
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 18 February 2020
Sec. Radiation Oncology
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.00135
 Paul Lesueur1,2,3,4*
Paul Lesueur1,2,3,4* Etienne Rapeaud1,2,3Ludovic De Marzi1Farid Goudjil1Christine Levy5Olivier Galatoire6Pierre Vincent Jacomet6Rémi Dendale1,2
Etienne Rapeaud1,2,3Ludovic De Marzi1Farid Goudjil1Christine Levy5Olivier Galatoire6Pierre Vincent Jacomet6Rémi Dendale1,2 Valentin Calugaru1,2
Valentin Calugaru1,2Introduction: Lacrymal cystic adenoid carcinoma is a rare disease for which optimal treatment is still debated. In fact, despite aggressive treatment such as eye sparing surgery or orbital exenteration, following by adjuvant radiotherapy, local recurrence and distant metastatic disease are common. This study aims to describe outcomes of eye surgery associated with high dose exclusive adjuvant proton beam irradiation.
Materials and Methods: This is a monocentric institutional retrospective study. We retrospectively reviewed records of patients treated in our institution since 2008 with high dose adjuvant proton irradiation for a lacrymal cystic adenoid carcinoma up to a maximum of 75.6Gy(RBE). Other histologies or patients treated with a mix of photon-proton were excluded. A total of 15 patients were finally included.
Results: Fifteen patients (80% women, 100% Performance status 0–1) with locally advanced disease (33% T3–T4, 47% R1–R2) were included. After a median follow-up of 67.4 months [13.4–122] the 3 years Overall Survival, local Progression free survival, and progression free survival rates were 78, 70, and 58%, respectively. Six patients exhibited a local recurrence. All patients with conservative surgery maintained their base-line visual acuity and visual field at last follow up. Four patients developed brain radionecrosis.
Conclusion: This is the largest series of patients with ACC treated with high dose adjuvant proton therapy. Proton therapy is a safe and efficient treatment and should be considered as an adjuvant irradiation modality to privilege, for patients with lacrimal ACC after conservative or radical eyeball surgery. Dose delivered to temporal lobe should be limited to avoid brain radionecrosis.
Adenoid cystic carcinoma (ACC) is a malignancy of secretory glands, including salivary glands and more rarely the lacrimal glands. Adenoid cystic carcinoma is the most common malignant epithelial neoplasm of the lacrimal gland (66% of cases) (1). The prognosis of lacrimal variant is classically poorer with a 3.5 folds higher mortality in comparison with the others glands subtypes. Despite aggressive treatment such as eye sparing surgery or orbital exenteration, following by adjuvant radiotherapy, local recurrence and distant metastatic disease are common. Indeed, according to a Surveillance, Epidemiology, and End Results Program (SEER) analysis the median overall survival (OS) was 7.6 years for ACC (2). The substantial morbidity and mortality of lacrymal ACC seems to be due to early perineural invasion and spread along major nerves, as well as along periosteal planes.
Given the scarcity of this tumor, the lack of prospective studies analyzing its treatment, and the limited and mixed results of retrospective studies, the appropriate therapy for local control is under debate.
Similarly as for head and neck ACC, the “gold-standard” treatment consists in radical surgery followed by post-operative radiotherapy (3). The use of adjuvant or concomittant systemic therapy is debated (4). In fact, ACC, whatever the gland involved, is classically considered as a radioresistant tumor, and dose escalation is essential to hope for a curative irradiation. ACC of the lacrimal gland is one of the best clinical presentation to exploit the benefits of proton irradiation, given the highly irregular target volume shape and the need for high dose in the presence of surrounded critical structures.
Previous reports on the effects of proton beam radiation (PBR) on lacrimal gland carcinoma are available but present several limits (5–7): heterogeneous histologic types are included in the same study, patients are treated with a mix of photon/proton irradiation, or ACC subgroup is often a small sample of the cohort. A recent retrospective study reported higher survival and lower recurrence rate, by using modern high dose proton-photon adjuvant irradiation in comparison with historical series, thus, supporting a rationale for high dose proton irradiation (5). In this published study 17 of the 18 included patients received a large dose of PBR (range 52.5 to 60CGE), as well as a smaller dose of photon radiation (range 12 to 23.4 CGE), administered by a linear accelerator (LINAC), for a total radiation dose of 71–76 CGE. The use of a small dose of photontherapy was argue on the fact that photons are more skin-sparing and thus reduces the skin toxicity associated with proton therapy. Photons can also improve the dose conformality.
