 Ruizhen Huang
Ruizhen Huang Chiyu Zhang
Chiyu Zhang Honglin Hu
Honglin Hu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oncol., 10 June 2021
Sec. Genitourinary Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.680842
This article is part of the Research TopicNephrectomy in Localized Renal Cell CarcinomaView all 6 articles
Objective: The choice of surgical method for clinically diagnosed T2 or higher stage kidney cancer remains controversial. Here, we systematically reviewed and collected published comparative studies on renal function, oncologic outcomes, and perioperative results of partial nephrectomy (PN) versus radical nephrectomy (RN) for larger renal tumors (T2 and above), and performed a meta-analysis.
Evidence Acquisition: Following searches of PubMed, Web of Science, and Embase, the original studies on PN vs. RN in the treatment of T2 renal cancer were screened through strict inclusion and exclusion criteria. RevMan 5.4 was used for data analysis of the perioperative results, renal function, and oncologic outcomes of the two surgical methods for T2 renal tumor therapy. The weighted mean difference was used as the combined effect size for continuous variables, while the odds ratio (OR) or risk ratio (RR) was used as the combined effect size for binary variables. Both variables used a 95% confidence interval (CI) to estimate statistical accuracy. In cases with low heterogeneity, the fixed-effects model was used to pool the estimated value; otherwise, the random-effects model was used when significant heterogeneity was detected.
Results: Fifteen retrospective studies including 5,056 patients who underwent nephrectomy (PN: 1975, RN: 3081) were included. The decline in estimated GFR (eGFR) after PN was lower than RN [(MD: −11.74 ml/min/1.73 m2; 95% CI: −13.15, −10.32; p < 0.00001)]. The postoperative complication rate of PN was higher than that of PN (OR: 2.09; 95% CI: 1.56, 2.80; p < 0.00001)], and the postoperative overall survival (OS) of PN was higher than that of RN (HR: 0.77; 95% CI: 0.65, 0.90; p = 0.002), and tumor recurrence (RR, 0.69; 95% CI: 0.53, 0.90; p = 0.007). No obvious publication bias was found in the funnel chart of the OS rates of the two groups of patients.
Conclusions: PN is beneficial for patients with T2 renal tumors in terms of OS and renal function protection. However, it is also associated with a higher risk of surgical complications.
Kidney cancer is a common tumor in the urinary system. According to the EAU Urology Kidney Cancer Diagnosis and Treatment Guidelines updated in 2014, radical nephrectomy (RN) should be performed for renal tumors of clinical T staging T2, or in patients with localized renal tumors that cannot be treated with nephron preservation (1). Clinically, for patients with localized T1a-b renal tumors, both partial nephrectomy (PN) and RN have been shown to have similar oncological effects. At the same time, studies have shown that patients with PN have less postoperative renal function decline than RN. Therefore, regardless of whether artificially-assisted laparoscopic or robot-assisted laparoscopic PN, PN is regarded as the best choice for the treatment of T1 renal tumors. It has been reported that the 10-year overall survival (OS) rate of patients with T1 stage renal tumors who underwent laparoscopic or open partial nephrectomy was associated with the patient’s age, comorbidities, surgical indications, and other factors, as well as the prediction of cancer-free survival rate, but not the surgical method itself. The choice of surgical method depends only on the surgeon’s preference and experience (2).
RN has long been the preferred surgical method for the treatment of T2 stage and larger renal tumors. Unfortunately, although this surgical method can effectively remove the tumor, the higher risk of postoperative renal insufficiency, postoperative bleeding, infection, and other underlying complications remain problematic compared to PN (3–5). Several observational studies have reported improved survival benefits for patients undergoing PN compared to those undergoing RN. The choice of PN over RN is considered important from a therapeutic perspective, because PN is associated with improved renal functional preservation, and may therefore be beneficial for prognosis and OS by lowering the risk of cardiovascular and metabolic sequelae (4, 6–8). Taken together, it seems, to some extent, that PN is superior to RN in the surgical management of renal cancer. However, recent studies involving PN in stage T2 or higher kidney tumors have attracted widespread attention, and among patients with larger kidney masses, PN does not compromise cancer-specific mortality. However, the choice of surgical method remains controversial. Therefore, we performed a systematic literature review and meta-analysis to summarize the efficacy and safety of PN vs. RN in the treatment of stage T2 or higher renal tumors.
The literature filter approach, search methods, information collection procedure, measured outcomes, and results synthesis were defined prospectively adhering to the PRISMA guidelines (9).
Original articles that met the following criteria were considered for inclusion: Original articles that involved studying the efficacy of PN vs. RN in the treatment of T2 renal tumors, or some subgroups; publications written in the English language; studies in which the patients undergoing nephrectomy were all adults (> 18 years old); both retrospective and prospective studies; studies meeting at least one of the required outcome indicators for this study. The exclusion criteria were as follows: Non-PN vs. RN research; comments, conference abstracts, reviews, or replies, in which relevant data could not be extracted; case reports; and studies in which the research subjects were animals, cells, or minors. The abstracts of the studies that met the inclusion criteria were scanned, and for those that met the requirements, a more comprehensive evaluation was performed by reviewing the full text. We also reviewed the reference lists of the original documents, and, to avoid unnecessary omission of any original documents required, we checked the references of similar meta-analysis articles.
We performed a search of the original research from PubMed database, Web of Science, and Embase from inception until September 2020. The search terms included the diagnostic terms “kidney mass” OR “renal cancer” OR “renal tumor” OR “7 cm” or “T2,” and the treatment intervention items “partial nephrectomy” OR “radical nephrectomy” OR “nephron-sparing surgery”. All steps were based on the meta-analysis of the PRISMA statement flow chart (Figure 1), and a comprehensive evaluation and data extraction was performed for the remaining articles.

Figure 1 PRISMA flow diagram of the search strategy and identification of relevant studies (10).
Prior to data extraction, an Excel table was prepared to store the required data. The data were extracted by RH and CZ in strict accordance with the inclusion and exclusion criteria, respectively. Any questions or disagreements regarding the data extraction from the two authors were negotiated with a third author (HH) to determine the final extraction plan. According to the collected statistics, the extracted information included literature characteristics (including author, case sources, study type, study period, number of cases in the PN and RN groups, surgical methods, average follow-up time), demographic characteristics (age, sex, tumor size, baseline renal function), perioperative outcomes (operation time, estimated blood loss, complications, length of stay in hospital), renal function outcomes (postoperative estimated GFR [eGFR], decline in eGFR), and tumor outcomes (tumor recurrence rate, overall survival rate, cancer-specific mortality, cancer-specific survival, and all-cause mortality).
The quality of the literature to be included was independently evaluated by RH and CZ. A third researcher (XW) independently evaluated the quality of the literature if there were divergences between the former two researchers. The results were then scored and a final decision was made. For randomized controlled trials, we used the Cochrane Systematic Evaluation Manual to conduct a comprehensive risk of bias assessment, including selection bias, outcome bias, test bias, attrition bias, and publication bias. The Newcastle-Ottawa scale (11) Documents with a score of ≤ 5 were considered low-quality, a score of 6–7 were classified as medium quality, and those with a score of 8–9 were classified as high-quality. The standards implemented by the Oxford University Center for Evidence-Based Medicine were used to further assess the level of documentary evidence (12).
RevMan 5.4, as recommended by the Cochrane manual, was used to statistically analyze the outcome indicators of each of the included studies. The weighted mean difference (WMD) was used as the combined effect size for continuous variables, while the odds ratio (OR) or risk ratio (RR) was used as the combined effect size for binary variables. Both variables used a 95% confidence interval (CI) to estimate statistical accuracy. The heterogeneity between each study was evaluated using Chi-square and I2, and statistical significance was set at p < 0.10. The random-effects model was used to combine the effect size in outcomes with significant heterogeneity (p < 0.1, I2 > 50%); otherwise, the fixed effects model was used (13). Sensitivity analysis was tested by the literature elimination method, in which the literature with the lowest weight and the literature with the lowest quality score in each index were eliminated to test whether the main results were robust. Publication bias was evaluated by visually inspecting the funnel plot.
Original literature in which data were presented as the median and interquartile ranges. Referred the validated mathematical model of (14, 15) to calculate the index data of the original literature and acquire the mean and standard deviation. The data conversion method was used to extract outcome indicators, such as cancer-specific survival (CSS), a natural logarithmic transformation of the HR of the original document [e.g., ln (HR)], thereby transforming the converted values into forest plots.
Fifteen retrospective studies including 5,056 patients who underwent nephrectomy (PN, 1975; RN, 3081) were included by careful selection (16–30). Among the included studies, the majority of cases were from the USA, and the remainder were varied. Single-center studies accounted for 60%, and the remaining 40% were multicenter studies. Except for some documents that did not clearly state the surgical method, most open surgeries were included in the documents. Interestingly, two original types of research on minimally invasive surgery are robot-assisted surgery (24, 27). The characteristics of the included studies are summarized in Table 1.
