 Marta Laganà1
Marta Laganà1 Cristina Gurizzan1
Cristina Gurizzan1 Elisa Roca1
Elisa Roca1 Diego Cortinovis2Diego Signorelli3Filippo Pagani3Anna Bettini4Lucia Bonomi4Silvia Rinaldi5
Diego Cortinovis2Diego Signorelli3Filippo Pagani3Anna Bettini4Lucia Bonomi4Silvia Rinaldi5 Rossana Berardi5Marco Filetti6
Rossana Berardi5Marco Filetti6 Raffaele Giusti6Sara Pilotto7Michele Milella7Salvatore Intagliata1Alice Baggi1
Raffaele Giusti6Sara Pilotto7Michele Milella7Salvatore Intagliata1Alice Baggi1 Alessio Cortellini8Hector Soto Parra9Matteo Brighenti10
Alessio Cortellini8Hector Soto Parra9Matteo Brighenti10 Fausto Petrelli11Chiara Bennati12Paolo Bidoli2
Fausto Petrelli11Chiara Bennati12Paolo Bidoli2 Marina Chiara Garassino3
Marina Chiara Garassino3 Alfredo Berruti1*
Alfredo Berruti1*- 1Medical Oncology, Department of Medical and Surgical Specialties, Radiological Sciences and Public Health University of Brescia, ASST-Spedali Civili, Brescia, Italy
- 2Medical Oncology, Ospedale S. Gerardo di Monza, Monza, Italy
- 3Medical Oncology, Fondazione IRCCS Istituto Nazionale Tumori, Milano, Italy
- 4Medical Oncology, ASST Papa Giovanni XXIII di Bergamo, Bergamo, Italy
- 5Medical Oncology, Ospedali Riuniti di Ancona, Ancona, Italy
- 6Medical Oncology, Azienda Ospedaliero Universitaria S. Andrea di Roma, Roma, Italy
- 7Medical Oncology, Università degli studi di Verona, Azienda Ospedaliera Universitaria Integrata, Verona, Italy
- 8Medical Oncology, Ospedale San Salvatore di L’Aquila, L’Aquila, Italy
- 9Medical Oncology, Policlinico Vittorio Emanuele di Catania, Catania, Italy
- 10Medical Oncology, Ospedale di Cremona, Cremona, Italy
- 11Ospedale Treviglio, ASST Bergamo Ovest, Treviglio, Italy
- 12Ospedale Santa Maria delle Croci di Ravenna, Ravenna, Italy
Objectives: The prevalence of Skeletal Related Adverse Events (SREs) in EGFR mutated non-small cell lung cancer (NSCLC) patients with bone metastases, treated with modern tyrosine kinase inhibitors (TKIs), has been scarcely investigated.
Materials and Methods: We retrospectively evaluated the data of EGFR mutated NSCLC patients with bone metastases treated with TKIs in 12 Italian centers from 2014 to 2019, with the primary aim to explore type and frequency of SREs.
Results: Seventy-seven out of 274 patients enrolled (28%) developed at least one major SRE: 55/274 (20%) bone fractures, 30/274 (11%) spinal cord compression, 5/274 (2%) hypercalcemia. Median time to the onset of SRE was 3.63 months. Nine patients (3%) underwent bone surgery and 150 (55%) radiation therapy on bone. SREs were more frequently observed within the 12 months from TKI start than afterwards (71 vs 29%, p 0.000). Patient Performance Status and liver metastases where independently associated with the risk of developing SREs. Median TKI exposure and overall survival were 11 and 28 months, respectively. Bone resorption inhibitors were associated with a lower risk of death (HR 0.722, 95% CI: 0.504–1.033, p = 0.075) although not statistically significant at multivariate analysis.
Conclusion: Bone metastatic NSCLC patients with EGFR mutated disease, treated with EGFR TKIs, have a relatively long survival expectancy and are at high risk to develop SREs. The early SRE occurrence after the TKI start provides the rationale to administer bone resorption inhibitors.
Introduction
Lung cancer is the leading cause of cancer death worldwide (1).
Despite the introduction of modern efficacious therapies, the prognosis of patients with metastatic disease still remains poor although highly variable, being dependent on genomic abnormalities and programmed death-ligand 1 (PD-L1) expression (2).
Genetic analysis allows the identification of somatic sensitizing mutations in epidermal growth factor receptor (EGFR), typically exon 19 deletion (Ex19del) and L858R. These mutations are found in among 15% of lung adenocarcinoma in European patients (2).
First- or second-generation EGFR tyrosine kinase inhibitors (EGFR-TKIs) (e.g., erlotinib, gefitinib, and afatinib), administered to patients whose tumors harbor these genotype alterations, led to marked tumor response and improved progression-free survival and quality of life over chemotherapy (3–5). Thanks to these efficacious drugs the overall survival of patients with activating EGFR mutations has increased from a median of 7.9 months in 2002 to 27.3 months in 2015 (6).
The prognosis of these patients is destined to further improve with the recent introduction in clinics of the third generation EGFR-TKI osimertinib (7).
NSCLC often metastasizes to bone and the frequency of bone metastasis (BM) is 30–40% during the clinical course of the disease (8).
The diagnosis of BM negatively impacts on patient’s quality of life (QoL) and is associated with poor survival (9). About 80% of bone metastatic lung cancer patients experience significant pain and more than 60% develop skeletal-related events (SREs), usually defined as bone surgery, bone radiation therapy, pathological fractures, spinal cord compression, and hypercalcemia (9).
SREs is therefore a composite endpoint, which encompasses both major complications, such as fractures, spinal cord compression, hypercalcemia, and local bone treatments, such as surgery and radiation therapy (10).
Published randomized clinical trials did not report whether the greater benefit obtained by modern TKIs over chemotherapy could translate or not into a fewer proportion of SREs (11).
The therapeutic strategies to manage BM and reduce the incidence of SREs include the administration of bisphosphonates (i.e. zoledronic acid) and Receptor Activator of Nuclear factor Kappa B Ligand (RANKL) inhibitors (denosumab). The results of a randomized prospective placebo controlled clinical trial have demonstrated that zoledronic acid is efficacious in preventing and delaying the SRE onset in lung cancer patients with bone metastases (10). In the same patient population, a subsequent prospective phase III randomized clinical trial demonstrated the superiority of denosumab over zoledronic acid in terms of prevention and delay of SREs (12). These randomized clinical trials were conducted before the introduction of TKIs in the management of lung cancer.
In this paper, we present the results of a retrospective multicenter study aiming to define the prevalence of SREs in EGFR mutated NSCLC patients, treated with first/second generation TKIs.
We also investigated the natural history of EGFR mutated NSCLC with BM, the prognostic factors, and the impact of bone resorption inhibitors on patient’s outcome.
Patients and Methods
Study Design
We conducted a retrospective, observational, multicenter study. Medical records of patients with bone metastases from EGFR-mutated NSCLC, treated with TKIs in 12 referral Italian centers from 2014 to 2019, were analyzed.
The primary aim of the study was to estimate the frequency of SREs. Secondary endpoints were to define in this study population overall survival, time to TKIs exposure and time to SRE. We also explored, both in univariate and multivariate analyses, prognostic factors, and factors predictive of SREs.
To be included in our study adult patients (≥18 years) with EGFR-mutated lung adenocarcinoma should have had bone metastatic involvement either at diagnosis or during the disease course (synchronous versus metachronous bone metastases) and identified through imaging assessment (e.g. standard x-rays, computed tomography scans, magnetic resonance imaging, or 18fluoro-deoxy-glucose positron-emission tomography of the skeleton). Patients with bone invasion by contiguity were excluded.
Clinical data were collected in an anonymized database, including demographic data such as age at cancer diagnosis, gender, Performance Status (PS) according to ECOG, major comorbidities, current or past smoking history, site and number of visceral metastases. We also recorded pathological data, including EGFR mutations, and blood chemistry data: i.e. alkaline phosphatase (ALP), lactate dehydrogenase (LDH), hemoglobin (HB).
For each patient, the type of TKI used was collected, specifying date of start and end of treatment. Dates of disease progression under TKI therapy (defined according Response Evaluation Criteria in Solid Tumors [RECIST] version 1.1), last follow-up, or death were also recorded.
