
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 25 February 2021
Sec. Radiation Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.625688
 Ling-Feng Liu1,2†
Ling-Feng Liu1,2† Qing-Song Li1,2†Yin-Xiang Hu1,2Wen-Gang Yang1,2Xia-Xia Chen1,2Zhu Ma1,2Wei-Wei OuYang1,2
Qing-Song Li1,2†Yin-Xiang Hu1,2Wen-Gang Yang1,2Xia-Xia Chen1,2Zhu Ma1,2Wei-Wei OuYang1,2 Yi-Chao Geng1,2Cheng Hu1,2
Yi-Chao Geng1,2Cheng Hu1,2 Sheng-Fa Su1,2*Bing Lu1,2*
Sheng-Fa Su1,2*Bing Lu1,2*Purpose: The role of radiotherapy, in addition to chemotherapy, has not been thoroughly determined in metastatic non-small cell lung cancer (NSCLC). The purpose of the study was to investigate the prognostic factors and to establish a model for the prediction of overall survival (OS) in metastatic NSCLC patients who received chemotherapy combined with the radiation therapy to the primary tumor.
Methods: The study retrospectively reviewed 243 patients with metastatic NSCLC in two prospective studies. A prognostic model was established based on the results of the Cox regression analysis.
Results: Multivariate analysis showed that being male, Karnofsky Performance Status score < 80, the number of chemotherapy cycles <4, hemoglobin level ≤120 g/L, the count of neutrophils greater than 5.8 ×109/L, and the count of platelets greater than 220 ×109/L independently predicted worse OS. According to the number of risk factors, patients were further divided into one of three risk groups: those having ≤ 2 risk factors were scored as the low-risk group, those having 3 risk factors were scored as the moderate-risk group, and those having ≥ 4 risk factors were scored as the high-risk group. In the low-risk group, 1-year OS is 67.7%, 2-year OS is 32.1%, and 3-year OS is 19.3%; in the moderate-risk group, 1-year OS is 59.6%, 2-year OS is 18.0%, and 3-year OS is 7.9%; the corresponding OS rates for the high-risk group were 26.2%, 7.9%, and 0% (P<0.001) respectively.
Conclusion: Metastatic NSCLC patients treated with chemotherapy in combination with thoracic radiation may be classified as low-risk, moderate-risk, or high-risk group using six independent prognostic factors. This prognostic model may help design the study and develop the plans of individualized treatment.
More than half of non-small cell lung cancer (NSCLC) patients have distant metastases at the time of initial diagnosis (1). Drug therapy is the main treatment for metastatic NSCLC. Molecular targeted therapy is recommended for metastatic NSCLC patients if sensitive gene aberrations are detected (2). Molecular targeted therapy has less toxicity and higher efficacy in comparison with conventional chemotherapy (3, 4). However, only approximately 30% of the patients may have positive responses from the molecular targeted therapy (5, 6), and therefore about 70% of patients require other systemic therapy (7, 8).
However, antibodies to the programmed death protein 1 (PD-1), such as the monotherapy drug pembrolizumab, can be utilized as a first-line treatment for the metastatic NSCLC patients, without sensitizing the anaplastic lymphoma kinase (ALK) or epidermal growth factor receptor (EGFR) changes with the programmed death ligand 1 (PD-L1) tumor proportion score (TPS) of 1% or higher (9). However, the cost of pembrolizumab is high, and many patients cannot afford pembrolizumab treatment. For NSCLC patients, pembrolizumab may not be considered cost-effective in treatment (10, 11). Thus, platinum-based doublet chemotherapy is the most extensively utilized modality in treating metastatic NSCLC patients without sensitive gene aberrations (8).
Platinum-based doublet chemotherapy generally produces about 30% response rates, with a median overall survival of 8 to 10 months, and similar efficacy with different chemotherapy regimens (12, 13). For patients with metastatic NSCLC, oncologists focused more on systemic therapy to control the metastatic lesions than local treatment to control the primary tumor. However, nearly 50% of patients with metastatic diseases have a local recurrence at the initial site of involvement, and local control and status of the primary tumor are associated with OS (14, 15). Our previous prospective studies and other retrospective studies showed that chemotherapy with concurrent thoracic radiation to the primary tumor produces favorable survival outcomes with acceptable toxicity (16–18). Yen et al. also demonstrated that the survival benefits of combining thoracic RT (45 Gy at least) and EGFR tyrosine kinase inhibitor (TKI) in metastatic NSCLC patients with sensitizing EGFR alterations (19). At present, increasing evidence shows that local treatment to all metastatic lesions can improve survival outcomes in patients with oligometastatic NSCLC (20–22). These publications suggested that some patients with metastatic diseases could benefit from the thoracic radiation to the primary tumor with system treatment (16–19). However, routine use of concurrent thoracic chemoradiation is not recommended for patients with metastatic NSCLC (23). A well-defined risk scoring system is essential to identify metastatic NSCLC patients who may benefit from chemotherapy with concurrent thoracic radiation to the primary tumor. The aim of this study is to determine the prognostic factors and to establish a model for the prediction of overall survival (OS) in metastatic NSCLC patients who received chemotherapy combined with radiation therapy to the primary tumor.
Clinical characteristics, such as gender, pathological type, weight loss, KPS, age, and metastatic status, are important prognostic factors of metastatic NSCLC. Furthermore, laboratory parameters, such as white blood cells, hemoglobin, platelets, fibrinogen, albumin, and lactate dehydrogenase, are also related to the prognosis of NSCLC (16, 24–28). These laboratory parameters are the routine testing items of metastatic NSCLC, which can be obtained conveniently and economically. Due to the uncertainties regarding concurrent thoracic radiotherapy in combination with chemotherapy, we hope to develop a prognostic model that is convenient for clinical application to estimate the overall survival outcome (23).
In our present study, we have developed a prognostic model on the basis of the parameters of pretreatment laboratory and clinical characteristics of metastatic NSCLC patients from two prospective studies (17, 18). Our purpose was to stratify patients into different risk groups and to identify a subgroup that may benefit from thoracic radiotherapy with concurrent chemotherapy.