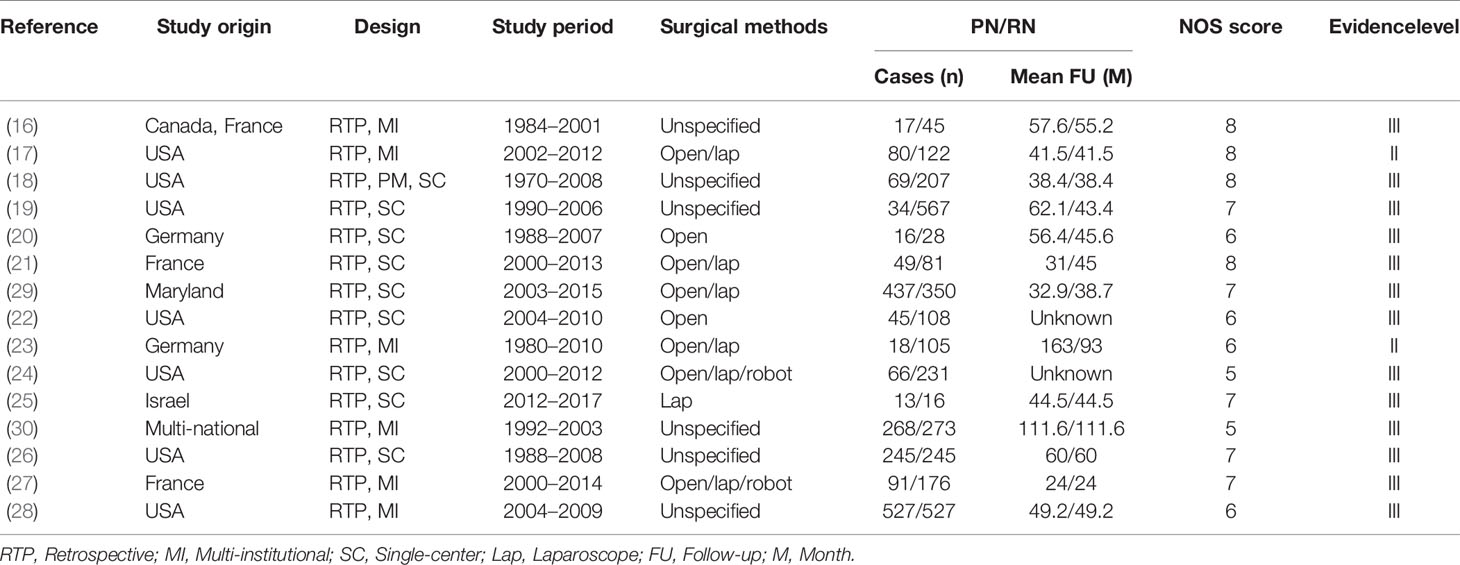
Table 1 Characteristics of the included studies.
Statistical analysis of some perioperative indicators (operating time, hospitalization time, and estimated blood loss during surgery) showed that compared to RN, patients who underwent PN had a longer operation time than those who underwent RN (MD: 44.85 min, 95% CI: 8.17, 81.52, p = 0.02; Figure 2), as well as a higher likelihood of estimated blood loss (MD: 103.85 ml, 95% CI: 77.13, 103.57; p < 0.00001, Figure 3). As for the length of stay, there was no significant difference between PN and RN. We combined the data of the length of stay in the literature and found no significant difference (MD: 0.12 days; 95% CI: −0.16, 0.41; p = 0.39, Figure 4).

Figure 2 Operative time.
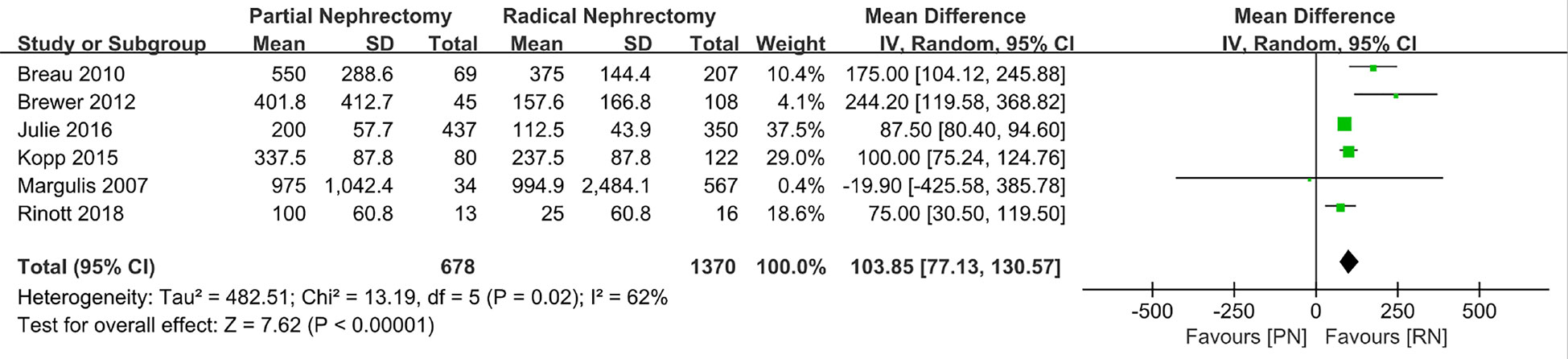
Figure 3 Estimated blood loss.
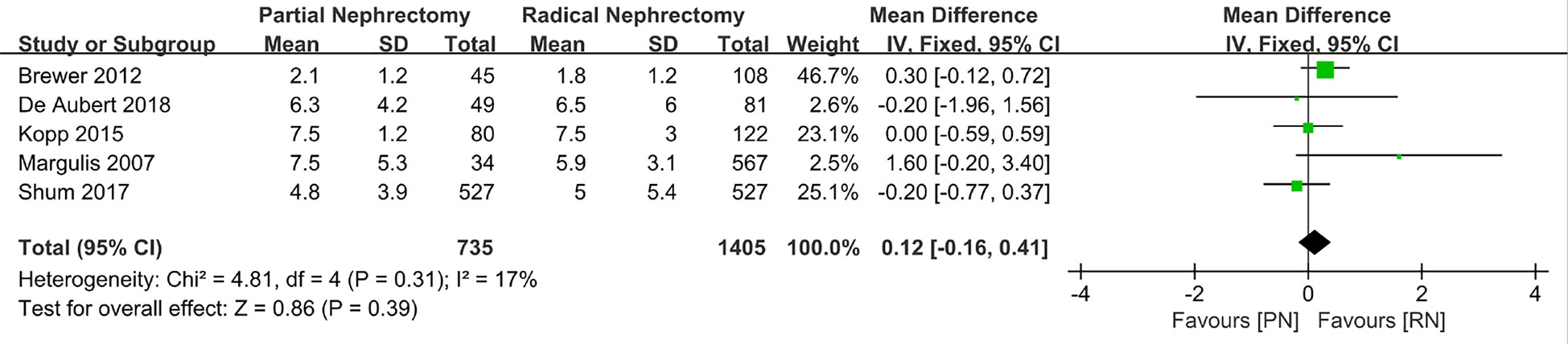
Figure 4 Length of stay.
We used the estimated glomerular filtration rate (eGFR) to estimate renal function and compared the preoperative eGFR, postoperative eGFR, and the decrease in eGFR (ΔeGFR: preoperative eGFR minus postoperative eGFR). The pooled effect size indicated that the preoperative eGFR was higher in patients with PN, and that these patients also had better baseline renal function (MD: 1.57 ml/min/1.73 Â m2; 95% CI: 0.70, 2.44; p = 0.0004; Figure 5). Moreover, after a short follow-up time, the postoperative renal function of patients who underwent RN was slightly worse than that of patients who underwent PN, as represented by the higher postoperative eGFR in the PN group (MD: 7.95 ml/min/1.73 Â m2; 95% CI: 4.86, 11.04; p < 0.00001; Figure 6). The renal function of the patients in both groups decreased following surgery. Our combined data analysis showed that ΔeGFR was statistically significant in the PN and RN groups, and that the decline in eGFR was even lower in the PN patients (MD: −11.74 Â min/1.73 m2; 95% CI: −13.15, −10.32; p < 0.00001; Figure 7); these findings indicated significantly better preservation of renal function in the PN group. Furthermore, the pooled results suggest a tendency for a lower complication rate in patients after RN surgery than after PN (OR: 2.09; 95% CI: 1.56, 2.80; p < 0.00001, Figure 8); thus, it seems that RN is superior in controlling postoperative complications.

Figure 5 Preoperative eGFR.

Figure 6 Postoperative eGFR.

Figure 7 Decline in eGFR.
