
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 03 August 2021
Sec. Breast Cancer
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.686625
This article is part of the Research TopicBreast Cancer in Young WomenView all 18 articles
 Françoise Rothé1†
Françoise Rothé1† Matteo Lambertini2,3*†Oranite Goldrat4Marion Maetens1,5
Matteo Lambertini2,3*†Oranite Goldrat4Marion Maetens1,5 Yacine Bareche1Jeremy Blanc1Ghizlane Rouas1Denis Larsimont6Christos Sotiriou1,7
Yacine Bareche1Jeremy Blanc1Ghizlane Rouas1Denis Larsimont6Christos Sotiriou1,7 Michail Ignatiadis1,7‡
Michail Ignatiadis1,7‡ Isabelle Demeestere4,8‡
Isabelle Demeestere4,8‡Background: Current fertility preservation strategies for young breast cancer patients planning a future motherhood include the association of controlled ovarian stimulation with the aromatase inhibitor letrozole (let-COS) to harvest mature oocytes while maintaining low estradiol levels. Despite this is a widely adopted protocol, the safety of let-COS on breast cancer outcomes has been poorly investigated and its use remains off-label. We assessed the safety of let-COS in breast cancer patients using circulating tumor DNA (ctDNA) as a surrogate biomarker of disease recurrence.
Methods: BROVALE is an interventional non-randomized prospective study designed to evaluate the efficacy and safety of let-COS for fertility preservation in early breast cancer patients before starting (neo)adjuvant chemotherapy. Letrozole was administered throughout the COS cycle, until ovulation triggering. Safety was a secondary endpoint. Data on oncological outcomes were collected during the follow-up as well as plasma and whole blood for evaluation of ctDNA levels at the time of enrollment (i.e. before starting let-COS) and oocyte retrieval (i.e. 48 hours after the last administration of letrozole). Targeted gene sequencing on the primary tumor samples was performed to identify specific mutations used for ctDNA analysis by digital PCR. DNA extracted from whole blood samples was used to discriminate between somatic and germline mutations.
Results: From April 2014 to May 2017, 29 young early breast cancer patients enrolled in the BROVALE study who had available tissue samples participated to the ctDNA substudy. Among them, 15 had at least one validated somatic mutation. ctDNA was undetectable neither before nor after let-COS in 9 of them. Six patients had detectable ctDNA in the plasma samples collected before Let-COS. No change in ctDNA level after let-COS was observed in 3 patients and the level decreased (fold-change ≤ 0.5) in two women. One patient experienced an increased (fold-change ≥ 2) in ctDNA level but without disease relapse 34 months after diagnosis.
Conclusions: No increase in ctDNA level was observed in 93% (14/15) of the patients receiving let-COS supporting its use as a safe strategy for young women with early breast cancer interested in fertility preservation before chemotherapy.
Recent advances in screening procedures and anticancer treatments have markedly improved survival in young early breast cancer patients (1). The majority of young women with newly diagnosed early breast cancer are candidates to receive neoadjuvant or adjuvant chemotherapy including gonadotoxic drugs that might severely impact their reproductive function and future fertility (2, 3). Therefore, oncofertility counseling is currently mandatory in all patients diagnosed during their reproductive years and, for women planning a future motherhood, fertility preservation before starting chemotherapy is standard of care (4–6).
Oocyte and/or embryo cryopreservation is currently the first strategy for fertility preservation to be offered to young early breast cancer patients (7). The standard approach to collect a maximum number of mature oocytes includes 10-15 days of controlled ovarian stimulation (COS) with gonadotropins using a gonadotropin-releasing hormone (GnRH) antagonist protocol to avoid premature spontaneous luteinizing-hormone (LH) peak (8). As this protocol is associated with a supraphysiological raise in estradiol levels, concerns have been raised on its potential detrimental prognostic effect in hormone-sensitive cancer such as breast cancer (9, 10). The co-administration of an aromatase inhibitor (letrozole) during COS allows to harvest several mature oocytes while maintaining low estradiol levels (11–13). A recent meta-analysis of 11 studies comparing standard COS with protocols including the administration of letrozole confirmed a similar efficacy in terms of oocyte yield, maturation and fertilization rates, but with significantly reduced estradiol levels when letrozole is included in the COS protocol (14). Despite this is a widely adopted protocol, the safety of letrozole-associated COS (let-COS) on breast cancer outcomes has been poorly investigated and its use is currently off-label in this indication.
Liquid biopsy evaluating the presence of circulating tumor DNA (ctDNA) is widely used as a minimally invasive tool offering a wide range of clinical applications (15). Among them, the detection of ctDNA during follow-up has been shown to be associated with a high risk of disease relapse in patients with early breast cancer (16–19).
In this study, we aimed to explore the safety of let-COS for oocyte and/or embryo cryopreservation in a prospective cohort of young women with early breast cancer who preserved their fertility before chemotherapy. For this purpose, in addition to oncological outcomes, we explored potential changes in ctDNA levels before and after let-COS as a possible surrogate measure of tumor development and predictor of disease relapse.
BReast cancer OVAry LEtrozole (BROVALE) (NCT02661932) is an interventional non-randomized prospective study designed to evaluate the efficiency and safety of let-COS for fertility preservation in young women with early breast cancer. Details of the study have been previously reported (12). The present biomarker analysis addressed one of the planned secondary endpoints of the study focusing on the safety of let-COS. For this purpose, the changes in ctDNA levels before and after let-COS as well as oncological outcomes were assessed.
In BROVALE, standard or random start COS protocol using gonadotropins (150 to 300 IU/day) and GnRH antagonist (0.25mg/d from day 6, or when follicles reached 14 mm) was applied in all patients. GnRH agonist or human chorionic gonadotropin (hCG) were used for triggering when at least two follicles exceed 18mm and transvaginal ultrasound-guided oocyte retrieval occurred 36 hours later. Letrozole (5mg/day per os) was administered throughout the COS cycle, starting one day before or concomitantly with gonadotropins until ovulation triggering as previously described (12).
The Ethic Committee of Erasme Hospital approved the study. Informed consent was obtained from all participants before study inclusion.
