
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 06 May 2021
Sec. Thoracic Oncology
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.602924
This article is part of the Research TopicTherapeutic Strategies in EGFR Mutant Lung CancerView all 26 articles
 Maria Gabriela O. Fernandes1,2,3*†
Maria Gabriela O. Fernandes1,2,3*† Catarina Sousa1†
Catarina Sousa1† Maria Jacob1Leonor Almeida1
Maria Jacob1Leonor Almeida1 Vanessa Santos1
Vanessa Santos1 David Araújo1Hélder Novais Bastos1,2,4Adriana Magalhães1Luís Cirnes3,5Conceição Souto Moura6
David Araújo1Hélder Novais Bastos1,2,4Adriana Magalhães1Luís Cirnes3,5Conceição Souto Moura6 Henrique Queiroga1,2
Henrique Queiroga1,2 Natália Cruz-Martins2,4,7Venceslau Hespanhol1,2,3
Natália Cruz-Martins2,4,7Venceslau Hespanhol1,2,3Background: Osimertinib efficacy in pre-treated patients with epidermal growth factor receptor (EGFR) T790M-mutated non-small cell lung cancer (NSCLC) has been demonstrated in clinical trials, but real-world data, particularly regarding resistance profile, remains limited. This study aims to analyze the resistance mechanisms acquired after treatment with Osimertinib.
Methods: Clinical outcomes and molecular results from re-biopsies at the time of osimertinib progression of EGFR T790M-mutated NSCLC patient were analyzed.
Results: Twenty-one patients with stage IV adenocarcinoma were included [median 69 years; 57.1% female; 85.7% never-smokers; 23.8% ECOG performance status (PS) ≥2]. Median PFS and OS were 13.4 (95% CI: 8.0–18.9) and 26.4 (95% IC: 8.9–43.8) months, respectively. At the time of analysis, 10 patients had tumor progression (47.6%). T790M loss occurred in 50%, being associated with earlier progression (median PFS 8.1 vs. 21.4 months, p = 0.011). Diverse molecular alterations were identified, including C797S mutation (n = 1), PIK3CA mutation (n = 2), MET amplification (n = 1), CTNNB1 mutation (n = 1), and DCTN1-ALK fusion (n = 1). Histological transformation into small cell carcinoma occurred in one patient.
Conclusions: This real-world life study highlights the relevance of re-biopsy at the time of disease progression, contributing to understand resistance mechanisms and to guide treatment strategies.
Patients with advanced non-small-cell lung cancer (NSCLC) with activating mutations in the epidermal growth factor receptor (EGFR) gene are eligible for EGFR tyrosine kinase inhibitors (TKIs). Despite the high response rates to first-line TKIs and a median progression-free survival (PFS) of 10–14 months (1–8), the disease ultimately progresses. In about 50–60% of patients, the acquired mechanism of resistance to first-line TKIs is a p.Thr790Met point mutation (T790M) in the EGFR gene. This mutation increases the receptor affinity for ATP binding, drastically reducing the drug activity (9–12).
Osimertinib is an irreversible EGFR-TKI that is selective for both EGFR and T790M resistance mutations (13). In the Phase III AURA3 trial (AZD9291 vs. Platinum-Based Doublet-Chemotherapy in Locally Advanced or Metastatic Non-Small Cell Lung Cancer), osimertinib was superior to platinum therapy plus pemetrexed in patients with T790M whom the disease progressed during first-line EGFR-TKI therapy with a median PFS of 10.1 months, and objective response rate (ORR) of 71% (14). Moreover, osimertinib had significant efficacy in patients with central nervous system (CNS) metastases (15). Recently, in the Phase III FLAURA trial (AZD9291 vs. Gefitinib or Erlotinib in Patients With Locally Advanced or Metastatic Non-small Cell Lung Cancer), Osimertinib was also superior in first-line (16).
Despite the survival data and response rates for osimertinib, acquired resistance, unfortunately, occurs after about 10 months (17). The mechanisms that determine disease progression are heterogeneous and not fully understood, including on-target EGFR-dependent and off-target independent mechanisms. EGFR-dependent mechanisms include new tertiary mutations, like the exon 20 C797S mutation, EGFR amplification or T790M disappearance. EGFR independent mechanisms can occur with bypass pathway activation, such as erb-b2 receptor tyrosine kinase 2 (HER2) and MET amplification, PIK3CA activating mutations, PTEN deletion, RAS mutations, fusions affecting anaplastic lymphoma kinase (ALK), and RET and others. There is also the possibility of phenotypic alteration, such as the transformation in small-cell lung cancer (SCLC) (18–20).
