 Mary Elizabeth Money1,2*
Mary Elizabeth Money1,2* Aghiles Hamroun3,4
Aghiles Hamroun3,4 Yan Shu5
Yan Shu5 Carolyn Matthews6
Carolyn Matthews6 Sara Ahmed Eltayeb7
Sara Ahmed Eltayeb7 Giuliano Ciarimboli7
Giuliano Ciarimboli7 Christine Noel Metz8,9
Christine Noel Metz8,9- 1Department of Medicine, School of Medicine, University of Maryland, Baltimore, MD, United States
- 2Department of Medicine, Meritus Medical Center, Hagerstown, MD, United States
- 3Lille University, Lille University Hospital Center, Nephrology Department, Lille, France
- 4Institut National de la Santé et de la Recherche Médicale (INSERM), Clinical Epidemiology Team, CESP, Villejuif, France
- 5Department of Pharmaceutical Sciences, School of Pharmacy, University of Maryland, Baltimore, MD, United States
- 6Texas Oncology, P.A., Dallas, TX, United States
- 7Medicine Clinic D, University Hospital Münster, Münster, Germany
- 8Institute of Molecular Medicine, Feinstein Institutes, Manhasset, NY, United States
- 9Department of Molecular Medicine, Donald and Barbara Zucker School of Medicine at Hofstra-Northwell, Hempstead, NY, United States
After more than four decades of post-approval, cisplatin is still an important treatment for numerous cancers. However, acute kidney injury (AKI), defined as significant impairment of renal filtration as discussed below, is the major limiting side effect of cisplatin, occurring in approximately 30% of patients (25–33% after the first course). Cisplatin also damages the kidneys’ ability to reabsorb magnesium in 40–100% of patients, with collateral health risks due to subsequent hypomagnesemia. Multiple methods and drugs have been proposed for preventing cisplatin-induced AKI, including saline infusion with or without mannitol, which has not always prevented AKI and has been found to activate a cellular stress response in renal tubular cells. While numerous reports and trials, as well as the National Comprehensive Cancer Network (NCCN), support premedication with magnesium and hydration, this practice has not been universally accepted. Many clinics administer intravenous magnesium (IV) only after identification of hypomagnesemia post-cisplatin treatment, thus placing patients at risk for AKI and chronic renal loss of magnesium. We present the following case report and additional supporting evidence identifying the immediate effect of IV magnesium prior to intraperitoneal cisplatin for cycle 4 because of documented hypomagnesemia resulting in normalization of oliguria, which had been experienced for the first three cycles. The patient subsequently requested and received IV magnesium before cisplatin for the next two cycles with continuation of normal urinary output. The effect of pretreatment with IV magnesium on urine output following cisplatin has not been previously reported and further supports pre-cisplatin administration. In addition, two recent meta-analyses of clinical trials and pre-clinical research are reviewed that demonstrate effectiveness of magnesium pretreatment to preventing AKI without reducing its chemotherapeutic efficacy. This case report with additional evidence supports the adoption of administration of 1–3 g IV magnesium before cisplatin as best practice to prevent cisplatin induced AKI and hypomagnesemia regardless of patient baseline serum magnesium levels.
Introduction
Oncologists now have numerous therapeutic agents for various cancers, but cisplatin, the first platinum compound the FDA approved in 1978, continues to be one of the most effective treatments against numerous cancers (1, 2). Cisplatin is highly effective in damaging cancer cell DNA, but its use is restrained by dose-limiting side effects, including AKI, considered to be the most serious toxicity, occurring in approximately one-third of patients (3). Even a single injection of cisplatin may result in a transient episode of AKI in 20–30% of patients (4, 5), which can be missed when measuring only the serum creatinine and blood urea nitrogen. Multiple reviews have discussed the molecular mechanism of AKI induced by cisplatin, which is beyond the scope of this case report (2, 6). Providers in outpatient clinics may not appreciate oliguria as a sign of AKI as manifested by the case report discussed below. Thus, identifying an agent that will prevent or ameliorate this irreversible side effect has been a priority.
The most recognized and followed recommendation to prevent AKI is fluid administration before and after cisplatin, typically with or without mannitol or furosemide (2, 7, 8). Magnesium administered concomitantly with cisplatin has been recommended by Vokes (9) since 1990 to prevent secondary hypomagnesemia due to distal tubular damage (10) and by multiple other clinicians to prevent AKI, (3, 11–16) but has not been established as a standard protocol and was not followed initially for this patient. This review will identify the benefits of this therapy for patients receiving cisplatin, regardless of serum magnesium levels, proposing the adoption of magnesium administration before cisplatin as best practice protocol.
Case Report
The patient is a 71-year-old board-certified internist who received intraperitoneal (IP) cisplatin and paclitaxel for recurrent ovarian cancer in December 2014.
Background: Stage 3C, poorly differentiated serous adenocarcinoma of the fallopian tube was diagnosed by exploratory surgery at Mercy Medical Center, Baltimore, MD by Dr. Neil Rosenshein in September 2012. Debulking was complete except for 1.5 cm tumor implant on the diaphragm. Chemotherapy with paclitaxel and carboplatin resulted in complete remission by 2013. Background medical history for patient includes: family history for breast cancer (mother and maternal grandmother); non-smoker, history of A–V dura fistula treated conservatively, primary hypothyroidism, allergic rhinitis; BP 112/78, pulse 72, BMI 20.9. Patient was entirely asymptomatic but CA 125 had increased from eight to 19 on 10/20/14 and a PET scan showed 1 cm implant on the right kidney on 10/31/14. Rather than accepting standard chemotherapy, the patient underwent exploratory laparotomy by Dr. Robert Edwards at Magee-Women’s hospital, UPMC, Pittsburgh, PA. No tumor implant was identified, but cell washings were atypical and an intraperitoneal port was placed for IP therapy.