Whole blood samples for genomic DNA preparation were collected in EDTA tubes at the time of enrollment (i.e. before let-COS) and at oocyte retrieval (i.e. 36 hours after last administration of letrozole). Plasma and whole blood were immediately stored at -80°c until DNA extraction. Formalin fixed paraffin embedded (FFPE) tumor samples were collected from participating patients.
Plasma cell-free DNA (cfDNA) was extracted using the QIAamp circulating nucleic acid kit (Qiagen). Genomic DNA was extracted from whole blood samples using the Qiagen DNeasy Blood & Tissue Kit to discriminate somatic from germline mutations. DNA from primary tumor samples (FFPE) was extracted using the Qiagen QIAamp DNA FFPE tissue kit.
Somatic mutations were identified from primary tumor samples by targeted gene sequencing using the Truseq Amplicon Cancer 48-gene Panel (Illumina, reference FC-130-1008). Sequence reads from the tumor and normal samples were aligned against the human genome reference version hg19/GRCh37 using the BWA (v.0.7.15) aligner with default parameter settings. In order to correct for mapping errors made by BWA around indels, a local realignment step was performed using IndelRealigner from the GATK (v.4.0.3.0) suite. When matched normal genomic DNA was available, somatic mutation calling was performed with two distinct variant callers, Manta (v.1.3.2)/Strelka (v.2.9.2) and Mutect 2 (v.4.0.3.0), using default parameters. When matched normal genomic DNA was not available, mutation calling was performed with two distinct variant callers, Pisces (v.5.1.6.54) & Mutect 2 (v.4.0.3.0), using default tumor mode only. Somatic mutations were annotated using ANNOVAR. Mutations were then filtered by selecting only exonic, non-synonymous single nucleotide variant (SNV) with a variant allele frequency (VAF) ≥ 8% and a coverage ≥ 1000 reads. Only known COSMIC (v.81) mutations with a frequency lower than 1% in the ExAC (v.0.3.1) database were used in further analysis.
The presence of plasma ctDNA was evaluated using the highly sensitive and precise digital PCR, a refined method of the conventional polymerase chain reaction (PCR). In particular, patient-specific droplet digital PCR (ddPCR) assays (Biorad PrimePCR ddPCR Mutation Assay or custom Assay) were used to detect the mutations identified in the tumor samples, with a single mutation being selected for each patient as previously reported (20).
Between April 2014 and May 2017, 31 early breast cancer patients with available tissue samples participated in the BROVALE ctDNA study. Two patients were excluded from further analysis due to low tumor DNA quantity (<50 ng; Supplementary Figure 1). All included patients underwent let-COS for fertility preservation before starting (neo)adjuvant chemotherapy. Out of 29 patients included in the present analysis, 12 (41.4%) had estrogen receptor (ER)-positive/HER2-negative tumors, 12 (41.4%) HER2-positive disease and 5 (17.2%) triple-negative breast cancer. Patients’ and oncological characteristics are summarized in Table 1.
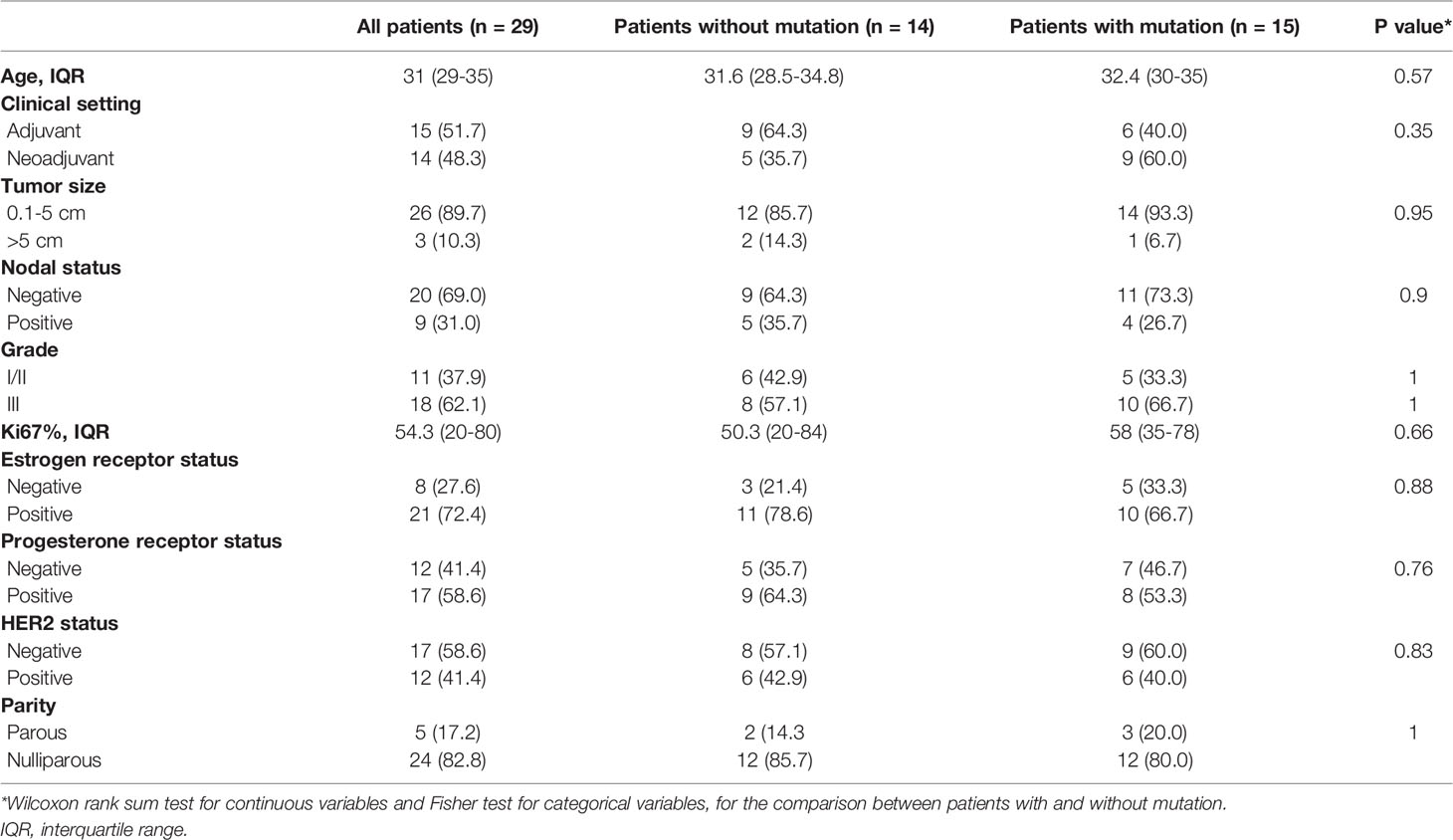
Table 1 Patients and tumor characteristics (n=29).