We retrospectively analyzed 243 eligible patients with metastatic NSCLC who were treated with chemotherapy and concurrent radiation to the primary tumor in two prospective studies (17, 18). The selection criteria were as follows: (1) histologically or cytology confirmed NSCLC; (2) newly diagnosed metastatic disease limited to ≤3 organs; (3) did not receive targeted therapy or immunotherapy during lifetime; (4) aged 18–75 years; (5) a Karnofsky Performance Status (KPS) score ≥70; (6) received at least two chemotherapy cycles and a thoracic radiation dose of at least 40 Gy in 2-Gy fractions; (7) received three-dimensional conformal radiation therapy [3DCRT] or intensity modulated radiation therapy [IMRT]; (8) had complete clinicopathologic and follow-up information; (9) had pretreatment records of blood routine, blood biochemistry, and coagulation function test within 1 week before treatment. This study was reviewed by the ethical review boards in China (Ethics Committee of Guizhou Cancer Hospital, Guiyang, China), and informed consents were obtained from all patients.
Clinicopathologic information included sex, age, KPS score, tumor histology, N stage, T stage, metastatic status at diagnosis, size of primary tumor, tumor size, and survival outcomes (dead or alive). Laboratory testing parameters included white blood cell (WBC) count, hemoglobin (Hb) level, platelet (PLT) count, neutrophil absolute value, lymphocyte absolute value, Neutrophil-to-Lymphocyte Ratio (NLR), albumin, serum calcium level, lactate dehydrogenase (LDH), alkaline phosphatase (ALP) level, plasma D-dimer, and fibrinogen.
All patients received the following first-line therapy: docetaxel plus cisplatin given every 21–28 days concurrent with thoracic radiation therapy. No induction chemotherapy was given before radiation. After the completion of thoracic radiotherapy, patients who were in remission or had stable disease continued chemotherapy for a total of 4–6 cycles. No maintenance therapy was given. Modern techniques (3D-CRT or IMRT) were utilized to deliver at least 40 Gy thoracic radiation dose (2 Gy per fraction) to all enrolled cases. It is noted that radiotherapy and chemotherapy were given concurrently, and that radiotherapy commenced within one week after the administration of the first course of chemotherapy. Details of the radiation therapy protocol were reported previously (17, 18).
The overall survival (OS) time was measured from the starting date of treatment to the date of death or the last follow-up. The Statistical Package for Social Sciences, version 15.0 (SPSS, Chicago, IL, USA) was used for statistical analysis. Receiver operating characteristic (ROC) curves with binary variable of OS longer or shorter than 10.0 months and Youden’s index were used to determine the best cut-off value for baseline values of continuous variables, such as white blood cell count, platelet count, hemoglobin level, etc., as a prognostic factor. The Kaplan-Meier method was used to calculate the OS, and the curves were compared with log-rank test results. Multivariate Cox regression analysis was utilized to test independent significant prognostic factors for OS. All factors with P value ≤0.10 in univariate analysis were further tested in the multivariate analysis. We developed a prognostic model to predict the survival of NSCLC patients based on the results of the Cox regression analysis. Harrell’s test was used to validate the model. All statistical tests were 2-sided, and P values < 0.05 were considered statistically significant.
A total of 243 eligible patients were included in this study, including 154 male and 89 female patients, aged 26–75 (median: 58) years. The most common site of metastatic disease at diagnosis was the bone (51.4% of patients); 90 (37%) had brain metastases and 78 (32%) patients had lung metastases. One hundred and five (43.2%) patients had a single metastasis. The clinical characteristics of the 243 patients are listed in Table 1.
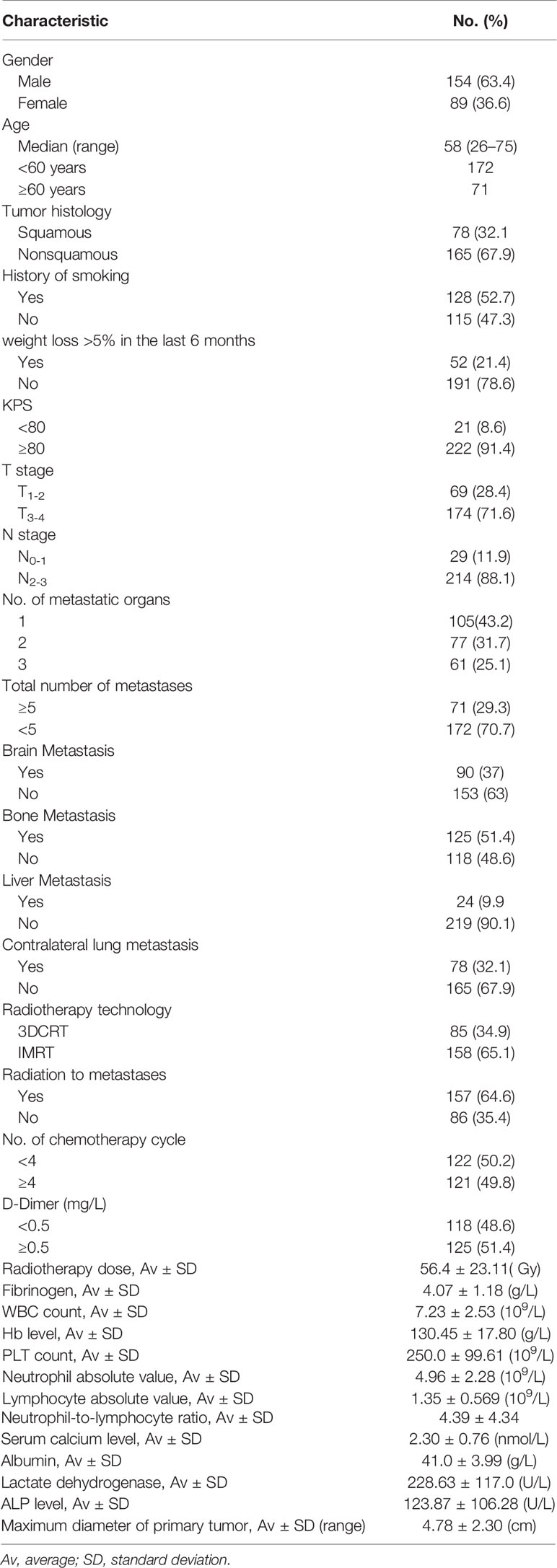
Table 1 Characteristics of 243 patients with metastatic NSCLC.
The follow-up periods ranged from 2.0 to 64.0 months, with a median follow-up period of 14.0 months. The median OS time for all patients was 13.0 months (95% confidence interval [CI]: 11.7–14.3), and the OS rates at 1, 2, and 3 years were 55.2%, 17.8%, and 11.0% respectively. Univariate analysis showed that sex, KPS score, T status, number of metastatic organs, brain metastasis, number of chemotherapy cycles, plasma D-dimer, fibrinogen level, WBC count, Hb level, PLT count, neutrophil count, NLR, serum albumin level, and ALP level were associated with OS significantly (Table 2). Multivariate analysis showed that being male, KPS score < 80, the number of chemotherapy cycles <4, Hb level ≤ 120g/L, neutrophil count >5.8 ×109/L, and PLT count >220 ×109/L had a negative effect on OS, as shown in Table 3.
