 Gerardo Rosati
Gerardo Rosati Giuseppe Aprile
Giuseppe Aprile Debora Basile
Debora Basile Antonio Avallone
Antonio Avallone
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Oncol., 02 March 2021
Sec. Gastrointestinal Cancers
Volume 11 - 2021 | https://doi.org/10.3389/fonc.2021.602596
This article is part of the Research TopicThe Treatment of RAS or BRAF Mutated Metastatic Colorectal Cancer: Challenges and PerspectivesView all 8 articles
Until a few years ago, the overall survival (OS) for metastatic colorectal cancer (mCRC) patients did not generally exceed 18–20 months in spite of a progressively evolving therapeutic armamentarium (1). Targeted therapies have revolutionized these results, leading to a marked increase in response rate (RR), progression-free survival (PFS), and OS. Despite these achievements, the benefits and toxicities may vary significantly from patient to patient and physicians’ decisions are best guided by the identification of predictive/prognostic biomarkers (2).
The development of a colorectal cancer, at least the sporadic ones (70–80%), proceeds over several years. Alongside an environmental genesis in which diet could be a cause, it is known that mutations in certain genes [neuroblastoma RAS (NRAS), Kirsten RAS (KRAS), mutant B rapidly accelerated fibrosarcoma (BRAF)], part of the downstream signaling pathways of the epidermal growth factor receptor (EGFR), are crucial in the process of carcinogenesis (3). Unfortunately, these mutations are also the main form of resistance to monoclonal antibodies such as cetuximab and panitumumab which, by binding to the extracellular domain of EGFR, inhibit cell growth which is otherwise nullified. The rat sarcoma virus (RAS) mutations of codons 12 and 13 of exon two, 59 and 61 of exon three, and 117 and 146 of exon four plus those of BRAF are therefore mandatory before treatment with anti-EGFR antibodies and can be found in about 60% of patients (4).
We here review the clinical usefulness of researching these mutations and express our opinion on the applicability and efficacy of potentially active compounds in these circumstances.
A pooled analysis of five randomized trials showed that mutant KRAS and BRAF (for BRAF see paragraph below) mCRC patients have shorter PFS and OS compared to those defined wild-type (wt), although not all the latter are sensitive to anti-EGFR antibodies (5). In these cases, PIK3CA gene mutation, phosphatase and tensin homolog (PTEN) loss, or human EGFR2 (HER2) amplification may lead to resistance to cetuximab and panitumumab. Mutated patients therefore need to be treated differently. While standard first-line chemotherapy doublets plus bevacizumab produce lesser benefits compared to wt patients, the combined use of oxaliplatin, irinotecan, and 5-fluorouracil (FOLFOXIRI) seems to bring better results (6). The data of second-line aflibercept and ramucirumab in combination with irinotecan and 5-fluorouracil (FOLFIRI) and those of regorafenib and trifluridine/tipiracil in pretreated patients suggest that these treatments are equally effective regardless of RAS mutations (7–9).
While uncommon RAS mutations—identified by more profound molecular analyses—might preclude the effectiveness of anti-EGFR antibodies in some wt patients, it is not clear how to eventually target RAS-mutant cancers. A meta-analysis showed that extending the RAS study to search for less frequent mutations has a significant impact on outcomes (10). A next-generation sequencing (NGS)-based companion diagnostic instrument has been validated to detect all RAS mutations in DNA extracted from formalin-fixed paraffin-embedded mCRC tumor samples (11). Although RAS is frequently mutated, its direct inhibition with specific target therapies (Table 1) has proved difficult.