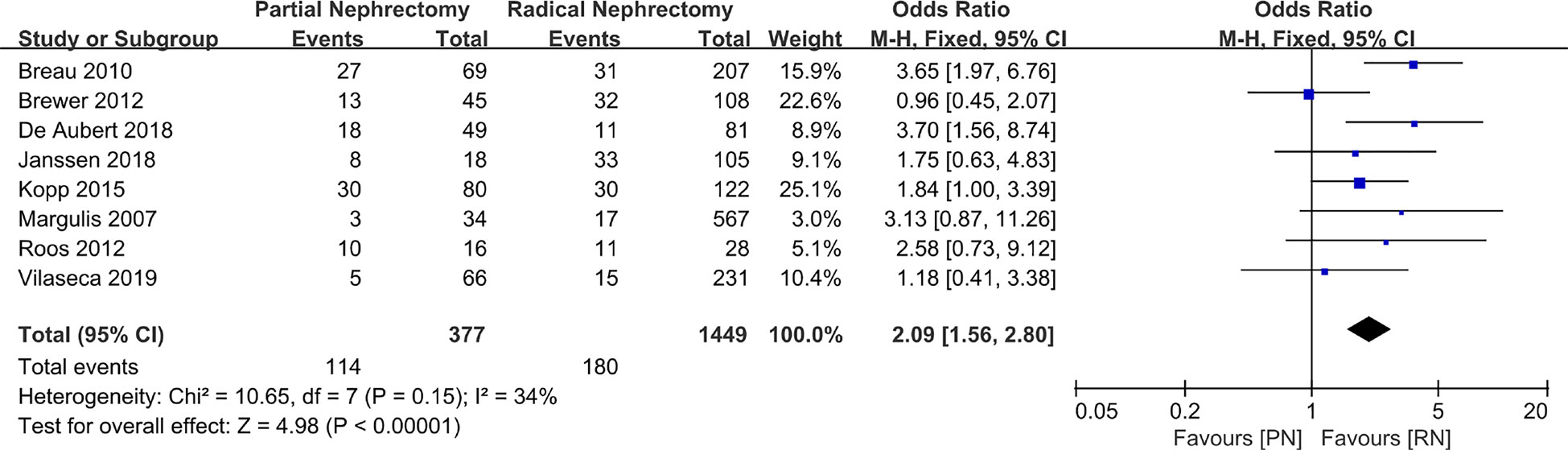
Figure 8 Complications.
With regard to the long-term outcome indicators, we failed to find any obvious differences between pooled cancer-specific mortality and cancer-specific survival, which indicate that PN and RN are not significantly different in the above two aspects (combined results, RR: 1.01; 95% CI: 0.46, 2.19; p = 0.99; Figure 9; and HR: 0.91; 95% CI: 0.68, 1.21; p = 0.66; Figure 10). The combined results showed a clear difference between PN and RN in terms of OS (HR: 0.77; 95% CI: 0.65, 0.90; p = 0.002; Figure 11). Patients who underwent PN generally had a longer OS than those who underwent RN, with low heterogeneity (I2 = 0%) among the included literature, showing a relatively stable pooled result. The combined effect size of all-cause mortality of PN patients was lower than that of RN patients (OR: 0.58; 95% CI: 0.39, 0.88; p = 0.01, Figure 12), also was it in the pooled tumor recurrence indicators (RR: 0.69; 95% CI: 0.53, 0.90; p = 0.007, Figure 13).
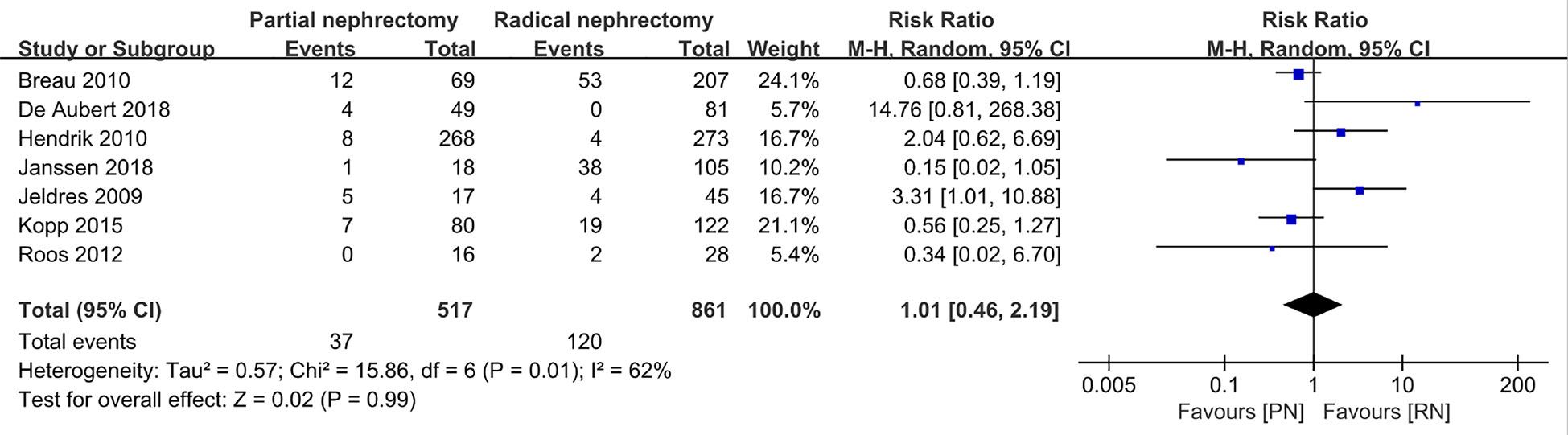
Figure 9 Cancer-specific mortality.
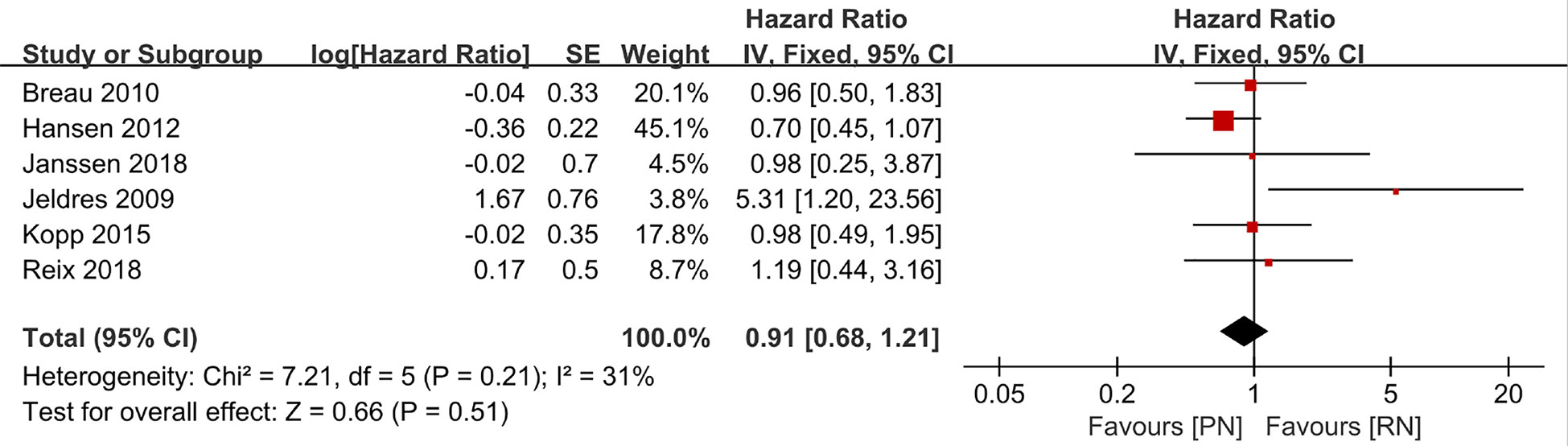
Figure 10 Cancer-specific survival.
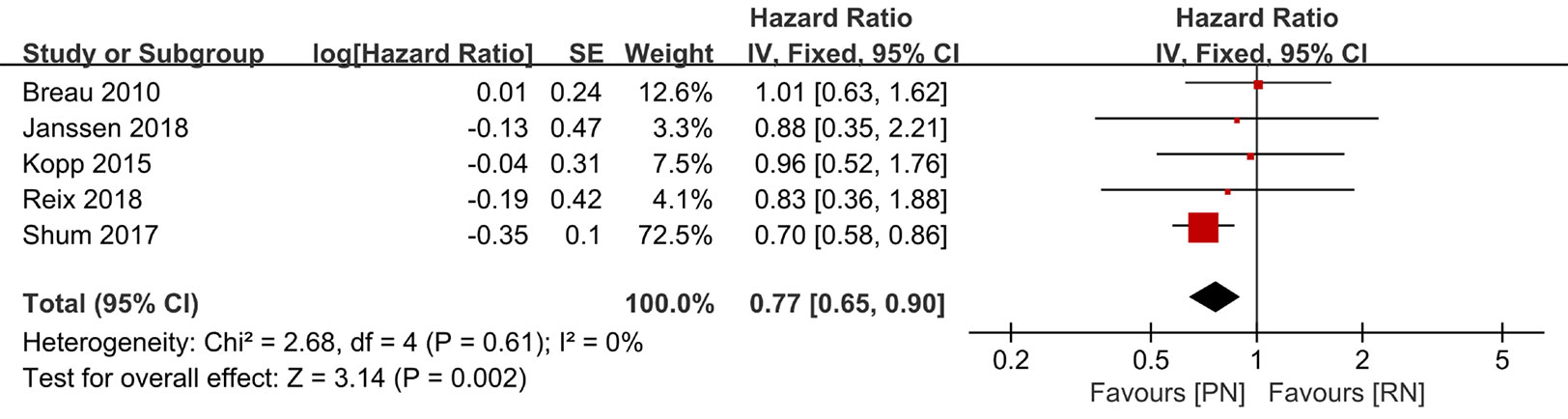
Figure 11 Overall survival.
