 Alexandre Bertucci1
Alexandre Bertucci1 François Bertucci1,2,3
François Bertucci1,2,3 Christophe Zemmour2Florence Lerebours4
Christophe Zemmour2Florence Lerebours4 Jean-Yves Pierga4,5
Jean-Yves Pierga4,5 Christelle Levy6
Christelle Levy6 Florence Dalenc7Julien Grenier8Thierry Petit9
Florence Dalenc7Julien Grenier8Thierry Petit9 Marguerite Berline2
Marguerite Berline2 Anthony Gonçalves1,2,3,10*
Anthony Gonçalves1,2,3,10*- 1Département d’Oncologie Médicale, Institut Paoli-Calmettes, Centre de Recherche en Cancérologie de Marseille (CRCM), INSERM UMR1068, CNRS UMR7258, Aix-Marseille Université, Marseille, France
- 2Laboratoire d’Oncologie Prédictive, CRCM, Institut Paoli-Calmettes, INSERM UMR1068, CNRS UMR7258, Aix-Marseille Université, Marseille, France
- 3Aix-Marseille Université, Faculté de Médecine, Marseille, France
- 4Département d’Oncologie Médicale, Institut Curie, Saint-Cloud, France
- 5Département d’Oncologie Médicale, Institut Curie, Université de Paris, Paris, France
- 6Breast Cancer Unit, François Baclesse Cancer Centre, Caen, France
- 7Département d’Oncologie Médicale, Institut Claudius Regaud, Institut Universitaire du Cancer, Oncopole Toulouse, France
- 8Département d’Oncologie Médicale, Institut Sainte Catherine, Avignon, France
- 9Département d’Oncologie Médicale, Centre Paul-Strauss, Strasbourg, France
- 10Oncodistinct Network, Bruxelles, Belgium
Inflammatory breast cancer (IBC) is a highly aggressive entity with a poor outcome and relative resistance to treatment. Despite progresses achieved during the last decades, the survival remains significantly lower than non-IBC. Recent clinical trials assessing PD-1/PD-L1 inhibitors showed promising results in non-IBC. Pembrolizumab, an anti-PD-1 monoclonal antibody, revolutionized the treatment of different cancers. Several recent studies suggested a potential interest of targeting the immune system in IBC by revealing a more frequent PD-L1 expression and an enriched immune microenvironment when compared with non-IBC. Here, we describe the rationale and design of PELICAN-IPC 2015-016/Oncodistinct-003 trial, an open-label, randomized, non-comparative, phase II study assessing efficacy, and safety of pembrolizumab in combination with anthracycline-containing neoadjuvant chemotherapy in HER2-negative IBC. The trial is ongoing. The primary endpoint is the pCR rate (ypT0/Tis, ypN0) in overall population and the co-primary endpoint is safety profile during a run-in phase. Key secondary objectives include tolerability, invasive disease-free, event-free and overall survivals, as well as collection of tumor and blood samples for translational research.
Clinical Trial Registration: https://clinicaltrials.gov/ (NCT03515798).
Introduction
Inflammatory breast cancer (IBC) is an uncommon (less than 5% of all BC) and very aggressive form of locally advanced BC. IBC has a clinical definition, which includes a rapidly (less than 6 months) enlarging, erythematous (which has to occupy at least one-third of the breast) and edematous breast (known as “peau d’orange”), which often presents without any underlying breast mass (1–3). Women with IBC are typically diagnosed at a younger age than patients with non-IBC (4, 5). IBCs are more frequently ductal than non-IBCs, with more frequent high grade, axillary lymph node involvement and metastases (more than 30%) at diagnosis (6, 7).
Biologically also, IBCs differs from non-IBCs, with more frequent hormone receptor (HR)-negativity and HER2-positivity (˜40% versus 15% in non-IBC) (8, 9), and a more angiogenic phenotype (10). IBCs display higher vascularity and an increased microvessel density (11, 12), and frequently include the presence of dermal lymphovascular emboli (13, 14). During the last two decades, IBC clinical tumor samples have been profiled using high-throughput molecular profiling technologies, mainly based on transcriptome analysis, in order to better delineate the molecular biology of disease (15). In 2013, the World IBC Consortium identified a robust 79-gene expression signature discriminating IBCs versus non-IBCs samples independently form the molecular subtypes (16). This signature notably suggested that alterations in TGF-β and immune response pathways are involved in the biology of IBC. Therefore, a particular tumor immune microenvironment is likely to participate into the unique biological patterns associated with IBC. Such importance of the tumor stroma has then been underlined by other research groups (17).
Significant therapeutic progresses were achieved during the past 50 years using a multidisciplinary approach, including neoadjuvant chemotherapy (NACT), followed by surgery and radiation therapy, and adjuvant anti-HER2 treatment and/or endocrine therapy –when indicated. However, the survival of IBC patients, when matched stage for stage, remains inferior to that of non-IBC patients. Research efforts are ongoing for many years to improve the treatment of disease. Due to the scarcity of the disease, its rapid progression and its unfavorable outcome, IBC-specific clinical trials have been rare. When they are not excluded, IBC patients are included in non-specific studies, being considered as locally advanced BC. Here, we present the rationale and the design of PELICAN-IPC 2015-016/Oncodistinct-003 trial, an open-label, multicentric, randomized, non-comparative, phase II study evaluating efficacy and safety of pembrolizumab in combination with neoadjuvant chemotherapy in HER2-negative IBC.
Neoadjuvant Chemotherapy in IBC
Historically, the long-term survival was dramatically low (<5%) when patients were treated with loco-regional treatment only, suggesting the strong metastatic potential of IBC. Incorporation of multi-agent NACT in the therapeutic strategy significantly improved the prognosis, and achievement of pathological complete response after chemotherapy was identified as a favorable prognostic factor.
Advances in IBC have been made paralleling locally advanced non-IBC such as multi-agent NACT including anthracycline-based regimen with addition of taxanes, and more recently with incorporation of anti-HER2 targeted therapies (trastuzumab, pertuzumab, neratinib, trastuzumab-emtansine) in HER2 amplified disease (18–22). Three IBC-specific trials evaluated addition of bevacizumab in HER2-positive (23) and HER2-negative (24) IBC in the neoadjuvant and adjuvant setting, and panitumumab (an anti-EGFR monoclonal antibody) in HER2-negative IBC in the neoadjuvant setting (25). Results were promising with bevacizumab in HER2-positive and with panitumumab in triple-negative (TN) IBC, but these drugs are not recommended in routine. To our knowledge there is no ongoing IBC-specific study further evaluating these agents. Importantly, these trials showed the feasibility of IBC-dedicated clinical trials, with more than 50 patients enrolled per year in the two French multicentric trials (23, 24). However, and despite the benefit of NACT, the results are insufficient, with a 5-year survival remaining between 30% and 50%. Thus, it remains crucial to improve the results by optimizing neoadjuvant systemic regimen.