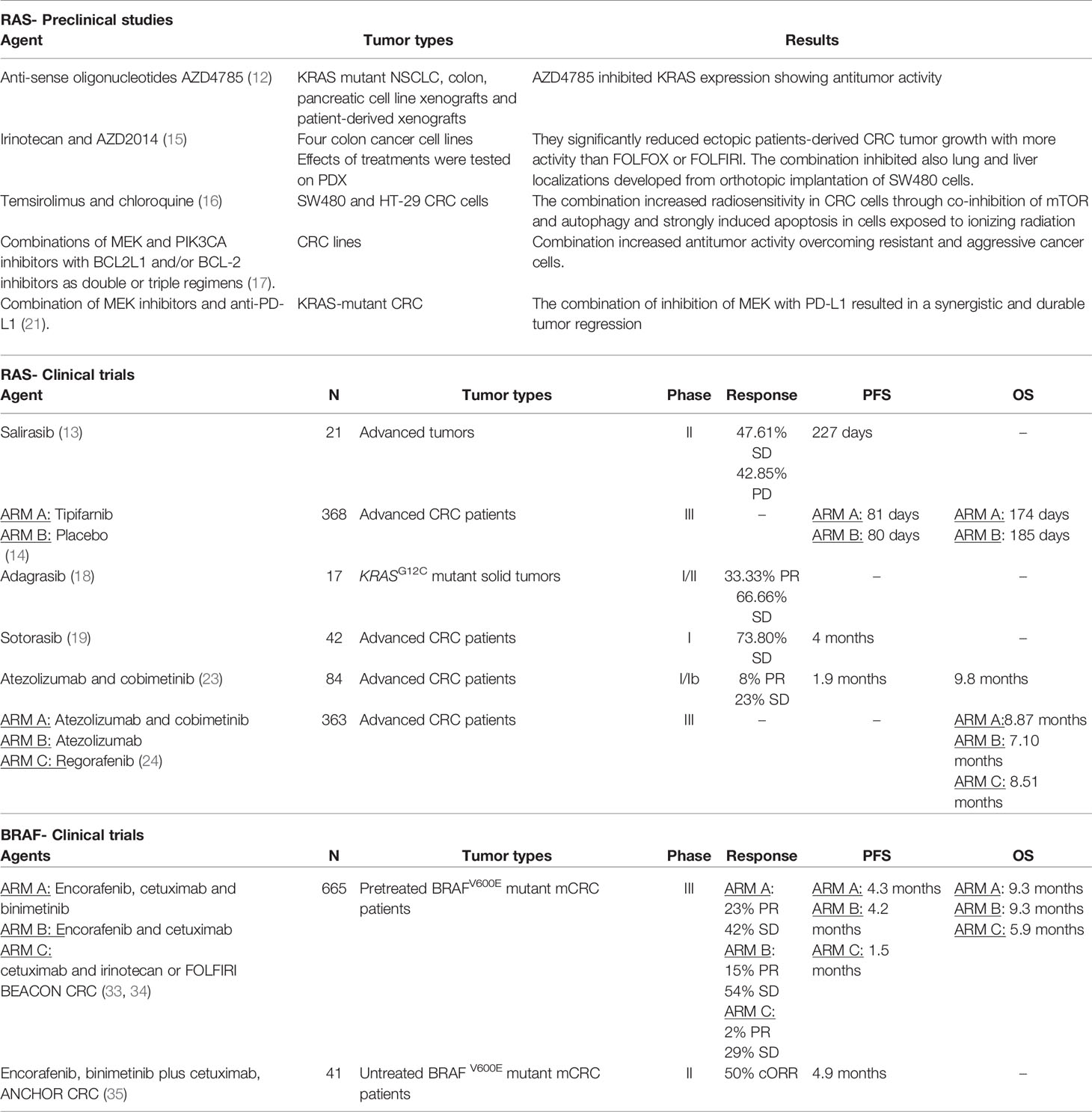
Table 1 Preclinical and clinical trials for targeted therapies in RAS and BRAF metastatic CRC.
This is the case of anti-sense oligonucleotides that have been shown to induce genetic depletion of mutant KRAS in preclinical models (12). Salirasib is an oral RAS inhibitor that competitively blocks the membrane association of RAS proteins. Although with a reduced number of subjects, a Japanese phase I study showed that salirasib was safe and well tolerated, a dose of 800 mg twice daily was recommended for phase II studies, and patients showed PFS of 227 days (17).