Treatment approaches for patients progressing from third-generation EGFR TKIs have not been clearly established. However, in case of disease progression without targeted therapy available, chemotherapy is still indicated and maintaining osimertinib beyond progression, with or without adjunctive radiotherapy, can be a useful option (21, 22). Although, a considerable amount of data is published on 3rd generation EGFR-TKIs, real-world data is limited. In this sense, this study aims to analyze the resistance profile of Osimertinib in a T790M EGFR-mutated population.
A retrospective analysis of T790M-mutated NSCLC patients treated with osimertinib, at the Centro Hospitalar e Universitário de São João (CHUSJ), Porto, Portugal, was performed. This study was conducted under the Declaration of Helsinki and was approved by the Ethics Committee of CHUSJ (243/20).
Eligible patients were required to have histologically confirmed stage IV NSCLC (based on TNM staging AJCC 8th edition), with an activating EGFR mutation, treated with osimertinib after progression with at least one 1st or 2nd generation TKI and with confirmed EGFR T790M mutation identified by re-biopsy at the time of progression. Patients initiated osimertinib between August 2016 and April 2019. Last data analysis was performed on 30 April 2020.
Patient demographics and clinical features, tumor histology, disease stage, lines of treatment received before osimertinib, and pattern of progression were recorded.
Molecular analyses from initial biopsies and re-biopsies at osimertinib progression were reviewed. Digital protein chain reaction (PCR) was used for EGFR T790M detection, and next-generation sequencing (NGS) at the time of progression was performed using a validated amplicon-based NGS (OncomineTM Focus Assay, ThermoFisher). These assays allow the analysis of targeted regions in EGFR, KRAS, NRAS, BRAF, MET, HER2, HER4, PIK3CA, and ALK genes plus the detection of ALK, ROS1, RET and NTRK (1, 2, and 3) gene fusions.
Most analysis was descriptive. Categorical variables are presented as relative frequencies and percentages, and continuous variables as median, interquartile range (IQR) and minimum and maximum values. Kaplan-Meier actuarial curves analysis was used to estimate OS, PFS and time to treatment discontinuation (TTD) for the entire cohort. Group comparisons were performed using the Mann-Whitney test. The significance level assumed was 0.05. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, IBM Corp, Chicago, IL, USA) software, version 25.0.
Twenty-one patients treated with osimertinib were included (Table 1), with median age of 69 (range 39–84) years, 12 (57.1%) were female, mostly never-smokers (n = 18; 85.7%). Of note, 13 (61.9%) patients were ≥65 years, and 5 (23.8%) had an ECOG performance status (PS) ≥2. All patients were diagnosed with stage IV adenocarcinoma [IVA n = 9 (42.9%); IVB n = 12 (57.1%)]. Exon 19 deletion and exon 21 L858R mutations were present, at initial biopsy, in 17 (85%) and 3 (15%) cases, respectively. The T790M mutation was detected by tissue biopsy in eight (38.1%), liquid biopsy in five (23.8%), and by both in 8 (38.1%) patients. Osimertinib was given as 2nd line treatment in 13 cases (61.9%), after a 1st or 2nd generation EGFR-TKI, and in 3rd or more line in eight cases (38.1%). The best ORR was 52.7% (nine partial responses; one complete response) and DCR 89.5% (seven with stable disease), respectively. Median PFS was 13.4 (95% CI: 8.0–18.9) months (Figure 1A). Of the 17 cases with an objective response/disease control, 10 subsequently progressed and underwent re-biopsy. There were eight patients with oligo-progression (80%) and two with systemic progression (20%). The main sites of progression were bone (n = 4), lung (n = 4), pleura (n = 2), CNS (n = 1), and liver (n = 1). Thirteen (61.9%) patients died, with a median OS since osimertinib initiation of 26.4 months (95% IC: 8.9–43.8) (Figure 1B).