Targeted gene sequencing was performed on primary tumor samples of the 29 included patients in order to identify somatic mutations for subsequent plasma ctDNA detection. Sixteen (55%) tumor samples presented at least 1 somatic mutation either in TP53 (44.8%) or PIK3CA (17.2%) genes. No mutations could be identified in the other interrogated genes. A single mutation was selected for each of the 16 patients, being TP53 and PIK3CA mutations in 11 and 5 patients, respectively (Figures 1A, B). Fifteen of them (93.8%) were further validated using highly sensitive patient-specific mutation ddPCR assays with a high concordance being observed in the variant allelic frequency (VAF) between targeted gene sequencing and ddPCR (Figure 2).
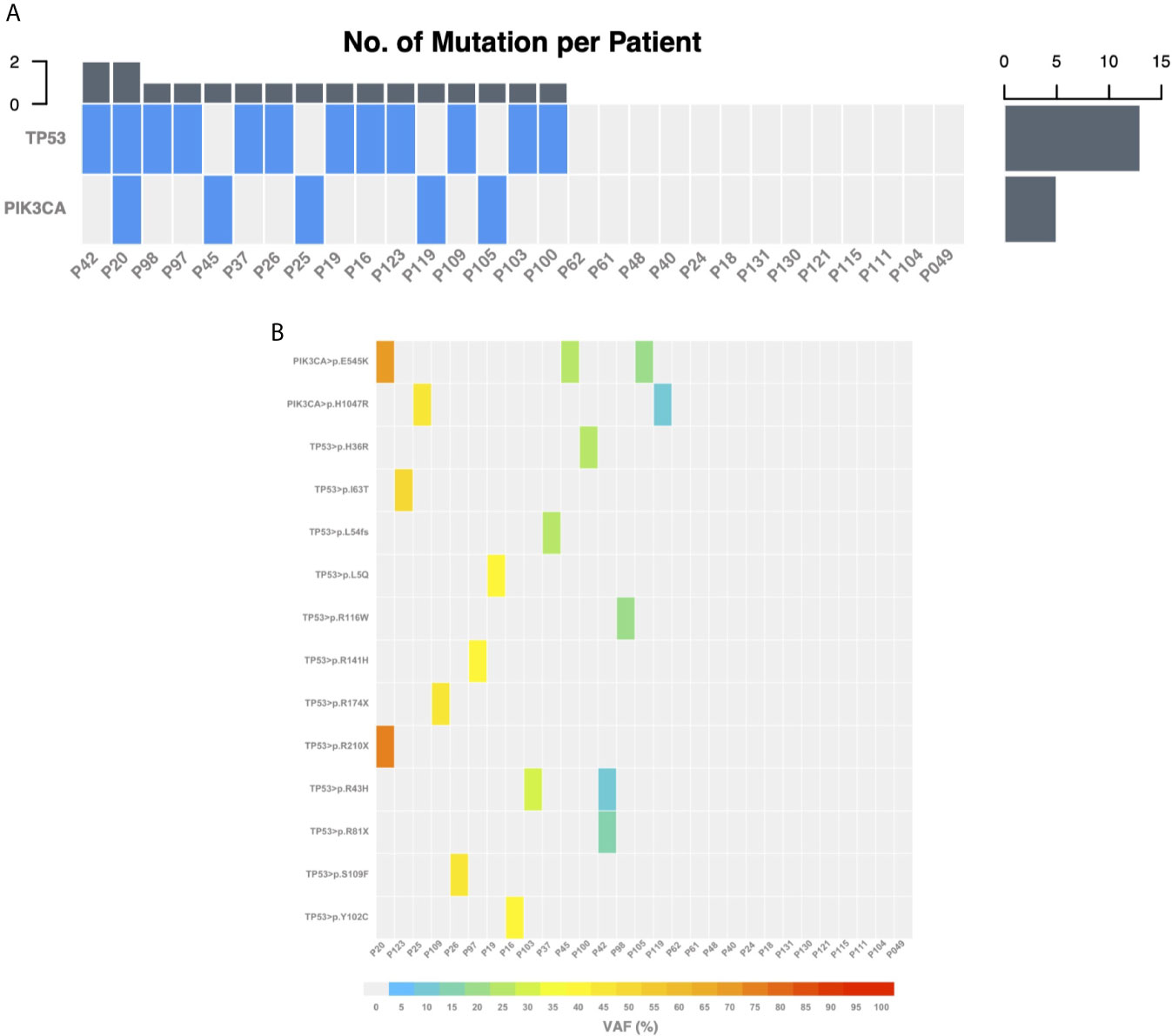
Figure 1 Somatic mutations identified using targeted gene sequencing on the primary tumor samples. (A) Heatmap of genes for which at least one mutation was indexed across the 29 patients. (B) Heatmap of the variant allele frequency for each specific mutation indexed across the 29 patients. VAF, variant allele frequency.