Immune Microenvironment in IBC
Escape from immune destruction is an important way set up by cancers to promote cell transformation and favor tumor growth, which has been known for decades in various tumor models. In BC, this process was more recently enlightened. Thus, various features associated with immune response have a significant predictive impact on therapeutic efficacy and survival. In BC and also IBC, tumor infiltrating lymphocytes (TIL) (26–28) and immune gene expression signatures have shown a prognostic impact, in particular for ER-negative and/or high proliferating tumors (29–32). Interestingly, studies on small BC series have also indicated that some NACT regimens, such as anthracyclines-taxanes combinations, could favor the attraction of lymphocytes to the tumor bed (33, 34). The Programmed cell death 1 (PD-1) receptor-ligand interaction is a major inhibitor pathway hijacked by tumors to suppress immune control (35–41). Under physiological conditions, when PD-1, which is expressed on the cell surface of activated T-cells, is engaged by its ligands, Programmed death-ligand 1 and 2 (PD-L1 and/or PD-L2), it mitigates lymphocyte activation and promotes T-regulatory cell development and function, allowing to terminate the immune response. PD-L1 and PD-L2 are either constitutively expressed or induced in various tissues, including different neoplastic diseases. PD-L2 regulates T-cell activation in lymphoid tissues, whereas PD-L1 serves to limit unneeded T-cell function in peripheral organs and tissues. Several studies have examined PD-L1 expression in BC at ARN and protein levels, using different scoring systems: various expression rates have been reported ranging from less than 2% to 55%, with discordant prognostic impact (42–49). Our group retrospectively analyzed PD-L1 mRNA expression in 45 BC cell lines and 5,454 clinical BC. Compared to normal tissue, we found PD-L1 expression as increased in 20% of clinical samples, and in almost 40% of basal-like subtypes. Expression of PD-L1 was associated with biological evidences of major cytotoxic immune response, such as TCR-related gene expression, indicative of a high T-cell infiltration. PD-L1 overexpression was not associated with survival in the overall population, but with better metastasis-free survival (MFS) and overall survival (OS) in basal-like tumors, independently from the clinico-pathological features. The pCR rate after NACT was higher in case of increased PD-L1 expression (50% versus 21%) (48).
Few studies have been specifically dedicated to IBC. In the World IBC Consortium series including 87 informative IBC samples (50), we identified and validated a robust 107-gene signature associated with pCR and strongly enriched for genes involved in both adaptative and innate immunity. In a cohort of 306 BC samples (51), including 112 IBC samples, PD-L1 was overexpressed in 38% of IBC samples compared to normal breast tissue. Such overexpression correlated with aggressive molecular subtypes (TNBC or basal-like and HER2-positive subtypes) and with a higher pCR rate to NACT as well as biological signs of antitumor T-cell cytotoxic response. There was no correlation with MFS and specific OS. Microenvironment of “PD-L1-high” IBC samples was in favor of a strong local cytotoxic immune response, with higher expression of T-cell-specific and CD8+ T-cell-specific gene signatures, and higher expression of T-cell receptor-related genes. In addition, these tumors displayed features of T-cell activation. However, some T-cells infiltrating the tumor had a phenotype of exhausted T-cells. Similar observations were reported at the protein level (52). In a recent study including 143 patients with IBC and 142 control subtype-matched patients with non-IBC, PD-L1 IHC expression on immune cells (SP142 antibody) was more frequent in IBC (42.9%) than in non-IBC (23.7%), and correlated with higher pCR rate and stromal TIL infiltration (53). This later was associated with improved overall survival in a multivariate model. Finally, recent next-generation sequencing studies have shown that IBC samples display higher tumor mutational burden (TMB) than non-IBC samples, independently from the molecular subtypes and tumor stage (54, 55). Such increased TMB in IBC might lead to increased tumor antigen-based attraction of cytotoxic T-cells and better sensitivity to immune checkpoint inhibitors.
Pembrolizumab and Other Anti-PD1/PD-L1 Agents in BC
Pembrolizumab, a humanized immunoglobulin (IgG4) monoclonal antibody (mAb), binds PD-1 with a high specificity, blocks the interaction with PD-L1 and PD-L2, and reactivates inhibited T-cells, which is expected to increase the antitumor immune response. This drug and other immune checkpoint inhibitors (ICI) targeting the PD-1/PD-L1 axis showed evidences of antitumor activity in several cancers, with a favorable toxicity profile compared to conventional chemotherapy. They are already registered in various indications, especially in the management of non-small cell lung cancer, melanoma, renal carcinoma, and classical Hodgkin lymphoma.
When administered as single agent in advanced BC, pembrolizumab, and other ICI such as atezolizumab or avelumab generated moderate but detectable antitumor activity, with objective response rate ranging between 3 to 18% (56). Of note, efficacy was higher in patients with TNBC, minimal pre-treatment exposure, and PD-L1- and/or TILs-positive tumors. Yet, in the KEYNOTE119 randomized phase III study involving pre-treated advanced TNBC, pembrolizumab was not better than chemotherapy at physician’s choice (57).
There is also a solid rationale to combine anti-PD1/PD-L1 agents with chemotherapy in BC, which may have significant immunomodulatory effects, and may in turn increase the antitumor activity of PD-1 pathway inhibition (58, 59). Indeed, even though cytotoxic drugs have historically been considered as immunosuppressive, they can also have pro-immune properties (60–67) by i) depleting immuno-suppressive cells, including regulatory T-cells and myeloid-derived suppressor cells, which stimulate a quiescent anti-tumor immune response, ii) inducing an immunogenic cell death, iii) improving presentation of tumor antigens by upregulating their expression or that of the major histocompatibility complex (MHC) class I molecules, iv) up-regulating co-stimulatory molecules (B7-1) or down-regulating co-inhibitory molecules (PD-L1 or B7-H4) expressed on tumor or immune cells, thus boosting the activity of T-cell effectors, and vi) enhancing tumor cells sensitivity to T-cell–mediated lysis through fas-, perforin-, and granzyme B–dependent mechanisms.
Recent results from clinical studies in TNBC have confirmed the potential for combination of chemotherapy and ICI. First, in the IMpassion130 phase III randomized study, first-line atezolizumab plus nab-paclitaxel improved progression-free survival over nab-paclitaxel alone in advanced TNBC. Benefit was restricted to patients with PD-L1-positive tumors, in which a strong numerical advantage in OS was suggested, leading to approval by both FDA and EMA (68). Very recently, first results of the KEYNOTE-355 phase III randomized trial (69), comparing several chemotherapy regimens (nab-paclitaxel, paclitaxel or carboplatine plus gemcitabine) plus placebo versus chemotherapy plus pembrolizumab in the same setting, have confirmed IMPassion130 results in terms of progression-free survival for patients with PD-L1 combined Positive Score (CPS) 10. However, statistical significance was not achieved in PD-L1 CPS 1 patients and OS data are still immature. In addition, IMpassion 131 failed to demonstrate any advantage for atezolizumab in combination with paclitaxel over paclitaxel alone (70). IMpassion 132, which evaluates atezolizumab with capecitabine or carboplatin-gemcitabine is still ongoing (71). Second, a significant improvement in pCR rate was recently reported when pembrolizumab was added to NACT (carboplatin/paclitaxel followed by AC) in non-metastatic TNBC, while preliminary analysis suggested a possible and promising advantage in event-free survival (72, 73). A similar improvement in pCR was recently demonstrated with atezolizumab when combined with anthracyclines/taxanes but carboplatin-free NACT in IMpassion 031 trial (74). Yet, results from other studies evaluating anti-PD-L1 antibodies such as durvalumab, another anti-PD-L1 antibody in combination with anthracyclines/taxanes (75), or atezolizumab in combination with anthracyclines-free regimen (NeoTripp trial: NCT002620280) NACT in TNBC failed to significantly improve pCR rates (76). Thus, the role of ICI in NACT of early BC remains to be defined. Of note, in both advanced and early settings, no new signal of toxicity was detected, and tolerance was similar to what expected with ICI in other tumor types.
