
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oncol. , 11 November 2020
Sec. Pediatric Oncology
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.579219
This article is part of the Research Topic Critical Complications In Pediatric Oncology and Hematopoietic Cell Transplant View all 31 articles
 Long Dao1†
Long Dao1† Dristhi Ragoonanan1†Sofia Yi1†Rita Swinford2
Dristhi Ragoonanan1†Sofia Yi1†Rita Swinford2 Demetrios Petropoulos1Kris M. Mahadeo1
Demetrios Petropoulos1Kris M. Mahadeo1 Shulin Li1*
Shulin Li1*Pediatric organ failure and transplant populations face significant risks of morbidity and mortality. The risk of organ failure itself may be disproportionately higher among pediatric oncology patients, as cancer may originate within and/or metastasize to organs and adversely affect their function. Additionally, cancer directed therapies are frequently toxic to organs and may contribute to failure. Recent reports suggest that nearly half of providers find it difficult to provide prognostic information regarding organ failure due to unknown disease trajectories. Unfortunately, there is a lack of uniform methodology in detecting the early symptoms of organ failure, which may delay diagnosis, initiation of treatment and hinder prognostic planning. There remains a wide array of outstanding scientific questions regarding organ failure in pediatrics but emerging data may change the landscape of prognostication. Liquid biopsy, in which disease biomarkers are detected in bodily fluids, offers a noninvasive alternative to tissue biopsy and may improve prompt detection of organ failure and prognostication. Here, we review potential liquid biopsy biomarkers for organ failure, which may be particularly useful among pediatric oncology patients. We synthesized information from publications obtained on PubMed, Google Scholar, clinicaltrials.gov, and Web of Science and categorized our findings based on the type of biomarker used to detect organ failure. We highlight the advantages and disadvantages specific to each type of organ failure biomarker. While much work needs to be done to advance this field and validate its applicability to pediatric cancer patients facing critical care complications, herein, we highlight promising areas for future discovery.
Remarkable therapeutic advancement in pediatric oncology may be limited by long-term toxicity, and in particular, acute and/or chronic organ dysfunction/failure (1, 2). The most common reason for intensive care unit (ICU) admission in pediatric cancer patients is acute organ failure (3). While the definition of multiple organ dysfunction syndrome in pediatric patients (p-MODS) remains to be sufficiently determined, there is growing recognition that decrements in organ function may reliably predict stepwise increases in mortality rate and current binary descriptors of normal function versus dysfunction may hinder opportunities for earlier intervention (4, 5).
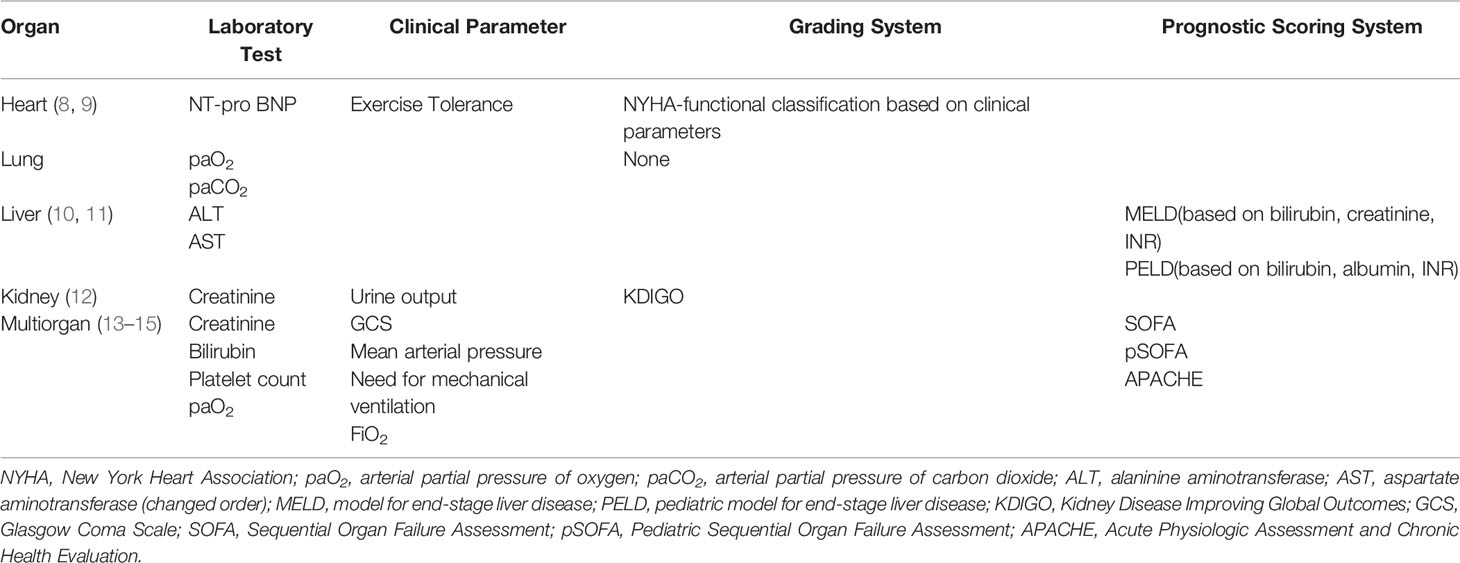
Among critically-ill pediatric oncology patients, overall ICU mortality ranges from 12-15 % in those with solid and hematologic malignancy, and can be as high as 60% in stem cell transplant (SCT) recipients (6, 7). Organ failure may occur acutely, sub-acutely or progress to chronic disease, and numerous studies have shown early detection may lead to critical timely intervention and improved outcomes. Currently, the gold standard diagnostic criteria for organ failure are organ specific and are based on laboratory, clinical or a combination of both parameters as summarized in Table 1 (8–15). Although these tests are widely used to diagnose organ failure, they are not predictive. Multiple scoring systems have been developed to attempt to predict the likelihood of developing single as well as multi-organ failure (Table 1). However, these are based on clinical evidence when organ dysfunction is already present.
In this review, we evaluate currently available biomarkers, their diagnostic accuracy, clinical applicability and potential impact on the prediction and early detection of organ failure. The role of chemokine and cytokine expression in the progression of organ failure has been more extensively characterized and are not included in this review (16–19). Here, we review various noninvasive biomarkers including microRNA, cell free DNA, histones, exosomes, circulating mitochondria and circulating endothelial cells as promising potential biomarkers of organ failure (Table 2).
