
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 24 May 2021
Sec. Skin Cancer
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.672172
This article is part of the Research TopicWomen in Skin Cancer: 2021View all 24 articles
 Katharina C. Kähler1*
Katharina C. Kähler1* Ralf Gutzmer2Friedegrund Meier3,4Lisa Zimmer5Markus Heppt6Anja Gesierich7Kai-Martin Thoms8Jochen Utikal9,10Jessica C. Hassel11Carmen Loquai12Claudia Pföhler13
Ralf Gutzmer2Friedegrund Meier3,4Lisa Zimmer5Markus Heppt6Anja Gesierich7Kai-Martin Thoms8Jochen Utikal9,10Jessica C. Hassel11Carmen Loquai12Claudia Pföhler13 Lucie Heinzerling6,14Martin Kaatz15Daniela Göppner16Annette Pflugfelder17
Lucie Heinzerling6,14Martin Kaatz15Daniela Göppner16Annette Pflugfelder17 Ann-Sophie Bohne1Imke Satzger2Lydia Reinhardt3,4Jan-Malte Placke5
Ann-Sophie Bohne1Imke Satzger2Lydia Reinhardt3,4Jan-Malte Placke5 Dirk Schadendorf5
Dirk Schadendorf5 Selma Ugurel5
Selma Ugurel5Background: The combination of BRAF and MEK inhibitors has become standard of care in the treatment of metastatic BRAF V600-mutated melanoma. Clinical factors for an early prediction of tumor response are rare. The present study investigated the association between the development of an early exanthema induced by vemurafenib or vemurafenib plus cobimetinib and therapy outcome.
Methods: This multicenter retrospective study included patients with BRAF V600-mutated irresectable AJCC-v8 stage IIIC/D to IV metastatic melanoma who received treatment with vemurafenib (VEM) or vemurafenib plus cobimetinib (COBIVEM). The development of an early exanthema within six weeks after therapy start and its grading according to CTCAEv4.0 criteria was correlated to therapy outcome in terms of best overall response, progression-free (PFS), and overall survival (OS).
Results: A total of 422 patients from 16 centers were included (VEM, n=299; COBIVEM, n=123). 20.4% of VEM and 43.1% of COBIVEM patients developed an early exanthema. In the VEM cohort, objective responders (CR/PR) more frequently presented with an early exanthema than non-responders (SD/PD); 59.0% versus 38.7%; p=0.0027. However, median PFS and OS did not differ between VEM patients with or without an early exanthema (PFS, 6.9 versus 6.0 months, p=0.65; OS, 11.0 versus 12.4 months, p=0.69). In the COBIVEM cohort, 66.0% of objective responders had an early exanthema compared to 54.3% of non-responders (p=0.031). Median survival times were significantly longer for patients who developed an early exanthema compared to patients who did not (PFS, 9.7 versus 5.6 months, p=0.013; OS, not reached versus 11.6 months, p=0.0061). COBIVEM patients with a mild early exanthema (CTCAEv4.0 grade 1-2) had a superior survival outcome as compared to COBIVEM patients with a severe (CTCAEv4.0 grade 3-4) or non early exanthema, respectively (p=0.047). This might be caused by the fact that 23.6% of patients with severe exanthema underwent a dose reduction or discontinuation of COBIVEM compared to only 8.9% of patients with mild exanthema.
Conclusions: The development of an early exanthema within 6 weeks after treatment start indicates a favorable therapy outcome upon vemurafenib plus cobimetinib. Patients presenting with an early exanthema should therefore be treated with adequate supportive measures to provide that patients can stay on treatment.
Melanoma patients treated with BRAF and MEK inhibitors frequently develop an exanthema, also referred to as “skin rash” by non-dermatologists. This exanthema is typically characterized by inflammatory macules and papules but may also present with pustules or urticae. Its first signs commonly show within the first four to six weeks after therapy start. In the pivotal COBRIM trial the incidence of a skin rash upon monotherapy with vemurafenib was reported to be around 67.5% and during combination therapy with vemurafenib/cobimetinib the incidence was slightly higher with 72.5% (1). However, the term “skin rash” covers a variety of cutaneous side effects and thus cannot be equated with exanthema. Studies of EGFR inhibitors demonstrated an association of skin rash development with an improved therapy outcome in various cancer entities including colorectal carcinoma, head-and-neck squamous cell carcinoma, non-small cell lung cancer, prostate cancer, gastro-esophageal cancer, pancreatic adenocarcinoma and cutaneous squamous cell carcinoma (2, 3). Thus, in these cancer entities patients presenting with a skin rash under EGFR inhibitor therapy are encouraged to continue this treatment with the prospect of an increased probability of a favorable treatment outcome. For BRAF and MEK inhibition in metastatic melanoma, so far, no correlation has been reported between treatment efficacy and outcome and the occurrence of cutaneous side effects.
The present study was aimed to investigate the frequency and severity of an early exanthema upon BRAF and MEK inhibition with vemurafenib alone or combined with cobimetinib and its association with therapy outcome in patients with metastatic melanoma.
This multicenter retrospective study was initiated by the Dermatologic Cooperative Oncology Group (DeCOG), and undertaken with Ethics Committee approval (Hannover University Medical School, 1612-2012). Patients were identified for study inclusion at clinical centers of the DeCOG based on the following eligibility criteria: histologically proven diagnosis of melanoma, unresectable metastatic disease in stage III or IV following the American Joint Committee on Cancer version 8 (AJCCv8) criteria (4), detection of a BRAF V600 mutation in the tumor tissue, treatment with vemurafenib as a single agent (VEM) or as the combination of cobimetinib plus vemurafenib (COBIVEM) within a time frame of June 01, 2012 and April 30, 2018, either as per clinical trial or via prescription, and availability of follow-up data after treatment start including adverse events, response and survival. The patients were identified at the centers via their digital hospital information systems or by chart review, and the requested data were extracted from the respective patient files.
The requested data were collected on standardized electronic case report forms and merged in one central database for analysis. The data comprised patient demographics, BRAF V600 mutation subtype, sites of metastasis, overall performance status (OPS) graded by Eastern Cooperative Oncology Group (ECOG) criteria, and serum LDH activity, all at onset of VEM or COBIVEM therapy. For categorization of metastatic sites, we used the AJCCv8 M category by grouping by localization of metastases regardless of serum LDH activity. The used groups were (a) metastases to skin and/or lymph nodes (skin/LN), (b) metastases to the lung (lung), (c) metastases to other organs (other organs), and (d) metastases to the brain (brain). Data on other systemic treatments received by the patients before VEM or COBIVEM were recorded as previous treatments. This pre-treatment was categorized into (a) regimens containing immune checkpoint inhibitors (checkpoint inhibition), and (b) regimens containing kinase inhibitors (BRAF/MEK inhibition). Collected data on the course and outcome of VEM or COBIVEM therapy included therapy duration, best response following RECIST criteria (5) categorizing into complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD), as well as progression-free (PFS) and overall survival (OS). Patients were grouped into either objective responders (CR+PR) or non-responders (SD+PD). An exanthema presenting within the first six weeks after start of VEM or COBIVEM therapy was considered as an early exanthema, regardless of its morphology (macular, papular, pustular, urticae). The severity of the exanthema was graded according to CTCAEv4.0 (grade 1, <10% body surface area (BSA); grade 2, 10-30% BSA; grade 3, 30-100% BSA; grade 4, 100% BSA and/or severe reduction of general condition; grade 5, death) (6).