By reporting the largest retrospective study of patients with lacrymal ACC treated by surgery and high dose post-operative exclusive proton beam irradiation, we aim to show that, in this indication, exclusive high dose proton irradiation is feasible.
We screened all patients with lacrymal ACC, treated with proton therapy from 2008 to march 2018, at Institut Curie Proton Therapy Center in Orsay (ICPO). Patients were retrospectively included according to the following inclusion criteria. Patients should have received an adjuvant or exclusive proton irradiation for a localized lacrymal ACC. Metastatic patients at the time of diagnosis were excluded. Diagnosis had to be confirmed by pathologic analysis, with biopsy from the primitive site, or from tumor resection. All patients older than 18 years could be included. Patients with poor performance status (PS), superior to 2, at diagnosis were not included. Tumor staging was based upon clinical information available in the medical records, and is reported according to the pathologic TNM staging of lacrimal gland carcinoma, AJCC 7th edition staging criteria. Patient, tumor, and treatment characteristics were extracted from the medical charts. The treatment of each patient was discussed by a multidisciplinary team.
Patients were clinically examined every week during the treatment to assess the radiation induced acute toxicity. After irradiation, every 6 months patients were reviewed by their radiation oncologist, and benefited from a full paraclinical examination. At each medical consultation a gadolinium-enhanced MRI and a thoraco-abdominal CT scan were performed. A blood sample looking for a pituitary axis dysfunction was also collected. Every 6 months an ophthalmological visit was scheduled with an evaluation of visual acuity and visual field. The Common Terminology Criteria for Adverse Events, Version 4.0 (CTCAE v4.0) has been used to assess the early and late toxicities. Follow up duration was calculated from the start of proton irradiation to the last clinical visit. The primary outcome was local progression-free survival (LPFS: Patient alive without in-field local recurrence).
The irradiation was performed for all the patients with 201 MeV protons (cyclotron C230 IBA - 230 MeV). The double scattering technique (DS) was the first technique used for this series of patients, then, patients treated more recently received pencil beam scanning (PBS) irradiation.
Patients were positioned supine on the couch and immobilized with a commercial thermoformable mask fixation system. All the patients benefited from a CT scan and a gadolinium-enhanced cerebral MRI, both with 1 mm slice thickness, for registration. The dose limiting structures were the optic nerve, chiasm, ocular globe, retina, brainstem, and temporal lobe. The target volume systematically included the post-surgical residual tumor and tumor bed as well as the sites of possible spread along the optic nerve-path. Three recurrence risk level target volumes were defined: a high, an intermediate and a low risk level. We apply a relative biological effectiveness (RBE) factor of 1.1 to all our prescriptions. In case of only biopsied patients or R2 resection, the high risk CTV 73.8Gy (RBE) (HR-CTV) corresponded to the gross tumor volume with a 3 mm margin, excluding the optic nerve and the ocular globe. In case of R0 or R1 resection, thus the HR-CTV was defined as the operative bed plus 3mm excluding the optic nerve and the ocular globe. The intermediate risk CTV 63Gy(RBE) (IR-CTV) included the ipsilateral half of the orbit, the external wall of orbit and the optic canal while the low risk CTV 54Gy(RBE) (LR-CTV) should encompass the homolateral cavernous sinus (Figure 1). Prophylactic irradiation of cervical lymph node was not proposed. Additional isotropic margins of 1, 2, and 3 mm were added to these volumes to, respectively, define the HR-PTV, the IR-PTV and the LR-PTV. The dose per fraction was 1.8Gy(RBE). For the treatment plans, an anterior oblique ipsilateral field and two superior oblique ipsilateral fields were generally used. For the reduction, the size of the superior oblique fields has been adapted to the different volumes. The dose constraints to the critical organs are summarized in Supplementary Table 1. Coverage of 95% of the target volume by 95% of the prescribed dose was expected.

Figure 1. Delineation of HR, IR and LR clinical target volumes.