Regarding bone involvement, the following data were collected: time of onset of BMs, if BMs were synchronous or metachronous with respect to first disease diagnosis; if they were osteolytic, osteoblastic, or mixed; and the number of bone sites involved. Furthermore, data about the occurrence of SREs, i.e. pathological fractures, hypercalcemia, spinal cord compression, bone radiotherapy, and bone surgery, were collected as well as whether a specific bone anti-resorptive treatment (bisphosphonates or denosumab) was introduced or not.
The study was firstly approved by the Institutional Review Board of the Coordinating Center in Brescia (SURMOS Study no. NP1848) and subsequently by the ethic committees of each participating institution.
SURMOS study was conducted in accordance with the Declaration of Helsinki for clinical studies.
Statistical Analysis
The primary endpoint was to define the prevalence of major SREs (fractures, spinal cord compression, and hypercalcemia) in EGFR mutated NSCLC patients with bone metastases, treated with TKIs.
Among secondary endpoints, we evaluated: 1) the prevalence of SREs according to standard definition (including also bone surgery and bone radiation therapy), 2) overall survival, that was defined as the time interval between the date of diagnosis of bone metastases and the date of death or the last known alive date, 3) time between primary diagnosis and occurrence of bone metastases, 4) time to the occurrence of SRE from the diagnosis of bone metastases, i.e. the interval between date of diagnosis of bone metastases to the first occurrence of either bone fracture, spinal cord compression, or hypercalcemia, and 5) time of TKI exposure (from the start to the end of TKI treatment, even beyond disease progression).
Descriptive statistics were used for patients’ demographics, tumor characteristics, and frequency of SREs. Categorized variables were expressed as percentages. Cut-off points were identified for continuous variables based on the median value or upper limit of normal ranges (for biochemical parameters).
Survival curves were calculated by the Kaplan-Meier method and differences compared by the log-rank test. The Cox’s proportional hazards regression model was employed to assess the Hazard ratios (HRs) and 95% confidence intervals (95% CIs) both in univariate and multivariate analyses, with the lowest risk group as the reference group. Only parameters significantly associated with OS or time to SRE in the univariate analysis (at p < 0.10) were included in the multivariate analysis model.
All p values are two-sided and p values less than 0.05 were considered statistically significant. Due to the explorative nature of this study, a formal calculation of the sample size was not performed. It was considered, however, that a minimum of 200 patients would have been required to have an adequate power for statistical analyses. Statistical Package for Social Science, SPSS, software (version 23.00, Chicago, IL, USA) was used for statistical analysis.
Results
Patient Characteristics and Treatment Administered
A total of 274 patients with bone metastatic, EGFR-mutated, NSCLC were collected to this study. Patient’s characteristics are summarized in Table 1.
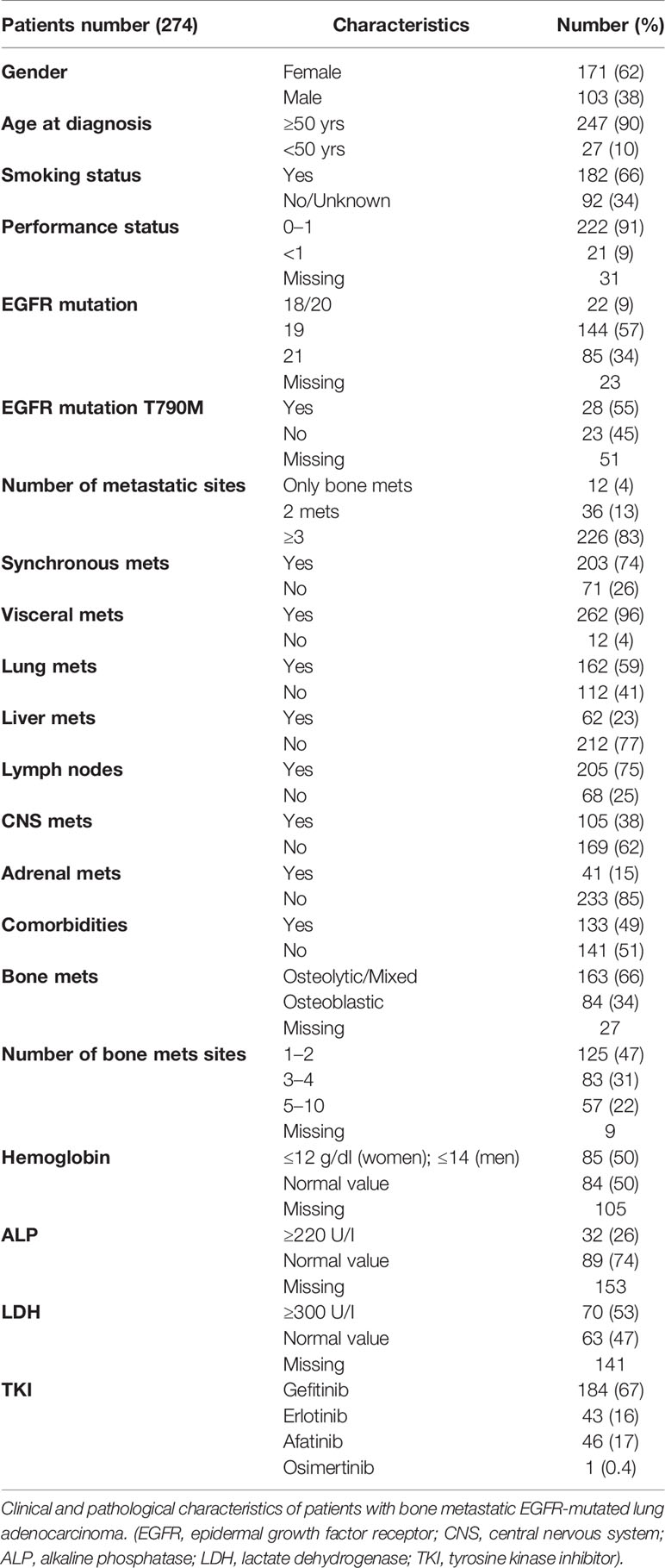
Table 1 Patient’s characteristics.
The median age was 50 years, 171 (62%) were female and 103 (38%) were male. The PS, available in 243 (89%) cases, was 0–1 in 222 (91%) and higher than 1 in 21 (9%) patients, respectively. One hundred eighty-two patients (66%) had a history of smoking habit (present or past). The mutational status, available in 251 patients (92%), was as follows: exons 18 in 14 (6%), exon 19 in 144 (57%), exon 20 in 8 (3%), and exon 21 in 85 (34%) patients. Four patients presented compound EGFR mutations: 1 exon 18 and 21, 3 exon 18 and 20.
Twenty-eight out of 51 available patients (55%) presented T790M mutation.
One hundred eighty-four patients received gefitinib (67%), 46 afatinib (17%), 43 erlotinib (16%). One patient (0.4%) received osimertinib. The median time to TKI exposure was 11,1 months (95% Confidence Interval [CI]: 9,8–12,4).
In 203 patients (74%) BMs were synchronous with diagnosis of advanced NSCLC, while 71 patients (26%) developed bone metastasis during follow-up. In 12 patients (4%) bone was the only metastatic site, 13% had bone plus one metastatic site, and 83% had at least two different metastatic sites in addition to bone. Concomitant visceral metastatic sites were lung in 162 (59%), liver in 62 (23%), lymph nodes in 205 (75%), adrenal glands in 41 (15%), and Central Nervous System (CNS) in 105 (38%) patients respectively.
The burden of bone involvement was available in 265 patients (97%). It was limited (1–2 sites) in 125 (47%), intermediate (3–4 sites) in 83 (31%), and extensive (5–10 sites) in 57 cases (22%). Osteolytic and mixed bone lesions were documented in 163 (66%) cases, the remaining 84 (34%) patients had osteoblastic metastasis. In the minority of patients in which blood parameters were available, hemoglobin levels were often below the normal range and high levels of both ALP and LDH were frequently observed.
Skeletal-Related Events and Relevant Predictive Factors
A total of 173 adverse SREs were recorded in the 274 patients examined in the present study (63%). Seventy-seven (28%) developed at least one major SRE: 55/274 (20%) presented bone fractures, 5/274 (2%) hypercalcemia, 30/274 (11%) spinal cord compression. Fourteen patients (5%) developed both pathological fractures and spinal cord compression, three patients (1%) presented hypercalcemia and pathological fractures. Nine patients (3%) underwent bone surgery and 150/274 (55%) radiation therapy on bone (Figure 1).