Data analysis was performed between January 01 and March 31, 2019. Survival (PFS, OS) was calculated from onset of VEM or COBIVEM until death or disease progression, respectively. If no such event occurred, the date of last patient contact was used as survival end point (censored observation). Survival curves, hazard ratios, and median survival times were calculated using the Kaplan–Meier method for censored failure time data. The log-rank test was used for comparison of survival probabilities between groups. Differences between groups were calculated using Fisher’s exact test or Chi square test. P<0.05 was considered statistically significant.
Data were collected of 422 patients at 16 clinical cancer centers in Germany. In total, 299 patients received VEM, 123 patients received COBIVEM. The patient flow is shown in Figure 1; detailed patient characteristics are presented in Tables 1, 2. An early exanthema occurring within the first 6 weeks after start of therapy occurred in 61 VEM patients (20.4%) (CTCAE grade 1, 62.3%; grade 2, 22.9%; grade 3, 11.4%; and grade 4, 3.2%) and in 53 COBIVEM patients (43.1%) (CTCAE grade 1, 28.3%; grade 2, 22.6%; grade 3, 45.2%; and grade 4, 3.7%). Representative patients from both cohorts are demonstrated in Figure 2. In the VEM cohort, most patient characteristics at therapy start were balanced between groups with and without occurrence of an early exanthema, besides patients’ sex with females more often represented within the group of patients developing early exanthema than males (p=0.043; Table 1). In the COBIVEM cohort, the overall performance status at therapy start differed significantly between groups with and without occurrence of an early exanthema with patients presenting at ECOG 0 being strongly over-represented in the group developing an early exanthema (p=0.0058; Table 2). Age or LDH were not identified to be an influencing factor for the incidence of early exanthema (p= 0.11, Table 2).
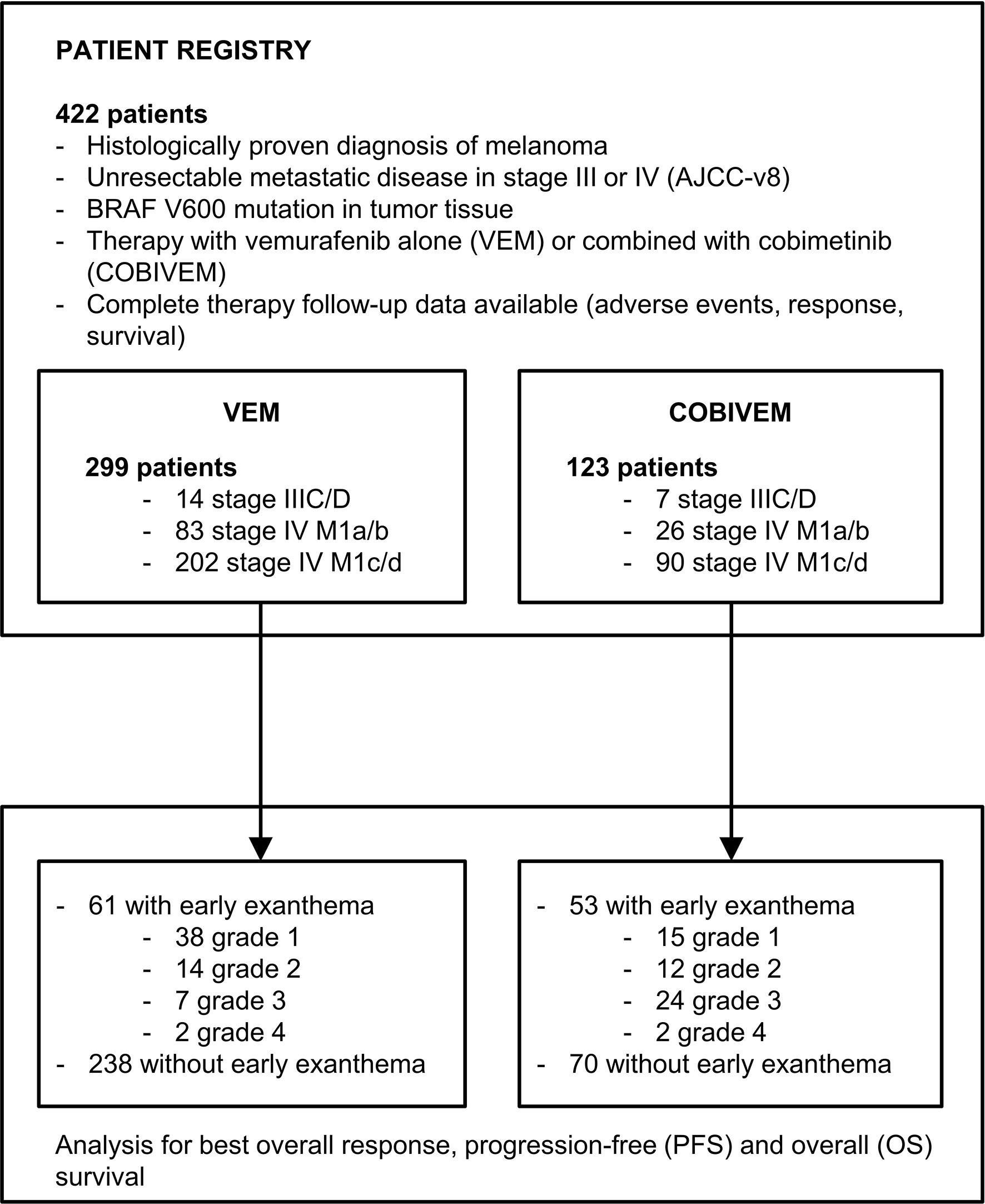
Figure 1 Schematic presentation of the study patient flow into patient registry. Patient inclusion criteria and grading of the early exanthemas was performed according to CTCAEv4.0 (grade 1, <10% body surface area (BSA); grade 2, 10-30% BSA; grade 3, 30-100% BSA; grade 4, 100% BSA and/or severe reduction of general condition).
