
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 29 March 2021
Sec. Gastrointestinal Cancers
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.632962
This article is part of the Research TopicThe Evolving Landscape, Clinical Implications and Future Perspective of Biomarkers in Gastrointestinal CancersView all 19 articles
 Alessandro Ottaiano1*†
Alessandro Ottaiano1*† Guglielmo Nasti1†
Guglielmo Nasti1† Mariachiara Santorsola1
Mariachiara Santorsola1 Vincenzo Altieri2Giuseppina Di Fruscio2Luisa Circelli3
Vincenzo Altieri2Giuseppina Di Fruscio2Luisa Circelli3 Amalia Luce4,5
Amalia Luce4,5 Alessia Maria Cossu4,5Giosuè Scognamiglio1
Alessia Maria Cossu4,5Giosuè Scognamiglio1 Francesco Perri1Marco Correra1
Francesco Perri1Marco Correra1 Andrea Belli1Paolo Delrio1
Andrea Belli1Paolo Delrio1 Gerardo Botti1‡
Gerardo Botti1‡ Michele Caraglia4,5‡
Michele Caraglia4,5‡Background: We previously reported that loss of KRAS mutations (“regressive” mutational trajectories) from primary tumors to metastases associated with the oligo-metastatic status in colorectal cancer (CRC). The present study was undertaken in order to analyze the mutational trajectories of KRAS in a well-characterized cohort of CRC patients who developed poly- or oligo-metastatic disease.
Material and Methods: Patients were treated and followed-up according to European Society of Medical Oncology guidelines. Primary CRC FFPE tissue and metastatic circulating-free DNA were extracted using the QIAamp DNA specific kits (Qiagen, Hilden, Germany). Samples were sequenced with the Oncomine Solid Tumour DNA kit (Thermo Fisher Scientific, Waltham, MA, USA). Plasma collection for liquid biopsy was done from 1 to 14 days before starting first-line chemotherapy. Analysis of the prognostic power of KRAS evolutionary trajectories was done with uni- and multivariate analyses.
Results: One-hundred-fourteen patients were enrolled. Sixty-three patients presented with mutated KRAS (mutKRAS) and 51 with wild-type KRAS (wtKRAS). KRAS mutational concordance was high (70.1%).Two divergent subsets were identified: mutKRAS in primary tumors and wtKRAS in metastatic ones (regressive: mutKRAS → wtKRAS in 8.8% of patients), and vice versa (progressive: wtKRAS → mutKRAS in 21.1% of patients). An association between KRAS regressive trajectory and the oligo-metastatic status (P <0.0001) was found. At multivariate analysis, regressive and progressive mutational trajectories emerged as independent prognostic factors for survival, with Hazard Ratios of 0.22 (CI 95%: 0.08–0.61; median survival: not reached) and 2.70 (CI 95%: 1.11–6.56, median survival: 12.1 months), respectively.
Conclusions: Our data provide evidence that the evolutionary trajectories of KRAS can have a strong clinical prognostic role and that they can be involved in discriminating between poly-metastatic aggressive vs oligo-metastatic indolent CRC.
Colorectal cancer (CRC) is the third cause of cancer-related death worldwide (1). About 30% of patients present at diagnosis with metastatic disease, and half of them will develop metastases after surgical resection of the primary tumor (2). The survival of metastatic colorectal cancer (mCRC) patients significantly improved in the last 20 years with the introduction of target-oriented drugs [anti-EGFR (Epidermal Growth Factor Receptor) and anti-angiogenic agents] associated with chemotherapy (fluoropirimidines, oxaliplatin and irinotecan); however, it still very rarely encompasses 30 months (3). The selection of patients on a genetic basis allowed the selection of those more prone to respond to specific treatments. In fact, it is now clear that mCRC patients bearing specific KRAS (Kirsten RAt Sarcoma viral oncogene homolog) mutations do not benefit from anti-EGFR treatment because mutated and constitutively hyper-activated KRAS determine a ligand-independent activation of EGFR (4). We previously reported that loss of KRAS mutations (“regressive” mutational trajectories) from primary tumors to metastases on FFPE (Formalin-Fixed Paraffin Embedded) resected tissues was associated with long-term survivals and the oligo-metastatic status in mCRC (5, 6). However, the evaluation of circulating tumor DNA (ctDNA) sequences, also called “liquid biopsy”, has provided a great opportunity to study the mutational evolution of cancers with a non-invasive, real-time and repeatable approach. On these bases, Misale et al. (7) demonstrated that the occurrence of KRAS point mutations preceded the resistance to anti-EGFR monoclonal antibodies in mCRC patients who experienced an initial response. Furthermore, Siravegna et al. (8) showed that in mCRC patients, during anti-EGFR treatment withdrawals, KRAS mutated mCRC cells regain drug-sensitivity due to decay in frequency of KRAS mutations which, in some cases, become undetectable. Altogether, these data indicate that mCRC genetics is dynamic and that the evaluation of the tumor mutational status in a single moment could not be representative of the cancer mutational evolution.