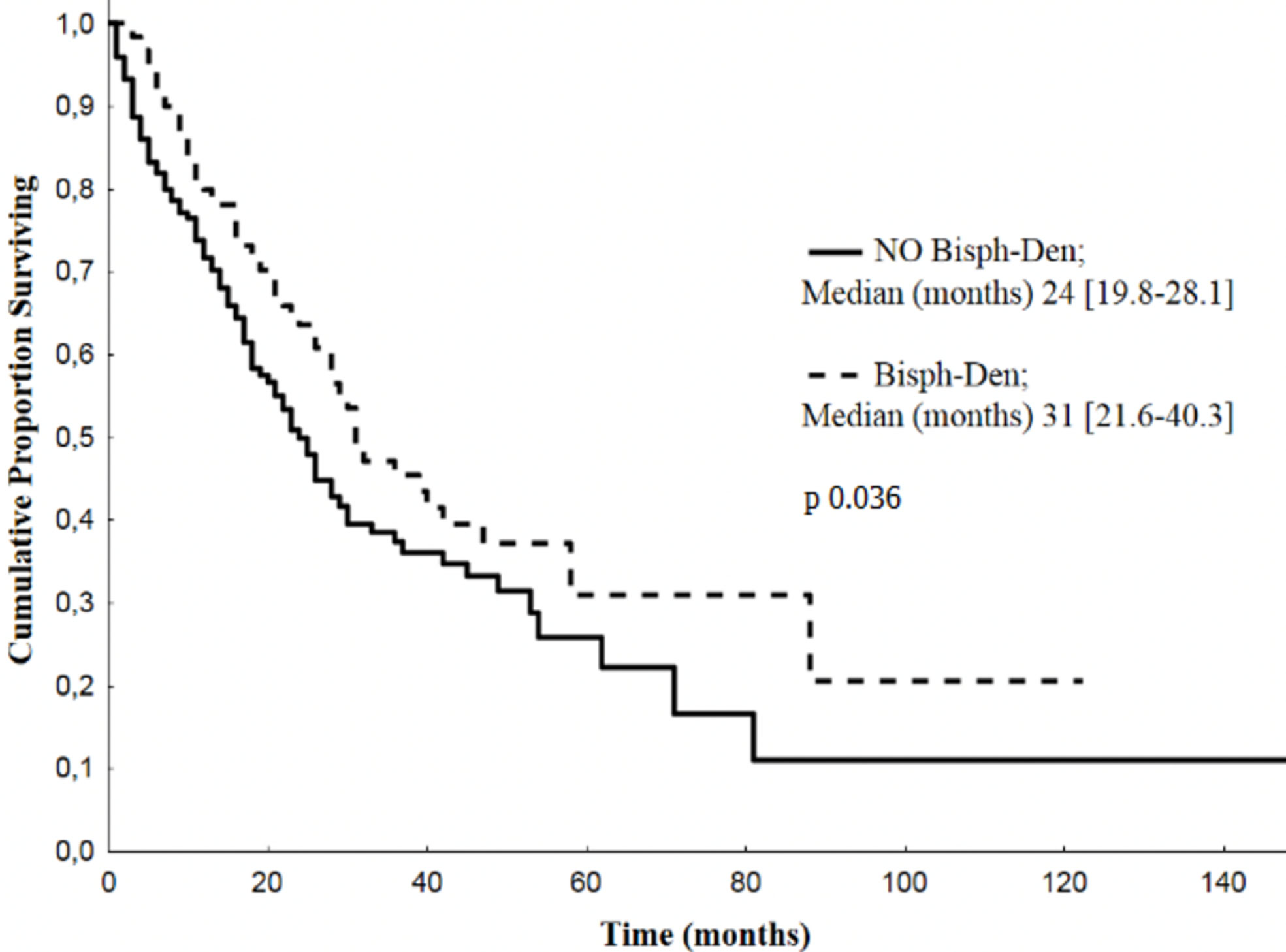
Figure 1 Frequencies of SREs. Percentage and number of global SREs occurred after diagnosis of BM EGFR-mutated lung cancer (EGFR, epidermal growth factor receptor; SRE, skeletal related event; BM, bone metastases).
The date of appearance of the first SRE was available in 135 out of the total of 173 SRE (78%). All the 77 major SREs were correctly placed during the treatment course. As shown on Figure 2, SREs occurred early after the diagnosis of BMs. In the patient subset who developed SREs, the median time to the onset of SRE from the diagnosis of BMs was 3.63 months (95% CI 0.79–6.47).
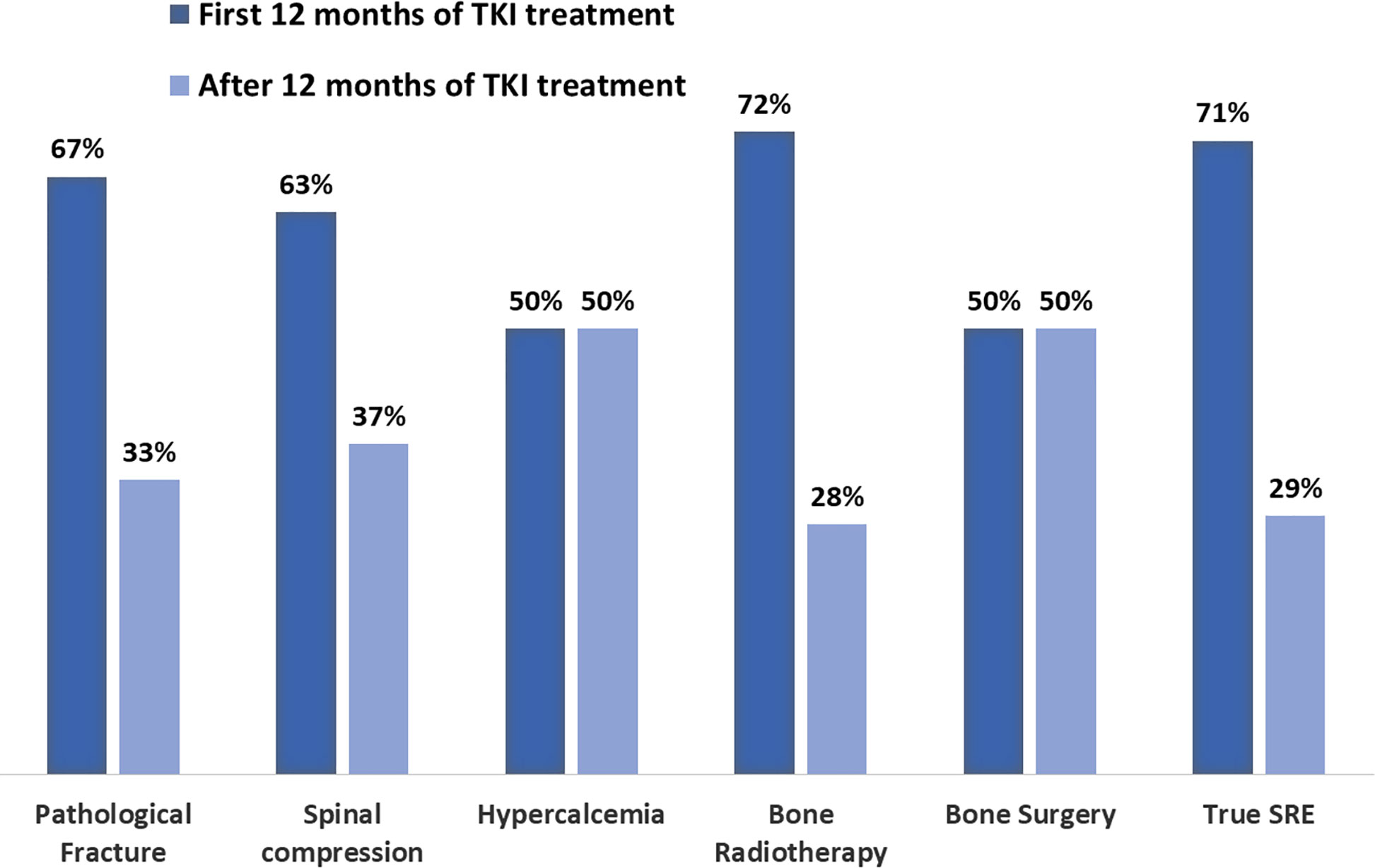
Figure 2 Time to first SRE. Kaplan-Meier estimates of time from diagnosis of bone metastases to onset of first skeletal related event (SRE, skeletal related event).