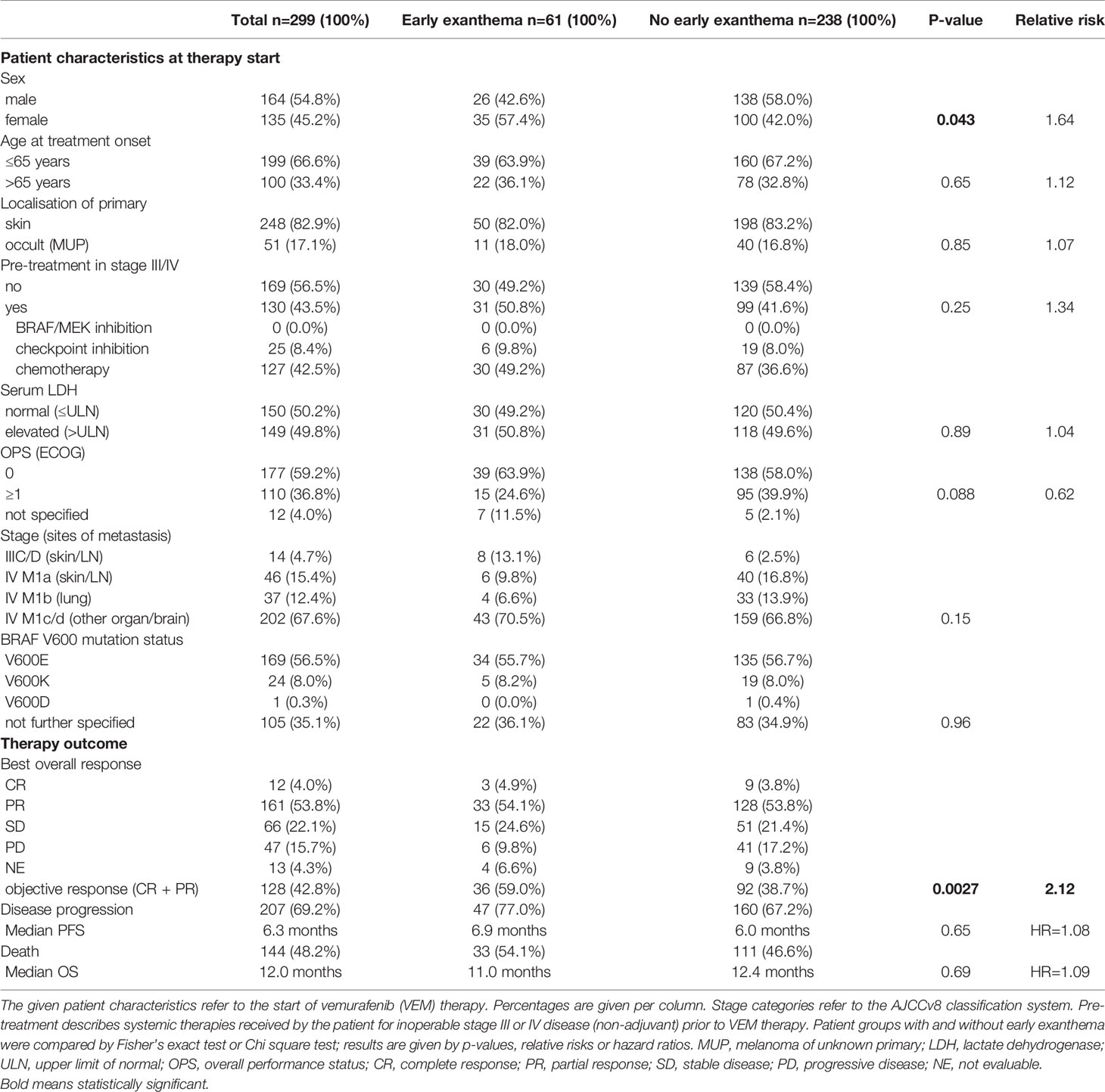
Table 1 Patients treated with vemurafenib (VEM).
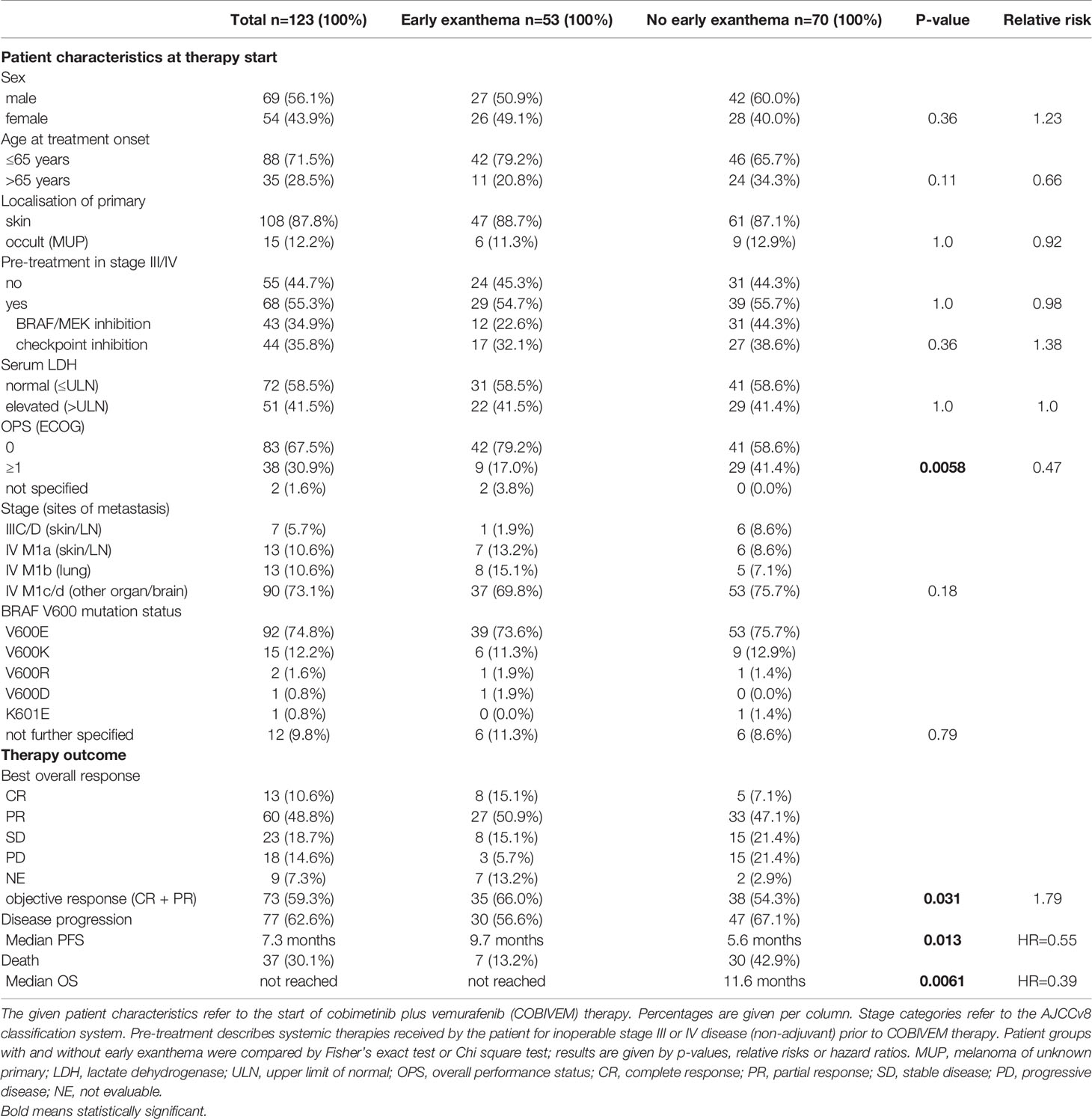
Table 2 Patients treated with cobimetinib plus vemurafenib (COBIVEM).