Patient's characteristics were described by mean and standard deviation or by median and range for continuous variables and by frequencies for categorical variables. LPFS was defined as the time from the first day of irradiation to the appearance of in-field local failure. Progression-free survival (PFS) and overall survival (OS) were defined as the time from the first day of irradiation treatment to the appearance of recurrence (in field or out-filed) and the death from any cause, respectively. For LPFS, patients not having any evidence of local failure on MRI were censored at last MRI. For PFS and OS, data were censored at the date of death or at the last available clinical encounter. Survival probability was estimated using the Kaplan-Meier method. Univariate analysis using Cox models (for continuous variable) and log-rank tests (for categorical variable) were performed to evaluate the effects of various variables on outcomes. Multivariable assessment was not performed considering the sample size.
This study was approved by French Ethics Committees and the National Commission on informatics and Liberties (MR003 Methodology). An information letter was sent to patients still alive at time of data collection. This study adhered to the Declaration of Helsinki.
Between January 2008 and December 2017, 15 patients received a proton irradiation for a lacrymal cystic adenoid carcinoma. All patients were treated at the at Institut Curie Proton Therapy Center in Orsay (ICPO). Twelve patients were women (80%). The median age at diagnosis was 43 years [min-max 23–68]. All patients had a performance status equal to 0 or 1. Two thirds of patients had a localized disease (T2N0M0) while the last third had an advanced local disease (T4 or T3N0M0). Sixty percent of the patients received adjuvant proton therapy after tumorectomy with ocular retention, while for the remaining patients had undergone a proton therapy after an exenteration. Most of patients benefited from a R0 surgery (n = 8) while for 7 patients it was reported an incomplete surgery (4 R1 with microscopic involvement margins and 3 R2 with macroscopic residual disease) Patient characteristics are described in Table 1.
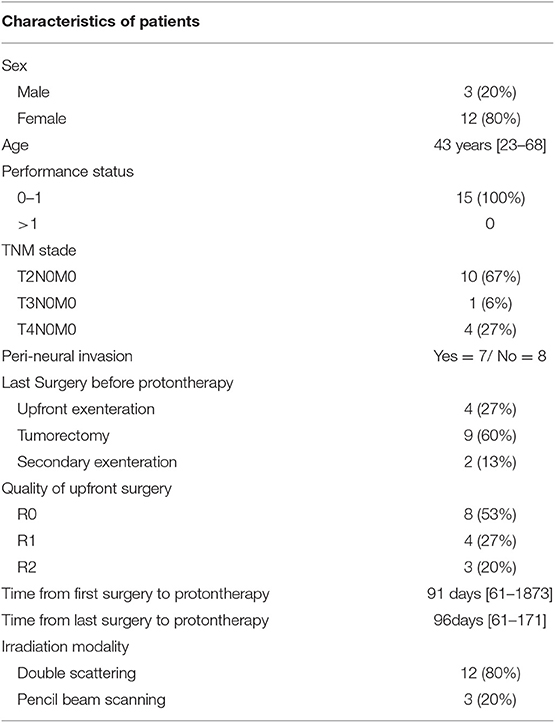
Table 1. Characteristics of patients included in the study at baseline.
Most of patients (n = 12) were treated with a double scattering technical (DS), with 3 dose levels as described above and five beams, reduction fields included (median n = 5 [4–6]). The high risk area received a median dose of 73.8Gy(RBE) [64–75.6] in 41 fractions of 1.8Gy(RBE). Patients started irradiation 3 months after the last surgery (96days [61–171]). The median proton-therapy duration was 60 days [46–67].
The median follow-up was 67.4 months [13.4–122]. Local progression free survival was 96.1 months [IC95 31.9- NR]. The progression free survival was 57.7 months [IC95 22.5- NR]. Overall survival median was not reached (Figure 2, Table 2).