Forty-one (30%) patients developed the first event before TKI introduction, among the remaining 94 patients, 22/33 (67%) developed bone fractures within the first 12 months of TKI therapy and 11/33 (33%) afterwards; the corresponding distribution of spinal cord compression was 10/16 (63%) and 6/16 (37%), hypercalcemia: 2/4 (50%) and 2/4 (50%), bone surgery: 1/2 (50%) and 1/2 (50%), radiation therapy: 58/81 (72%) and 23/81 (28%), respectively (Figure 3).
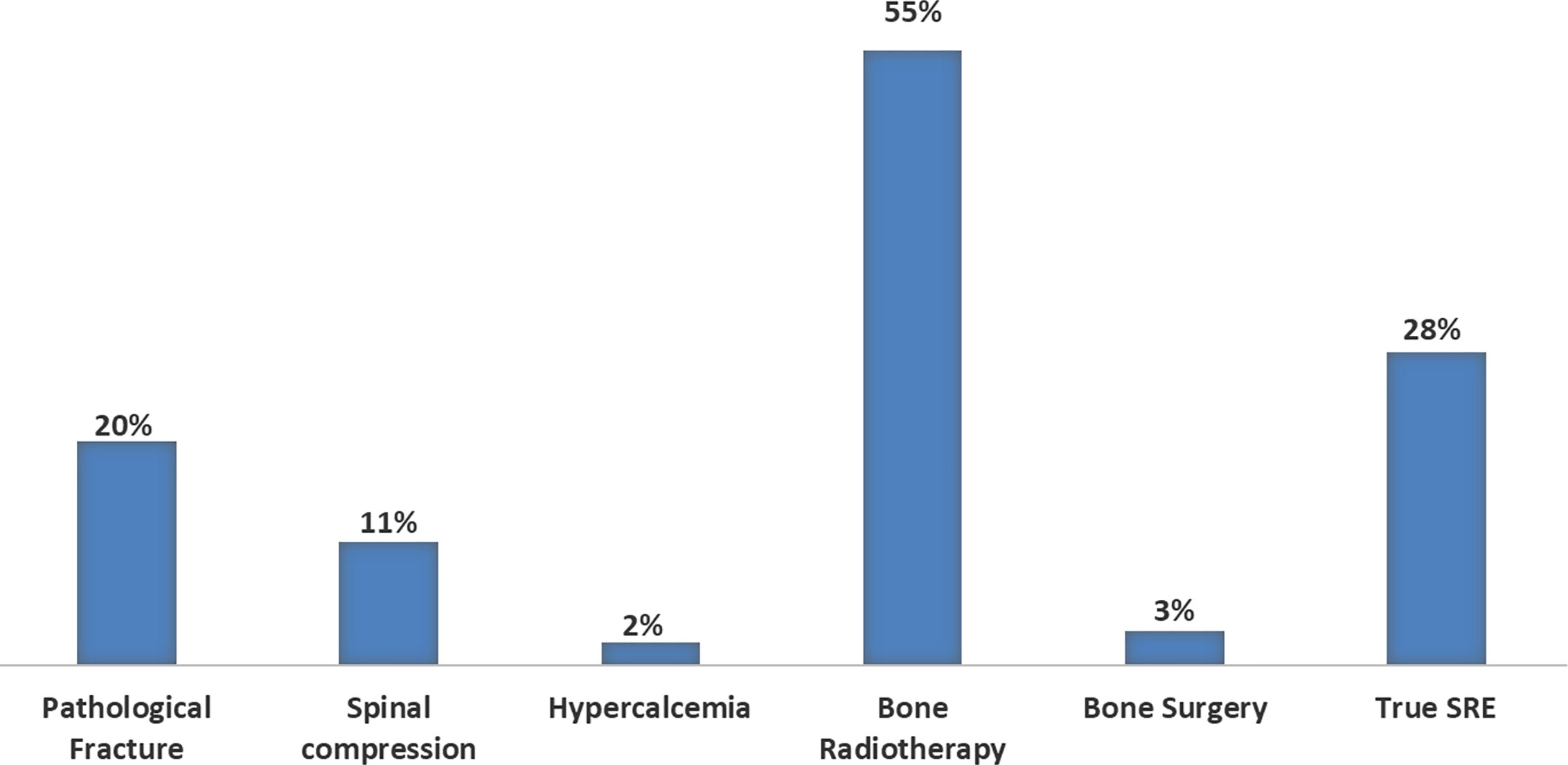
Figure 3 Frequencies of SRE before and after the first 12 months of TKI treatment. Percentage and number of global SREs occurred after diagnosis of BM EGFR-mutated lung cancer before and after the first 12 months of TKI treatment, respectively (EGFR, epidermal growth factor receptor; SRE, skeletal related event; BM, bone metastases; TKI, tyrosine kinase inhibitor).
One hundred and twenty-two patients (45%) received bone resorption inhibitors: 79 (29%) bisphosphonates, 46 (17%) denosumab, 3 patients (1%) received both drugs.
In the univariate analysis depicted in Table 2, PS and the presence of liver metastasis were significantly associated with the occurrence of SREs. Both variables maintained their predictive role in multivariate analysis: PS (HR 2.124, 95% CI: 1.046–4.313, p = 0.037), liver metastasis (HR 1.946, 95% CI: 1.169–3.239, p = 0.010).
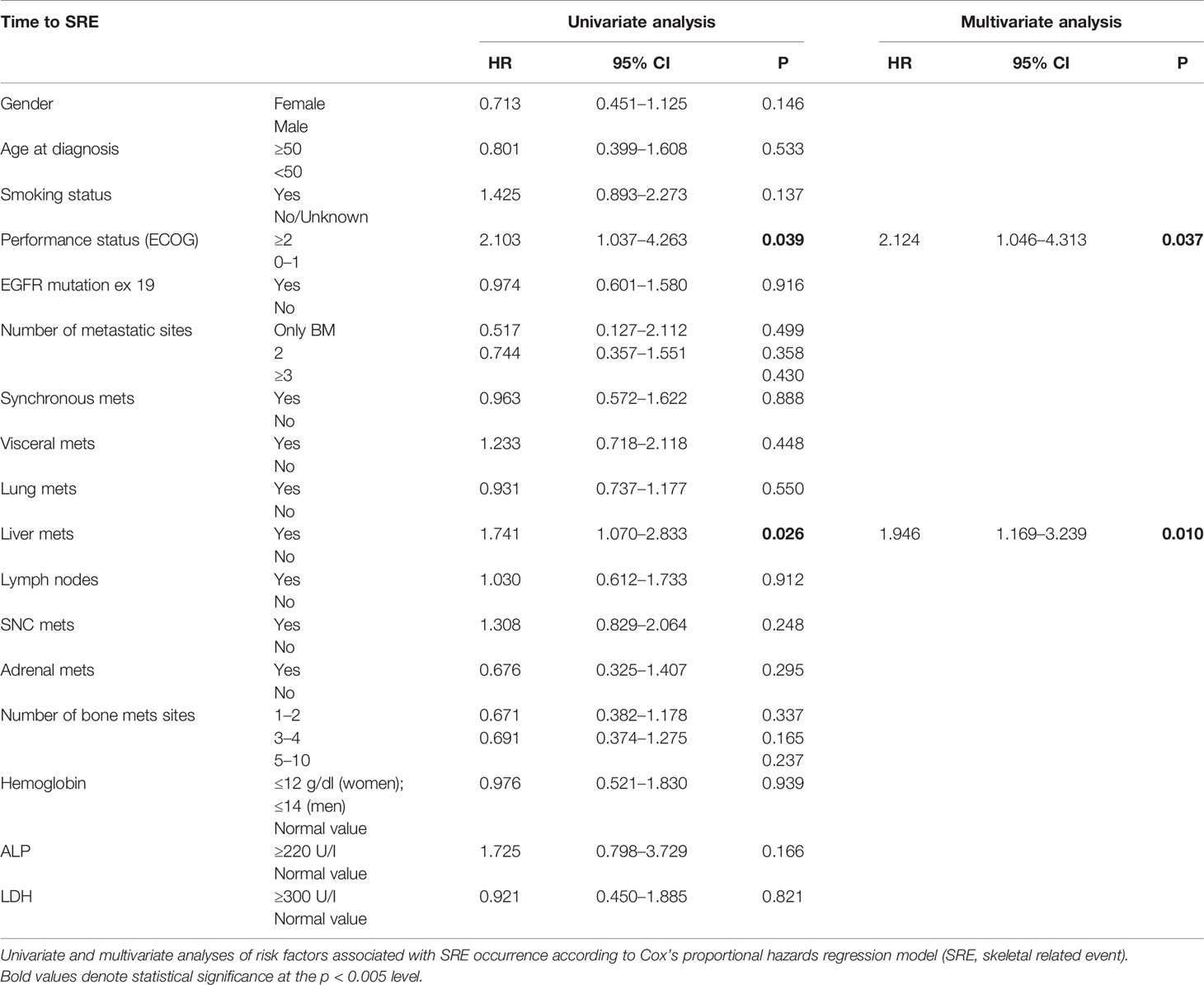
Table 2 Predictive factors of SRE onset.