Baseline serum lab included: blood urea nitrogen (BUN) 16, creatinine (Cr) 0.7, and magnesium 2.0 mg/dL (normal range: 1.7–2.2) on 12/26/14. Cisplatin and paclitaxel were administered via IP infusion every 21 days for six cycles beginning on 12/29/14 (day 1). Paclitaxel 135 mg/m2 in 500 ml of normal saline intravenous (IV) over 3 h was administered on day 1. After 1 L of normal saline IV, cisplatin at 75 mg/m2 was given in 1 L of normal saline IP followed by a second liter of normal saline IP, if tolerated. Another liter of normal saline IV was subsequently administered, too. Significant oliguria (concentrated, dark urine estimated at <30 cc h) was observed within 3 h after IP cisplatin. This oliguria and abdominal distention with pain continued for the next 36–48 h despite >2,000 cc oral intake of liquids and an additional liter of normal saline IV the following day.
Because the patient (an internist) recognized the disproportional oliguria, the on-call provider was consulted that evening within 6 h of cisplatin administration, but no action was recommended since the patient still had some urine output. AKI, which manifested as oliguria, was not recognized and stat renal function studies were not ordered. Diuresis had occurred by 1/3/15 when the following tests were obtained prior to having urgent surgery for a fractured wrist due to a fall on ice: BUN 20, Cr 0.74, and magnesium 1.3 mg/dL.
Oral magnesium oxide >500 mg was consumed daily. Intravenous magnesium was not administered unless serum magnesium dropped below 1.5 mg/dL, which was only checked immediately before each cycle of chemotherapy and not in between. On 2/9/15, prior to the next cycle, which had been delayed for 3 weeks due to a wrist fracture, BUN was 22, Cr 0.8, and magnesium 1.8.
The patient continued to experience severe oliguria immediately following cisplatin IP administration, lasting for approximately 48–72 h for the next two cycles, but on day 1 of cycle 4 on 3/25/15, 4 g (32.48 mEq) magnesium sulfate was administered IV prior to chemotherapy for a serum magnesium of 1.0 mg/dL. (Serum magnesium had been 1.6 on 3/2/15). The patient immediately observed normal urinary output on day 2 post-cisplatin and thereafter. In addition, abdomen distention and pain were significantly less than during the prior cycles.
Recognizing this response, the physician-patient completed a literature search regarding the effect of magnesium on cisplatin toxicity and consulted with a scientist who had recently published studies in rodents demonstrating the benefits of pretreating with magnesium to protect against cisplatin-induced AKI (17). Therefore, the patient subsequently requested and received 2 g of magnesium sulfate IV pre-cisplatin (on day 2) for cycles 5 and 6 even though serum magnesium was 1.7 mg/dL. To clearly demonstrate the effectiveness, she recorded the fluid intake and output for day 2, cycle 6: 4,800 cc combined IV, IP, and oral route, with a concomitant urine output of 4,950 cc in 24 h. The patient continued to demonstrate improved tolerance to the IP treatment with the administration of IV magnesium preceding cisplatin.
After completion of the six cycles, on 6/29/15, relevant values were: BUN 19, serum Cr 0.9, and magnesium 1.9. Patient at that time was receiving 1–2 g of IV magnesium weekly and has continued to suffer from persistent hypomagnesemia requiring 600 mg of oral magnesium threonate in divided doses daily to prevent tetany. These effects are presumed due to the irreversible AKI from cycles 1–3 prior to pretreatment with magnesium in subsequent cisplatin cycles. Glomerular filtration rate from 2015 until 2020 has been greater than 59 ml/min and current renal function on 8/27/20 was: BUN 23, Cr 1.04. As a physician, the patient strongly supports this case report to prevent AKI, hypermagnesemia, and the discomfort associated with intraperitoneal cisplatin that was diminished with magnesium preceding cisplatin.
Discussion
Overview of Acute Kidney Injury by Cisplatin
According to the Kidney Disease Improving Global Outcomes (KDIGO), AKI is defined as ≥0.3 mg/dL increase in serum creatinine or a 0.5 ml/kg/h decrease in urine output within 48 h; whereas Common Toxicity Criteria for Adverse Events Version 4.0 (CTCAE v4.0) agrees on serum creatinine increase ≥0.3 mg/dL but with no time consideration (5).
Using CTCAE v4.0 criteria, 26.5% of patients experienced AKI after the first round of cisplatin-based chemotherapy in one retrospective study for urothelial cancer, resulting in >40% being unable to receive the planned second round, and 50% reduction in 3-year survival (5). Consequently, mortality is increased among patients with AKI, frequently due to inability to continue chemotherapy as scheduled (18, 19).
Risk factors for renal damage include people who are older, female, African American (20), smokers, have hypoalbuminemia, prior kidney damage, hypomagnesemia, dehydration, and/or have concomitant medical conditions such as diabetes, liver disease and use of angiotensin receptor blockers, angiotensin-converting enzyme inhibitors, diuretic therapy, and non-steroidal anti-inflammatory drugs (16–18).
Cisplatin is freely filtered at the glomeruli but is subsequently absorbed by the proximal tubule cell where it becomes a more potent toxin by multiple enzymatic pathways including gamma glutamyl transpeptidase (GGT), which has the highest activity in the kidneys (2, 6, 21).
However, a consistent amount of cisplatin is secreted from the blood into the urine through the cells of proximal tubules (22). Here, cisplatin uptake is accomplished by the human copper transport protein 1 (Ctr1) and the organic cation transporter 2 (OCT2) (23) located on the basolateral side of the proximal (24) and distal (25) renal tubules, as well as by passive diffusion (26). Concentration in the proximal tubule may be five times greater than the blood (27), with intrinsic damage of the proximal and distal tubules resulting in renal tubular cells death, affecting renal tubular blood flow, decreasing glomerular filtration rate, and preventing reabsorption of magnesium and other electrolytes (2). Excretion from the tubular cells is dependent on multidrug extrusion transporters (MATEs) (6, 28). Although renal tubular cells may recover, fibrotic scarring may occur resulting in chronic kidney disease (CKD) (29).
Bunel et al. (29) in a small human study, identified an increase in urinary biomarkers for acute renal damage within 3 h after cisplatin administration, but a diagnostic rise in plasma creatinine in each patient with AKI was delayed until 3–6 days post-administration, by which time urinary biomarkers had normalized.
