 Aini Hyytiäinen1,2
Aini Hyytiäinen1,2 Wafa Wahbi1,2
Wafa Wahbi1,2 Otto Väyrynen1
Otto Väyrynen1 Kauko Saarilahti3
Kauko Saarilahti3 Peeter Karihtala4
Peeter Karihtala4 Tuula Salo1,2,5,6,7
Tuula Salo1,2,5,6,7 Ahmed Al-Samadi1,2*
Ahmed Al-Samadi1,2*- 1Department of Oral and Maxillofacial Diseases, Clinicum, University of Helsinki, Helsinki, Finland
- 2Translational Immunology Programme, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 3Department of Oncology, Helsinki University Hospital and University of Helsinki, Helsinki, Finland
- 4Department of Oncology, Helsinki University Hospital Comprehensive Cancer Centre and University of Helsinki, Helsinki, Finland
- 5Department of Pathology, University of Helsinki, Helsinki, Finland
- 6Cancer Research and Translational Medicine Research Unit, University of Oulu, Oulu, Finland
- 7Oulu Medical Research Centre, Oulu University Hospital, University of Oulu, Oulu, Finland
Background: Head and neck squamous cell carcinoma (HNSCC) carries poor survival outcomes despite recent progress in cancer treatment in general. Angiogenesis is crucial for tumour survival and progression. Therefore, several agents targeting the pathways that mediate angiogenesis have been developed. We conducted a systematic review to summarise the current clinical trial data examining angiogenesis inhibitors in HNSCC.
Methods: We carried out a literature search on three angiogenesis inhibitor categories—bevacizumab, tyrosine kinase inhibitors and endostatin—from Ovid MEDLINE, Cochrane Library, Scopus and ClinicalTrials.gov database.
Results: Here, we analysed 38 clinical trials, total of 1670 patients, investigating 12 angiogenesis inhibitors. All trials were in phase I or II, except one study in phase III on bevacizumab. Angiogenesis inhibitors were used as mono- and combination therapies together with radio-, chemo-, targeted- or immunotherapy. Among 12 angiogenesis inhibitors, bevacizumab was the most studied drug, included in 13 trials. Although bevacizumab appeared effective in various combinations, it associated with high toxicity levels. Endostatin and lenvatinib were well-tolerated and their anticancer effects appeared promising.
Conclusions: Most studies did not show benefit of angiogenesis inhibitors in HNSCC treatment. Additionally, angiogenesis inhibitors were associated with considerable toxicity. However, some results appear encouraging, suggesting that further investigations of angiogenesis inhibitors, particularly in combination therapies, for HNSCC patients are warranted.
Systematic Review Registration: PROSPERO (https://www.crd.york.ac.uk/prospero/), identifier CRD42020157144.
Introduction
Head and neck squamous cell carcinoma (HNSCC) is the eighth most common neoplasm worldwide with more than 600 000 new cases and 350 000 deaths reported in 2018 (1). HNSCC can arise from subsites within the oral cavity, oropharynx, hypopharynx, larynx and nasopharynx (2). The most common risk factors include excess tobacco and alcohol consumption and human papillomavirus (HPV) infection (2). Currently, the primary treatment of HNSCC patients consists of surgery and (chemo-) radiotherapy either alone or in combination (3). Despite intensive research and progress in cancer therapy, survival outcomes in patients with locoregionally advanced disease remains poor, with a five-year overall survival (OS) rate reaching only around 50% (4).
Angiogenesis (neo-angiogenesis, new blood vessel formation) is crucial for tumour growth, invasion and metastasis (5). Angiogenesis is a hallmark of tumour progression and has been studied in many cancer types, including HNSCC (6). Angiogenesis is primarily mediated by the vascular endothelial growth factor (VEGF) pathway (7). Two major categories of agents have been developed to target this pathway: antibody-based agents and VEGF receptor tyrosine kinase inhibitors (TKIs) (6). The US Food and Drug Administration (US FDA) has approved several anti-angiogenic agents to treat solid tumours, such as colorectal cancer, renal cell carcinoma, ovarian cancer, gastric cancer and thyroid cancer (7). Contrary to concerns that angiogenesis inhibitors could increase hypoxia and lead to treatment resistance, these inhibitors in preclinical models appear to overcome resistance and preclinically synergise with traditional therapies such as radiation (8). Paradoxically, such therapies normalise tumour vasculature, increase tumour blood flow and reduce hypoxia, and, thus, carry synergistic effects with radiation and chemotherapy (8, 9).
Despite the crucial role of angiogenesis in HNSCC, as yet no anti-angiogenic agent enjoys clinical use for these patients, and conclusive data from clinical trials on anti-angiogenic drugs in HNSCC remain unavailable. This systematic review aims to summarise the current data from clinical trials on three angiogenesis inhibitor categories (bevacizumab, TKIs and endostatin) in HNSCC patients.
Materials and Methods
Protocol and Registration
This review was registered at the international prospective register of systematic reviews PROSPERO (https://www.crd.york.ac.uk/prospero/) under registration number CRD42020157144.
Search Strategy
Since there is no clear definition of angiogenesis inhibitors and several compounds with anti-angiogenic effects together with other antitumour effects exist, here we included only the three primary classifications of angiogenesis inhibitors: bevacizumab, TKIs and endostatin.
We conducted a literature search in November 2019 using three databases (Ovid MEDLINE, Cochrane Library and Scopus) and the National Library of Medicine website (https://ClinicalTrials.gov). We conducted a literature search in November 2019 using three databases (Ovid MEDLINE, Cochrane Library and Scopus) and the National Library of Medicine website (https://ClinicalTrials.gov). We used the following search terms: (“head and neck cancer” OR “head and neck squamous cell carcinoma”) AND (“angiogenesis inhibitors” OR bevacizumab OR avastin OR “Bayer 205” OR semaxanib OR su5416 OR thrombospondin OR abt-510 OR pazopanib OR votrient OR sunitinib OR su11248 OR su11248 OR sorafenib OR nexavar OR ranibizumab OR lucenti OR endostatin OR ramucirumab OR cyramza OR vandetanib OR zd6474 OR zactima OR axitinib OR inlyta OR cabozantinib OR cometriq OR cabometyx OR lenvatinib OR lenvima OR regorafenib OR ziv-aflibercept OR zaltrap OR “VEGFR antagonists” OR VEGF OR “vascular endothelial growth factor”) AND (“randomized controlled trials” OR “clinical trials”). We gathered the search results in Mendeley, and used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to illustrate the results in a flowchart (10). We excluded any duplicates and articles that did not meet the listed inclusion criteria (Supplementary Table 1). Three independent researchers (AH, WW and OV) carried out the literature search, screened all retrieved article titles and abstracts, discarded duplicates and verified that the included articles satisfied our inclusion criteria. Three articles were published after the search was completed (11–13) and were subsequently added to our review.
Data Extraction
For the included articles, we extracted the following information: (1) basic article information including first author, publication year, trial year, trial phase, treatment setting and follow-up time period; (2) patient and tumour characteristics including the number of patients treated and the cancer type; (3) trial methods including regimens for each treatment arm and evaluation criteria; (4) treatment effect and survival information including complete response rate (CR), partial response rate (PR), overall response rate (ORR), stable disease (SD), progressive disease (PD), disease control rate (DCR), overall survival (OS) and progression-free survival (PFS); (5) toxicity of the treatment; and (6) study conclusions.
Results
Search Results
We found a total of 373 articles from our database search (234 from Ovid MEDLINE, 84 from Cochrane Library and 55 from Scopus), 62 from our ClinicalTrials.gov search and three articles were published after the initial search and subsequently added to the systematic review (Figure 1). From these, 38 articles met the inclusion criteria and were included in this systematic review. All clinical trials were carried out on patients with recurrent, metastatic or locally advanced HNSCC.
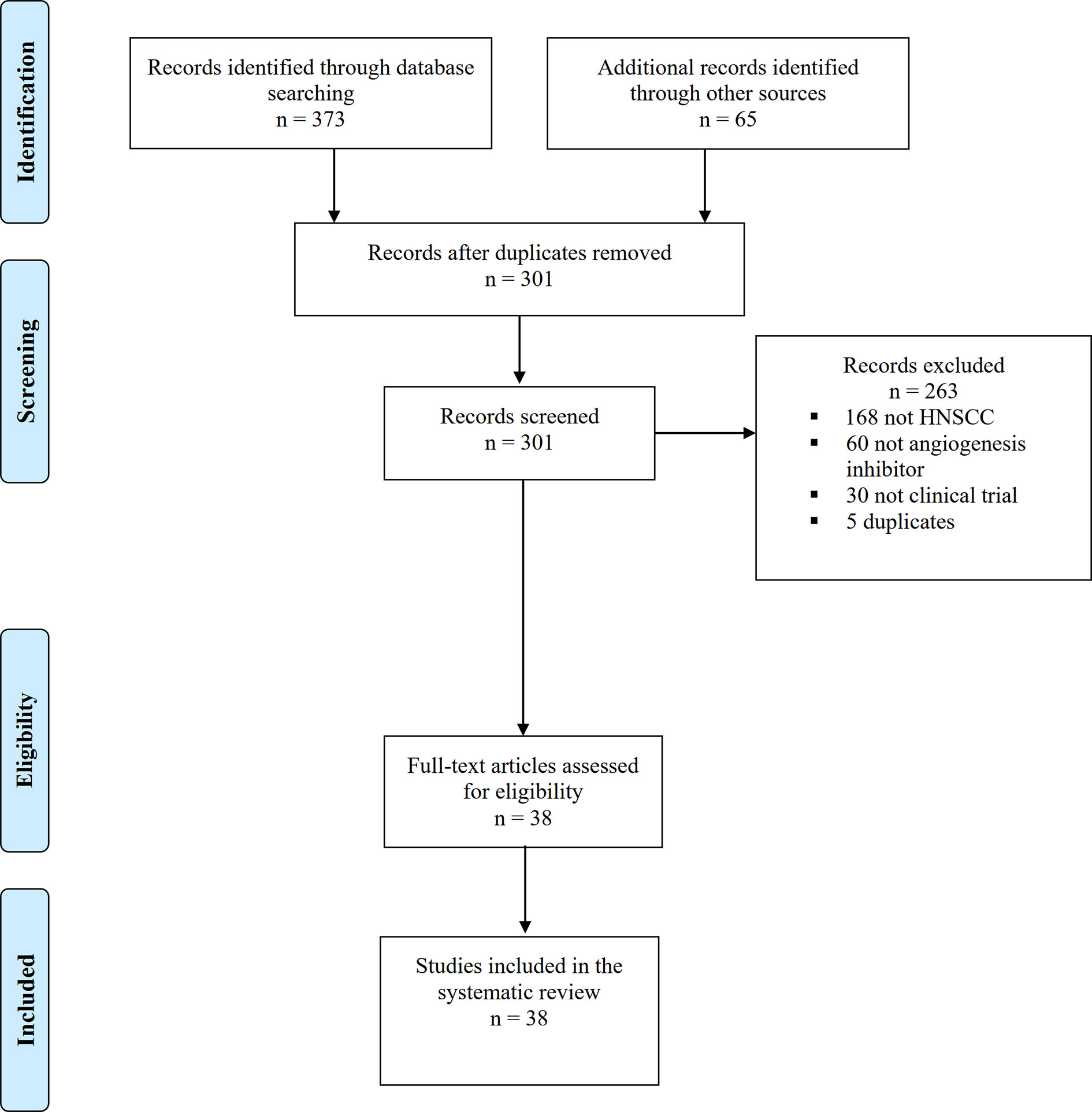
Figure 1 PRISMA flow chart with search results and studies included and excluded in different steps.