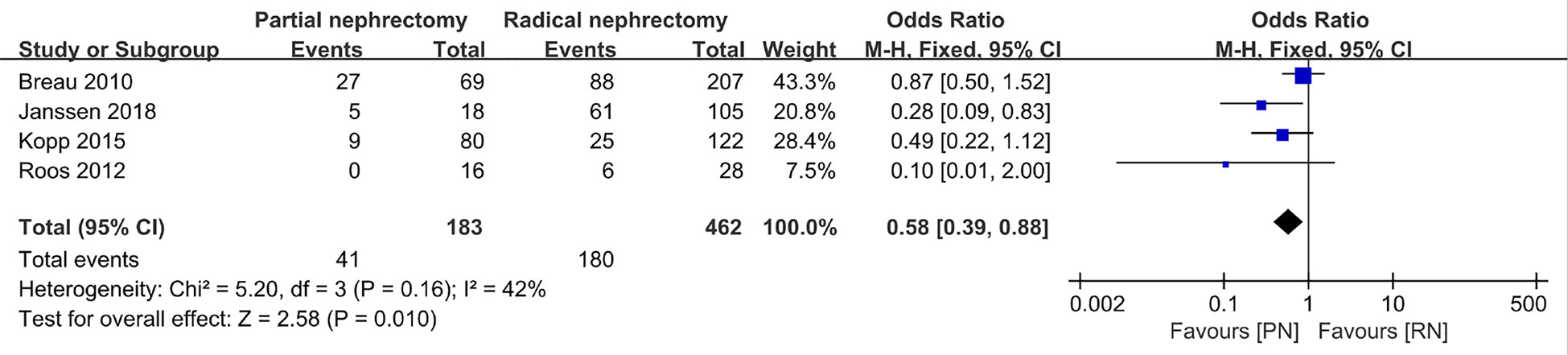
Figure 12 All-cause mortality.
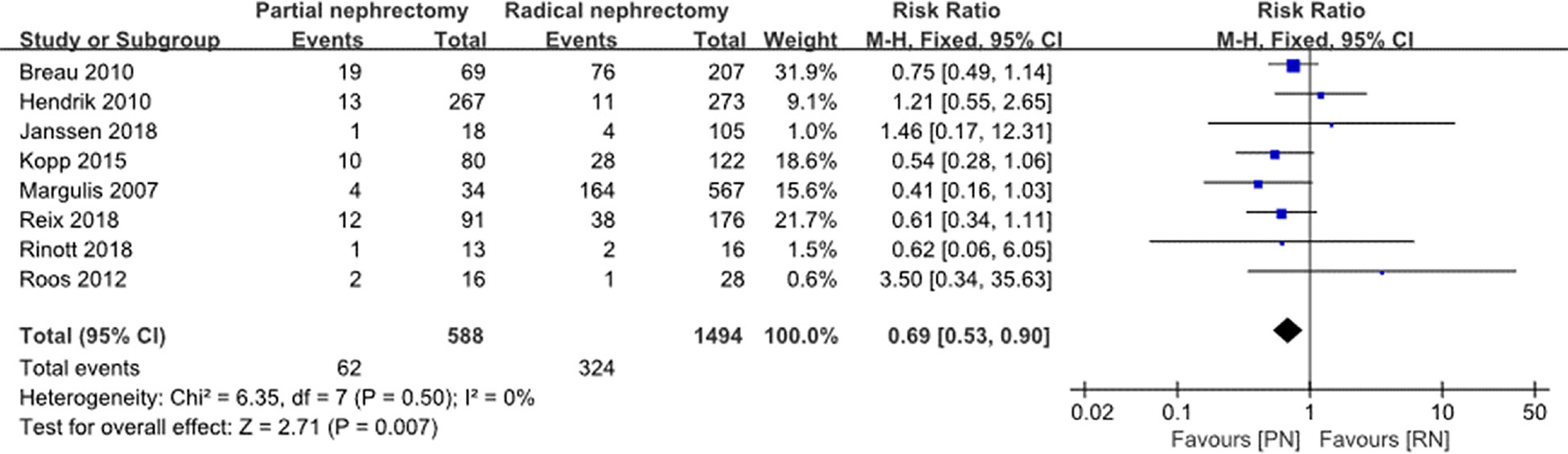
Figure 13 Tumor recurrence.
Sensitivity analysis of each combined result was performed by eliminating the original documents with the lowest weight and the lowest quality score in each outcome index one by one. As a result, the changes in p-values and the heterogeneity of the combined indicators were recorded and composed in the form of a table. Most of the outcome indicators did not change significantly after removing the relevant original literature one by one. By removing the lowest weighted reference study of the operation time, the heterogeneity was significantly changed from 86% to 0%, but after excluding the lowest quality score, there was no significant change (Table 2). In this study, the random-effects model was used to combine the effect size for the indicators with high heterogeneity (I2 > 50%); otherwise, the fixed effects model was used. In order to detect related publication bias, a funnel chart of OS was reported, as shown in Figure 14. All included documents were within 95% CI, and no obvious publication bias was observed.
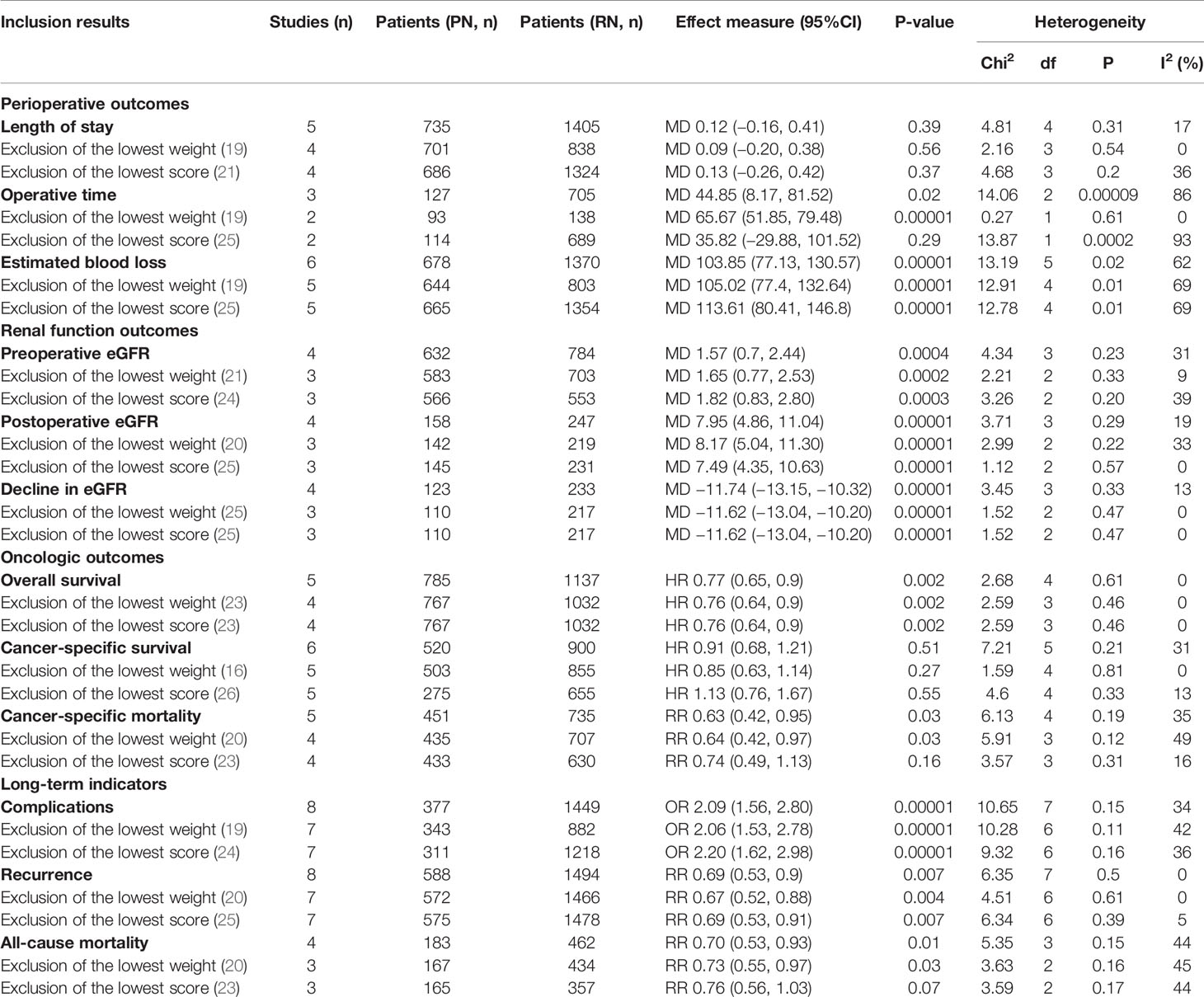
Table 2 Results of sensitivity analysis about comparison of PN vs. RN.
