote ML, Ruterbusch JJ, Ghanem K, Schwartz AG, Vigneau FD, et al. Racial Differences in 21-Gene Recurrence Scores Among Patients With Hormone Receptor-Positive, Node-Negative Breast Cancer. J Clin Oncol (2018) 36:652–8. doi: 10.1200/JCO.2017.74.5448
29. Gorey KM, Luginaah IN, Schwartz KL, Fung KY, Balagurusamy M, Bartfay E, et al. Increased Racial Differences on Breast Cancer Care and Survival in America: Historical Evidence Consistent With a Health Insurance Hypothesis, 1975-2001. Breast Cancer Res Treat (2009) 113:595–600. doi: 10.1007/s10549-008-9960-1
30. Park HK, Ruterbusch JJ, Cote ML. Recent Trends in Ovarian Cancer Incidence and Relative Survival in the United States by Race/Ethnicity and Histologic Subtypes. Cancer Epidemiol Biomarkers Prev (2017) 26:1511–8. doi: 10.1158/1055-9965.EPI-17-0290
31. Colt JS, Schwartz K, Graubard BI, Davis F, Ruterbusch J, DiGaetano R, et al. Hypertension and Risk of Renal Cell Carcinoma Among White and Black Americans. Epidemiology (2011) 22:797–804. doi: 10.1097/EDE.0b013e3182300720
32. Beebe-Dimmer JL, Nock NL, Neslund-Dudas C, Rundle A, Bock CH, Tang D, et al. Racial Differences in Risk of Prostate Cancer Associated With Metabolic Syndrome. Urology (2009) 74:185–90. doi: 10.1016/j.urology.2009.03.013
33. Peres LC, Risch H, Terry KL, Webb PM, Goodman MT, Wu AH, et al. Racial/Ethnic Differences in the Epidemiology of Ovarian Cancer: A Pooled Analysis of 12 Case-Control Studies. Int J Epidemiol (2018) 47:460–72. doi: 10.1093/ije/dyx252
34. Schwartz K, Ruterbusch JJ, Colt JS, Miller DC, Chow WH, Purdue MP. Racial Disparities in Overall Survival Among Renal Cell Carcinoma Patients With Young Age and Small Tumors. Cancer Med (2016) 5:200–8. doi: 10.1002/cam4.578
35. Bandera EV, Qin B, Moorman PG, Alberg AJ, Barnholtz-Sloan JS, Bondy M, et al. Obesity, Weight Gain, and Ovarian Cancer Risk in African American Women. Int J Cancer (2016) 139:593–600. doi: 10.1002/ijc.30115
36. Callahan CL, Schwartz K, Corley DA, Ruterbusch JJ, Zhao WK, Shuch B, et al. Understanding Racial Disparities in Renal Cell Carcinoma Incidence: Estimates of Population Attributable Risk in Two US Populations. Cancer Causes Control (2020) 31:85–93. doi: 10.1007/s10552-019-01248-1
37. Olson SH, Atoria CL, Cote ML, Cook LS, Rastogi R, Soslow RA, et al. The Impact of Race and Comorbidity on Survival in Endometrial Cancer. Cancer Epidemiol Biomarkers Prev (2012) 21:753–60. doi: 10.1158/1055-9965.EPI-11-0735
38. Silverman DT, Hoover RN, Brown LM, Swanson GM, Schiffman M, Greenberg RS, et al. Why do Black Americans Have a Higher Risk of Pancreatic Cancer Than White Americans? Epidemiology (2003) 14:45–54. doi: 10.1097/00001648-200301000-00013
39. Banerjee M, George J, Yee C, Hryniuk W, Schwartz K. Disentangling the Effects of Race on Breast Cancer Treatment. Cancer (2007) 110:2169–77. doi: 10.1002/cncr.23026
40. Simon MS, Lamerato L, Krajenta R, Booza JC, Ruterbusch JJ, Kunz S, et al. Racial Differences in the Use of Adjuvant Chemotherapy for Breast Cancer in a Large Urban Integrated Health System. Int J Breast Cancer (2012) 453985:2012. doi: 10.1155/2012/453985