Bevacizumab
Bevacizumab, the first US FDA-approved angiogenesis inhibitor, is a humanised monoclonal antibody against VEGF-A. Approved by the US-FDA as a first-line treatment for metastatic colorectal cancer and for other malignancies such as advanced non-squamous non-small cell lung cancer (NSCLC), ovarian cancer, renal cell carcinoma (RCC) and glioblastoma multiforme, it is used alone or in combination with other treatments (14, 15). Bevacizumab was the most frequently studied angiogenesis inhibitor in HNSCC featured in a total of 13 trials among 866 patients (Table 1). The largest trial was a phase III (11), while the remainder were phase I or II trials. Eleven trials used bevacizumab as a first-line treatment, one trial used it as a first- or second-line treatment and one trial used it as second-line treatment. Bevacizumab was used in combination with different therapies administered in doses of 10–15 mg/kg.
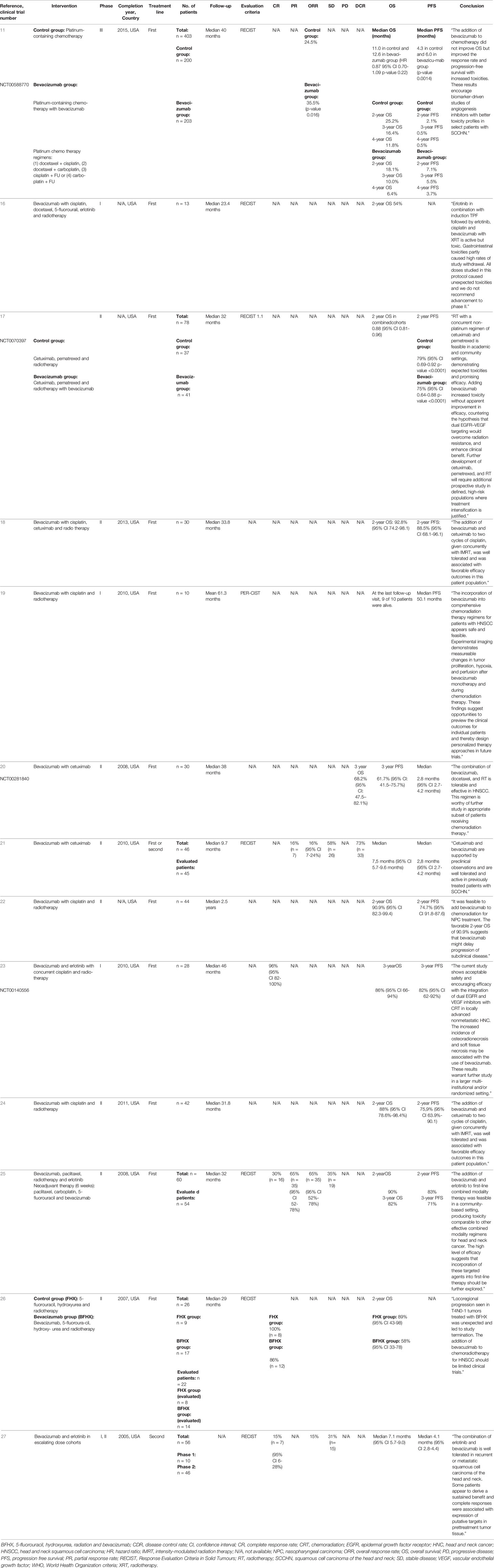
Table 1 Summary of the bevacizumab clinical trials for head and neck squamous cell carcinoma.
In the phase III study, 403 patients were randomly assigned to receive platinum-based chemotherapy with or without bevacizumab as a first-line treatment (11). There was a minor but statistically nonsignificant increase in median OS (median OS with chemotherapy 11.0 months and with the addition of bevacizumab 12.6 months; hazard ratio (HR) 0.87; 95% CI 0.70–1.09; p=0.22). The addition of bevacizumab to chemotherapy improved PFS and response rates significantly. Median PFS was 6.0 months with bevacizumab + chemotherapy and 4.3 months with chemotherapy alone (p=0.0014). ORR was 35.5% in the bevacizumab + chemotherapy group and 24.5% in the chemotherapy only group (p=0.016). The addition of bevacizumab increased toxicities.
Four trials, three as first-line treatment, combined bevacizumab and epidermal growth factor TKI erlotinib with different types of chemotherapy or chemoradiotherapy. The combination of bevacizumab, erlotinib and chemoradiotherapy (cisplatin, docetaxel and 5-fluorouracil) was active, but toxic (16). In this phase I study, gastrointestinal toxicities caused high rates of patient withdrawal and the combination was not recommended to advance to phase II (16). The other studies with bevacizumab and erlotinib, however, showed more promising results. Bevacizumab and erlotinib with concurrent cisplatin and radiotherapy demonstrated an encouraging efficacy with acceptable safety in nonmetastatic, locally advanced HNSCC (23). Complete response rates were achieved in 96% of patients (95% CI 82–100%) and 3-year OS and PFS reached 86% and 82%, respectively (95% CI 66–94% and 62–92%) (23). Neoadjuvant therapy (6 weeks) consisting of paclitaxel, carboplatin, 5-fluorouracil and bevacizumab followed by bevacizumab and erlotinib in combination with radiotherapy and paclitaxel showed good efficacy and proved safe (25). ORR was 65% (95% CI 52–78%) and 2-year OS and PFS were 90% and 83%, respectively (95% CI 78.6–98.4% and 63.9–90.1%). Bevacizumab and erlotinib were also studied in escalating dose cohorts as the second-line treatment for metastatic or recurrent HNSCC (27). The combination was well-tolerated with a median OS of 7.1 months (95% CI 5.7–9.0 months) and PFS of 4.1 months (95% CI 2.8–4.4 months) (27).
In addition, bevacizumab was combined with cetuximab in three trials. The addition of bevacizumab to cetuximab, pemetrexed and radiotherapy as a first-line treatment increased toxicities without apparent improvement in efficacy (17). Moreover, 2-year PFS was 79% with cetuximab + chemoradiotherapy and 75% when bevacizumab was added (95% CI 0.69–0.92%for the control group and 0.64–0.88% for the bevacizumab group) (17). Bevacizumab and cetuximab with cisplatin and radiotherapy as a first-line treatment was well-tolerated with favourable survival rates, where 2-year OS and PFS reached 92.8% and 88.5%, respectively (95% CI 74.21–98.1% and 68.1–96.1%) (18). In a clinical trial examining bevacizumab and cetuximab in metastatic or recurrent HNSCC as the first- or second-line treatment, an ORR of 16% was reported (95% CI 7–24%) with a median OS and PFS of 7.5 and 2.8 months, respectively (95% CI 5.7–9.6 and 2.7–4.2 months). The treatment was well-tolerated (21).
In five clinical trials, bevacizumab was combined with chemoradiation as a first-line treatment. Bevacizumab with 5-fluorouracil, hydroxyurea and radiotherapy proved toxic and the study was interrupted early after adding bevacizumab to chemoradiation led to acute toxicity (26). The CR rate with chemoradiation alone was 100% compared to 86% when chemoradiation was combined with bevacizumab. In addition, 2-year OS reached 89% (95% CI 43–98%) in the control group falling to 58% (95% CI 33–78%) in the bevacizumab group (26). Other trials reported more promising results. For instance, bevacizumab combined with docetaxel and radiotherapy was well-tolerated and effective with a 3-year OS of 68.2% (95% CI 47.5–82.1%) and a PFS of 61.7% (95% CI 41.5–75.7%) (20). Adding bevacizumab to cisplatin and radiotherapy was also well-tolerated and studied in three trials. In a phase II trial, 2-year OS was 88% (95% CI 78.6–98.4%), while 2-year PFS was 75.9% (95% CI 63.9–90.1%) (24). Another phase II trial also reported encouraging survival rates of a similar magnitude: 2-year OS was 90.9% (95% CI 82.3–99.4%) and 2-year PFS was 74.7% (95% CI 91.8–87.6%) (22). Finally, a phase I trial reported a median PFS of 50.1 months (19).
To summarise, three studies with bevacizumab reported significant toxicities with no treatment efficacy: one in combination with erlotinib and chemoradiotherapy, one with cetuximab and chemoradiotherapy and one with chemoradiotherapy. The other ten trials reported more acceptable safety profiles and efficacy. Supplementary Table 2 summarises the toxicity analysis of bevacizumab.