Two farnesyltransferase inhibitors (FTI), tipifarnib and lonafarnib, were tested in phase III clinical trials in patients with advanced stage pancreatic cancer, NSCLC, mCRC, and acute myeloid leukemia. They showed no clinical efficacy in KRAS-driven cancer, leading to the conclusion that targeting post-translational modifications in RAS are ineffective (18).
Another way to achieve RAS inhibition may be to antagonize other proteins of its pathway, as in the case of mitogen-activated protein kinase (MAPK) or phosphatidylinositol 3-kinase (PIK3CA)/Akt/mTOR inhibitors. The PI3K/Akt/mammalian target of rapamycin (mTOR) plays an important role in intracellular functions, regulating cell proliferation, growth, cell size, metabolism and motility. Thus, the combination of irinotecan and AZD2014 significantly reduces cell invasion capacity by 70% and inhibits the growth of colon cancer derived from the ectopic patient, demonstrating greater potency than oxaliplatin and 5-fluorouracil (FOLFOX) or FOLFIRI. Furthermore, the combination totally inhibited the metastases developed by the orthotopic implantation of SW480 cells (13). Another study has shown that the combination of temsirolimus, mTOR inhibitor, and chloroquine, an autophagy inhibitor, increases radiosensitivity in colorectal cancer cells. In particular, ionizing radiation activated the proteins downstream of mTOR and induced autophagy, while chloroquine inhibited autophagy in the advanced stage and did not affect the proteins downstream of mTOR (14).
Another strategy is to use combined therapies. The anti-apoptotic protein BCL2L1 increases the efficacy of MEK inhibition, determining a strong cytostatic response and a further apoptotic action. Combinations of MEK and PIK3CA inhibitors with BCL2L1 and/or BCL-2 inhibitors as double or triple regimens showed increasing antitumor activity (15). This strategy mostly involves MEK inhibitors as a therapeutic backbone, although exploring combinations with newer agents that target other elements of the MAPK pathway could achieve a more optimal inhibition of RAF-MEK-ERK signaling. However, the limitation of these therapies is the tolerability that leads to a reduction in clinical activity through a reduction in doses.
More promising and in the process of clinical development are other molecules. Adagrasib binds to KRASG12C, locking it in an inactive state. This inhibitor is currently being tested in a study involving 17 patients with KRASG12C mutant solid tumors, mostly non-small cell lung cancer or mCRC. Most of them reported low toxicity and 12 were valuable for the response: four had partial responses and eight had stable disease (SD). All responders received a dose of 600 mg twice a day; one with mCRC had a 47% reduction, 6 weeks after the start of treatment (19). Sotorasib, another small similar molecule, has been evaluated in 42 pretreated mCRC patients in a phase I study showing that at the 960 mg dose the most relevant grade 3 or 4 toxicities, diarrhea and anemia, occurred in 11.6% of cases, while 7.1% of patients had a confirmed response, and 31 of them (73.8%) had SD. The median progression-free survival was 4.0 months (range, 0.0+ to 11.1+) (20).
In addition, the use of immunotherapy may be effective in the presence of RAS mutations, since the reduction in the number of tumor-infiltrating lymphocytes (TILs), the negative influence on the tumor microenvironment, and the increase in the expression of programmed cell death ligand 1 (PD-L1) are often observed in RAS-mutated tumors. One study demonstrated an objective regression of lung metastases via a polyclonal CD8+ T cell response against mutant KRAS p.G12D in TILs obtained from a patient with mCRC (26). Preclinical evidence of KRAS-mutant colorectal cancer shows that targeted inhibition of mitogen-activated protein kinase (MAPK) (MEK) deeply blocks the naive priming of CD8 (+) T cells in tumor-bearing mice and increases their number inside. The combination of inhibition of MEK with PD-L1 results in a synergistic and lasting tumor regression (16).