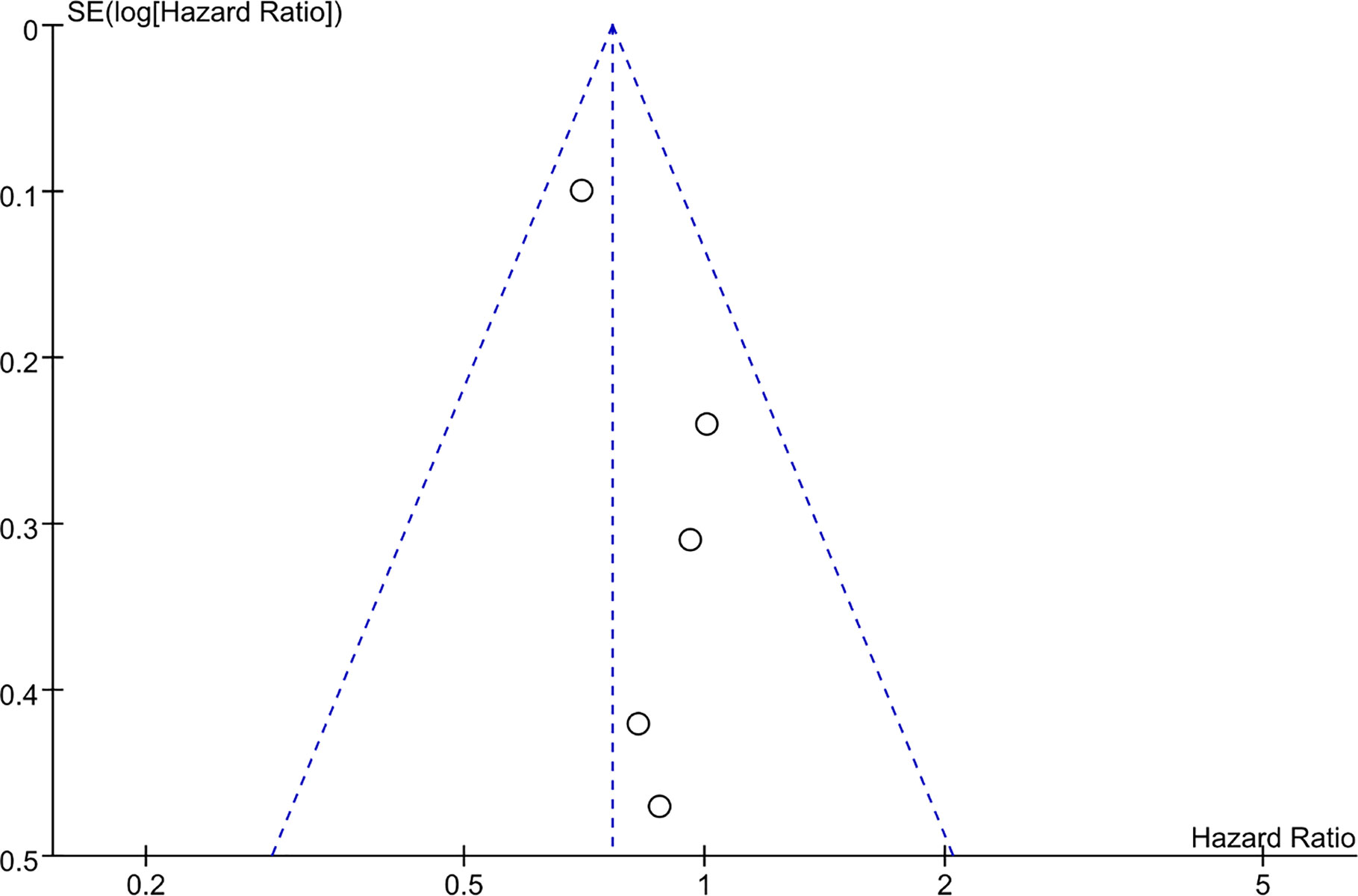
Figure 14 Funnel plot concerning overall survival.
We categorized the trials into two subgroups: clear cell carcinoma group and non-clear cell carcinoma group according to the cancer histology; based on the Fuhrman Grade, the low-grade (I-II) group and the high-grade (III-IV) group were also considered to be analyzed. Accordingly, 5 trials were included in the cancer histology subgroup, and 5 trials were also included in the Fuhrman Grade subgroup (Figure 15). The OR value in the low-grade subgroup was 1.13 (95%CI, 0.86, 1.49) and that in the high-grade subgroup was 0.84 (95% CI; 0.64, 1.01). Furthermore, the OR value in the clear cell carcinoma group was 0.64(95%CI, 0.34, 1.21) and that in the and non-clear cell carcinoma was 1.56 (95% CI; 0.83, 2.93). However, a high degree of heterogeneity was observed in the cancer histology subgroup (I2 = 75%).
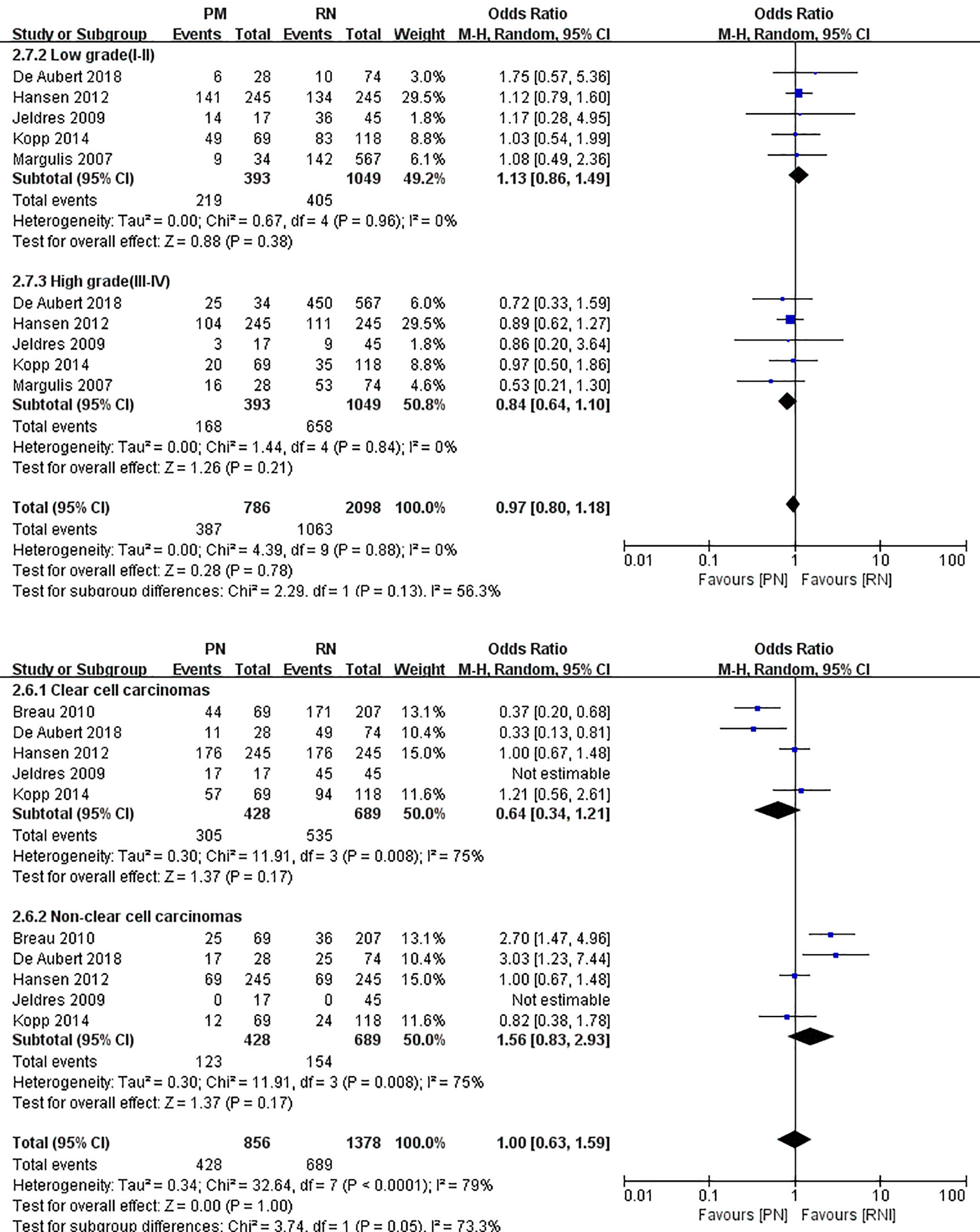
Figure 15 Subgroup analysis of Fuhrman Grade and cancer histology.