Patient Prognosis and Survival Outcomes
Median follow-up of enrolled patients was 23 months (range 1–117). At the last follow-up examination, 152 patients (55%) were dead. Median overall survival (OS) from the diagnosis of bone metastases was 28 months (95% CI: 24.1–31.8) (Figure 4).
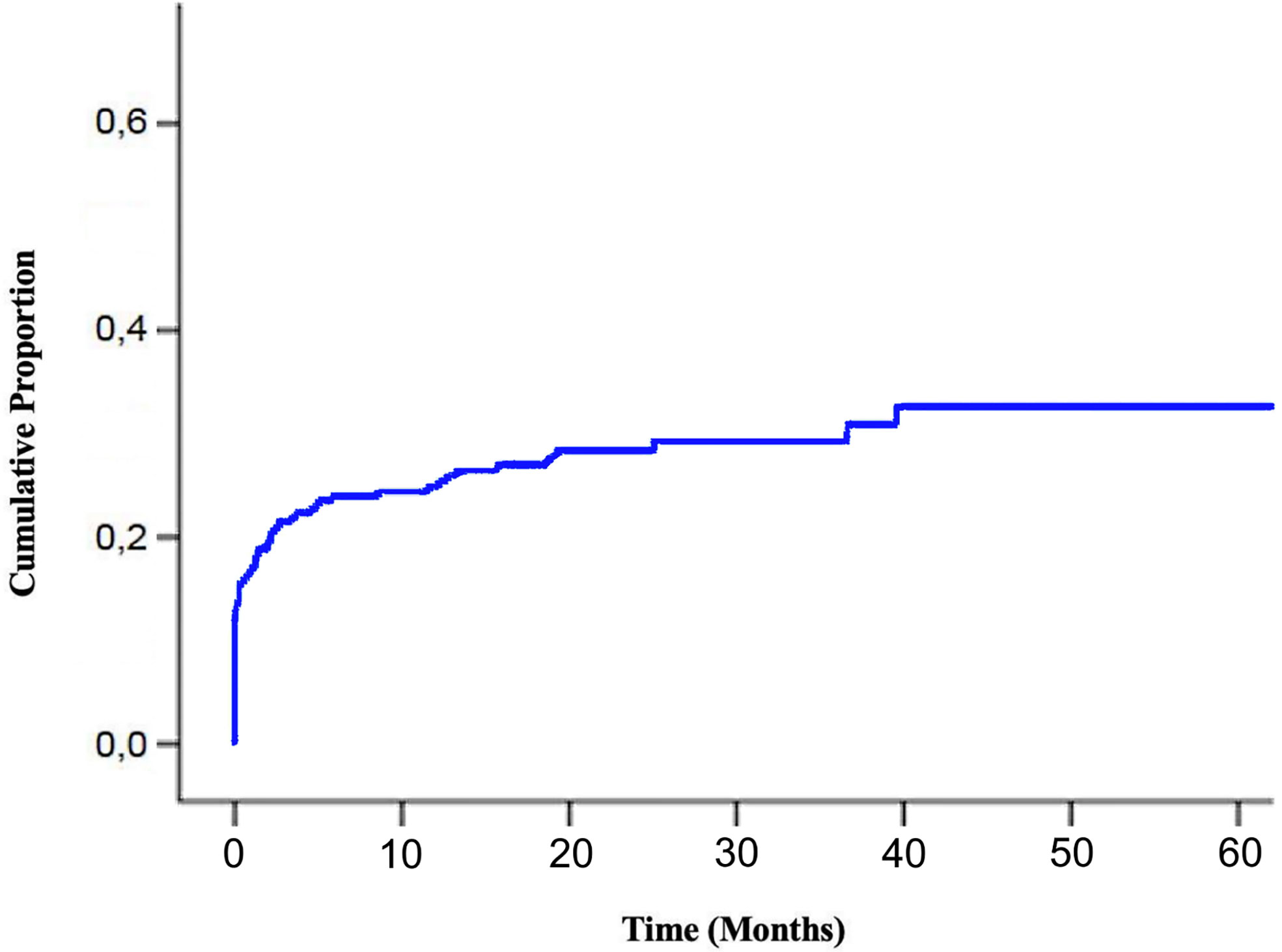
Figure 4 Overall Survival of BM EGFR-mutated patients. Kaplan-Meier estimates of overall survival of EGFR-mutated lung cancer patients after diagnosis of bone metastases (BM, bone metastases; EGFR, epidermal growth factor receptor).
Median OS of patients who developed synchronous bone metastases was 29 months (95% CI: 22.8–35.2) as opposed to 24 months (range 15.4–32.6) of patients who presented metachronous bone metastases (p = 0.010).
Among the 33 potential prognostic factors analyzed in univariate analysis, the female gender (HR 0.684, 95% CI: 0.493–0.949, p = 0.023), EGFR Mutation of Exon 19 (HR 0.601, 95% CI: 0.416–0.867, p = 0.007) and the presence of synchronous bone metastasis (HR 0.631, 95% CI: 0.444–0.896, p= 0.010) were significantly associated with a lower risk of death.
On the contrary, smoking habit (HR 1.487, 95% CI: 1.061–2.084, p= 0.021), PS ≥ 2 (HR 1.877, 95% CI: 1.055–3.341, p = 0.032), ALP ≥220 U/I (HR 1.938, 95% CI: 1.147–3.276, p = 0.013), and LDH ≥300 U/I (HR 1.782, 95% CI: 1.126–2.821, p = 0.014) were significantly associated with a higher death risk (Table 3).