Sorafenib
Sorafenib (BAY-43-9006) is an anticancer drug approved by the US FDA to treat unresectable hepatocellular carcinoma, radioactive iodine refractory thyroid cancer and advanced renal cell carcinoma (28). The anticancer effects of sorafenib are mediated primarily by targeting both the RAF/MEK/ERK pathway and the receptor tyrosine kinases, including VEGFR (VEGFR-1, VEGFR-2 and VEGFR-3), platelet-derived growth factor receptor (PDGFR), FLT3, Ret and c-KIT (29, 30).
Sorafenib was studied in 5 phase II clinical trials among a total of 201 patients (Table 2) three times as a monotherapy and twice in combination with cisplatin, 5-fluorouracil and cetuximab. The sorafenib dose across all trials was 400-mg twice daily as a continuous treatment. As a single agent in the first- or second-line advanced setting, ORR of 3.7% was reported (95% CI 0.1–19%) with a median OS of 4.2 months (95% CI 3.6–8.7 months) (35). In the other two monotherapy studies, ORR was not reported, although the median OS was 8.0 months when administered to patients who primarily received previous chemo- and/or radiotherapy and 9.0 months when administered as a first-line treatment (95% CI 2.4–9.8 and 7–14 months), with a median PFS of 3.4 and 4.0 months, respectively (95% CI 1.8–4 and 2–4 months) (32, 34). Sorafenib in combination with cetuximab demonstrated no clinical benefit with an ORR of 8% and median OS or PFS of 5.7 and 3.2 months, respectively (31). The combination of sorafenib with cisplatin and 5-fluorouracil emerged as a feasible regimen as a first-line treatment with an ORR of 77.8% and median OS and PFS of 11.8 and 7.2 months, respectively (33). Overall, sorafenib was well-tolerated with a modest anticancer activity. Supplementary Table 2 summarises the toxicity analysis for sorafenib.
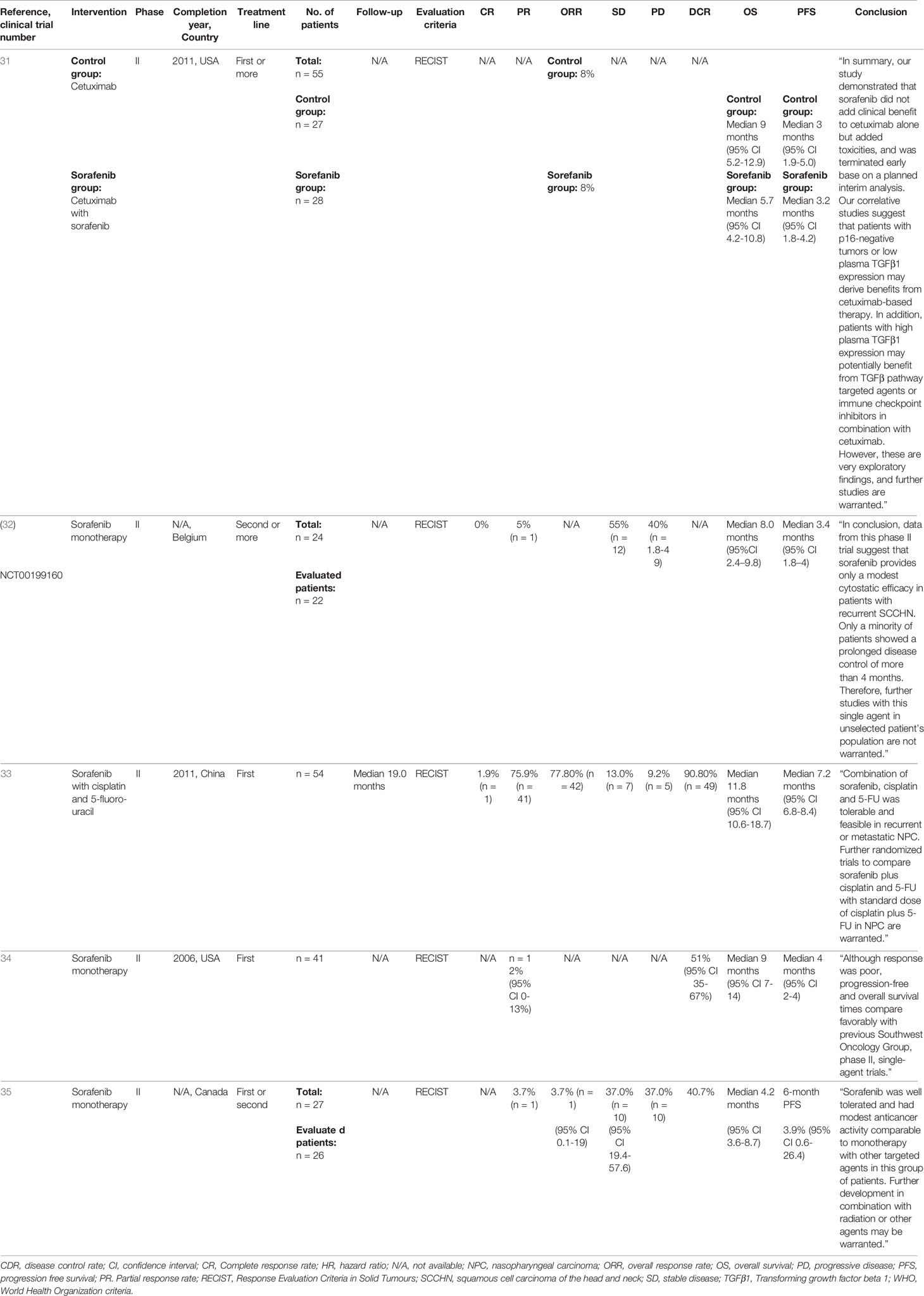
Table 2 Summary of the sorafenib clinical trials for head and neck squamous cell carcinoma.
Sunitinib and Semaxinib
Sunitinib (SU11248) inhibits multiple receptor tyrosine kinases including VEGFR-1, -2 and -3, KIT, foetal liver tyrosine kinase receptor 3 (FLT3), PDGFRα and PDGFRβ, colony-stimulating factor receptor type 1 (CSF1R) and the glial cell line–derived neutrophilic factor receptor (GDNF) (33, 36). Approved by the US FDA, sunitinib treats advanced renal cell carcinoma and advanced gastrointestinal stromal tumours (37). Semaxinib (SU5416), a predecessor of sunitinib, has poor pharmacological properties and limited efficacy (38).
Sunitinib was studied in 4 trials among a total of 91 patients (Table 3): in two as a monotherapy, in one after platinum-based chemotherapy and in one in combination with bortezomib (Table 3). No ORR was reported in any of these studies. In the only trial that treated patients using sunitinib as a first-line treatment, no objective responses were observed and the trial was discontinued prematurely (42). As a monotherapy, 1-year OS rates of 22% and 14% (22% in patients with Eastern Cooperative Oncology Group Performance Status (PS) 0–1 and 14% with PS 2) were reported, while in another monotherapy study, median OS and PFS reached 102 and 60 days, respectively (40, 41). After prior platinum-based chemotherapy, a clinical benefit rate (CBR = SD + PR + CR) was achieved in 28.6% of patients, with no CR, while median OS and PFS reached 10.5 and 3.5 months, respectively (39). Treatment with sunitinib was well-tolerated, although the anticancer effect remained modest.
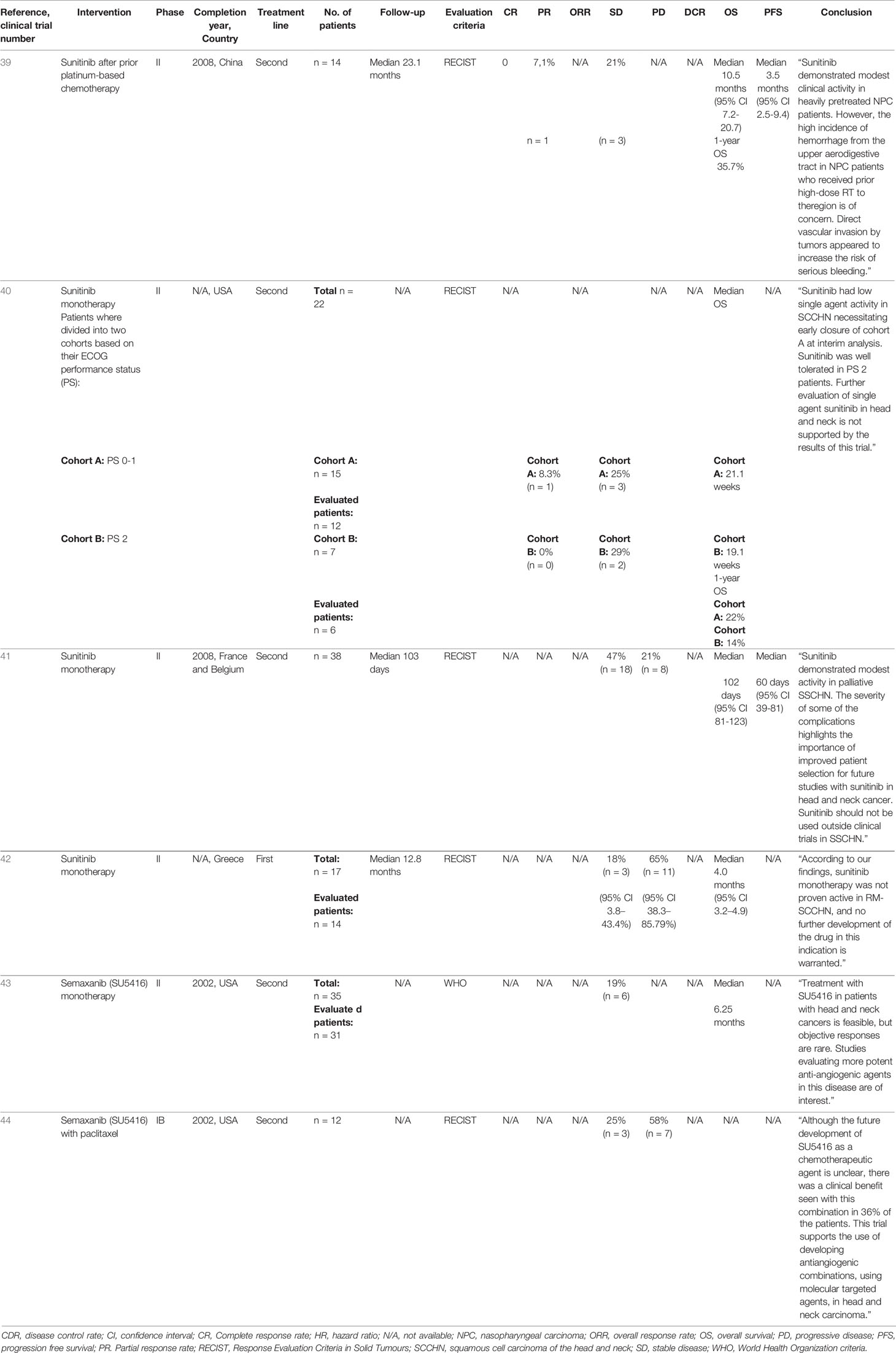
Table 3 Summary of the sunitinib and semaxanib clinical trials for head and neck squamous cell carcinoma.