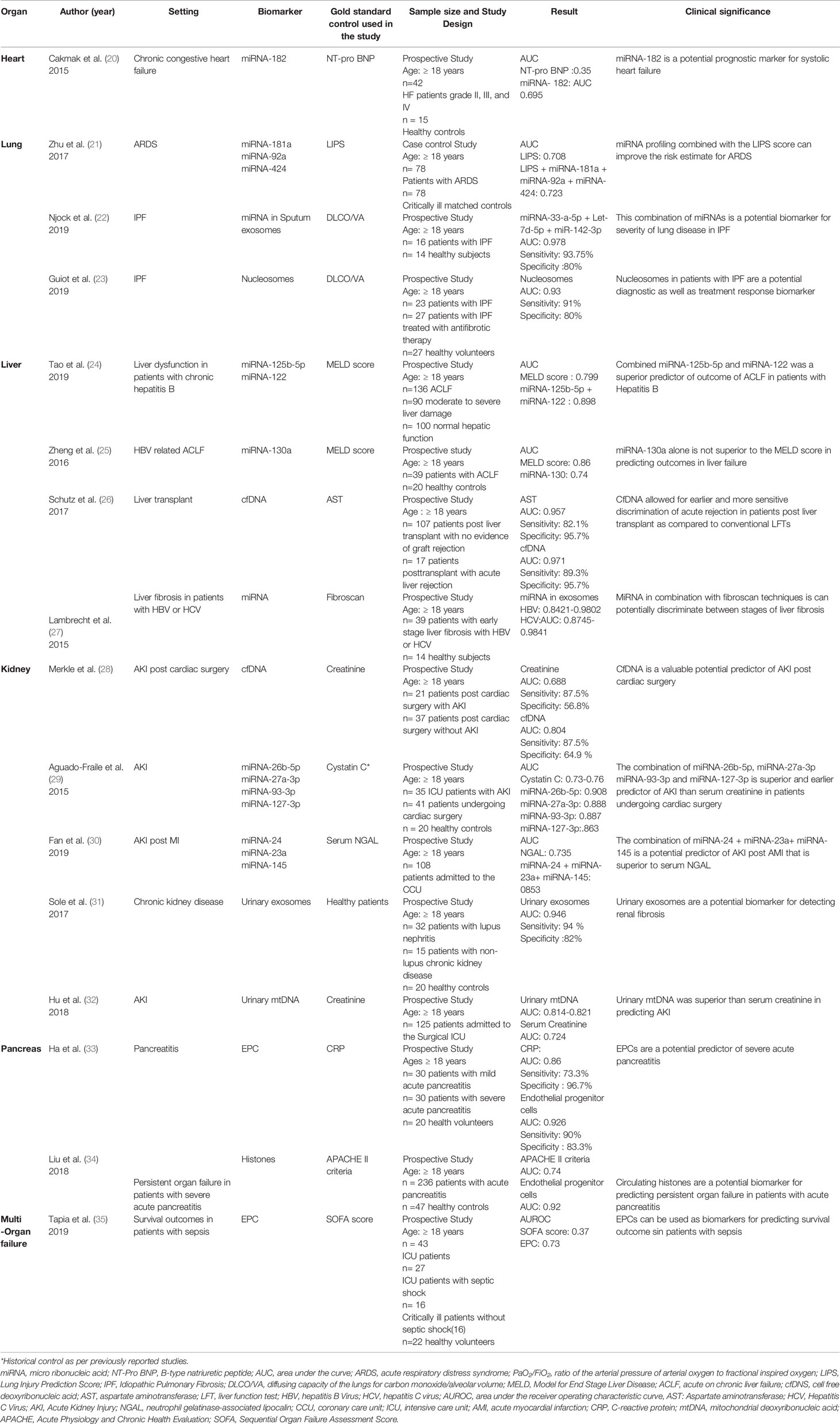
Table 2 Summary of Studies Examining Organ Failure.
Cell-free DNA are small degraded fragments of DNA, derived from the apoptosis of nucleated cells and circulate freely in the blood plasma (36). Under normal physiological conditions, healthy subjects have lower levels of cfDNA compared to patients with systemic illnesses, making them a possible biomarker of organ failure (37).
CfDNA has been studied in the blood of patients undergoing cardiac surgery to predict late acute kidney injury (AKI). The ROC generated from cfDNA of patients had improved detection of AKI (AUC = 0.804) compared to the ROC generated from the serum creatinine of patients (AUC = 0.688) (28). Karlas et al used total plasma cfDNA to assess hepatic fibrosis in comparison to current methods such as transient elastography. Plasma cfDNA concentrations did indeed correlate with degree of hepatic fibrosis and severity in non-alcoholic fatty liver disease (p value < 0.001) (38).
While the above studies utilize total plasma cfDNA, a recent study has shown that in the plasma of lung transplant patients, donor-derived cfDNA (ddcfDNA) could be identified and quantified, with patients with increased levels of ddcfDNA having a higher risk of allograft failure (39). Thus, ddcfDNA can be used as a tissue specific biomarker to determine the likelihood of organ failure due to allograft rejection. DdcfDNA has also been utilized in the risk stratification of organ rejection post heart transplant in pediatrics and adults as reported by North et al. (40).
While these studies highlight the potential of cfDNA as a novel biomarker for organ dysfunction, further work is required to identify tissue-specific DNA which would more reliably diagnose organ failure in children.
Micro RNAs (miRNA) are small, single-stranded, non-coding ribonucleotides that negatively regulate gene expression at the post-transcriptional level and play a role in cell proliferation, differentiation, repair and apoptosis (41). While each miRNA may regulate hundreds of genes, multiple miRNAs may work cooperatively to target one gene and despite their vast heterogeneity, miRNAs can display tissue-specific expression patterns (41, 42). MiRNAs are actively released into circulation as well as extracellular spaces including saliva and urine in response to toxic cellular insults either as extracellular vesicles or bound to RNA-binding proteins. This protein bound complex allows miRNA to persist in a stable form that is resistant to degradation, making them ideal biomarker candidates.
While the prognostic value of miRNAs has been reported for the prediction of outcomes for oncology patients as well as the prediction of multiple types of organ failure, there is a scarcity of data on its use to predict organ failure in pediatric patients (43, 44). Schneider et al showed that increased levels of miRNA-21, miRNA-126 and miRNA-423 predicted more favorable outcomes for patients with heart failure with fewer hospital readmissions (45). Cakmak et al demonstrated upregulation of miRNA-182 in patients with heart failure and found that it was superior to pro-brain type natriuretic peptide (pro-BNP), a biomarker often used in predicting heart failure. This study also showed that multiple miRNAs can undergo significant dysregulation in patients with organ failure and isolated 28 dysregulated miRNAs in patients with heart failure (20). In an attempt to increase its prognostic significance, Goren et al showed that multiple miRNA values can be combined into a single “miRNA score” for heart failure (46). Similarly, Zhu et al showed the benefit of combining multiple miRNAs with an already established grading system for the prediction of acute respiratory distress syndrome (21).