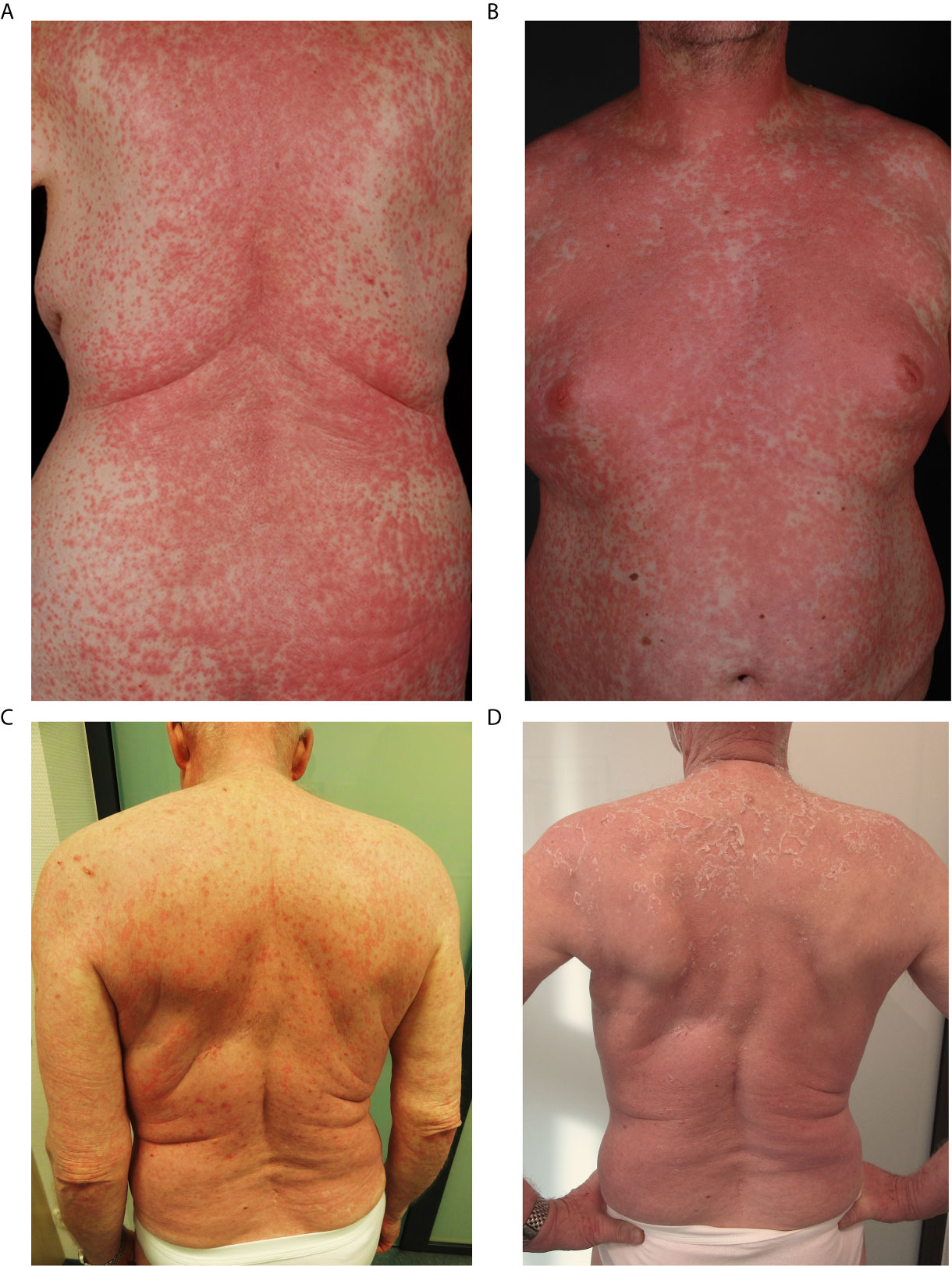
Figure 2 Representative patients from the study cohorts showing an early exanthema defined as onset within 6 weeks upon start of vemurafenib (A) or vemurafenib plus cobimetinib (B), both grade 4 according to CTCAEv4.0. (C) Exanthem during vemurafenib and cobimetinib (D) follow-up after 4 weeks of topical and systemic steroids.
All patients started with the initial doses of 960 mg vemurafenib orally b.i.d. (VEM) or vemurafenib 960 mg orally b.i.d. plus cobimetinib 60 mg orally once daily (COBIVEM). Due to the occurrence of an early exanthema, 32.7% of VEM patients and 26.8% of COBIVEM patients had a dose reduction, and 11.4% of VEM and 5.7% of COBIVEM patients had a therapy discontinuation. At database closure on September 30, 2019, the median follow-up time was 21.6 months. 48.2% of the VEM patients and 30.1% of the COBIVEM patients had died. Of the patients alive, 27.4% were still on VEM treatment, and 30.8% on COBIVEM treatment.
As best overall response, 4.0% of VEM patients achieved a CR, 53.8% achieved a PR, 22.1% showed a SD, and 15.7% revealed a disease progression. 4.3% of the patients were not evaluable for treatment response due to other reasons. Patients presenting an early exanthema upon VEM revealed a superior therapy response with an objective response rate (CR+PR) of 59.0% in patients showing an early exanthema versus 38.7% in patients without this cutaneous reaction (p=0.0027; Table 1). In the patient cohort treated with COBIVEM, 10.6% of patients achieved a CR, 48.8% achieved a PR, 18.7% showed a SD, and 14.6% revealed disease progression. 7.3% of the patients were not evaluable for therapy response. Here again, patients showing an early exanthema upon treatment had a higher objective response rate than patients who did not (66.0% versus 54.3%; p=0.031; Table 2).
With regard to survival after therapy start, for patients treated with VEM median PFS and OS were not significantly different for patients with or without an early exanthema (6.9 versus 6.0 months, p=0.65; 11.0 versus 12.4 months, p=0.69 respectively, Figures 3A, B). Additionally, the respective Kaplan-Meier survival curves were almost identical in shape and were crossing each other repeatedly. In contrast, for patients treated with COBIVEM survival after therapy start was significantly better in patients presenting an early exanthema. Median PFS and OS were significantly prolonged in patients showing an early exanthema versus patients who did not (PFS, 9.7 versus 5.6 months, p=0.013; OS, not reached versus 11.6 months, p=0.0061; Figures 4A, B). With regard to the severity of the early exanthema, patients who developed a mild exanthema (CTCAE grade 1-2) had a superior outcome in terms of PFS and OS compared to patients who developed a severe (CTCAE grade 3-4) exanthema or patients who developed no exanthema (p=0.047, Figures 4C, D).