41. Beebe-Dimmer JL, Ruterbusch JJ, Cooney KA, Bolton A, Schwartz K, Schwartz AG, et al. Racial Differences in Patterns of Treatment Among Men Diagnosed With De Novo Advanced Prostate Cancer: A Seer-Medicare Investigation. Cancer Med (2019) 8:3325–35. doi: 10.1002/cam4.2092
42. Xu J, Janisse J, Ruterbusch J, Ager J, Schwartz KL. Racial Differences in Treatment Decision-Making for Men With Clinically Localized Prostate Cancer: A Population-Based Study. J Racial Ethn Health Disparities (2016) 3:35–45. doi: 10.1007/s40615-015-0109-8
43. Krieger N, Quesenberry C Jr., Peng T, Horn-Ross P, Stewart S, Brown S, et al. Social Class, Race/Ethnicity, and Incidence of Breast, Cervix, Colon, Lung, and Prostate Cancer Among Asian, Black, Hispanic, and White Residents of the San Francisco Bay Area, 1988-92 (United States). Cancer Causes Control (1999) 10:525–37. doi: 10.1023/A:1008950210967
45. Census of Population and Houseing (1990) Summary Tape File 3. Technical Documentation. U.S. Census Bureau (1991).
46. Klassen AC, Curriero FC, Hong JH, Williams C, Kulldorff M, Meissner HI, et al. The Role of Area-Level Influences on Prostate Cancer Grade and Stage at Diagnosis. Prev Med (2004) 39:441–8. doi: 10.1016/j.ypmed.2004.04.031
47. Singh GK. Area Deprivation and Widening Inequalities in US Mortality, 1969-1998. Am J Public Health (2003) 93:1137–43. doi: 10.2105/AJPH.93.7.1137
48. Movva S, Noone AM, Banerjee M, Patel DA, Schwartz K, Yee CL, et al. Racial Differences in Cervical Cancer Survival in the Detroit Metropolitan Area. Cancer (2008) 112:1264–71. doi: 10.1002/cncr.23310
49. Roseland ME, Schwartz K, Ruterbusch JJ, Lamerato L, Krajenta R, Booza J, et al. Influence of Clinical, Societal, and Treatment Variables on Racial Differences in ER-/PR- Breast Cancer Survival. Breast Cancer Res Treat (2017) 165:163–8. doi: 10.1007/s10549-017-4300-y
50. Schildkraut JM, Abbott SE, Alberg AJ, Bandera EV, Barnholtz-Sloan JS, Bondy ML, et al. Association Between Body Powder Use and Ovarian Cancer: The African American Cancer Epidemiology Study (Aaces). Cancer Epidemiol Biomarkers Prev (2016) 25:1411–7. doi: 10.1158/1055-9965.EPI-15-1281
51. Patel MI, Wang A, Kapphahn K, Desai M, Chlebowski RT, Simon MS, et al. Racial and Ethnic Variations in Lung Cancer Incidence and Mortality: Results From the Women’s Health Initiative. J Clin Oncol (2016) 34:360–8. doi: 10.1200/JCO.2015.63.5789
52. Schwartz KL, Crossley-May H, Vigneau FD, Brown K, Banerjee M. Race, Socioeconomic Status and Stage at Diagnosis for Five Common Malignancies. Cancer Causes Control (2003) 14:761–6. doi: 10.1023/A:1026321923883
53. Powell IJ, Dey J, Dudley A, Pontes JE, Cher ML, Sakr W, et al. Disease-Free Survival Difference Between African Americans and Whites After Radical Prostatectomy for Local Prostate Cancer: A Multivariable Analysis. Urology (2002) 59:907–12. doi: 10.1016/S0090-4295(02)01609-6
54. Epstein RM, Street RL. Patient-Centered Communication in Cancer Care: Promoting Healing and Reducing Suffering, in (Ed 07-6225). Bethesda: Bethesda,MD, National Cancer Institute, NIH Publication No. 07-6225 (2007).