Methods of PELICAN-IPC 2015-016/ONCODISTINCT-003 Study
The currently insufficient results of NACT in IBC, the relatively peculiar immune microenvironment of IBC when compared to non-IBC, and efficacy of pembrolizumab in BC led us to launch the PELICAN trial.
Study Design and Participants
PELICAN-IPC 2015-016/Oncodistinct-003 is a prospective, multicenter, open-label, randomized, non-comparative, phase II study evaluating pembrolizumab in combination with NACT in HER2-negative IBC. The trial was registered in ClinicalTrials.gov database (NCT03515798). The study, promoted by Institut Paoli-Calmettes (Marseille, France) is being conducted in up to 21 centers (13 in France, 8 in Belgium), 10 of them being activated on January 2020. Patients are eligible to the study, if they have a previously untreated, histologically-confirmed diagnosis of HER2-negative IBC as defined according to 8th American Joint Committee on Cancer (AJCC) classification: breast erythema, edema and/or peau d’orange, occupying at least 1/3 of the breast, with or without underlying palpable mass, duration of history of no more than 6 months. The main other inclusion and exclusion criteria are listed in Table 1. In PELICAN trial, all HER2-negative IBC patients are eligible, resulting in a mixed population of triple-negative and hormone receptor-positive/HER2-negative tumors. While we acknowledge that this is a significant limitation of the study, this is justified by the rarity of the disease and the anticipated difficulties of recruitment if restricted to a single IBC subtype. In addition, previous studies in the field, which provided the basis to our statistical hypothesis, were performed in a similar setting. Moreover, the design includes stratification on hormone receptor status and will allow a specific analysis in triple negative subtype, the most likely to benefit according to recent results (see Statistics section).
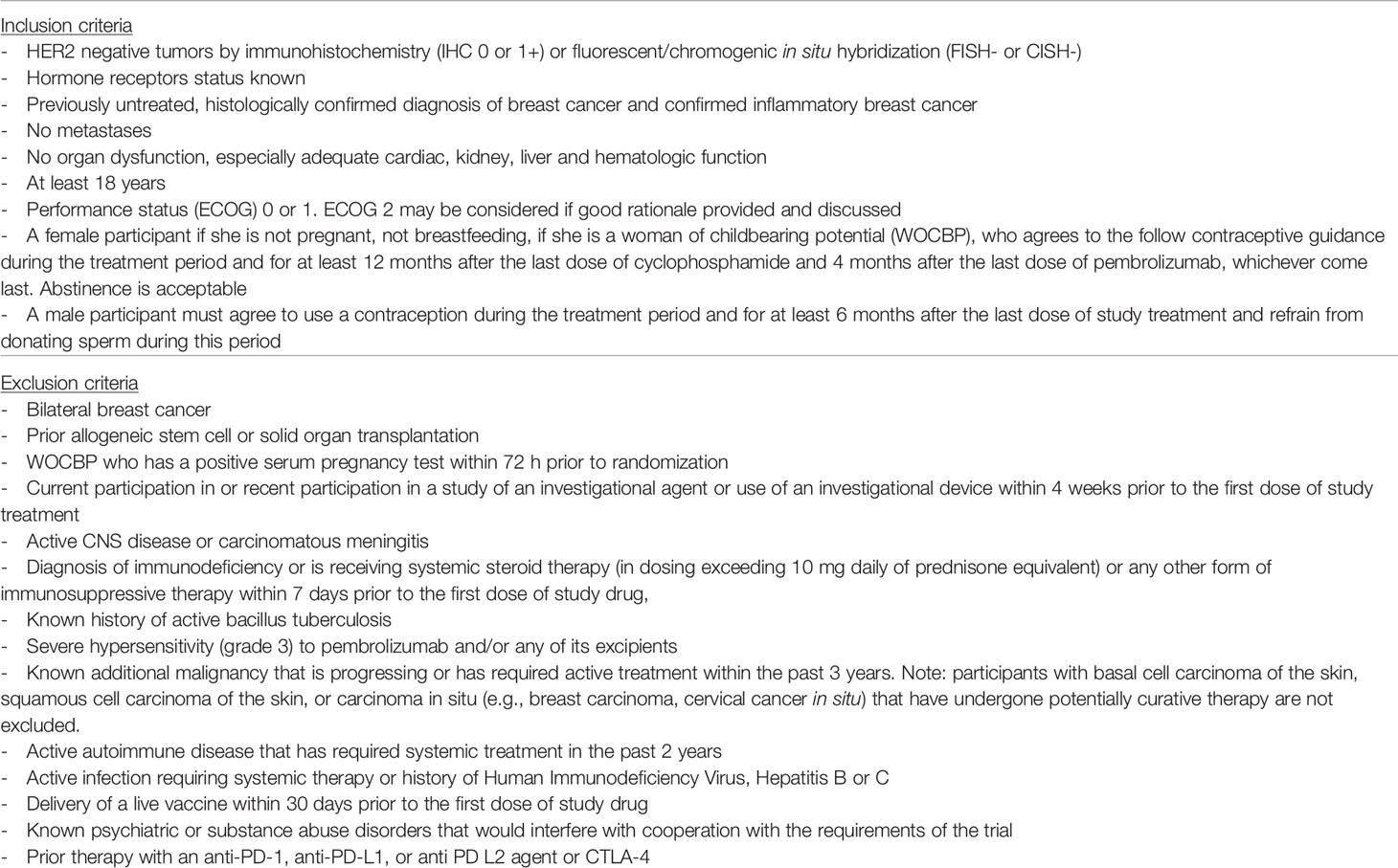
Table 1 Eligibility criteria of the PELICAN-IPC 2015-016/Oncodistinct-003 trial.
Study Procedures and Treatment
Patients are to be randomly assigned within 28 days from initiation of screening with a 2/1 ratio between NACT without (arm A) or with (arm B) pembrolizumab. The randomization procedure is assessed with block and is stratified by centers and hormone receptor status (positive HR is defined as tumor cell staining by immunohistochemistry ≥10% for ER and/or PR). To increase the randomness of the assignments, the permuted-block randomization schedule is generated within varying block sizes. A minimum and maximum number of patients of each phenotype (TN/non-TN) are respected in order to keep the adequate power.