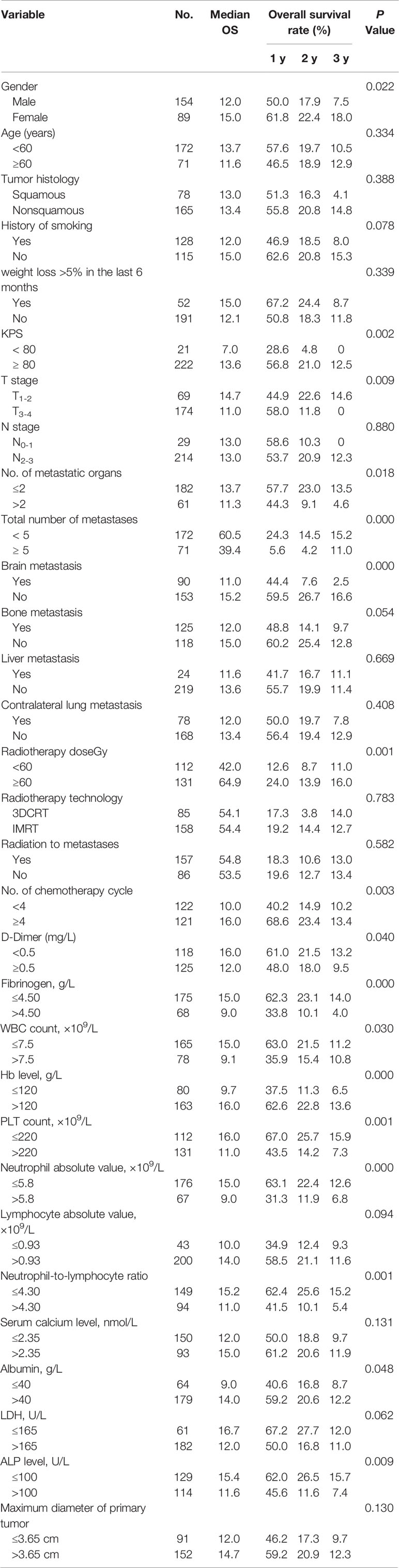
Table 2 Univariate analysis of factors potentially associated with overall survival outcomes.
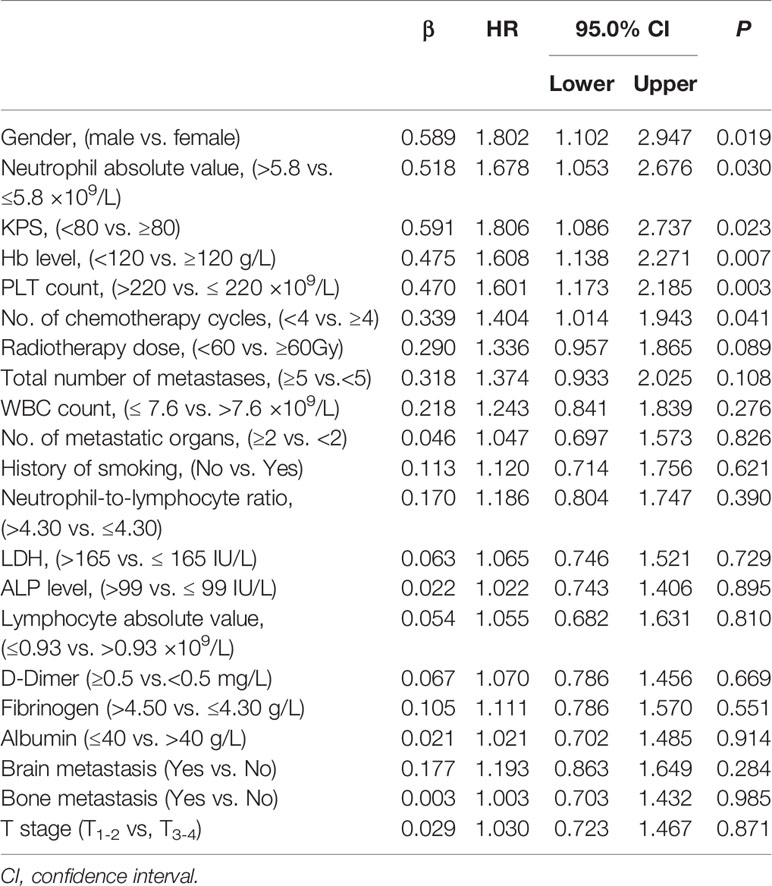
Table 3 Multivariate analysis of factors for the prediction of overall survival.
A prognostic model was established based on 6 independent risk factors (being male, KPS score < 80, a number of chemotherapy cycles < 4, Hb level ≤ 120g/L, neutrophil count >5.8 ×109/L, and PLT count >220 ×109/L). Risk groups were defined by the number of presenting risk factors (0, 1, 2, 3, 4, 5, or 6). These 6 parameters were scored as “0” if there were no risk factors and ‘‘+1’’ if there was an additional risk factor. Therefore, a total prognostic score for each patient was calculated ranging from 0 to 6. All patients had at least one of these six risk factors, 24 patients had only one risk factor (group 1), 69 patients had two risk factors (group 2), 89 patients had three risk factors (group 3), 49 patients had four risk factors (group 4), 12 patients had five risk factors (group 5), and no patient had all six risk factors. The median OS time for these five groups were 19.6 (95% CI: 12.2–27.0), 17.0 (95% CI: 12.8–21.2), 14.0 (95% CI: 11.7–16.3), 9.0 (95% CI: 7.2–10.8), and 8.0 (95% CI: 5.9–10.1) months respectively (P <0.001; Figure 1). Group comparison analysis revealed no significant differences in OS between group 1 and group 2 (P=0.124), and between group 4 and group 5 (P= 0.334). Significant differences were observed among other groups (P <0. 05).