Summary of Studies Demonstrating Effectiveness of Magnesium in Humans
In 2019, two systematic reviews and meta-analysis of therapies directed at prevention of cisplatin AKI were published, both suggesting a benefit with pre-administration of IV magnesium (30, 31) (Table 1). Casanova reviewed all placebo-controlled trials published up to 2017 (22 met their criteria), and concluded that 1 g (8 mEq) of IV magnesium before cisplatin reduced AKI (30).
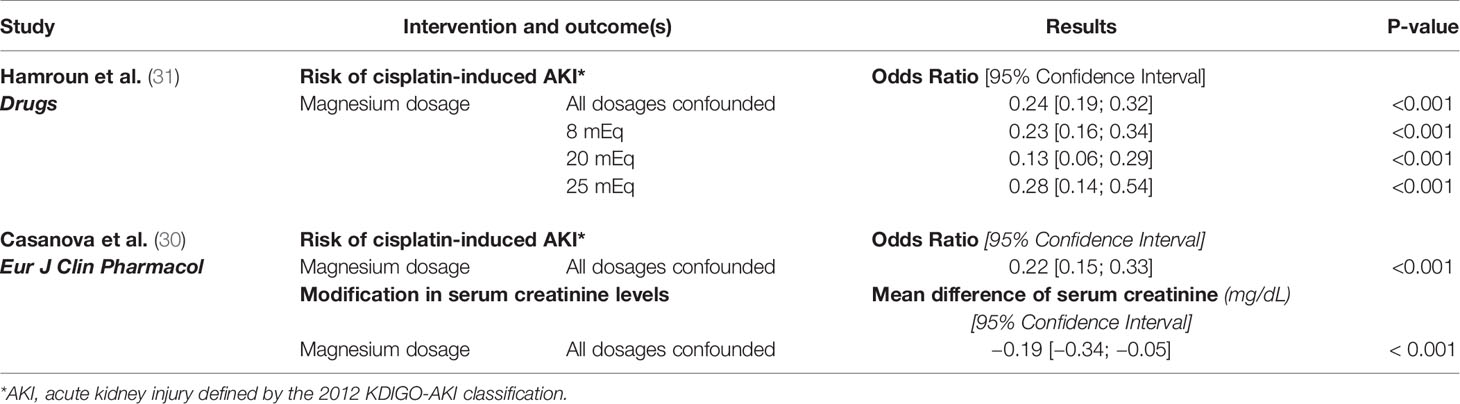
Table 1 Published results on the association between cisplatin-induced AKI* and magnesium administration.
Hamroun et al. (31) searched Pubmed, Embase, and Web of Science from January 1, 1978, to June 1, 2018, assessing cisplatin AKI as defined by the 2012 AKI-KDIGO classification, which identified stage 1 as either serum creatinine 1.5–1.9 times OR ≥0.3 mg/dL (≥26.5 mmol/L) increase above baseline, or urine output decrease to 0.5 ml/kg/h for 6–12 h; stage 2: serum creatinine 2–2.9 × baseline, or decrease in urine output <0.5 ml/kg/h for × 12 h; stage 3: serum creatinine 3 × baseline or urine output <0.3 ml/kg/h (32). Of 4,520 eligible studies reviewed, 51 articles fulfilled the authors’ selection criteria, which included evaluating 21 different prevention methods. A meta-analysis was only performed on those studies that used magnesium at the same time as the first dose of cisplatin (15 observational involving 1,841 patients), and demonstrated a significant AKI protection for all grades of injury (31). Based upon analysis of the data regarding stage 1 AKI, “25 mEq of magnesium was associated with a significant nephron-protective effect (OR 0.20 [0.12–0.31], with a positive trend test (p = 0.002)” (31).
Magnesium Prevents Renal Toxicity in Animal Studies: Potential Mechanisms
Like humans, laboratory animals exhibit hypomagnesemia and AKI following serial cisplatin doses. Cisplatin specifically targets the proximal tubules, which comprise a significant portion of the kidneys. The proximal tubules contain a high density of epithelial cells with a large number of mitochondria necessary for providing the critical regulatory (pH balance, absorption, and secretion) and endocrine functions of the kidneys. In mice, organic cation transporters 1 and 2 (OCT 1 and OCT2) located on proximal tubule epithelial cells are considered to be the main transporters involved in cisplatin uptake by the renal proximal tubules (33, 34). Thus, this segment of the nephron is most susceptible to cisplatin-induced AKI (35, 36). Once taken up by the renal epithelial cell, cisplatin mediates its acute toxic effects by enhancing inflammation [via the Extracellular Signal Regulated Kinase (ERK) and Signal Transducer and Activator of Transcription 3 (STAT3) signaling and subsequent cytokine production], increasing oxidative stress and by inducing cell death (apoptosis, necrosis, and autophagy).
Animal studies also demonstrate that cisplatin treatment lowers serum magnesium levels (37, 38) and that poor magnesium status enhances cisplatin-induced AKI (17, 37, 39, 40). Although the exact mechanism(s) involved are not completely understood, there is some evidence showing that magnesium absorption is impaired by cisplatin-mediated renal damage, suggesting that magnesium deficiency augments cisplatin uptake (probably via OCT2 and Ctr1) and reduces elimination (via MATE1) by kidney epithelial cells. Most importantly, the nephrotoxicity of cisplatin can be blocked by early and sustained magnesium supplementation in magnesium-deficient animals, preventing irreversible kidney injury (17, 39). Additional data support that the host’s magnesium status regulates multiple pathways associated with cisplatin-induced AKI, including oxidative stress, inflammation and apoptosis, and early magnesium supplementation protects against cisplatin-induced kidney damage through modulating these pathways (17, 40). Finally, while magnesium deficiency was associated with significantly larger tumors in mice and reduced cisplatin-mediated tumor killing in vivo, early magnesium supplementation was shown to protect the kidneys against cisplatin-mediated damage without compromising cisplatin anti-tumor efficacy while additionally potentiating the cytotoxic effect (39, 40). Together, these data strongly support that early magnesium supplementation exerts kidney-protective effects and may improve the anti-tumor efficacy of cisplatin.
