 Tianxiang Lei
Tianxiang Lei Fengbo Tan
Fengbo Tan Zhouhua Hou2
Zhouhua Hou2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 22 January 2021
Sec. Gastrointestinal Cancers
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.596500
This article is part of the Research Topic Gastric Cancer Phenotype and Treatment View all 39 articles
Purpose: Hepatitis B virus reactivation (HBVr) in patients with gastrointestinal stromal tumors (GISTs) have not been sufficiently characterized. This study aimed to review the possible mechanism of HBVr induced by imatinib and explore appropriate measures for patient management and monitoring.
Methods: The clinical data of GIST patients who experienced HBVr due to treatment with imatinib at Xiangya Hospital (Changsha, Hunan, China) were retrospectively analyzed. A literature review was also conducted.
Results: Five cases were analyzed, including 3 cases in this study. The average age of the patients was 61.8 y, with male preponderance (4 of 5 vs. 1 of 5). These patients received imatinib as adjuvant treatment (n=4) or as neoadjuvant treatment (n=1). Primary tumors were mostly located in the stomach (n=4) or rectum (n=1). High (n=3) or intermediate (n=1) recurrence risk was categorized using the postoperative pathological results (n=4). Imatinib was then started at 400 (n=4) or 200 mg (n=1) daily. Patients first reported abnormal liver function during the 2th (n=1),6th (n=3), or 10th (n=1) month of treatment with imatinib. Some patients (n=4) discontinued imatinib following HBVr; notably, 1 month after discontinuation, 1 patient experienced HBVr. Antivirals (entecavir n=4, tenofovir n=1), artificial extracorporeal liver support (n=1), and liver transplant (n=1) were effective approaches to treating HBVr. Most patients (n=3) showed favorable progress, 1 patient underwent treatment, and 1 patient died due to severe liver failure induced by HBVr.
Conclusions: Although HBVr is a rare complication (6.12%), HBV screening should be conducted before starting treatment with imatinib in GIST patients. Prophylactic therapy for hepatitis B surface antigen positive patients, prompt antiviral treatment and cessation of imatinib are also necessary.
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal neoplasms located in the digestive tract, with an estimated annual incidence of 1–2 per 100,000 globally (1, 2). Most cases of GIST have activated mutations in KIT and platelet-derived growth receptor alpha (PDGFRA). Since 2000, imatinib has been found to target KIT changes in GIST cells (3). More than 80% of GIST patients have benefited from treatment with imatinib (4). This therapy has become one of the standard treatments for GIST (5).
Hepatitis B virus reactivation (HBVr) is a common complication in tumor patients with chronic HBV infection and simultaneously undergoing cytotoxic chemotherapy or immunosuppressive therapy (6). HBV is a major global health problem chronically affecting more than 257 million people worldwide (7). However, HBVr in tumor patients may lead to liver function injury or fatal liver failure. This occurrence can interrupt therapy, delaying the effective treatment of tumor patients and consequently affecting prognosis.
However, the risk for HBVr during the treatment of GISTs by using imatinib is poorly understood. To the best of our knowledge, only 2 cases have been reported worldwide (8, 9). Thus, it is urgent to clarify the mechanism and summarize such cases in order to draw attention from the medical community and provide clinical guidance for patient management.
We retrospectively reviewed the data of 869 patients with GIST from January 2007 to June 2020 through the hospital information system of Xiangya Hospital of Central South University (Changsha, Hunan, China). A total of 440 patients received imatinib as adjuvant treatment (n=428) or neoadjuvant treatment (n=12); 49 patients tested positive for hepatitis B surface antigen (HBsAg), whereas 391 tested negative. Finally, 3 cases (6.12%) of HBVr due to imatinib for GIST were recorded. This study protocol was approved by the Medical Ethics Committee of Xiangya Hospital, Central South University (Changsha, Hunan, China).
A 50-year-old woman with a history of HBV infection over 20 years presented with abdominal pain, hematemesis, hematochezia, and even syncope on December 29, 2018. The patient had no experience using antivirals for HBV or hepatotoxic drugs. She was diagnosed with GIST by gastroscopy and abdominal-pelvic computed tomography (CT) scan. At the time of diagnosis, the patient had a normal liver function. Serologic tests for HBV showed that the patient was positive for HBsAg, hepatitis B e-antibody (HBeAb), hepatitis B core antigen (HBcAg) but negative for hepatitis B e-antigen (HBeAg) and hepatitis B surface antibody (HBsAb). The HBV DNA level was 3.10 × 104 IU/mL (normal, <10 IU/mL). The patient underwent resection of two tumors with partial resection of the stomach on January 11, 2019. Postoperative pathology confirmed the diagnosis of two gastric GISTs [size, 10.5 cm × 7 cm × 6 cm and 4 cm × 2.5 cm × 2 cm; mitosis, both>5/50 high-power field (HPF)]. Immunohistochemistry indicated that the tumors were positive for CD34, CD117, Dog1, and Ki-67 (3%). Mutational analysis demonstrated a mutation in KIT exon 11. The patient was classified as high-risk under the modified National Institutes of Health (NIH) classification system (2008) (10). To reduce the risk of tumor recurrence, administration of imatinib 400 mg daily was started postoperatively in January 2019.
