 Tao Shi1†
Tao Shi1† Shuai Zhu2†
Shuai Zhu2† Hengjuan Guo3†
Hengjuan Guo3† Xiongfei Li2
Xiongfei Li2 Shikang Zhao2
Shikang Zhao2 Yanye Wang2
Yanye Wang2 Xi Lei2
Xi Lei2 Dingzhi Huang4
Dingzhi Huang4 Ling Peng5*
Ling Peng5* Ziming Li6*
Ziming Li6* Song Xu2*
Song Xu2*- 1Precision Medicine Center, Tianjin Medical University General Hospital, Tianjin, China
- 2Department of Lung Cancer Surgery, Tianjin Key Laboratory of Lung Cancer Metastasis and Tumor Microenvironment, Lung Cancer Institute, Tianjin Medical University General Hospital, Tianjin, China
- 3Department of Respiratory and Critical Care, Tianjin Medical University General Hospital, Tianjin, China
- 4Department of Thoracic Oncology, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China
- 5Department of Radiotherapy, The First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China
- 6Shanghai Lung Cancer Center, Shanghai Chest Hospital, Shanghai Jiao Tong University, Shanghai, China
Introduction: Previous studies have demonstrated that programmed cell death-ligand 1 (PD-L1) serves as biomarker for poor prognosis and survival in advanced-stage non-small cell lung cancer (NSCLC) patients. However, the merit of PD-L1 expression to predict the prognosis of early stage NSCLC patients who underwent complete resection remains controversial. In the present study, we performed a meta-analysis to investigate the relationship between PD-L1 expression and prognosis in patients with early stage resected NSCLC.
Methods: Electronic databases, including PubMed, EMBASE, and the Cochrane Library, were searched until July 23 2020 for studies evaluating the expression of PD-L1 and the prognosis of resected NSCLCs. Hazard ratios (HRs) with 95% confidence intervals (CIs) of overall survival (OS) and disease-free survival (DFS) were pooled and analyzed. Heterogeneity and publication bias analyses were also assessed.
Results: A total of 15 studies involving 3,790 patients were considered in the present meta-analysis. The pooled HR indicated that PD-L1 expression related to a much shorter DFS (HR = 1.56, 95% CI: 1.18–2.05, p < 0.01), as well a significantly worse OS (HR = 1.68, 95% CI: 1.29–2.18, p < 0.01). Furthermore, our analysis indicated that PD-L1 expression was significantly associated with gender (male vs. female: OR = 1.27, 95% CI:1.01–1.59, p = 0.038), histology (ADC vs. SCC: OR = 0.54, 95% CI:0.38–0.77, p = 0.001), TNM stage (I vs. II–III: OR = 0.45, 95% CI:0.34–0.60, p = 0.000), smoking status (Yes vs No: OR = 1.43, 95% CI:1.14–1.80, p = 0.002) and lymph node metastasis (N+ vs N−: OR = 1.97, 95% CI:1.26–3.08, p = 0.003).
Conclusions: The results of this meta-analysis suggest that PD-L1 expression predicts an unfavorable prognosis in early stage resected NSCLCs. The role of personalized anti-PD-L1/PD-1 immunotherapy in the adjuvant settings of resected NSCLC warrants further investigation.
Introduction
Lung cancer is the most commonly diagnosed cancer and a leading cause of cancer-related deaths (1). Surgery is the standard treatment for early stage non-small cell lung cancer (NSCLC); however, postoperative prognosis remains unsatisfactory, with a 5-year survival rate ranging between 71 and 83% (2).Therefore, it is essential to identify new biomarkers for efficient clinical decision making and improve patient outcomes. Currently, blockade of the programmed cell death 1 (PD-1)/PD-1 ligand 1 (PD-L1) signaling pathway is one of the most promising immunotherapeutic strategies in boosting the immune system in the fight against cancer (3, 4). Programmed death 1 (PD-1), an important immune checkpoint molecule, is an immune-inhibitory receptor expressed on the surface of activated T cells in response to persistent inflammatory stimuli (5, 6). PD-L1 expressed on the tumor cells binds to the PD-1 receptors on activated T cells, resulting in the inhibition of the cytotoxic T cells. Blockade of the PD-1/PD-L1 pathway with monoclonal antibodies is a promising therapeutic strategy, with prominent clinical benefits of this checkpoint-blockade observed in recent clinical trials (7, 8).
Previously, a study has demonstrated that PD-L1 is a marker of poor prognosis and survival in advanced-stage NSCLC patients (9). A meta-analysis, performed on six studies with 1,157 patients, demonstrated that NSCLC patients with positive PD-L1 expression exhibited a much poorer OS (10). Another meta-analysis by Li et al., which included the largest number of patients (fifty studies with 11,383 patients), also indicated that PD-L1 IHC expression was related to poor overall survival (11). However, the searching deadline for Li’s study was January 2018, and more recent studies focusing on PD-L1 and prognosis in NSCLC were missing. More importantly, all of previous studies, including Li’s study, were performed on the NSCLC patients of both early and advanced stages, and they only took OS into account. Therefore, the impact of PD-L1 expression in the prognosis of patients with early stage NSCLCs following complete resection remains controversial. In the present study, we performed a meta-analysis of all available evidence not only to analyze OS but also assess the correlation between PD-L1 expression and DFS in early stage surgically resected NSCLC patients, which is more accurate and valuable to reflect the influence of PD-L1 expression on the survival of NSCLC.
Methods
This study was reported on the basis of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (Supplementary Data 1).