Importance of Magnesium Homeostasis and Health Risks Associated with Hypomagnesemia
Over 300 biological enzymes are dependent on magnesium, the second most abundant intracellular cation, and fourth most abundant cation in the body (41). The normal body contains 22–26 g of magnesium; 52.9% in the bone, 27% in the muscle, 19.3 in soft tissue, 0.5% in red blood cells, and 0.3% in the serum (42).
Although magnesium deficiency is almost always asymptomatic (43), it may lead to long-term health problems including but not limited to: affecting cardiac electrical activity, including sudden death; association with insulin resistance, inhibiting acute phase of insulin release in hyperglycemia; contributing to progression of atherosclerosis by affecting lipid concentrations; hypertension; osteoporosis; increase frequency in renal calculi; reactive airway disease; muscle weakness; and multiple non-specific complaints including: fatigue, anorexia, fibromyalgia, tendonopathy, tetany, and mood alterations (41).
Measurement of the serum magnesium level is not an accurate reflection of total body stores. Renal excretion is predominantly responsible for maintaining serum balance with 70–80% of non-protein bound magnesium being filtered at the glomerulus, 95% of the magnesium in plasma is reabsorbed by the kidneys (60% at the ascending loop of Henle and 10% in the distal tubule, resulting in a loss of only 100 mg) (41, 42, 44).
Although not labeled AKI, the most common evidence of early renal damage is hypomagnesemia, first identified in 1979 (45). Hypomagnesemia may enhance the severity of nephrotoxicity (46). In addition, observational studies in humans, similar to those in animals, have demonstrated that premedication with magnesium prior to cisplatin may reduce the nephrotoxicity of magnesium loss. In 1990, Vokes (9) reported a randomized study of 23 patients treated with cisplatin for head and neck cancer using oral magnesium aspartate hydrochloride either by continuous oral magnesium, with dosage being increased or magnesium supplemented intravenously if unable to be tolerated versus intermittent administration only if the serum magnesium level dropped to ≤1.4 mg/dL. All patients receiving intermittent magnesium required magnesium at some point in the study, but 80% of patients receiving continuous magnesium never developed hypomagnesemia in a given cycle. Likewise, Martin et al. (47) demonstrated in 1992 that both intravenous (3 g before each cycle) and oral magnesium supplementation (2 g orally every 8 h, days 2–21 of each cycle) appeared effective in prevention of cisplatin-induced hypomagnesemia in the majority of patients with only mild gastrointestinal side effects observed with the oral group. Vokes concluded that “preventive administration of a magnesium supplement can ameliorate, if not completely eradicate, cisplatin-induced hypomagnesaemia.” (9) Hodgkinson, in 2006, also recommended routine supplementation of magnesium with each cycle of cisplatin to prevent cisplatin-induced hypomagnesemia (48). Most recently, a recent review by Duan supports magnesium administration to prevent AKI in elderly patients receiving cisplatin along with short hydration and amifostine (49).
Intravenous magnesium has been shown to be safe (50) and effective in multiple other medical conditions. It has been used to prevent AKI in contrast-induced nephropathy in primary percutaneous coronary intervention (51) and when administered intraoperatively with major laparoscopic abdominal surgery (52). Magnesium sulfate has been demonstrated to be more effective than anticonvulsants in acute eclampsia and reduces the risk of eclampsia by 50% in pre-eclampsia (41, 53). It has been used for status asthmaticus, torsades de pointes, and a higher concentration of magnesium has been correlated with better survival in chronic kidney disease (54). Lactate clearance has been shown to decrease in critically ill patients with severe sepsis with magnesium supplementation achieving a serum magnesium level near the upper limit of normal.
How exactly IV magnesium prevents AKI when given prior to cisplatin in humans is currently unknown and possibly involves numerous pathways as discussed previously. Although magnesium downregulated the OCT2 transporter and upregulated the MATE transporter, preventing AKI in rats, (55) this was not observed with acute exposure in recent experiments using cells expressing human OCT2 performed by Dr. Ciarimboli (see Figure 1 A–C). Therefore, further studies will be necessary to completely understand how magnesium prevents AKI in humans. Other drugs have demonstrated a downregulation of human OCT2 (hOCT2), protecting against AKI, such as carvedilol, (58) while metformin and cimetidine have been competitive substrates for hOCT2. Research has shown the renal protective effects of both of these agents from cisplatin toxicity (59, 60). However, two meta-analyses have both identified that IV magnesium prevents AKI from cisplatin and recommend it over all other agents at this time.