On June 25, 2019, the patient presented with nausea, vomiting, and jaundice. Liver function tests showed elevated aspartate transaminase (AST) at 434.0 U/L (normal, 13.0–35.0 U/L), alanine transaminase (ALT) at 407.0 U/L (normal, 7.0–40.0 U/L), total bilirubin at 24.5 umol/L (normal, 1.7–17.1 umol/L), and direct bilirubin at 12.4 umol/L (normal, 0.0–6.8 umol/L). No change in serum HBV serology was indicated, and the HBV DNA level increased to 3.57 × 106 IU/mL. With the exclusion of other causes of liver injury such as infection with hepatitis A, C, or E virus, cytomegalovirus, Epstein-Barr virus, and autoimmune hepatitis, a diagnosis of imatinib-related chronic HBV reactivation was established. Thus, the patient immediately received entecavir (0.5 mg/d), discontinued imatinib, and took artificial extracorporeal liver support 3 times for severe liver damage. After 1 month, the symptoms and liver function abnormalities resolved. The HBV DNA level decreased to 6.59 × 102 IU/mL. After discharge, the patient continued to take entecavir (0.5 mg/d) (up to present). In January 2020, the patient resumed taking low-dose imatinib (100 mg/d), with doses increased to 200 mg/d in February 2020 and 300 mg/d from March up to present. Patient recovery was uneventful. In April 2020, her liver function subsequently remained within normal ranges, No HBV DNA was detected, and no evidence of GIST recurrence was found in the abdominal–pelvic CT scan.
A 59-year-old man without any symptoms was diagnosed with GIST by physical examination including gastroscopy in November 2018. He was diagnosed with HBV infection 20 years ago without undergoing antiviral therapy. After admission to the local hospital, he tested positive for HBsAg, HBeAb, and HBcAg but negative for HBsAb, HBeAg, hepatitis C virus, and normal liver function. He underwent laparoscopic complete stomach resection of the tumor with an uncomplicated postoperative course. The mass was diagnosed as a gastric GIST and categorized as high-risk in accordance with the modified NIH classification system (2008) (10). (size, 7 cm × 5 cm × 4 cm mitosis, >5/50 HPF). Immunohistochemistry showed the following: CD117(+), CD34(+), Dog-1(+), and Ki-67 (<8%). Adjuvant treatment with imatinib (400 mg/d) was started on December 23, 2018.
In January 2019, the patient manifested abdominal pain. Laboratory and imaging tests showed normal results. The abdominal pain resolved after symptomatic treatment. In February 2019, the patient presented with edema of eyelids, hands, and ankles as side effects of imatinib. On May 15, 2019, the patient was admitted to a local hospital because of increasing systemic edema. Owing to serious side effects, imatinib administration was stopped. From November 2018 to May 2019, the patient received imatinib (400 mg/d), and his liver function was normal. No other hepatotoxic medication, except for imatinib, was taken.
However, after discontinuing imatinib, the patient reported dizziness, body weakness, and weight loss in June 2019. The patient was immediately admitted to Xiangya hospital. Laboratory findings showed the following measurements: ALT, 977.1 U/L (normal, 7.0–40.0 U/L); AST, 1382.0 U/L (normal, 13.0–35.0 U/L); total bilirubin, 20.5 umol/L (normal, 1.7–17.1 umol/L); and direct bilirubin, 11.3 umol/L (normal, 0.0–6.8 umol/L). Serology results indicated no change in serum HBV; moreover, HBV DNA was 6.11 × 107 IU/mL (normal < 10 IU/mL), and the tumor marker CA125 was 82.73U/mL (normal, 0–35.00 U/mL). However, positron emission tomography–computed tomography did not indicate recurrence or metastasis of GIST and other tumors. Thus, HBVr was identified as the potential cause of liver damage, and the patient was immediately administered entecavir (0.5 mg/d). However, the clinical condition of the patient progressively deteriorated because of severe hepatitis caused by HBVr. The patient ultimately developed severe liver failure leading to death.
A 51-year-old man was found to have multiple hepatic masses and a gastric mass after a physical examination in September 2019. The patient subsequently underwent radical surgical resection for the gastric mass and palliative resection for the hepatic masses in a local hospital. The patient had a history of HBV infection of over 10 years but received no antiviral therapy for HBV. During hospitalization, the patient showed normal liver function, tested positive for HBsAg, HBeAb, and HBcAb, and tested negative for HBsAb, HBcAb, and hepatitis C virus. Pathological examination revealed that the gastric mass was a high-risk gastric GIST (size, 4.5 cm × 3.5 cm × 3 cm; mitotic index>10/50 HPF), which stained positive for CD117, CD34, DOG1, and ki-67 (20%). The liver mass was a metastatic GIST (the maximum tumor diameter was 1.5 cm), which stained positive for DOG1; one lymph node was metastatic (1/1). Additional molecular analysis confirmed the mutation in KIT exon 11. The liver metastases were only partly removed, requiring lifetime treatment with imatinib (400 mg/d), which the patient started to receive in January 2020.