MiRNA profiling has also been shown to be useful in distinguishing the etiology of organ failure. Patients with acute liver failure (ALF) as a result of either HCV or cirrhosis were both found to have elevated levels of miRNA122. (47, 48). Weis et al also highlighted its potential in differentiating hepatocellular carcinoma (HCC) from liver dysfunction secondary to cirrhosis without the need for a biopsy and showed it was superior to alpha fetal protein, the only currently used biomarker utilized for HCC (49). Additionally, serum miRNAs have been shown to be a predictive biomarker in AKI. Aguado-Fraile et al verified that elevated serum miRNA-26b-5p, miRNA-27a-3p,miRNA-93-3p and miRNA-127-3p levels in patients with normal kidney function prior to cardiac surgery predicted AKI development post-operatively. Furthermore, this change in miRNA levels occurred days before the serum creatinine increased, highlighting both its worth as a novel predictor of AKI and the correlation of miRNA level with disease severity (29).
While the use of miRNA as a biomarker for organ failure is promising, further work is needed to determine the prognostic significance of these abnormal miRNAs in order to maximize their clinical utility in pediatric organ failure.
Endothelial progenitor cells (EPCs) are a subpopulation of stem cells that have been identified in the peripheral blood in response to endothelial damage secondary to insults, including vascular injury and ischemia. They are believed to be critical to maintain vascular integrity and endogenously restore and repair damaged vascular endothelium. Although EPCs have been studied as biomarkers for organ dysfunction, current studies in regards to EPCs and their role in cancer focus on their role as prognostic biomarkers (50).
Increased levels of EPCs are associated with decreased cardiovascular mortality amongst patients with coronary artery disease (51). Moazzami et al also showed that decreased levels of a subpopulation of EPCs known as circulating progenitor cells (CPCs) are associated with a worse prognosis and is a stronger factor in outcomes than the presence of stress-induced myocardial ischemia in patients with coronary artery disease (52). More recently, Lieu et al demonstrated the use of EPCs in predicting persistent organ failure in patients with severe acute pancreatitis (SAP) and showed the level of EPCs correlate negatively to clinical scores that are used to grade SAP including the Ranson and acute physiology and chronic health evaluation (APACHE) scores (53). Interestingly, patients with persistent organ failure had lower levels of EPCs, though still elevated from the healthy volunteers than those with transient organ failure. Tapia et al showed that though there was an increase in the number of EPCs, the protein expression of endothelial growth factor receptor-2 (VEGFR-2) and CD34 in the CEPCs (CD133+) was lower in critically ill patients with septic or non-septic shock and lowest in patients that did not survive (35).
In a pediatric study, EPCs were reported to be highly correlated with pulmonary arterial hypertension in pediatric patients with congenital heart disease (54). EPCs have also been reported to stratify risk in adult patients with chronic kidney disease (CKD),however the same did not hold true for pediatric patients with predialysis CKD (55).
While the role of EPCs as a biomarker for organ failure is promising, these cell levels are altered by multiple other factors including age, underlying chronic diseases such as diabetes mellitus, frequency of dialysis and the use of immunosuppressive drugs thus limiting its current value and application to pediatrics (56).
Exosomes are micro vesicles, roughly 30-100 nm in diameter, released from cells after fusion with an intermediate endocytic compartment (57). These microvesicles contain various biomolecular cargo that are transported across cell membranes. Under physiological conditions, exosomes are present and widely distributed in bodily fluids and are often treated as therapeutic targets or diagnostic and prognostic biomarkers in patients with cancer. Their widespread availability also make them an easily accessible noninvasive potential biomarker (58–60).
Sole et al examined miR-29c in urinary exosomes to determine whether patients with lupus nephritis would develop end-stage renal disease. They found that the contents of these microvesicles correlated with renal chronicity but not with renal function, suggesting that it could possibly be used as an early biomarker for development of renal fibrosis (31). Exosomes have also been used as biomarkers of renal injury within the context of preeclampsia. Gilani et al found that in women with preeclamptic podocyte related renal injuries, a significantly higher ratio of podocin-positive to nephrin-positive extracellular vesicles was found when compared to the urine of women with normotensive pregnancies, indicating proteinuria and renal injury (61).
Njock et al analyzed exosomes in the sputum to find biomarkers for idiopathic pulmonary fibrosis. They found exosomes containing mir-142-3p were negatively correlated with the diffusing capacity of the lungs and therefore severity of the disease (22). Lambrecht et al investigated the role of plasma exosomal miRNAs in distinguishing between healthy individuals and patients with hepatitis B and C who had early stage fibrosis. They found that certain exosomal miRNA cargos could be used to distinguish between healthy patients and HBV and HCV groups. However, whether these exosomes can diagnose liver fibrosis of any origin remains unclear (27). While the aforementioned studies highlight the potential for exosomes as a biomarker of organ failure in adults, there is currently a lack of similar research in pediatrics and further research is needed to evaluate its applicability in children.
Nucleosomes are complexes composed of a histone core surrounded by DNA base pairs. Under normal physiological conditions, nucleosomes are released during apoptosis. However in pathological conditions, as in the case of organ failure, the normal phagocytic clearance mechanisms are overwhelmed and nucleosomes are released into circulation (62). These nucleosomes are remarkably stable and can be measured from the serum using immunoassay techniques. Current studies focus on their role as biomarkers with which to diagnose patients with cancers or with which to stratify patients for more tailored therapy (63).
Nucleosome levels have also been shown to be capable of differentiating the acuity and pathogenesis of organ failure. In a cohort of surgical and non-surgical ICU patients, patients who were septic had higher levels of nucleosomes upon admission than those who were not. This, however, was comparable to already established clinical scoring systems and did not provide additional predictive benefit (64). Craig et al showed that there are elevated nucleosome levels in patients with ALF in comparison to patients with chronic liver disease. However, there was no significant difference in nucleosome levels in severity of liver dysfunction or outcome (65). Additionally, nucleosome levels have been shown to be adversely related to cardiac outcomes and also elevated in familial cardiomyopathy (66, 67) In pediatrics, elevated levels of nucleosomes were found to be associated with increased mortality in pediatric acute respiratory distress syndrome (p<0.001) (68).
Mitochondria are cellular organelles whose DNA (mtDNA) has been found to reflect a potential damage-associated molecular pattern. They are released extracellularly during necrosis in response to inflammation and have been found to be associated with the severity of a variety of diseases. Thus, mtDNA may be a potential biomarker for organ failure (69, 70). Publications that have examined the role of mtDNA in cancer focus on both copy number as a diagnostic and prognostic marker and on mutations within mtDNA as an additional prognostic marker (71–74).