The combination of atezolizumab and the MEK inhibitor cobimetinib has also aroused interest. Although the efficacy of immunotherapy in patients with mCRC has generally been limited to tumors with mismatched DNA repair deficiencies or microsatellite instability (MSI-H) (27), responses were observed in 7 out of 84 patients (6 responders were microsatellite low/stable, 1 was microsatellite instable) in a phase I/Ib study (21). While the most common adverse events related to the treatment were diarrhea (67%), rash (48%), and fatigue (40%), clinical activity of atezolizumab and cobimetinib was reported regardless of KRAS/BRAF state. This potential synergistic activity was not confirmed in a subsequent phase III study, even though the recruitment of patients with MSI-H was no more than 5% emphasizing that the benefits of immunotherapy should be limited only to them (22).
BRAF, a serine-threonine protein kinase, is the primary effector of RAS signaling and is mutated in roughly 10% of mCRC patients. BRAF mutations occur most frequently (>90%) at the valine 600 residue (BRAFV600E) and are usually and mutually exclusive with RAS mutations (28). The presence of the BRAFV600E mutation characterizes a subgroup of patients with poor prognosis and modest benefit from standard treatments (29).
In recent years, FOLFOXIRI plus bevacizumab has been introduced as a possible standard of care in these cases (30). The use of this intensive combination was mainly supported by a subgroup analysis of 28 BRAFV600E mutated patients in the TRIBE trial, which showed a median OS of 19.0 months in those treated with FOLFOXIRI/bevacizumab, whereas patients treated with FOLFIRI/bevacizumab had a shorter median OS of 10.7 months (31). However, TRIBE 2 trial did not confirm a greater benefit for BRAF mutant patients with FOLFOXIRI/bevacizumab compared to mFOLFOX6/bevacizumab (32). A potential major efficacy of an antiangiogenic agent in combination with chemotherapy has also been reported in second-line treatment of BRAFV600E mCRC patients. A subgroup analysis of the VELOUR study showed that patients treated with aflibercept more FOLFIRI reported a doubled median OS than those treated with chemotherapy alone (33). However, the value of these data should be carefully considered given the small number of patients studied.
Unlike the favorable results observed in melanoma patients, treatment with BRAF inhibitor alone yielded low clinical activity in mCRC, due to insufficient inhibition of MAPK pathway through a feedback EGFR reactivation (34, 35). BRAF inhibitors were therefore combined with anti-EGFR antibodies plus or minus MEK inhibitors. A relevant clinical benefit of this strategy was demonstrated for the first time in the large, randomized phase III BEACON trial (23). In this trial, 665 BRAFV600E mCRC patients, after one or two prior regimens, were randomized to receive the BRAF inhibitor encorafenib in combination with the anti-EGFR antibody cetuximab plus (triplet therapy) or minus the MEK inhibitor binimetinib (doublet therapy) or cetuximab in combination with irinotecan or FOLFIRI (standard therapy). The primary endpoints of the study were OS and RR. In the primary analysis, the triplet and doublet therapy, compared with standard therapy, resulted in significantly longer median OS (9.0, 8.4, and 5.4 months, respectively) and higher RR (26, 20, and 2%, respectively), with manageable safety profile. Interestingly, update results of the BEACON trial showed similar OS with either triplet and doublet combinations and a higher rate of adverse events in the first group compared to the other (65.8 versus 57.4%) (24). So, FDA approved encorafenib plus cetuximab in previously treated BRAFV600E mCRC patients. This strategy has been foreshadowed in the first-line treatment of these patients. However, when examining the use of triplet therapy in the latter context, the first results of the phase II ANCHOR-CRC trial did not live up to expectations, reporting a median PFS of only 5 months (25).
Therefore, the role of the doublet and triplet inhibition of EGFR pathway in the first-line treatment of BRAFV600E mCRC patients is still not determined and additional therapeutic strategies, addressing the rapid acquisition of resistance, are needed to improve the efficacy of BRAF inhibitors in this disease.