Regular laboratory examination after treatment with imatinib for 3 months showed that the patient had mildly elevated ALT, 80.0 U/L (normal, 9.0–50.0 U/L), but no symptoms and signs. Laboratory examination after treatment with imatinib for 6 months showed further increases in ALT to 282.6 U/L (normal, 9.0–50.0 U/L), AST to 154.0 U/L (normal, 15.0–40.0 U/L), total bilirubin to 19.9 umol/L (normal, 1.7–17.1 umol/L), and direct bilirubin to 10.5 umol/L (normal, 0.0–6.8 umol/L). HBV DNA was 4.99 × 108 IU/ml (normal, < 10 IU/ml). Serology testing results showed that HBsAg and HBcAb were positive, whereas HBsAb, HBeAb, and HBeAg were negative. After excluding other causes of hepatitis, we considered that hepatitis could be attributable to HBVr. Thus, entecavir (0.5 mg/d) was administered, and imatinib was discontinued immediately. The patient now was followed up under close observation.
We performed a literature search in PubMed for other reported cases by using the terms “Hepatitis B virus reactivation”, “Gastrointestinal stromal tumors,” and “imatinib” and identified only 2 case reports (8, 9). The aforementioned cases, together with the 3 cases presented in the current study, complete the 5 cases currently reported (Table 1).
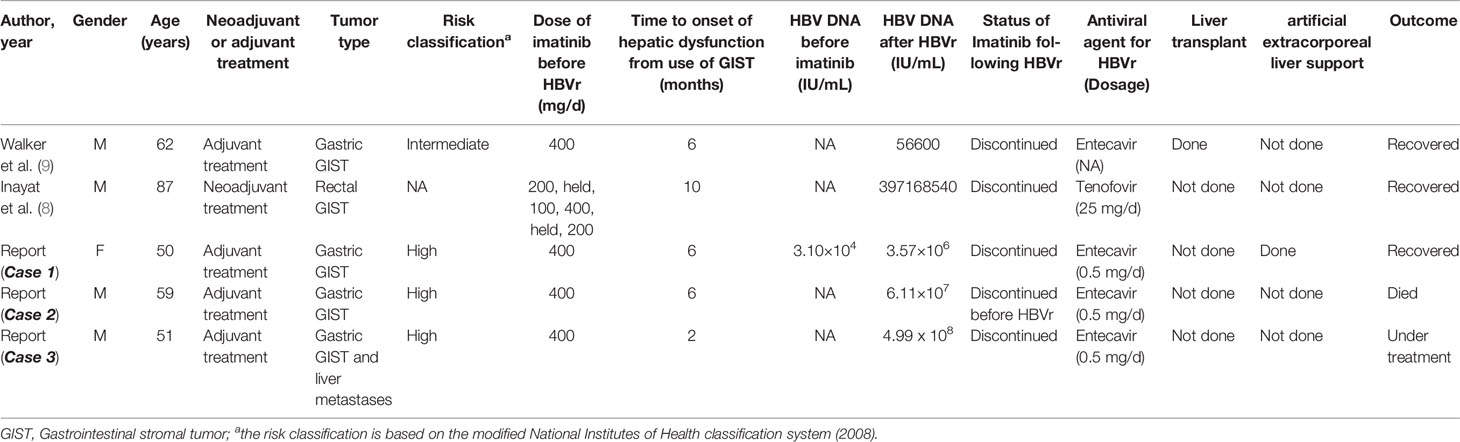
Table 1 Characteristics of cases with GIST who suffered HBV reactivation after receiving imatinib.
In the 5 cases, the average age of the patients was 61.8 y (range: 50–87 y), with a male-to-female ratio of 4:1. Four patients received imatinib as adjuvant treatment for intermediate—(n=1) or high-risk (n=3) recurrence based on the modified NIH classification system (2008) (10), and 1 patient received neoadjuvant treatment. Primary tumors were located in the stomach (n=4) or rectum (n=1), and one of our patients with a gastric GIST had liver metastasis. Imatinib at 400 mg daily was started in accordance with consensus-based medication (10) in 4 patients and 200 mg daily in 1 patient suffering from chronic kidney disease (stage 3b). Abnormal liver function was reported in 3 patients during the 6th month of treatment with imatinib at 400 mg/d and in 1 patient during the 2nd month of the same treatment at the same dose. Meanwhile 1 patient was diagnosed with HBVr during the 10th month of treatment with 6 dose adjustments of imatinib, as follows: 200 mg/d for 10 d, held for 2 weeks; 100 mg/d for 3 months; and 400 mg/d for 40 d, held for 2 weeks, and restarted at 200 mg/d imatinib. We observed the change in HBV DNA (3.10 × 104 IU/mL to 3.57 × 106 IU/mL) before and after HBVr in 1 patient, which was attributed to treatment with imatinib, as well as the high level of HBV DNA following HBVr in 4 patients.
Treatment with imatinib was stopped in all patients following HBVr. Four patients received entecavir as antiviral treatment, and 1 patient received tenofovir. Two patients accepted liver transplant or artificial extracorporeal liver support to reverse the deterioration of their liver function. Three patients successfully recovered, 1 patient underwent treatment, and 1 patient died due to severe liver failure.