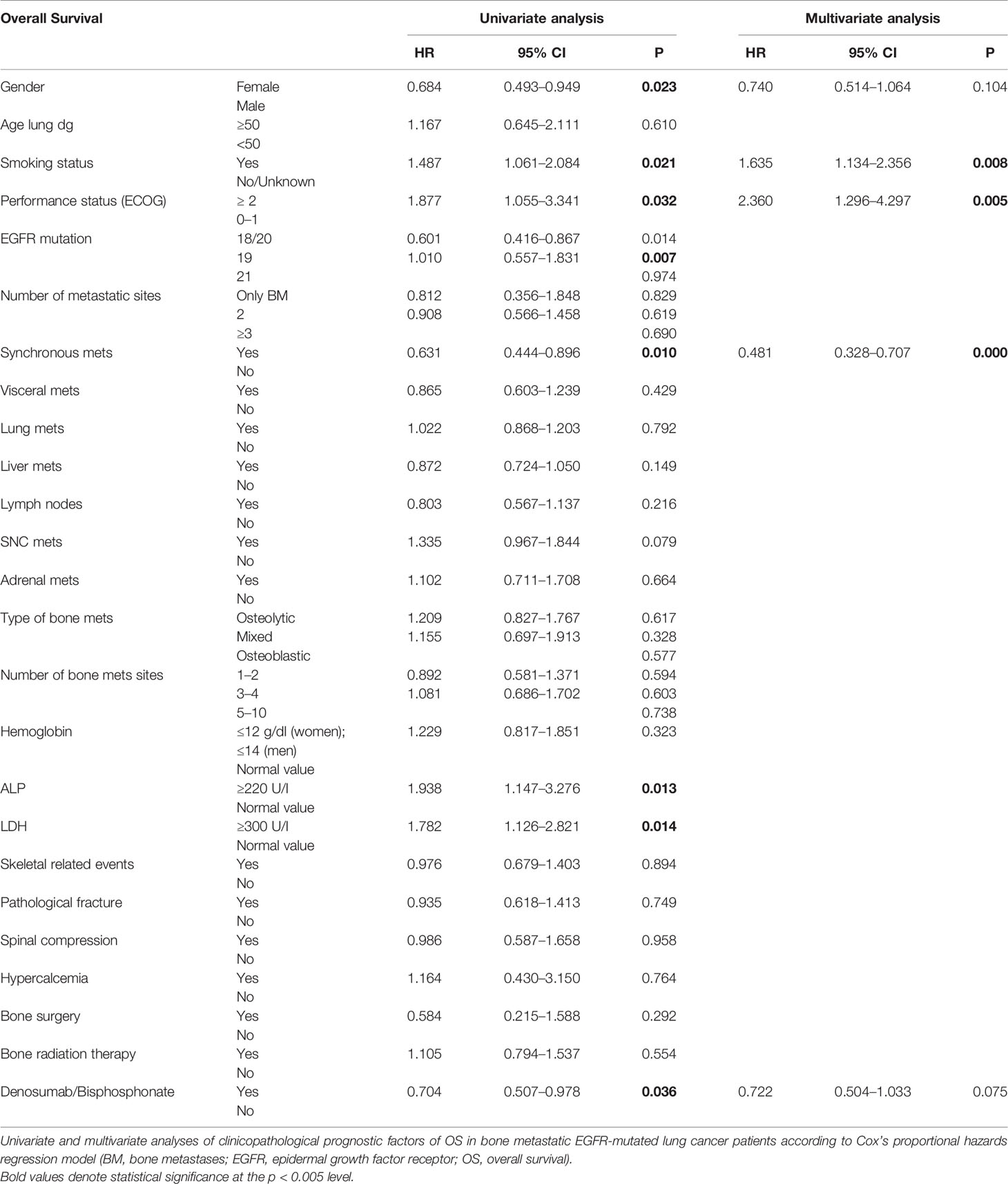
Table 3 Prognostic factors of BM OS.
At multivariate analysis, smoking habit (HR 1.635, 95% CI: 1.134–2.356, p = 0.008), PS (HR 2.360, 95% CI: 1.296–4.297, p = 0.005), and the presence of synchronous bone metastasis (HR 0.481, 95% CI: 0.328–0.707, p = 0.000) maintained a significant association with the death risk. Due to the low number of patients with available data, LDH and ALP were not included in the multivariate model.
The administration of bisphosphonates or denosumab was significantly associated with a lower risk of death at univariate analysis (HR 0.704, 95% CI: 0.507–0.978, p = 0.036) (Figure 5) with a tendency to maintain a prognostic significance at multivariate analysis (HR 0.722, 95% CI: 0.504–1.033, p = 0.075).
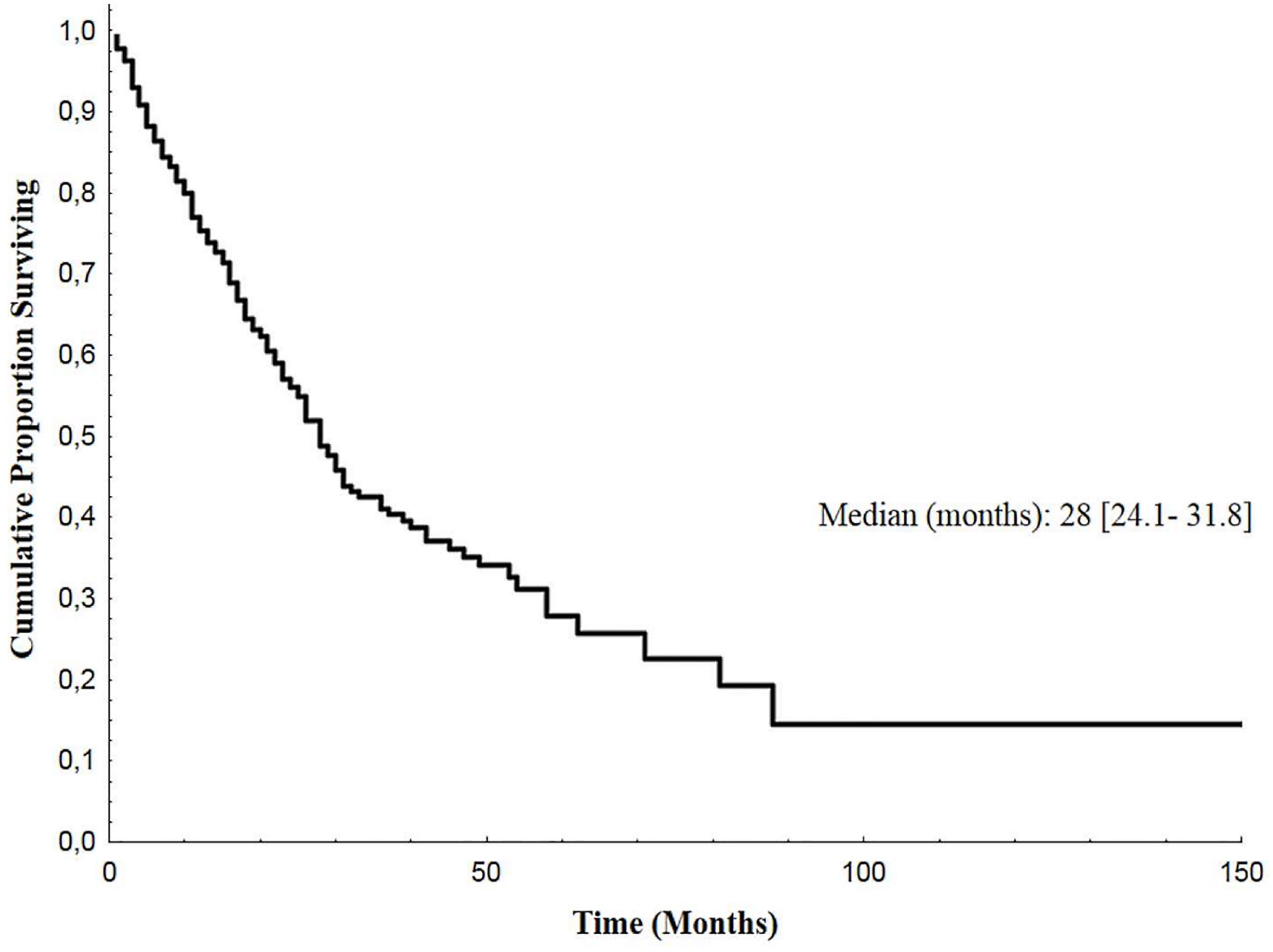
Figure 5 Overall Survival according to administration of bone resorption inhibitors. Kaplan-Meier estimates of overall survival of EGFR-mutated lung cancer patients after diagnosis of bone metastases according to the administration of bisphosphonates/denosumab (EGFR, epidermal growth factor receptor).
Discussion
Bone metastases have a negative impact on quality of life and prognosis of lung cancer patients due to bone pain and the elevated risk of SREs (8). The frequency of SREs in EGFR mutated lung cancer with bone metastases have been scarcely documented in literature (Table 4) and the benefit of TKIs on bone pain and SREs prevention have not evaluated in randomized clinical trials (11). The natural history of the disease and frequency of SREs of lung cancer patients with bone metastases have been described in a large number of Italian patients (n = 661) (18). In this series, the median survival after bone metastases diagnosis was 9.5 months and the distribution of major SRE was 16% fractures, 6% spinal cord compression, and 2% hypercalcemia. In this paper, 30% of patients were treated of TKIs, but this subset was not analyzed separately.