Relevant studies were retrieved by searching PubMed, Embase, and the Central Registry of Controlled Trials of the Cochrane Library, using the following terms: “Carcinoma, Non-Small Cell Lung” AND “PD-L1 protein, human” AND “Prognosis”. (Supplementary Data 2) The final search period was July 23 2020. Two authors (SX and SZ) performed the search independently. We restricted our research to studies published in English.
Eligible studies were in agreement with the following criteria: (1) the histology type of cancer was NSCLC; (2) valid TNM stage and cancer differentiation, as well as sufficient survival data, such as hazard ratio (HR) with 95% confidence intervals (CI), OS, and DFS were available (3) were published in English; (4) evaluated the association between PD-L1 expression and prognosis or pathological features; (5) involved early stage resectable NSCLC patients; (6) had similar research experimental design and methods; (7) PD-L1 expression was divided into high (positive) and low (negative) categories; and (8) relevant information could be extracted from the full-text study. Exclusion criteria included: (1) duplicate reports, ongoing studies, letters, conference papers, and reviews; (2) studies regarding lung cancer cell lines, animal models, and other types of cancer; (3) studies with insufficient survival data for which HR and CI could not be determined; (4) papers not published in English; (5) methods and experimental design differed from those of the selected studies.
The Newcastle–Ottawa quality assessment scale (NOS) and National Institute for Clinical Excellence (NICE) quality assessment scale was performed to assess methodological quality and risk of bias for cohort studies and case series studies, respectively. The primary outcomes of our study were disease-free survival (DFS) and overall survival (OS). The characteristic details of the publications, including the first author’s name, publication year, tumor type, PD-L1 level, stage, the evaluation method of the PD-L1expression, were extracted by two independent investigators. Any disagreement was discussed between investigators to reach a consensus. Multivariate analysis results were extracted as some included studies performed univariate analysis. We used the data directly from the included studies, providing precise HR (95% CI). In the case of studies only providing Kaplan–Meier survival curves, the Engauge Digitizer version 2.11 software was used to extract relevant numerical values from survival curves and calculate the HR (95% CI) (12, 13).