In the experimental arm, pembrolizumab (intravenous administration at a dose of 200 mg every 3 weeks starting on cycle 2) is combined with conventional anthracycline/taxane-based NACT. Since anthracyclines have been shown to strongly induce immunogenic cell death, IFN gamma production and dendritic and T-cell tumor infiltration in mouse models (60, 61, 64, 66, 67), pembrolizumab is started on cycle 2, assuming that it should maximize potential sequential synergism. In addition, differing pembrolizumab initiation on cycle 2 should help evaluating the safety of the combination, by identifying patients with specific chemotherapy-induced toxicities. In the initial version of the protocol, the anthracyclines part of NACT was different according to the HR status: non-TN IBC (HR-positive and HER2-negative) patients were to receive 3-weekly 5-fluorouracil 500 mg/m², epirubicin 100 mg/m², cyclophosphamide 500 mg/m² (FEC100) from C1 to C4, whereas TN IBC (HR-negative and HER2-negative) were to receive epirubicin 90 mg/m² and cyclophosphamide 600 mg/m² every 2 weeks with G-CSF support, i.e., a dose dense (DD-EC) regimen from C1 to C4. A subsequent amendment homogenized the anthracycline-based schedule and all patients are now to receive DD-EC, whatever the HR status. Following anthracyclines sequence, all patients receive weekly paclitaxel for 12 injections (from C5 to C8). Details of design are shown in Figure 1.
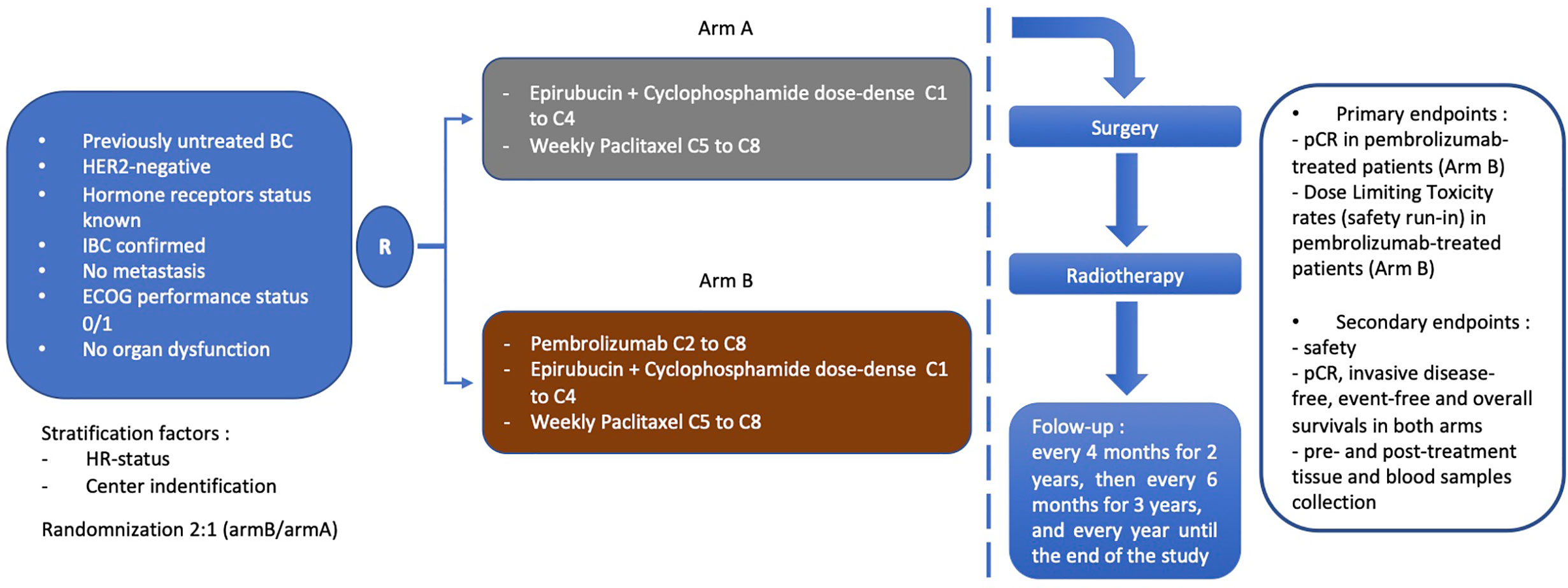
Figure 1 Design of PELICAN-IPC 2015-016/Oncodistinct-003 trial. BC, breast cancer; IBC, inflammatory breast cancer; HR, hormone receptor; pCR, pathological complete response.
Mastectomy with axillary lymph node dissection is to be performed within 4–6 weeks after the last chemotherapy administration. Pathological analysis is assessed by the local pathologist of each center and by a centralized reviewer. Radiotherapy starts 3 to 6 weeks after the surgery. Dose and frequency are left to investigator’s discretion and according to the site’s standard practice. Adjuvant endocrine therapy (if HR-positive disease) and/or capecitabine (if residual disease in TN IBC and no DPD enzyme deficit identified by plasma uracil dosage) is to be given after radiotherapy completion according to the site’s standard practice. After local treatment is completed, patients are followed every 4 months (+/- 28 days) for 2 years, then every 6 months for 3 years, and every year until the end of the study.
Outcomes
The primary endpoint is a central evaluation of pCR rate (as defined as ypT0/Tis, ypN0 following 8th AJCC classification) of the resected breast specimen and all sampled ipsilateral lymph nodes following NACT with/without pembrolizumab. A co-primary endpoint of safety is also included to determine if combining pembrolizumab and DD-EC exposes to significant toxicity. Thus, a run-in safety phase is to be conducted in order to stop the trial in case of unacceptable toxicity, as defined by the incidence of dose limiting toxicities (DLTs).
The secondary endpoints include the safety profile and tolerability of the combination, pCR rate by local assessment, invasive disease-free, event-free, and overall survivals (iDFS, EFS, and OS) in each arm. Since identification of predictive biomarkers for pembrolizumab efficacy is of critical importance, pharmacodynamics measurements and search for biological/immunological correlates are planned on pre- and post-treatment tissue and blood samples regularly collected before, during, and after treatment.
Statistics
The PELICAN trial is designed and powered to demonstrate that experimental group (arm B) achieves a pCR rate higher than a predefined undesirable rate of 20%. To reject the null hypothesis of a truly inefficient regimen (H0: p≤20%) at 5% error risk, following a Simon’s 2-stage optimal procedure, a total of 54 patients in arm B is necessary to obtain a power of 90% assuming a true pCR rate of 40%. Furthermore, to reach a power of 80% to reject the null hypothesis at 5% error risk in HR-negative (arm B), there must be at least 32 HR-negative patients and no more than 25 HR-positive patients to be recruited in arm B. A total of 27 patients are planned to be enrolled in the control arm (arm A), leading to a total of 81 patients planned. Predefined pCR of 20% was set-up according to several studies demonstrating a pCR rate between 20% and 28% in HER2-negative IBC receiving anthracyclines-taxanes NACT. The duration of enrolment is planned to 24 months. The randomized phase II design was selected to provide a control arm not directly compared to the experimental arm but allowing verifying the expected pCR rate with a conventional NACT in the selected population.