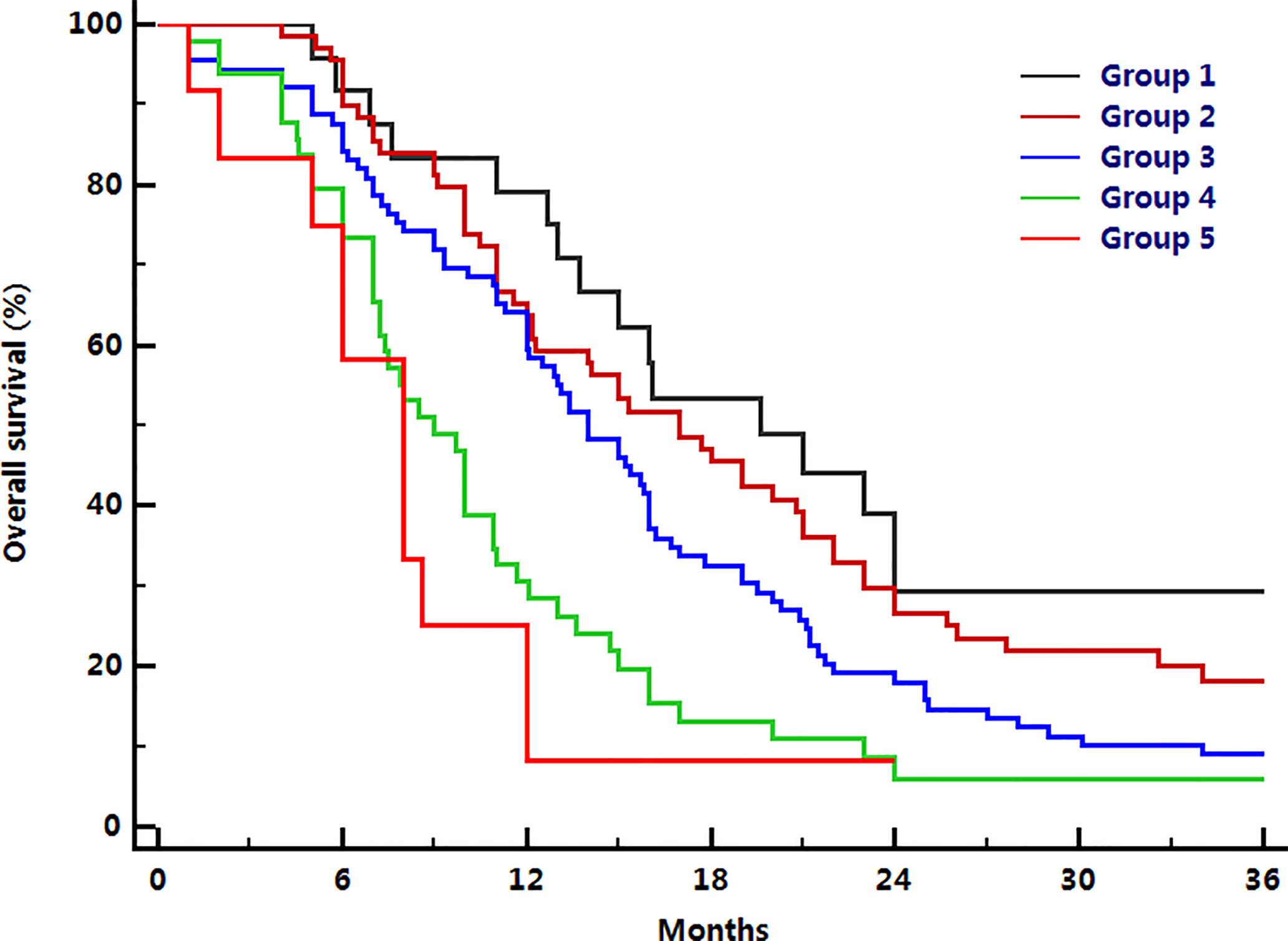
Figure 1 Comparison of overall survival among six groups.
The number of patients was small in group 1, only 24 cases, and there was no significant difference in the overall survival outcomes between group 1 and group 2. Thus, group 1 and group 2 were merged into the same risk group. Based on the same consideration, group 4 and group 5 were also merged into the same risk group. Therefore, all patients were further assigned to one of three risk groups based on the number of presenting risk factors: those having ≤ 2 risk factors were scored as the low-risk group, those with 3 risk factors were scored as the moderate-risk group, and those with ≥ 4 risk factors were scored as the high-risk group. The median OS rates were 17.0 (95% CI: 13.3–20.7) months for the low-risk group, 14.0 (95% CI: 11.7–16.3) months for the moderate-risk group, and 8.0 (95% CI: 6.8–9.2) months for the high-risk group. The 1-year OS rates for low-risk, moderate-risk, and high-risk group were 67.7%, 59.6%, and 26.2%; 2-year OS rates were 32.1%, 18.0%, and 7.9%; 3-year OS rates were 19.3%, 7.9%, and 0%, respectively (P<0.001, Figure 2).