Imatinib has indeed changed the fate of patients with GIST and Philadelphia chromosome-positive chronic myeloid leukemia by targeting the oncogenic drivers of these diseases—BCR–ABL1 and KIT and/or PDGFRA—mutations that promote the function of tyrosine kinase activities (11). The importance of imatinib, as the mainstay of treatment for GIST, has been emphasized in various clinical guidelines (10, 12, 13). The side effects of imatinib are usually mild and generally well tolerated by most GIST patients (14). HBVr rarely occurs in patients infected with chronic HBV. However, when GIST patients with chronic HBV infection receive imatinib, the risk for HBVr is present. Without timely adequate recognition and treatment, HBVr can lead to an unfavorable prognosis or even death, such as that in Case 2, or increase the risk of tumor recurrence and progression, such as that in Case 3. GIST patients with chronic HBV infection and treated with imatinib rarely suffer from HBVr; regardless, these cases need to be consolidated to raise awareness of complications.
No unified diagnostic criteria for HBVr have been established worldwide; however, a consensus has been reached for patients with HBsAg(+)/HBcAb(-) or HBsAg(-)/HBcAb(+) receiving immunosuppressive therapy or chemotherapy. HBVr is defined as the occurrence of any of the following: a hundredfold increase in the HBV DNA level, the recurrence of detectable HBV DNA or positive HBsAg, or HBV DNA > 105 IU/mL without a previously known HBV DNA level baseline (7, 15). Imatinib-induced hepatotoxicity has been reported and the incidence is less than 2.5% in patients with GIST (16); however, liver dysfunction usually resolves with either dose reduction or the discontinuation of the drug, which clearly contradicts Case 2 in the current study. Thus, the 3 cases presented meet the definition of HBVr. Notably, HBVr occurs not only in patients with overt chronic HBV infection but also in patients with resolved HBV infection (17).
HBVr is usually divided into two stages: (i) immediately after immunosuppressive therapy with the induction of HBV replication, reflecting a sharp increase in serum HBV DNA, and (ii) during withdrawal or a decrease in immune suppression. In stage (ii), patients tend to develop immune reconstitution that may lead to hepatocellular injury and even liver failure (18).
The mechanism by which imatinib induces HBVr has yet to be determined. However, a review of the relevant literature suggests that imatinib is directly and/or indirectly (by immunosuppressive function) involved in HBVr (Table 2). HBV covalently closed circular DNA and low levels of HBV DNA and RNA can be detected in host hepatocytes even in patients who have recovered from HBV and produced HBsAg after complete clearance of serum HBsAg and HBV DNA from a recent infection (26). When the immunity of the body, particularly the cellular immune function, is inhibited, viral replication increases, inducing an imbalance in the mechanisms that lead to HBVr (27). The imbalance between host immune response and HBV replication seem to indirectly cause HBVr. Although imatinib was not defined as an immunosuppressant, evidence has suggested that it exhibits an immunoregulatory effect. Imatinib at 400–800 mg/d inhibits the differentiation and function of dendritic cells (DCs), reducing the efficiency of priming cytotoxic T cell lymphocytes (CTLs) (19, 20). It also reduces memory B-cell frequencies and the secondary expansion of memory CTLs, resulting in impaired protection against reinfection (21, 22). Moreover, several in vitro studies using T cells isolated from human peripheral blood have demonstrated a dose-dependent reduction in T-cell proliferation and activation in the presence of imatinib (23, 24). Imatinib also inhibits immunity to several disease, such as herpes zoster infection (28), tuberculosis (29), Epstein Barr Virus-positive lymphoproliferative disease (30), and sclerotic-type chronic graft-versus-host disease, in addition to HBVr (31). However, imatinib can stimulate anticancer responses mediated by T cells, interferon-producing killer DCs and NK cells in patients (11, 32–34). Thus, further research is needed to distinguish the difference in effect of imatinib between viral immunity regulation and tumor immunity regulation.
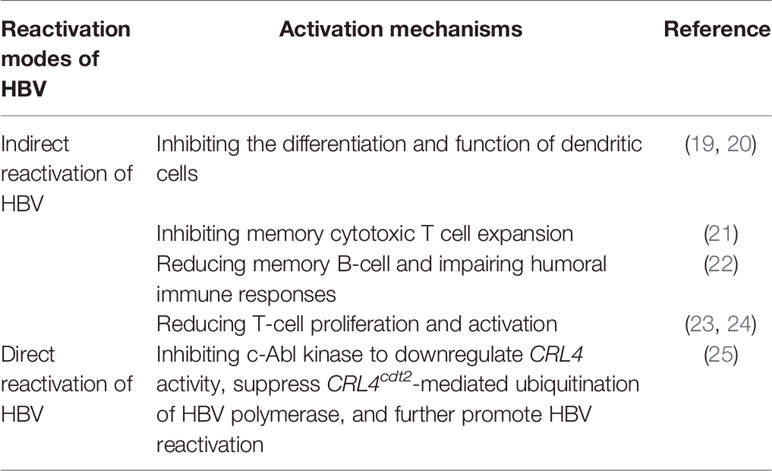
Table 2 Mechanism of Hepatitis B virus reactivation induced by imatinib.