Semaxinib was studied twice among a total of 47 patients, in one study as a monotherapy and in another in combination with paclitaxel, both as second-line treatment (Table 3). As a monotherapy, a dose of 145 mg/m2 was administered twice daily for 8 weeks, while in combination with paclitaxel at a dose of 110 mg/m2 on days 1, 15, 22 and 25, for a total of 42 cycles (43, 44). Semaxinib as a monotherapy had a median OS of 6.25 months with no severe toxicities. In combination with paclitaxel, SD was reported in 3/12 (25%) and PD in 7/12 (58%) patients (43, 44). Supplementary Table 2 summarises the toxicity analyses of sunitinib and semaxanib.
Other Tyrosine Kinase Anti-Angiogenesis Inhibitor Drugs
Lenvatinib, a multikinase inhibitor against VGFR1-3, was approved by US FDA and European Union to treat several solid cancers including thyroid cancer, renal cell carcinoma, and hepatocellular carcinoma (45). In addition to its role in inhibiting VEGFR1-3, it inhibits PDGFR-α, c-Kit, and the RET proto-oncogene (46). Lenvatinib was studied twice as a combination therapy with pembrolizumab among a total of 36 patients (Table 4). Both studies showed promising results and manageable safety profile. Chen et al., reported an ORR of 28.6% (95% CI 5.0-52.2) with median OS of 6.2 months (95% CI 2.9-9.6) (12). On the other hand, Taylor et al., reported a higher ORR which reached to 46% (95% CI 24.4-67.8) (13).
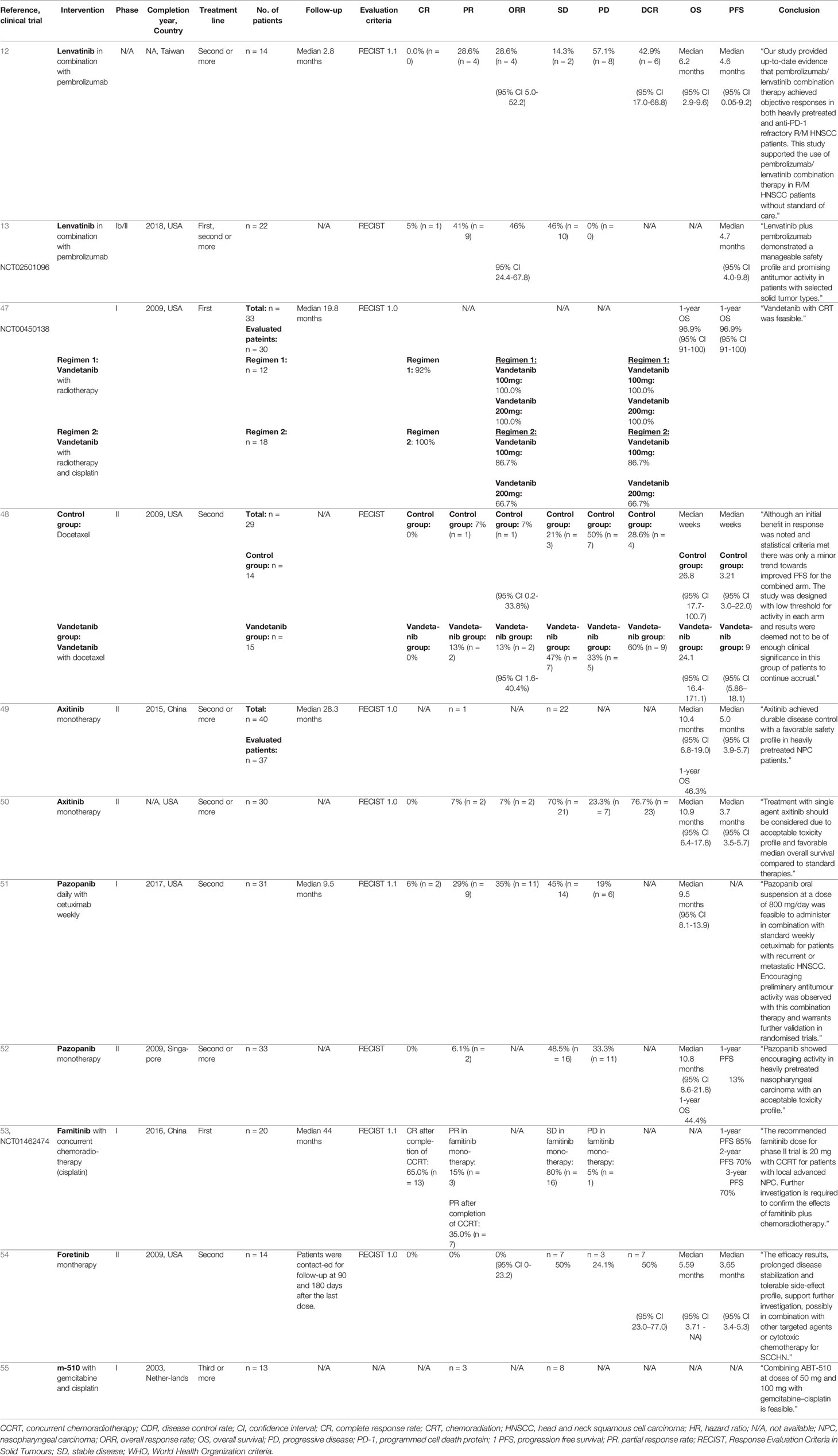
Table 4 Summary of the other tyrosine kinase anti-angiogenesis inhibitors clinical trials for head and neck squamous cell carcinoma.
Vandetanib, a multikinase inhibitor, was approved by the US FDA to treat symptomatic or progressive, unresectable or metastatic medullary thyroid cancer (56). It binds to VEGF and epidermal growth factor (EGF) receptor families as well as RET (rearranged-during-transfection), BRK (breast tumour kinase), TIE2 (receptor-like tyrosine kinase) and Src (proto-oncogene tyrosine-protein kinase) receptors (56). Vandetanib was studied twice as a combination therapy among a total of 62 patients (Table 4), but the conclusions from these studies were inconclusive. As a first-line treatment, vandetanib in combination with radiotherapy as a first-line treatment resulted in an ORR of 100.0% (95% CI 61.0–100.0%) (47). When combined with radiotherapy and cisplatin, vandetanib yielded ORRs of 86.7% (100-mg vandetanib) and 66.7% (200-mg vandetanib; 95% CI 62.1–96.3% and 30.9–90.3%, respectively) (47). As a second-line treatment, the combination of vandetanib and docetaxel exhibited insufficient clinical significance (48). The safety profile of vandetanib in both studies was feasible.
Axitinib is a multitarget TKI approved by the US FDA for the treatment of renal cell carcinoma (57). Axitinib inhibits VEGFR-1, - 2 and -3, PDGFR-α, PDGFR-β and c-KIT (58). Axitinib was studied twice among a total of 70 patients as second-line treatment for metastatic or recurrent HNSCC (Table 4). In both studies, monotherapy with a continuous dose of 5–10-mg twice daily was administered. The median OS reached 10.4 and 10.9 months, respectively, and treatment was well-tolerated (49, 50).
Pazopanib is a small-molecule multikinase inhibitor that inhibits VEGF receptors (1, 2 and 3), PD-ECGFR-α and -β and the stem-cell factor receptor (SCF) c-KIT (59). Several countries have approved pazopanib for the treatment of advanced soft-tissue sarcoma and renal cell carcinoma (60). Two trials on pazopanib were included here, carried out among a total of 64 patients and both using pazopanib as the second- or more-line treatment of metastatic or recurrent HNSCC (Table 4). The trials used a daily pazopanib dose between 200–800 mg. One phase II trial studied pazopanib as a monotherapy and reported a safety profile with a PR of 6.1% and 1-year OS and PFS of 44.4% and 13%, respectively (52). In a phase I trial, pazopanib was combined with cetuximab, achieving CR in 6% and PR in 29% of patients. ORR was 35% and the safety profile was acceptable (51).
Famitinib is a receptor TKI that binds to several RTKs including VEGFR-2 and -3, SCF receptor c-KIT and PDGFR (61). One phase I trial among a total of 20 patients studied famitinib as a monotherapy and in combination with cisplatin and radiotherapy as a first-line treatment (famitinib at an initial dose of 12.5 mg/day, increased to 16.5, 20.0 and 25.0 mg/day) (53). Famitinib as a single agent was well-tolerated, with a PR for famitinib monotherapy of 15% and, after completion of treatment with chemoradiotherapy, increasing to 35%. CR was achieved in 65% of patients after completing treatment. PFS at 1-, 2- and 3-years follow-up reached 85%, 70% and 70%, respectively (53).
Foretinib, an experimental drug not yet in clinical use, is a small molecule that inhibits hepatocyte growth factor (HGF) receptor c-MET and VEGFR-2 (62). Foretinib was studied as a single agent in one phase II trial among 14 patients, at a dose of 240 mg for 5 days on a 14-day treatment cycle. ORR was 0% (95% CI 0–23.2%) with a median OS and PFS of 5.59 and 3.65 months, respectively (95% CI 3.71–NA and 3.4–5.3 months). The side effects were tolerable (54).