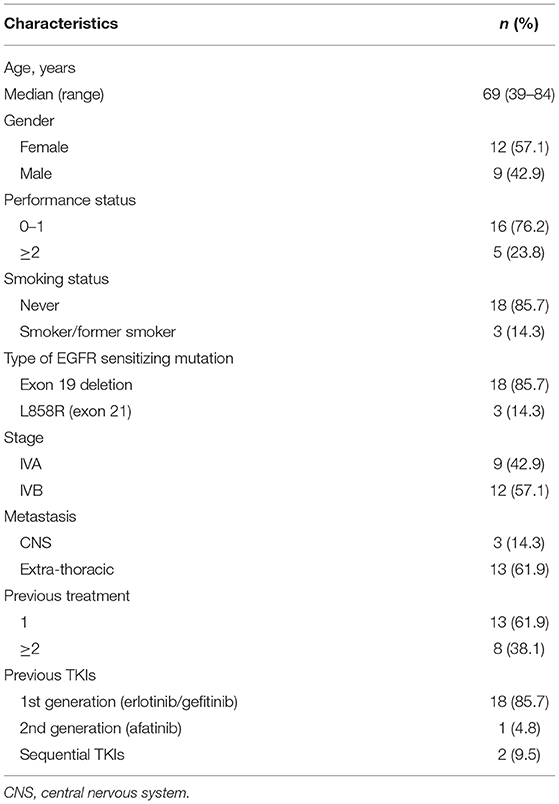
Table 1. Baseline patients' characteristics.
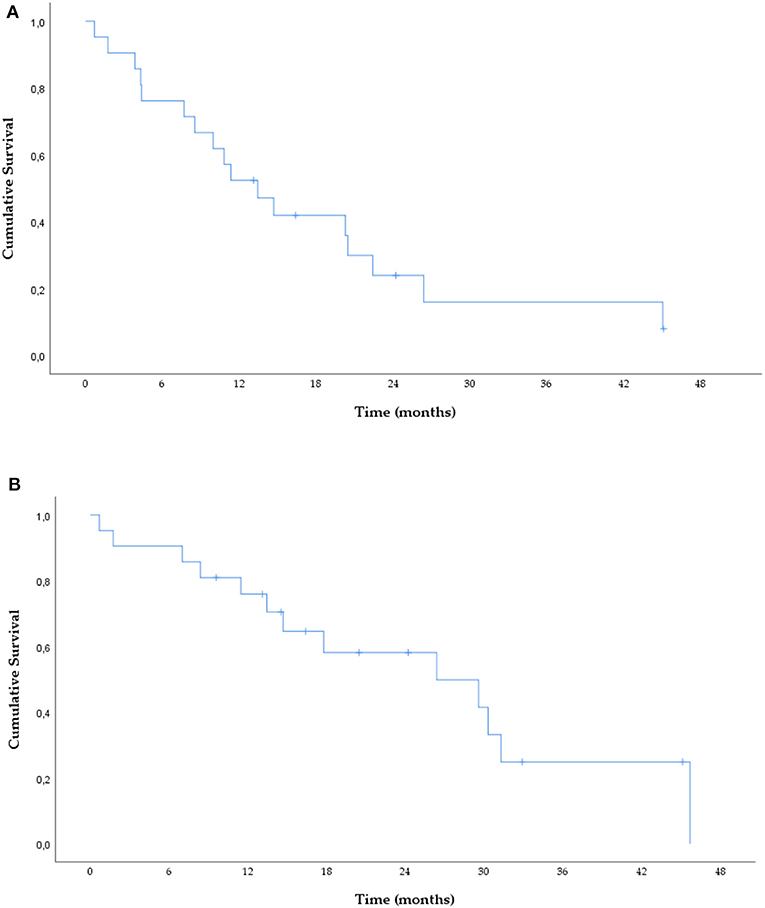
Figure 1. PFS (A) and OS (B) under osimertinib treatment.
Osimertinib was well-tolerated, with only two cases reporting grade ≥3 AE, corresponding to pneumonitis resolved with definite discontinuation (9.5%) and corticosteroids treatment.
At the time of analysis, 10 patients had tumor progression (47.6%), and the resistance profile is summarized in Figure 2 and Table 2.
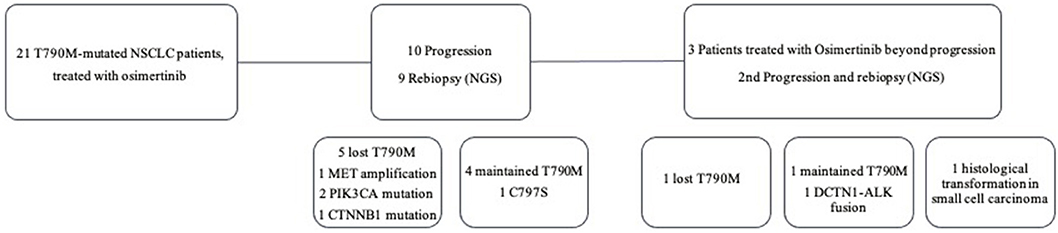
Figure 2. Treatment and resistance profile of NSCLC patients post-osimertinib progression.