The present study was undertaken in order to analyze the mutational trajectories of KRAS in a well-characterized cohort of mCRC patients and to correlate those trajectories with the prognosis and the extent of the disease (oligo- versus poly-metastatic status).
This was a retrospective, non-interventional and biomarkers study officially approved by the Scientific Directorate on November 11, 2020. The source of data was the electronic database reporting clinical records of CRC patients who underwent to radical excision of primary tumor from 2015 to 2018 and characterization of KRAS mutational status. Thereafter, they developed metastatic and unresectable disease and were enrolled into the study upon signature of an informed consent to perform a liquid biopsy for KRAS reassessment just before starting the first-line chemotherapy. The treatments were administered at the SSD (Struttura Semplice Dipartimentale) Innovative Therapies for Abdominal Metastases of the Istituto Nazionale Tumori di Napoli, IRCCS “G. Pascale. Oligo-metastatic patients were intended as those having one to three lesions per organ with a maximum tumor diameter smaller than 70 mm and no lesions encompassing 25 mm diameter. To avoid clear negative prognostic influences, some clinical criteria for patients’ inclusion were established a priori and consisted on: Performance Status ECOG (Eastern Cooperative Oncology Group) 0 or 1, age <80 years and life expectancy of at least three months. According to these criteria, 114 patients were selected: 63 had KRAS mutations (mutated KRAS: mutKRAS), 51 were KRAS wild-type (wtKRAS) (see DNA sequencing). Treatments were chosen according to ESMO (European Society of Medical Oncology) guidelines (9). All patients signed a written informed consent before treatment administration and molecular assessments. The primary outcome of this study was the analysis of the prognostic power of different KRAS evolutionary trajectories between the mutational status in primary tumor and that in liquid biopsy at metastases occurrence in both wild-type (wtKRAS → wtKRAS and wtKRAS → mutKRAS) and mutated (mutKRAS → mutKRAS and mutKRAS → wtKRAS) CRCs. Patients harboring double mutations of KRAS or NRAS or BRAF (v-raf murine sarcoma viral oncogene homolog B) mutations were not included in this study.
Total body Computed Tomography (tbCT) scan and CEA (CarcinoEmbryonic Antigen) monitoring were not centralized and were done every three months. The response to chemotherapy was evaluated by RECIST (Response Evaluation Criteria In Solid Tumours v1.1) (10). Complete response (CR) was defined as complete disappearance of all detectable evidence of disease on tbCT. Partial response (PR) was defined as at least a 30% decrease in the sum of diameters of target lesions. Stable disease (SD) was defined as everything between 30% decrease and 20% growth of tumour size. Progressive disease (PD) was defined as at least a 20% increase in the sum of diameters of target lesions. Disease Control (DC) was the sum of CR + PR + SD.
Six mL of whole blood was collected through sting of a peripheral vein, using Vacutainer® with EDTA as anticoagulant (K2EDTA, purple cap, Becton Dickinson). Plasma was separated by two sequential centrifugation steps (the first at room temperature for 10 min at 1,500×g and the second at 2,000×g for the same time and temperature). Plasma was stored at −80°C until analysis (see beyond).
Circulating-free (cf)-DNA was extracted from 1-ml samples of plasma with a commercial kit (QIAamp Circulating Nucleic Acid Kit; QIAGEN GmbH, Hilden, Germany) according to the manufacturer instructions. Cf-DNA samples were then stored at −20°C. FFPE tissue DNA was extracted from three 10 µm FFPE sections using the QIAamp DNA FFPE Tissue kit (Qiagen, Hilden, Germany) and the QIAcube apparatus (Qiagen). The DNA quantity was evaluated with the dsDNA HS assay kit using the Qubit 2.0 Fluorometer (Invitrogen, Monza, Italy).
Tumour samples were sequenced with the Oncomine Solid Tumour DNA kit (Thermo Fisher Scientific, Waltham, MA, USA) covering hotspot variants and actionable mutations of 22 genes involved in colon cancer. However, our analysis focused on KRAS-related genetic results. Ten nanograms of genomic DNA (gDNA) were used to prepare libraries according to the manufacturer’s instructions.
The amplified libraries were sequenced on the Ion Torrent PGM semiconductor (https://www.thermofisher.com/it/en/home/life-science/sequencing/next-generation-sequencing/ion-torrent-next-generation-sequencingworkflow.html) and the data were analyzed using the torrent suite software v5.0 (Thermo Fisher Scientific) and the obtained variants confirmed by the integrative genome viewer (IGV) from the Broad Institute. The limit of mutations detection (LOD) of tissue NGS approach is 2% allelic frequency. Reference sequence for KRAS was NM_004958.4. Mutations were also checked according to ClinVar identifier numbers (https://www.ncbi.nlm.nih.gov/clinvar/intro/).