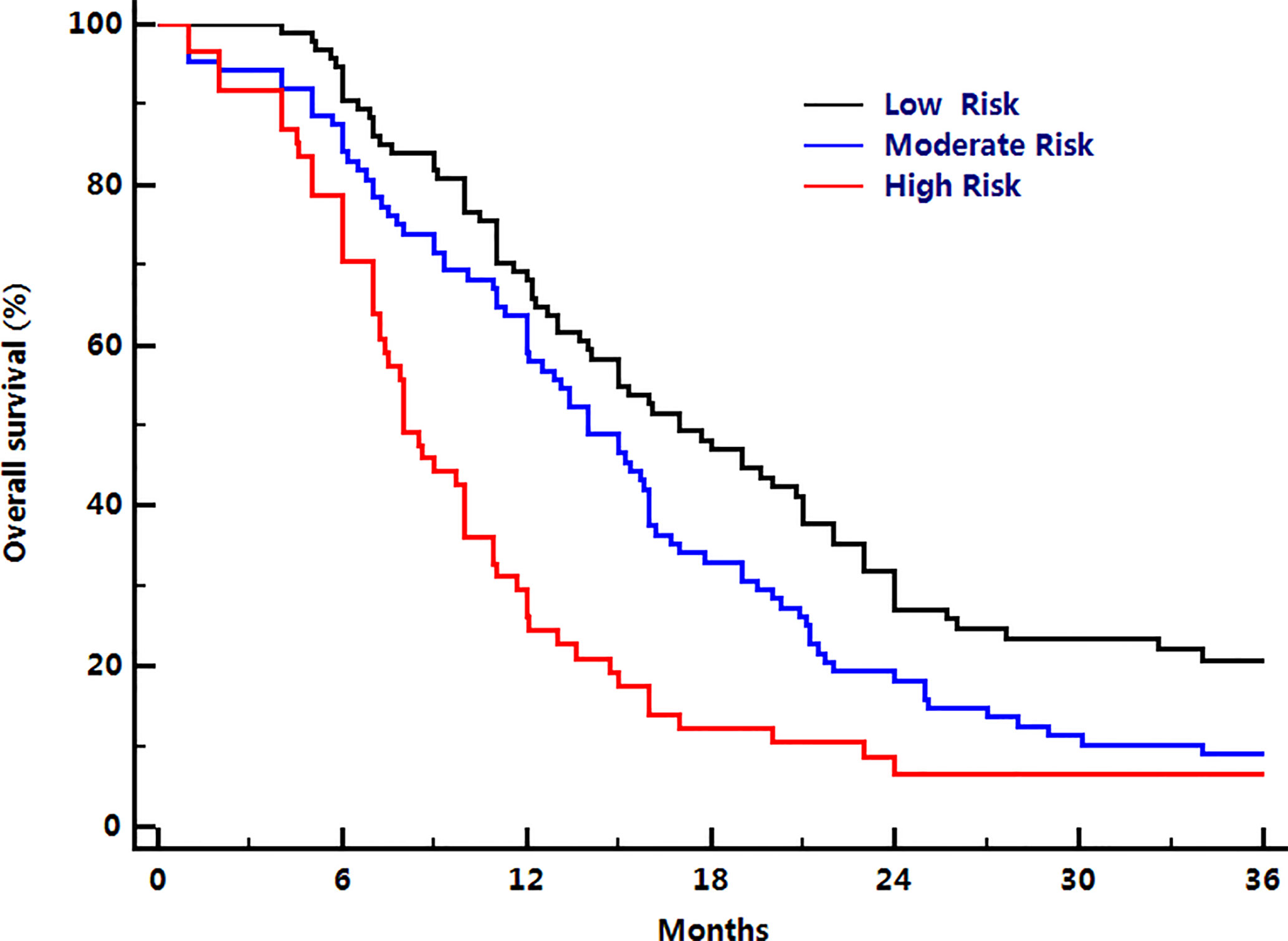
Figure 2 Comparison of overall survival among three different risk groups.
Among these three risk groups, group comparison analysis revealed significant differences in OS time between any two groups (low-risk: moderate-risk group, P= 0.023; low-risk: high-risk group, P< 0.001; moderate-risk: high-risk group, P< 0.001). Herrell’s c-index was 0.672. When the whole group was subdivided into those with oligometastatic (who had <5 metastases) (P<0.001) and non-oligometastatic diseases (who had ≥5 metastases) (P = 0.026), overall survival time among these three risk groups remained significant.
Around 60% of patients initially diagnosed with NSCLC have distant metastases (1). Recently, there has been increasing evidence demonstrating that a subset of patients with metastatic diseases could benefit from radiation therapy to the primary tumor with concurrent chemotherapy. However, not all patients could benefit from this treatment modality, and there is no consensus on the use of concurrent chemotherapy and radiotherapy for NSCLC (23). Therefore, we collected data from two prospective studies to identify patients with metastatic diseases who may benefit from chemotherapy administered concurrently with radiation therapy to the primary tumor. In this research, we developed a practical prognostic model based on laboratory and clinical parameters and demonstrated its predictive effect on the overall survival of metastatic NSCLC patients treated with chemotherapy with concurrent radiation to the primary tumor.
In this study, multivariate analysis showed that 6 factors have an effect on overall survival including two clinical parameters (sex, KPS score), one treatment-related parameter (the number of chemotherapy cycles), and three hematological parameters (Hb level, neutrophil, and PLT count).
As inflammation plays an important role in the pathogenesis and tumor progression in patients with NSCLC (29), hematological markers of systemic inflammation could be considered as potential prognostic factors for overall survival. Additionally, neutrophils and lymphocytes appear to be the main candidates for this role. Consistent with the result of a previous study (26), neutrophil count was related to overall survival in this study. It has been shown that tumor cells aggregate with PLTs, evade recognition by the immune system, adhere to distant vascular endothelial cells, and continue to metastasize, invade, and grow through the blood circulation (30). PLT counts in lung cancer patients are significantly increased compared with the healthy population, and high platelet count indicates poor prognosis for NSCLC patients (30, 31). Hemoglobin is an important biomarker for anemia. Cancer-related anemia is a multifactorial issue, which is associated with the nutritional, metabolic, and immune components of cancer, as well as the progression and severity of cancer (32). Hb level is a significant predictor of survival outcomes in patients with NSCLC (33, 34). Consistent with the result of previous publications, we also found neutrophil count, PLT count, and Hb levels were independent prognostic factors for OS in metastatic NSCLC patients treated with concurrent chemoradiotherapy.
According to ASCO guidelines, 4–6 chemotherapy cycles were recommended for stage IV NSCLC (35). We found that when patients were grouped according to the number of chemotherapy cycles, the overall survival time of patients receiving ≥4 cycles of chemotherapy was prolonged. In this study, multivariate analysis showed that the number of cycles of chemotherapy had a statistically significant effect on OS. Consistent with the result of previous publications, we also found that good performance status and female sex were associated with better OS (24, 25, 27, 36, 37).
The prognosis of metastatic NSCLC can be extremely different because of its heterogeneous characteristics, so it is necessary to establish a well-defined risk scoring system to predict the survival of metastatic NSCLC. Ulas et al. established a laboratory prognostic index (LPI) in advanced NSCLC patients based on hematologic and biochemical parameters. From their result, LPI combined with clinical parameters may help formulate individualized treatment plans and predict survival rates (25). Gagnon et al. developed a Montreal prognostic score based on LDH, albumin, CRP, and neutrophil lymphocyte ratio in incurable lung cancer patients. Montreal prognostic score divided patients into three distinct groups: the median OS times were 2.5, 8.2, and 18.2 months, respectively (log-rank, P <0.001) (38).
The risk of death is highly variable because of the interactions between clinical characteristics and treatment. However, there was no risk scoring system to predict the survival of metastatic NSCLC patients treated with chemotherapy with concurrent radiation to the primary tumor. This study classified patients into low-risk, moderate-risk, and high-risk groups based on six independent prognostic factors.