The STATA 15.0 (Stata Corporation, College Station, USA) software and R package 4.0.2 were used for data synthesis and analysis.
The random-effects model was employed in case of potential heterogeneity and to avoid underestimation of standard errors of pooled estimates in this meta-analysis. HRs for DFS and OS with 95% CIs according to the expression status of PD-L1 were pooled. The pooled odds ratios (ORs) were used to investigate the correlation between PD-L1 expression and clinicopathological features.
The heterogeneity test was performed using the Cochrane’s Q test (Chi-squared test; Chi2) and I2 metric (14). A chi-squared P value <0.1 or an I2 statistic >50% was defined as statistically significant heterogeneity (15). Moreover, the potential publication bias was assessed through Begg’s funnel plots (16). P <0.05 was considered as statistically significant based on the two-sided test. Subgroup analysis was conducted according to gender, histology, TNM stage, smoking status, and lymph node metastasis. An HR >1 reflected longer OS or DFS for PD-L1 negative patients.
Sensitivity analyses (17) were conducted to investigate the influence of a specific study on the pooled risk estimate by removing one study in each turn (Figures 2D, 3D, Supplementary Data 3).
Results
We identified 1,719 potentially relevant records through our search. A total of 1,558 studies were excluded after reviewing the title and abstract as their research contents failed to meet our inclusion criteria. Subsequently, the full texts of 92 articles were carefully screened, and a total of 15 studies (18–32) were found eligible for the final analysis. Figure 1 summarizes the flow chart depicting the process followed for study selection. No article was excluded by methodological quality and risk of bias and sensitivity analysis for significant heterogeneity (Figures 2D, 3D).
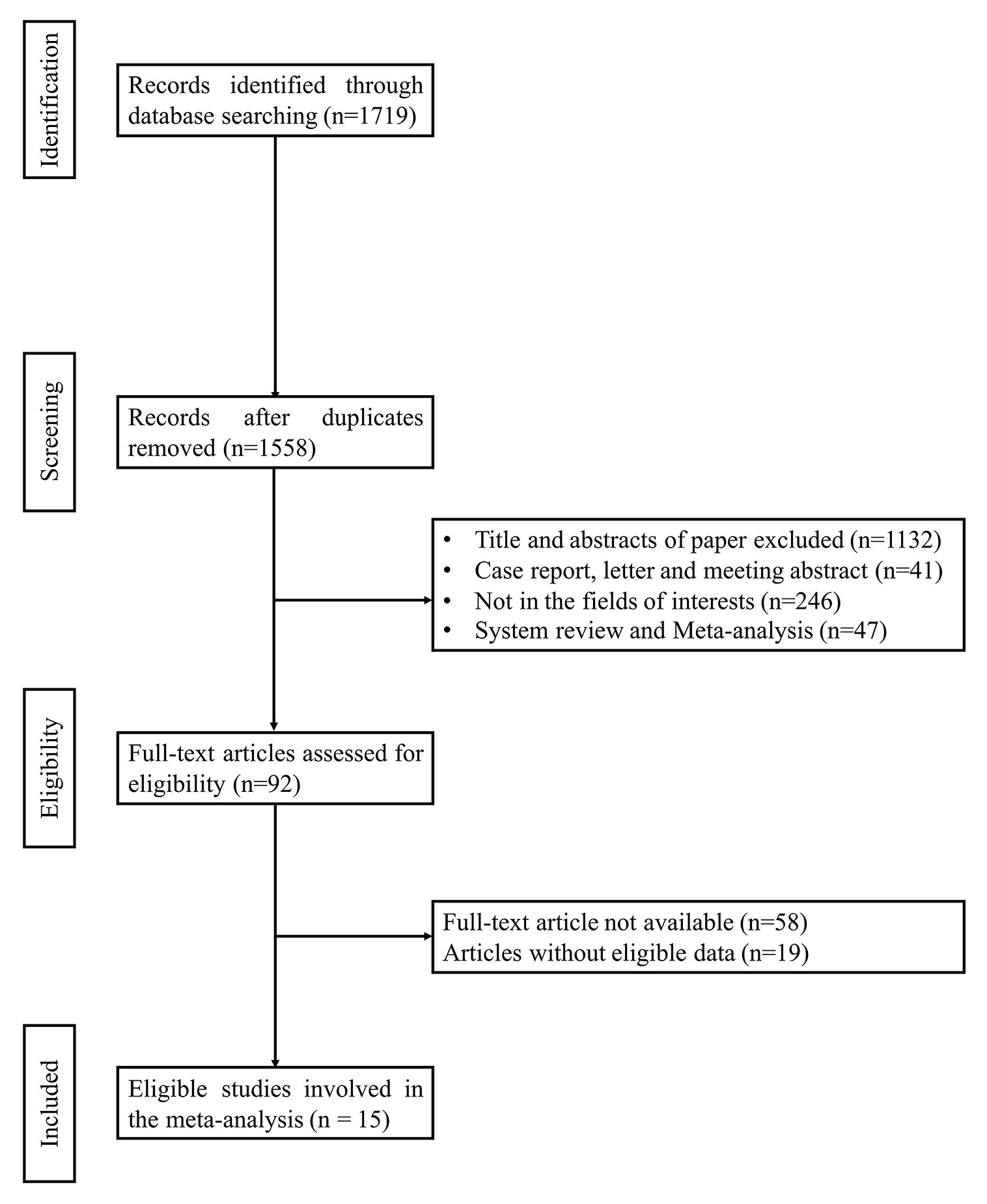
Figure 1 Flow chart of selection process to identify studies eligible for pooling.
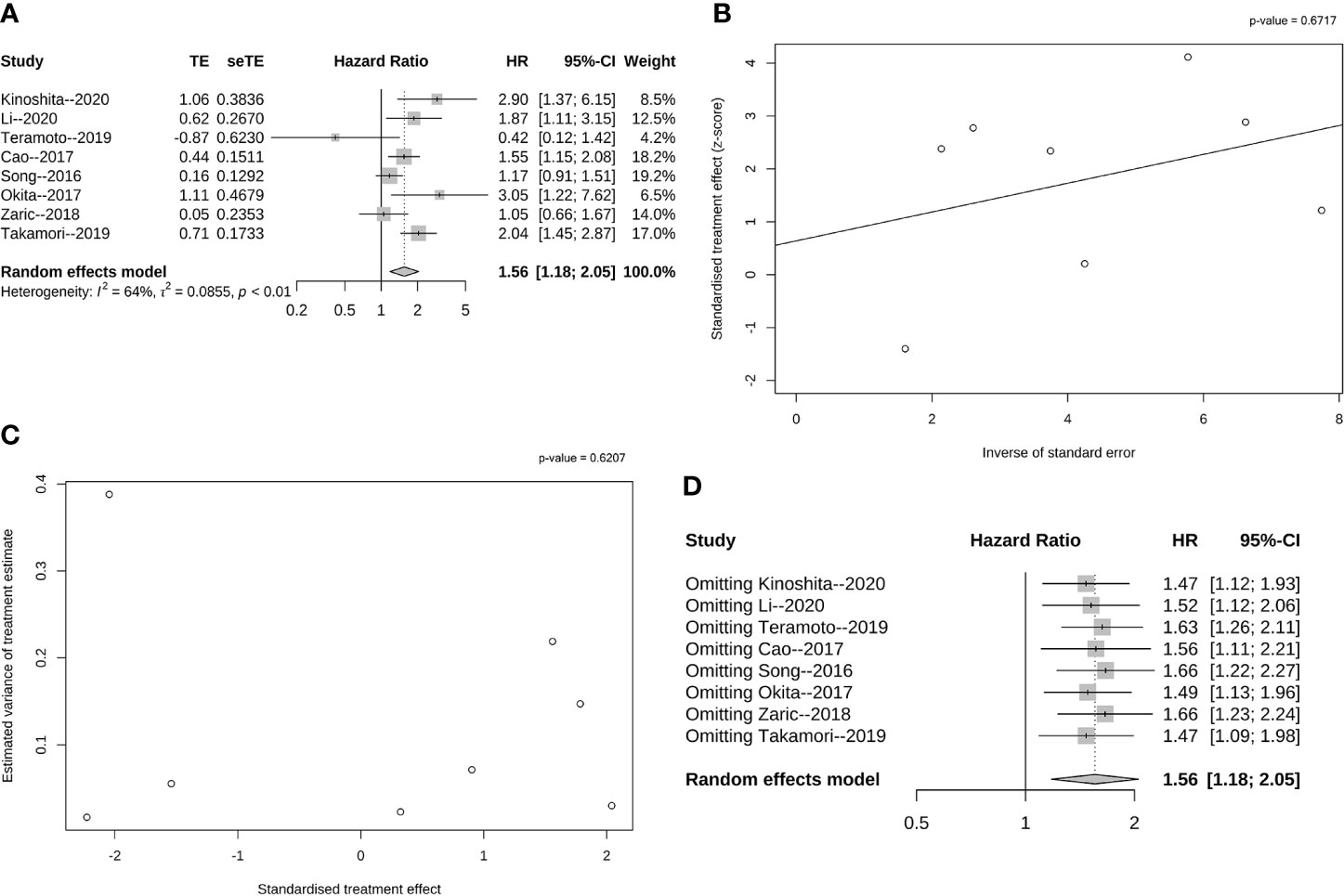
Figure 2 Pooled analysis of DFS according to PD-L1 expression. (A) Forest plot of HR for the association between PD-L1 expression and DFS with early stage resected non-small cell lung cancer; (B) Funnel graph of potential publication bias of HR for DFS in the eligible studies by Egger’s test; (C) Funnel graph of potential publication bias of HR for DFS in the eligible studies by Begg’s test. (D) Sensitivity analysis for DFS via elimination of each study in turn.