Associations between KRAS mutations and clinical and pathologic variables were evaluated by χ2 test. P <0.05 was considered statistically significant. The primary outcome measure was the Overall Survival (OS), measured from the start of the first-line chemotherapy until death from any cause. The Kaplan–Meier product limit method was applied to graph OS. The study was exploratory considering the scarcity of data about the prognostic power of different mutational evolutions of KRAS oncogene in primary vs metastatic lesions and, thus, it does not have a pre-specified study design. All patients registered in an observational database (STORIA database) (11) between 2015 and 2018 and who accepted to perform liquid biopsy before starting first-line chemotherapy were enrolled. We chose do not prolong the enrolment period to avoid any prognostic interferences related to therapeutic and methodologic changes occurring in clinical practice. With an estimated survival difference between patients with KRAS mutational regression (defined as an expected rare group, mutKRAS → wtKRAS) vs patients with stably mutated KRAS (mutKRAS → mutKRAS) higher than 50% at 12 months, an estimated ratio mutKRAS → wtKRAS:mutKRAS → mutKRAS of about 1:10, a sample size of at least 60 patients was required to generate a significant hypothesis (P <0.005) on survival time differences at Log-Rank Test.
Univariate analysis was performed with the Log-Rank test. Multivariate analysis was performed through the Cox proportional-hazards regression in order to analyze the effect of several risk factors (co-variates) on OS. The HR is the estimate of the end-point probability and it can be interpreted as the instantaneous relative risk of an event (death), at any time, for an individual with the risk factor present compared with an individual with the risk factor absent, given both individuals are the same on all other covariates. Covariates were selected after consensus discussion between authors and were dichotomized: age <65 vs age ≥65, male vs female, left sided vs right sided, one involved organ vs two or more, response to first-line chemotherapy (Disease Control vs No Disease Control), KRAS mutational evolution in mutated KRAS (mutKRAS → mutKRAS vs mutKRAS → wtKRAS) and in wild-type KRAS (wtKRAS → wtKRAS vs wtKRAS → mutKRAS). 95% confidence intervals (CI) of HR are also reported. Statistical analysis was performed using the MedCalc® 9.3.7.0 and Excel software.
One-hundred-fourteen patients who received surgical removal and KRAS oncogene evaluation of a primary CRC between 2015 and 2018 accepted to reassess KRAS mutational status through liquid biopsy before starting the first-line chemotherapy for the occurrence of distant and non-resectable metastases. However, first-line and subsequent chemotherapies were established according to the KRAS assessed on the primary FFPE tumoral tissue as established by National Regulatory Authorities (a detailed description is reported in Table S1). Table 1 shows the clinic-pathologic characteristics of patients according to the KRAS mutational status in primary tumors. Overall, 63 patients presented with mutKRAS and 51 with wtKRAS. The three most frequent mutations were p.G12D (19 patients), p.G13D (nine patients) and p.G12V (seven patients). There were no statistically significant associations at χ2 test between the mutational status of KRAS on primary tumors and age (<65 vs ≥65 years), gender (male vs female), grading (G1/G2 vs G3), side of primary tumor (left vs right), pT (pT1/pT2 vs pT3 vs pT4), and lymphnodes involvement (pN: 0 vs 1–3 vs >3). According to Oncology Societies’ guidelines and National Pharmaceutical Authorities’ regulations, patients bearing mutKRAS in primary tumors did not receive anti-EGFR-based treatments (Table 2). In this patients’ setting, the use of chemotherapy (CT) and bevacizumab was predominant (56/63 patients, 88.8%); conversely, in wtKRAS patients the 76.4% of them was treated with CT plus an anti-EGFR agent (39/51 patients). Interestingly, wtKRAS patients received more CT lines (43.3% vs 20.6% in mutKRAS patients) and had a longer cumulative median time-on-therapy (20.5 vs 16.9 months in mutKRAS patients). This was indirectly related to the detrimental prognostic effect on survival of mutKRAS (11).