In addition to indirect reactivation by immunosuppression, imatinib can directly activate HBV. Moreover, c-Abl kinase promotes the CRL4Cdt2 mediated ubiquitination of HBV polymerase and further suppresses HBV replication. However, inhibiting c-Abl kinase activity with imatinib can lead to the accumulation of HBV polymerase protein and release of HBV, and consequently to HBVr (25). Clinical HBV replication in patients with chronic HBV may be activated via direct and indirect pathways; however the exact mechanism of HBVr induced by imatinib is unknown and needs further study.
With the introduction of imatinib, GIST patients often have a good prognosis of long-term survival and quality of life. However, some patients develop HBVr, causing acute fatal liver failure and even death. According to the guideline (35), imatinib is associated with a moderate risk (1% to 10% incidence rate of HBVr). Therefore, early prevention, diagnosis, and treatment of HBVr are extremely significant for GIST patients receiving imatinib therapy.
Prompt identification of HBV-infected patients is mandatory before administering imatinib to prevent HBVr (36). HBV prophylaxis, identification of HBV patients, or reactivation monitoring can effectively prevent imatinib discontinuation. Conducting HBsAg and HBcAb tests is widely recommended before administering immunosuppressors (37, 38). If chronic HBV infection is evident, HBsAb, HBeAg, HBeAb, and HBV DNA may be tested selectively for risk stratification (39). HBsAg-positive tumor patients are suggested to undergo antiviral therapy 1 week before receiving immunosuppressors or are given antivirals and imatinib simultaneously and continue to suppress the risk for HBVr during treatment. The reason is that HBVr-induced hepatitis is more difficult to control and cure (37). Prophylactic therapy can potentially reduce the incidence of HBVr (40). ALT, AST and HBV DNA should be tested every 3 to 6 months during prophylaxis (6). Moreover, HBcAb-positive and HBsAg-negative GIST patients should be monitored every 1-3 months for their ALT, HBV DNA and HBsAg levels during treatment (6, 41). If the tests turn positive under close surveillance, antiviral treatment is started immediately (42). In principle, both therapy for HBV patients with normal immunity function and therapy for HBVr patients should reach the same therapeutic endpoint (43). GIST patients receiving antivirals during treatment with imatinib need to continue their antivirals for 6–12 months after treatment with imatinib (37, 44).
When GIST patients experience HBVr, treatment with imatinib should be stopped, and antiviral treatment should be immediately initiated to avoid unfavorable outcomes. As soon as HBVr was evident, imatinib was instantly discontinued in 4 (except Case 2) of the 5 cases presented. Most patients had a good prognosis. Owing to its efficacy in reducing the occurrence of HBVr, lamivudine is widely used in the treatment of cancer patients undergoin g chemotherapy (45). However, long-term use of lamivudine may lead to HBV resistance mutations and drug resistance. Compared with lamivudine, some more recent drugs such as entecavir may reduce the risk of drug resistance (46). Numerous studies (47, 48) have shown that entecavir can effectively inhibit viral replication and improve liver inflammation; moreover, it has an adequate safety index. Thus, entecavir is often considered as a first-line agent. Tenofovir disoproxil fumarate and tenofovir alafenamide fumarate also provide alternatives (49, 50).
One patient had artificial extracorporeal liver support and another patient had a liver transplant, and each had a good prognosis. Although some GIST patients with HBVr underwent antiviral and supportive treatment, their liver function still deteriorated. If liver injury could not be controlled by antivirals and liver-protective drugs, prompt artificial extracorporeal liver support as treatment choice would save the patient as in Case 1. For a favorable prognosis, a liver transplant is also a therapeutic choice (the case in Walker’s study) for patients with tumors (such as GIST) and suffering acute liver failure.
However, our study has several limitations. First, a small number of cases was included in the review, and the follow-up period was short. Second, this study is a retrospective study with possible selection bias. Third, the management and monitoring of HBVr in patients with GIST were not based on research concerning GIST patients with HBVr induced by imatinib but were merely suggested as feasible by current clinical evidence. More prospective clinical random control trials are needed to improve clinical understanding of severe complications.
HBVr has a relatively low incidence rate (6.12%). Regardless, the occurrence of HBVr in GIST patients undergoing treatment with imatinib cannot be ignored, particularly in China, which has a high rate of HBV infection. HBVr prophylaxis and monitoring seem effective and safe for the management of these patients. Thus, serology testing for HBsAg and HBcAb in GIST patients and prophylactic therapy for patients at high risk for HBVr needs to be conducted prior to the initiation of treatment with imatinib. Meanwhile, cessation of treatment with imatinib and initiation of antiviral therapy are mandatory following HBVr.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Xiangya Hospital of Central South University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
TL was the lead investigator and contributed to writing the article. HL, FT, and ZH were the chief investigator and the senior author of the article. PL and XZ assisted with setting up the project and its promotion and helped with editing of the report. All authors contributed to the article and approved the submitted version.