According to a 2-stage optimal design, an interim analysis is planned when 19 patients will be evaluable for the primary endpoint (pCR) in the experimental arm. At this interim evaluation, the study will stop for futility if no more than 4 patients have a documented pCR. If the patient accrual continues, the true pCR rate following NACT plus pembrolizumab will be estimated at the end of study with 90% confidence interval in all patients who received at least one dose of pembrolizumab. The overall hypothesis of a truly ineffective experimental arm will be accepted if the lower bound of the above estimated 90% bilateral confidence interval (CI) is inferior to 20%, or equivalently if no more than 15 patients out of a total of 54 evaluable patients have a documented pCR. In addition, the true pCR rate in patients enrolled in the HR-negative (TN IBC) strata will also be estimated. In this subgroup analysis, the true pCR rate will be estimated with 90% bilateral CI using an exact method for binomial proportions in one-stage clinical trials. The hypothesis of a truly ineffective experimental arm in this subgroup of interest will be accepted if the lower bound of the above estimated 90% exact bilateral CI is inferior to 20% and rejected otherwise.
According to standard practice in phase I studies, run-in phase conducted will enroll a maximum of 6 patients who completed 21 days after the first administration in two consecutive sub-cohorts (3+3). If at least 2 out of the 3 patients enrolled in the first sub-cohort report a DLT episode, the accrual of patients will be stopped, and the combination will be declared too toxic to warrant further investigation. If 1 or less than 1 patient (≤1 patient) reported a DLT in the first sub-cohort, 3 additional patients will be enrolled in the run-in phase. At the end, the combination will be declared sufficiently safe if less than 2 patients report a DLT out of the 6 evaluable patients enrolled in the run-in phase.
The incidence of reported adverse events during the treatment period will be summarized according to the treatment arm, by primary system organ class, CTCAE v5.0 severity grade, type of adverse event, and relationship to the study drug. Locally assessed pCR rate will be estimated with 90% exact confidence intervals. Time-to-event outcomes will be censored at the time of last follow-up visit. IDFS, EFS and OS will be estimated using the Kaplan-Meier method. Pointwise estimations for 3-year and 5-year IDFS, EFS, and OS will be provided with corresponding 90% asymptotic confidence interval.
Conclusion
To our knowledge, the PELICAN-IPC 2015-016/Oncodistinct-003 study (NCT03515798) is the first one to investigate the efficacy of ICI in patients with IBC, a rare but difficult-to-treat form of BC. Pembrolizumab is combined to chemotherapy in the neoadjuvant setting. Even if the recent most promising results remain modest in BC compared with more immunogenic cancers such as lung cancer or melanoma, they are significant notably in metastatic TNBC when combined to chemotherapy. Furthermore, IBC display few molecular characteristics that may suggest higher efficiency than in non-IBC: more frequent TN subtype, more frequent PD-L1-positivity and higher TMB independently from the molecular subtypes. Enrolment began in July 2018 and the estimated study completion date is 2022.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Protection des Personnes IIe de France VII (hôpital de Bicêtre, Le Kremlin Bicêtre, FRANCE). The participants or legal guardian provided written informed consent to participate in this study.
Author Contributions
AG was involved in the conceptualization of the manuscript. AB wrote the first draft of the manuscript. FB and AG revised the manuscript. AB was in charge of the tables and figure. All authors contributed to the article and approved the submitted version.
Funding
This study was designed and led by the study investigators. MSD France provides financial support and the supply of the study drug for the trial.
Conflict of Interest
AG reports travel expenses, accommodation, and meeting registration from Astra Zeneca, Pfizer, Roche, and Novartis.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank all patients who accepted to participate in this study and their family.
References
1. Chang S, Parker SL, Pham T, Buzdar AU, Hursting SD. Inflammatory breast carcinoma incidence and survival: the surveillance, epidemiology, and end results program of the National Cancer Institute, 1975-1992. Cancer (1998) 82:2366–72. doi: 10.1002/(SICI)1097-0142(19980615)82:12<2366::AID-CNCR10>3.0.CO;2-N
2. Dawood S, Merajver SD, Viens P, Vermeulen PB, Swain SM, Buchholz TA, et al. International expert panel on inflammatory breast cancer: consensus statement for standardized diagnosis and treatment. Ann Oncol (2011) 22:515–23. doi: 10.1093/annonc/mdq345
3. Cristofanilli M, Valero V, Buzdar AU, Kau S-W, Broglio KR, Gonzalez-Angulo AM, et al. Inflammatory breast cancer (IBC) and patterns of recurrence: understanding the biology of a unique disease. Cancer (2007) 110:1436–44. doi: 10.1002/cncr.22927
4. Anderson WF, Chu KC, Chang S. Inflammatory Breast Carcinoma and Noninflammatory Locally Advanced Breast Carcinoma: Distinct Clinicopathologic Entities? JCO (2003) 21:2254–9. doi: 10.1200/JCO.2003.07.082
5. Hance KW, Anderson WF, Devesa SS, Young HA, Levine PH. Trends in Inflammatory Breast Carcinoma Incidence and Survival: The Surveillance, Epidemiology, and End Results Program at the National Cancer Institute. JNCI: J Natl Cancer Institute (2005) 97:966–75. doi: 10.1093/jnci/dji172
6. van Uden DJP, Bretveld R, Siesling S, de Wilt JHW, Blanken-Peeters CFJM. Inflammatory breast cancer in the Netherlands; improved survival over the last decades. Breast Cancer Res Treat (2017) 162:365–74. doi: 10.1007/s10549-017-4119-6
7. Dawood S, Ueno NT, Valero V, Woodward WA, Buchholz TA, Hortobagyi GN, et al. Differences in survival among women with stage III inflammatory and noninflammatory locally advanced breast cancer appear early: A large population-based study. Cancer (2011) 117:1819–26. doi: 10.1002/cncr.25682
8. Charafe-Jauffret E, Tarpin C, Bardou V-J, Bertucci F, Ginestier C, Braud A-C, et al. Immunophenotypic analysis of inflammatory breast cancers: identification of an’inflammatory signature.’. J Pathol (2004) 202:265–73. doi: 10.1002/path.1515
9. Ben Hamida A, Labidi IS, Mrad K, Charafe-Jauffret E, Ben Arab S, Esterni B, et al. Markers of subtypes in inflammatory breast cancer studied by immunohistochemistry: Prominent expression of P-cadherin. BMC Cancer (2008) 8:28. doi: 10.1186/1471-2407-8-28
10. Bieche I. Molecular Profiling of Inflammatory Breast Cancer: Identification of a Poor-Prognosis Gene Expression Signature. Clin Cancer Res (2004) 10:6789–95. doi: 10.1158/1078-0432.CCR-04-0306
11. McCarthy NJ, Yang X, Linnoila IR, Merino MJ, Hewitt SM, Parr AL, et al. Microvessel density, expression of estrogen receptor alpha, MIB-1, p53, and c-erbB-2 in inflammatory breast cancer. Clin Cancer Res (2002) 8:3857–62.