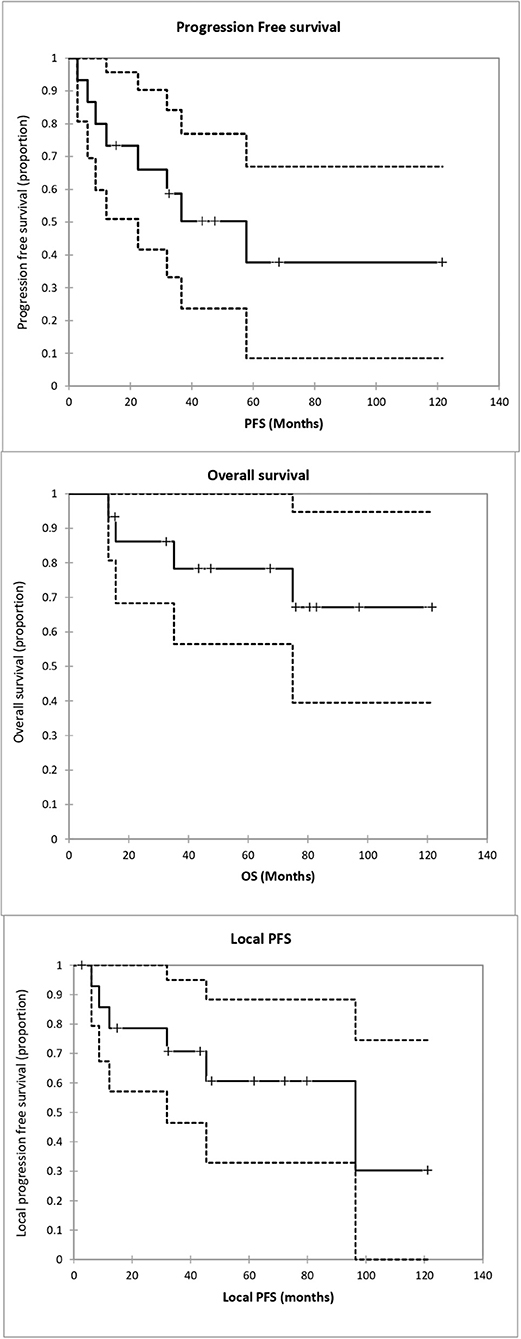
Figure 2. Progression free survival (PFS), Overall Survival (OS) and local progression free survival since irradiation start.

Table 2. Overall and progression free survival rates at 1, 2, 3 and 5 years.
On univariate analysis, none of the tested factors (sex, age, TNM stage, quality of upfront surgery, volume of high risk CTV, Time From last surgery to irradiation) were predicted of local PFS, PFS, or OS. Only D95% of HR-PTV was predictive of a better overall survival (p = 0.05), and showed a trend to a better PFS (p = 0.08) (Table 3).

Table 3. Prognostic factor (univariate analysis).
Eight patients exhibited a recurrence. Two of them presented a single local relapse, two others patients showed a metastatic relapse, while 4 exhibited both. About local recurrences, 3 intra orbitary relapses were described. All were inside the low risk irradiated volume. Two local recurrences were out of field: inside the infra temporal area for the first one, and along the surgical approach (meningeal fronto-coronal aperture). No patients exhibit recurrences inside the intermediate or high risk irradiated volume. Two patients, treated at first line with adjuvant protontherapy, received a proton reirradiation for their local relapse (after secondary exenteration for the first case, and for an ethmoid relapse in the second one).
Concerning acute toxicity (during the treatment, or the 3 months following the end of the irradiation), there was no grade III or IV toxicity. All patients presented at least a grade I radiodermitis, and 6 of them a grade II. Others grade I-II symptoms reported, relative to irradiation, were: Nausea(n = 4), keratitis (n = 1), alopecia (n = 2) and peri-orbital oedema (n = 1).
Twelve patients developed at least one late radiation-induced toxicity (Table 4). Four patients presented a brain radionecrosis, and for two of them, radionecrosis was symptomatic and needed medication (Grade III according to RTOG scale). One patient developed temporal epilepsy, while the other one presented a brain radionecrosis with a chronic osteitis of the skull bone closest to the involved tumoral site (considered as a grade IV toxicity). This last patient received two proton therapy courses with total dose of 146 Gy (RBE) because of a local recurrence, with no mention of radionecrosis on MRI before the second proton therapy.
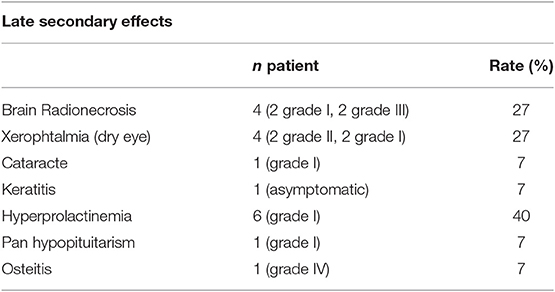
Table 4. Late secondary effects relative to irradiation.