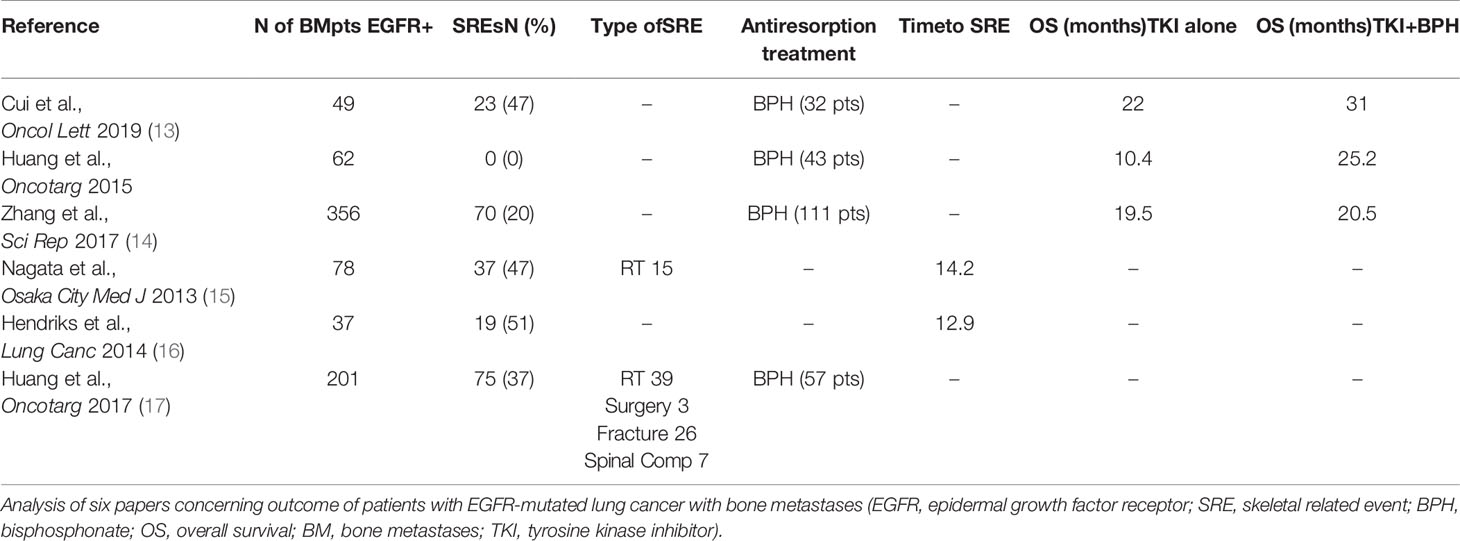
Table 4 Review of the literature.
In this multicenter retrospective series, involving bone metastatic patients with EGFR mutated NSCLC, the frequency of SREs, according to the standard definition that also includes bone surgery and radiation therapy was 58%. This proportion is similar to that reported in the above mentioned Italian series of bone metastatic lung cancer patients (18), 94.3% of them treated with chemotherapy. Also, the proportion of major SREs (28%), observed in the present study, is similar to that reported in the mentioned series as well as in other published bone metastatic patient series with different primary histologies (19–21). The outcome of patients with EGFR mutated lung cancer with bone metastases have been evaluated in six published papers in which the SRE frequency was 0% in only one paper (22), while ranged between 20 and 51% in the remaining five papers (13–17) (Table 4). On the bases of these results, TKIs seem to be not effective in preventing SREs, despite their great efficacy in controlling the disease. This hypothesis is further strengthened by the short time from the diagnosis of BM to the appearance of SRE (3.63 months) observed in our series and the greater distribution of these events in the first 12 months, a period in which the tumor is generally responsive to TKIs.
Preclinical in vivo studies demonstrated that EGFR is essential for osteoblast proliferation (23) and down-regulated EGFR signaling was shown to favor the senescence of osteoprogenitors and the decline in bone formation on the endosteal surface of cortical bone (24). The administration of EGFR inhibitors, therefore, could impair the osteoblast mediated bone repair thus favoring the early occurrence of SREs despite the efficacy of these drugs. This hypothesis deserves to be further explored.
Wnt signaling is aberrantly activated in lung cancer (25). Abnormal activation of this pathway is implicated in driving the formation of lung cancer bone metastasis and has a relevant involvement in the cancer induced bone lesions (26). Moreover, Wnt signaling has also a significant negative impact on lung cancer prognosis and therapeutic resistance, specifically as regard as TKI therapy (25). On these bases there is a strong rationale for the testing drug targeting this pathway in association with currently available TKIs, with the aims of prevent bone progression, SREs and overcome/delay treatment resistance (25, 26).
The occurrence of SRE in prostate cancer patients is significantly associated with a poor prognosis (27). This was not the case in this series of TKI treated lung cancer patients. This observation may imply a long deterioration of quality of life in this patient subset in case of occurrence of an SRE.
The overall survival of 28 months, observed in this patient series does not differ from that observed in clinical trials and published case series (3–5), so the presence of bone metastases in TKI treated patients seem to be not related to poorer prognosis. The prognostic factors observed in univariate and multivariate analyses (i.e. ECOG Performance Status, smoking habit, and synchronous bone metastasis) in this study are in line to those observed in published series (3–5).
Several randomized prospective clinical trials have demonstrated that bone resorption inhibitors are efficacious in preventing SREs of bone metastatic lung cancer patients (10, 12). These trials were conducted before the introduction of TKIs in clinics, so we do not have a formal demonstration of their efficacy in this clinical setting. In the present series, these drugs failed to correlate with a lower SRE proportion, due to their delayed administration (i.e. after the onset of the first SRE) in many cases. The great proportion of SREs observed in the present study and their early onset provide a strong rationale for the introduction of bisphosphonates and denosumab in this setting. Interestingly, the administration of these drugs was associated with better prognosis, that just failed to attain the statistical significance in multivariate analysis. A positive effect of bisphosphonate administration on survival of EGFR mutated lung cancer patients submitted to TKIs was previously observed in 3 published series (13, 14, 22) (Table 4).
Despite the recommendation of using anti-bone reabsorption agents, only 45% of our population received these drugs and most of them start treatment after SREs onset. The reason could be related to the fact of TKI are expected to very efficacious in this setting. At last but not at least physicians are afraid of the possible occurrence of jawbone osteonecrosis, one of the most severe adverse reactions.
Bisphosphonates could enhance the antineoplastic effects of EGFR-TKIs in NSCLC with EGFR mutation both in vitro (28) and in vivo (14). Pertinently, the results of a randomized clinical trial of denosumab versus zoledronic acid in patients with various primary malignancies have shown a survival advantage favoring denosumab in the subset of patients with NSCLC (29). On the bases of this background, the synergism between bone resorption and EGFR inhibitors in lung cancer patients deserves to be explored.
The retrospective nature and the absence of a post progression analysis are the main limitations of this study.
Conclusions
In conclusion, bone metastatic NSCLC patients with EGFR mutated disease, treated with modern EGFR inhibitors, have a relatively long survival expectancy and are at high risk to develop skeletal related events. Since SREs occur early after the TKI start, there is a rationale to administer bone resorption inhibitors. Whether bisphosphonate or denosumab have the potential to improve survival when associated to TKIs is a matter of future research.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The study was firstly approved by the Institutional Review Board of the Coordinating Center in Brescia (SURMOS Study no. NP1848) and subsequently by the ethic committees of each participating institution.
Author Contributions
All authors contributed to the study design and data collection for all the Italian institutions involved in the study. Material preparation and analysis were performed by ML and CG. The first draft of the manuscript was written by ML, CG, and AlfB. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We are grateful to our patients and their families.