While in recent years the possibility of overcoming the BRAF mutation has emerged more concretely, in our opinion RAS still remains a difficult target. Although the National Cancer Institute launched a program in 2013 to develop new promising agents through preclinical and clinical trials, their impact in the near future could be marginal for tumors harboring specific mutations, as they do not ensure a substantial change in therapeutic prospects for the majority of patients.
GR and AA wrote the manuscript. All authors participated in drafting and editing the manuscript. All authors contributed to the article and approved the submitted version.
This work was supported by the Italian Ministry of Health (RF-2016-02363314).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Tournigand C, André T, Achille E, Lledo G, Flesh M, Mery-Mignard D, et al. Folfiri followed by Folfox6 or the reverse sequence in advanced colorectal cancer: a randomized gercor study. J Clin Oncol (2004) 22:229–37. doi: 10.1200/JCO.2004.05.113
2. Koncina E, Haan S, Rauh S, Letellier E. Prognostic and predictive molecular biomarkers for colorectal cancer: updates and challanges. Cancers (2020) 12:319. doi: 10.3390/cancers12020319
3. Bogaert J, Prenen H. Molecular genetics of colorectal cancer. Ann Gastroenterol Q Publ Hell Soc Gastroenterol (2014) 27:9–14.
4. Zarkavelis G, Boussios S, Papadaki A, Katsanos KH, Christodoulou DK, Pentheroudakis G. Current and future biomarkers in colorectal cancer. Ann Gastroenterol (2017) 30:613–21. doi: 10.20524/aog.2017.0191
5. Modest DP, Ricard I, Heinemann V, Hegewisch-Becker S, Schmiegel W, Porschen, et al. Outcome according to KRAS-, NRAS-and BRAF-mutation as well as KRAS mutation variants: Pooled analysis of five randomized trials in metastatic colorectal cancer by the AIO colorectal cancer study group. Ann Oncol O J Eur Soc Med Oncol (2016) 27:1746–53. doi: 10.1093/annonc/mdw261
6. Satake H, Sunakawa Y, Miyamoto Y, Nakamura M, Nakayama H, Shiozawa M, et al. A phase II trial of 1st-line modified-FOLFOXIRI plus bevacizumab treatment for metastatic colorectal cancer harboring RAS mutation: JACCRO CC-11. Oncotarget (2018) 9:18811–20. doi: 10.18632/oncotarget.24702
7. Van Cutsem E, Cervantes A, Adam R, Sobrero A, Van Krieken JH, Aderka D, et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol (2016) 27:1386–422. doi: 10.1093/annonc/mdw235
8. Van Cutsem E, Martinelli E, Cascinu S, Sobrero A, Banzi M, Seitz JF, et al. Regorafenib for patients with metastatic colorectal cancer who progressed after standard therapy: results of the large, single-arm, open-label phase IIIb CONSIGN study. Oncologist (2019) 24:185–92. doi: 10.1634/theoncologist.2018-0072
9. Van Cutsem E, Mayer RJ, Laurent S, Winkler R, Grávalos C, Benavides M, et al. The subgroups of the phase III RECOURSE trial of trifluridine/tipiracil (TAS-102) versus placebo with best supportive care in patients with metastatic colorectal cancer. Eur J Cancer (2018) 90:63–72. doi: 10.1016/j.ejca.2017.10.009
10. Sorich MJ, Wiese MD, Rowland A, Kichenadasse G, McKinnon RA, Karapetis CS. Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: a meta-analysis of randomized, controlled trials. Ann Oncol (2015) 26:13–21. doi: 10.1093/annonc/mdu378