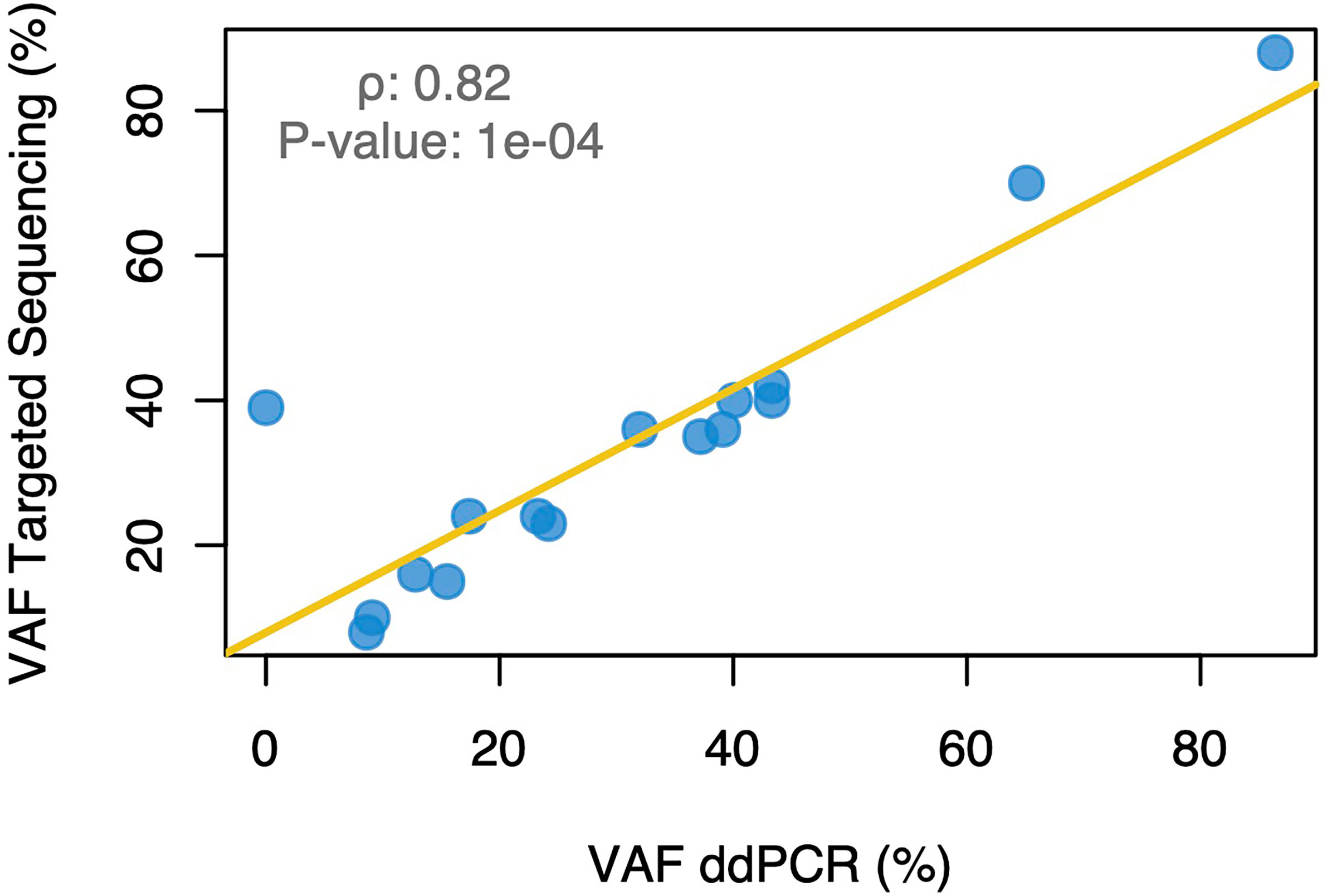
Figure 2 Correlation between the variant allele frequency of the somatic mutations identified using targeted gene sequencing and droplet digital PCR. VAF, variant allele frequency; ddPCR, droplet digital PCR.
For these 15 patients, the median duration of the stimulation was 9 days (range 5-14) and median estradiol peak reached 291pg/ml (range 55-928). A median of 6 mature oocytes were collected (range 1-21) (Table 2).
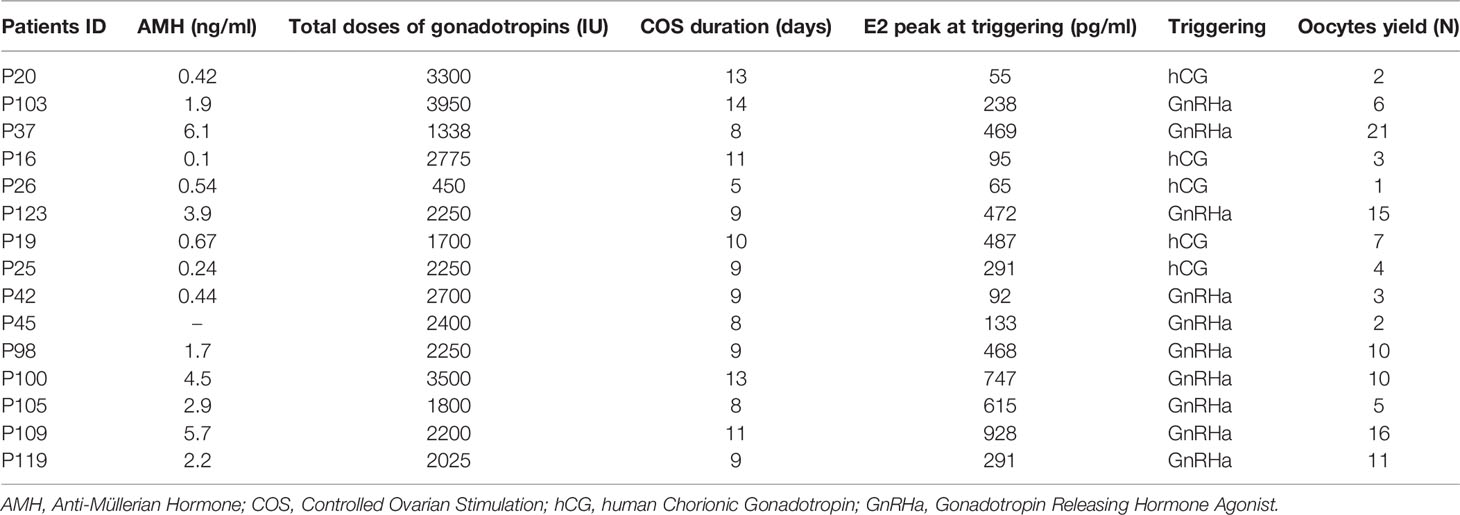
Table 2 Characteristics of the COS cycles.