Timmermans et al found mtDNA levels to be elevated in patients with septic shock. Di Caro et al additionally demonstrated this facet in pediatric patients (75). Dhondup showed low circulating levels of mtDNA to be associated with greater mortality in chronic heart failure. McGill et al found that elevated levels of mtDNA are associated with poorer outcomes in patients with liver failure (76–78). MtDNA can be isolated from the blood as well as urine and the latter has been explored as a biomarker for kidney injury. Eirin et al demonstrated elevated levels of mtDNA in patients with hypertension and its correlation with renal dysfunction, while Hu et al demonstrated urinary mtDNA to be a more sensitive predictor of AKI in post-operative patients than serum creatinine (32, 79). MtDNAs have also been shown to play a role in organ dysfunction and rejection post-transplant. Pollara et al demonstrated a correlation between elevated donor plasma mitochondrial DNA levels and early allograft dysfunction in liver transplant recipients, suggesting a role for circulating mtDAMPs in allograft outcomes (80).
Histones are proteins found extracellularly and within the nucleus that have been found to be elevated in patients with cancer and are associated with cell death and toxicity (81, 82). Abrams et al examined circulating histone levels in patients with trauma-induced lung injuries and found that high levels of circulating histones were associated with the incidence of acute lung injury and Sequential Organ Failure Assessment (SOFA) scores (83). Liu et al demonstrated that histones predicted disease severity in severe acute pancreatitis with higher predictive values for persistent organ failure and mortality than the currently used scoring indices for pancreatitis (34). Elevated histone levels have also been shown in patients with acute liver injury, acute kidney damage, and correlate with markers of disease severity and mortality (84, 85).
Other studies have analyzed the relationship between high levels of circulating histones and multiple organ failure. In patients with multiple organ dysfunction syndrome, there was a strong correlation between circulating histone levels and markers of organ injury, disease severity and p-SOFA scores. Furthermore, the authors observed that sera from patients with high histone levels were non-selectively toxic to primary cells from a variety of organs, including the lungs, livers and kidneys and therefore a possible mediator for multiple organ dysfunction syndrome (86).
Biomarkers are surrogate indirect indicators of a pathological or physiological process. In pediatrics, there has been limited progress in the identification and development of biomarkers to predict organ failure, its severity and outcome and its response to therapy. Identifying suitable biomarkers for organ dysfunction in pediatrics could potentially help improve risk stratification and possibly patient outcomes. It may also help to reduce the psychological stress, patients and their families may experience for more invasive procedures as well as reduce the health care costs and risks associated with these procedures which often require sedation.
Currently for biomarkers reported in the literature, there is a high degree of heterogeneity in the levels amongst patients based on age, sex and existing comorbidities. Levels of cfDNA for example are much higher in elderly patients due to decreased level of clearance by phagocytosis whilst changes in cfDNA methylation occur rapidly during childhood (87, 88). Limitations of these reported studies include lack of age-matched controls, limited sample sizes and lack of studies that included pediatric patients. These limitations make it impossible to assess age-related changes of the biomarkers reported and limits its generalizability to pediatric patients where age and weight specific normal ranges is unknown. Barriers to development of pediatric biomarkers include low prevalence of disease in pediatric vs adult patients and parental reluctance to participate in research, particularly for healthy controls making sample acquisition challenging (89).
Additionally in order to develop meaningful and clinically useful biomarkers, further research is needed to establish the optimal timing and method of sample collection as well as standardization of laboratory techniques. It should also be noted that none of these potential biomarkers in this review are truly organ-specific and may be a marker for multiple diseases thereby limiting its usefulness. Further work is therefore needed in distinguishing each biomarker from their respective molecular or cellular background in order to enhance its clinical utility. Presently there are multiple ongoing pediatric clinical trials to identify biomarkers in pediatric patients with lung, cardiac and renal injury amongst others (90–95).
Current ongoing or planned trials for pediatric oncology patients include the identification of biomarkers to detect cardiac injury and renal injury post chemotherapy (96–99).
Although there is still much work to be done, among pediatric oncology patients, there is promising utility for several of the biomarkers reviewed. Future studies might examine (i) the use of cfDNA and mtDNA post hematological or solid organ transplant in detecting organ rejection (ii) the use of MiRNA to determine risk of AKI among patients with post-surgical tumor resection (iii) serial sampling of EPCs in predicting progressive organ failure (iv) the use of histones as a predictor for multi-organ dysfunction syndrome and (v) the use of exosomes and nucleosomes to predict persistent or chronic organ failure in pediatric cancer patients.
Although many potential biomarkers exist to predict organ failure among pediatric cancer patients, all come with shared and unique challenges that limit their clinical value at this time. Additionally, while much research has been focused on heart failure and sepsis, a leading cause of multi-organ failure, there has been little headway in the application of these potential biomarkers to lung injury, for which there is currently no prognostic score or standard severity grading and diagnosis remains reliant on clinical markers. Despite the need for further studies, the data is promising. Pediatric oncology and critical care investigators should be encouraged to investigate these biomarkers further as they hold great potential for future use.
LD, SY, and DR were all major contributors in writing and editing this manuscript. RS, DP, KM, and SL were major contributors in editing the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Cohen EP, Pais P, Moulder JE. Chronic kidney disease after hematopoietic stem cell transplantation. Semin Nephrol (2010) 30(6):627–34. doi: 10.1016/j.semnephrol.2010.09.010
2. Faraci M, Bertaina A, Dalissier A, Ifversen M, Schulz A, Gennery A, et al. Solid organ transplantation after hematopoietic stem cell transplantation in childhood: A multicentric retrospective survey. Am J Transplant (2019) 19(6):1798–805. doi: 10.1111/ajt.152
3. Dean NP, Fenix JB, Spaeder M, Levin A. Evaluation of a Pediatric Early Warning Score Across Different Subspecialty Patients. Pediatr Crit Care Med (2017) 18(7):655–60. doi: 10.1097/PCC.0000000000001176
4. Graciano AL, Balko JA, Rahn DS, Ahmad N, Giroir BP. The Pediatric Multiple Organ Dysfunction Score (P-MODS): development and validation of an objective scale to measure the severity of multiple organ dysfunction in critically ill children. Crit Care Med (2005) 33(7):1484–91. doi: 10.1097/01.CCM.0000170943.23633.47
5. Marshall JC, Cook DJ, Christou NV, Bernard GR, Sprung CL, Sibbald WJ. Multiple organ dysfunction score: a reliable descriptor of a complex clinical outcome. Crit Care Med (1995) 23(10):1638–52. doi: 10.1097/00003246-199510000-00007
6. Hauser MJ, Tabak J, Baier H. Survival of patients with cancer in a medical critical care unit. Arch Intern Med (1982) 142(3):527–9. doi: 10.1001/archinte.1982.00340160107022
7. Rowan CM, Gertz SJ, McArthur J, Fitzgerald JC, Nitu ME, Loomis A, et al. Invasive Mechanical Ventilation and Mortality in Pediatric Hematopoietic Stem Cell Transplantation: A Multicenter Study. Pediatr Crit Care Med (2016) 17(4):294–302. doi: 10.1097/PCC.0000000000000673
8. de Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet (2003) 362(9380):316–22. doi: 10.1016/S0140-6736(03)13976-1