This study was supported by the Hunan Provincial Clinical Medical Technology Innovation Guidance Project, China (2018SK52604).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
ALT, alanine transaminase; AST, aspartate transaminase; CT, computed tomography; GISTs, gastrointestinal stromal tumors; HBcAg, hepatitis B core antigen; HBeAb, hepatitis B e-antibody; HBeAg, hepatitis B e-antigen; HBsAb, hepatitis B surface antibody; HBsAg, hepatitis B surface antigen; HPF, high-power field; HBVr, hepatitis B virus reactivation; NIH, National Institutes of Health; PDGFRA, platelet-derived growth receptor alpha.
1. von Mehren M, Randall RL, Benjamin RS, Boles S, Bui MM, Ganjoo KN, et al. Soft Tissue Sarcoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw (2018) 16(5):536–63. doi: 10.6004/jnccn.2018.0025
2. Mantese G. Gastrointestinal stromal tumor: epidemiology, diagnosis, and treatment. Curr Opin Gastroenterol (2019) 35(6):555–9. doi: 10.1097/MOG.0000000000000584
3. Joensuu H, Roberts PJ, Sarlomo-Rikala M, Andersson LC, Tervahartiala P, Tuveson D, et al. Effect of the tyrosine kinase inhibitor STI571 in a patient with a metastatic gastrointestinal stromal tumor. N Engl J Med (2001) 344(14):1052–6. doi: 10.1056/NEJM200104053441404
4. Verweij J, Casali PG, Zalcberg J, LeCesne A, Reichardt P, Blay JY, et al. Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: randomised trial. Lancet (2004) 364(9440):1127–34. doi: 10.1016/S0140-6736(04)17098-0
5. Chang SC, Liao CH, Wang SY, Tsai CY, Chiang KC, Cheng CT, et al. Feasibility and Timing of Cytoreduction Surgery in Advanced (Metastatic or Recurrent) Gastrointestinal Stromal Tumors During the Era of Imatinib. Med (Baltimore) (2015) 94(24):e1014. doi: 10.1097/MD.0000000000001014
6. European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol (2017) 67(2):370–98. doi: 10.1016/j.jhep.2017.03.021
7. Chinese Society of Infectious Diseases CMA. Chinese Society of Hepatology CMA. [The guidelines of prevention and treatment for chronic hepatitis B (2019 version)]. Zhonghua Gan Zang Bing Za Zhi (2019) 27(12):938–61. doi: 10.3760/cma.j.issn.1007-3418.2019.12.007
8. Inayat F, Song F, Ali NS, Aslam MH, Aloma A, Hachem H, et al. Hepatitis B virus reactivation following imatinib therapy: A comparative review of 9 cases. J Oncol Pharm Pract (2019) 25(6):1500–8. doi: 10.1177/1078155218790337
9. Walker EJ, Simko JP, Ko AH. Hepatitis B viral reactivation secondary to imatinib treatment in a patient with gastrointestinal stromal tumor. Anticancer Res (2014) 34(7):3629–34.
10. Li J, Ye Y, Wang J, Zhang B, Qin S, Shi Y, et al. Chinese consensus guidelines for diagnosis and management of gastrointestinal stromal tumor. Chin J Cancer Res (2017) 29(4):281–93. doi: 10.21147/j.issn.1000-9604.2017.04.01
11. Zitvogel L, Rusakiewicz S, Routy B, Ayyoub M, Kroemer G. Immunological off-target effects of imatinib. Nat Rev Clin Oncol (2016) 13(7):431–46. doi: 10.1038/nrclinonc.2016.41
12. Casali PG, Abecassis N, Bauer S, Biagini R, Bielack S, Bonvalot S, et al. Gastrointestinal stromal tumours: ESMO–EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol (2018) 29:iv68–78. doi: 10.1093/annonc/mdy095
13. Landi B, Blay JY, Bonvalot S, Brasseur M, Coindre JM, Emile JF, et al. Gastrointestinal stromal tumours (GISTs): French Intergroup Clinical Practice Guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO). Dig Liver Dis (2019) 51(9):1223–31. doi: 10.1016/j.dld.2019.07.006
14. Waller CF. Imatinib Mesylate. Recent Results Cancer Res (2018) 212:1–27. doi: 10.1007/978-3-319-91439-8_1
15. Choi J, Lim YS. Characteristics, Prevention, and Management of Hepatitis B Virus (HBV) Reactivation in HBV-Infected Patients Who Require Immunosuppressive Therapy. J Infect Dis (2017) 216(suppl_8):S778–S84. doi: 10.1093/infdis/jix178
16. Seidel C, Fenner M, Langer F, Bantel H, Ganser A, Grunwald V. Imatinib-induced liver cirrhosis in a patient with advanced gastrointestinal stroma tumor (GIST). BMC Cancer (2012) 12:186. doi: 10.1186/1471-2407-12-186
17. Masarone M, De Renzo A, La Mura V, Sasso FC, Romano M, Signoriello G, et al. Management of the HBV reactivation in isolated HBcAb positive patients affected with Non Hodgkin Lymphoma. BMC Gastroenterol (2014) 14:31. doi: 10.1186/1471-230X-14-31