The presence of ctDNA was assessed in the plasma samples collected before and after Let-COS using ddPCR. In 9 out of 15 patients, ctDNA was not detectable before nor after let-COS. None of them had disease relapse during follow-up (Table 3). Six patients had detectable ctDNA in the plasma samples collected before Let-COS (Figure 3). An increase in ctDNA level after let-COS (fold-change ≥ 2) was observed in only one patient without disease relapse at the last follow-up visit 34 months after breast cancer diagnosis (P123). On the contrary, 3 patients had no change in ctDNA level after let-COS (P103-P16-P26), one of whom developed disease-relapse after 13 months of follow-up and died (P26). This patient was diagnosed with triple-negative breast cancer (T2N2) and had the highest average number of mutated copies in the plasma before and after the procedure (427.03 and 467.67 ctDNA copies/ml, respectively). Other 2 patients (P20-P37) had a decrease in ctDNA level after let-COS (fold-change ≤ 0.5), one of whom developed disease-relapse (P37) (Table 3).
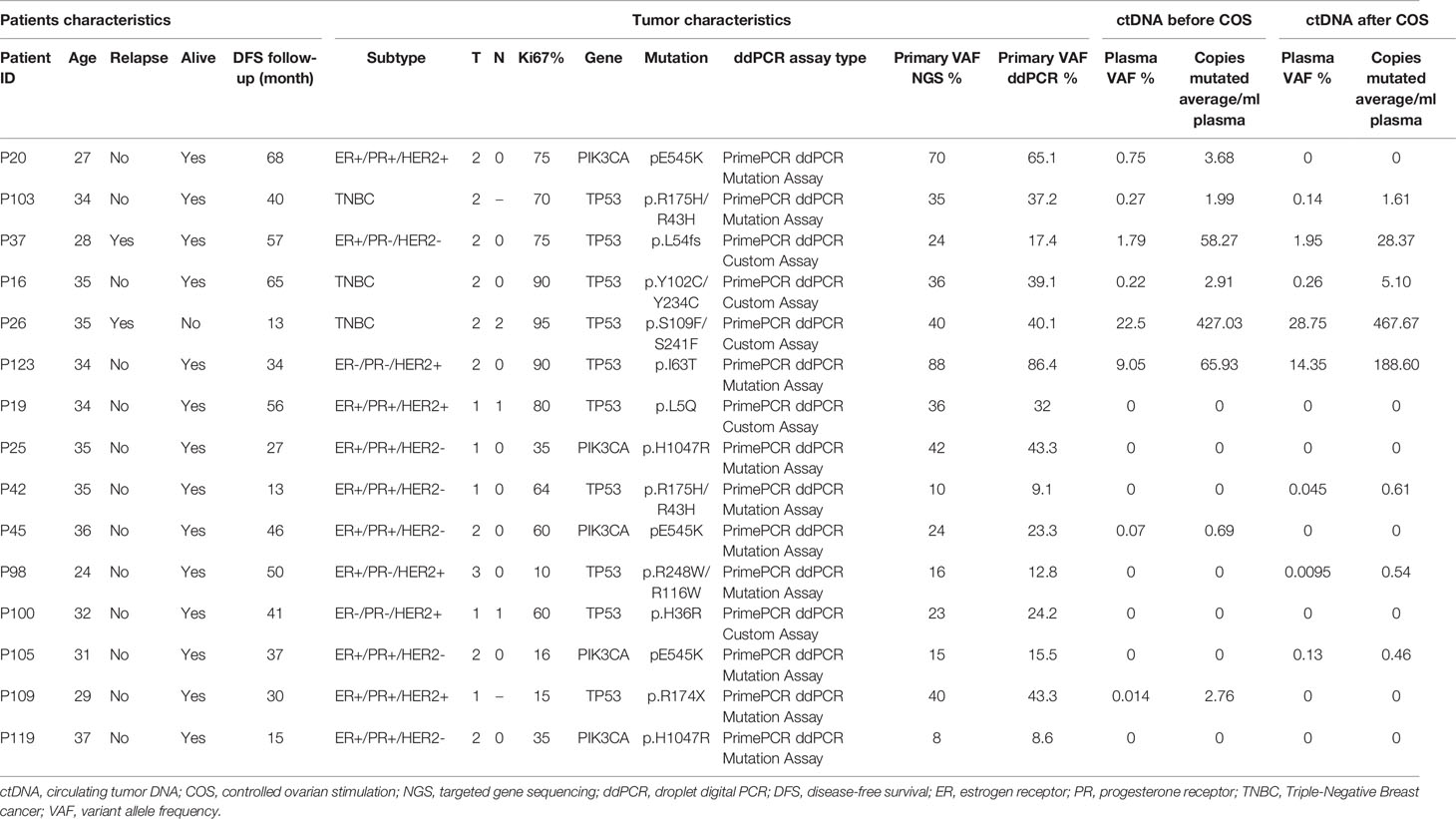
Table 3 Characteristics of the patients with identified mutations, targeted gene sequencing and droplet digital PCR results and changes in circulating tumor DNA before and after controlled ovarian stimulation (total n = 15).