11. Udar N, Lofton-Day C, Dong J, Vavrek D, Jung AS, Meier K, et al. Clinical validation of the next-generation sequencing-based extended RAS panel assay using metastatic colorectal cancer patient samples from the phase 3 PRIME study. J Cancer Res Clin Oncol (2018) 144:2001–10. doi: 10.1007/s00432-018-2688-3
12. Ross SJ, Revenko AS, Hanson LL, Ellston R, Staniszewska A, Whalley N, et al. Targeting KRAS-dependent tumors with AZD4785, a high-affinity therapeutic antisense oligonucleotide inhibitor of KRAS. Sci Transl Med (2017) 9:eaal5253. doi: 10.1126/scitranslmed.aal5253
13. Reita D, Bour C, Benbrika R, Groh A, Pencreach E, Guérin E, et al. Synergistic anti-tumor effect of mTOR inhibitors with irinotecan on colon cancer cells. Cancers (2019) 17:1581. doi: 10.3390/cancers11101581
14. Shiratori H, Kawai K, Hata K, Tanaka T, Nishikawa T, Otani K, et al. The combination of temsirolimus and chloroquine increases radiosensitivity in colorectal cancer cells. Oncol Rep (2019) 42:377–85. doi: 10.3892/or.2019.7134
15. Horn T, Ferretti S, Ebel N, Tam A, Ho S, Harbinski F, et al. High-order drug combinations are required to effectively kill colorectal cancer cells. Cancer Res (2016) 76:6950–63. doi: 10.1158/0008-5472.CAN-15-3425
16. Ebert PJR, Cheung J, Yang Y, McNamara E, Hong R, Moskalenko M, et al. MAP kinase inhibition promotes T cell and anti-tumor activity in combination with PD-L1 checkpoint blockade. Immunity (2016) 44:609–21. doi: 10.1016/j.immuni.2016.01.024
17. Furuse J, Kurata T, Okano N, Fujisaka Y, Naruge D, Shimizu T, et al. An early clinical trial of salirasib, an oral RAS inhibitor, in Japanese patients with relapsed/refractory solid tumors. Cancer Chemother Pharmacol (2018) 82:511–9. doi: 10.1007/s00280-018-3618-4
18. Ryan MB, Corcoran RB. Therapeutic strategies to target RAS-mutant cancers. Nat Rev Clin Oncol (2018) 15:709–20. doi: 10.1038/s41571-018-0105-0
19. Romero D. Two new agents target KRAS G12C. Nat Rev Clin Oncol (2020) 17:6. doi: 10.1038/s41571-019-0304-3
20. Hong DS, Fakih MG, Strickler JH, Desai J, Durm GA, Shapiro GI, et al. KRASG12C inhibition with sotorasib in advanced solid tumors. N Eng J Med (2020) 383:1207–17. doi: 10.1056/NEJMoa1917239
21. Hellmann MD, Kim TW, Lee CB, Goh BC, Miller WH Jr, Oh DY, et al. Phase Ib study of atezolizumab combined with cobimetinib in patients with solid tumors. Ann Oncol (2019) 30:1134–42. doi: 10.1093/annonc/mdz113
22. Eng C, Kim TW, Bendell J, Argilés G, Tebbutt NC, Di Bartolomeo M, et al. Atezolizumab with or without cobimetinib versus regorafenib in previously treated metastatic colorectal cancer (IMblaze370): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol (2019) 20:849–61. doi: 10.1016/S1470-2045(19)30027-0
23. Kopetz S, Grothey A, Tabernero J. Encorafenib, Binimetinib, and Cetuximab in BRAF V600E-Mutated Colorectal Cancer. Reply. N Engl J Med (2020) 382:877–8. doi: 10.1056/NEJMc1915676
24. Kopetz S, Grothey A, Van Cutsem E, Yaeger R, Wasan HS, Yoshino T, et al. Encorafenib plus cetuximab with or without binimetinib for BRAF V600E metastatic colorectal cancer: Updated survival results from a randomized, three-arm, phase III study versus choice of either irinotecan or FOLFIRI plus cetuximab (BEACON CRC). Abstract retrieved from Abstracts in ASCO database. (Accession No. 4001). J Clin Oncol (2020) 38(15_suppl):4001–1. doi: 10.1200/JCO.2020.38.15_suppl.4001