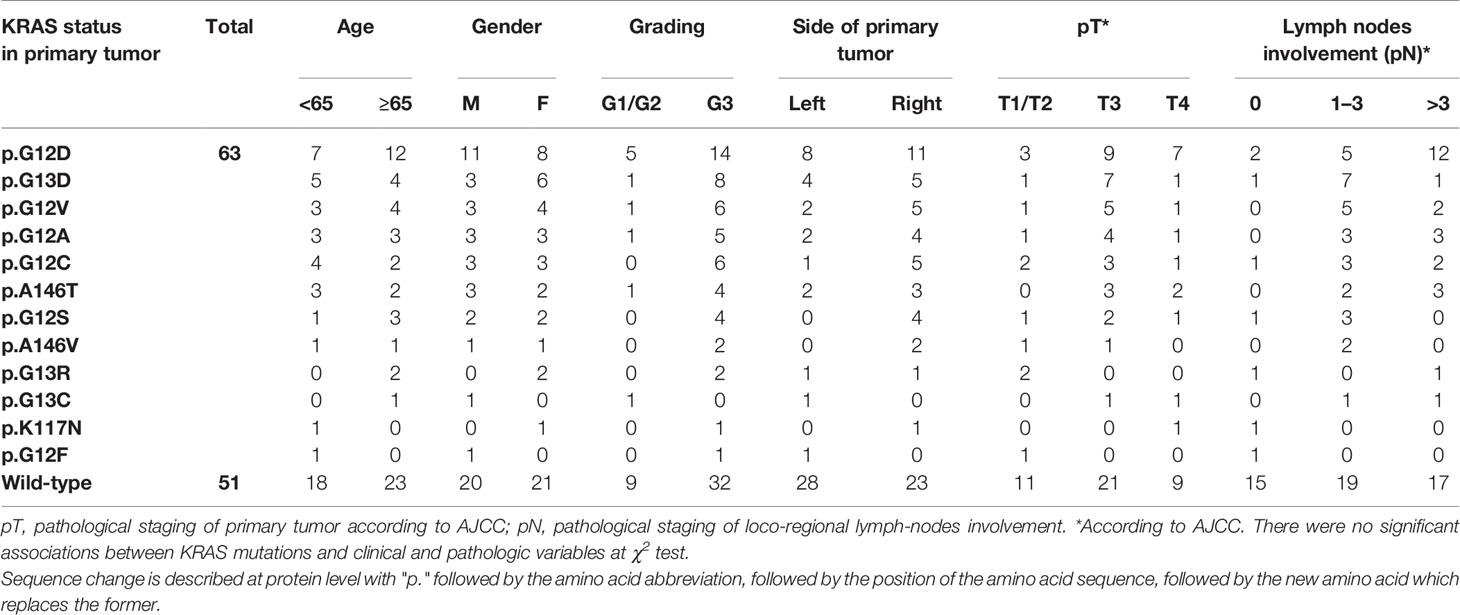
Table 1 Clinico-pathological characteristics according to KRAS status at diagnosis.
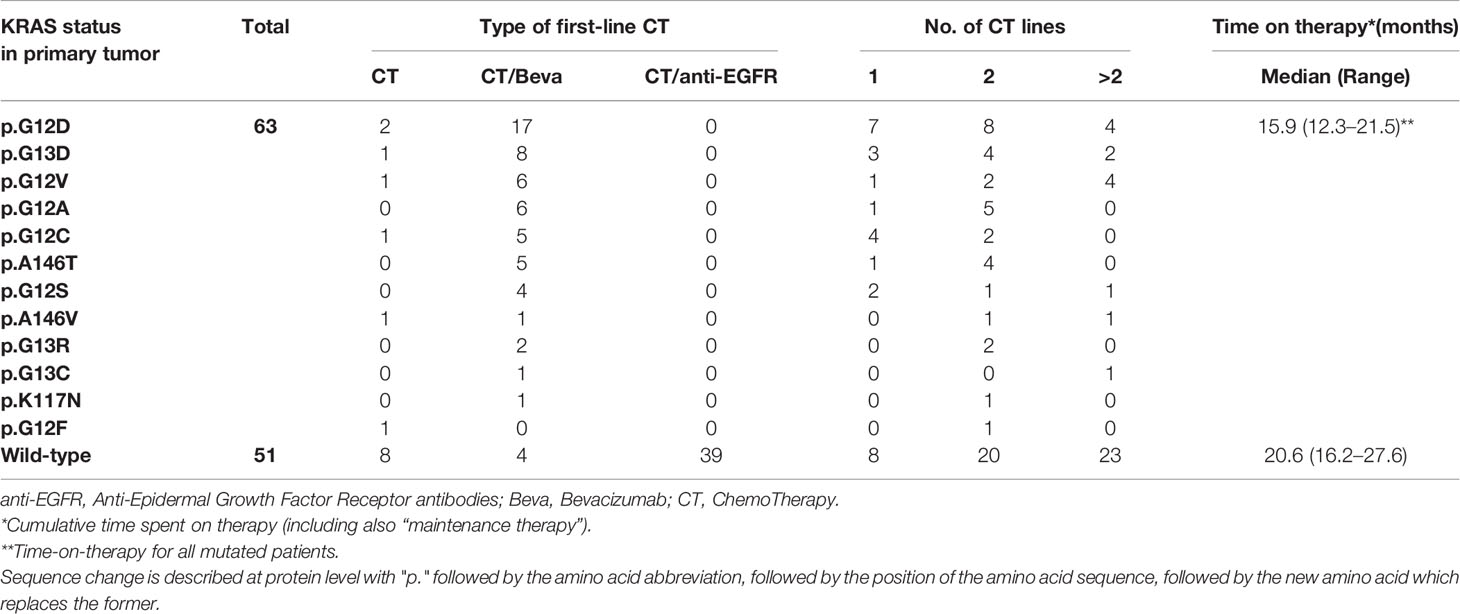
Table 2 Treatment characteristics according to KRAS status at diagnosis.