With advances in science and technology, PN for the treatment of larger kidney tumors is no longer theoretically feasible. However, RN is still regarded as a surgical method with greater reference value for larger clinical T2 renal tumors ≥ 7 cm. Based on this, the specific implementation of PN or RN remains controversial. The purpose of this study was to conduct a detailed systematic review and meta-analysis to evaluate whether the clinical diagnosis of T2 renal tumors should be PN or RN. To better understand the advantages and disadvantages of PN and RN in the treatment of T2 renal tumors, statistical analysis was performed with the aim to provide a reference for controversy in choosing PN or RN in cancer therapy and citing published retrospective research sample data for combined statistical analysis. We found that PN required a longer operation time (MD: 44.85 min; 95% CI: 8.17, 81.52; p = 0.02) and had higher intraoperative blood loss than RN (MD: 103.85 ml; 95% CI: 77.13, 103.57; p < 0.00001), which is a more technically demanding surgical method. PN also results in more complications compared to RN. Despite the above advantages, the benefits of RN in terms of OS and renal function protection are minimal compared to those of PN in the treatment of T2 stage renal cancer.
Because of a similar oncology control effect as RN, PN is also efficient in retaining residual renal function and reducing the incidence of postoperative chronic kidney disease in patients, which further benefits the cardiovascular system and the OS of patients. For T2 stage renal tumors, our combined effect size showed that neither PN nor RN was statistically significant in terms of cancer-specific mortality and cancer-specific survival rates. These findings indicate similarities in the effects of oncologic control in T2 stage renal tumors. Alanee et al. (31) obtained data from the SEER database to analyze the results of the surgical treatment of T2 renal tumors, and showed that compared to RN-treated patients, the cancer-specific mortality rate of PN was not inferior to RN (HR: 0.68; 95% CI: 0.50 –0.94). Further investigation showed that sex, age, race, tumor size > 10 cm, localized disease, and histopathological classification were all related to improved survival rate following PN (all p-values < 0.05). However, Hansen et al. (26) suggested that even in patients with relatively unfavorable tumor pathological results, PN would not reduce cancer-specific mortality, which was supported by the results of their multivariate analysis (HR, 0.67; 95% CI, 0.39–1.17, p = 0.2). Furthermore, according to research by Kopp et al. (17, 32), patients with renal cancer with R.E.N.A.L. scores ≥ 10 at stage T2 had an increased risk of tumor progression and decreased OS, suggesting that R.E.N.A.L. scores may be a more accurate reference tool for evaluating tumor prognosis than simple pathological staging. In our combined results, OS (HR: 0.77; 95% CI: 0.65, 0.90; p = 0.002), one of the main efficacy evaluation indexes of cancer treatment, showed significant differences between the two therapies, and the OS of the PN group was significantly better than that of the RN group. As the average follow-up time of each retrospective study that met the inclusion criteria was generally different (PN ranges from 24–163 months, RN ranges from 24–111.6 months), loss to follow-up deviation may still exist. Therefore, even if the statistics are not heterogeneous after merging, they still pose a huge information deviation. A larger sample in a multi-center, multi-country, multi-ethnic comprehensive analysis is essential. However, the combined OS in this study is still meaningful and can be used as a reference to provide a basis for clinical treatment.
For larger renal cell carcinoma, both the difficulty of the surgical procedure and the incidence of postoperative complications are increased while selecting partial nephrectomy as the strategy. A retrospective study conducted by Kopp et al. (17, 32) in the same patients population examined two different indicators: the survival rate and renal function score of PN vs. RN. They revealed that the two surgical methods had no significant difference in terms of the renal function score and survival rate of patients with T2 tumors, but that the incidence of complications in the PN group was significantly higher than that in the RN group (17.5% vs. 2.5%; p < 0.001), and 10% of patients had urine leakage after surgery. Furthermore, the operative time of patients who underwent PN was significantly longer than that of those who underwent RN (221 min vs. 153 min, p = 0.001). A longer operation time means longer intraoperative exposure, longer conditions of stress and ischemia, and longer tumor resection time and kidney reconstruction time than RN, all of which may lead to an increased incidence of postoperative complications. In addition, the larger the tumor, the larger the scope of resection, and the more complex the nature of the tumor, the higher the technological requirements for the surgeon. A larger resection scope can reduce the benefits of renal function, which are important risk factors the incidence of complications. During a prospective, randomized study in nephron sparing surgery (NSS)or RN conducted by the European Organization for Research and Treatment of Cancer Genito-Urinary Group (EORTC-GU) noninferiority phase 3 trial 30904, approximately 50% of the study subjects had T2 stage renal cancer. The results of the study found that in PN vs. RN, the incidence of bleeding (3.1% vs. 1.2%), urinary fistula (4.4% vs. 0%), and the rate of secondary operations (4.4% vs. 2.4%) were higher in the PN group (33). Studies have reported (34) that PN was associated with a significant incidence of complications and reduced renal function in patients with renal cancer > 7 cm. However, the postoperative results of selective indication PN were surprising in that they were similar to those of RN. In the case of selecting indications, the estimated values of 5-year cancer-free survival (CFS), CSS, and OS rates were 85.7%, 98%, and 93.9%, respectively, which were significantly higher than the 5-year CFS (60.5%), CSS (78.5%), and OS (70.6%) in the imperative indication group. In the sample study population, the necessary indications [defined as bilateral tumors, preoperative kidney disease (CKD stage < 2), and solitary kidney] and selective indications seem to play a key role in the prognosis. Breau et al. (18) retrospectively studied PN and RN and reported a low complication rate in both groups, and that urine leak in the PN group was resolved spontaneously under the action of the drainage tube and/or when the ureteral stent placed after the abdominal cavity was closed. Their research provides strong evidence for the safety and effectiveness of PN in the treatment of T2 renal cancer. In terms of postoperative complications, the risk of PN treatment for T2 renal cancer is also acceptable. Schwentner et al. (23) performed a study with a mean follow-up time of up to 102 months and confirmed that it is feasible to implement PN for renal cancer ≥ 7 cm in terms of acceptable technology and complications. Our combined results showed a lower tumor recurrence rate in the PN group (RR: 0.69; 95% CI: 0.53, 0.90; p = 0.007). When performing PN, patients are at a higher risk of local recurrence; therefore, the patients with more aggressive disease were probably managed with RN, resulting in a higher recurrence rate. As RN tends to be the preferred choice of surgery for larger tumors, selection bias may have led to this combined result, and a larger sample size investigation should be conducted for further validation. Based on these studies and our combined effect on complications, we believe that nephron-sparing surgery should be considered in patients with stage T2 RCC. The strict control of surgical indications and tumor conditions before PN surgery will provide the greatest benefits to patients.
Preoperative eGFR (17, 21, 24, 29) in the original literature, postoperative eGFR (17, 20, 21, 25), and decline in eGFR (20–22, 25) within a limited follow-up period to evaluate the effect of PN vs. RN on renal function. Cumulative analysis of the included studies showed that the preoperative eGFR was higher and the baseline renal function was better in patients who underwent PN (MD: 1.57 ml/min/1.73 Â m2; 95% CI: 0.70, 2.44; p = 0.0004). In addition, the postoperative eGFR in the PN group was higher than that in the RN group (MD: 7.95 Â ml/min/1.73 Â m2; 95% CI: 4.86, 11.04; p < 0.00001). ΔeGFR was significant in both PN and RN, but showed a smaller reduction in PN (MD: –11.74 Â ml/min/1.73 m2; 95% CI: –13.15, –10.32; p < 0.00001), indicating that PN is superior to RN in terms of preserving renal function. Due to the advantages of PN in preserving nephrons and protecting renal function, the use of PN for the treatment of larger renal tumors is justified. Clark et al. (3) dynamically measured the changes in 24-h urine CrCl and used the Cockcroft–Gault formula to calculate the eGFR. Their results demonstrated that the effect of PN on the deterioration of renal function during the postoperative period was minimal, while the effect of RN was pronounced. According to the results of Kopp et al. (17, 32), the average eGFR decreased more in patients with T2 renal cancer who underwent RN than those who underwent PN (–19.7 vs. –11.9 ml/min; p = 0.006); at the same time, the incidence of CKD caused by decreased renal function increased (40.2% vs. 16.3%; p < 0.001). Low-level eGFR accompanied by renal insufficiency may be related to the risk of increased mortality, increased cardiovascular events, and prolonged hospital stay. In line with this, the lower the eGFR value classification of CKD at each stage, the higher the risk of complications (8).