9. Association TCCotNYH. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston: Little, Brown & Co (1994). p. 253–6.
10. Kamath PS, Kim WR. Advanced Liver Disease Study G. The model for end-stage liver disease (MELD). Hepatology (2007) 45(3):797–805. doi: 10.1002/hep.21563
11. McDiarmid SV, Anand R, Lindblad AS, Principal I. Institutions of the Studies of Pediatric Liver Transplantation Research G. Development of a pediatric end-stage liver disease score to predict poor outcome in children awaiting liver transplantation. Transplantation (2002) 74(2):173–81. doi: 10.1097/00007890-200207270-00006
12. Kellum JAL, Norbert, Aspelin P, Barsoum RS, Burdmann EA, Goldstein SL, et al. Kidney disease: Improving global outcomes (KDIGO) acute kidney injury work group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl (2012) 2(1):1–138. doi: 10.1038/kisup.2012.2
13. Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA (2016) 315(8):801–10. doi: 10.1001/jama.2016.0287
14. Mohamed El-Mashad G, Said El-Mekkawy M, Helmy Zayan M. [Paediatric sequential organ failure assessment (pSOFA) score: A new mortality prediction score in the paediatric intensive care unit]. Pediatr (Barc) (2019). 92(5):277–85. doi: 10.1016/j.anpedi.2019.05.018
15. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med (1985) 13(10):818–29. doi: 10.1097/00003246-198510000-00009
16. Anders HJ, Vielhauer V, Schlondorff D. Chemokines and chemokine receptors are involved in the resolution or progression of renal disease. Kidney Int (2003) 63(2):401–15. doi: 10.1046/j.1523-1755.2003.00750.x
17. Matsui M, Roche L, Geroult S, Soupe-Gilbert ME, Monchy D, Huerre M, et al. Cytokine and Chemokine Expression in Kidneys during Chronic Leptospirosis in Reservoir and Susceptible Animal Models. PloS One (2016) 11(5):e0156084. doi: 10.1371/journal.pone.0156084
18. Bhatia M, Zemans RL, Jeyaseelan S. Role of chemokines in the pathogenesis of acute lung injury. Am J Respir Cell Mol Biol (2012) 46(5):566–72. doi: 10.1165/rcmb.2011-0392TR
19. Hartl D, Griese M, Nicolai T, Zissel G, Prell C, Reinhardt D, et al. A role for MCP-1/CCR2 in interstitial lung disease in children. Respir Res (2005) 6:93. doi: 10.1186/1465-9921-6-93
20. Cakmak HA, Coskunpinar E, Ikitimur B, Barman HA, Karadag B, Tiryakioglu NO, et al. The prognostic value of circulating microRNAs in heart failure: preliminary results from a genome-wide expression study. J Cardiovasc Med (Hagerstown) (2015) 16(6):431–7. doi: 10.2459/JCM.0000000000000233
21. Zhu Z, Liang L, Zhang R, Wei Y, Su L, Tejera P, et al. Whole blood microRNA markers are associated with acute respiratory distress syndrome. Intensive Care Med Exp (2017) 5(1):38. doi: 10.1186/s40635-017-0155-0
22. Njock MS, Guiot J, Henket MA, Nivelles O, Thiry M, Dequiedt F, et al. Sputum exosomes: promising biomarkers for idiopathic pulmonary fibrosis. Thorax (2019) 74(3):309–12. doi: 10.1136/thoraxjnl-2018-211897
23. Guiot J, Struman I, Chavez V, Henket M, Herzog M, Scoubeau K, et al. Altered epigenetic features in circulating nucleosomes in idiopathic pulmonary fibrosis. Clin Epigenet (2017) 9:84. doi: 10.1186/s13148-017-0383-x
24. Tao YC, Wang ML, Wang M, Ma YJ, Bai L, Feng P, et al. Quantification of circulating miR-125b-5p predicts survival in chronic hepatitis B patients with acute-on-chronic liver failure. Digest Liver Dis Off J Ital Soc Gastroenterol Ital Assoc Study Liver (2019) 51(3):412–8. doi: 10.1016/j.dld.2018.08.030
25. Zheng QF, Zhang JY, Wu JS, Zhang Y, Liu M, Bai L, et al. Upregulation of miRNA-130a Represents Good Prognosis in Patients With HBV-Related Acute-on-Chronic Liver Failure: A Prospective Study. Med (Baltimore) (2016) 95(6):e2639. doi: 10.1097/MD.0000000000002639
26. Schutz E, Fischer A, Beck J, Harden M, Koch M, Wuensch T, et al. Graft-derived cell-free DNA, a noninvasive early rejection and graft damage marker in liver transplantation: A prospective, observational, multicenter cohort study. PloS Med (2017) 14(4):e1002286. doi: 10.1371/journal.pmed.1002286
27. Lambrecht J, Jan Poortmans P, Verhulst S, Reynaert H, Mannaerts I, van Grunsven LA. Circulating ECV-Associated miRNAs as Potential Clinical Biomarkers in Early Stage HBV and HCV Induced Liver Fibrosis. Front Pharmacol (2017) 8:56. doi: 10.3389/fphar.2017.00056
28. Merkle J, Daka A, Deppe AC, Wahlers T, Paunel-Gorgulu A. High levels of cell-free DNA accurately predict late acute kidney injury in patients after cardiac surgery. PloS One (2019) 14(6):e0218548. doi: 10.1371/journal.pone.0218548
29. Aguado-Fraile E, Ramos E, Conde E, Rodriguez M, Martin-Gomez L, Lietor A, et al. A Pilot Study Identifying a Set of microRNAs As Precise Diagnostic Biomarkers of Acute Kidney Injury. PloS One (2015) 10(6):e0127175. doi: 10.1371/journal.pone.0127175
30. Fan PC, Chen CC, Peng CC, Chang CH, Yang CH, Yang C, et al. A circulating miRNA signature for early diagnosis of acute kidney injury following acute myocardial infarction. J Transl Med (2019) 17(1):139. doi: 10.1186/s12967-019-1890-7
31. Sole C, Cortes-Hernandez J, Felip ML, Vidal M, Ordi-Ros J. miR-29c in urinary exosomes as predictor of early renal fibrosis in lupus nephritis. Nephrol dialysis Transplant Off Publ Eur Dialysis Transplant Assoc - Eur Renal Association (2015) 30(9):1488–96. doi: 10.1093/ndt/gfv128
32. Hu Q, Ren J, Wu J, Li G, Wu X, Liu S, et al. Urinary Mitochondrial DNA Levels Identify Acute Kidney Injury in Surgical Critical Illness Patients. Shock (Augusta Ga) (2017) 48(1):11–7. doi: 10.1097/SHK.0000000000000830
33. Ha X-Q, Song Y-J, Zhao H-B, Ta W-W, Gao H-W, Feng Q-S, et al. Endothelial progenitor cells in peripheral blood may serve as a biological marker to predict severe acute pancreatitis. World J Gastroenterol (2017) 23(14):2592–600. doi: 10.3748/wjg.v23.i14.2592