55. Gilligan T, Coyle N, Frankel RM, Berry DL, Bohlke K, Epstein RM, et al. Patient-Clinician Communication: American Society of Clinical Oncology Consensus Guideline. J Clin Oncol (2017) 35:3618–32. doi: 10.1200/JCO.2017.75.2311
56. Shen MJ, Peterson EB, Costas-Muniz R, Hernandez MH, Jewell ST, Matsoukas K, et al. The Effects of Race and Racial Concordance on Patient-Physician Communication: A Systematic Review of the Literature. J Racial Ethn Health Disparities (2018) 5:117–40. doi: 10.1007/s40615-017-0350-4
57. Penner LA, Eggly S, Griggs JJ, Underwood W, III H, Albrecht TL. Life-Threatening Disparities: The Treatment of Black and White Cancer Patients. J Soc Issues (2012) 68. doi: 10.1111/j.1540-4560.2012.01751.x
58. Albrecht TL, Penner LA, Cline RJ, Eggly SS, Ruckdeschel JC. Studying the Process of Clinical Communication: Issues of Context, Concepts, and Research Directions. J Health Commun (2009) 14(Suppl 1):47–56. doi: 10.1080/10810730902806794
59. Hamel LM, Dougherty DW, Albrecht TL, Wojda M, Jordan A, Moore TF, et al. Unpacking Trial Offers and Low Accrual Rates: A Qualitative Analysis of Clinic Visits With Physicians and Patients Potentially Eligible for a Prostate Cancer Clinical Trial. JCO Oncol Pract (2020) 16:e124–31. doi: 10.1200/JOP.19.00444
60. Hamel LM, Penner LA, Albrecht TL, Heath E, Gwede CK, Eggly S. Barriers to Clinical Trial Enrollment in Racial and Ethnic Minority Patients With Cancer. Cancer Control (2016) 23:327–37. doi: 10.1177/107327481602300404
61. Penner LA, Dovidio JF, Gonzalez R, Albrecht TL, Chapman R, Foster T, et al. The Effects of Oncologist Implicit Racial Bias in Racially Discordant Oncology Interactions. J Clin Oncol (2016) 34:2874–80. doi: 10.1200/JCO.2015.66.3658
62. Penner LA, Dovidio JF, Hagiwara N, Foster T, Albrecht TL, Chapman RA, et al. An Analysis of Race-related Attitudes and Beliefs in Black Cancer Patients: Implications for Health Care Disparities. J Health Care Poor Underserved (2016) 27:1503–20. doi: 10.1353/hpu.2016.0115
63. Eggly S, Harper FW, Penner LA, Gleason MJ, Foster T, Albrecht TL. Variation in Question Asking During Cancer Clinical Interactions: A Potential Source of Disparities in Access to Information. Patient Educ Couns (2011) 82:63–8. doi: 10.1016/j.pec.2010.04.008
64. Otto AK, Reblin M, Harper FWK, Hamel LM, Moore TF, Ellington L, et al. Impact of Patients’ Companions on Clinical Encounters Between Black Patients and Their non-Black Oncologists. JCO Oncol Pract (2021), OP2000820. doi: 10.1200/OP.20.00820
65. Eggly S, Barton E, Winckles A, Penner LA, Albrecht TL. A Disparity of Words: Racial Differences in Oncologist-Patient Communication About Clinical Trials. Health Expect (2015) 18:1316–26. doi: 10.1111/hex.12108
66. Hamel LM, Penner LA, Eggly S, Chapman R, Klamerus JF, Simon MS, et al. Do Patients and Oncologists Discuss the Cost of Cancer Treatment? An Observational Study of Clinical Interactions Between African American Patients and Their Oncologists. J Oncol Pract (2017) 13:e249–58. doi: 10.1200/JOP.2016.015859
67. Thompson HS, Valdimarsdottir HB, Winkel G, Jandorf L, Redd W. The Group-Based Medical Mistrust Scale: Psychometric Properties and Association With Breast Cancer Screening. Prev Med (2004) 38:209–18. doi: 10.1016/j.ypmed.2003.09.041