The results of comparative analysis showed 1121 patients with incident stage 4 or higher CKD, including 183 patients who underwent PN and 938 patients who underwent RN. Patients with larger tumors (T2) treated with PN showed an increased incidence of clinically significant postoperative CKD than those with T1 tumors (35). Besides, Mariusdottir et al. (36) revealed that the development of new-onset CKD was significantly lower after PN than after RN [n = 9 (*20%) vs. 19 (43%), p = 0.002]. Multivariate logistic regression analysis indicated that RN was an independent prognostic factor for new-onset CKD (OR = 3.07; 95% CI, 1.03–9.79; p = 0.04), which indicates that the renal function of patients with renal cancer should be assessed before surgery. If the patient’s CKD stage reaches stage 2, especially stage 2b, when PN is feasible, the strategy of nephron preservation surgery should be considered (37). A similar study was conducted by Chung et al. (38), the results of which demonstrated that compared to RN, PN had a more favorable effect on the OS of patients with renal dysfunction (CKD stage I and II) before surgery. However, for patients with CKD stage III, PN showed no obvious improvement in postoperative renal function, with no significant improvement in 5-year mortality.
To the best of our knowledge, the operation time of PN is longer than that of RN, irrespective of whether it is an open or minimally invasive surgery. According to the statistics of our hospital database, PN has a longer intraoperative time, even in patients with relatively small renal tumors. Additionally, previous literature shows that the average operation time of PN vs. RN in patients with T2 or greater renal tumors can be referred to. Our combined results showed the same result (MD: 44.85 min; 95% CI: 8.17, 81.52; p = 0.02). It is also worth noting that the combined effect size was heterogeneous (I2 = 86%). In the sensitivity analysis, we removed the lowest weighted reference (19) and found that the I2 dropped to 0%, while the literature with the lowest quality score (25) remained highly heterogeneous. The literature data increase the heterogeneity of the overall effect size. We further generated a forest plot and found that the data in the literature were also meaningless. The 95% CI intersects the invalid line in the middle. After removing the literature, the heterogeneity was significantly reduced, indicating that the data on operation time may not be suitable for use in this study. In general, PN requires a longer operation time than RN. The length of the operation is closely related to the operator and the configuration of personnel and equipment related to the operation. In the subgroup analyses, results showed that a high degree of heterogeneity in the cancer histology subgroup (I2 = 75%). The findings presented here must be generalized with caution because of heterogeneity, or, in other words, it seems whether PN or RN is not so closely related to the histology classification of kidney cancer. However, people that were in different Fuhrman Grade may have different surgical effects. The specific operational situation in each country was uneven, and inevitable information bias may have emerged during the data collection. In view of this, a complete, large-sample, multi-country, multi-ethnic prospective randomized trial is essential to validate our findings.
The shortcomings of this study are as follows: 1) The original documents included after the screening were all retrospective studies that had a large risk of information bias, and failing to include prospective randomized controlled studies may have had an adverse impact on our results; 2) for some articles that did not directly provide relevant data, we used the calculation methods provided by evidence-based medicine and statistical references, which may have led to selection bias; 3) due to insufficient data, we failed to conduct a hierarchical analysis and exploration based on the classification of postoperative complications, surgical methods (open, hand-assisted, and robot-assisted laparoscopy strategies), tumor pathological classification, and ischemia-reperfusion time for further recognition of the overall effect of PN vs. RN; 4) the choice of PN or RN was determined by the surgeon, and the time span of patients included in the study was large, during which, some surgical indications in these guidelines may have changed; and 5) the experience of the surgeon is different from the level of surgery, which may have an impact on the evaluation of PN and RN.
With the rise of PN as a method for the treatment of larger renal tumors, although PN is inferior to RN in terms of the operation time, intraoperative blood loss, and postoperative complications, it is still effective for larger kidney tumors. It is safe and feasible because of its outstanding preservation of kidney function, better OS, and lower all-cause mortality. PN is the first choice for the treatment of larger renal tumors; however, a more comprehensive consideration is necessary for patients with kidney masses at stage T2 or higher. Moreover, it is important to fully consider tumor factors and the deterioration of renal function before surgery to minimize postoperative complications, accelerate postoperative recovery, and improve quality of life, which is the end goal of treatment. Nevertheless, it is necessary to evaluate a larger sample size of PN vs. RN for the treatment of stage T2 or larger renal tumors, and further prospective randomized controlled studies will make the evaluation of efficacy more convincing.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
RH, CZ, XW, and HH acquired, analyzed, and interpreted the data and drafted the paper. HH conceptualized the study and design, analysis, and interpretation of data. RH performed manuscript writing and editing. All authors contributed to the article and approved the submitted version.
This work was supported by grants from the National Natural Science Foundation of China (No. 81860128) and the Natural Science Foundation of Jiangxi Province (No. 20171BAB205016). The funders had no role in the performance of the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Ljungberg B, Bensalah K, Canfield S, Dabestani S, Hofmann F, Hora M, et al. EAU Guidelines on Renal Cell Carcinoma: 2014 Update. Eur Urol (2015) 67(5):913–24. doi: 10.1016/j.eururo.2015.01.005
2. Lane BR, Campbell SC, Gill IS. 10-Year Oncologic Outcomes After Laparoscopic and Open Partial Nephrectomy. J Urol (2013) 190(1):44–9. doi: 10.1016/j.juro.2012.12.102
3. Clark AT, Breau RH, Morash C, Fergusson D, Doucette S, Cagiannos I. Preservation of Renal Function Following Partial or Radical Nephrectomy Using 24-Hour Creatinine Clearance. Eur Urol (2008) 54(1):143–49. doi: 10.1016/j.eururo.2008.03.037
4. Huang WC, Levey AS, Serio AM, Snyder M, Vickers AJ, Raj GV, et al. Chronic Kidney Disease After Nephrectomy in Patients With Renal Cortical Tumours: A Retrospective Cohort Study. Lancet Oncol (2006) 7(9):735–40. doi: 10.1016/S1470-2045(06)70803-8
5. Huang WC, Elkin EB, Levey AS, Jang TL, Russo P. Partial Nephrectomy Versus Radical Nephrectomy in Patients With Small Renal Tumors–Is There a Difference in Mortality and Cardiovascular Outcomes? J Urol (2009) 181(1):55–61; discussion -2. doi: 10.1016/j.juro.2008.09.017
6. Karellas ME, O’Brien MF, Jang TL, Bernstein M, Russo P. Partial Nephrectomy for Selected Renal Cortical Tumours of >/= 7 cm. BJU Int (2010) 106(10):1484–7. doi: 10.1111/j.1464-410X.2010.09405.x
7. Long CJ, Canter DJ, Kutikov A, Li T, Simhan J, Smaldone M, et al. Partial Nephrectomy for Renal Masses >/= 7 cm: Technical, Oncological and Functional Outcomes. BJU Int (2012) 109(10):1450–6. doi: 10.1111/j.1464-410X.2011.10608.x
8. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic Kidney Disease and the Risks of Death, Cardiovascular Events, and Hospitalization. N Engl J Med (2004) 351(13):1296–305. doi: 10.1056/NEJMoa041031
9. Available at: http://www.prisma-statement.org/documents/PRISMA%202009%20checklist.pdf.
10. Moher D, Liberati A, Tetzlaff J, Altman DG, , The PRISMA Group. Preferred Reporting Items for Systematic Reviewsand Meta-Analyses: The PRISMA Statement. PLoSMed (2009) 6(7):e1000097. doi: 10.1371/journal.pmed1000097
11. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available at: www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
12. Phillips B, Ball C, Sackett D, Badenoch D, Straus S. Levels of Evidence and Grades of Recommendation. Oxf Cent Evid Based Med Website. Available at: http://www.cebm.net/index.aspx?o=1025.
13. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. Cochrane Collab (2011). Available at: http://handbook.cochrane.org2011.