25. Grothey A, Tabernero J, Taieb J, Yaeger R, Yoshino T, Maiello E, et al. ANCHOR CRC: a single-arm phase 2 study of encorafenib, binimetinib plus cetuximab in previously untreated BRAF V600E mutant metastatic colorectal cancer. Abstract retrieved from in Abstracts in ESMO GI database. (Accession No. LBA-5). Ann Oncol (2020) 31(3_suppl):S242–3. doi: 10.1016/j.annonc.2020.04.080
26. Tran E, Robbins PF, Lu Y-C, Prickett TD, Gartner JJ, Jia L, et al. T-cell transfer therapy targeting mutant KRAS in cancer. N Engl J Med (2016) 375:2255–62. doi: 10.1056/NEJMoa1609279
27. Le DT, Uram JN, Wang H, Bartlett BR, Kemberling H, Eyring AD, et al. PD-1 blockade in tumors with mismatch-repair deficiency. N Engl J Med (2015) 372:2509–20. doi: 10.1056/NEJMoa1500596
28. Custodio A, Feliu J. Prognostic and predictive biomarkers for epidermal growth factor receptor-targeted therapy in colorectal cancer: beyond KRAS mutations. Crit Rev Oncol Hematol (2013) 85:45–81. doi: 10.1016/j.critrevonc.2012.05.001
29. Seligmann JF, Fisher D, Smith CG, Richman SD, Elliott F, Brown S, et al. Investigating the poor outcomes of BRAF-mutant advanced colorectal cancer: analysis from 2530 patients in randomised clinical trials. Ann Oncol (2017) 28:562–8. doi: 10.1093/annonc/mdw645
30. Yoshino T, Arnold D, Taniguchi H, Pentheroudakis G, Yamazaki K, Xuet R-H, et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: a JSMO-ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann Oncol (2018) 29:44–70. doi: 10.1093/annonc/mdx738
31. Loupakis F, Cremolini C, Masi G, Lonardi S, Zagonel V, Salvatore L, et al. Initial therapy with FOLFOXIRI and bevacizumab for metastatic colorectal cancer. N Engl J Med (2014) 371:1609–18. doi: 10.1056/NEJMoa1403108
32. Cremolini C, Antoniotti C, Rossini D, Lonardi S, Loupakis F, Pietrantonio F, et al. Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): a multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol (2020) 21:497–507. doi: 10.2139/ssrn.3478102
33. Wirapati P, Pomella V, Vandenbosch B, Kerr P, Maiello E, Jeffery GM, et al. Velour trial biomarkers update: Impact of RAS, BRAF, and sidedness on aflibercept activity. Abstract retrieved from Abstracts in ASCO database. (Accession No. 3538). J Clin Oncol (2017) 38(15_suppl):3538–8. doi: 10.1200/JCO.2017.35.15_suppl.3538
34. Kopetz S, Desai J, Chan E, Hecht JR, O’Dwyer PJ, Maruet D, et al. Phase II pilot study of vemurafenib in patients with metastatic BRAF-mutated colorectal cancer. J Clin Oncol (2015) 33:4032–8. doi: 10.1200/JCO.2015.63.2497
Keywords: BRAF mutation, colorectal cancer, metastatic disease, RAS mutation, targeted therapies
Citation: Rosati G, Aprile G, Basile D and Avallone A (2021) Perspectives in the Treatment of RAS or BRAF Mutated Metastatic Colorectal Cancer Patients. Front. Oncol. 11:602596. doi: 10.3389/fonc.2021.602596
Received: 03 September 2020; Accepted: 18 January 2021;
Published: 02 March 2021.
Edited by:
Claudia Von Arx, Imperial College London, United KingdomReviewed by:
Michele Ghidini, IRCCS Foundation Ca ‘Granda Ospedale Maggiore Policlinico, ItalyCopyright © 2021 Rosati, Aprile, Basile and Avallone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gerardo Rosati, b25jb2dlcnJ5QHlhaG9vLml0; Antonio Avallone, YXZhbGxvYW50b25pb0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.