ABT-510 is a synthetic peptide that inhibits several pro-angiogenic growth factors including VEGF, bFGF, HGF and interleukin 8 (IL-8) (63). One trial among 13 patients examined ABT-510 in combination with gemcitabine–cisplatin chemotherapy in later lines of metastatic HNSCC (50–100-mg dose of ABT-510 twice daily) (55). Treatment was well- tolerated and PR was reported in 3/13 (23%) and SD in 8/13 (62%) patients (55).
Supplementary Table 2 summarises the toxicity analyses of the drugs discussed above.
Endostatin
Endostatin is a broad-spectrum angiogenesis inhibitor approved by the State Food and Drug Administration of China for the treatment of non-small cell lung cancer (64), but has not enjoyed approval by other regulatory authorities. Endostatin is a naturally occurring protein, featuring a 20-kDa fragment of type XVIII collagen (65). Endostatin inhibits endothelial cell proliferation, migration/invasion and tube formation, and appears to bind to a variety of receptors, including VEGFR-2 and -3, integrin α5β1 and αVβ3 and Glypican-1 and -4 (65, 66).
Endostatin was studied in 3 clinical trials among 186 patients (Table 5), in two trials in combination with chemotherapy (cisplatin, paclitaxel, 5-fluorouracil or gemcitabine) and in one trial with radiotherapy (67–69). In one study, recombinant human endostatin adenovirus (E10A) was administered at a dose of 1.0 × 1012 virus particles on days 1 and 8 for 4 cycles (69). In the other trials, a dose of 15 mg/day was administered for 14 days (67, 68). When endostatin was added to radiotherapy as a first-line treatment, CR was achieved in 60.0% and PR in 40.0% of patients compared with a CR of 61.5% and PR of 38.5% in the control group (radiotherapy with cisplatin) (67). Survival rates improved with endostatin: 2-year OS and PFS rates reached 100% in the endostatin group compared to 69.6% and 67.3% in the control group (radiotherapy with cisplatin) (67). Endostatin in combination with cisplatin and gemcitabine as a second-line treatment yielded an ORR of 85.7% and 1-year OS and PFS rates of 90.2% and 69.8%, respectively (68). In the study with E10A, the effect of endostatin in combination with cisplatin and paclitaxel proved beneficial in patients with HNSCC compared to the control group (chemotherapy only) (69). ORR with E10A was 39.7% compared to 29.9% in the control group (p=0.154; chemotherapy only) (69). The median OS was 19.10 months in the E10A group and 14.53 months when chemotherapy alone was administered [p=0.366, HR 0.79 (95% CI 0.47–)] (69). Across all trials, endostatin was well-tolerated with no significant systemic toxicity, revealing promising anticancer effects when administered as a combination therapy. Supplementary Table 2 summarises the toxicity analysis of endostatin.
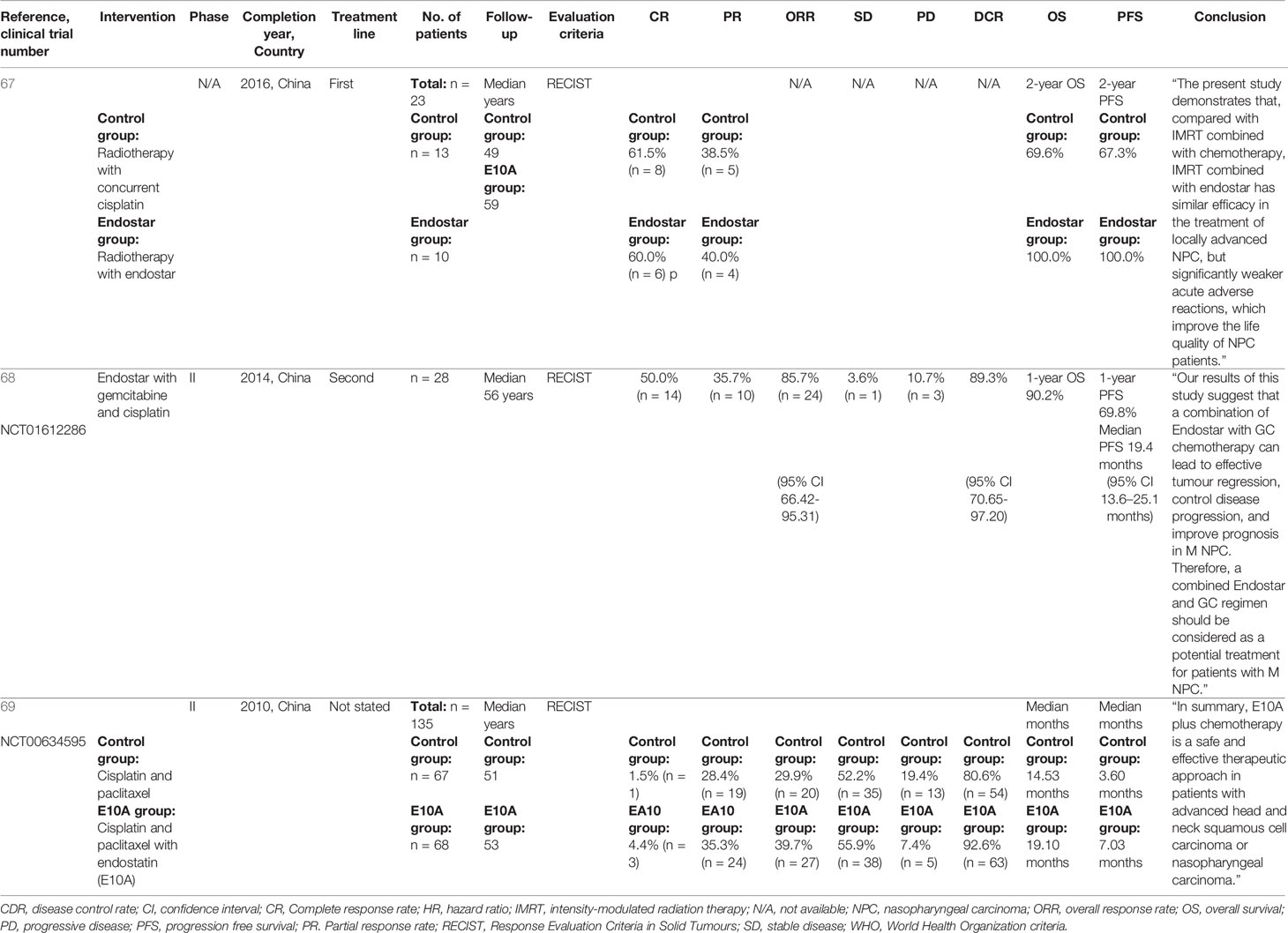
Table 5 Summary of the endostatin clinical trials for head and neck squamous cell carcinoma.
Discussion
Angiogenesis plays a crucial role in tumour growth, invasion and metastasis, while the overexpression of VEGF in HNSCC associates with advanced disease and a poor prognosis (70, 71). Several therapeutic agents have been developed to target angiogenesis pathways, although they have yet to receive approval for the treatment of HNSCC. In this systematic review, we summarised the published data regarding bevacizumab, TKIs and endostatin in HNSCC clinical trials.
Bevacizumab has been approved by the US FDA to treat several malignancies as a monotherapy or in combination with chemo- or radiotherapies (15). Preclinical data point towards encouraging results with bevacizumab in HNSCC as well, since an in vitro study on HNSCC cell lines showed that bevacizumab decreased VEGF secretion (72). In another study on the xenografts of HNSCC cell lines, bevacizumab was tested in combination with radiation, resulting in significant decreases in angiogenesis, the inhibition of tumour growth and an increase in tumour cell apoptosis compared to radiation alone (73). In HNSCC clinical trials, bevacizumab was the most frequently studied drug and was analysed in several combinations as well. In some trials, significant toxicities were reported (16, 17, 26), although in other studies, the same combinations appeared well-tolerated with encouraging results (11, 18, 19, 21–25, 27). Three categories of combinations were used in the trials: (1) bevacizumab in combination with erlotinib and chemotherapy/chemoradiotherapy (16, 23, 27); (2) bevacizumab in combination with cetuximab and chemotherapy/chemoradiotherapy (17, 18, 21) and (3) bevacizumab in combination with chemotherapy or chemoradiotherapy (11, 19, 20, 22, 24, 26). Significant toxicities, such as a perforation, fistula, diarrhoea, mucositis, dysphagia, haemorrhage and hematologic toxicity, were reported in one trial from all of these treatment combinations, and no further trials were recommended (16, 17, 26). Other studies described more promising results and encouraging ORR or survival rates. Bevacizumab was also the only drug that had progressed to a phase III trial. For instance, in 2019, results from a large phase III trial were published (11), and the addition of bevacizumab significantly improved both PFS and ORR, although a statistically significant improvement to OS was not achieved. Unfortunately, the addition of bevacizumab associated with a higher rate of treatment-related grade 3–5 bleeding events (6.7% vs. 0.5%; p<0.001) and treatment-related deaths (9.3% vs. 3.5%; p=0.022) (11).
Famitinib, a TKI, tended to be the most promising experimental drug. It was studied in one trial as an initial monotherapy for two weeks, immediately followed by its use in combination with cisplatin and radiotherapy (53) among patients with stage III–IV HNSCC. Famitinib was well- tolerated and, in combination with chemoradiotherapy, CR was achieved in 65% of patients and 1-, 2- and 3-year PFS reached 85%, 70% and 70%, respectively (53). However, the lack of comparison group limits the generalisability of these results. Some TKIs yielded inconsistent results in various trials and the findings remain inconclusive. Vandetanib showed varying results with an ORR of 13% (PR in 2/15 patients) with docetaxel following progression to platinum-based therapy (48). In a curative setting, combining vandetanib with radiotherapy yielded 100% ORR, while when combined with radiotherapy and cisplatin, it yielded an ORR of 86.7% (at a dose of 100-mg vandetanib) and 66.7% (at a dose of 200-mg vandetanib), respectively (47). Sorafenib and sunitinib were both well-tolerated, although the therapeutic effects of either drug remained modest (31–35, 39–42).