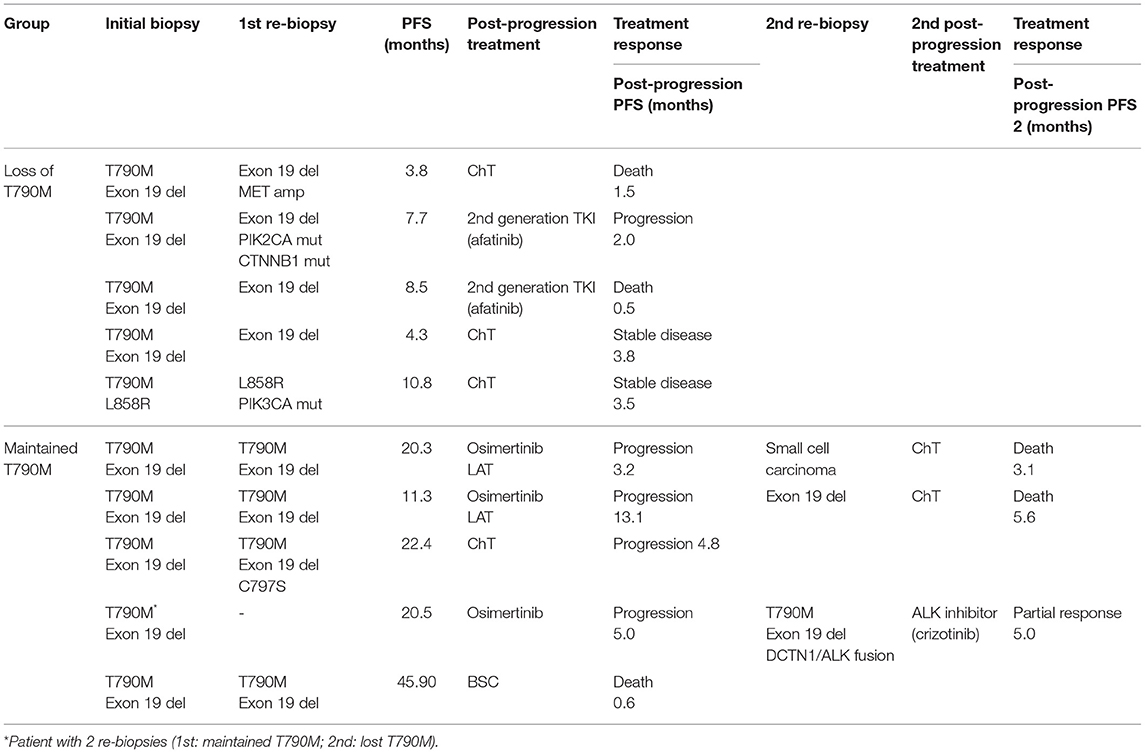
Table 2. Resistance profile of osimertinib.
A total of 12 re-biopsies were analyzed among the 10 patients who progressed (Figure 2). Molecular testing was performed in all cases, 10 on tissue biopsy (83.3%), including 8 computed tomography (CT)-guided percutaneous core needle biopsy (PCNB), one ultrasound-guided liver biopsy and one CT-guided soft tissue biopsy, and two (16.7%) on liquid biopsy. The patients that performed liquid biopsy presented no clinical conditions for tissue biopsy (n = 1) or inaccessible disease (n = 1).
T790M mutation loss occurred in 50% of cases (n = 6), but other molecular changes were also found among this group, including PIK3CA mutation (n = 2), MET amplification (n = 1), and CTNNB1 mutation (n = 1). In the T790M-persistent group, a patient presented a newly exon 20 C797S mutation and another a DCTN1-ALK fusion (n = 1). Histological transformation in SCLC occurred in one patient.
T790M mutation loss was associated with earlier progression [PFS: median 8.1 (range: 3.8–11.3) vs. 21.4 months (range: 20.3–45.0), p = 0.011] and worse OS [median 13.0 (range: 7.0–30.3) vs. 32.1 months (range: 29.6–45.7), p = 0.019].