34. Liu T, Huang W, Szatmary P, Abrams ST, Alhamdi Y, Lin Z, et al. Accuracy of circulating histones in predicting persistent organ failure and mortality in patients with acute pancreatitis. BJS (British J Surgery) (2017) 104(9):1215–25. doi: 10.1002/bjs.10538
35. Tapia P, Gatica S, Cortes-Rivera C, Otero C, Becerra A, Riedel CA, et al. Circulating Endothelial Cells From Septic Shock Patients Convert to Fibroblasts Are Associated With the Resuscitation Fluid Dose and Are Biomarkers for Survival Prediction. Crit Care Med (2019) 47(7):942–50. doi: 10.1097/CCM.0000000000003778
36. Mandel P, Metais P. Les acides nucléiques du plasma sanguine chez l’homme. C R Seances Soc Biol Fil (1948) 142(3-4):241–3.
37. Meddeb R, Dache ZAA, Thezenas S, Otandault A, Tanos R, Pastor B, et al. Quantifying circulating cell-free DNA in humans. Sci Rep (2019) 9(1):5220. doi: 10.1038/s41598-019-41593-4
38. Karlas T, Weise L, Kuhn S, Krenzien F, Mehdorn M, Petroff D, et al. Correlation of cell-free DNA plasma concentration with severity of non-alcoholic fatty liver disease. J Transl Med (2017) 15(1):106. doi: 10.1186/s12967-017-1208-6
39. Agbor-Enoh S, Wang Y, Tunc I, Jang MK, Davis A, De Vlaminck I, et al. Donor-derived cell-free DNA predicts allograft failure and mortality after lung transplantation. EBioMedicine (2019) 40:541–53. doi: 10.1016/j.ebiom.2018.12.029
40. North PE, Ziegler E, Mahnke DK, Stamm KD, Thomm A, Daft P, et al. Cell-free DNA donor fraction analysis in pediatric and adult heart transplant patients by multiplexed allele-specific quantitative PCR: Validation of a rapid and highly sensitive clinical test for stratification of rejection probability. PloS One (2020) 15(1):e0227385. doi: 10.1371/journal.pone.0227385
41. Bartel DP. MicroRNAs: target recognition and regulatory functions. Cell (2009) 136(2):215–33. doi: 10.1016/j.cell.2009.01.002
42. Shi N, Deng L, Chen W, Zhang X, Luo R, Jin T, et al. Is MicroRNA-127 a Novel Biomarker for Acute Pancreatitis with Lung Injury? Dis Markers (2017) 2017:1204295. doi: 10.1155/2017/1204295
43. Zhou M, Wang X, Shi H, Cheng L, Wang Z, Zhao H, et al. Characterization of long non-coding RNA-associated ceRNA network to reveal potential prognostic lncRNA biomarkers in human ovarian cancer. Oncotarget (2016) 7(11):12598–611. doi: 10.18632/oncotarget.7181
44. Jin X, Chen Y, Chen H, Fei S, Chen D, Cai X, et al. Evaluation of Tumor-Derived Exosomal miRNA as Potential Diagnostic Biomarkers for Early-Stage Non-Small Cell Lung Cancer Using Next-Generation Sequencing. Clin Cancer Res (2017) 23(17):5311–9. doi: 10.1158/1078-0432.CCR-17-0577
45. Schneider S, Silvello D, Martinelli NC, Garbin A, Biolo A, Clausell N, et al. Plasma levels of microRNA-21, -126 and -423-5p alter during clinical improvement and are associated with the prognosis of acute heart failure. Mol Med Rep (2018) 17(3):4736–46. doi: 10.3892/mmr.2018.8428
46. Goren Y, Kushnir M, Zafrir B, Tabak S, Lewis BS, Amir O. Serum levels of microRNAs in patients with heart failure. Eur J Heart Fail (2012) 14(2):147–54. doi: 10.1093/eurjhf/hfr155
47. Dubin PH, Yuan H, Devine RK, Hynan LS, Jain MK, Lee WM, et al. Micro-RNA-122 levels in acute liver failure and chronic hepatitis C. J Med Virol (2014) 86(9):1507–14. doi: 10.1002/jmv.23987
48. Roderburg C, Benz F, Vargas Cardenas D, Koch A, Janssen J, Vucur M, et al. Elevated miR-122 serum levels are an independent marker of liver injury in inflammatory diseases. Liver Int Off J Int Assoc Study Liver (2015) 35(4):1172–84. doi: 10.1111/liv.12627
49. Weis A, Marquart L, Calvopina DA, Genz B, Ramm GA, Skoien R. Serum MicroRNAs as Biomarkers in Hepatitis C: Preliminary Evidence of a MicroRNA Panel for the Diagnosis of Hepatocellular Carcinoma. Int J Mol Sci (2019) 20(4):864. doi: 10.3390/ijms20040864
50. Wang HH, Cui YL, Zaorsky NG, Lan J, Deng L, Zeng XL, et al. Mesenchymal stem cells generate pericytes to promote tumor recurrence via vasculogenesis after stereotactic body radiation therapy. Cancer Lett (2016) 375(2):349–59. doi: 10.1016/j.canlet.2016.02.033
51. Werner N, Kosiol S, Schiegl T, Ahlers P, Walenta K, Link A, et al. Circulating endothelial progenitor cells and cardiovascular outcomes. N Engl J Med (2005) 353(10):999–1007. doi: 10.1056/NEJMoa043814
52. Moazzami K, Lima BB, Hammadah M, Ramadan R, Al Mheid I, Kim JH, et al. Association Between Change in Circulating Progenitor Cells During Exercise Stress and Risk of Adverse Cardiovascular Events in Patients With Coronary Artery Disease. JAMA Cardiol (2019) 5(2):147–55. doi: 10.1001/jamacardio.2019.4528
53. Liu J, Zou GJ, Yang L, Rong S, Li BQ, Tong ZH, et al. Early Prediction of Persistent Organ Failure by Circulating Endothelial Progenitor Cells in Patients With Acute Pancreatitis. Shock (Augusta Ga) (2018) 50(3):265–72. doi: 10.1097/SHK.0000000000001065
54. Sun HX, Li GJ, Du ZH, Bing Z, Ji ZX, Luo G, et al. The relationship between endothelial progenitor cells and pulmonary arterial hypertension in children with congenital heart disease. BMC Pediatr (2019) 19(1):502. doi: 10.1186/s12887-019-1884-x
55. Jie KE, Zaikova MA, Bergevoet MW, Westerweel PE, Rastmanesh M, Blankestijn PJ, et al. Progenitor cells and vascular function are impaired in patients with chronic kidney disease. Nephrol Dial Transplant (2010) 25(6):1875–82. doi: 10.1093/ndt/gfp749
56. Ozkok A, Yildiz A. Endothelial Progenitor Cells and Kidney Diseases. Kidney Blood Press Res (2018) 43(3):701–18. doi: 10.1159/000489745
57. Johnstone RM, Adam M, Hammond JR, Orr L, Turbide C. Vesicle formation during reticulocyte maturation. Association of plasma membrane activities with released vesicles (exosomes). J Biol Chem (1987) 262(19):9412–20.