KRAS mutational concordance (mutKRAS or wtKRAS in both primary and liquid biopsy at metastases occurrence: mutKRAS → mutKRAS and wtKRAS → wtKRAS) was high (70.1%). However, two divergent subsets were identified: 1. mutKRAS in primary tumors and wtKRAS in metastatic ones (mutKRAS → wtKRAS in 8.8% of patients), and vice versa (wtKRAS → mutKRAS in 21.1% of patients) (Table 3). These subsets are particularly interesting because they represent a dynamic aspect of cancer heterogeneity. Table 3 shows some clinical characteristics that could have influenced the genetic evolution of KRAS. There were statistically significant associations: 1. adjuvant chemotherapy based on capecitabine and oxaliplatin more frequently preceded the evolution towards mutKRAS from wtKRAS (wtKRAS → mutKRAS) (P = 0.001), 2. There was a strong association between KRAS regressive trajectory (mutKRAS → wtKRAS) and the oligometastatic status (P <0.0001) (see Material and Methods for the definition of oligo-metastatic disease), 3. Regression of mutKRAS (mutKRAS → wtKRAS) before starting first-line chemotherapy was associated with response to CT alone or CT plus bevacizumab (P = 0.026) (Table 3).
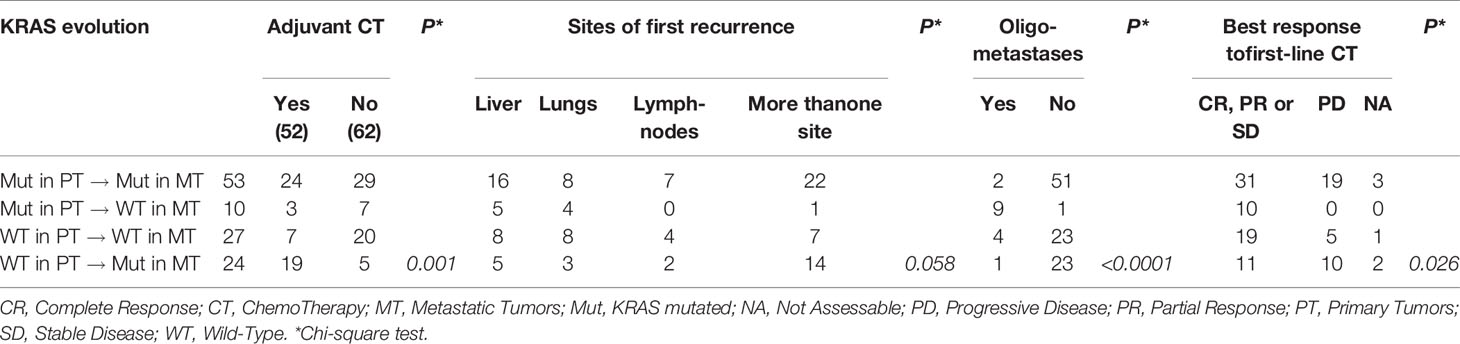
Table 3 Tumor burden, adjuvant chemotherapy and response to first-line CT according to KRAS evolution.
Given the opportunity to distinguish four KRAS evolutionary subsets, we studied the prognostic impact of these subsets on survival, the most reliable and synthetic outcome. Time-to-progression was not evaluated considering the potential prognostic biases related to different first-line chemotherapies and/or different therapeutic sequences. Table 4 and Figure 1 show respectively, univariate analysis of overall survival (OS) and Kaplan Meyer curves depicting the survival of patients according to different evolutionary subsets. After a median follow-up for the whole series of 25.0 months, median OS (mOS) of KRAS genetically concordant patients was 9.6 for mutKRAS → mut KRAS and 27.5 months for wtKRAS → wtKRAS. Median OS (mOS) for mutKRAS → wtKRAS (“regressive trajectory”) was not reached (NR), while median mOS in patients developing KRAS mutations in metastatic tumors from wtKRAS in primary lesions (wtKRAS → mutKRAS) was 12.1 months (P = 0.0001 at Long Rank test).
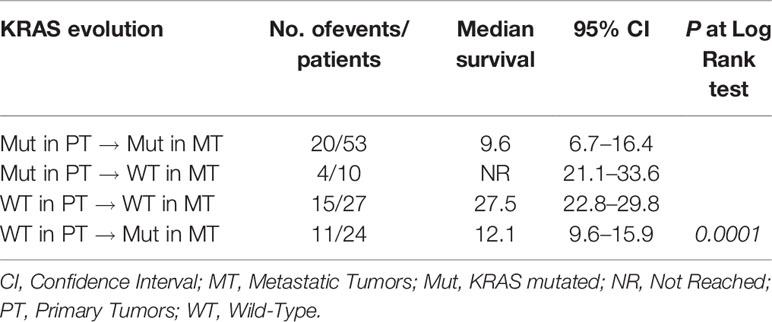
Table 4 Univariate analysis of KRAS mutations’ evolution prognostic power.