All radionecrosis occurred in patients treated with double scattering irradiation with a prescription dose of 75.6Gy(RBE) delivered to the HR-PTV (n = 3) or in patients who received a reirradiation (n = 1). For these patients maximal doses delivered to the temporal lobe (at first treatment) were comprised between 73.51Gy(RBE) and 75.7Gy(RBE). Patients with a HR-PTV dose prescription of 73.8Gy(RBE) did not develop any radionecrosis. Dmean and Dmax delivered to the homolateral temporal lobe were 13.06Gy(RBE)[6.75–16.29] and 74.02Gy(RBE)[63.08–75.70].
Post radiation hyperprolactinemia was found for 6 patients, and one patient showed a pan-hypopituitarism which did not require any supplementation. Median Dmax and Dmean delivered to the pituitary were respectively, 53.70 Gy(RBE) [44.07–66.62] and 38.9Gy(RBE) [17.8-53.1]].
At last follow up, all patients with conservative surgery kept a stable bilateral vision compared to pre-proton therapy exams. Four patients presented a chronic grade I-II xeropthalmia. Dmax delivered to the optic chiasm and to homolateral optic nerve were 52.3Gy(RBE)[41.73–55.2] and 60.52Gy(RBE) [58.78–63.78]. Dmean and Dmax delivered to the homolateral ocular globe were 31.74Gy(RBE) [26.3–38.8]] and 66.18Gy(RBE) [55.9–73.7].
To our knowledge we reported here the largest series of patients with ACC treated with high dose adjuvant proton therapy. The overall treatment strategy in our institution consisted in a gross total resection (eye preservative surgery or exenteration) followed by high-dose adjuvant proton-therapy to a median total dose of 73.8 Gy(RBE). Given the retrospective nature of the study, the rare nature of this malignancy and thus the small number of patients in this report, we can only attempt to identify trends; it is not possible to arrive at statistically significant conclusions. It is unfortunately the main limit of our study.
However, our study suggests that high dose adjuvant proton beam irradiation was well-tolerated without high grade acute skin toxicity and produced satisfying rates of local control with limited chronic grade 3 toxicity. Patients benefited from a regular and rigorous audiometric and visual monitoring and None of the 9 patients, still having their eye at irradiation, developed grade III or IV ocular toxicity. Only few patients exhibited manageable grade II keratitis or xerophtalmia. We could however regret the lack of objective in-depth ophthalmologic evaluation such as Optical Coherence Tomography or measure of visual evoked potential. There were probably some patients with infra clinical radiation induced optic ways abnormalities who could not be detected with in routine ophthalmological evaluation.
In the literature, at standard fractionation, a 5 and 10% risk of symptomatic radiation necrosis is predicted to occur at an EQD2 of 72 Gy [range, 60–84] and 90 Gy [range, 84–102] (8, 9). Here, the radionecrosis rate is much higher, since 26% (4/15) of the patients experienced a radionecrosis. For example this rate is closer to that found in patients with locally advanced nasopharyngeal carcinoma treated with radiotherapy alone with a dose escalation (higher than in our study: 81Gy(RBE) vs. 73.8Gy(RBE) (10). This unexpected rates of radionecrosis for the prescribed dose in our study, could be caused by the use of a generic 1.1 RBE value for proton and thus the underestimation of the RBE-weighted dose at the end of proton beams. Indeed, considering our ballistic, high LET could be concentrated in the homolateral temporal lobe, and real biological dose delivered could be underestimated (11). Beddok et al. reported a brain radionecrosis rate of 35% in their series of 17 patients with previously untreated stages III–IVa nasopharyngeal carcinoma (12). These patients were treated with the same protontherapy technical as in our series. These complication is clearly inherent to the protontherapy technical. The use of new tools such as FROG a graphics processing unit (GPU)-based forward calculation tool developed at CNAO (Centro Nazionale di Adroterapia Oncologica) and at HIT (Heidelberg Ion Beam Therapy Center) for fast and accurate calculation of both physical and biological dose could be useful to limit the risk of radionecrosis (13).
The 3 years OS, local PFS and PFS rates were 78, 70, and 58%, respectively. These survival rates are close to these reported by recent retrospectives studies with modern radiotherapy modalities (5, 14, 15). Table 5 reports outcomes and toxicities from 11 recent retrospective studies (5, 14–23). All these series are heterogeneous and small. This makes direct comparisons very difficult. Wolkow (5), reported in 2018, a similar 3 years OS rate of 80% with an adjuvant high dose proton-photon mix irradiation but with higher PFS rate than us (75% for 5years PFS vs. 38% in our study). Nevertheless, our patients had a more advanced disease which could explain the shorter PFS reported in our study in comparison with Wolkow's. Indeed in Wolkow's series, there were one T3 stage and 5 T1a stage whereas in the present study we had 5 T3 or T4 stage without any T1 stage. Ahmad et al. in a series of 53 patients with lacrimal gland adenoid cystic carcinoma, found that tumor size >2.5 cm in greatest dimension correlated with significantly worse disease-free survival compared with smaller tumors (24). This difference between our population and Wolkow's could explain this PFS difference.