Of the 10 progressing patients, nine received at least one subsequent treatment, three received osimertinib beyond progression (33.3%), two of them in association with local ablative treatment (LAT), and six initiated a new treatment line [ChT (n = 4); another EGFR-TKI (n = 2)]. One patient received best supportive care (BSC). The patient with DCTN1-ALK fusion started crizotinib, presenting a partial response at the 3-month CT evaluation. The three patients who received osimertinib beyond progression had a new re-biopsy at the time of 2nd progression (Figure 2), and all received a new treatment line (2 ChT). The median post-progression PFS (ppPFS) was 5.0 months (range: 3.2–13.1; all cases with progression). The ppPFS of those who received a new treatment line was 2.7 months (range: 0.5–4.8; 2 cases without progression), p = 0.12.
Randomized controlled trials are the gold standard in clinical research. Still, real-world data is essential to verify the effectiveness, safety, application of treatment in the general population and to understand the patient's evolution in daily clinical practice. This is the first report of osimertinib in pre-treated EGFR T790M-mutated NSCLC patients in our population, focusing on the resistance mechanisms, and progression profile.
Identifying the resistance profile is critical in selecting the appropriate treatment after osimertinib, as several biological mechanisms of acquired resistance have been identified. To fully capture the diversity of resistance mechanisms is essential to repeat a biopsy to obtain the best possible sample that harbors the alteration responsible for progression with the less invasive and safer technique. However, obtaining tissue samples from patients experiencing progressive disease after EGFR-TKI failure remains a challenge. Rate of patients submitted to re-biopsy ranges from 50 to 60% in different series (23–25). With the analysis of circulating tumor DNA (ctDNA), liquid biopsy is a promising technique considering its invasiveness, repeatability, and accessibility. Some studies proved the role of ctDNA based assays to detect EGFR activations mutations and the T790M. In the osimertinib progression setting, in AURA3 trial, ctDNA genomic profile detected several resistance mechanisms, including MET amplification (26). Nevertheless, the use of cfDNA presents some limitations and challenges, especially considering the occurrence of false-negative results associated with the absence or low DNA of tumoral origin present on plasma or analytical limitations and to the difficulty to detect small cell-transformation. In the setting of EGFR progressive disease, both tissue and liquid assays, are complementary.
Comprehensive NGS panels help to define the genomic diversity of resistance mechanisms and are particularly important in this setting, where there is no single alteration to detect.
In this group, concerning osimertinib efficacy, ORR was 52.7%, median PFS 13.4 and median OS 26.4 months, similar to data from other real-world studies. All patients underwent a new biopsy at the time of progression, mainly tissue re-biopsy, and two liquid biopsies. All samples were evaluated with a targeted gene panel NGS.
We found that T790M mutation loss is common in Osimertinib-resistant cases (50%), consistent with previous studies (21, 27–30). Also, T790M mutation loss was associated with a shorter median PFS, which agrees with a previous study in which acquired resistance to osimertinib mediated by T790M mutation loss was associated with early progression, lower PFS and shorter TTD (28).
Molecular analyses from the AURA 3 trial revealed the presence of acquired EGFR mutations in 21% of patients, most commonly a new exon 20 point mutation C797S (14%) (26). In our series, only one patient acquired the C797S mutation. Most of the molecular alterations found were in EGFR-independent pathways, two PIK3CA mutation, one MET amplification, one CTNNB1 mutation, and one DCTN1-ALK fusion. In one patient occurred histological transformation into SCLC, a mechanism previously described in other studies (18, 20, 31).
Until today, no specific drug has been approved for the treatment of Osimertinib resistant patients, and a plethora of strategies are being explored. Rechallenge with 1st/2nd generation TKIS for C797S occurring in trans can be an option (32). Innumerous therapeutic combinations between osimertinib and antiangiogenics can be an option to overcome EGFR-dependent resistance mechanisms (33). Combination of Osimertinib and other inhibitors can help overcome resistance mediated through alternative kinase activation, as MET, MEK, and BRAF inhibitors (34–36). For most patients, platinum-based doublet chemotherapy is the only available option.