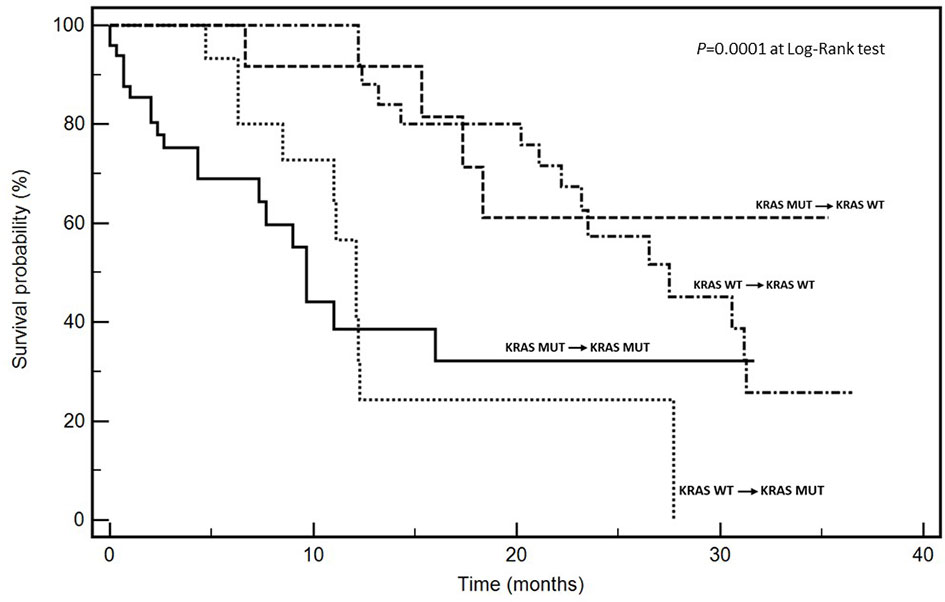
Figure 1 Kaplan-Meier survival curves according to KRAS mutational trajectories.
A multivariate analysis was performed including as dichotomized co-variates, age (<65 vs ≥65 years), gender (male vs female), side (left vs right), extent of metastatic involvement (one vs multiple sites), response to first-line CT [CR/PR/SD (DC, Disease Control) vs PD (no DC)], genetic concordance in mutKRAS vs regressive trajectory (mutKRAS → wtKRAS), and genetic concordance in wtKRAS vs progressive trajectory (wtKRAS → mutKRAS). Interestingly, the following conclusions from the statistical analysis can be derived: i. metastatic involvement (one vs multiple sites; mOS: 30.6 vs 11.0 months; HR: 4.16, CI 1.25–13.7), ii. response to first-line CT (DC vs no DC; mOS: 28.3 vs 9.6.0 months; HR: 2.11, CI 1.78–4.26), and KRAS evolutionary iii. regressive (mutKRAS → mutKRAS vs mutKRAS → wtKRAS; mOS: 9.6 months vs NR; HR: 0.22, CI 0.08–0.61) and iv. progressive trajectories (wtKRAS → wtKRAS vs wtKRAS → mutKRAS; mOS: 27.5 vs 12.1 months; HR: 2.70, CI 1.11–6.56) emerged as independent prognostic factors for OS (Table 5).
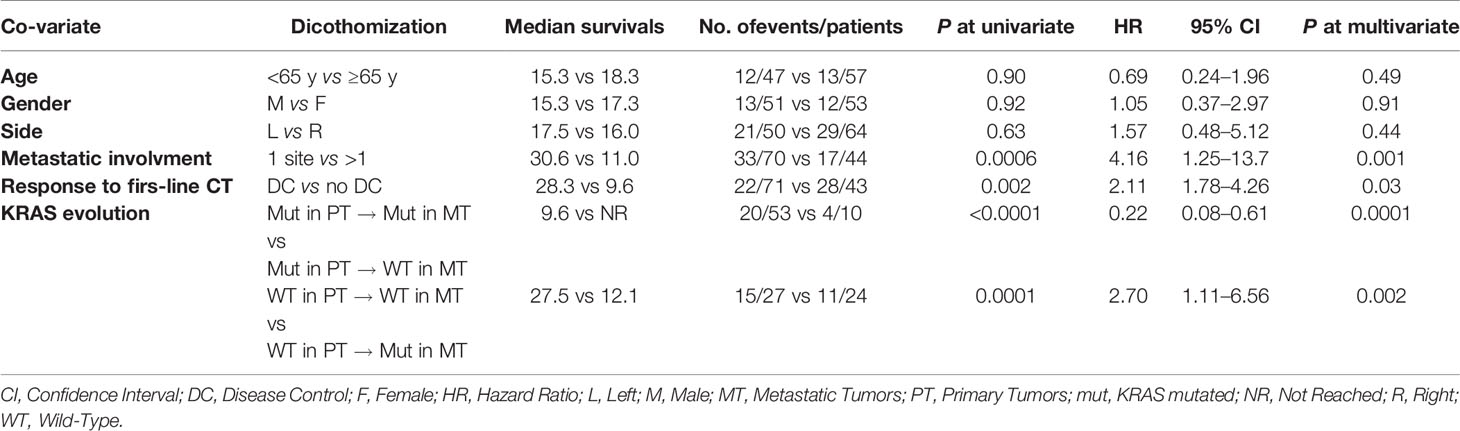
Table 5 Multivariate analysis of RAS mutations’ evolution prognostic power.