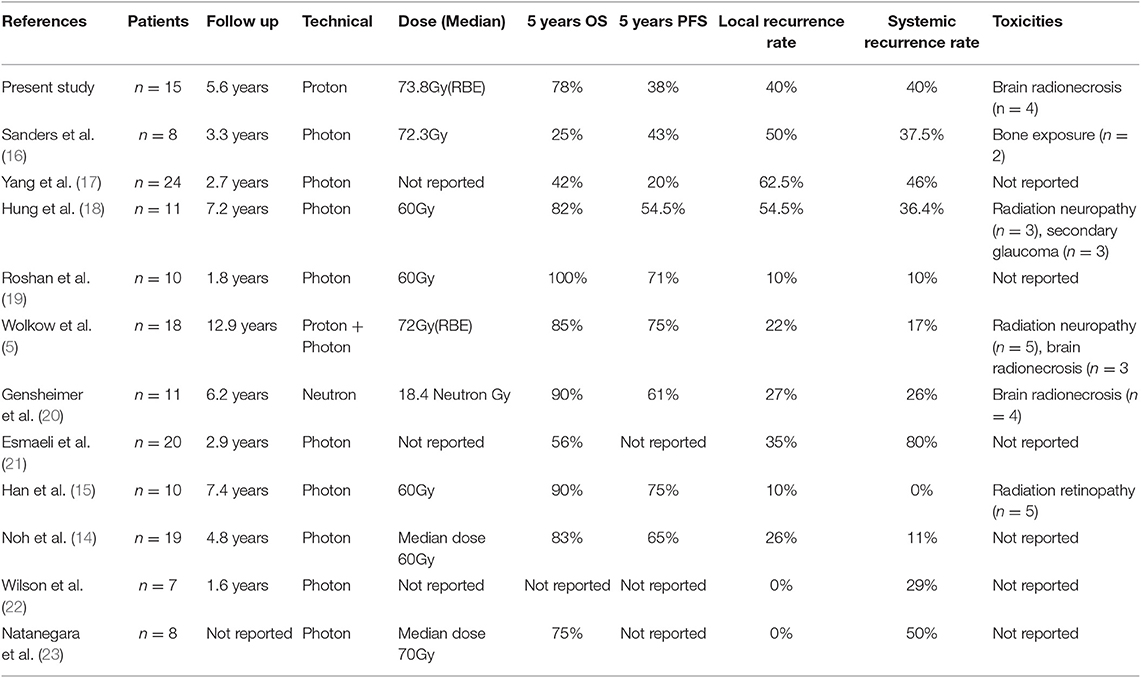
Table 5. Systematic review of studies dealing with irradiation for lacrymal gland adenoid cystic carcinoma.
If at equivalent doses, conventional radiotherapy and protontherapy should lead to the same local control rate, thus why the radiation oncologists should prefer proton-therapy? Late toxicity is expected lower in case of proton beam irradiation, particularly concerning late cognitive impairment. Indeed cognitive deterioration is a largely unrecognized sequela following irradiation of patients with head and neck cancers especially with nasopharyngeal cancer, or sinus carcinoma (25, 26). For example, in Mc Dowell's cross-sectional cohort including 102 long-term nasopharyngeal cancer survivors, impaired MoCA scores (<23) were observed in 32% of patients 7.5 years after IMRT. These patients treated with IMRT showed moderate to high rates of neurocognitive impairment and clinically significant apathy, disinhibition, and executive dysfunction (25). Meyers made the same conclusion for patients with irradiated paranasal sinuses tumors. Over 19 patients, half of the patients had difficulty learning new information, and 80% had accelerated forgetting of the information over time (27). Patients with irradiated lacrimal ACC are exposed to the same risk of cognitive deterioration. In fact frontal and temporal lobes are just behind the target volume. Based on these considerations, proton irradiation is probably the best technical to avoid long term cognitive sequelae, and could be preferred to photon irradiation. Hsiao et al., defined as threshold, a Dmean <36Gy and V60Gy <10% for temporal lobes, to reduce radiation induced cognitive impairment (28). In our population treated with proton therapy, Dmean to the homolateral temporal lobe was 13.06Gy(RBE)[6.75–16.29], far from doses reported in studies with IMRT (10, 26, 28), and may preserve the patients from cognitive disturbance. However, to a avoid cognitive disturbance, practitioners should be very careful with the distribution of high LET in order to reduce brain radionecrosis risk.