12. Colpaert CG, Vermeulen PB, Benoy I, Soubry A, van Roy F, van Beest P, et al. Inflammatory breast cancer shows angiogenesis with high endothelial proliferation rate and strong E-cadherin expression. Br J Cancer (2003) 88:718–25. doi: 10.1038/sj.bjc.6600807
13. Bonnier P, Charpin C, Lejeune C, Romain S, Tubiana N, Beedassy B, et al. Inflammatory carcinomas of the breast: A clinical, pathological, or a clinical and pathological definition? Int J Cancer (1995) 62:382–5. doi: 10.1002/ijc.2910620404
14. Amparo RS, Angel CDM, Ana LH, Antonio LC, Vicente MS, Carlos F-M, et al. Inflammatory Breast Carcinoma: Pathological or Clinical Entity? Breast Cancer Res Treat (2000) 64:269–73. doi: 10.1023/A:1026512722789
15. Bertucci F, Finetti P, Vermeulen P, Van Dam P, Dirix L, Birnbaum D, et al. Genomic profiling of inflammatory breast cancer: a review. Breast (2014) 23:538–45. doi: 10.1016/j.breast.2014.06.008
16. Van Laere SJ, Ueno NT, Finetti P, Vermeulen P, Lucci A, Robertson FM, et al. Uncovering the molecular secrets of inflammatory breast cancer biology: an integrated analysis of three distinct affymetrix gene expression datasets. Clin Cancer Res (2013) 19:4685–96. doi: 10.1158/1078-0432.CCR-12-2549
17. Rybczynska AA, Boersma HH, de Jong S, Gietema JA, Noordzij W, Dierckx RAJO, et al. Avenues to molecular imaging of dying cells: Focus on cancer. Med Res Rev (2018) 38:1713–68. doi: 10.1002/med.21495
18. Viens P, Tarpin C, Roche H, Bertucci F. Systemic therapy of inflammatory breast cancer from high-dose chemotherapy to targeted therapies: the French experience. Cancer (2010) 116:2829–36. doi: 10.1002/cncr.25168
19. Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, Tjulandin S, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet (2010) 375:377–84. doi: 10.1016/S0140-6736(09)61964-4
20. Gianni L, Pienkowski T, Im Y-H, Roman L, Tseng L-M, Liu M-C, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol (2012) 13:25–32. doi: 10.1016/S1470-2045(11)70336-9
21. Chan A, Delaloge S, Holmes FA, Moy B, Iwata H, Harvey VJ, et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol (2016) 17:367–77. doi: 10.1016/S1470-2045(15)00551-3
22. von Minckwitz G, Huang C-S, Mano MS, Loibl S, Mamounas EP, Untch M, et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N Engl J Med (2019) 380:617–28. doi: 10.1056/NEJMoa1814017
23. Pierga J-Y, Petit T, Delozier T, Ferrero J-M, Campone M, Gligorov J, et al. Neoadjuvant bevacizumab, trastuzumab, and chemotherapy for primary inflammatory HER2-positive breast cancer (BEVERLY-2): an open-label, single-arm phase 2 study. Lancet Oncol (2012) 13:375–84. doi: 10.1016/S1470-2045(12)70049-9
24. Bertucci F, Fekih M, Autret A, Petit T, Dalenc F, Levy C, et al. Bevacizumab plus neoadjuvant chemotherapy in patients with HER2-negative inflammatory breast cancer (BEVERLY-1): a multicentre, single-arm, phase 2 study. Lancet Oncol (2016) 17:600–11. doi: 10.1016/S1470-2045(16)00011-5
25. Matsuda N, Wang X, Lim B, Krishnamurthy S, Alvarez RH, Willey JS, et al. Safety and Efficacy of Panitumumab Plus Neoadjuvant Chemotherapy in Patients With Primary HER2-Negative Inflammatory Breast Cancer. JAMA Oncol (2018) 4:1207–13. doi: 10.1001/jamaoncol.2018.1436
26. Denkert C, Loibl S, Noske A, Roller M, Müller BM, Komor M, et al. Tumor-Associated Lymphocytes As an Independent Predictor of Response to Neoadjuvant Chemotherapy in Breast Cancer. J Clin Oncol (2010) 28:105–13. doi: 10.1200/JCO.2009.23.7370
27. Loi S, Michiels S, Salgado R, Sirtaine N, Jose V, Fumagalli D, et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: results from the FinHER trial. Ann Oncol (2014) 25:1544–50. doi: 10.1093/annonc/mdu112
28. Ali HR, Provenzano E, Dawson S-J, Blows FM, Liu B, Shah M, et al. Association between CD8+ T-cell infiltration and breast cancer survival in 12 439 patients. Ann Oncol (2014) 25:1536–43. doi: 10.1093/annonc/mdu191
29. Rody A, Holtrich U, Pusztai L, Liedtke C, Gaetje R, Ruckhaeberle E, et al. T-cell metagene predicts a favorable prognosis in estrogen receptor-negative and HER2-positive breast cancers. Breast Cancer Res (2009) 11:R15. doi: 10.1186/bcr2234
30. Teschendorff AE, Miremadi A, Pinder SE, Ellis IO, Caldas C. An immune response gene expression module identifies a good prognosis subtype in estrogen receptor negative breast cancer. Genome Biol (2007) 8:R157. doi: 10.1186/gb-2007-8-8-r157
31. Sabatier R, Finetti P, Mamessier E, Raynaud S, Cervera N, Lambaudie E, et al. Kinome expression profiling and prognosis of basal breast cancers. Mol Cancer (2011) 10:86. doi: 10.1186/1476-4598-10-86
32. Sabatier R, Finetti P, Cervera N, Lambaudie E, Esterni B, Mamessier E, et al. A gene expression signature identifies two prognostic subgroups of basal breast cancer. Breast Cancer Res Treat (2011) 126:407–20. doi: 10.1007/s10549-010-0897-9
33. Demaria S, Volm MD, Shapiro RL, Yee HT, Oratz R, Formenti SC, et al. Development of tumor-infiltrating lymphocytes in breast cancer after neoadjuvant paclitaxel chemotherapy. Clin Cancer Res (2001) 7:3025–30.