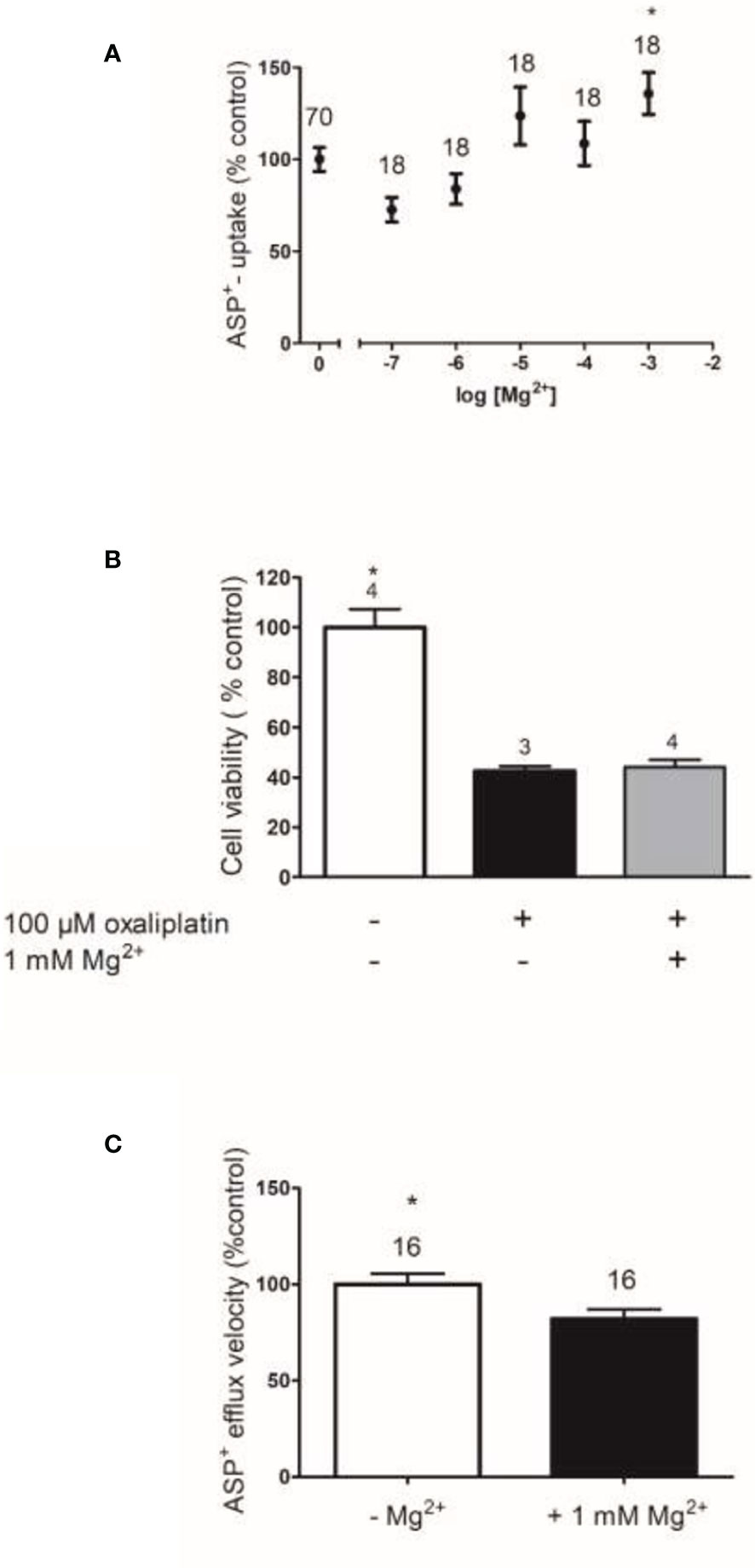
Figure 1 The effects of Mg2+ on hOCT2 function (A), on hOCT2-mediated Oxaliplatin toxicity (B), and on hMATE1 function (C). Function of the transporters was measured as uptake (hOCT2) or efflux (hMATE1) of the fluorescent organic cation 4-[4-(dimethylamino)styryl]-N-methylpyridinium (ASP+) as described in Wilde et al. (56) and Kantauskaite et al. (57) Panel (A) shows the changes of ASP+ uptake by hOCT2 stably expressed in Human Embryonic Kidney (HEK) cells in dependence from extracellular Mg2+ concentration compared to what was measured in Mg2+ absence (mean ± SEM). Only 1 mM Mg2+ significantly increased ASP+ uptake by hOCT2 (Kruskal–Wallis test with Dunn’s multiple comparison test). The presence of Mg2+ stimulates the activity of hOCT2, a transporter mediating nephrotoxicity of platinum derivatives, therefore regulation of hOCT2 by Mg2+ cannot explain Mg2+ protective effects against cisplatin nephrotoxicity. (B) shows the effects of Mg2+ supplementation (1 mM) on toxicity of 100 µM Oxaliplatin measured with a 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay in hOCT2 overexpressing HEK cells (mean ± SEM). The presence of 1 mM Mg2+ does not protect the cells against hOCT2-mediated Oxaliplatin toxicity. Finally, (C) shows the changes of ASP+ efflux by hMATE1 stably expressed in HEK cells in dependence from extracellular Mg2+ concentration compared to what measured in Mg2+ absence (mean ± SEM). The extracellular presence of 1 mM Mg2+ slightly but significantly decreases the function of hMATE1 (Mann–Whitney-test), which is an efflux transporter for platinum derivatives. Therefore, also a regulation of hMATE1 by Mg2+ cannot explain Mg2+ protective effects against cisplatin nephrotoxicity. In (A, C) the numbers above the columns represent the number of replicates measured in at least three independent experiments. In (B) they represent the number of independent experiments.
Conclusion
Currently, there is no dispute regarding the renal toxicity associated with cisplatin. AKI, based on elevation of serum creatinine or decreased urine output, occurs in approximately one-third of all patients receiving cisplatin. Hypomagnesemia occurs in 40–100% of patients following cisplatin and may persist long after chemotherapy completion, reflecting irreversible cisplatin-mediated kidney damage. What has been controversial is the administration of IV magnesium prior to each dose of cisplatin, rather than after inevitable hypomagnesemia is subsequently identified. Compelling recent reviews of human trials and animal studies clearly support the pre-administration of IV magnesium for ameliorating both AKI and hypomagnesemia. Acute cisplatin-induced nephrotoxicity (including AKI and hypomagnesemia) may cause persistent and irreversible kidney impairment, resulting in further health complications.
Hesitancy regarding IV magnesium prior to cisplatin may have originated from the early termination of the Combined Oxaliplatin Neurotoxicity Prevention (CONcePT) in 2007, in which calcium/magnesium was infused before oxaliplatin chemotherapy for colon cancer to prevent neurotoxicity. Although initial data suggested a 52% reduction in oxaliplatin’s killing efficacy following calcium/magnesium administration, (61) this was subsequently reversed in 2008 and Wu, in 2012, published a systematic review concluding that IV calcium/magnesium does not impair oxaliplatin effectiveness (56). In addition, there has been no evidence in any of the trials analyzed that magnesium affected the chemotherapeutic effect of cisplatin, and a higher magnesium level actually potentiated cisplatin chemotherapeutic effect in mice (40). Finally, the OCT2 transporter that is involved in the cisplatin/oxaliplatin uptake and subsequent AKI has not been identified in tumors.