The global strategy to cure lacrimal ACC have yet to be determined. If preservative surgery (when possible) and adjuvant radiotherapy are unquestionable, the irradiation modality and the role of intra-arterial neoadjuvant chemotherapy are still discussed (29, 30).
Given our results, we can conclude that proton therapy is a safe and efficient treatment and should be considered as an adjuvant irradiation modality to privilege, when available, for patients with lacrimal ACC after conservative or radical eyeball surgery, particularly to preserve cognitive structures or contralateral optic pathways.
However, radiation oncologists should pay attention to the volume of brain irradiated with high dose, such as to avoid brain radionecrosis.
The datasets generated for this study are available on request to the corresponding author.
This study was approved by French Ethics Committees and the National Commission on informatics and Liberties (MR003 Methodology). An information letter was sent to patients still alive at time of data collection. This study adhered to the Declaration of Helsinki.
PL wrote the synopsis, the manuscript, computed statistical analyses, and recorded medical data. ER recorded medical data. VC recorded medical data, wrote the synopsis, helped write and improve the manuscript. CL, OG, PJ, and RD were the treating physicians for most of these patients and participated in proofreading. LD and FG were the medical physicists involved in the treatment planification.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2020.00135/full#supplementary-material
1. Bernardini FP, Devoto MH, Croxatto JO. Epithelial tumors of the lacrimal gland: an update. Curr Opin Ophthalmol. (2008) 19:409–13. doi: 10.1097/ICU.0b013e32830b13e1
2. Mallen-St Clair J, Arshi A, Tajudeen B, Abemayor E, St John M. Epidemiology and treatment of lacrimal gland tumors: a population-based cohort analysis. JAMA Otolaryngol Head Neck Surg. (2014) 140:1110–6. doi: 10.1001/jamaoto.2014.2846
3. Mendenhall WM, Morris CG, Amdur RJ, Werning JW, Hinerman RW, Villaret DB. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck. (2004) 26:154–62. doi: 10.1002/hed.10380
4. Le Tourneau C, Razak ARA, Levy C, Calugaru V, Galatoire O, Dendale R, Desjardins L, Gan HK. Role of chemotherapy and molecularly targeted agents in the treatment of adenoid cystic carcinoma of the lacrimal gland. Br J Ophthalmol. (2011) 95:1483–9. doi: 10.1136/bjo.2010.192351
5. Wolkow N, Jakobiec FA, Lee H, Sutula FC. Long-term outcomes of globe-preserving surgery with proton beam radiation for adenoid cystic carcinoma of the lacrimal Gland. Am J Ophthalmol. (2018) 195:43–62. doi: 10.1016/j.ajo.2018.07.024
6. Holliday EB, Esmaeli B, Pinckard J, Garden AS, Rosenthal DI, Morrison WH, et al. A multidisciplinary orbit-sparing treatment approach that includes proton therapy for epithelial tumors of the orbit and ocular adnexa. Int J Radiat Oncol Biol Phys. (2016) 95:344–52. doi: 10.1016/j.ijrobp.2015.08.008
7. Woo KI, Sagiv O, Han J, Frank SJ, Kim Y-D, Esmaeli B. Eye-preserving surgery followed by adjuvant radiotherapy for lacrimal gland carcinoma: outcomes in 37 patients. Ophthal Plast Reconstr Surg. (2018) 34:570–4. doi: 10.1097/IOP.0000000000001106
8. Lawrence YR, Li XA, el Naqa I, Hahn CA, Marks LB, Merchant TE, Dicker AP. Radiation dose–volume effects in the brain. Int J Radiat Oncol Biol Phys. (2010) 76:S20–7. doi: 10.1016/j.ijrobp.2009.02.091