In this work, we found that the genetic dynamics of mCRC is clinically relevant since patients bearing divergent mutational evolution have a prognosis consistent with the results of liquid biopsy: in fact, patients bearing mutKRAS at liquid biopsy from a wtKRAS in primary tumor have both poorer survival and responsiveness to chemotherapy similar to KRAS mutated CRCs. This subset could represent a particularly aggressive phenotype on an evolutionary point of view (“progressive” genetic trajectory). By contrast, in 8.8% of cases we observed a “regressive” mutational trajectory that was associated to the best prognosis and high responsiveness to chemotherapy independently from the lack of anti-EGFR treatment administration. The last data are particularly surprising and could indicate that additional unexplored anti-tumoral mechanisms could work to downsize the neoplastic population. Multivariate analysis showed that both mutational trajectories had an independent and significant prognostic power. As in our previous studies (5, 6), we cannot definitively demonstrate if this effect depends on a negative immunologic selection (12) or on a spontaneous genetic devolution. Our translational studies are in progress to identify and isolate, from oligo-metastatic CRC patients, eventual T-cells responsible of mutKRAS clones’ elimination.
Surprisingly, we found that “progressive” genetic trajectories (wtKRAS → mutKRAS) were much more frequent in patients treated with adjuvant chemotherapy (Table 3). These findings were consistent with two previous studies performed in well-defined models of oligo-metastatic CRC (5, 6). We hypothesized that chemotherapy would induce a genetic remodelling. The existence of this selection mechanisms was supported by our findings on much more divergent mutational signatures and events between primary and matched metastases when the resection of metachronous metastases was preceded by adjuvant chemotherapy (mutational sharing: >90% in non-chemotherapy-pre-treated lesions vs <15% in chemotherapy-pre-treated lesions). In other words, RAS wild-type CRC patients progressing after oxaliplatin/capecitabine-based adjuvant chemotherapy developed more RAS mutations and resistance to anti-EGFR treatments than metastatic patients who did not receive adjuvant treatment. Therefore, chemotherapy could induce both genetic remodelling and evolutionary pushing. The neoplastic progeny of chemotherapy pre-treated CRC patients could have much more extensive intra-tumour mutation heterogeneity including some clones evolved towards mutKRAS. In our opinion, a similar effectwas observed in a very recent study by Wu et al. (13) reporting a trial on the use of osimertinib in completely resected EGFR mutated non-small cell lung cancers (NSCLC). Osimertinib adjuvant administration was less effective on disease-free survival when preceded by chemotherapy. Importantly, we are describing our scientific observations and not deploring adjuvant chemotherapy that is a standard of care in high-risk resected CRC and NSCLC. A useful suggestion rising from our work would be to reassess the mutational status of KRAS, particularly in patients underwent to adjuvant chemotherapies, in order to predict the major risk to develop a chemotherapy-induced genetic remodelling requiring both more aggressive treatment strategies and more careful follow-up.
Some limitations of the present study deserve to be discussed. The sample size is limited to 114 patients. In fact, about half of patients did not accept to reassess KRAS with liquid biopsy in order to modulate the planningof the therapeutic approach that remained based on the first FFPE tissue RAS evaluation. Furthermore, only 10 patients showed a regressive trajectory of KRAS (mutKRAS → wtKRAS) and this was related to the lower incidence of this effect if compared to the progressive trajectory (wtKRAS → mutKRAS) which represents an advantageous gain for cancer cells. First-line treatments were physiologically heterogeneous according to clinical and genetic assessments; however, the mono-institutional and exploratory nature of this study, along with the uniformity of technical approaches, makes our results precious and informative. Moreover, we did not evaluate KRAS status at different time-points because of budget limitations. This is a limit and a missed opportunity to observe the complete KRAS cancer cells “plasticity” during the time. Finally, we did not investigate if wtKRAS patients on liquid biopsy were again responsive to anti-EGFR treatments. The latter is a crucial question, which deserves to be explored in large prospective trials. At this stage, we can observe that our patients bearing a regressive trajectory (mutKRAS → wtKRAS) were responsive to treatments and had a good OS regardless of whether they did not receive anti-EGFR agents in first or second lines of treatments.