Previous publications showed that chemotherapy alone produces median overall survival time, and 1- and 2-year OS rates were approximately 8.0 months, 30.0%, and 10.0%, respectively for metastatic NSCLC (13, 39). In this study, the median OS were 17.0 months for the low-risk group, 14.0 months for the moderate-risk group, and 8.0 months for the high-risk group; the 1-year OS rates for the low-risk, moderate-risk, and high-risk groups were 67.7%, 59.6%, and 26.2%; 2-year OS rates were 32.1%, 18.0%, and 7.9%; 3-year OS rates were 19.3%, 7.9%, and 0% respectively. Our findings indicated that the combination of systemic chemotherapy and concurrent radiotherapy to the primary thoracic tumor could further improve survival for low-risk and moderate-risk patients. For high-risk patients, the addition of radiotherapy resulted in no improvement in survival compared with chemotherapy alone (13, 39, 40). Based on current data, we suggest risk-adapted therapy for metastatic NSCLC: low-risk and moderate-risk patients may benefit from radiotherapy to the primary tumor with concurrent chemotherapy, and high-risk patients might be treated with chemotherapy alone.
Literature data supported the role of local treatment in oligometastatic NSCLC disease (20, 22). However, there was no uniform definition of oligometastatic disease in NSCLC (16, 18, 20, 22, 41–43). According to our institutional data and other reports, nearly 90% of stage IV NSCLC patients have metastases confined to one to three organs (12, 14, 44). In this study, all patients had metastases confined to three or fewer organs (regardless of the number of metastatic lesions in each organ). In 2019, the European consensus group proposed a provisional definition of oligometastatic NSCLC as follows: maximum of five metastases and three organs (45). We found that the number of metastatic lesions were associated with OS in univariate analysis. When the entire group was divided according to the total number of metastases (< 5 metastases vs. ≥5 metastases), the prognostic model retained significance for predicting OS. Thus, we propose that this model can be applied to patients with oligometastatic (< 5 metastases) or non-oligometastatic (≥5 metastases) diseases.
We acknowledge several limitations in the current study. Pharmacotherapy has been the main treatment for metastatic NSCLC and still plays an irreplaceable role. In recent years, molecular targeted therapy and immunotherapy have yielded good survival outcomes in patients with metastatic NSCLC (46, 47). For metastatic NSCLC patients, thoracic radiation plus molecular targeted therapy or immunotherapy may produce better survival outcomes as compared with molecular targeted therapy or immunotherapy alone (19, 48, 49). Since none of the patients in this study have received molecular targeted therapy or immunotherapy, we cannot comment on whether the current predictive model is applicable for metastatic NSCLC patients treated with thoracic radiation in combination with targeted therapy or immunotherapy. Thus, it is necessary to further investigate a prognostic model for metastatic NSCLC with thoracic radiotherapy combined with targeted therapy or immunotherapy. Moreover, we did not directly compare survival outcomes between chemotherapy alone and chemotherapy with concurrent radiotherapy to the primary tumor in different risk subgroups. Therefore, we suggest further investigation on the efficacy of concurrent radiotherapy to the primary tumor in different subgroups of metastatic NSCLC treated with chemotherapy.
Metastatic NSCLC patients treated with chemotherapy in combination with thoracic radiation were classified as low-risk, moderate-risk, or high-risk group using six independent prognostic factors (sex, KPS score, number of chemotherapy cycles, Hb level, neutrophil, and PLT count). Risk-adapted therapy of radiation to the primary tumor based on systemic chemotherapy for the low-risk or moderate-risk and chemotherapy alone for the high-risk group may be the appropriate treatment. The value of concurrent radiation for metastatic NSCLC patient needs to be further investigated in different risk subgroups, and additional studies are necessary to establish a predictive model for metastatic NSCLC treated with thoracic radiation in combination with targeted therapy or immunotherapy.
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
This study was reviewed by the ethical review boards in China (Ethics Committee of Guizhou Cancer Hospital, GuiYang, China). The patients/participants provided their written informed consent to participate in this study.
S-FS and BL designed the study. L-FL, Q-SL, Y-XH, W-GY, X-XC, ZM, W-WO, Y-CG, and CH collected the data. L-FL and Q-SL drafted and prepared the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by grants from Guizhou Provincial Education Office, China [grant number KY (2016) 032] and Guizhou Province’s Science and Technology Major Project, China [grant number Qian-J Zhong (2015) 2003]. The funders were not involved in research design, information collection and analysis, decision to publish, or writing the manuscripts.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin (2018) 68:7–30. doi: 10.3322/caac.21442
2. Besse B, Adjei A, Baas P, Meldgaard P, Nicolson M, Paz-Ares L, et al. 2nd ESMO Consensus Conference on Lung Cancer: non-small-cell lung cancer first-line/second and further lines of treatment in advanced disease. Ann Oncol (2014) 25:1475–84. doi: 10.1093/annonc/mdu123
3. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med (2009) 361:947–57. doi: 10.1056/NEJMoa0810699
4. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol (2011) 12:735–42. doi: 10.1016/s1470-2045(11)70184-x
5. Tanaka T, Matsuoka M, Sutani A, Gemma A, Maemondo M, Inoue A, et al. Frequency of and variables associated with the EGFR mutation and its subtypes. Int J Cancer (2010) 126:651–5. doi: 10.1002/ijc.24746