Preclinical studies with endostatin demonstrated the suppression of HNSCC cell migration and invasion, as well as high levels of cell apoptosis and reduced tumour angiogenesis (74–76). Based on our systematic review, endostatin emerged as the most promising drug for inhibiting angiogenesis in HNSCC clinical trials with feasible safety profiles and promising anticancer effects. Endostatin was analysed in three Chinese trials, with encouraging ORR and survival rates reported. The combination of endostatin with cisplatin and gemcitabine yielded an ORR of 85.7% (68). When endostatin was added to radiotherapy, similar response and survival rates were achieved in a small first-line study compared to chemoradiotherapy, although significantly fewer acute adverse events were reported in the endostatin arm (67). Furthermore, endostatin received approval for the treatment of NSCLC in China, but not for HNSCC (65). One phase II trial of endostatin was completed in the US on patients with advanced neuroendocrine tumours, although no significant tumour regression was reported (77).
Immunotherapy is the newest treatment modality for HNSCC patients. Based on boosting the patient’s own immune system to eliminate cancer cells, immunotherapy surpasses conventional chemotherapy in its specificity and decreases therapy-related morbidities. Two immunotherapies, pembrolizumab and nivolumab, have received FDA and European Medicines Agency (EMA) approval to treat HNSCC (78, 79). Only one angiogenesis inhibitor, lenvatinib, was tested in combination with immunotherapy, pembrolizumab, and gave a promising anti-tumour activity in two trials (12, 13). Interestingly, two out of ten patients who had failed previous anti-PD-1 therapy, achieved partial response when they received pembrolizumab/lenvatinib combination therapy.
Across all 38 trials included in this systematic review, only one was in phase III, while the others were in phase I (8), II (24), I/II (2) or unspecified (2). Bevacizumab was included in the largest number of trials, and the phase III trial was also the largest study consisting of a total of 403 patients (11). The other trials enrolled only 10 to 70 participants. Trials with TKIs featured small study populations, comprising only 10–40 patients each. In addition, one large phase II study on endostatin consisted of a total of 153 patients (69). The studies examined featured a variety of different comparison groups and a variety of previous treatment lines and, thus, direct interstudy comparisons should be avoided. Further extensive randomised trials, particularly with well-tolerated endostatin and a combination of lenvatinib with immunotherapy, are truly needed in order to gain a clearer understanding of their benefit in HNSCC patients.
Conclusions
Angiogenesis is a hallmark of tumour progression and targeting angiogenesis has proved successful as a cancer treatment approach in some solid tumours. Although the clinical benefit of angiogenesis inhibitors in treating HNSCC patients remains unclear and they associate with considerable toxicity, few trials gave encouraging results. Further clinical studies are still needed to evaluate which, if any, angiogenesis inhibitors are beneficial to patients with advanced HNSCC. Specifically, further data are needed to identify the most effective combinations with other adjuvant therapies such as immunotherapy, especially with regards to identifying those patients who will benefit most from treatment.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
AH designed the study, performed the literature search, extracted the data and wrote the manuscript. WW performed the literature search and extracted the data. OV performed the literature search and extracted the data. KS designed the study and interpreted the results. PK designed the study and interpreted the results. TS designed the study and interpreted the results. AA-S designed the study, interpreted the results and supervised the work. All authors contributed to the article and approved the submitted version.
Funding
The authors gratefully acknowledge the following funders of this study: the Sigrid Jusélius Foundation, the Cancer Society of Finland, the Oulu University Hospital MRC grant, Helsinki University Central Hospital research funds, the Jane and Aatos Erkko Foundation, and the Medicinska Understödsföreningen Liv och Hälsa Foundation.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors acknowledge Tiina Heino and Katri Larmo for assisting with the systematic search.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.683570/full#supplementary-material
Abbreviations
BRK, Breast tumour kinase; CDR, Disease control rate; CI, Confidence interval; CR, Complete response rate; CSF1R, Colony stimulating factor receptor type 1; EGF, Epidermal growth factor; EMA, European Medicines Agency; FLT3, Foetal liver tyrosine kinase receptor 3; GDNF, Glial cell line–derived neutrophilic factor receptor; HGF, Hepatocyte growth factor; HNSCC, Head and neck squamous cell carcinoma; HPV, Human papillomavirus; HR, Hazard ratio; NSCLC, Non-squamous non-small cell lung cancer; ORR, Overall response rate; OS, Overall survival; PD, Progressive disease; PD-1, Programmed cell death protein; PDGFR, Platelet-derived growth factor receptor; PFS, Progression-free survival; PR, Partial response rate; RCC, Renal cell carcinoma; RECIST, Response Evaluation Criteria in Solid Tumours; RET, Rearranged-during-transfection; SD, Stable disease; Src, Proto-oncogene tyrosine-protein kinase; TIE2, Receptor-like tyrosine kinase; TKIs, Receptor tyrosine kinase inhibitors; US FDA, US Food and Drug Administration; VEGF, Vascular endothelial growth factor; WHO, World Health Organisation criteria.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin (2018) 68:394–424. doi: 10.3322/caac.21492
2. Marur S, Forastiere AA. Head and Neck Squamous Cell Carcinoma: Update on Epidemiology, Diagnosis, and Treatment. Mayo Clin Proc (2016) 91:386–96. doi: 10.1016/j.mayocp.2015.12.017
3. Sacco AG, Cohen EE. Current Treatment Options for Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma. J Clin Oncol (2015) 33:3305–13. doi: 10.1200/JCO.2015.62.0963
4. Gatta G, Botta L, Sánchez MJ, Anderson LA, Pierannunzio D, Licitra L. Prognoses and Improvement for Head and Neck Cancers Diagnosed in Europe in Early 2000s: The EUROCARE-5 Population-Based Study. Eur J Cancer (2015) 51:2130–43. doi: 10.1016/j.ejca.2015.07.043
5. Folkman J. Role of Angiogenesis in Tumor Growth and Metastasis. Semin Oncol (2002) 29:15–8. doi: 10.1053/sonc.2002.37263
6. Carla C, Daris F, Cecilia B, Francesca B, Francesca C, Paolo F. Angiogenesis in Head and Neck Cancer: A Review of the Literature. J Oncol (2012) 2012:358472. doi: 10.1155/2012/358472
7. Vassilakopoulou M, Psyrri A, Argiris A. Targeting Angiogenesis in Head and Neck Cancer. Oral Oncol (2015) 51:409–15. doi: 10.1016/j.oraloncology.2015.01.006
8. Seiwert TY, Cohen EEW. Targeting Angiogenesis in Head and Neck Cancer. Semin Oncol (2008) 35:274–85. doi: 10.1053/j.seminoncol.2008.03.005
9. Jain RK. Normalizing Tumor Microenvironment to Treat Cancer: Bench to Bedside to Biomarkers. J Clin Oncol (2013) 31:2205–18. doi: 10.1200/JCO.2012.46.3653
10. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst Rev (2015) 4:1. doi: 10.1186/2046-4053-4-1
11. Argiris A, Li S, Savvides P, Ohr JP, Gilbert J, Levine MA, et al. Phase III Randomized Trial of Chemotherapy With or Without Bevacizumab in Patients With Recurrent or Metastatic Head and Neck Cancer. J Clin Oncol (2019) 37:3266–74. doi: 10.1200/JCO.19.00555
12. Chen T-H, Chang PM-H, Yang M-H. Combination of Pembrolizumab and Lenvatinib Is a Potential Treatment Option for Heavily Pretreated Recurrent and Metastatic Head and Neck Cancer. J Chin Med Assoc (2021) 84:361–7. doi: 10.1097/JCMA.0000000000000497
13. Taylor MH, Lee C-H, Makker V, Rasco D, Dutcus CE, Wu J, et al. Phase IB/II Trial of Lenvatinib Plus Pembrolizumab in Patients With Advanced Renal Cell Carcinoma, Endometrial Cancer, and Other Selected Advanced Solid Tumors. J Clin Oncol (2020) 38:1154–63. doi: 10.1200/JCO.19.01598
14. de Aguiar RB, de Moraes JZ. Exploring the Immunological Mechanisms Underlying the Anti-Vascular Endothelial Growth Factor Activity in Tumors. Front Immunol (2019) 10:1023. doi: 10.3389/fimmu.2019.01023