34. Ladoire S, Mignot G, Dabakuyo S, Arnould L, Apetoh L, Rébé C, et al. In situ immune response after neoadjuvant chemotherapy for breast cancer predicts survival. J Pathol (2011) 224:389–400. doi: 10.1002/path.2866
35. Ahmadzadeh M, Johnson LA, Heemskerk B, Wunderlich JR, Dudley ME, White DE, et al. Tumor antigen–specific CD8 T cells infiltrating the tumor express high levels of PD-1 and are functionally impaired. Blood (2009) 114:1537–44. doi: 10.1182/blood-2008-12-195792
36. Dong H, Strome SE, Salomao DR, Tamura H, Hirano F, Flies DB, et al. Tumor-associated B7-H1 promotes T-cell apoptosis: A potential mechanism of immune evasion. Nat Med (2002) 8:793–800. doi: 10.1038/nm730
37. Francisco LM, Salinas VH, Brown KE, Vanguri VK, Freeman GJ, Kuchroo VK, et al. PD-L1 regulates the development, maintenance, and function of induced regulatory T cells. J Exp Med (2009) 206:3015–29. doi: 10.1084/jem.20090847
38. Hamel KM, Cao Y, Wang Y, Rodeghero R, Kobezda T, Chen L, et al. B7-H1 expression on non-B and non-T cells promotes distinct effects on T- and B-cell responses in autoimmune arthritis. Eur J Immunol (2010) 40:3117–27. doi: 10.1002/eji.201040690
39. Zou W, Chen L. Inhibitory B7-family molecules in the tumour microenvironment. Nat Rev Immunol (2008) 8:467–77. doi: 10.1038/nri2326
40. Iwai Y, Ishida M, Tanaka Y, Okazaki T, Honjo T, Minato N. Involvement of PD-L1 on tumor cells in the escape from host immune system and tumor immunotherapy by PD-L1 blockade. Proc Natl Acad Sci (2002) 99:12293–7. doi: 10.1073/pnas.192461099
41. Reiss KA, Forde PM, Brahmer JR. Harnessing the power of the immune system via blockade of PD-1 and PD-L1: a promising new anticancer strategy. Immunotherapy (2014) 6:459–75. doi: 10.2217/imt.14.9
42. Ghebeh H, Mohammed S, Al-Omair A, Qattant A, Lehe C, Al-Qudaihi G, et al. The B7-H1 (PD-L1) T Lymphocyte-Inhibitory Molecule Is Expressed in Breast Cancer Patients with Infiltrating Ductal Carcinoma: Correlation with Important High-Risk Prognostic Factors. Neoplasia (2006) 8:190–8. doi: 10.1593/neo.05733
43. Ghebeh H, Tulbah A, Mohammed S, ElKum N, Amer SMB, Al-Tweigeri T, et al. Expression of B7-H1 in breast cancer patients is strongly associated with high proliferative Ki-67-expressing tumor cells. Int J Cancer (2007) 121:751–8. doi: 10.1002/ijc.22703
44. Ghebeh H, Barhoush E, Tulbah A, Elkum N, Al-Tweigeri T, Dermime S. FOXP3+ Tregs and B7-H1+/PD-1+T lymphocytes co-infiltrate the tumor tissues of high-risk breast cancer patients: Implication for immunotherapy. BMC Cancer (2008) 8:57. doi: 10.1186/1471-2407-8-57
45. Schalper KA, Velcheti V, Carvajal D, Wimberly H, Brown J, Pusztai L, et al. In Situ Tumor PD-L1 mRNA Expression Is Associated with Increased TILs and Better Outcome in Breast Carcinomas. Clin Cancer Res (2014) 20:2773–82. doi: 10.1158/1078-0432.CCR-13-2702
46. Soliman H, Khalil F, Antonia S. PD-L1 Expression Is Increased in a Subset of Basal Type Breast Cancer Cells. PloS One (2014) 9:e88557. doi: 10.1371/journal.pone.0088557
47. Mittendorf EA, Philips AV, Meric-Bernstam F, Qiao N, Wu Y, Harrington S, et al. PD-L1 Expression in Triple-Negative Breast Cancer. Cancer Immunol Res (2014) 2:361–70. doi: 10.1158/2326-6066.CIR-13-0127
48. Sabatier R, Finetti P, Mamessier E, Adelaide J, Chaffanet M, Ali HR, et al. Prognostic and predictive value of PDL1 expression in breast cancer. Oncotarget (2015) 6:5449–64. doi: 10.18632/oncotarget.3216
49. Wimberly H, Brown JR, Schalper K, Haack H, Silver MR, Nixon C, et al. PD-L1 Expression Correlates with Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy in Breast Cancer. Cancer Immunol Res (2015) 3:326–32. doi: 10.1158/2326-6066.CIR-14-0133
50. Bertucci F, Ueno NT, Finetti P, Vermeulen P, Lucci A, Robertson FM, et al. Gene expression profiles of inflammatory breast cancer: correlation with response to neoadjuvant chemotherapy and metastasis-free survival. Ann Oncol (2014) 25:358–65. doi: 10.1093/annonc/mdt496
51. Bertucci F, Finetti P, Colpaert C, Mamessier E, Parizel M, Dirix L, et al. PDL1 expression in inflammatory breast cancer is frequent and predicts for the pathological response to chemotherapy. Oncotarget (2015) 6:13506–19. doi: 10.18632/oncotarget.3642
52. Arias-Pulido H, Cimino-Mathews A, Chaher N, Qualls C, Joste N, Colpaert C, et al. The combined presence of CD20 + B cells and PD-L1 + tumor-infiltrating lymphocytes in inflammatory breast cancer is prognostic of improved patient outcome. Breast Cancer Res Treat (2018) 171:273–82. doi: 10.1007/s10549-018-4834-7
53. Van Berckelaer C, Rypens C, van Dam P, Pouillon L, Parizel M, Schats KA, et al. Infiltrating stromal immune cells in inflammatory breast cancer are associated with an improved outcome and increased PD-L1 expression. Breast Cancer Res (2019) 21:28. doi: 10.1186/s13058-019-1108-1
54. Liang X, Vacher S, Boulai A, Bernard V, Baulande S, Bohec M, et al. Targeted next-generation sequencing identifies clinically relevant somatic mutations in a large cohort of inflammatory breast cancer. Breast Cancer Res (2018) 20:88. doi: 10.1186/s13058-018-1007-x
55. Bertucci F, Rypens C, Finetti P, Guille A, Adélaïde J, Monneur A, et al. NOTCH and DNA repair pathways are more frequently targeted by genomic alterations in inflammatory than in non-inflammatory breast cancers. Mol Oncol (2019) 13(3): 504–19. doi: 10.1002/1878-0261.12621
56. Planes-Laine G, Rochigneux P, Bertucci F, Chrétien A-S, Viens P, Sabatier R, et al. PD-1/PD-L1 Targeting in Breast Cancer: The First Clinical Evidences Are Emerging. A Literature Review. Cancers (2019) 11:1033. doi: 10.3390/cancers11071033
57. Cortés J, Lipatov O, Im S-A, Gonçalves A, Lee KS, Schmid P, et al. KEYNOTE-119: Phase III study of pembrolizumab (pembro) versus single-agent chemotherapy (chemo) for metastatic triple negative breast cancer (mTNBC). Ann Oncol (2019) 30:v859–60. doi: 10.1093/annonc/mdz394.010