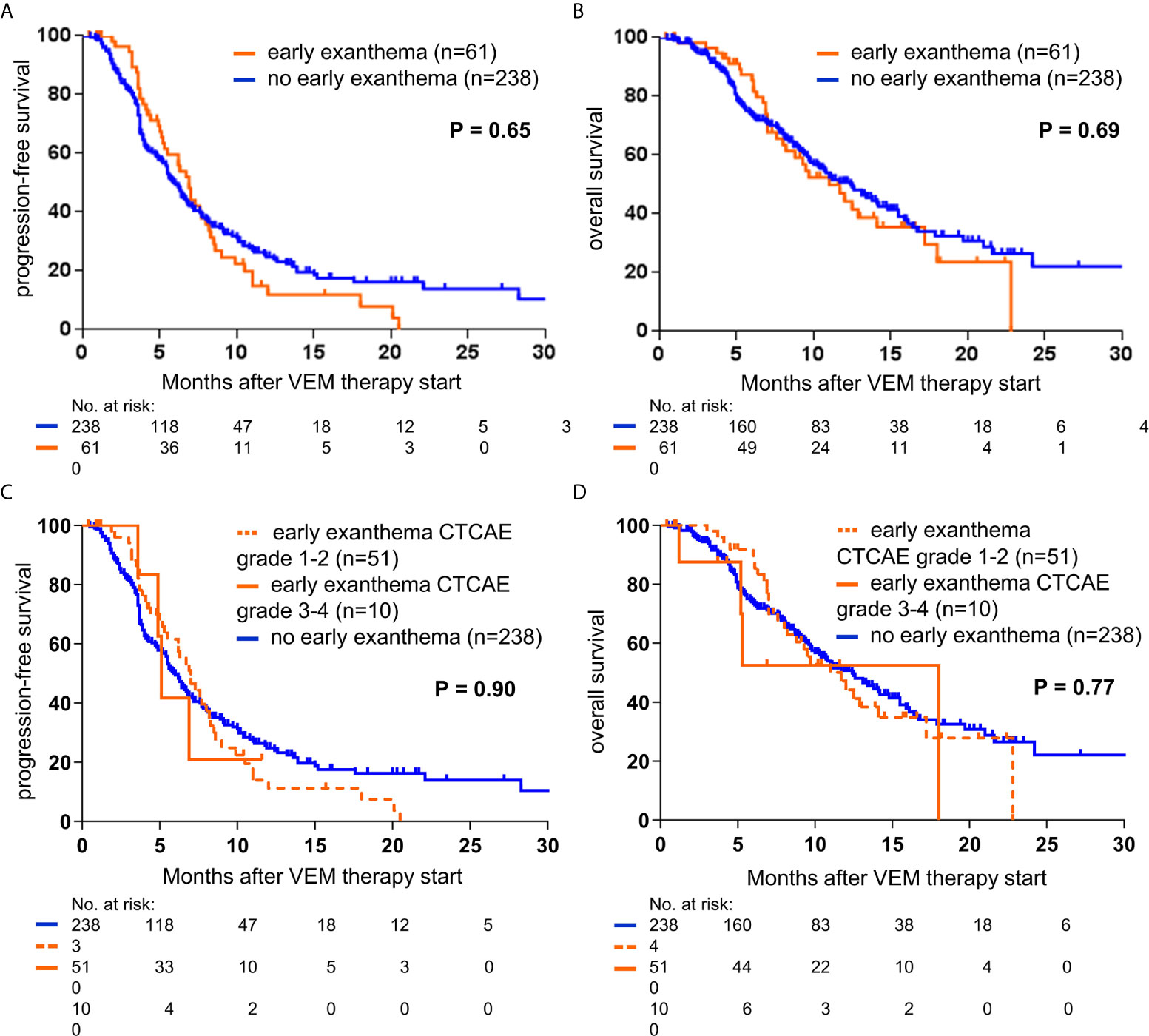
Figure 3 Kaplan-Meier curves showing the probability of progression-free (A, C), and overall survival (B, D), of metastatic melanoma patients treated with vemurafenib (VEM; n=299). Survival curves are displayed for patients with or without presentation of early exanthema upon treatment. Censored observations are indicated by vertical bars. P-values were calculated using the log rank test.
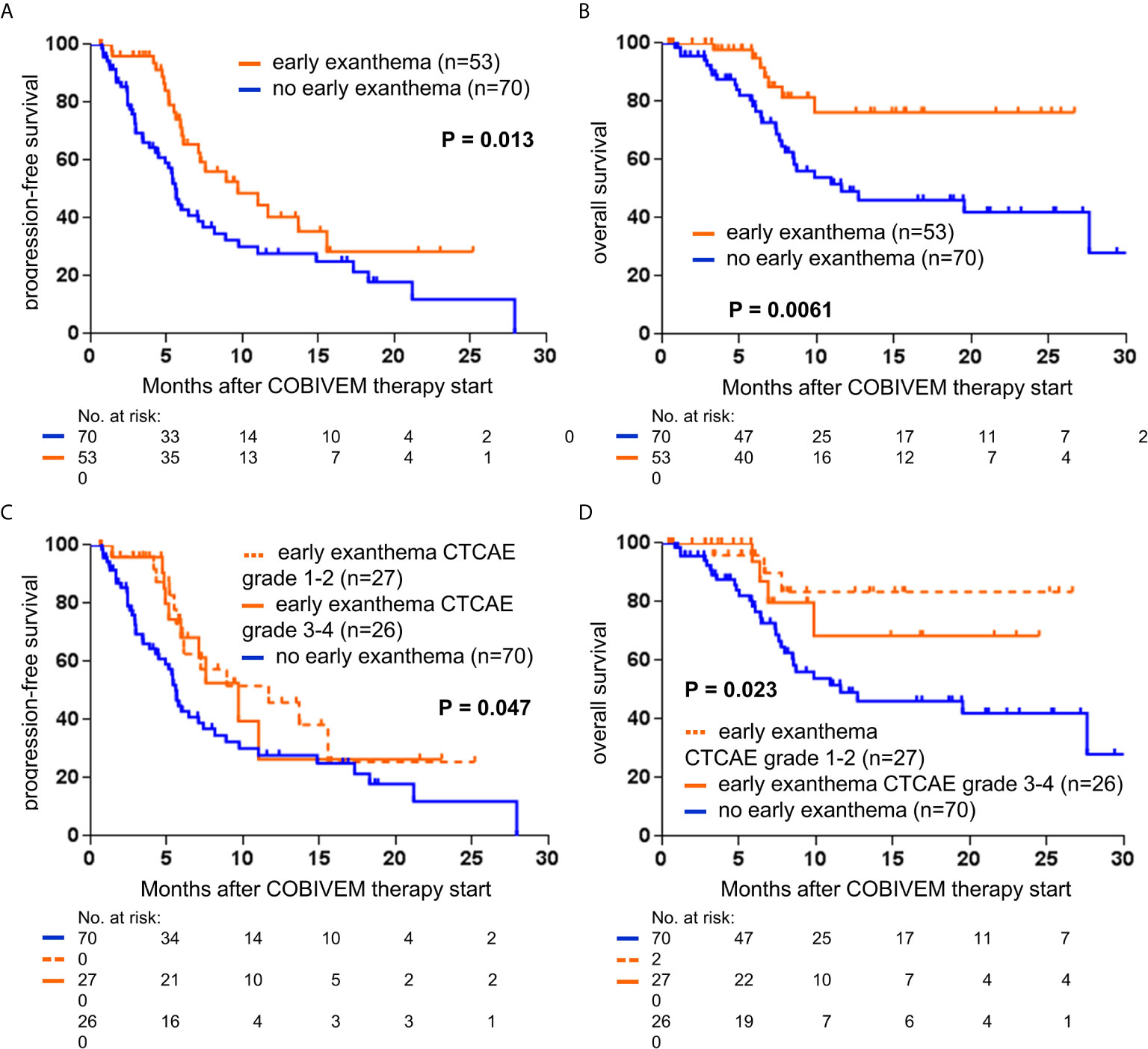
Figure 4 Kaplan-Meier curves showing the probability of progression-free (A, C) and overall survival (B, D) of metastatic melanoma patients treated with vemurafenib plus cobimetinib (COBIVEM; n=123). Survival curves are displayed for patients with or without presentation of early exanthema upon treatment. Censored observations are indicated by vertical bars. P-values were calculated using the log rank test.