15. Lin Z, Zhang Q, Luo W. Angiogenesis Inhibitors as Therapeutic Agents in Cancer: Challenges and Future Directions. Eur J Pharmacol (2016) 793:76–81. doi: 10.1016/j.ejphar.2016.10.039
16. Ahn PH, Machtay M, Anne PR, Cognetti D, Keane WM, Wuthrick E, et al. Phase I Trial Using Induction Ciplatin, Docetaxel, 5-FU and Erlotinib Followed by Cisplatin, Bevacizumab and Erlotinib With Concurrent Radiotherapy for Advanced Head and Neck Cancer. Am J Clin Oncol (2018) 41:441–6. doi: 10.1097/COC.0000000000000317
17. Argiris A, Bauman JE, Ohr J, Gooding WE, Heron DE, Duvvuri U, et al. Phase II Randomized Trial of Radiation Therapy, Cetuximab, and Pemetrexed With or Without Bevacizumab in Patients With Locally Advanced Head and Neck Cancer. Ann Oncol (2016) 27:1594–600. doi: 10.1093/annonc/mdw204
18. Fury MG, Xiao H, Sherman EJ, Baxi S, Smith-Marrone S, Schupak K, et al. Phase II Trial of Bevacizumab + Cetuximab + Cisplatin With Concurrent Intensity-Modulated Radiation Therapy for Patients With Stage III/IVB Head and Neck Squamous Cell Carcinoma. Head Neck (2016) 38:566. doi: 10.1002/hed.24041
19. Nyflot MJ, Kruser TJ, Traynor AM, Khuntia D, Yang DT, Hartig GK, et al. Phase 1 Trial of Bevacizumab With Concurrent Chemoradiation Therapy for Squamous Cell Carcinoma of the Head and Neck With Exploratory Functional Imaging of Tumor Hypoxia, Proliferation, and Perfusion. Int J Radiat Oncol Biol Phys (2015) 91:942–51. doi: 10.1016/j.ijrobp.2014.11.029
20. Yao M, Galanopoulos N, Lavertu P, Fu P, Gibson M, Argiris A, et al. Phase II Study of Bevacizumab in Combination With Docetaxel and Radiation in Locally Advanced Squamous Cell Carcinoma of the Head and Neck. Head Neck (2015) 37:1665–71. doi: 10.1002/hed.23813
21. Argiris A, Kotsakis AP, Hoang T, Worden FP, Savvides P, Gibson MK, et al. Cetuximab and Bevacizumab: Preclinical Data and Phase II Trial in Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck. Ann Oncol (2013) 24:220–5. doi: 10.1093/annonc/mds245
22. Lee NY, Zhang Q, Pfister DG, Kim J, Garden AS, Mechalakos J, et al. Addition of Bevacizumab to Standard Chemoradiation for Locoregionally Advanced Nasopharyngeal Carcinoma (RTOG 0615): A Phase 2 Multi-Institutional Trial. Lancet Oncol (2012) 13:172–80. doi: 10.1016/S1470-2045(11)70303-5
23. Yoo DS, Kirkpatrick JP, Craciunescu O, Broadwater G, Peterson BL, Carroll MD, et al. Prospective Trial of Synchronous Bevacizumab, Erlotinib, and Concurrent Chemoradiation in Locally Advanced Head and Neck Cancer. Clin Cancer Res (2012) 18:1404–14. doi: 10.1158/1078-0432.CCR-11-1982
24. Fury MG, Lee NY, Sherman E, Lisa D, Kelly K, Lipson B, et al. A Phase 2 Study of Bevacizumab With Cisplatin Plus Intensity-Modulated Radiation Therapy for Stage III/IVB Head and Neck Squamous Cell Cancer. Cancer (2012) 118:5008–14. doi: 10.1002/cncr.27498
25. Hainsworth JD, Spigel DR, Greco FA, Shipley DL, Peyton J, Rubin M, et al. Combined Modality Treatment With Chemotherapy, Radiation Therapy, Bevacizumab, and Erlotinib in Patients With Locally Advanced Squamous Carcinoma of the Head and Neck: A Phase II Trial of the Sarah Cannon Oncology Research Consortium. Cancer J (2011) 17:267–72. doi: 10.1097/PPO.0b013e3182329791
26. Salama JK, Haraf DJ, Stenson KM, Blair EA, Witt ME, Williams R, et al. A Randomized Phase II Study of 5-Fluorouracil, Hydroxyurea, and Twice-Daily Radiotherapy Compared With Bevacizumab Plus 5-Fluorouracil, Hydroxyurea, and Twice-Daily Radiotherapy for Intermediate-Stage and T4N0-1 Head and Neck Cancers. Ann Oncol (2011) 22:2304–9. doi: 10.1093/annonc/mdq736
27. Cohen EEW, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, et al. Erlotinib and Bevacizumab in Patients With Recurrent or Metastatic Squamous-Cell Carcinoma of the Head and Neck: A Phase I/II Study. Lancet Oncol (2009) 10:247–57. doi: 10.1016/S1470-2045(09)70002-6
28. Keating GM. Sorafenib: A Review in Hepatocellular Carcinoma. Target Oncol (2017) 12:243–53. doi: 10.1007/s11523-017-0484-7
29. Liu L, Cao Y, Chen C, Zhang X, McNabola A, Wilkie D, et al. Sorafenib Blocks the RAF/MEK/ERK Pathway, Inhibits Tumor Angiogenesis, and Induces Tumor Cell Apoptosis in Hepatocellular Carcinoma Model PLC/PRF/5. Cancer Res (2006) 66:11851–8. doi: 10.1158/0008-5472.CAN-06-1377
30. Marisi G, Cucchetti A, Ulivi P, Canale M, Cabibbo G, Solaini L, et al. Ten Years of Sorafenib in Hepatocellular Carcinoma: Are There Any Predictive and/or Prognostic Markers? World J Gastroenterol (2018) 24:4152–63. doi: 10.3748/wjg.v24.i36.4152
31. Gilbert J, Schell MJ, Zhao X, Murphy B, Tanvetyanon T, Leon ME, et al. A Randomized Phase II Efficacy and Correlative Studies of Cetuximab With or Without Sorafenib in Recurrent and/or Metastatic Head and Neck Squamous Cell Carcinoma. Oral Oncol (2015) 51:376–82. doi: 10.1016/j.oraloncology.2014.12.011
32. Lalami Y, Garcia C, Flamen P, Ameye L, Paesmans M, Awada A. Phase II Trial Evaluating the Efficacy of Sorafenib (BAY 43-9006) and Correlating Early Fluorodeoxyglucose Positron Emission Tomography-CT Response to Outcome in Patients With Recurrent and/or Metastatic Head and Neck Cancer. Head Neck (2016) 38:347–54. doi: 10.1002/hed.23898
33. Xue C, Huang Y, Huang PY, Yu QT, Pan JJ, Liu LZ, et al. Phase II Study of Sorafenib in Combination With Cisplatin and 5-Fluorouracil to Treat Recurrent or Metastatic Nasopharyngeal Carcinoma. Ann Oncol (2013) 24:1055–61. doi: 10.1093/annonc/mds581
34. Williamson SK, Moon J, Huang CH, Guaglianone PP, LeBlanc M, Wolf GT, et al. Phase II Evaluation of Sorafenib in Advanced and Metastatic Squamous Cell Carcinoma of the Head and Neck: Southwest Oncology Group Study S0420. J Clin Oncol (2010) 28:3330–5. doi: 10.1200/JCO.2009.25.6834
35. Elser C, Siu LL, Winquist E, Agulnik M, Pond GR, Chin SF, et al. Phase II Trial of Sorafenib in Patients With Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck or Nasopharyngeal Carcinoma. J Clin Oncol (2007) 25:3766–73. doi: 10.1200/JCO.2006.10.2871
36. Ferrari SM, Centanni M, Virili C, Miccoli M, Ferrari P, Ruffilli I, et al. Sunitinib in the Treatment of Thyroid Cancer. Curr Med Chem (2019) 26:963–72. doi: 10.2174/0929867324666171006165942
38. Chow LQM, Eckhardt SG. Sunitinib: From Rational Design to Clinical Efficacy. J Clin Oncol (2007) 25:884–96. doi: 10.1200/JCO.2006.06.3602
39. Hui EP, Ma BBY, King AD, Mo F, Chan SL, Kam MKM, et al. Hemorrhagic Complications in a Phase II Study of Sunitinib in Patients of Nasopharyngeal Carcinoma Who Has Previously Received High-Dose Radiation. Ann Oncol (2011) 22:1280–7. doi: 10.1093/annonc/mdq629
40. Choong NW, Kozloff M, Taber D, Hu HS, Wade J 3rd, Ivy P, et al. Phase II Study of Sunitinib Malate in Head and Neck Squamous Cell Carcinoma. Invest New Drugs (2010) 28:677–83. doi: 10.1007/s10637-009-9296-7
41. Machiels J-PH, Henry S, Zanetta S, Kaminsky M-C, Michoux N, Rommel D, et al. Phase II Study of Sunitinib in Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck: GORTEC 2006-01. J Clin Oncol (2010) 28:21–8. doi: 10.1200/JCO.2009.23.8584
42. Fountzilas G, Fragkoulidi A, Kalogera-Fountzila A, Nikolaidou M, Bobos M, Calderaro J, et al. A Phase II Study of Sunitinib in Patients With Recurrent and/or Metastatic Non-Nasopharyngeal Head and Neck Cancer. Cancer Chemother Pharmacol (2010) 65:649–60. doi: 10.1007/s00280-009-1070-1
43. Fury MG, Zahalsky A, Wong R, Venkatraman E, Lis E, Hann L, et al. A Phase II Study of SU5416 in Patients With Advanced or Recurrent Head and Neck Cancers. Invest New Drugs (2007) 25:165–72. doi: 10.1007/s10637-006-9011-x
44. Cooney MM, Tserng K-Y, Makar V, McPeak RJ, Ingalls ST, Dowlati A, et al. A Phase IB Clinical and Pharmacokinetic Study of the Angiogenesis Inhibitor SU5416 and Paclitaxel in Recurrent or Metastatic Carcinoma of the Head and Neck. Cancer Chemother Pharmacol (2005) 55:295–300. doi: 10.1007/s00280-004-0871-5
45. Hussein Z, Mizuo H, Hayato S, Namiki M, Shumaker R. Clinical Pharmacokinetic and Pharmacodynamic Profile of Lenvatinib, an Orally Active, Small-Molecule, Multitargeted Tyrosine Kinase Inhibitor. Eur J Drug Metab Pharmacokinet (2017) 42:903–14. doi: 10.1007/s13318-017-0403-4
46. Zschäbitz S, Grüllich C. Lenvantinib: A Tyrosine Kinase Inhibitor of VEGFR 1-3, FGFR 1-4, Pdgfrα, KIT and RET. Recent Results Cancer Res Fortschr Der Krebsforsch Prog Dans Les Rech Sur Le Cancer (2018) 211:187–98. doi: 10.1007/978-3-319-91442-8_13