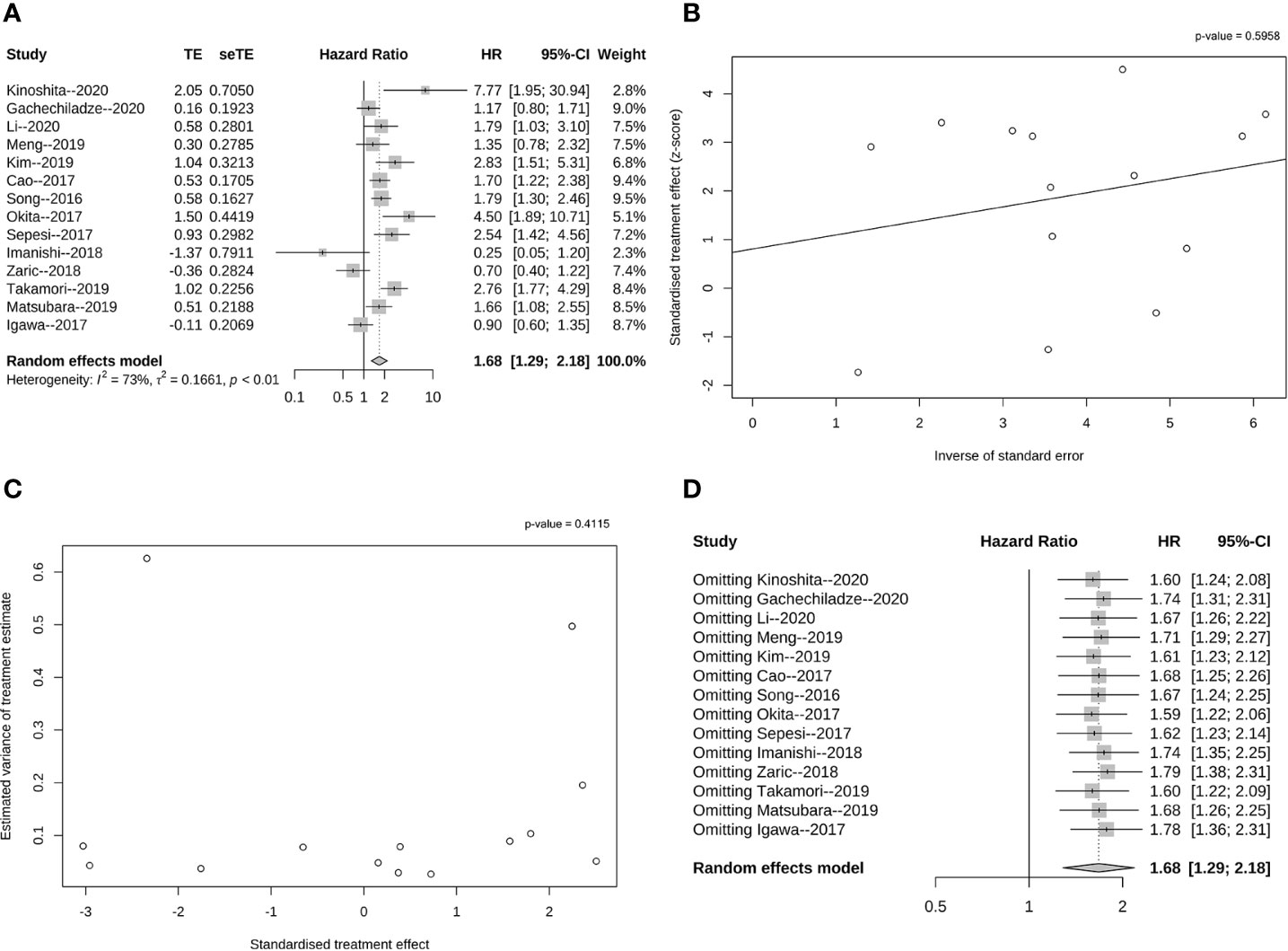
Figure 3 Pooled analysis of OS according to PD-L1 expression. (A) Forrest plot of HR for the association between PD-L1 expression and OS with early stage resected non-small cell lung cancer; (B) Funnel graph of potential publication bias of HR for OS in the eligible studies by Egger’s test; (C) Funnel graph of potential publication bias of HR for OS in the eligible studies by Begg’s test. (D) Sensitivity analysis for OS via elimination of each study in turn.
In all articles, resectability was a necessary intervention. All 15 studies were retrospective and published between 2016 and 2020. Fourteen of 15 studies recorded OS data, while only eight out of 15 studies presented only DFS information. Overall, 15 studies comprising of 3,790 patients were included in the pooled analysis and, all selected studies used immunohistochemistry or H-score assays to evaluate PD-L1 expression in tumor cells and/or tumor-infiltrating lymphocytes (TILs). Table 1 summarized the characteristics of all involved studies, including peri-operative therapy and PD-L1 detection information.