This work may have a strong practice-changing power in our context since results of liquid biopsy are considered not standard and the National Sanitary System does not reimburse the relative costs. Our results strongly suggest that a single KRAS mutational status determination at the diagnosis is nor correct neither useful because cancer clonal heterogeneity can determine a change of the mutational status over the space (in different sites of disease localization) and time, as already suggested by other researchers (4, 7, 8). In our opinion, our work could contribute to provide a biological basis to approach KRAS testing with a more dynamic attitude (liquid biopsy) giving both new prognostic and therapeutic chances. The identification of regressive genetic trajectories (mutKRAS → wtKRAS) in specific mCRC patients could open unexpected therapeutic scenarios. In fact, in this subset, treatment with anti-EGFR-based drugs (cetuximab or panitumumab) could regain relevance and it deserves to be further explored in clinical trials. Furthermore, our data provides an additional direct evidence that studies of the evolutionary trajectories of KRAS can have a strong clinical and prognostic impact also in discriminating between poly-metastatic aggressive vs oligo-metastatic indolent CRC subsets.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Conceptualization, AO, GN, and MS. Methodology, VA, GD, and LC. Software, FP and AB. Validation, GB, GN, and GS. Formal analysis, AO, MaC, and PD. Investigation, AO, GN, AL, and MiC. Resources, GN. Data curation, AO and MiC. Writing/original draft preparation, AO, MS, and MiC. Writing/review and editing, GN, GB, and GS. Supervision, MiC. All authors contributed to the article and approved the submitted version.
This work was funded by Mrs. Antonietta Nacca.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge the LILT (Lega Italiana per la Lotta contro i Tumori—sezione di Napoli) for the precious collaboration.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.632962/full#supplementary-material
1. Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin DM, Piñeros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer (2019) 144:1941–53. doi: 10.1002/ijc.31937
2. Hadden WJ, de Reuver PR, Brown K, Mittal A, Samra JS, Hugh TJ. Resection of colorectal liver metastases and extra-hepatic disease: a systematic review and proportional meta-analysis of survival outcomes. HPB (Oxford) (2016) 18:209–20. doi: 10.1016/j.hpb.2015.12.004
3. Nappi A, Berretta M, Romano C, Tafuto S, Cassata A, Casaretti R, et al. Metastatic Colorectal Cancer: Role of Target Therapies and Future Perspectives. Curr Cancer Drug Targets (2018) 18:421–9. doi: 10.2174/1568009617666170209095143
4. Serna-Blasco R, Sanz-Álvarez M, Aguilera Ó, García-Foncillas J. Targeting the RAS-dependent chemoresistance: The Warburg connection. Semin Cancer Biol (2019) 54:80–90. doi: 10.1016/j.semcancer.2018.01.016
5. Ottaiano A, Caraglia M, Di Mauro A, Botti G, Lombardi A, Galon J, et al. Evolution of Mutational Landscape and Tumor Immune-Microenvironment in Liver Oligo-Metastatic Colorectal Cancer. Cancers (Basel) (2020) 12:3073. doi: 10.3390/cancers12103073
6. Ottaiano A, Circelli L, Lombardi A, Scala S, Martucci N, Galon J, et al. Genetic trajectory and immune microenvironment of lung-specific oligometastatic colorectal cancer. Cell Death Dis (2020) 11:275. doi: 10.1038/s41419-020-2480-6
7. Misale S, Yaeger R, Hobor S, Scala E, Janakiraman M, Liska D, et al. Emergence of KRAS mutations and acquired resistance to anti-EGFR therapy in colorectal cancer. Nature (2012) 486:532–6. doi: 10.1038/nature11156
8. Siravegna G, Mussolin B, Buscarino M, Corti G, Cassingena A, Crisafulli G, et al. Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat Med (2015) 21:795–801. doi: 10.1038/nm.3870
9. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol (2016) 27:1386–422. doi: 10.1093/annonc/mdw235
10. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
11. Ottaiano A, Normanno N, Facchini S, Cassata A, Nappi A, Romano C, et al. Study of Ras Mutations’ Prognostic Value in Metastatic Colorectal Cancer: STORIA Analysis. Cancers (Basel) (2020) 12:1919. doi: 10.3390/cancers12071919
12. Tran E, Robbins PF, Lu YC, Prickett TD, Gartner JJ, Jia L, et al. T-Cell Transfer Therapy Targeting Mutant KRAS in Cancer. N Engl J Med (2016) 375:2255–62. doi: 10.1056/NEJMoa1609279
Keywords: KRAS, metastatic colorectal cancer, DNA, liquid biopsy, prognosis
Citation: Ottaiano A, Nasti G, Santorsola M, Altieri V, Di Fruscio G, Circelli L, Luce A, Cossu AM, Scognamiglio G, Perri F, Correra M, Belli A, Delrio P, Botti G and Caraglia M (2021) KRAS Mutational Regression Is Associated With Oligo-Metastatic Status and Good Prognosis in Metastatic Colorectal Cancer. Front. Oncol. 11:632962. doi: 10.3389/fonc.2021.632962
Received: 24 November 2020; Accepted: 10 March 2021;
Published: 29 March 2021.
Edited by:
Jaw-Yuan Wang, Kaohsiung Medical University Hospital, TaiwanReviewed by:
Giovanni Li Volti, University of Catania, ItalyCopyright © 2021 Ottaiano, Nasti, Santorsola, Altieri, Di Fruscio, Circelli, Luce, Cossu, Scognamiglio, Perri, Correra, Belli, Delrio, Botti and Caraglia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alessandro Ottaiano, YS5vdHRhaWFub0Bpc3RpdHV0b3R1bW9yaS5uYS5pdA==
†These authors share first authorship
‡These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.