47. Papadimitrakopoulou VA, Frank SJ, Cohen EW, Hirsch FR, Myers JN, Heymach JV, et al. Phase I Study of Vandetanib With Radiation Therapy With or Without Cisplatin in Locally Advanced Head and Neck Squamous Cell Carcinoma. Head Neck (2016) 38:439–47. doi: 10.1002/hed.23922
48. Limaye S, Riley S, Zhao S, O’Neill A, Posner M, Adkins D, et al. A Randomized Phase II Study of Docetaxel With or Without Vandetanib in Recurrent or Metastatic Squamous Cell Carcinoma of Head and Neck (SCCHN). Oral Oncol (2013) 49:835–41. doi: 10.1016/j.oraloncology.2013.04.010
49. Hui EP, Ma BBY, Loong HHF, Mo F, Li L, King AD, et al. Efficacy, Safety, and Pharmacokinetics of Axitinib in Nasopharyngeal Carcinoma: A Preclinical and Phase Ii Correlative Study. Clin Cancer Res (2018) 24:1030–7. doi: 10.1158/1078-0432.CCR-17-1667
50. Swiecicki PL, Zhao L, Belile E, Sacco AG, Chepeha DB, Dobrosotskaya I, et al. A Phase II Study Evaluating Axitinib in Patients With Unresectable, Recurrent or Metastatic Head and Neck Cancer. Invest New Drugs (2015) 33:1248–56. doi: 10.1007/s10637-015-0293-8
51. Adkins D, Mehan P, Ley J, Siegel MJ, Siegel BA, Dehdashti F, et al. Pazopanib Plus Cetuximab in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: An Open-Label, Phase 1b and Expansion Study. Lancet Oncol (2018) 19:1082–93. doi: 10.1016/S1470-2045(18)30350-4
52. Lim W-T, Ng Q-S, Ivy P, Leong S-S, Singh O, Chowbay B, et al. A Phase II Study of Pazopanib in Asian Patients With Recurrent/Metastatic Nasopharyngeal Carcinoma. Clin Cancer Res (2011) 17:5481–9. doi: 10.1158/1078-0432.CCR-10-3409
53. Chen Q, Tang L, Liu N, Han F, Guo L, Guo S, et al. Famitinib in Combination With Concurrent Chemoradiotherapy in Patients With Locoregionally Advanced Nasopharyngeal Carcinoma: A Phase 1, Open-Label, Dose-Escalation Study. Cancer Commun (2018) 38:66. doi: 10.1186/s40880-018-0330-z
54. Seiwert T, Sarantopoulos J, Kallender H, McCallum S, Keer HN, Blumenschein GJ. Phase II Trial of Single-Agent Foretinib (GSK1363089) in Patients With Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck. Invest New Drugs (2013) 31:417–24. doi: 10.1007/s10637-012-9861-3
55. Gietema JA, Hoekstra R, de Vos FYFL, Uges DRA, van der Gaast A, Groen HJM, et al. A Phase I Study Assessing the Safety and Pharmacokinetics of the Thrombospondin-1-Mimetic Angiogenesis Inhibitor ABT-510 With Gemcitabine and Cisplatin in Patients With Solid Tumors. Ann Oncol (2006) 17:1320–7. doi: 10.1093/annonc/mdl102
56. Fallahi P, Di Bari F, Ferrari SM, Spisni R, Materazzi G, Miccoli P, et al. Selective Use of Vandetanib in the Treatment of Thyroid Cancer. Drug Des Devel Ther (2015) 9:3459–70. doi: 10.2147/DDDT.S72495
57. Sonpavde G, Hutson TE. Recent Advances in the Therapy of Renal Cancer. Expert Opin Biol Ther (2007) 7:233–42. doi: 10.1517/14712598.7.2.233
58. Sonpavde G, Hutson TE, Rini BI. Axitinib for Renal Cell Carcinoma. Expert Opin Investig Drugs (2008) 17:741–8. doi: 10.1517/13543784.17.5.741
59. Chellappan DK, Chellian J, Ng ZY, Sim YJ, Theng CW, Ling J, et al. The Role of Pazopanib on Tumour Angiogenesis and in the Management of Cancers: A Review. BioMed Pharmacother (2017) 96:768–81. doi: 10.1016/j.biopha.2017.10.058
60. Miyamoto S, Kakutani S, Sato Y, Hanashi A, Kinoshita Y, Ishikawa A. Drug Review: Pazopanib. Jpn J Clin Oncol (2018) 48:503–13. doi: 10.1093/jjco/hyy053
61. Ge S, Zhang Q, He Q, Zou J, Liu X, Li N, et al. Famitinib Exerted Powerful Antitumor Activity in Human Gastric Cancer Cells and Xenografts. Oncol Lett (2016) 12:1763–8. doi: 10.3892/ol.2016.4909
62. Kogata Y, Tanaka T, Ono YJ, Hayashi M, Terai Y, Ohmichi M. Foretinib (GSK1363089) Induces p53-Dependent Apoptosis in Endometrial Cancer. Oncotarget (2018) 9:22769–84. doi: 10.18632/oncotarget.25232
63. Recouvreux MV, Camilletti MA, Rifkin DB, Becu-Villalobos D, Díaz-Torga G. Thrombospondin-1 (TSP-1) Analogs ABT-510 and ABT-898 Inhibit Prolactinoma Growth and Recover Active Pituitary Transforming Growth Factor-β1 (Tgf-β1). Endocrinology (2012) 153:3861–71. doi: 10.1210/en.2012-1007
64. Folkman J. Antiangiogenesis in Cancer Therapy–Endostatin and Its Mechanisms of Action. Exp Cell Res (2006) 312:594–607. doi: 10.1016/j.yexcr.2005.11.015
65. Walia A, Yang JF, Huang Y-H, Rosenblatt MI, Chang J-H, Azar DT. Endostatin’s Emerging Roles in Angiogenesis, Lymphangiogenesis, Disease, and Clinical Applications. Biochim Biophys Acta (2015) 1850:2422–38. doi: 10.1016/j.bbagen.2015.09.007
66. Abdollahi A, Hahnfeldt P, Maercker C, Gröne H-J, Debus J, Ansorge W, et al. Endostatin’s Antiangiogenic Signaling Network. Mol Cell (2004) 13:649–63. doi: 10.1016/s1097-2765(04)00102-9
67. Kang M, Wang F, Liao X, Zhou P, Wang R. Intensity-Modulated Radiotherapy Combined With Endostar has Similar Efficacy But Weaker Acute Adverse Reactions Than IMRT Combined With Chemotherapy in the Treatment of Locally Advanced Nasopharyngeal Carcinoma. Medicine (Baltimore) (2018) 97:e11118. doi: 10.1097/MD.0000000000011118
68. Jin T, Li B, Chen X-Z. A Phase II Trial of Endostar Combined With Gemcitabine and Cisplatin Chemotherapy in Patients With Metastatic Nasopharyngeal Carcinoma (NCT01612286). Oncol Res (2013) 21:317–23. doi: 10.3727/096504014X13983417587401
69. Ye W, Liu R, Pan C, Jiang W, Zhang L, Guan Z, et al. Multicenter Randomized Phase 2 Clinical Trial of a Recombinant Human Endostatin Adenovirus in Patients With Advanced Head and Neck Carcinoma. Mol Ther J Am Soc Gene Ther (2014) 22:1221–9. doi: 10.1038/mt.2014.53
70. Shemirani B, Crowe DL. Head and Neck Squamous Cell Carcinoma Lines Produce Biologically Active Angiogenic Factors. Oral Oncol (2000) 36:61–6. doi: 10.1016/s1368-8375(99)00052-4
71. Smith BD, Smith GL, Carter D, Sasaki CT, Haffty BG. Prognostic Significance of Vascular Endothelial Growth Factor Protein Levels in Oral and Oropharyngeal Squamous Cell Carcinoma. J Clin Oncol (2000) 18:2046–52. doi: 10.1200/JCO.2000.18.10.2046
72. Heydar H, Mansouri K, Norooznezhad M, Norooznezhad F, Mohamadnia A, Bahrami N. Bevacizumab Inhibits Angiogenic Cytokines in Head and Neck Squamous Cell Carcinoma: From Gene to the Protein. Int J Hematol Stem Cell Res (2018) 12:136–41. doi: 10.1200/JCO.2000.18.10.2046
73. Hoang T, Huang S, Armstrong E, Eickhoff JC, Harari PM. Enhancement of Radiation Response With Bevacizumab. J Exp Clin Cancer Res (2012) 31:37. doi: 10.1186/1756-9966-31-37
74. Wilson RF, Morse MA, Pei P, Renner RJ, Schuller DE, Robertson FM, et al. Endostatin Inhibits Migration and Invasion of Head and Neck Squamous Cell Carcinoma Cells. Anticancer Res (2003) 23:1289–95. doi: 10.1186/1756-9966-31-37
75. Adhim Z, Lin X, Huang W, Morishita N, Nakamura T, Yasui H, et al. E10A, an Adenovirus-Carrying Endostatin Gene, Dramatically Increased the Tumor Drug Concentration of Metronomic Chemotherapy With Low-Dose Cisplatin in a Xenograft Mouse Model for Head and Neck Squamous-Cell Carcinoma. Cancer Gene Ther (2012) 19:144–52. doi: 10.1038/cgt.2011.79
76. Nyberg P, Heikkilä P, Sorsa T, Luostarinen J, Heljasvaara R, Stenman U-H, et al. Endostatin Inhibits Human Tongue Carcinoma Cell Invasion and Intravasation and Blocks the Activation of Matrix Metalloprotease-2, -9, and -13. J Biol Chem (2003) 278:22404–11. doi: 10.1074/jbc.M210325200
77. Kulke MH, Bergsland EK, Ryan DP, Enzinger PC, Lynch TJ, Zhu AX, et al. Phase II Study of Recombinant Human Endostatin in Patients With Advanced Neuroendocrine Tumors. J Clin Oncol (2006) 24:3555–61. doi: 10.1200/JCO.2006.05.6762
78. Cohen EEW, Bell RB, Bifulco CB, Burtness B, Gillison ML, Harrington KJ, et al. The Society for Immunotherapy of Cancer Consensus Statement on Immunotherapy for the Treatment of Squamous Cell Carcinoma of the Head and Neck (HNSCC). J Immunother Cancer (2019) 7:184. doi: 10.1186/s40425-019-0662-5
Keywords: anti-angiogenesis, head and neck cancer, therapy, endostatin, bevacizumab
Citation: Hyytiäinen A, Wahbi W, Väyrynen O, Saarilahti K, Karihtala P, Salo T and Al-Samadi A (2021) Angiogenesis Inhibitors for Head and Neck Squamous Cell Carcinoma Treatment: Is There Still Hope? Front. Oncol. 11:683570. doi: 10.3389/fonc.2021.683570
Received: 21 March 2021; Accepted: 17 May 2021;
Published: 14 June 2021.
Edited by:
Christophe Le Tourneau, Institut Curie, FranceReviewed by:
Amanda Psyrri, University General Hospital Attikon, GreeceSandro J. Stoeckli, Kantonsspital St. Gallen, Switzerland
Copyright © 2021 Hyytiäinen, Wahbi, Väyrynen, Saarilahti, Karihtala, Salo and Al-Samadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmed Al-Samadi, YWhtZWQuYWwtc2FtYWRpQGhlbHNpbmtpLmZp