18. Hoofnagle JH. Reactivation of hepatitis B. Hepatology (2009) 49(5 Suppl):S156–65. doi: 10.1002/hep.22945
19. Boissel N, Rousselot P, Raffoux E, Cayuela JM, Maarek O, Charron D, et al. Defective blood dendritic cells in chronic myeloid leukemia correlate with high plasmatic VEGF and are not normalized by imatinib mesylate. Leukemia (2004) 18(10):1656–61. doi: 10.1038/sj.leu.2403474
20. Appel S, Boehmler AM, Grunebach F, Muller MR, Rupf A, Weck MM, et al. Imatinib mesylate affects the development and function of dendritic cells generated from CD34+ peripheral blood progenitor cells. Blood (2004) 103(2):538–44. doi: 10.1182/blood-2003-03-0975
21. Mumprecht S, Matter M, Pavelic V, Ochsenbein AF. Imatinib mesylate selectively impairs expansion of memory cytotoxic T cells without affecting the control of primary viral infections. Blood (2006) 108(10):3406–13. doi: 10.1182/blood-2006-04-018705
22. de Lavallade H, Khoder A, Hart M, Sarvaria A, Sekine T, Alsuliman A, et al. Tyrosine kinase inhibitors impair B-cell immune responses in CML through off-target inhibition of kinases important for cell signaling. Blood (2013) 122(2):227–38. doi: 10.1182/blood-2012-11-465039
23. Seggewiss R, Lore K, Greiner E, Magnusson MK, Price DA, Douek DC, et al. Imatinib inhibits T-cell receptor-mediated T-cell proliferation and activation in a dose-dependent manner. Blood (2005) 105(6):2473–9. doi: 10.1182/blood-2004-07-2527
24. Dietz AB, Souan L, Knutson GJ, Bulur PA, Litzow MR, Vuk-Pavlovic S. Imatinib mesylate inhibits T-cell proliferation in vitro and delayed-type hypersensitivity in vivo. Blood (2004) 104(4):1094–9. doi: 10.1182/blood-2003-12-4266
25. Hou L, Zhao J, Gao S, Ji T, Song T, Li Y, et al. Restriction of hepatitis B virus replication by c-Abl-induced proteasomal degradation of the viral polymerase. Sci Adv (2019) 5(2):eaau7130. doi: 10.1126/sciadv.aau7130
26. Yang HC, Kao JH. Persistence of hepatitis B virus covalently closed circular DNA in hepatocytes: molecular mechanisms and clinical significance. Emerg Microbes Infect (2014) 3(9):e64. doi: 10.1038/emi.2014.64
27. Oh MJ, Lee HJ. A study of hepatitis B virus reactivation associated with rituximab therapy in real-world clinical practice: a single-center experience. Clin Mol Hepatol (2013) 19(1):51–9. doi: 10.3350/cmh.2013.19.1.51
28. Mattiuzzi GN, Cortes JE, Talpaz M, Reuben J, Rios MB, Shan J, et al. Development of Varicella-Zoster virus infection in patients with chronic myelogenous leukemia treated with imatinib mesylate. Clin Cancer Res (2003) 9(3):976–80.
29. Daniels JM, Vonk-Noordegraaf A, Janssen JJ, Postmus PE, van Altena R. Tuberculosis complicating imatinib treatment for chronic myeloid leukaemia. Eur Respir J (2009) 33(3):670–2. doi: 10.1183/09031936.00025408
30. Bekkenk MW, Vermeer MH, Meijer CJ, Jansen PM, Middeldorp JM, Stevens SJ, et al. EBV-positive cutaneous B-cell lymphoproliferative disease after imatinib mesylate. Blood (2003) 102(12):4243. doi: 10.1182/blood-2003-07-2436
31. Arai S, Pidala J, Pusic I, Chai X, Jaglowski S, Khera N, et al. A Randomized Phase II Crossover Study of Imatinib or Rituximab for Cutaneous Sclerosis after Hematopoietic Cell Transplantation. Clin Cancer Res (2016) 22(2):319–27. doi: 10.1158/1078-0432.CCR-15-1443
32. Balachandran VP, Cavnar MJ, Zeng S, Bamboat ZM, Ocuin LM, Obaid H, et al. Imatinib potentiates antitumor T cell responses in gastrointestinal stromal tumor through the inhibition of Ido. Nat Med (2011) 17(9):1094–100. doi: 10.1038/nm.2438
33. Larmonier N, Janikashvili N, LaCasse CJ, Larmonier CB, Cantrell J, Situ E, et al. Imatinib mesylate inhibits CD4+ CD25+ regulatory T cell activity and enhances active immunotherapy against BCR-ABL- tumors. J Immunol (2008) 181(10):6955–63. doi: 10.4049/jimmunol.181.10.6955
34. Smyth MJ. Imatinib mesylate–uncovering a fast track to adaptive immunity. N Engl J Med (2006) 354(21):2282–4. doi: 10.1056/NEJMcibr061878
35. Perrillo RP, Gish R, Falck-Ytter YT. American Gastroenterological Association Institute technical review on prevention and treatment of hepatitis B virus reactivation during immunosuppressive drug therapy. Gastroenterology (2015) 148(1):221–44.e3. doi: 10.1053/j.gastro.2014.10.038