This case report along with supporting documentation provided by both clinical and pre-clinical studies clearly demonstrate the effectiveness of IV magnesium before cisplatin in preventing acute kidney injury manifested by oliguria. We recommend that at least 2 g of magnesium be administered prior to cisplatin since a recent study by Uhm found that 1 g still resulted in 33% of patients developing hypomagnesium (57), while a study by Hase supported the use of 20 mEq/L or approximately 2.5 g. (62)
Therefore, if we are to follow our oath to do no harm, it is imperative that IV magnesium administration with cisplatin become a “best practice” guideline at all oncology centers.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics Statement
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
MM: concept for paper and case report. AH: review of human studies and comparison of recent meta-analyses, and development of table comparing these. CM: editing and review of paper. YS: review of renal receptors and effect of magnesium on them. CNM: summary of research in animals and editing of manuscript. SE: assistance in experiments using magnesium with human renal transporters GC: development and analysis of experiments using magnesium with human renal transporters. All authors contributed to the article and approved the submitted version.
Funding
Source for funding: Medical Research Fund Community Foundation of Washington County, Inc 37 S. Potomac Street Hagerstown, MD 21740.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Dasari S, Bernard Tchounwou P. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur J Pharmacol (2014) 740:364–78. doi: 10.1016/j.ejphar.2014.07.025
2. Manohar S, Leung N. Cisplatin Nephrotoxicity: A Review of the Literature. J Nephrol (2018) 31(1):15–25. doi: 10.1007/s40620-017-0392-z
3. Crona DJ, Faso A, Nishijima TF, McGraw KA, Galsky MD, Milowsky MI. A Systematic Review of Strategies to Prevent Cisplatin-Induced Nephrotoxicity. Oncologist (2017). doi: 10.1634/theoncologist.2016-0319
4. Madias NE, Harrington JT. Platinum nephrotoxicity. Am J Med (1978) 65(2):307–14. doi: 10.1016/0002-9343(78)90825-2
5. Ishitsuka R, Miyazaki J, Ichioka D, Inoue T, Kageyama S, Sugimoto M, et al. Impact of acute kidney injury defined by CTCAE v4.0 during first course of cisplatin-based chemotherapy on treatment outcomes in advanced urothelial cancer patients. Clin Exp Nephrol (2017) 21(4):732–40. doi: 10.1007/s10157-016-1327-z
6. Volarevic V, Djokovic B, Jankovic MG, Harrell CR, Fellabaum C, Djonov V, et al. Molecular mechanisms of cisplatin-induced nephrotoxicity: A balance on the knife edge between renoprotection and tumor toxicity. J BioMed Sci (2019) 26(1):25. doi: 10.1186/s12929-019-0518-9
7. Yao X, Panichpisal K, Kurtzman N, Nugent K. Cisplatin nephrotoxicity: A review. Am J Med Sci (2007) 334(2):115–24. doi: 10.1097/MAJ.0b013e31812dfe1e
8. Launay-Vacher V, Rey JB, Isnard-Bagnis C, Deray G, Daouphars M. Prevention of cisplatin nephrotoxicity: State of the art and recommendations from the European Society of Clinical Pharmacy Special Interest Group on Cancer Care. Cancer Chemother Pharmacol (2008). doi: 10.1007/s00280-008-0711-0
9. Vokes EE, Mick R, Vogelzang NJ, Geiser R, Douglas F. A randomised study comparing intermittent to continuous administration of magnesium aspartate hydrochloride in cisplatin-induced hypomagnesaemia. Br J Cancer (1990). doi: 10.1038/bjc.1990.429
11. Kimura T, Ozawa T, Hanai N, Hirakawa H, Suzuki H, Hosoi H, et al. Renal protective effect of a hydration supplemented with magnesium in patients receiving cisplatin for head and neck cancer. J Otolaryngol - Head Neck Surg (2018) 47(1):10. doi: 10.1186/s40463-018-0261-3
12. Oka T, Kimura T, Suzumura T, et al. Magnesium supplementation and high volume hydration reduce the renal toxicity caused by cisplatin-based chemotherapy in patients with lung cancer: A toxicity study. BMC Pharmacol Toxicol (2014). doi: 10.1186/2050-6511-15-70
13. Kidera Y, Kawakami H, Sakiyama T, et al. Risk factors for cisplatin-induced nephrotoxicity and potential of magnesium supplementation for renal protection. PloS One (2014). doi: 10.1371/journal.pone.0101902
14. Muraki K, Koyama R, Honma Y, et al. Hydration with magnesium and mannitol without furosemide prevents the nephrotoxicity induced by cisplatin and pemetrexed in patients with advanced non-small cell lung cancer. J Thorac Dis (2012). doi: 10.3978/j.issn.2072-1439.2012.10.16
15. Matsui M, Saito Y, Yamaoka S, Yokokawa Y, Morikawa Y, Makimoto A, et al. Kidney-protective effect of magnesium supplementation in cisplatin-containing chemotherapy for pediatric cancer: A retrospective study. J Pediatr Hematol Oncol (2018) 40(5):379–81. doi: 10.1097/MPH.0000000000001159
16. Grašič Kuhar C, Strojan P, Zadnik V, Zakotnik B. Importance of magnesium sulfate supplementation in the prevention of hypomagnesemia and hypocalcemia during chemoradiation in head and neck cancer. J Trace Elem Med Biol (2018) 50:327–31. doi: 10.1016/j.jtemb.2018.07.012
17. Solanki MH, Chatterjee PK, Gupta M, Xue X, Plagov A, Metz MH, et al. Magnesium protects against cisplatin-induced acute kidney injury by regulating platinum accumulation. Am J Physiol - Ren Physiol (2014) 307(4):F369–84. doi: 10.1152/ajprenal.00127.2014
18. Silver SA, Harel Z, McArthur E, Nash DM, Acedillo R, Kitchlu A, et al. Causes of death after a hospitalization with AKI. J Am Soc Nephrol (2018) 29(3):1001–10. doi: 10.1681/ASN.2017080882
19. Bhat ZY, Cadnapaphornchai P, Ginsburg K, et al. Understanding the risk factors and long- term consequences of cisplatin-associated acute kidney injury: An observational cohort study. PloS One (2015). doi: 10.1371/journal.pone.0142225
20. De Jongh FE, Van Veen RN, Veltman SJ, de Wit R, van der Burg MEL, van den Bent MJ, et al. Weekly high-dose cisplatin is a feasible treatment option: Analysis on prognostic factors for toxicity in 400 patients. Br J Cancer (2003) 88(8):1199–206. doi: 10.1038/sj.bjc.6600884
21. Townsend DM, Deng M, Zhang L, Lapus MG, Hanigan MH. Metabolism of cisplatin to a nephrotoxin in proximal tubule cells. J Am Soc Nephrol (2003) 14(1):1–10. doi: 10.1097/01.ASN.0000042803.28024.92
22. Reece PA, Stafford I, Russell J, Gill PG. Nonlinear renal clearance of ultrafilterable platinum in patients treated with cis-dichlorodiammineplatinum (II). Cancer Chemother Pharmacol (1985) 15(3):295–9. doi: 10.1007/BF00263904
23. Ciarimboli G, Ludwig T, Lang D, Gill PG. Cisplatin nephrotoxicity is critically mediated via the human organic cation transporter 2. Am J Pathol (2005) 15(3):295–9. doi: 10.1016/S0002-9440(10)61234-5
24. Motohashi H, Sakurai Y, Saito H, Masuda S, Urakami Y, Goto M, et al. Gene expression levels and immunolocalization of organic ion transporters in the human kidney. J Am Soc Nephrol (2002) 13(4):866–74.