14. Hozo SP, Djulbegovic B, Hozo I. Estimating the Mean and Variance From the Median, Range, and the Size of a Sample. BMC Med Res Methodol (2005) 5:13. doi: 10.1186/1471-2288-5-13
15. Wan X, Wang W, Liu J, Tong T. Estimating the Sample Mean and Standard Deviation From the Sample Size, Median, Range and/or Interquartile Range. BMC Med Res Methodol (2014) 14:135. doi: 10.1186/1471-2288-14-135
16. Jeldres C, Patard JJ, Capitanio U, Perrotte P, Suardi N, Crepel M, et al. Partial Versus Radical Nephrectomy in Patients With Adverse Clinical or Pathologic Characteristics. Urology (2009) 73(6):1300–5. doi: 10.1016/j.urology.2008.08.492
17. Kopp RP, Liss MA, Mehrazin R, Wang S, Lee HJ, Jabaji R, et al. Analysis of Renal Functional Outcomes After Radical or Partial Nephrectomy for Renal Masses >/=7 cm Using the RENAL Score. Urology (2015) 86(2):312–9. doi: 10.1016/j.urology.2015.02.067
18. Breau RH, Crispen PL, Jimenez RE, Lohse CM, Blute ML, Leibovich BC. Outcome of Stage T2 or Greater Renal Cell Cancer Treated With Partial Nephrectomy. J Urol (2010) 183(3):903–8. doi: 10.1016/j.juro.2009.11.037
19. Margulis V, Tamboli P, Jacobsohn KM, Swanson DA, Wood CG. Oncological Efficacy and Safety of Nephron-Sparing Surgery for Selected Patients With Locally Advanced Renal Cell Carcinoma. BJU Int (2007) 100(6):1235–9. doi: 10.1111/j.1464-410X.2007.07225.x
20. Roos FC, Brenner W, Thomas C, Jager W, Thuroff JW, Hampel C, et al. Functional Analysis of Elective Nephron-Sparing Surgery vs Radical Nephrectomy for Renal Tumors Larger Than 4 cm. Urology (2012) 79(3):607–13. doi: 10.1016/j.urology.2011.10.073
21. de Saint Aubert N, Audenet F, McCaig F, Delavaud C, Verkarre V, Le Guilchet T, et al. Nephron Sparing Surgery in Tumours Greater Than 7cm. Prog Urol (2018) 28(6):336–43. doi: 10.1016/j.purol.2018.03.009
22. Brewer K, O’Malley RL, Hayn M, Safwat MW, Kim H, Underwood W 3rd, et al. Perioperative and Renal Function Outcomes of Minimally Invasive Partial Nephrectomy for T1b and T2a Kidney Tumors. J Endourol (2012) 26(3):244–8. doi: 10.1089/end.2011.0384
23. Schwentner C, Janssen MWW, Linxweiler J, Terwey S, Rugge S, Ohlmann CH, et al. Survival Outcomes in Patients With Large (≥7cm) Clear Cell Renal Cell Carcinomas Treated With Nephron-Sparing Surgery Versus Radical Nephrectomy: Results of a Multicenter Cohort With Long-Term Follow-Up. PloS One (2018) 13(5). doi: 10.1371/journal.pone.0196427
24. Vilaseca A, Guglielmetti G, Vertosick EA, Sjoberg DD, Grasso A, Benfante NE, et al. Value of Partial Nephrectomy for Renal Cortical Tumors of cT2 or Greater Stage: A Risk-Benefit Analysis of Renal Function Preservation Versus Increased Postoperative Morbidity. Eur Urol Oncol (2020) 3(3):365–71. doi: 10.1016/j.euo.2019.04.003
25. Rinott Mizrahi G, Freifeld Y, Klein I, Boyarsky L, Zreik R, Orlin I, et al. Comparison of Partial and Radical Laparascopic Nephrectomy: Perioperative and Oncologic Outcomes for Clinical T2 Renal Cell Carcinoma. J Endourol (2018) 32(10):950–4. doi: 10.1089/end.2018.0199
26. Hansen J, Sun M, Bianchi M, Rink M, Tian Z, Hanna N, et al. Assessment of Cancer Control Outcomes in Patients With High-Risk Renal Cell Carcinoma Treated With Partial Nephrectomy. Urology (2012) 80(2):347–53. doi: 10.1016/j.urology.2012.04.043
27. Reix B, Bernhard JC, Patard JJ, Bigot P, Villers A, Suer E, et al. Overall Survival and Oncological Outcomes After Partial Nephrectomy and Radical Nephrectomy for cT2a Renal Tumors: A Collaborative International Study From the French Kidney Cancer Research Network Uroccr. Prog Urol (2018) 28(3):146–55. doi: 10.1016/j.purol.2017.12.004
28. Shum CF, Bahler CD, Sundaram CP. Matched Comparison Between Partial Nephrectomy and Radical Nephrectomy for T2 N0 M0 Tumors, a Study Based on the National Cancer Database. J Endourol (2017) 31(8):800–5. doi: 10.1089/end.2017.0190
29. An JY, Ball MW, Gorin MA, Hong JJ, Johnson MH, Pavlovich CP, et al. Partial vs Radical Nephrectomy for T1-T2 Renal Masses in the Elderly: Comparison of Complications, Renal Function, and Oncologic Outcomes. Urology (2017) 100:151–7. doi: 10.1016/j.urology.2016.10.047
30. Van Poppel H, Da Pozzo L, Albrecht W, Matveev V, Bono A, Borkowski A, et al. A Prospective, Randomised EORTC Intergroup Phase 3 Study Comparing the Oncologic Outcome of Elective Nephron-Sparing Surgery and Radical Nephrectomy for Low-Stage Renal Cell Carcinoma. Eur Urol (2011) 59(4):543–52. doi: 10.1016/j.eururo.2010.12.013
31. Alanee S, Nutt M, Moore A, Holland B, Dynda D, Wilber A, et al. Partial Nephrectomy for T2 Renal Masses: Contemporary Trends and Oncologic Efficacy. Int Urol Nephrol (2015) 47(6):945–50. doi: 10.1007/s11255-015-0975-3
32. Kopp RP, Mehrazin R, Palazzi KL, Liss MA, Jabaji R, Mirheydar HS, et al. Survival Outcomes After Radical and Partial Nephrectomy for Clinical T2 Renal Tumours Categorised by R.E.N.A.L. Nephrometry Score. BJU Int (2014) 114(5):708–18. doi: 10.1111/bju.12580
33. Van Poppel H, Da Pozzo L, Albrecht W, Matveev V, Bono A, Borkowski A, et al. A Prospective Randomized EORTC Intergroup Phase 3 Study Comparing the Complications of Elective Nephron-Sparing Surgery and Radical Nephrectomy for Low-Stage Renal Cell Carcinoma. Eur Urol (2007) 51(6):1606–15. doi: 10.1016/j.eururo.2006.11.013
34. Bigot P, Hetet JF, Bernhard JC, Fardoun T, Audenet F, Xylinas E, et al. Nephron-Sparing Surgery for Renal Tumors Measuring More Than 7 cm: Morbidity, and Functional and Oncological Outcomes. Clin Genitourin Cancer (2014) 12(1):e19–27. doi: 10.1016/j.clgc.2013.09.004
35. Leppert JT, Lamberts RW, Thomas IC, Chung BI, Sonn GA, Skinner EC, et al. Incident CKD After Radical or Partial Nephrectomy. J Am Soc Nephrol (2018) 29(1):207–16. doi: 10.1681/ASN.2017020136
36. Mariusdottir E, Jonsson E, Marteinsson VT, Sigurdsson MI, Gudbjartsson T. Kidney Function Following Partial or Radical Nephrectomy for Renal Cell Carcinoma: A Population-Based Study. Scand J Urol (2013) 47(6):476–82. doi: 10.3109/21681805.2013.783624
37. Hamilton ZA, Capitanio U, Lane BR, Larcher A, Yim K, Dey S, et al. Should Partial Nephrectomy be Considered “Elective” in Patients With Stage 2 Chronic Kidney Disease? A Comparative Analysis of Functional and Survival Outcomes After Radical and Partial Nephrectomy. World J Urol (2019) 37(11):2429–37. doi: 10.1007/s00345-019-02650-9
38. Chung JS, Son NH, Lee SE, Hong SK, Jeong CW, Kwak C, et al. Partial Versus Radical Nephrectomy for T1-T2 Renal Cell Carcinoma in Patients With Chronic Kidney Disease Stage III: A Multiinstitutional Analysis of Kidney Function and Survival Rate. J Korean Med Sci (2018) 33(43):e277. doi: 10.3346/jkms.2018.33.e277
Keywords: kidney cancer, partial nephrectomy, radical nephrectomy, meta-analysis, renal function, oncologic outcome
Citation: Huang R, Zhang C, Wang X and Hu H (2021) Partial Nephrectomy Versus Radical Nephrectomy for Clinical T2 or Higher Stage Renal Tumors: A Systematic Review and Meta-Analysis. Front. Oncol. 11:680842. doi: 10.3389/fonc.2021.680842
Received: 15 March 2021; Accepted: 21 May 2021;
Published: 10 June 2021.
Edited by:
Antonio Augusto Ornellas, National Cancer Institute (INCA), BrazilReviewed by:
Ari Adamy, Santa Casa Hospital, BrazilCopyright © 2021 Huang, Zhang, Wang and Hu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Honglin Hu, aG9uZ2xpbmh1QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.