68. Penner LA, Harper FWK, Dovidio JF, Albrecht TL, Hamel LM, Senft N, et al. The Impact of Black Cancer Patients’ Race-Related Beliefs and Attitudes on Racially-Discordant Oncology Interactions: A Field Study. Soc Sci Med (2017) 191:99–108. doi: 10.1016/j.socscimed.2017.08.034
69. Senft N, Hamel LM, Manning MA, Kim S, Penner LA, Moore TF, et al. Willingness to Discuss Clinical Trials Among Black vs White Men With Prostate Cancer. JAMA Oncol (2020). doi: 10.1001/jamaoncol.2020.3697
70. Hamel LM, Moulder R, Albrecht TL, Boker S, Eggly S, Penner LA. Nonverbal Synchrony as a Behavioural Marker of Patient and Physician Race-Related Attitudes and a Predictor of Outcomes in Oncology Interactions: Protocol for a Secondary Analysis of Video-Recorded Cancer Treatment Discussions. BMJ Open (2018) 8:e023648. doi: 10.1136/bmjopen-2018-023648
71. Hamel LM, Moulder R, Harper FWK, Penner LA, Albrecht TL, Eggly S. Examining the Dynamic Nature of Nonverbal Communication Between Black Patients With Cancer and Their Oncologists. Cancer (2020). doi: 10.1002/cncr.33352
72. Sansoni JE, Grootemaat P, Duncan C. Question Prompt Lists in Health Consultations: A Review. Patient Educ Couns (2015) 98(12):1454–64. doi: 10.1016/j.pec.2015.05.015
73. Brandes K, Linn AJ, Butow PN, van Weert JC. The Characteristics and Effectiveness of Question Prompt List Interventions in Oncology: A Systematic Review of the Literature. Psychooncology (2015) 24:245–52. doi: 10.1002/pon.3637
74. Dimoska A, Tattersall MH, Butow PN, Shepherd H, Kinnersley P. Can a “Prompt List” Empower Cancer Patients to Ask Relevant Questions? Cancer (2008) 113:225–37. doi: 10.1002/cncr.23543
75. Henselmans I, De Haes HC, Smets EM. Enhancing Patient Participation in Oncology Consultations: A Best Evidence Synthesis of Patient-Targeted Interventions. Psychooncology (2013) 22:961–77. doi: 10.1002/pon.3099
76. Eggly S, Tkatch R, Penner LA, Mabunda L, Hudson J, Chapman R, et al. Development of a Question Prompt List as a Communication Intervention to Reduce Racial Disparities in Cancer Treatment. J Cancer Educ (2013) 28:282–9. doi: 10.1007/s13187-013-0456-2
77. Eggly S, Hamel LM, Foster TS, Albrecht TL, Chapman R, Harper FWK, et al. Randomized Trial of a Question Prompt List to Increase Patient Active Participation During Interactions With Black Patients and Their Oncologists. Patient Educ Couns (2017) 100:818–26. doi: 10.1016/j.pec.2016.12.026
78. Eggly S, Hamel LM, Heath E, Manning MA, Albrecht TL, Barton E, et al. Partnering Around Cancer Clinical Trials (PACCT): Study Protocol for a Randomized Trial of a Patient and Physician Communication Intervention to Increase Minority Accrual to Prostate Cancer Clinical Trials. BMC Cancer (2017) 17:807. doi: 10.1186/s12885-017-3804-5
79. Hamel LM, Thompson HS, Albrecht TL, Harper FW. Designing and Testing Apps to Support Patients With Cancer: Looking to Behavioral Science to Lead the Way. JMIR Cancer (2019) 5:e12317. doi: 10.2196/12317
80. Ford CL, Airhihenbuwa CO. The Public Health Critical Race Methodology: Praxis for Antiracism Research. Soc Sci Med (2010) 71:1390–8. doi: 10.1016/j.socscimed.2010.07.030
81. Thompson HS. Tackling Racial Disparities Through Novel Approaches to Engage Communities in Research. Cancer Letter (2021) 47(4).