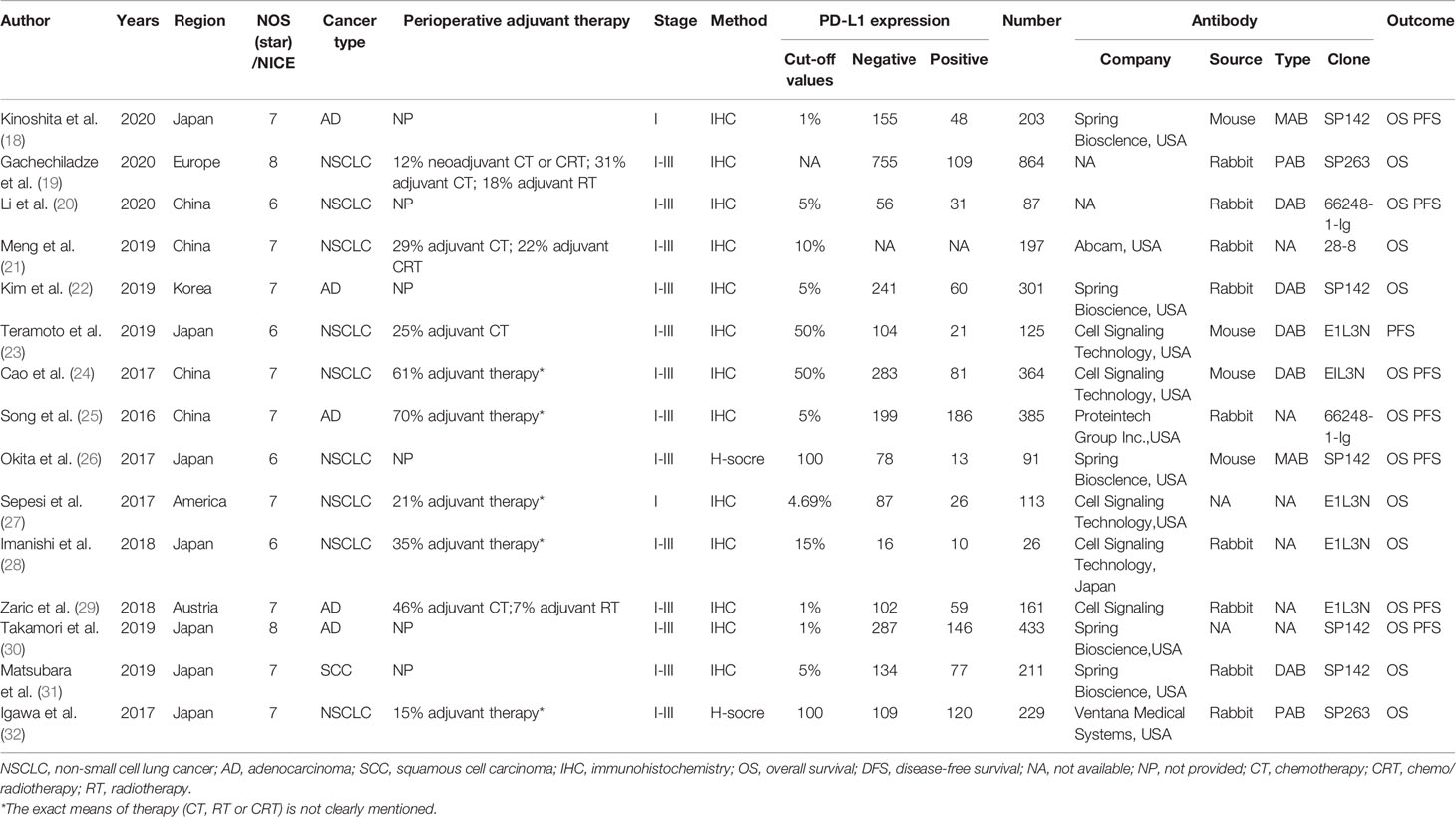
Table 1 Summary characteristics of included studies.
As shown in Figure 2A, the overall pooled HR indicated that the high PD-L1 expression was related to a significantly shorter DFS (HR = 1.56, 95% CI: 1.18–2.05, p < 0.01). Further analysis demonstrated heterogeneity among the eight studies (I² = 64%, p<< 0.01), and we hence performed Egger’s and Begg’s tests. According to Egger’s test (p = 0.671, Figure 2B) and Begg’s test (p = 0.620, Figure 2C), no publication bias influenced the HRs for DFS. Additionally, this confirmed that a negative correlation existed between PD-L1 expression and DFS in the case of resectable NSCLC patients.
In NSCLC patients, the positive expression of PD-L1 on tumor tissues was associated with significantly poorer OS when compared to those indicating negative PD-L1 expression (HR = 1.68, 95% CI: 1.29–2.18, p < 0.01, Figure 3A). Furthermore, heterogeneity was observed among the 15 studies (I² = 73%, P < 0.01). However, Egger’s (p = 0.595, Figure 3B) and Begg’s tests (p = 0.411, Figure 3C) demonstrated no publication bias influencing the HRs for OS, confirming the negative correlation of PD-L1 expression and OS for resectable NSCLC patients.
The correlation of PD-L1 expression and clinical characteristics was further analyzed, including gender, histology, tumor stage, smoking status, and lymph node metastasis. We observed that PD-L1 expression was significantly associated with gender (male vs. female: OR = 1.27, 95% CI:1.01–1.59, p = 0.038), histology (ADC vs. SCC: OR = 0.54, 95% CI:0.38–0.77, p = 0.001), TNM stage (I vs. II–III: OR = 0.45, 95% CI:0.34–0.60, p = 0.000), smoking status (Yes vs No: OR = 1.43,95% CI:1.14–1.80, p = 0.002) and lymph node metastasis (N+ vs N−:OR = 1.97, 95%CI:1.26–3.08, p = 0.003) (Table 2).