Regarding resistance to osimertinib, oligo-progression is frequent, being present in our series in more than 2/3 of patients. Schmid et al. (37) also reported this finding in 73% of cases. In this situation, LATs and osimertinib continuation beyond progression can be beneficial (37). In about one-third of cases, osimertinib treatment was continued beyond progression, with a longer ppPFS than patients who started a new treatment line, although not significant (5.0 vs. 2.0 months, p = 0.22). In the remaining cases, a new treatment line was started, mostly ChT. Two patients who lost the T790M and maintained the exon 19 deletion were treated with 2nd generation TKI afatinib, with a poor outcome. Crizotinib was initiated in a patient with DCTN1-ALK fusion with partial response.
Although, being a single center, retrospective study with small sample size, it illustrates the feasibility and relevance of performing re-biopsies, and NGS to study the resistance mechanisms at the time of progression, opening the window for new therapeutic strategies as demonstrated.
Re-biopsy at the time of disease progression is feasible outside clinical trials, being of extreme usefulness to understand the underlying resistance mechanisms, to guide treatment strategies and, consequently, contributing to increase patient's survival.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by CHUSJ (approval n° 243/20).
CS and MGOF: conceptualization and writing—original draft preparation. CS, MGOF, and NC-M: methodology. CS and NC-M: formal analysis. CS, MJ, and LA: investigation and data curation. CS, MGOF, MJ, LA, and NC-M: writing—review and editing. VH and HQ: supervision. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We acknowledge the work of the members of our thoracic oncology department, patients, and their relatives. NC-M acknowledges the Portuguese Foundation for Science and Technology under the Horizon 2020 Program (PTDC/PSI-GER/28076/2017).
1. Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. (2009) 361:947–57. doi: 10.1056/NEJMoa0810699
2. Hanna N, Johnson D, Temin S, Baker S Jr, Brahmer J, Ellis PM, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of clinical oncology clinical practice guideline update. J Clin Oncol. (2017) 35:3484–515. doi: 10.1200/JCO.2017.74.6065
3. Mitsudomi T, Morita S, Yatabe Y, Negoro S, Okamoto I, Tsurutani J, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. (2010) 11:121–8. doi: 10.1016/S1470-2045(09)70364-X
4. Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. (2011) 12:735–42. doi: 10.1016/S1470-2045(11)70184-X
5. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. (2012) 13:239–46. doi: 10.1016/S1470-2045(11)70393-X
6. Sequist LV, Yang JC, Yamamoto N, O'Byrne K, Hirsh V, Mok T, et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol. (2013) 31:3327–34. doi: 10.1200/JCO.2012.44.2806
7. Wu YL, Zhou C, Hu CP, Feng J, Lu S, Huang Y, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol. (2014) 15:213–22. doi: 10.1016/S1470-2045(13)70604-1
8. Wu YL, Zhou C, Liam CK, Wu G, Liu X, Zhong Z, et al. First-line erlotinib versus gemcitabine/cisplatin in patients with advanced EGFR mutation-positive non-small-cell lung cancer: analyses from the phase III, randomized, open-label, ENSURE study. Ann Oncol. (2015) 26:1883–9. doi: 10.1093/annonc/mdv270
9. Arcila ME, Oxnard GR, Nafa K, Riely GJ, Solomon SB, Zakowski MF, et al. Rebiopsy of lung cancer patients with acquired resistance to EGFR inhibitors and enhanced detection of the T790M mutation using a locked nucleic acid-based assay. Clin Cancer Res. (2011) 17:1169–80. doi: 10.1158/1078-0432.CCR-10-2277
10. Oxnard GR, Arcila ME, Sima CS, Riely GJ, Chmielecki J, Kris MG, et al. Acquired resistance to EGFR tyrosine kinase inhibitors in EGFR-mutant lung cancer: distinct natural history of patients with tumors harboring the T790M mutation. Clin Cancer Res. (2011) 17:1616–22. doi: 10.1158/1078-0432.CCR-10-2692