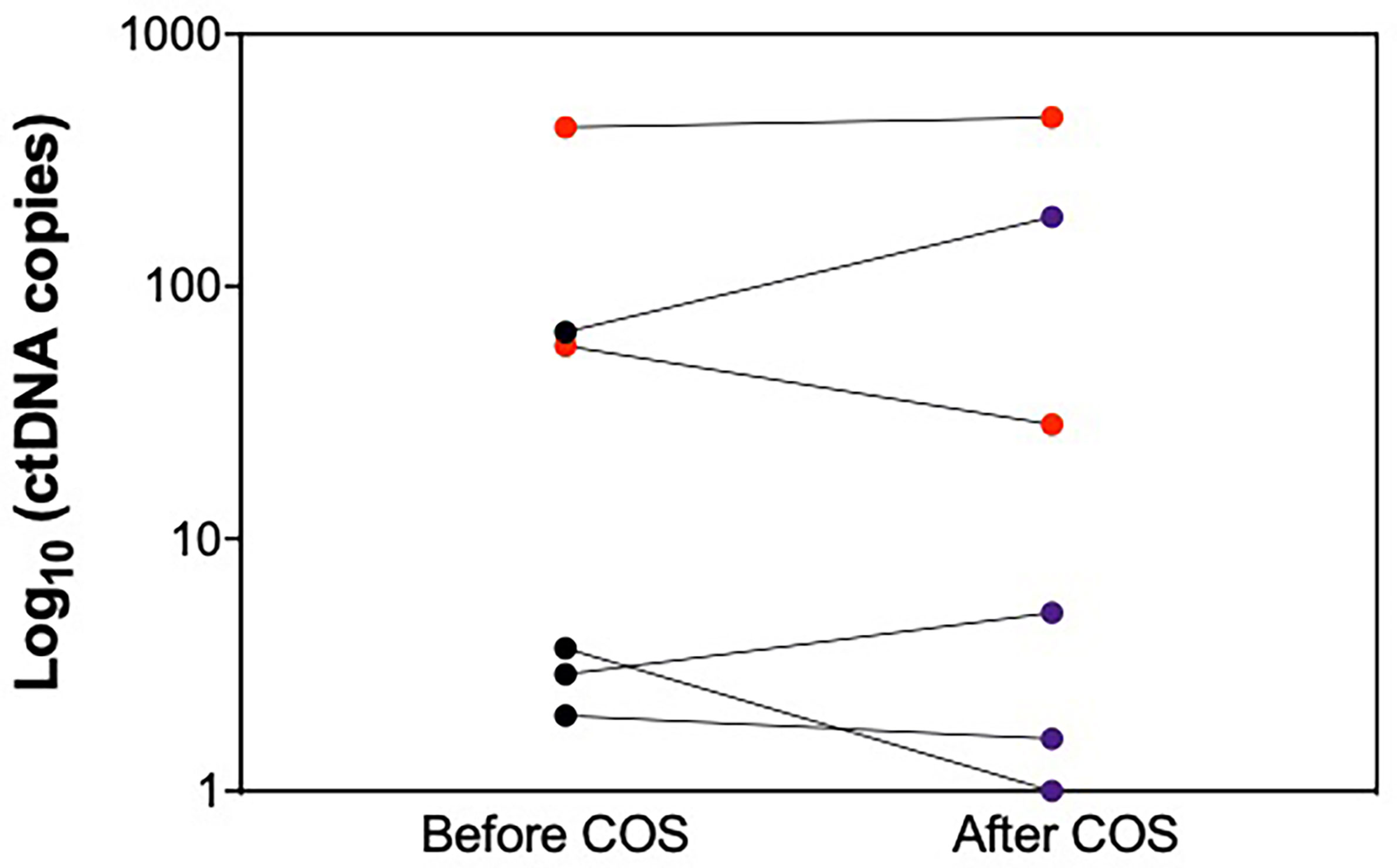
Figure 3 Changes in circulating tumor DNA levels between the time of enrollment (i.e. before starting letrozole-associated controlled ovarian stimulation) and oocyte retrieval (i.e. 48 hours after the last administration of letrozole). Red dots = disease relapse during oncologic follow-up. Violet = no disease relapse during oncologic follow-up. ctDNA, circulating tumor DNA; COS, controlled ovarian stimulation.
In young women with early breast cancer interested in preserving fertility before starting neoadjuvant or adjuvant chemotherapy, oocyte and/or embryo cryopreservation following Let-COS protocol is widely adopted and recommended (21–23). However, the safety of this approach relies mainly on one single-center prospective non-randomized study showing no difference in risk of recurrence between 120 breast cancer patients who performed Let-COS for oocyte and/or embryo cryopreservation and a control group of 217 patients who did not preserve their fertility before starting chemotherapy (13). In a recent large prospective multicenter Swedish study including 380 women with breast cancer who underwent COS for fertility preservation between 1995 and 2017, the 5-year survival proportion was similar compared to breast cancer patients who did not perform COS (24). In this study, Let-COS was offered to only 59% of the patients. Moreover, oncological characteristics of the population were not reported, leading to important potential biases in the survival analysis (24).
Therefore, defining the safety of performing COS for oocyte and/or embryo cryopreservation in breast cancer patients remains a clinical research priority (25). As shown in a recent survey involving breast cancer specialists, more than one third of them are concerned about the potential detrimental prognostic effect of COS in patients with breast cancer (10).
To our knowledge, this biomarker analysis is the first study addressing the safety of performing let-COS for fertility preservation in young breast cancer patients using ctDNA as a surrogate biomarker of disease recurrence. Indeed, among the wide range of clinical applications of this sensitive minimally invasive tool, molecular relapse detection is one of the most promising (16–19).
We first performed targeted gene sequencing in the primary tumors in order to identify the somatic mutations to be assessed for ctDNA detection in the plasma samples. Mutations were only present in TP53 and PIK3CA genes that are known to be the two most frequently mutated genes in breast cancer (26). Notably, 15 out of the 16 mutations identified in the primary tumors were further validated using ddPCR. In our study, ctDNA was detected in 40% of the plasma samples before let-COS and the initiation of chemotherapy. This is similar to previous studies reporting a detection rate of approximately 50% in patients with newly diagnosed early breast cancer irrespective of molecular subtype and prior to any treatment (27).
Reassuringly, let-COS did not induce the emergence of ctDNA in these patients, although the majority of patients had hormone receptor-positive disease and supraphysiological estradiol levels (>500pg/ml) were reached in a third of them. In our study, ctDNA was detected in 6 patients at enrollment but increased in only one of them. Importantly, no negative effect on her oncological outcomes was observed. Notably, the patient exhibiting the highest ctDNA level at both time-points relapsed shortly after entering the study and died. She was affected by triple-negative breast cancer and had the shortest stimulation duration characterized by very low estradiol levels during COS. On the contrary, all patients with undetectable or very low ctDNA levels remained disease-free at the time of the last follow-up. The observation that there was no increase in ctDNA levels in the majority of the patients indirectly supports the lack of potential detrimental prognostic effect of a short-course of hormonal manipulation with let-COS in young women with early breast cancer before exposure to chemotherapy.