58. Zhao Z, Yang Y, Zeng Y, He M. A microfluidic ExoSearch chip for multiplexed exosome detection towards blood-based ovarian cancer diagnosis. Lab Chip (2016) 16(3):489–96. doi: 10.1039/C5LC01117E
59. Liu Q, Yu Z, Yuan S, Xie W, Li C, Hu Z, et al. Circulating exosomal microRNAs as prognostic biomarkers for non-small-cell lung cancer. Oncotarget (2017) 8(8):13048–58. doi: 10.18632/oncotarget.14369
60. Liu T, Zhang X, Gao S, Jing F, Yang Y, Du L, et al. Exosomal long noncoding RNA CRNDE-h as a novel serum-based biomarker for diagnosis and prognosis of colorectal cancer. Oncotarget (2016) 7(51):85551–63. doi: 10.18632/oncotarget.13465
61. Gilani SI, Anderson UD, Jayachandran M, Weissgerber TL, Zand L, White WM, et al. Urinary Extracellular Vesicles of Podocyte Origin and Renal Injury in Preeclampsia. J Am Soc Nephrol (2017) 28(11):3363–72. doi: 10.1681/ASN.2016111202
62. Holdenrieder S, Stieber P. Clinical use of circulating nucleosomes. Crit Rev Clin Lab Sci (2009) 46(1):1–24. doi: 10.1080/10408360802485875
63. Bauden M, Pamart D, Ansari D, Herzog M, Eccleston M, Micallef J, et al. Circulating nucleosomes as epigenetic biomarkers in pancreatic cancer. Clin Epigenet (2015) 7:106. doi: 10.1186/s13148-015-0139-4
64. Chen Q, Ye L, Jin Y, Zhang N, Lou T, Qiu Z, et al. Circulating nucleosomes as a predictor of sepsis and organ dysfunction in critically ill patients. Int J Infect Dis (2012) 16(7):e558–64. doi: 10.1016/j.ijid.2012.03.007
65. Craig DG, Lee P, Pryde EA, Masterton GS, Hayes PC, Simpson KJ. Circulating apoptotic and necrotic cell death markers in patients with acute liver injury. Liver Int (2011) 31(8):1127–36. doi: 10.1111/j.1478-3231.2011.02528.x
66. Yang G, Chen S, Ma A, Lu J, Wang T. Identification of the difference in the pathogenesis in heart failure arising from different etiologies using a microarray dataset. Clinics (Sao Paulo) (2017) 72(10):600–8. doi: 10.6061/clinics/2017(10)03
67. Nymo SH, Ueland T, Askevold E, Dahl CP, Gullestad L, Aukrust P, et al. Circulating nucleosomes in chronic heart failure. Int J Cardiol (2016) 203:742–3. doi: 10.1016/j.ijcard.2015.10.219
68. Yehya N, Thomas NJ, Margulies SS. Circulating nucleosomes are associated with mortality in pediatric acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol (2016) 310(11):L1177–84. doi: 10.1152/ajplung.00067.2016
69. Harrington JS, Choi AMK, Nakahira K. Mitochondrial DNA in Sepsis. Curr Opin Crit Care (2017) 23(4):284–90. doi: 10.1097/MCC.0000000000000427
70. Al Amir Dache Z, Otandault A, Tanos R, Pastor B, Meddeb R, Sanchez C, et al. Blood contains circulating cell-free respiratory competent mitochondria. FASEB J (2020) 34(3):3616–30. doi: 10.1096/fj.201901917RR
71. Weerts MJ, Sieuwerts AM, Smid M, Look MP, Foekens JA, Sleijfer S, et al. Mitochondrial DNA content in breast cancer: Impact on in vitro and in vivo phenotype and patient prognosis. Oncotarget (2016) 7(20):29166–76. doi: 10.18632/oncotarget.8688
72. Reznik E, Miller ML, Senbabaoglu Y, Riaz N, Sarungbam J, Tickoo SK, et al. Mitochondrial DNA copy number variation across human cancers. Elife (2016) 5:e10769. doi: 10.7554/eLife.10769
73. Gopal RK, Kubler K, Calvo SE, Polak P, Livitz D, Rosebrock D, et al. Widespread Chromosomal Losses and Mitochondrial DNA Alterations as Genetic Drivers in Hurthle Cell Carcinoma. Cancer Cell (2018) 34(2):242–55 e5. doi: 10.1016/j.ccell.2018.06.013
74. Li S, Wan P, Peng T, Xiao K, Su M, Shang L, et al. Associations between sequence variations in the mitochondrial DNA D-loop region and outcome of hepatocellular carcinoma. Oncol Lett (2016) 11(6):3723–8. doi: 10.3892/ol.2016.4466
75. Di Caro V, Walko TD,3, Bola RA, Hong JD, Pang D, Hsue V, et al. Plasma Mitochondrial DNA–a Novel DAMP in Pediatric Sepsis. Shock (2016) 45(5):506–11. doi: 10.1097/SHK.0000000000000539
76. Timmermans K, Kox M, Scheffer GJ, Pickkers P. Plasma Nuclear and Mitochondrial DNA Levels, and Markers of Inflammation, Shock, and Organ Damage in Patients with Septic Shock. Shock (2016) 45(6):607–12. doi: 10.1097/SHK.0000000000000549
77. Dhondup Y, Ueland T, Dahl CP, Askevold ET, Sandanger O, Fiane A, et al. Low Circulating Levels of Mitochondrial and High Levels of Nuclear DNA Predict Mortality in Chronic Heart Failure. J Card Fail (2016) 22(10):823–8. doi: 10.1016/j.cardfail.2016.06.013
78. McGill MR, Staggs VS, Sharpe MR, Lee WM, Jaeschke H. Acute Liver Failure Study G. Serum mitochondrial biomarkers and damage-associated molecular patterns are higher in acetaminophen overdose patients with poor outcome. Hepatology (2014) 60(4):1336–45. doi: 10.1002/hep.27265