6. Qian H, Gao F, Wang H, Ma F. The efficacy and safety of crizotinib in the treatment of anaplastic lymphoma kinase-positive non-small cell lung cancer: a meta-analysis of clinical trials. BMC Cancer (2014) 14:683. doi: 10.1186/1471-2407-14-683
7. Cheng Y, Wang Y, Zhao J, Liu Y, Gao H, Ma K, et al. Real-world EGFR testing in patients with stage IIIB/IV non-small-cell lung cancer in North China: A multicenter, non-interventional study. Thoracic Cancer (2018) 9:1461–9. doi: 10.1111/1759-7714.12859
8. Zhou Q, Song Y, Zhang X, Chen GY, Zhong DS, Yu Z, et al. A multicenter survey of first-line treatment patterns and gene aberration test status of patients with unresectable Stage IIIB/IV nonsquamous non-small cell lung cancer in China (CTONG 1506). BMC Cancer (2017) 17:462. doi: 10.1186/s12885-017-3451-x
9. Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho BC, Turna HZ, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, phase 3 trial. Lancet (2019) 393:1819–30. doi: 10.1016/s0140-6736(18)32409-7
10. Hu X, Hay JW. First-line pembrolizumab in PD-L1 positive non-small-cell lung cancer: A cost-effectiveness analysis from the UK health care perspective. Lung Cancer (2018) 123:166–71. doi: 10.1016/j.lungcan.2018.07.012
11. Liao W, Huang J, Hutton D, Li Q. Cost-effectiveness analysis of first-line pembrolizumab treatment for PD-L1 positive, non-small cell lung cancer in China. J Med Econ (2019) 22:344–9. doi: 10.1080/13696998.2019.1570221
12. Scagliotti GV, De Marinis F, Rinaldi M, Crino L, Gridelli C, Ricci S, et al. Phase III randomized trial comparing three platinum-based doublets in advanced non-small-cell lung cancer. J Clin Oncol (2002) 20:4285–91. doi: 10.1200/JCO.2002.02.068
13. Schiller JH, Harrington D, Belani CP, Langer C, Sandler A, Krook J, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med (2002) 346:92–8. doi: 10.1056/NEJMoa011954
14. Mehta N, Mauer AM, Hellman S, Haraf DJ, Cohen EE, Vokes EE, et al. Analysis of further disease progression in metastatic non-small cell lung cancer: implications for locoregional treatment. Int J Oncol (2004) 25:1677–83. doi: 10.3892/ijo.25.6.1677
15. Higginson DS, Chen RC, Tracton G, Morris DE, Halle J, Rosenman JG, et al. The impact of local and regional disease extent on overall survival in patients with advanced stage IIIB/IV non-small cell lung carcinoma. Int J Radiat Oncol Biol Phys (2012) 84):e385–92. doi: 10.1016/j.ijrobp.2012.04.045
16. Lopez Guerra JL, Gomez D, Zhuang Y, Hong DS, Heymach JV, Swisher SG, et al. Prognostic Impact of Radiation Therapy to the Primary Tumor in Patients With Non-small Cell Lung Cancer and Oligometastasis at Diagnosis. Int J Radiat Oncol Biol Phys (2012) 84:e61–e7. doi: 10.1016/j.ijrobp.2012.02.054
17. Su SF, Hu YX, Ouyang WW, Lu B, Ma Z, Li QS, et al. Overall survival and toxicities regarding thoracic three-dimensional radiotherapy with concurrent chemotherapy for stage IV non-small cell lung cancer: results of a prospective single-center study. BMC Cancer (2013) 13:474. doi: 10.1186/1471-2407-13-474
18. Su S, Li T, Lu B, Wang X, Li J, Chen M, et al. Three-Dimensional Radiation Therapy to the Primary Tumor With Concurrent Chemotherapy in Patients With Stage IV Non-Small Cell Lung Cancer: Results of a Multicenter Phase 2 Study From PPRA-RTOG, China. Int J Radiat Oncol Biol Phys (2015) 93:769–77. doi: 10.1016/j.ijrobp.2015.08.012
19. Yen YC, Hsu HL, Chang JH, Lin WC, Chang YC, Chang CL, et al. Efficacy of thoracic radiotherapy in patients with stage IIIB-IV epidermal growth factor receptor-mutant lung adenocarcinomas who received and responded to tyrosine kinase inhibitor treatment. Radiother Oncol (2018) 129:52–60. doi: 10.1016/j.radonc.2018.03.007
20. Iyengar P, Wardak Z, Gerber DE, Tumati V, Ahn C, Hughes RS, et al. Consolidative Radiotherapy for Limited Metastatic Non-Small-Cell Lung Cancer: A Phase 2 Randomized Clinical Trial. JAMA Oncol (2018) 4:e173501. doi: 10.1001/jamaoncol.2017.3501
21. Stephens SJ, Moravan MJ, Salama JK. Managing Patients With Oligometastatic Non-Small-Cell Lung Cancer. J Oncol Pract (2018) 14:23–31. doi: 10.1200/jop.2017.026500
22. Gomez DR, Tang C, Zhang J, Blumenschein GR Jr., Hernandez M, Lee JJ, et al. Local Consolidative Therapy Vs. Maintenance Therapy or Observation for Patients With Oligometastatic Non-Small-Cell Lung Cancer: Long-Term Results of a Multi-Institutional, Phase II, Randomized Study. J Clin Oncol (2019) 37:1558–65. doi: 10.1200/jco.19.00201
23. Moeller B, Balagamwala EH, Chen A, Creach KM, Giaccone G, Koshy M, et al. Palliative thoracic radiation therapy for non-small cell lung cancer: 2018 Update of an American Society for Radiation Oncology (ASTRO) Evidence-Based Guideline. Pract Radiat Oncol (2018) 8:245–50. doi: 10.1016/j.prro.2018.02.009
24. Wakelee HA, Wang W, Schiller JH, Langer CJ, Sandler AB, Belani CP, et al. Survival differences by sex for patients with advanced non-small cell lung cancer on Eastern Cooperative Oncology Group trial 1594. J Thorac Oncol (2006) 1:441–6. doi: 10.1016/S1556-0864(15)31609-9
25. Ulas A, Turkoz FP, Silay K, Tokluoglu S, Avci N, Oksuzoglu B, et al. A laboratory prognostic index model for patients with advanced non-small cell lung cancer. PloS One (2014) 9:e114471. doi: 10.1371/journal.pone.0114471
26. Teramukai S, Kitano T, Kishida Y, Kawahara M, Kubota K, Komuta K, et al. Pretreatment neutrophil count as an independent prognostic factor in advanced non-small-cell lung cancer: an analysis of Japan Multinational Trial Organisation LC00-03. Eur J Cancer (2009) 45:1950–8. doi: 10.1016/j.ejca.2009.01.023
27. Hoang T, Dahlberg SE, Sandler AB, Brahmer JR, Schiller JH, Johnson DH. Prognostic models to predict survival in non-small-cell lung cancer patients treated with first-line paclitaxel and carboplatin with or without bevacizumab. J Thorac Oncol (2012) 7:1361–8. doi: 10.1097/JTO.0b013e318260e106