Table 2 The relationship between PD-L1 expression and clinicopathologic features.
In addition, we also investigated the different cutoff values of PD-L1 expression on the survival. We found that PD-L1 expression at 5% cutoff value was not correlated to DFS (HR = 1.39, 95% CI: 0.89–2.17, p = 0.142) (Supplementary Data 4), but indicated a significantly worse OS (HR = 1.93, 95% CI: 1.57–2.36, p = 0.000) (Supplementary Data 5). However, PD-L1 expression at 1% cutoff value was correlated with a poor DFS (HR = 1.76, 95% CI: 1.03–3.02, p = 0.040) (Supplementary Data 6) but not for OS (HR = 2.19, 95% CI: 0.66–7.22, p = 0.199) (Supplementary Data 7). We propose that the discrepancy for these findings may be attributed to limited data and non-uniform PD-L1 detection platforms.
Discussion
Immune checkpoint inhibitors targeting PD-1/PD-L1 have improved survival in patients with advanced NSCLC in second- and first-line settings (33–37). The PACIFIC trial reported a DFS benefit in patients with locally advanced, unresectable stage III NSCLC who received durvalumab consolidation therapy (38). Owing to the success of immune checkpoint inhibitors in advanced NSCLC, these agents are currently under investigation in the neo- or adjuvant setting for resected NSCLC patients (39–42) Therefore, it is important to understand the impact of PD-1/PD-L1 expression on the prognosis of early stage, resected NSCLC patients. Several studies have demonstrated that PD-L1 is a biomarker indicating poor prognosis and survival in advanced-stage NSCLC patients. However, as reported by previous studies, the expression of PD-L1 on the prognosis of early stage resected NSCLC remains controversial. A comprehensive analysis is required to integrate all available data and provide further insight on this issue.
By summarizing the data available from included studies, our results confirmed that the PD-L1 expression indicates an unfavorable prognosis in early stage resected NSCLC as well. Our conclusion that PD-L1 positive or high expression indicated a significantly inferior OS in early stage resected NSCLC, is consistent with the previous analysis for all stages or advanced stage NSCLC patients (9–11). Additionally, we demonstrate that DFS, which was not explored by the previous studies, is also negatively correlated with PD-L1 expression in early stage resected NSCLC. Lastly, based on subgroup analysis, we observed that the PD-L1 expression was associated with gender, histology, tumor stage, smoking status, and lymph node metastasis.
Our analysis provided evidence to support that the PD-L1 expression may have prognostic value in predicting survival of patients with resected NSCLC. However, there were several limitations to our study. Firstly, this was based on a retrospective analysis. A prospective analysis is required to further clarify these issues. Secondly, 12 out of 15 included studies were performed in Asian population. Although it was not our intention to ignore the data from non-Asian population, the lack of data from non-Asian population is still a limitation for our meta-analysis. Therefore, future investigation should focus more on the PD-L1 expression in early stage non-Asian NSCLC patients. Thirdly, the different adjuvant treatment strategies post-surgery and follow-up also influence the survival of patients with NSCLC undergoing resection, which could have influenced the analysis. Moreover, the cutoff value of the defined PD-L1 expression was rather different among the included studies. We have to categorize high (positive) and low (negative) PD-L1 expression and study the correlation between PD-L1 expression and post-operative survival. Finally, the platform and antibody of PD-L1 detection was not uniform either in the included studies. We have mentioned this issue in Table 1.
Conclusions
In conclusion, our meta-analysis suggests that PD-L1 expression indicates an unfavorable prognosis in early stage resected NSCLC patients. In the adjuvant settings resected NSCLC, the role of individualized anti-PD-L1/PD-1 immunotherapy merits further investigated.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
Author Contributions
TS, SZ, and HG retrieved and analyzed all of the data in the study. XFL, YW, XL, and SKZ revised the manuscript for important intellectual contents. LP and DH reviewed and edited the manuscript. SX, ZL, and LP designed, checked, and supervised all study processes. All authors contributed to the article and approved the submitted version.
Funding
The present study was funded by the National Natural Science Foundation of China (No. 81772464), Natural Science Foundation of Zhejiang Province, China (No. LY19H160041), Shanghai Science and Technology Commission Guidance Projects (No. 18411968200), Medical-Engineering Joint Funds from Shanghai Jiao Tong University (No. YG2017MS81) and Shanghai Chest Hospital Project of Collaborative Innovation (No. YJXT20190209).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2021.567978/full#supplementary-material
Supplementary Data Sheet 1 | The PRISMA checklist of the manuscript.
Supplementary Data Sheet 2 | The search strategy of the manuscript.
Supplementary Data Sheet 3 | The data of sensitivity analyses.
Supplementary Data Sheet 4 | Forest plot of HR for the association between PD-L1 expression and DFS with early stage resected non-small cell lung cancer. (PD-L1 expression at 5% cutoff value).
Supplementary Data Sheet 5 | Forest plot of HR for the association between PD-L1 expression and OS with early stage resected non-small cell lung cancer. (PD-L1 expression at 5% cutoff value).
Supplementary Data Sheet 6 | Forest plot of HR for the association between PD-L1 expression and DFS with early stage resected non-small cell lung cancer. (PD-L1 expression at 1% cutoff value).
Supplementary Data Sheet 7 | Forest plot of HR for the association between PD-L1 expression and OS with early stage resected non-small cell lung cancer. (PD-L1 expression at 1% cutoff value).