11. Sun JM, Ahn MJ, Choi YL, Ahn JS, Park K. Clinical implications of T790M mutation in patients with acquired resistance to EGFR tyrosine kinase inhibitors. Lung Cancer. (2013) 82:294–8. doi: 10.1016/j.lungcan.2013.08.023
12. Yu HA, Arcila ME, Rekhtman N, Sima CS, Zakowski MF, Pao W, et al. Analysis of tumor specimens at the time of acquired resistance to EGFR-TKI therapy in 155 patients with EGFR-mutant lung cancers. Clin Cancer Res. (2013) 19:2240–7. doi: 10.1158/1078-0432.CCR-12-2246
13. Cross DA, Ashton SE, Ghiorghiu S, Eberlein C, Nebhan CA, Spitzler PJ, et al. AZD9291, an irreversible EGFR TKI, overcomes T790M-mediated resistance to EGFR inhibitors in lung cancer. Cancer Discov. (2014) 4:1046–61. doi: 10.1158/2159-8290.CD-14-0337
14. Mok TS, Wu YL, Ahn MJ, Garassino MC, Kim HR, Ramalingam SS, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med. (2017) 376:629–40. doi: 10.1056/NEJMoa1612674
15. Wu YL, Ahn MJ, Garassino MC, Han JY, Katakami N, Kim HR, et al. CNS efficacy of osimertinib in patients with T790M-positive advanced non-small-cell lung cancer: data from a randomized phase III trial (AURA3). J Clin Oncol. (2018) 36:2702–9. doi: 10.1200/JCO.2018.77.9363
16. Soria J-C, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in untreated EGFR-mutated advanced non–small-cell lung cancer. N Engl J Med. (2017) 378:113–25. doi: 10.1056/NEJMoa1713137
17. Janne PA, Yang JC, Kim DW, Planchard D, Ohe Y, Ramalingam SS, et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N Engl J Med. (2015) 372:1689–99. doi: 10.1056/NEJMoa1411817
18. Minari R, Bordi P, Tiseo M. Third-generation epidermal growth factor receptor-tyrosine kinase inhibitors in T790M-positive non-small cell lung cancer: review on emerged mechanisms of resistance. Transl Lung Cancer Res. (2016) 5:695–708. doi: 10.21037/tlcr.2016.12.02
19. Lazzari C, Gregorc V, Karachaliou N, Rosell R, Santarpia M. Mechanisms of resistance to osimertinib. J Thorac Dis. (2019) 12:2851–8. doi: 10.21037/jtd.2019.08.30
20. Leonetti A, Sharma S, Minari R, Perego P, Giovannetti E, Tiseo M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br J Cancer. (2019) 121:725–37. doi: 10.1038/s41416-019-0573-8
21. Le X, Puri S, Negrao MV, Nilsson MB, Robichaux J, Boyle T, et al. Landscape of EGFR-dependent and -independent resistance mechanisms to osimertinib and continuation therapy beyond progression in EGFR-mutant NSCLC. Clin Cancer Res. (2018) 24:6195–203. doi: 10.1158/1078-0432.CCR-18-1542
22. Cortellini A, Leonetti A, Catino A, Pizzutillo P, Ricciuti B, De Giglio A, et al. Osimertinib beyond disease progression in T790M EGFR-positive NSCLC patients: a multicenter study of clinicians' attitudes. Clin Transl Oncol. (2020) 22:844–51. doi: 10.1007/s12094-019-02193-w
23. Kawamura T, Kenmotsu H, Omori S, Nakashima K, Wakuda K, Ono A, et al. Clinical factors predicting detection of T790M mutation in rebiopsy for EGFR-mutant non-small-cell lung cancer. Clin Lung Cancer. (2018) 19:e247–52. doi: 10.1016/j.cllc.2017.07.002
24. Ichihara E, Hotta K, Kubo T, Higashionna T, Ninomiya K, Ohashi K, et al. Clinical significance of repeat rebiopsy in detecting the EGFR T790M secondary mutation in patients with non-small cell lung cancer. Oncotarget. (2018) 9:29525–31. doi: 10.18632/oncotarget.25705
25. Zhou J, Zhao C, Zhao J, Wang Q, Chu X, Li J, et al. Re-biopsy and liquid biopsy for patients with non-small cell lung cancer after EGFR-tyrosine kinase inhibitor failure. Thoracic cancer. (2019) 10:957–65. doi: 10.1111/1759-7714.13035
26. Papadimitrakopoulou V, Wu YL, Han JY, Ahn MJ, Ramalingam S, John T, et al. LBA51 analysis of resistance mechanisms to osimertinib in patients with EGFR T790M advanced NSCLC from the AURA3 study. Ann Oncol. (2018) 29:viii741. doi: 10.1093/annonc/mdy424.064