36. Kusumoto S, Tobinai K. Screening for and management of hepatitis B virus reactivation in patients treated with anti-B-cell therapy. Hematol Am Soc Hematol Educ Program (2014) 2014(1):576–83. doi: 10.1182/asheducation-2014.1.576
37. Terrault NA, Lok ASF, McMahon BJ, Chang KM, Hwang JP, Jonas MM, et al. Update on Prevention, Diagnosis, and Treatment of Chronic Hepatitis B: AASLD 2018 Hepatitis B Guidance. Clin Liver Dis (Hoboken) (2018) 12(1):33–4. doi: 10.1002/cld.728
38. Jang JW, Choi JY, Bae SH, Yoon SK, Chang UI, Kim CW, et al. A randomized controlled study of preemptive lamivudine in patients receiving transarterial chemo-lipiodolization. Hepatology (2006) 43(2):233–40. doi: 10.1002/hep.21024
39. Huang SC, Yang HC, Kao JH. Hepatitis B reactivation: diagnosis and management. Expert Rev Gastroenterol Hepatol (2020) 14(7):565–78. doi: 10.1080/17474124.2020.1774364
40. Liu CJ, Chen PJ, Chen DS, Kao JH. Hepatitis B virus reactivation in patients receiving cancer chemotherapy: natural history, pathogenesis, and management. Hepatol Int (2013) 7(2):316–26. doi: 10.1007/s12072-011-9279-6
41. Law MF, Ho R, Cheung CK, Tam LH, Ma K, So KC, et al. Prevention and management of hepatitis B virus reactivation in patients with hematological malignancies treated with anticancer therapy. World J Gastroenterol (2016) 22(28):6484–500. doi: 10.3748/wjg.v22.i28.6484
42. Liu WP, Xiao XB, Xue M, Wang GQ, Wang XP, Song YQ, et al. Prophylactic Use of Entecavir for Lymphoma Patients With Past Hepatitis B Virus Infection: A Randomized Controlled Trial. Clin Lymphoma Myeloma Leuk (2019) 19(2):103–8. doi: 10.1016/j.clml.2018.11.008
43. Sarri G, Westby M, Bermingham S, Hill-Cawthorne G, Thomas H, Guideline Development G. Diagnosis and management of chronic hepatitis B in children, young people, and adults: summary of NICE guidance. BMJ (2013) 346:f3893. doi: 10.1136/bmj.f3893
44. Sarin SK, Kumar M, Lau GK, Abbas Z, Chan HL, Chen CJ, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int (2016) 10(1):1–98. doi: 10.1007/s12072-015-9675-4
45. Loomba R, Rowley A, Wesley R, Liang TJ, Hoofnagle JH, Pucino F, et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann Intern Med (2008) 148(7):519–28. doi: 10.7326/0003-4819-148-7-200804010-00008
46. Tang LSY, Covert E, Wilson E, Kottilil S. Chronic Hepatitis B Infection: A Review. JAMA (2018) 319(17):1802–13. doi: 10.1001/jama.2018.3795
47. Chang TT, Gish RG, de Man R, Gadano A, Sollano J, Chao YC, et al. A comparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med (2006) 354(10):1001–10. doi: 10.1056/NEJMoa051285
48. Chang TT, Lai CL, Kew Yoon S, Lee SS, Coelho HS, Carrilho FJ, et al. Entecavir treatment for up to 5 years in patients with hepatitis B e antigen-positive chronic hepatitis B. Hepatology (2010) 51(2):422–30. doi: 10.1002/hep.23327
49. Gentile G, Andreoni M, Antonelli G, Sarmati L. Screening, monitoring, prevention, prophylaxis and therapy for hepatitis B virus reactivation in patients with haematologic malignancies and patients who underwent haematologic stem cell transplantation: a systematic review. Clin Microbiol Infect (2017) 23(12):916–23. doi: 10.1016/j.cmi.2017.06.024
50. Sarmati L, Andreoni M, Antonelli G, Arcese W, Bruno R, Coppola N, et al. Recommendations for screening, monitoring, prevention, prophylaxis and therapy of hepatitis B virus reactivation in patients with haematologic malignancies and patients who underwent haematologic stem cell transplantation-a position paper. Clin Microbiol Infect (2017) 23(12):935–40. doi: 10.1016/j.cmi.2017.06.023
Keywords: hepatitis B virus, reactivation, gastrointestinal stromal tumors, imatinib, mechanism
Citation: Lei T, Tan F, Hou Z, Liu P, Zhao X and Liu H (2021) Hepatitis B Virus Reactivation in Gastrointestinal Stromal Tumor Patients Treated With Imatinib. Front. Oncol. 10:596500. doi: 10.3389/fonc.2020.596500
Received: 19 August 2020; Accepted: 07 December 2020;
Published: 22 January 2021.
Edited by:
Domenico M. D’Ugo, Catholic University of the Sacred Heart, ItalyReviewed by:
Manidhar Reddy Lekkala, University of Rochester, United StatesCopyright © 2021 Lei, Tan, Hou, Liu, Zhao and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heli Liu, aGVsaWxpdUBjc3UuZWR1LmNu
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.