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thoracic Oncol (2016) 11(1):39–51. doi: 10.1016/j.jtho.2015.09.009
3. Topalian SL, Drake CG, Pardoll DM. Targeting the PD-1/B7-H1(PD-L1) pathway to activate anti-tumor immunity. Curr Opin Immunol (2012) 24(2):207–12. doi: 10.1016/j.coi.2011.12.009
4. Lu J, Lee-Gabel L, Nadeau MC, Ferencz TM, Soefje SA. Clinical evaluation of compounds targeting PD-1/PD-L1 pathway for cancer immunotherapy. J Oncol Pharm Practice (2015) 21(6):451–67. doi: 10.1177/1078155214538087
5. Inaguma S, Lasota J, Wang Z, Felisiak-Golabek A, Ikeda H, Miettinen M. Clinicopathologic profile, immunophenotype, and genotype of CD274 (PD-L1)-positive colorectal carcinomas. Modern Pathol (2017) 30(2):278–85. doi: 10.1038/modpathol.2016.185
6. Zou W, Wolchok JD, Chen L. PD-L1 (B7-H1) and PD-1 pathway blockade for cancer therapy: Mechanisms, response biomarkers, and combinations. Sci Trans Med (2016) 8(328):328rv4. doi: 10.1126/scitranslmed.aad7118
7. Zheng P, Zhou Z. Human Cancer Immunotherapy with PD-1/PD-L1 Blockade. Biomarkers Cancer (2015) 7(Suppl 2):15–8. doi: 10.4137/bic.s29325
8. Wang Y, Wang H, Yao H, Li C, Fang JY, Xu J. Regulation of PD-L1: Emerging Routes for Targeting Tumor Immune Evasion. Front Pharmacol (2018) 9:536. doi: 10.3389/fphar.2018.00536
9. Okuma Y, Hosomi Y, Nakahara Y, Watanabe K, Sagawa Y, Homma S. High plasma levels of soluble programmed cell death ligand 1 are prognostic for reduced survival in advanced lung cancer. Lung Cancer (Amsterdam Netherlands) (2017) 104:1–6. doi: 10.1016/j.lungcan.2016.11.023
10. Wang A, Wang HY, Liu Y, Zhao MC, Zhang HJ, Lu ZY, et al. The prognostic value of PD-L1 expression for non-small cell lung cancer patients: a meta-analysis. Eur J Surg Oncol (2015) 41(4):450–6. doi: 10.1016/j.ejso.2015.01.020
11. Li H, Xu Y, Wan B, Song Y, Zhan P, Hu Y, et al. The clinicopathological and prognostic significance of PD-L1 expression assessed by immunohistochemistry in lung cancer: a meta-analysis of 50 studies with 11,383 patients. Transl Lung Cancer Res (2019) 8(4):429–49. doi: 10.21037/tlcr.2019.08.04
12. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med (1998) 17(24):2815–34. doi: 10.1002/(sici)1097-0258(19981230)17:24<2815::aid-sim110>3.0.co;2-8
13. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials (2007) 8:16. doi: 10.1186/1745-6215-8-16
14. Dinnes J, Deeks J, Kirby J, Roderick P. A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy. Health Technol Assess (Winchester Engl) (2005) 9(12):1–113. doi: 10.3310/hta9120
15. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ (Clinical Res ed) (2003) 327(7414):557–60. doi: 10.1136/bmj.327.7414.557
16. Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics (1994) 50(4):1088–101.
17. Patsopoulos NA, Evangelou E, Ioannidis JP. Sensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluation. Int J Epidemiol (2008) 37(5):1148–57. doi: 10.1093/ije/dyn065
18. Kinoshita F, Takada K, Yamada Y, Oku Y, Kosai K, Ono Y, et al. Combined Evaluation of Tumor-Infiltrating CD8 + and FoxP3 + Lymphocytes Provides Accurate Prognosis in Stage IA Lung Adenocarcinoma. Ann Surg Oncol (2020) 27(6):2102–9. doi: 10.1245/s10434-019-08029-9
19. Gachechiladze M, Škarda J, Skanderová D, Überall I, Kolek V, Smičkova P, et al. Prognostic value of tumor-infiltrating lymphocytes (TILs) and their association with PD-L1 expression and DNA repair protein RAD51 in patients with resected non-small cell lung carcinoma. Lung Cancer (Amsterdam Netherlands) (2020) 147:30–8. doi: 10.1016/j.lungcan.2020.06.025
20. Li X, Xu Z, Cui G, Yu L, Zhang X. BTLA expression in stage I–III non–small-cell lung cancer and its correlation with PD-1/PD-L1 and clinical outcomes. OncoTargets Ther (2020) 13:215–24. doi: 10.2147/OTT.S232234
21. Meng X, Gao Y, Yang L, Jing H, Teng F, Huang Z, et al. Immune Microenvironment Differences Between Squamous and Non-squamous Non–small-cell Lung Cancer and Their Influence on the Prognosis. Clin Lung Cancer (2019) 20(1):48–58. doi: 10.1016/j.cllc.2018.09.012
22. Kim M, Chung YS, Kim KA, Shim HS. Prognostic factors of acinar- or papillary-predominant adenocarcinoma of the lung. Lung Cancer (Amsterdam Netherlands) (2019) 137:129–35. doi: 10.1016/j.lungcan.2019.09.026
23. Teramoto K, Igarashi T, Kataoka Y, Ishida M, Hanaoka J, Sumimoto H, et al. Clinical significance of PD-L1-positive cancer-associated fibroblasts in pN0M0 non-small cell lung cancer. Lung Cancer (Amsterdam Netherlands) (2019) 137:56–63. doi: 10.1016/j.lungcan.2019.09.013