28. Chen YM, Lai CH, Rau KM, Huang CH, Chang HC, Chao TY, et al. Impact of clinical parameters and systemic inflammatory status on epidermal growth factor receptor-mutant non-small cell lung cancer patients readministration with epidermal growth factor receptor tyrosine kinase inhibitors. BMC Cancer (2016) 16:868. doi: 10.1186/s12885-016-2917-6
29. Shoji F. Clinical impact of the systemic immune-inflammation index in non-small cell lung cancer patients. Ann Transl Med (2020) 8:668. doi: 10.21037/atm.2020.03.180
30. Zhang SS, Zhang M, Yuan L, Zou ZQ. Analysis of platelet parameters and activation markers in hematologic metastases of lung cancer. Chin Med J (Engl) (2019) 132:735–7. doi: 10.1097/cm9.0000000000000138
31. Zhu JF, Cai L, Zhang XW, Wen YS, Su XD, Rong TH, et al. High plasma fibrinogen concentration and platelet count unfavorably impact survival in non-small cell lung cancer patients with brain metastases. Chin J Cancer (2014) 33:96–104. doi: 10.5732/cjc.012.10307
32. Macciò A, Madeddu C, Gramignano G, Mulas C, Tanca L, Cherchi MC, et al. The role of inflammation, iron, and nutritional status in cancer-related anemia: results of a large, prospective, observational study. Haematologica (2015) 100:124–32. doi: 10.3324/haematol.2014.112813
33. Topkan E, Selek U, Ozdemir Y, Yildirim BA, Guler OC, Mertsoylu H, et al. Chemoradiotherapy-induced hemoglobin nadir values and survival in patients with stage III non-small cell lung cancer. Lung Cancer (2018) 121:30–6. doi: 10.1016/j.lungcan.2018.04.016
34. Takigawa N, Segawa Y, Okahara M, Maeda Y, Takata I, Kataoka M, et al. Prognostic factors for patients with advanced non-small cell lung cancer: univariate and multivariate analyses including recursive partitioning and amalgamation. Lung Cancer (1996) 15:67–77. doi: 10.1016/0169-5002(96)00571-5
35. Azzoli CG, Temin S, Giaccone G. 2011 Focused Update of 2009 American Society of Clinical Oncology Clinical Practice Guideline Update on Chemotherapy for Stage IV Non-Small-Cell Lung Cancer. J Oncol Pract (2012) 8:63–6. doi: 10.1200/jop.2011.000374
36. Berardi R, Rinaldi S, Santoni M, Newsom-Davis T, Tiberi M, Morgese F, et al. Prognostic models to predict survival in patients with advanced non-small cell lung cancer treated with first-line chemo- or targeted therapy. Oncotarget (2016) 7:26916–24. doi: 10.18632/oncotarget.8309
37. Ben Amar J, Ben Safta B, Zaibi H, Dhahri B, Baccar MA, Azzabi S. Prognostic factors of advanced stage non-small-cell lung cancer. Tunis Med (2016) 94:360–7.
38. Gagnon B, Agulnik JS, Gioulbasanis I, Kasymjanova G, Morris D, MacDonald N. Montreal prognostic score: estimating survival of patients with non-small cell lung cancer using clinical biomarkers. Br J Cancer (2013) 109:2066–71. doi: 10.1038/bjc.2013.515
39. Aarts MJ, van den Borne BE, Biesma B, Kloover JS, Aerts JG, Lemmens VE. Improvement in population-based survival of stage IV NSCLC due to increased use of chemotherapy. Int J Cancer (2015) 136):E387–95. doi: 10.1002/ijc.29216
40. Morgensztern D, Waqar S, Subramanian J, Gao F, Govindan R. Improving survival for stage IV non-small cell lung cancer: a surveillance, epidemiology, and end results survey from 1990 to 2005. J Thorac Oncol (2009) 4:1524–9. doi: 10.1097/JTO.0b013e3181ba3634
41. Cheruvu P, Metcalfe SK, Metcalfe J, Chen Y, Okunieff P, Milano MT. Comparison of outcomes in patients with stage III versus limited stage IV non-small cell lung cancer. Radiat Oncol (2011) 6:80. doi: 10.1186/1748-717X-6-80
42. Parikh RB, Cronin AM, Kozono DE, Oxnard GR, Mak RH, Jackman DM, et al. Definitive primary therapy in patients presenting with oligometastatic non-small cell lung cancer. Int J Radiat Oncol Biol Phys (2014) 89:880–7. doi: 10.1016/j.ijrobp.2014.04.007
43. Jabbour SK, Daroui P, Moore D, Licitra E, Gabel M, Aisner J. A novel paradigm in the treatment of oligometastatic non-small cell lung cancer. J Thorac Dis (2011) 3:4–9. doi: 10.3978/j.issn.2072-1439.2010.12.09
44. Li FH, Lu B, HY F, Han L, QS L, HQ L, et al. Metastasis features of 546 patients with stage IV non-small cell lung cancer at first visit and the significance in radiotherapy. Chin J Radiat Oncol (2012) 21:122–5. doi: 10.3760/cma.j.issn.1004-4221.2012.02.008
45. Dingemans AC, Hendriks LEL, Berghmans T, Levy A, Hasan B, Faivre-Finn C, et al. Definition of Synchronous Oligometastatic Non-Small Cell Lung Cancer-A Consensus Report. J Thorac Oncol (2019) 14:2109–19. doi: 10.1016/j.jtho.2019.07.025
46. Hirsch FR, Scagliotti GV, Mulshine JL, Kwon R, Curran WJ Jr., Wu YL, et al. Lung cancer: current therapies and new targeted treatments. Lancet (2017) 389:299–311. doi: 10.1016/s0140-6736(16)30958-8
47. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2016) 375:1823–33. doi: 10.1056/NEJMoa1606774
48. Theelen WSME, Peulen HMU, Lalezari F, van der Noort V, de Vries JF, Aerts JGJV, et al. Effect of Pembrolizumab After Stereotactic Body Radiotherapy vs Pembrolizumab Alone on Tumor Response in Patients With Advanced Non-Small Cell Lung Cancer: Results of the PEMBRO-RT Phase 2 Randomized Clinical Trial. JAMA Oncol (2019) 5:1276–82. doi: 10.1001/jamaoncol.2019.1478
Keywords: prognostic model, overall survival, metastasis, non-small cell lung cancer, chemoradiotherapy
Citation: Liu L-F, Li Q-S, Hu Y-X, Yang W-G, Chen X-X, Ma Z, OuYang W-W, Geng Y-C, Hu C, Su S-F and Lu B (2021) Prognostic Model to Predict Overall Survival for Metastatic Non-Small Cell Lung Cancer Patients Treated With Chemotherapy Combined With Concurrent Radiation Therapy to the Primary Tumor: Analysis From Two Prospective Studies. Front. Oncol. 11:625688. doi: 10.3389/fonc.2021.625688
Received: 03 November 2020; Accepted: 19 January 2021;
Published: 25 February 2021.
Edited by:
Alessio Bruni, University Hospital of Modena, ItalyReviewed by:
Nan Bi, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaCopyright © 2021 Liu, Li, Hu, Yang, Chen, Ma, OuYang, Geng, Hu, Su and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sheng-Fa Su, c3VzaGVuZ2ZhMjAwNUAxNjMuY29t; Bing Lu, Z3lsdWJpbmcyMDE5QHNpbmEuY24=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.