27. Piotrowska Z, Isozaki H, Lennerz JK, Gainor JF, Lennes IT, Zhu VW. Landscape of acquired resistance to osimertinib in EGFR-mutant NSCLC and clinical validation of combined EGFR and RET inhibition with osimertinib and BLU-667 for acquired RET fusion. Cancer Discov. (2018) 8:1529–39. doi: 10.1158/2159-8290.CD-18-1022
28. Oxnard GR, Hu Y, Mileham KF, Husain H, Costa DB, Tracy P, et al. Assessment of resistance mechanisms and clinical implications in patients with EGFR T790M-positive lung cancer and acquired resistance to osimertinib. JAMA Oncol. (2018) 4:1527–34. doi: 10.1001/jamaoncol.2018.2969
29. Mehlman C, Cadranel J, Rousseau-Bussac G, Lacave R, Pujals A, Girard N, et al. Resistance mechanisms to osimertinib in EGFR-mutated advanced non-small-cell lung cancer: a multicentric retrospective French study. Lung Cancer. (2019) 137:149–56. doi: 10.1016/j.lungcan.2019.09.019
30. Lee J, Kim HS, Lee B, Kim HK, Sun JM, Ahn JS, et al. Genomic landscape of acquired resistance to third-generation EGFR tyrosine kinase inhibitors in EGFR T790M-mutant non-small cell lung cancer. Cancer. (2020) 126:2704–12. doi: 10.1002/cncr.32809
31. Zhang YC, Zhou Q, Wu YL. Clinical management of third-generation EGFR inhibitor-resistant patients with advanced non-small cell lung cancer: current status and future perspectives. Cancer Lett. (2019) 459:240–7. doi: 10.1016/j.canlet.2019.05.044
32. Niederst MJ, Hu H, Mulvey HE, Lockerman EL, Garcia AR, Piotrowska Z, et al. The allelic context of the C797S mutation acquired upon treatment with third-generation EGFR inhibitors impacts sensitivity to subsequent treatment strategies. Clin Cancer Res. (2015) 21:3924–33. doi: 10.1158/1078-0432.CCR-15-0560
33. Janjigian YY, Smit EF, Groen HJ, Horn L, Gettinger S, Camidge DR, et al. Dual inhibition of EGFR with afatinib and cetuximab in kinase inhibitor-resistant EGFR-mutant lung cancer with and without T790M mutations. Cancer Discov. (2014) 4:1036–45. doi: 10.1158/2159-8290.CD-14-0326
34. Ou SI, Agarwal N, Ali SM. High MET amplification level as a resistance mechanism to osimertinib (AZD9291) in a patient that symptomatically responded to crizotinib treatment post-osimertinib progression. Lung Cancer. (2016) 98:59–61. doi: 10.1016/j.lungcan.2016.05.015
35. York ER, Varella-Garcia M, Bang TJ, Aisner DL, Camidge DR. Tolerable and effective combination of full-dose crizotinib and osimertinib targeting MET amplification sequentially emerging after T790M positivity in EGFR-mutant non-small cell lung cancer. J Thorac Oncol. (2017) 12:e85–e8. doi: 10.1016/j.jtho.2017.02.020
36. Ho CC, Liao WY, Lin CA, Shih JY, Yu CJ, Yang JC. Acquired BRAF V600E mutation as resistant mechanism after treatment with osimertinib. J Thorac Oncol. (2017) 12:567–72. doi: 10.1016/j.jtho.2016.11.2231
Keywords: non-small cell lung cancer, EGFR T790M mutation, osimertinib, resistance, real-world data, next generation sequencing
Citation: Fernandes MGO, Sousa C, Jacob M, Almeida L, Santos V, Araújo D, Novais Bastos H, Magalhães A, Cirnes L, Moura CS, Queiroga H, Cruz-Martins N and Hespanhol V (2021) Resistance Profile of Osimertinib in Pre-treated Patients With EGFR T790M-Mutated Non-small Cell Lung Cancer. Front. Oncol. 11:602924. doi: 10.3389/fonc.2021.602924
Received: 04 September 2020; Accepted: 23 February 2021;
Published: 06 May 2021.
Edited by:
Yaxiong Zhang, Sun Yat-sen University Cancer Center (SYSUCC), ChinaReviewed by:
Sagun Parakh, University of Melbourne, AustraliaCopyright © 2021 Fernandes, Sousa, Jacob, Almeida, Santos, Araújo, Novais Bastos, Magalhães, Cirnes, Moura, Queiroga, Cruz-Martins and Hespanhol. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Gabriela O. Fernandes, Z2Zlcm5hbmRlc0BtZWQudXAucHQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.