25. Holzer AK, Varki NM, Le QT, Gibson MA, Naredi P, Howell SB. Expression of the human copper influx transporter 1 in normal and malignant human tissues. J Histochem Cytochem (2006) 54(9):1041–9. doi: 10.1369/jhc.6A6970.2006
26. Martinho N, Santos TCB, Florindo HF, Silva LC. Cisplatin-membrane interactions and their influence on platinum complexes activity and toxicity. Front Physiol (2019). doi: 10.3389/fphys.2018.01898
27. Kuhlmann MK, Burkhardt G, Köhler H. Insights into potential cellular mechanisms of cisplatin nephrotoxicity and their clinical application. Nephrol Dial Transplant (1997) 12(12):2478–80. doi: 10.1093/ndt/12.12.2478
28. Oh GS, Kim HJ, Shen AH, Lee SB, Khadka D, Pandit A, et al. Cisplatin-induced kidney dysfunction and perspectives on improving treatment strategies. Electrolyte Blood Press (2014) 12(2):55–65. doi: 10.5049/EBP.2014.12.2.55
29. Bunel V, Tournay Y, Baudoux T, et al. Early detection of acute cisplatin nephrotoxicity: Interest of urinary monitoring of proximal tubular biomarkers. Clin Kidney J (2017). doi: 10.1093/ckj/sfx007
30. Casanova AG, Hernández-Sánchez MT, López-Hernández FJ, et al. Systematic review and meta-analysis of the efficacy of clinically tested protectants of cisplatin nephrotoxicity. Eur J Clin Pharmacol (2019). doi: 10.1007/s00228-019-02771-5
31. Hamroun A, Lenain R, Bigna JJ, et al. Prevention of Cisplatin-Induced Acute Kidney Injury: A Systematic Review and Meta-Analysis. Drugs (2019). doi: 10.1007/s40265-019-01182-1
32. Mizuno T, Sato W, Ishikawa K, Shinjo H, Miyagawa Y, Noda Y, et al. KDIGO (Kidney Disease: Improving Global Outcomes) criteria could be a useful outcome predictor of cisplatin-induced acute kidney injury. Oncol (2012) 82(6):354–9. doi: 10.1159/000338664
33. Filipski KK, Mathijssen RH, Mikkelsen TS, Schinkel AH, Sparreboom A. Contribution of organic cation transporter 2 (OCT2) to cisplatin-induced nephrotoxicity. Clin Pharmacol Ther (2009) 86(4):396–402. doi: 10.1038/clpt.2009.139
34. Franke RM, Kosloske AM, Lancaster CS, Filipski KK, Hu C, Zolk O, et al. Influence of Oct1/Oct2-deficiency on cisplatin-induced changes in urinary N-acetyl-β-D-glucosaminidase. Clin Cancer Res (2010) 16(16):4198–206. doi: 10.1158/1078-0432.CCR-10-0949
35. Miller RP, Tadagavadi RK, Ramesh G, Reeves WB. Mechanisms of cisplatin nephrotoxicity. Toxins (Basel) (2010) 2(11):2490–518. doi: 10.3390/toxins2112490
36. Peres LAB, da Cunha AD Jr. Acute nephrotoxicity of cisplatin: molecular mechanisms. J Bras Nefrol ʹorgão Of Soc Bras e Latino-Americana Nefrol (2013). doi: 10.5935/0101-2800.20130052
37. Yokoo K, Murakami R, Matsuzaki T, Yoshitom K, Hamada A, Saito H. Enhanced renal accumulation of cisplatin via renal organic cation transporter deteriorates acute kidney injury in hypomagnesemic rats. Clin Exp Nephrol (2009). doi: 10.1007/s10157-009-0215-1
38. Van Angelen AA, Glaudemans B, Van Der Kemp AWCM, Hoenderop JGJ, Bindels RJM. Cisplatin-induced injury of the renal distal convoluted tubule is associated with hypomagnesaemia in mice. Nephrol Dial Transplant (2013) 28(4):879–89. doi: 10.1093/ndt/gfs499
39. Solanki MH, Chatterjee PK, Xue X, Gupta M, Rosales I, yeboah MM, et al. Magnesium protects against cisplatin-induced acute kidney injury without compromising cisplatin-mediated killing of an ovarian tumor xenograft in mice. Am J Physiol Physiol (2015) 309(1):F35–47. doi: 10.1152/ajprenal.00096.2015
40. Kumar G, Solanki MH, Xue X, et al. Magnesium improves cisplatin-mediated tumor killing while protecting against cisplatin-induced nephrotoxicity. Am J Physiol - Ren Physiol (2017). doi: 10.1152/ajprenal.00688.2016
42. Jahnen-Dechent W, Ketteler M. Magnesium basics. CKJ Clin Kidney J (2012). doi: 10.1093/ndtplus/sfr163
43. Fox C, Ramsoomair D, Carter C. Magnesium: Its proven and potential clinical significance. South Med J (2001). doi: 10.1097/00007611-200112000-00013
44. Fawcett WJ, Haxby EJ, Male DA. Magnesium: Physiology and pharmacology. Br J Anaesth (1999). doi: 10.1093/bja/83.2.302
45. Schilsky RL, Anderson T. Hypomagnesemia and renal magnesium wasting in patients receiving cisplatin. Ann Intern Med (1979) 8(3):164–9. doi: 10.7326/0003-4819-90-6-929
46. Lajer H, Kristensen M, Hansen HH, Nielsen S, Frøkiaer J, Ostergaard LF, et al. Magnesium depletion enhances cisplatin-induced nephrotoxicity. Cancer Chemother Pharmacol (2005) 56(5):535–42. doi: 10.1007/s00280-005-1010-7