Vemurafenib is a selective inhibitor of V600-mutated BRAF, and was the first-in-class mitogen-activated protein (MAP) kinase pathway inhibitor approved for the treatment of melanoma (7). Subsequently, the combination therapy of vemurafenib together with the MEK inhibitor cobimetinib was approved for metastatic melanoma due to the significant prolongation of survival times shown by clinical trial data (1, 8). Nevertheless, predictive markers of the treatment outcome of either vemurafenib monotherapy or vemurafenib plus cobimetinib combination therapy are rare and most often characterized by low specificity. Elevated serum LDH, as well as multiple organ involvement by metastases were shown to be associated with a less favorable treatment outcome of BRAF/MEK inhibition (9). However, these parameters are likewise associated with a poor treatment outcome upon immune checkpoint inhibition (10). Thus, other biomarkers associated with treatment outcome are urgently required to indicate a patient’s individual probability to benefit from vemurafenib/cobimetinib therapy. Optimally, these markers are detectable immediately before treatment start. However, biomarkers which become evident shortly after treatment start like cutaneous adverse events may also be of great help.
So far, only one retrospective analysis showed a possible correlation between the cutaneous side effects panniculitis and vitiligo-like lesions and the treatment outcome upon the BRAF plus MEK inhibitor combination dabrafenib and trametinib (11). Another retrospective case series showed a correlation between different cutaneous and extra-cutaneous adverse events including vitiligo, erythema nodosum, uveitis and keratitis sicca and the treatment outcome upon BRAF inhibitors either administered alone or in combination with MEK inhibitors (12). However, all these adverse events were reported in patients under BRAF/MEK inhibition, but at low frequencies and thus are of little use as predictive markers of treatment response in the majority of patients treated with BRAF/MEK inhibitors.
In contrast, exanthema is a common adverse event in patients treated with BRAF/MEK inhibitors (13). In clinical trials, 15.7% of patients treated with encorafenib/binimetinib developed a low grade rash/maculopapular rash (high grade 1%). Additional 3.1% showed an acneiform exanthem (high grade 0%). 27.7% of patients treated with dabarafenib/trametinib developed a low grade rash/maculopapular rash (high grade 1.5%). Additional 6.6% showed an acneiform exanthema (high grade 0%). The combination of vemurafenib/cobimetinib induced in 56.3% of patients a low grade rash/maculopapular rash (high grade 12.6%). Additional 13.8% showed an acneiform exanthema (high grade 2.4%). Important to acknowledge is the fact, that non-dermatologists do not differentiate between the common term rash and the specific characteristics of e.g. a maculopapular exanthema or acneiform exanthema (13). Additionally, in clinical trials the onset of exanthema is not specified, so the reported incidence of exanthema does not give further information about the rate of early exanthemas within the first weeks of treatment initiation. Moreover, an exanthema develops early during treatment, most often within the first four to six weeks of treatment, and is easily detectable by an inspection of the patient’s skin (13). These advantages render the detection of an early exanthema as a useful indicator of a favorable treatment outcome.
Interestingly, in the VEM cohort, females were more often represented within the group of patients developing early exanthema than males (p=0.043; Table 1). This has also been demonstrated to be a known risk factor for rash induced by BRAF/MEK inhibitors in the metaanalysis of Hopkins et al. (14).
This early exanthema is usually treated by a dose reduction of the BRAF/MEK inhibitors in combination with topical steroids and only in rare, severe cases with systemic steroids. Due to their early exanthema, 32.7% of VEM patients and 26.8% of COBIVEM patients needed a dose reduction.
Indeed, in our study we found that the occurrence of an exanthema within the first six weeks of treatment was significantly associated with an improved response rate and a prolonged survival in terms of PFS and OS in patients treated with COBIVEM. In patients treated with VEM, the development of an early exanthema was correlated with an improved objective response, but did not show an association to an improved survival.
Possible reasons for this differential impact on survival remain to be elucidated. First it should be mentioned that the early exanthema during COBIVEM and other BRAF/MEK combination therapies has to be differentiated from the acneiform rash induced specifically by MEK inhibitor monotherapies. This acneiform rash commonly occurs later during treatment, most often between week 6 and 12 after treatment start, and has a well-defined causal mechanism (13). The early exanthema developing within the first six weeks of COBIVEM treatment might be induced by the immune activation described for MEK inhibition therapies. It has been demonstrated that COBIVEM as well as dabrafenib plus trametinib therapy induces a type I interferon response in keratinocytes which acts proinflammatory and antineoplastically (15). In histopathology analysis, a slight basal layer vacuolization, dermal edema and a superficial dermal perivascular lymphocyte and eosinophil infiltrate was described (16). Also, it has been demonstrated that a pre-treatment with MEK inhibitors enhances immune responses, tumor-infiltrating T cells, and an immune-stimulating tumor microenvironment (17).