82. Zavala VA, Bracci PM, Carethers JM, Carvajal-Carmona L, Coggins NB, Cruz-Correa MR, et al. Cancer Health Disparities in Racial/Ethnic Minorities in the United States. Br J Cancer (2021) 124:315–32. doi: 10.1038/s41416-020-01038-6
83. Rothstein R. The Color of Law: A Forgotten History of How Our Government Segregated America. Norton WW. Liveright Publishing (2017).
84. Smitherman HC Jr., Baker RS, Wilson MR. Socially Accountable Academic Health Centers: Pursuing a Quadripartite Mission. Acad Med (2019) 94:176–81. doi: 10.1097/ACM.0000000000002486
85. Vince RA Jr. Eradicating Racial Injustice in Medicine-If Not Now, When? JAMA (2020) 324:451–2. doi: 10.1001/jama.2020.12432
86. Williams DR, Cooper LA. Reducing Racial Inequities in Health: Using What We Already Know to Take Action. Int J Environ Res Public Health (2019) 16(4):606. doi: 10.3390/ijerph16040606
87. Smitherman HCKLAANF. Dying Before Their Time III. 19-Year (1999-2017) Comparative Analysis of Excess Mortality in Detroit (Psa 1-a). Detroit, MI: Detroit Area Agency on Aging, 20 A.D. (2020) p. 1–28.
88. Hamel LM, Chapman R, Malloy M, Eggly S, Penner LA, Shields AF, et al. Critical Shortage of African American Medical Oncologists in the United States. J Clin Oncol (2015) 33:3697–700. doi: 10.1200/JCO.2014.59.2493
89. Shelton RC, Charles TA, Dunston SK, Jandorf L, Erwin DO. Advancing Understanding of the Sustainability of Lay Health Advisor (LHA) Programs for African-American Women in Community Settings. Transl Behav Med (2017) 7:415–26. doi: 10.1007/s13142-017-0491-3
90. Beebe-Dimmer JL, Albrecht TL, Baird TE, Ruterbusch JJ, Hastert T, Harper FWK, et al. The Detroit Research on Cancer Survivors (Rocs) Pilot Study: A Focus on Outcomes After Cancer in a Racially Diverse Patient Population. Cancer Epidemiol Biomarkers Prev (2019) 28:666–74. doi: 10.1158/1055-9965.EPI-18-0123
91. Beebe-Dimmer JL, Ruterbusch JJ, Harper FWK, Baird TM, Finlay DG, Rundle AG, et al. Physical Activity and Quality of Life in African American Cancer Survivors: The Detroit Research on Cancer Survivors Study. Cancer (2020) 126:1987–94. doi: 10.1002/cncr.32725
92. Hastert TA, Kyko JM, Reed AR, Harper FWK, Beebe-Dimmer JL, Baird TE, et al. Financial Hardship and Quality of Life Among African American and White Cancer Survivors: The Role of Limiting Care Due to Cost. Cancer Epidemiol Biomarkers Prev (2019) 28:1202–11. doi: 10.1158/1055-9965.EPI-18-1336
Keywords: disparities, co-morbidities, cancer treatment, physician-patient communication, socio-economic
Citation: Simon MS, Raychaudhuri S, Hamel LM, Penner LA, Schwartz KL, Harper FWK, Thompson HS, Booza JC, Cote M, Schwartz AG and Eggly S (2021) A Review of Research on Disparities in the Care of Black and White Patients With Cancer in Detroit. Front. Oncol. 11:690390. doi: 10.3389/fonc.2021.690390
Received: 02 April 2021; Accepted: 08 June 2021;
Published: 07 July 2021.
Edited by:
Farnam Mohebi, University of California, Berkeley, United StatesReviewed by:
Ahmed Abdalla Agab Eldour, Kordofan University, South SudanCopyright © 2021 Simon, Raychaudhuri, Hamel, Penner, Schwartz, Harper, Thompson, Booza, Cote, Schwartz and Eggly. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael S. Simon, c2ltb25tQGthcm1hbm9zLm9yZw==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.