79. Eirin A, Saad A, Tang H, Herrmann SM, Woollard JR, Lerman A, et al. Urinary Mitochondrial DNA Copy Number Identifies Chronic Renal Injury in Hypertensive Patients. Hypertension (Dallas Tex 1979) (2016) 68(2):401–10. doi: 10.1161/HYPERTENSIONAHA.116.07849
80. Pollara J, Edwards RW, Lin L, Bendersky VA, Brennan TV. Circulating mitochondria in deceased organ donors are associated with immune activation and early allograft dysfunction. JCI Insight (2018) 3(15): e121622. doi: 10.1172/jci.insight.121622
81. Kang R, Xie Y, Zhang Q, Hou W, Jiang Q, Zhu S, et al. Intracellular HMGB1 as a novel tumor suppressor of pancreatic cancer. Cell Res (2017) 27(7):916–32. doi: 10.1038/cr.2017.51
82. Thalin C, Lundstrom S, Seignez C, Daleskog M, Lundstrom A, Henriksson P, et al. Citrullinated histone H3 as a novel prognostic blood marker in patients with advanced cancer. PloS One (2018) 13(1):e0191231. doi: 10.1371/journal.pone.0191231
83. Abrams ST, Zhang N, Manson J, Liu T, Dart C, Baluwa F, et al. Circulating histones are mediators of trauma-associated lung injury. Am J Respir Crit Care Med (2013) 187(2):160–9. doi: 10.1164/rccm.201206-1037OC
84. Wen Z, Lei Z, Yao L, Jiang P, Gu T, Ren F, et al. Circulating histones are major mediators of systemic inflammation and cellular injury in patients with acute liver failure. Cell Death Dis (2016) 7(9):e2391. doi: 10.1038/cddis.2016.303
85. Nakazawa D, Kumar SV, Marschner J, Desai J, Holderied A, Rath L, et al. Histones and Neutrophil Extracellular Traps Enhance Tubular Necrosis and Remote Organ Injury in Ischemic AKI. J Am Soc Nephrol (2017) 28(6):1753–68. doi: 10.1681/ASN.2016080925
86. Cheng Z, Abrams ST, Alhamdi Y, Toh J, Yu W, Wang G, et al. Circulating Histones Are Major Mediators of Multiple Organ Dysfunction Syndrome in Acute Critical Illnesses. Crit Care Med (2019) 47(8):e677–e84. doi: 10.1097/CCM.0000000000003839
87. Islam SA, Goodman SJ, MacIsaac JL, Obradovic J, Barr RG, Boyce WT, et al. Integration of DNA methylation patterns and genetic variation in human pediatric tissues help inform EWAS design and interpretation. Epigenet Chromatin (2019) 12(1):1. doi: 10.1186/s13072-018-0245-6
88. Jylhava J, Kotipelto T, Raitala A, Jylha M, Hervonen A, Hurme M. Aging is associated with quantitative and qualitative changes in circulating cell-free DNA: the Vitality 90+ study. Mech Ageing Dev (2011) 132(1-2):20–6. doi: 10.1016/j.mad.2010.11.001
89. Shores DR, Everett AD. Children as Biomarker Orphans: Progress in the Field of Pediatric Biomarkers. J Pediatr (2018) 193:14–20 e31. doi: 10.1016/j.jpeds.2017.08.077
90. Genetic Variability and Biomarkers in Children With Acute Lung Injury. Available at: https://ClinicalTrials.gov/show/NCT01048996.
91. Identifying PARDS Endotypes. Available at: https://ClinicalTrials.gov/show/NCT03539783.
92. Predictive Value of Troponin I for Acute Respiratory Distress Syndrome in Children With Shock. Available at: https://ClinicalTrials.gov/show/NCT02361840.
93. Prognostication Biomarkers in Pediatric Cardiac Arrest. Available at: https://ClinicalTrials.gov/show/NCT02769026.
94. Use of Biomarkers to Optimize Fluid Dosing,CRRT Initiation and Discontinuation in Pediatric ICU Patients With AKI. Available at: https://ClinicalTrials.gov/show/NCT01416298.
95. Use of NGAL for Fluid Dosing and CRRT Initiation in Pediatric AKI. Available at: https://ClinicalTrials.gov/show/NCT03541785.
96. Cancer Therapy Effects on the Heart. Available at: https://ClinicalTrials.gov/show/NCT04262830.
97. Preventing Cardiac Sequelae in Pediatric Cancer Survivors. Available at: https://ClinicalTrials.gov/show/NCT01805778.
98. Study to Evaluate Blood and Urine Kidney Injury Markers to Facilitate Early Detection of Renal Adverse Drug Events in Pediatric Cancer Patients Treated With Nephrotoxic Chemotherapy. Available at: https://ClinicalTrials.gov/show/NCT04308642.
99. Cisplatin Induced Kidney Toxicity. Available at: https://ClinicalTrials.gov/show/NCT04442516.
Keywords: oncology, organ failure, liquid biopsy, biomarkers, diagnostics
Citation: Dao L, Ragoonanan D, Yi S, Swinford R, Petropoulos D, Mahadeo KM and Li S (2020) The Organ Trail: A Review of Biomarkers of Organ Failure. Front. Oncol. 10:579219. doi: 10.3389/fonc.2020.579219
Received: 02 July 2020; Accepted: 15 October 2020;
Published: 11 November 2020.
Edited by:
Ronald Ray Morrison, St. Jude Children’s Research Hospital, United StatesReviewed by:
Pietro Merli, Bambino Gesù Children Hospital (IRCCS), ItalyCopyright © 2020 Dao, Ragoonanan, Yi, Swinford, Petropoulos, Mahadeo and Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shulin Li, c2xpNEBtZGFuZGVyc29uLm9yZw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.