58. Zitvogel L, Apetoh L, Ghiringhelli F, André F, Tesniere A, Kroemer G. The anticancer immune response: indispensable for therapeutic success? J Clin Invest (2008) 118:1991–2001. doi: 10.1172/JCI35180
59. Emens LA, Middleton G. The Interplay of Immunotherapy and Chemotherapy: Harnessing Potential Synergies. Cancer Immunol Res (2015) 3:436–43. doi: 10.1158/2326-6066.CIR-15-0064
60. Mattarollo SR, Loi S, Duret H, Ma Y, Zitvogel L, Smyth MJ. Pivotal Role of Innate and Adaptive Immunity in Anthracycline Chemotherapy of Established Tumors. Cancer Res (2011) 71:4809–20. doi: 10.1158/0008-5472.CAN-11-0753
61. Zhu S, Waguespack M, Barker SA, Li S. Doxorubicin Directs the Accumulation of Interleukin-12 Induced IFN into Tumors for Enhancing STAT1 Dependent Antitumor Effect. Clin Cancer Res (2007) 13:4252–60. doi: 10.1158/1078-0432.CCR-06-2894
62. Ma Y, Aymeric L, Locher C, Mattarollo SR, Delahaye NF, Pereira P, et al. Contribution of IL-17–producing γδ T cells to the efficacy of anticancer chemotherapy. J Exp Med (2011) 208:491–503. doi: 10.1084/jem.20100269
63. Ma Y, Adjemian S, Mattarollo SR, Yamazaki T, Aymeric L, Yang H, et al. Anticancer Chemotherapy-Induced Intratumoral Recruitment and Differentiation of Antigen-Presenting Cells. Immunity (2013) 38:729–41. doi: 10.1016/j.immuni.2013.03.003
64. Apetoh L, Mignot G, Panaretakis T, Kroemer G, Zitvogel L. Immunogenicity of anthracyclines: moving towards more personalized medicine. Trends Mol Med (2008) 14:141–51. doi: 10.1016/j.molmed.2008.02.002
65. Galluzzi L, Senovilla L, Zitvogel L, Kroemer G. The secret ally: immunostimulation by anticancer drugs. Nat Rev Drug Discovery (2012) 11:215–33. doi: 10.1038/nrd3626
66. Black M, Barsoum IB, Truesdell P, Cotechini T, Macdonald-Goodfellow SK, Petroff M, et al. Activation of the PD-1/PD-L1 immune checkpoint confers tumor cell chemoresistance associated with increased metastasis. Oncotarget (2016) 7:10557–67. doi: 10.18632/oncotarget.7235
67. Rios-Doria J, Durham N, Wetzel L, Rothstein R, Chesebrough J, Holoweckyj N, et al. Doxil Synergizes with Cancer Immunotherapies to Enhance Antitumor Responses in Syngeneic Mouse Models. Neoplasia (2015) 17:661–70. doi: 10.1016/j.neo.2015.08.004
68. Schmid P, Chui SY, Emens LA. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. Reply. N Engl J Med (2019) 380:987–8. doi: 10.1056/NEJMc1900150
69. Cortes J, Cescon DW, Rugo HS, Nowecki Z, Im S-A, Yusof MM, et al. KEYNOTE-355: Randomized, double-blind, phase III study of pembrolizumab + chemotherapy versus placebo + chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer. JCO (2020) 38:1000–0. doi: 10.1200/JCO.2020.38.15_suppl.1000
70. Miles DW, Gligorov J, André F, Cameron D, Schneeweiss A, Barrios CH, et al. LBA15 Primary results from IMpassion131, a double-blind placebo-controlled randomised phase III trial of first-line paclitaxel (PAC) ± atezolizumab (atezo) for unresectable locally advanced/metastatic triple-negative breast cancer (mTNBC). Ann Oncol (2020) 31:S1147–8. doi: 10.1016/j.annonc.2020.08.2243
71. Cortés J, André F, Gonçalves A, Kümmel S, Martín M, Schmid P, et al. IMpassion132 Phase III trial: atezolizumab and chemotherapy in early relapsing metastatic triple-negative breast cancer. Future Oncol (London England) (2019) 15:1951–61. doi: 10.2217/fon-2019-0059
72. Nanda R, Liu MC, Yau C, Shatsky R, Pusztai L, Wallace A, et al. Effect of Pembrolizumab Plus Neoadjuvant Chemotherapy on Pathologic Complete Response in Women With Early-Stage Breast Cancer: An Analysis of the Ongoing Phase 2 Adaptively Randomized I-SPY2 Trial. JAMA Oncol (2020) 15:1951–61. doi: 10.1001/jamaoncol.2019.6650
73. Schmid P, Cortes J, Pusztai L, McArthur H, Kümmel S, Bergh J, et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N Engl J Med (2020) 382:810–21. doi: 10.1056/NEJMoa1910549
74. Harbeck N, Zhang H, Barrios CH, Saji S, Jung KH, Hegg R, et al. LBA11 IMpassion031: Results from a phase III study of neoadjuvant (neoadj) atezolizumab + chemotherapy in early triple-negative breast cancer (TNBC). Ann Oncol (2020) 31:S1144. doi: 10.1016/j.annonc.2020.08.2239
75. Loibl S, Untch M, Burchardi N, Huober J, Sinn BV, Blohmer J-U, et al. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol (2019) 30:1279–88. doi: 10.1093/annonc/mdz158
76. Gianni L, Huang C-S, Egle D, Bermejo B, Zamagni C, Thill M, et al. Abstract GS3-04: Pathologic complete response (pCR) to neoadjuvant treatment with or without atezolizumab in triple negative, early high-risk and locally advanced breast cancer. NeoTRIPaPDL1 Michelangelo randomized study. In: General Session Abstracts. San Antonio breast cancer symposium: American Association for Cancer Research (2020). p. GS3–04-GS3-04. doi: 10.1158/1538-7445.SABCS19-GS3-04
Keywords: immune checkpoint inhibitor, inflammatory breast cancer, neoadjuvant therapy, PDL1, pembrolizumab
Citation: Bertucci A, Bertucci F, Zemmour C, Lerebours F, Pierga J-Y, Levy C, Dalenc F, Grenier J, Petit T, Berline M and Gonçalves A (2020) PELICAN-IPC 2015-016/Oncodistinct-003: A Prospective, Multicenter, Open-Label, Randomized, Non-Comparative, Phase II Study of Pembrolizumab in Combination With Neo Adjuvant EC-Paclitaxel Regimen in HER2-Negative Inflammatory Breast Cancer. Front. Oncol. 10:575978. doi: 10.3389/fonc.2020.575978
Received: 24 June 2020; Accepted: 28 October 2020;
Published: 25 November 2020.
Edited by:
Cesar Augusto Santa-Maria, Johns Hopkins Medicine, United StatesReviewed by:
Russell B. McBride, Icahn School of Medicine at Mount Sinai, United StatesSangeetha Reddy, University of Texas Southwestern Medical Center, United States
Copyright © 2020 Bertucci, Bertucci, Zemmour, Lerebours, Pierga, Levy, Dalenc, Grenier, Petit, Berline and Gonçalves. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anthony Gonçalves, Z29uY2FsdmVzYUBpcGMudW5pY2FuY2VyLmZy