In terms of study limitations, this biomarker analysis has a relatively limited sample size. Formal statistical calculations could not be performed. Moreover, despite promising, to date the role of ctDNA as a tool for disease monitoring in patients with early breast cancer remains experimental without direct clinical application yet. However, importantly, this analysis was conducted within an interventional non-randomized prospective study and all biological samples were prospectively collected.
In conclusion, this biomarker analysis of the BROVALE study showed no increase in ctDNA levels in 93% of young women with early breast cancer who received let-COS for oocyte and/or embryo cryopreservation as a strategy to preserve fertility before starting neoadjuvant or adjuvant chemotherapy. These data indirectly support the use of this strategy as a safe approach in young early breast cancer patients interested in fertility preservation before chemotherapy initiation. Further validation of these findings in a large prospective clinical trial is warranted.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
This study involving human participants was reviewed and approved by Erasme Hospital. The patients/participants provided their written informed consent to participate in this study.
FR, ML, MI, and ID contributed to the conception and design of the study. OG and ID contributed to patients’ enrollment in the BROVALE study and sample collection. FR, ML, MM, YB, JB, GR, DL, CS, and MI contributed to sample storage, processing, analysis and interpretation. The results were interpreted by FR, ML, MI, and ID. The initial manuscript was drafted by FR, ML, MI, and ID. All authors contributed to the article and approved the submitted version.
This study received partial financial support from the Belgian Fund for Scientific Research (FNRS)-Operation Télévie (grant number: 7452815F), Fonds Erasme (no grant number), and by an ESMO Translational Research Fellowship grant (no grant number). ML is supported by the Italian Ministry of Health - 5 x 1000 funds 2017 (no grant number) and the Italian Association for Cancer Research (AIRC; grant number MFAG 2020 ID 24698) for pursuing in his research efforts in the field of oncofertility.
ML acted as a consultant for Roche, AstraZeneca, Novartis, and Lilly, and received honoraria from Roche, Lilly, Novartis, Pfizer, Sandoz, and Takeda outside the submitted work. MI acted as a consultant for Novartis, and Seattle Genetics, and his Institution received research grants from Roche, Pfizer and Natera Inc. ID acted as a consultant for Roche and received speaker’s fees from Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer FS declared a past co-authorship with one of the authors ML to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ML acknowledges the support from the European Society for Medical Oncology (ESMO) for a Translational Research Fellowship at the Institut Jules Bordet (Brussels, Belgium) during the conduction of this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.686625/full#supplementary-material
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin (2021) 71(1):7–33. doi: 10.3322/caac.21654
2. Partridge AH, Hughes ME, Warner ET, Ottesen RA, Wong Y-N, Edge SB, et al. Subtype-Dependent Relationship Between Young Age at Diagnosis and Breast Cancer Survival. J Clin Oncol (2016) 34(27):3308–14. doi: 10.1200/JCO.2015.65.8013
3. Lambertini M, Pinto AC, Ameye L, Jongen L, Del Mastro L, Puglisi F, et al. The Prognostic Performance of Adjuvant! Online and Nottingham Prognostic Index in Young Breast Cancer Patients. Br J Cancer (2016) 115(12):1471–8. doi: 10.1038/bjc.2016.359
4. Oktay K, Harvey BE, Partridge AH, Quinn GP, Reinecke J, Taylor HS, et al. Fertility Preservation in Patients With Cancer: Asco Clinical Practice Guideline Update. J Clin Oncol (2018) 36(19):1994–2001. doi: 10.1200/JCO.2018.78.1914
5. Lambertini M, Peccatori FA, Demeestere I, Amant F, Wyns C, Stukenborg J-B, et al. Fertility Preservation and Post-Treatment Pregnancies in Post-Pubertal Cancer Patients: ESMO Clinical Practice Guidelines†. Ann Oncol (2020) 31(12):1664–78. doi: 10.1016/j.annonc.2020.09.006
6. ESHRE Guideline Group on Female Fertility Preservation, Anderson RA, Amant F, Braat D, D’Angelo A, Chuva de Sousa Lopes SM, et al. ESHRE Guideline: Female Fertility Preservation. Hum Reprod Open (2020) 2020(4):hoaa052. doi: 10.1093/hropen/hoaa052
7. Razeti MG, Spinaci S, Spagnolo F, Massarotti C, Lambertini M. How I Perform Fertility Preservation in Breast Cancer Patients. ESMO Open (2021) 6(3):100112. doi: 10.1016/j.esmoop.2021.100112
8. Lambertini M, Pescio MC, Viglietti G, Goldrat O, Mastro LD, Anserini P, et al. Methods of Controlled Ovarian Stimulation for Embryo/Oocyte Cryopreservation in Breast Cancer Patients. Expert Rev Qual Life Cancer Care (2017) 2(1):47–59. doi: 10.1080/23809000.2017.1270760
9. Biglia N, Torrisi R, D’Alonzo M, Codacci Pisanelli G, Rota S, Peccatori FA. Attitudes on Fertility Issues in Breast Cancer Patients: An Italian Survey. Gynecol Endocrinol (2015) 31(6):458–64. doi: 10.3109/09513590.2014.1003293