References
1. Malvezzi M, Bertuccio P, Rosso T, Rota M, Levi F, La Vecchia C, et al. European cancer mortality predictions for the year 2015: does lung cancer have the highest death rate in EU women? Ann Oncol (2015) 26:779–86. doi: 10.1093/annonc/mdv001
2. Zappa C, Mousa SA. Non-small cell lung cancer: current treatment and future advances. Transl Lung Cancer Res (2016) 5:288–300. doi: 10.21037/tlcr.2016.06.07
3. Mok TS, Wu Y-L, Thongprasert S, Yang C-H, Chu D-T, Saijo N, et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N Engl J Med (2009) 361:947–57. doi: 10.1056/NEJMoa0810699
4. Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol (2012) 13:239–46. doi: 10.1016/S1470-2045(11)70393-X
5. Wu Y-L, Zhou C, Hu C-P, Feng J, Lu S, Huang Y, et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol (2014) 15:213–22. doi: 10.1016/S1470-2045(13)70604-1
6. Popat S. Osimertinib as First-Line Treatment in EGFR -Mutated Non–Small-Cell Lung Cancer. N Engl J Med (2018) 378:192–3. doi: 10.1056/NEJMe1714580
7. Ramalingam SS, Vansteenkiste J, Planchard D, Cho BC, Gray JE, Ohe Y, et al. Overall Survival with Osimertinib in Untreated, EGFR -Mutated Advanced NSCLC. N Engl J Med (2020) 382:41–50. doi: 10.1056/NEJMoa1913662
8. Kuchuk M, Kuchuk I, Sabri E, Hutton B, Clemons M, Wheatley-Price P. The incidence and clinical impact of bone metastases in non-small cell lung cancer. Lung Cancer (2015) 89:197–202. doi: 10.1016/j.lungcan.2015.04.007
9. Cho YJ, Cho YM, Kim SH, Shin KH, Jung ST, Kim HS. Clinical analysis of patients with skeletal metastasis of lung cancer. BMC Cancer (2019) 19:1–10. doi: 10.1186/s12885-019-5534-3
10. Rosen LS, Gordon D, Tchekmedyian NS, Yanagihara R, Hirsh V, Krzakowski M, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors. Cancer (2004) 100:2613–21. doi: 10.1002/cncr.20308
11. Vaidya A, Flores SK, Cheng Z-M, Nicolas M, Deng Y, Opotowsky AR, et al. EPAS1 Mutations and Paragangliomas in Cyanotic Congenital Heart Disease. N Engl J Med (2018) 378:1259–61. doi: 10.1056/NEJMc1716652
12. Henry DH, Costa L, Goldwasser F, Hirsh V, Hungria V, Prausova J, et al. Randomized, Double-Blind Study of Denosumab Versus Zoledronic Acid in the Treatment of Bone Metastases in Patients With Advanced Cancer (Excluding Breast and Prostate Cancer) or Multiple Myeloma. J Clin Oncol (2011) 29:1125–32. doi: 10.1200/JCO.2010.31.3304
13. Cui X, Li S, Gu J, Lin Z, Lai B, Huang L, et al. Retrospective study on the efficacy of bisphosphonates in tyrosine kinase inhibitor−treated patients with non−small cell lung cancer exhibiting bone metastasis. Oncol Lett (2019) 18(5):5437–47. doi: 10.3892/ol.2019.10870
14. Zhang G, Cheng R, Zhang Z, Jiang T, Ren S, Ma Z, et al. Bisphosphonates enhance antitumor effect of EGFR-TKIs in patients with advanced EGFR mutant NSCLC and bone metastases. Sci Rep (2017) 7:42979. doi: 10.1038/srep42979
15. Nagata M, Kudoh S, Mitsuoka S, Suzumura T, Umekawa K, Tanaka H, et al. Skeletal-related events in advanced lung adenocarcinoma patients evaluated EGFR mutations. Osaka City Med J (2013) 59(1):45–52.
16. Hendriks LEL, Smit EF, Vosse BAH, Mellema WW, Heideman DAM, Bootsma GP, et al. EGFR mutated non-small cell lung cancer patients: More prone to development of bone and brain metastases? Lung Cancer (2014) 84:86–91. doi: 10.1016/j.lungcan.2014.01.006
17. Huang S-M, Yang J-J, Chen H-J, Wu S-P, Bai X-Y, Zhou Q, et al. Epidermal growth factor receptor is associated with the onset of skeletal related events in non-small cell lung cancer. Oncotarget (2017) 8:81369–76. doi: 10.18632/oncotarget.18759
18. Santini D, Barni S, Intagliata S, Falcone A, Ferraù F, Galetta D, et al. Natural History of Non-Small-Cell Lung Cancer with Bone Metastases. Sci Rep (2015) 5:18670. doi: 10.1038/srep18670
19. Berruti A, Libè R, Laganà M, Ettaieb H, Sukkari MA, Bertherat J, et al. Morbidity and mortality of bone metastases in advanced adrenocortical carcinoma: a multicenter retrospective study. Eur J Endocrinol (2019) 180:311–20. doi: 10.1530/EJE-19-0026
20. Grisanti S, Bianchi S, Locati LD, Triggiani L, Vecchio S, Bonetta A, et al. Bone metastases from head and neck malignancies: Prognostic factors and skeletal-related events. PLoS One (2019) 14:e0213934. doi: 10.1371/journal.pone.0213934
21. Iacovelli R, Santini D, Rizzo M, Felici A, Santoni M, Verzoni E, et al. Bone metastases affect prognosis but not effectiveness of third-line targeted therapies in patients with metastatic renal cell carcinoma. Can Urol Assoc J (2015) 9:263. doi: 10.5489/cuaj.2377
22. Huang C-Y, Wang L, Feng C-J, Yu P, Cai X-H, Yao W-X, et al. Bisphosphonates enhance EGFR-TKIs efficacy in advanced NSCLC patients with EGFR activating mutation: A retrospective study. Oncotarget (2016) 7:66480–90. doi: 10.18632/oncotarget.5515
23. Linder M, Hecking M, Glitzner E, Zwerina K, Holcmann M, Bakiri L, et al. EGFR controls bone development by negatively regulating mTOR-signaling during osteoblast differentiation. Cell Death Differ (2018) 25:1094–106. doi: 10.1038/s41418-017-0054-7
24. Liu G, Xie Y, Su J, Qin H, Wu H, Li K, et al. The role of EGFR signaling in age-related osteoporosis in mouse cortical bone. FASEB J (2019) 33:11137–47. doi: 10.1096/fj.201900436RR
25. Yang J, Chen J, He J, Li J, Shi J, Cho WC, et al. Wnt signaling as potential therapeutic target in lung cancer. Expert Opin Ther Targets (2016) 20:999–1015. doi: 10.1517/14728222.2016.1154945
26. Xi Y, Chen Y. Wnt signaling pathway: implications for therapy in lung cancer and bone metastasis. Cancer Lett (2014) 353:8–16. doi: 10.1016/j.canlet.2014.07.010
27. Oefelein MG, Ricchiuti V, Conrad W, Resnick MI. Skeletal Fractures Negatively Correlate With Overall Survival in Men With Prostate Cancer. J Urol (2002) 168:1005–7. doi: 10.1016/S0022-5347(05)64561-2
28. Chang JW-C, Hsieh J-J, Shen Y-C, Yeh K-Y, Wang C-H, Li Y-Y, et al. Bisphosphonate zoledronic acid enhances the inhibitory effects of gefitinib on EGFR-mutated non-small cell lung carcinoma cells. Cancer Lett (2009) 278:17–26. doi: 10.1016/j.canlet.2008.12.019
29. Scagliotti GV, Hirsh V, Siena S, Henry DH, Woll PJ, Manegold C, et al. Overall Survival Improvement in Patients with Lung Cancer and Bone Metastases Treated with Denosumab Versus Zoledronic Acid: Subgroup Analysis from a Randomized Phase 3 Study. J Thorac Oncol (2012) 7:1823–9. doi: 10.1097/JTO.0b013e31826aec2b
Keywords: bone metastasis, non-small cell lung cancer, skeletal related events, tyrosine kinase inhibitors, epidermal growth factor receptor
Citation: Laganà M, Gurizzan C, Roca E, Cortinovis D, Signorelli D, Pagani F, Bettini A, Bonomi L, Rinaldi S, Berardi R, Filetti M, Giusti R, Pilotto S, Milella M, Intagliata S, Baggi A, Cortellini A, Soto Parra H, Brighenti M, Petrelli F, Bennati C, Bidoli P, Garassino MC and Berruti A (2020) High Prevalence and Early Occurrence of Skeletal Complications in EGFR Mutated NSCLC Patients With Bone Metastases. Front. Oncol. 10:588862. doi: 10.3389/fonc.2020.588862
Received: 20 August 2020; Accepted: 19 October 2020;
Published: 12 November 2020.
Edited by:
Dianwen Song, Shanghai First People’s Hospital, ChinaReviewed by:
Abdul Malik Tyagi, Emory University, United StatesMaria Francesca Baietti, VIB KU Leuven Center for Cancer Biology, Belgium
Copyright © 2020 Laganà, Gurizzan, Roca, Cortinovis, Signorelli, Pagani, Bettini, Bonomi, Rinaldi, Berardi, Filetti, Giusti, Pilotto, Milella, Intagliata, Baggi, Cortellini, Soto Parra, Brighenti, Petrelli, Bennati, Bidoli, Garassino and Berruti. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alfredo Berruti, YWxmcmVkby5iZXJydXRpQGdtYWlsLmNvbQ==