47. Martin M, Diaz-Rubio E, Casado A, Vega JML, Sastre J, Almenarez J. Intravenous and oral magnesium supplementations in the prophylaxis of cisplatin-induced hypomagnesemia: Results of a controlled trial. Am J Clin Oncol Cancer Clin Trials (1992) 15(4):348–51. doi: 10.1097/00000421-199208000-00016
48. Hodgkinson E, Neville-Webbe HL, Coleman RE. Magnesium Depletion in Patients Receiving Cisplatin-based Chemotherapy. Clin Oncol (2006). doi: 10.1016/j.clon.2006.06.011
49. Duan ZY, Cai GY, Li JJ, Chen XM. Cisplatin-induced renal toxicity in elderly people. Ther Adv Med Oncol (2020). doi: 10.1177/1758835920923430
50. Lewis J. Intravenous infusion of magnesium sulfate is not associated with cardiovascular, liver, kidney, and metabolic toxicity in adults. J Clin Transl Res (2018) 4(1):47–55. doi: 10.18053/jctres.04.201801.002
51. Firouzi A, Maadani M, Kiani R, Shakerian F, Shakerian HR, Zahedmehr A, et al. Intravenous magnesium sulfate: new method in prevention of contrast-induced nephropathy in primary percutaneous coronary intervention. Int Urol Nephrol (2015) 47(3):521–5. doi: 10.1007/s11255-014-0890-z
52. Oh TK, Oh AY, Ryu JH, Koo BW, Lee YJ, Do SH. Retrospective analysis of the association between intraoperative magnesium sulfate infusion and postoperative acute kidney injury after major laparoscopic abdominal surgery. Sci Rep (2019) 9(1):2833. doi: 10.1038/s41598-019-39106-4
53. Euser AG, Cipolla MJ. Magnesium sulfate for the treatment of eclampsia a brief review. Stroke (2009). doi: 10.1161/STROKEAHA.108.527788
54. Leenders NHJ, Vervloet MG. Magnesium: A magic bullet for cardiovascular disease in chronic kidney disease? Nutrients (2019). doi: 10.3390/nu11020455
55. Saito Y, Okamoto K, Kobayashi M, Narumi K, Yamada T, Iseki K. Magnesium attenuates cisplatin-induced nephrotoxicity by regulating the expression of renal transporters. Eur J Pharmacol (2017). doi: 10.1016/j.ejphar.2017.05.034
56. Wu Z, Ouyang J, He Z, Zhang S. Infusion of calcium and magnesium for oxaliplatin-induced sensory neurotoxicity in colorectal cancer: A systematic review and meta-analysis. Eur J Cancer (2012). doi: 10.1016/j.ejca.2012.03.018
57. Uhm SJ, Meszaros E, Hammonds K, Patel I, Herrington JD. Characterizing the impact of magnesium and potassium-supplemented hydration with cisplatin and the subsequent electrolyte replacement requirements. J Oncol Pharm Pract (2020) 6:23975. doi: 10.1177/1078155220948590
58. Guo D, Yang H, Li Q, Bae HJ, Obianom O, Zeng S, et al. Selective Inhibition on Organic Cation Transporters by Carvedilol Protects Mice from Cisplatin-Induced Nephrotoxicity. Pharm Res (2018) 35(11):204. doi: 10.1007/s11095-018-2486-2
59. Li J, Gui Y, Ren J, et al. Metformin protects against cisplatin-induced tubular cell apoptosis and acute kidney injury via AMPKα-regulated autophagy induction. Sci Rep (2016). doi: 10.1038/srep23975
60. Katsuda H, Yamashita M, Katsura H, Yu J, Waki Y, Nagata N, et al. Protecting cisplatin-induced nephrotoxicity with cimetidine does not affect antitumor activity. Biol Pharm Bull (2010) 33(11):1867–71. doi: 10.1248/bpb.33.1867
61. Hochster HS, Grothey A, Childs BH. Use of calcium and magnesium salts to reduce oxaliplatin-related neurotoxicity [10]. J Clin Oncol (2007) 1078155220948590. doi: 10.1200/JCO.2007.13.5251
Keywords: intravenous magnesium, cisplatin, acute kidney damage, oliguria, hypomagnesemia, nephrotoxicity, ovarian cancer, intra-peritoneal chemotherapy
Citation: Money ME, Hamroun A, Shu Y, Matthews C, Ahmed Eltayeb S, Ciarimboli G and Metz CN (2021) Case Report and Supporting Documentation: Acute Kidney Injury Manifested as Oliguria Is Reduced by Intravenous Magnesium Before Cisplatin. Front. Oncol. 11:607574. doi: 10.3389/fonc.2021.607574
Received: 17 September 2020; Accepted: 22 January 2021;
Published: 26 February 2021.
Edited by:
David A. Gewirtz, Virginia Commonwealth University, United StatesReviewed by:
Kameswaran Ravichandran, University of Colorado Denver, United StatesDenis Soulieres, University of Montreal Hospital Centre (CRCHUM), Canada
Copyright © 2021 Money, Hamroun, Shu, Matthews, Ahmed Eltayeb, Ciarimboli and Metz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mary Elizabeth Money, ZHIubS5lLm1vbmV5QGdtYWlsLmNvbQ==