10. Lambertini M, Di Maio M, Pagani O, Curigliano G, Poggio F, Del Mastro L, et al. The BCY3/BCC 2017 Survey on Physicians’ Knowledge, Attitudes and Practice Towards Fertility and Pregnancy-Related Issues in Young Breast Cancer Patients. Breast (2018) 42:41–9. doi: 10.1016/j.breast.2018.08.099
11. Oktay K, Turan V, Bedoschi G, Pacheco FS, Moy F. Fertility Preservation Success Subsequent to Concurrent Aromatase Inhibitor Treatment and Ovarian Stimulation in Women With Breast Cancer. J Clin Oncol (2015) 33(22):2424–9. doi: 10.1200/JCO.2014.59.3723
12. Goldrat O, Gervy C, Englert Y, Delbaere A, Demeestere I. Progesterone Levels in Letrozole Associated Controlled Ovarian Stimulation for Fertility Preservation in Breast Cancer Patients. Hum Reprod (2015) 30(9):2184–9. doi: 10.1093/humrep/dev155
13. Kim J, Turan V, Oktay K. Long-Term Safety of Letrozole and Gonadotropin Stimulation for Fertility Preservation in Women With Breast Cancer. J Clin Endocrinol Metab (2016) 101(4):1364–71. doi: 10.1210/jc.2015-3878
14. Bonardi B, Massarotti C, Bruzzone M, Goldrat O, Mangili G, Anserini P, et al. Efficacy and Safety of Controlled Ovarian Stimulation With or Without Letrozole Co-administration for Fertility Preservation: A Systematic Review and Meta-Analysis. Front Oncol (2020) 10:574669. doi: 10.3389/fonc.2020.574669
15. De Mattos-Arruda L, Siravegna G. How to Use Liquid Biopsies to Treat Patients With Cancer. ESMO Open (2021) 266(2):100060. doi: 10.1016/j.esmoop.2021.100060
16. Garcia-Murillas I, Schiavon G, Weigelt B, Ng C, Hrebien S, Cutts RJ, et al. Mutation Tracking in Circulating Tumor DNA Predicts Relapse in Early Breast Cancer. Sci Transl Med (2015) 7(302):302ra133. doi: 10.1126/scitranslmed.aab0021
17. Olsson E, Winter C, George A, Chen Y, Howlin J, Tang M-HE, et al. Serial Monitoring of Circulating Tumor DNA in Patients With Primary Breast Cancer for Detection of Occult Metastatic Disease. EMBO Mol Med (2015) 7(8):1034–47. doi: 10.15252/emmm.201404913
18. Coombes RC, Page K, Salari R, Hastings RK, Armstrong A, Ahmed S, et al. Personalized Detection of Circulating Tumor DNA Antedates Breast Cancer Metastatic Recurrence. Clin Cancer Res (2019) 25(14):4255–63. doi: 10.1158/1078-0432.CCR-18-3663
19. Garcia-Murillas I, Chopra N, Comino-Méndez I, Beaney M, Tovey H, Cutts RJ, et al. Assessment of Molecular Relapse Detection in Early-Stage Breast Cancer. JAMA Oncol (2019) 5(10):1473–8. doi: 10.1001/jamaoncol.2019.1838
20. Rothé F, Silva MJ, Venet D, Campbell C, Bradburry I, Rouas G, et al. Circulating Tumor DNA in HER2-Amplified Breast Cancer: A Translational Research Substudy of the NeoALTTO Phase III Trial. Clin Cancer Res (2019) 25(12):3581–8. doi: 10.1158/1078-0432.CCR-18-2521
21. Ruddy KJ, Gelber SI, Tamimi RM, Ginsburg ES, Schapira L, Come SE, et al. Prospective Study of Fertility Concerns and Preservation Strategies in Young Women With Breast Cancer. J Clin Oncol (2014) 32(11):1151–6. doi: 10.1200/JCO.2013.52.8877
22. Ruggeri M, Pagan E, Bagnardi V, Bianco N, Gallerani E, Buser K, et al. Fertility Concerns, Preservation Strategies and Quality of Life in Young Women With Breast Cancer: Baseline Results From an Ongoing Prospective Cohort Study in Selected European Centers. Breast (2019) 47:85–92. doi: 10.1016/j.breast.2019.07.001
23. Blondeaux E, Massarotti C, Fontana V, Poggio F, Arecco L, Fregatti P, et al. The PREgnancy and FERtility (PREFER) Study Investigating the Need for Ovarian Function and/or Fertility Preservation Strategies in Premenopausal Women With Early Breast Cancer. Front Oncol (2021) 11:690320. doi: 10.3389/fonc.2021.690320
24. Marklund A, Eloranta S, Wikander I, Kitlinski ML, Lood M, Nedstrand E, et al. Efficacy and Safety of Controlled Ovarian Stimulation Using GnRH Antagonist Protocols for Emergency Fertility Preservation in Young Women With Breast Cancer-a Prospective Nationwide Swedish Multicenter Study. Hum Reprod (2020) 35(4):929–38. doi: 10.1093/humrep/deaa029
25. Arecco L, Perachino M, Damassi A, Latocca MM, Soldato D, Vallome G, et al. Burning Questions in the Oncofertility Counseling of Young Breast Cancer Patients. Breast Cancer (Auckl) (2020) 14:1178223420954179. doi: 10.1177/1178223420954179
26. Nik-Zainal S, Davies H, Staaf J, Ramakrishna M, Glodzik D, Zou X, et al. Landscape of Somatic Mutations in 560 Breast Cancer Whole-Genome Sequences. Nature (2016) 534(7605):47–54. doi: 10.1038/nature17676
Keywords: breast cancer, fertility preservation, letrozole, ovarian stimulation, circulating tumor DNA
Citation: Rothé F, Lambertini M, Goldrat O, Maetens M, Bareche Y, Blanc J, Rouas G, Larsimont D, Sotiriou C, Ignatiadis M and Demeestere I (2021) Circulating Tumor DNA to Interrogate the Safety of Letrozole-Associated Controlled Ovarian Stimulation for Fertility Preservation in Breast Cancer Patients. Front. Oncol. 11:686625. doi: 10.3389/fonc.2021.686625
Received: 27 March 2021; Accepted: 19 July 2021;
Published: 03 August 2021.
Edited by:
Luigi Formisano, University of Naples Federico II, ItalyReviewed by:
Umberto Malapelle, University of Naples Federico II, ItalyCopyright © 2021 Rothé, Lambertini, Goldrat, Maetens, Bareche, Blanc, Rouas, Larsimont, Sotiriou, Ignatiadis and Demeestere. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matteo Lambertini, bWF0dGVvLmxhbWJlcnRpbmlAdW5pZ2UuaXQ=
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.