Interestingly, patients developing a mild exanthema revealed a stronger benefit from COBIVEM therapy than patients with a severe exanthema or patients without any exanthema. This finding might be explained by the fact that of the patients who developed a severe exanthema, 18.7% underwent a dose reduction of COBIVEM and 4.9% completely discontinued the treatment, compared to only 8.1% of patients who developed a mild exanthema that needed a dose reduction and 0.8% that discontinued the treatment. In contrast, it has been shown that dose reductions of BRAF/MEK inhibitors due to early toxicity in the first 28 days are significantly associated with improved survival, progression free survival and response (18, 19). However, following our present results, patients developing an early exanthema upon COBIVEM are patients with a high probability of a favorable therapy outcome and should thus be supported to continue treatment with COBIVEM. This support can be provided by an adequate therapeutic management of the exanthema, e.g. by the use of topical corticosteroids and/or anti-pruritics.
In conclusion, our results indicate that the development of an early exanthema upon BRAF/MEK inhibition with COBIVEM is a surrogate marker of a favorable therapy outcome in metastatic melanoma patients. Thus, patients presenting with an early exanthema under COBIVEM therapy should be treated with adequate supportive measures to provide that patients can stay on treatment. As a limitation, our findings result from a retrospective analysis and should therefore be confirmed in prospective clinical trials or registries.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Ethics Committee approval (Hannover University Medical School, 1612-2012). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
SU and KK contributed to conception and design of the study. All authors contributed to the acquisition pf data. SU organized the database. SU and KK performed the statistical analysis. KK wrote the first draft of the manuscript. SU and KK wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
This study was performed within the network of study centers of the German Dermatologic Cooperative Oncology Group (DeCOG). This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
KK has served as consultant or/and has received honoraria from Amgen, Roche, Bristol Myers Squibb, Merck Sharp and Dohme, Pierre Fabre, and Novartis, and received travel support from Amgen, Merck Sharp and Dohme, Bristol Myers Squibb, Amgen, Pierre Fabre, Medac, and Novartis. RG received honoraria for lectures and advisory boards, research support and meeting support from Almirall Hermal, Amgen, Astra Zeneca, Bristol Myers Squibb, Leo, Merck Serono, Merck Sharp and Dohme, Pierre Fabre, Roche, Sanofi Genzyme, Regeneron, Sun Pharma, Takeda, Pfizer, Novartis, Johnson&Johnson, 4SC, and Incyte. FM has received travel support or/and speaker’s fees or/and advisor’s honoraria by Novartis, Roche, BMS, MSD and Pierre Fabre, and research funding from Novartis and Roche. LZ has served as consultant and/or has received honoraria from Roche, Bristol Myers Squibb, Merck Sharp and Dohme, Novartis, Pierre Fabre, and Sanofi, and received travel support from Bristol Myers Squibb, Merck Sharp and Dohme, Amgen, Pierre Fabre, and Novartis. MH has received consultant and/or speaker honoraria form Bristol Myers Squibb, Novartis, Merck Sharp and Dohme, Sanofi, Roche and travel support from Novartis, and Bristol Myers Squibb. AG reports speakers honoraria from Bristol Myers Squibb, Merck Sharp and Dohme, and Roche, advisory board honoraria from Bristol Myers Squibb, Novartis, Merck Sharp and Dohme, Pierre Fabre, Pfizer, Roche and Sanofi Genzyme, and travel support from Bristol Myers Squibb, Merck Sharp and Dohme, Novartis, and Roche. K-MT received honoraria for lectures and advisory boards from Bristol-Myers Squibb, Roche, Novartis, Merck Sharp and Dohme, Pierre Fabre, LEO, Galderma, AbbVie, La Roche-Posay and Candela, and travel support from Bristol-Myers Squibb, Roche, Novartis, Merck Sharp and Dohme, Pierre Fabre, LEO, and Candela. JU is on the advisory board or has received honoraria and travel support from Amgen, Bristol Myers Squibb, GSK, LeoPharma, Merck Sharp and Dohme, Novartis, Pierre Fabre, Roche, Sanofi outside the submitted work. JH reports speakers honoraria from Bristol Myers Squibb, Novartis, Merck Sharp and Dohme, and Roche, advisory board honoraria from Merck Sharp and Dohme, Pierre Fabre, Sunpharma and Sanofi Genzyme, and travel support from Bristol Myers Squibb, and Pierre Fabre. CL declares speakers and advisory board honoraria and travel support from Bristol Myers Squibb, Merck Sharp and Dohme, Merck Serono, Novartis, Roche, Amgen, Pierre Fabre, and Sun Pharma. CP received speaker or consultant honoraria and travel support from Novartis, Bristol Myers Squibb, Roche, Merck Serono, Merck Sharp and Dohme, Celgene, AbbVie, and LEO. LH received grants from Novartis, and has received speaker or consultant fees personal fees from Amgen, Bristol Myers Squibb, Merck Sharp and Dohme, Roche, Curevac, Pierre Fabre, Roche, Novartis, and Sanofi. MK has received grants from Bristol Myers Squibb, Merck Sharp and Dohme, Leo, Novartis, and Roche.
DG declares speakers and advisory honoraria as well as travel support from Bristol Myers Squibb, Novartis, Pierre Fabre, Sanofi Genzyme, Amgen, Galderma, Janssen, and Roche.
DS declares advisory board and speakers honoraria from Roche, Novartis, Bristol-Myers-Squibb, MSD, Merck-Serono, Sanofi, Nektar, Amgen, Hexal, InFlaRx, Array, Pierre Fabre, Immunocore, Philogen Sun Pharma, Regeneron, and Ultimovacs, as well as grant and travel support from Roche, Novartis, Bristol-Myers-Squibb, MSD, Merck-Serono, and Sanofi. SU declares research support from Bristol Myers Squibb, and Merck Serono, speakers and advisory board honoraria from Bristol Myers Squibb, Merck Sharp and Dohme, Merck Serono, Novartis and Roche, and travel support from Bristol Myers Squibb, Merck Sharp, and Dohme.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We wish to thank all patients participating in this study, as well as their families and caregivers.
1. Dréno B, Ribas A, Larkin J, Ascierto PA, Hauschild A, Thomas L, et al. Incidence, Course, and Management of Toxicities Associated With Cobimetinib in Combination With Vemurafenib in the coBRIM Study. Ann Oncol (2017) 28(5):1137–44. doi: 10.1093/annonc/mdx040
2. Abdel-Rahman O, Fouad M. Correlation of Cetuximab-Induced Skin Rash and Outcomes of Solid Tumor Patients Treated With Cetuximab: A Systematic Review and Meta-Analysis. Crit Rev Oncol Hematol (2015) 93(2):127–35. doi: 10.1016/j.critrevonc.2014.07.005
3. Sonnenblick A, de Azambuja E, Agbor-Tarh D, Bradbury I, Campbell C, Huang Y, et al. Lapatinib-Related Rash and Breast Cancer Outcome in the ALTTO Phase III Randomized Trial. J Natl Cancer Inst (2016) 108(8):djw037. doi: 10.1093/jnci/djw037
4. Gershenwald JE, Scolyer RA, Hess KR, Sondak VK, Long GV, Ross MI, et al. For Members of the American Joint Committee on Cancer Melanoma Expert Panel and the International Melanoma Database and Discovery Platform. Melanoma Staging: Evidence-based Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA Cancer J Clin (2017) 67(6):472–92. doi: 10.3322/caac.21409
5. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. New Guidelines to Evaluate the Response to Treatment in Solid Tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst (2000) 92(3):205–16. doi: 10.1093/jnci/92.3.205
6. National Cancer Institute Enterprise Vocabulary Services. Criteria for Adverse Events (Ctcae) . Available at: https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf (Accessed May 14, 2020).
7. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J, et al. Brim-3 Study Group. Improved Survival With Vemurafenib in Melanoma With BRAF V600E Mutation. N Engl J Med (2011) 364(26):2507–16. doi: 10.1056/NEJMoa1103782
8. Ascierto PA, McArthur GA, Dréno B, Atkinson V, Liszkay G, Di Giacomo AM, et al. Cobimetinib Combined With Vemurafenib in Advanced BRAF(V600)-mutant Melanoma (coBRIM): Updated Efficacy Results From a Randomised, Double-Blind, Phase 3 Trial. Lancet Oncol (2016) 17(9):1248–60. doi: 10.1016/S1470-2045(16)30122-X
9. Petrelli F, Ardito R, Merelli B, Lonati V, Cabiddu M, Seghezzi S, et al. Prognostic and Predictive Role of Elevated Lactate Dehydrogenase in Patients With Melanoma Treated With Immunotherapy and BRAF Inhibitors: A Systematic Review and Meta-Analysis. Melanoma Res (2019) 29(1):1–12. doi: 10.1097/CMR.0000000000000520
10. Hodi FS, Chiarion-Sileni V, Gonzalez R, Grob JJ, Rutkowski P, Cowey CL, et al. Nivolumab Plus Ipilimumab or Nivolumab Alone Versus Ipilimumab Alone in Advanced Melanoma (CheckMate 067): 4-Year Outcomes of a Multicentre, Randomised, Phase 3 Trial. Lancet Oncol (2018) 19(11):1480–92. doi: 10.1016/S1470-2045(18)30700-9
11. Consoli F, Manganoni AM, Grisanti S, Petrelli F, Venturini M, Rangoni G, et al. Panniculitis and Vitiligo Occurring During BRAF and MEK Inhibitors Combination in Advanced Melanoma Patients: Potential Predictive Role of Treatment Efficacy. PloS One (2019) 14(4):e0214884. doi: 10.1371/journal.pone.0214884
12. Ben-Betzalel G, Baruch EN, Boursi B, Steinberg-Silman Y, Asher N, Shapira-Frommer R, et al. Possible Immune Adverse Events as Predictors of Durable Response to BRAF Inhibitors in Patients With BRAF V600-Mutant Metastatic Melanoma. Eur J Cancer (2018) 101:229–35. doi: 10.1016/j.ejca.2018.06.030
13. Heinzerling L, Eigentler TK, Fluck M, Hassel JC, Heller-Schenck D, Leipe J, et al. Tolerability of BRAF/MEK Inhibitor Combinations: Adverse Event Evaluation and Management. ESMO Open (2019) 4(3):e000491. doi: 10.1136/esmoopen-2019-000491
14. Hopkins AM, Rathod AD, Rowland A, Kichenadasse G, Sorich MJ. Risk Factors for Severe Rash With Use of Vemurafenib Alone or in Combination With Cobimetinib for Advanced Melanoma: Pooled Analysis of Clinical Trials. BMC Cancer (2020) 20:157. doi: 10.1186/s12885-020-6659-0
15. Lulli D, Carbone ML, Pastore S. The MEK Inhibitors Trametinib and Cobimetinib Induce a Type I Interferon Response in Human Keratinocytes. Int J Mol Sci (2017) 18(10):2227. doi: 10.3390/ijms18102227
16. Naqash AR, File DM, Ziemer CM, Whang YE, Landman P, Googe PB, et al. Cutaneous Adverse Reactions in B-RAF Positive Metastatic Melanoma Following Sequential Treatment With B-RAF/MEK Inhibitors and Immune Checkpoint Blockade or Vice Versa. A Single-Institutional Case-Series. J Immunother Cancer (2019) 7(1):4. doi: 10.1186/s40425-018-0475-y
17. Kuske M, Westphal D, Wehner R, Schmitz M, Beissert S, Praetorius C, et al. Immunomodulatory Effects of BRAF and MEK Inhibitors: Implications for Melanoma Therapy. Pharmacol Res (2018) 136:151–9. doi: 10.1016/j.phrs.2018.08.019
18. Hopkins AM, Van Dyk M, Rowland A, Sorich MJ. Effect of Early Adverse Events on Response and Survival Outcomes of Advanced Melanoma Patients Treated With Vemurafenib or Vemurafenib Plus Cobimetinib: A Pooled Analysis of Clinical Trial Data. Pigment Cell Melanoma Res (2019) 32(4):576–83. doi: 10.1111/pcmr.12773
19. Lewis K, Hauschild A, Larkin J, Ribas A, Flaherty KT, McArthur GA, et al. Effect of Concomitant Dosing With Acid-Reducing Agents and Vemurafenib Dose on Survival in Patients With BRAFV600 Mutation-Positive Metastatic Melanoma Treated With Vemurafenib ± Cobimetinib. Eur J Cancer (2019) 116:45–55. doi: 10.1016/j.ejca.2019.05.002
Keywords: melanoma, vemurafenib, cobimetinib, BRAF/MEK inhibition, skin toxicity, therapy outcome
Citation: Kähler KC, Gutzmer R, Meier F, Zimmer L, Heppt M, Gesierich A, Thoms K-M, Utikal J, Hassel JC, Loquai C, Pföhler C, Heinzerling L, Kaatz M, Göppner D, Pflugfelder A, Bohne A-S, Satzger I, Reinhardt L, Placke J-M, Schadendorf D and Ugurel S (2021) Early Exanthema Upon Vemurafenib Plus Cobimetinib Is Associated With a Favorable Treatment Outcome in Metastatic Melanoma: A Retrospective Multicenter DeCOG Study. Front. Oncol. 11:672172. doi: 10.3389/fonc.2021.672172
Received: 25 February 2021; Accepted: 26 April 2021;
Published: 24 May 2021.
Edited by:
Colette Pameijer, Pennsylvania State University, United StatesReviewed by:
Gagan Chhabra, University of Wisconsin-Madison, United StatesCopyright © 2021 Kähler, Gutzmer, Meier, Zimmer, Heppt, Gesierich, Thoms, Utikal, Hassel, Loquai, Pföhler, Heinzerling, Kaatz, Göppner, Pflugfelder, Bohne, Satzger, Reinhardt, Placke, Schadendorf and Ugurel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katharina C. Kähler, a2thZWhsZXJAZGVybWF0b2xvZ3kudW5pLWtpZWwuZGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.