24. Cao L, Wang X, Li S, Zhi Q, Wang Y, Wang L, et al. PD-L1 is a prognostic biomarker in resected NSCLC patients with moderate/high smoking history and elevated serum SCCA level. J Cancer (2017) 8(16):3251–60. doi: 10.7150/jca.21118
25. Song Z, Yu X, Cheng G, Zhang Y. Programmed death-ligand 1 expression associated with molecular characteristics in surgically resected lung adenocarcinoma. J Transl Med (2016) 14(1):188. doi: 10.1186/s12967-016-0943-4
26. Okita R, Maeda A, Shimizu K, Nojima Y, Saisho S, Nakata M. PD-L1 overexpression is partially regulated by EGFR/HER2 signaling and associated with poor prognosis in patients with non-small-cell lung cancer. Cancer Immunol Immunother: CII (2017) 66(7):865–76. doi: 10.1007/s00262-017-1986-y
27. Sepesi B, Cuentas EP, Canales JR, Behrens C, Correa AM, Vaporciyan A, et al. Programmed Death Cell Ligand 1 (PD-L1) Is Associated With Survival in Stage I Non-Small Cell Lung Cancer. Semin Thoracic Cardiovasc Surg (2017) 29(3):408–15. doi: 10.1053/j.semtcvs.2017.05.008
28. Imanishi N, Hirai A, Yoneda K, Shimajiri S, Kuwata T, Tashima Y, et al. Programmed death-ligand 1 (PD-L1) expression in pleomorphic carcinoma of the lung. J Surg Oncol (2018) 117(7):1563–9. doi: 10.1002/jso.25041
29. Zaric B, Brcic L, Buder A, Brandstetter A, Buresch JO, Traint S, et al. PD-1 and PD-L1 Protein Expression Predict Survival in Completely Resected Lung Adenocarcinoma. Clin Lung Cancer (2018) 19(6):e957–e63. doi: 10.1016/j.cllc.2018.08.014
30. Takamori S, Takada K, Azuma K, Jogo T, Shimokawa M, Toyokawa G, et al. Prognostic Impact of Programmed Death-Ligand 2 Expression in Primary Lung Adenocarcinoma Patients. Ann Surg Oncol (2019) 26(6):1916–24. doi: 10.1245/s10434-019-07231-z
31. Matsubara T, Takada K, Azuma K, Takamori S, Toyokawa G, Haro A, et al. A Clinicopathological and Prognostic Analysis of PD-L2 Expression in Surgically Resected Primary Lung Squamous Cell Carcinoma. Ann Surg Oncol (2019) 26(6):1925–33. doi: 10.1245/s10434-019-07257-3
32. Igawa S, Sato Y, Ryuge S, Ichinoe M, Katono K, Hiyoshi Y, et al. Impact of PD-L1 Expression in Patients with Surgically Resected Non-Small-Cell Lung Cancer. Oncology (2017) 92(5):283–90. doi: 10.1159/000458412
33. Brahmer J, Reckamp K, Baas P, Crinò L, Eberhardt W, Poddubskaya E, et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N Engl J Med (2015) 373(2):123–35. doi: 10.1056/NEJMoa1504627
34. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med (2015) 373(17):1627–39. doi: 10.1056/NEJMoa1507643
35. Herbst R, Baas P, Kim D, Felip E, Pérez-Gracia J, Han J, et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet (London Engl) (2016) 387(10027):1540–50. doi: 10.1016/S0140-6736(15)01281-7
36. Rittmeyer A, Barlesi F, Waterkamp D, Park K, Ciardiello F, von Pawel J, et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): a phase 3, open-label, multicentre randomised controlled trial. Lancet (2017) 389(10066):255–65. doi: 10.1016/s0140-6736(16)32517-x
37. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N Engl J Med (2016) 375(19):1823–33. doi: 10.1056/NEJMoa1606774
38. Antonia S, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer. N Engl J Med (2017) 377(20):1919–29. doi: 10.1056/NEJMoa1709937
39. Study of Pembrolizumab (MK-3475) vs Placebo for Participants With Non-small CellLung Cancer After Resection With or Without Standard Adjuvant Therapy (MK-3475-091/KEYNOTE-091) (PEARLS).
40. Double Blind Placebo Controlled Controlled Study of Adjuvant MEDI4736 In Completely Resected NSCLC.
41. Study to Assess Safety and Efficacy of Atezolizumab (MPDL3280A) Compared to Best Supportive Care Following Chemotherapy in Patients With Lung Cancer [IMpower010].
Keywords: PD-L1, NSCLC, meta-analysis, prognosis, resection
Citation: Shi T, Zhu S, Guo H, Li X, Zhao S, Wang Y, Lei X, Huang D, Peng L, Li Z and Xu S (2021) The Impact of Programmed Death-Ligand 1 Expression on the Prognosis of Early Stage Resected Non-Small Cell Lung Cancer: A Meta-Analysis of Literatures. Front. Oncol. 11:567978. doi: 10.3389/fonc.2021.567978
Received: 31 May 2020; Accepted: 07 January 2021;
Published: 23 February 2021.
Edited by:
Qing Zhou, Guangdong Provincial People’s Hospital Lung Cancer Institute, ChinaReviewed by:
Li Li, Army Medical University, ChinaAsrar AlAhmadi, The Ohio State University, United States
Copyright © 2021 Shi, Zhu, Guo, Li, Zhao, Wang, Lei, Huang, Peng, Li and Xu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Song Xu, eHVzb25nMTk4QGhvdG1haWwuY29t; Ziming Li, bGl6aW1pbmcxOTgwQDE2My5jb20=; Ling Peng, cGVuZ2xpbmdAemp1LmVkdS5jbg==
†These authors have contributed equally to this work