9. Tuan JKL, Ha TC, Ong WS, Siow TR, Tham IWK, Yap SP, et al. Late toxicities after conventional radiation therapy alone for nasopharyngeal carcinoma. Radiother Oncol J Eur Soc Ther Radiol Oncol. (2012) 104:305–11. doi: 10.1016/j.radonc.2011.12.028
10. Yeh S-A, Huang Y-J. Dose escalation for patients with locally advanced nasopharyngeal carcinoma treated with radiotherapy alone. Am J Clin Oncol. (2007) 30:401–5. doi: 10.1097/COC.0b013e31803377b3
11. Paganetti H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Phys Med Biol. (2014) 59:R419–72. doi: 10.1088/0031-9155/59/22/R419
12. Beddok A, Feuvret L, Noel G, Bolle S, Deberne M, Mammar H, et al. Efficacy and toxicity of proton with photon radiation for locally advanced nasopharyngeal carcinoma. Acta Oncol. (2019) 58:472–4. doi: 10.1080/0284186X.2018.1543948
13. Choi K, Mein SB, Kopp B, Magro G, Molinelli S, Ciocca M, et al. FRoG-a new calculation engine for clinical investigations with proton and carbon ion beams at CNAO. Cancers. (2018) 10. doi: 10.3390/cancers10110395
14. Noh JM, Lee E, Ahn YC, Oh D, Kim Y-D, Woo KI, et al. Clinical significance of post-surgical residual tumor burden and radiation therapy in treating patients with lacrimal adenoid cystic carcinoma. Oncotarget. (2016) 7:60639–46. doi: 10.18632/oncotarget.10259
15. Han J, Kim Y-D, Woo KI, Sobti D. Long-term outcomes of eye-sparing surgery for adenoid cystic carcinoma of lacrimal Gland. Ophthal Plast Reconstr Surg. (2018) 34:74–8. doi: 10.1097/IOP.0000000000000877
16. Sanders JC, Mendenhall WM, Werning JW. Adenoid cystic carcinoma of the lacrimal gland. Am J Otolaryngol. (2016) 37:144–7. doi: 10.1016/j.amjoto.2015.09.015
17. Yang J, Zhou C, Wang Y, Fan X, Jia R. Multimodal therapy in the management of lacrimal gland adenoid cystic carcinoma. BMC Ophthalmol. (2019) 19:125. doi: 10.1186/s12886-019-1110-5
18. Hung J-Y, Wei Y-H, Huang C-H, Chen L-W, Fuh C-S, Liao S-L. Survival outcomes of eye-sparing surgery for adenoid cystic carcinoma of lacrimal gland. Jpn J Ophthalmol. (2019) 63:344–51. doi: 10.1007/s10384-019-00671-w
19. Roshan V, Pathy S, Mallick S, Chander S, Sen S, Chawla B. Adjuvant radiotherapy with three-dimensional conformal radiotherapy of lacrimal gland adenoid cystic carcinoma. J Clin Diagn Res. (2015) 9:XC05–7. doi: 10.7860/JCDR/2015/14452.6669
20. Gensheimer MF, Rainey D, Douglas JG, Liao JJ, Laramore GE, Jian-Amadi A, et al. Neutron radiotherapy for adenoid cystic carcinoma of the lacrimal gland. Ophthal Plast Reconstr Surg. (2013) 29:256–60. doi: 10.1097/IOP.0b013e318295f99b
21. Esmaeli B, Ahmadi MA, Youssef A, Diba R, Amato M, Myers JN, et al. Outcomes in patients with adenoid cystic carcinoma of the lacrimal gland. Ophthal Plast Reconstr Surg. (2004) 20:22–6. doi: 10.1097/01.IOP.0000105518.72611.4F
22. Wilson KF, Ward PD, Spector ME, Marentette LJ. Orbitocranial approach for treatment of adenoid cystic carcinoma of the lacrimal gland. Ann Otol Rhinol Laryngol. (2011) 120:397–400. doi: 10.1177/000348941112000609
23. Natanegara IAAA, Koornneef L, Veenhof K, Gonzáles DG, Boukes RJ. An alternative approach for the management of adenocystic carcinoma of the lacrimal gland. Orbit. (1990) 9:101–5. doi: 10.3109/01676839009012354
24. Ahmad SM, Esmaeli B, Williams M, Nguyen J, Fay A, Woog J, Selvadurai D, et al. American Joint Committee on Cancer classification predicts outcome of patients with lacrimal gland adenoid cystic carcinoma. Ophthalmology. (2009) 116:1210–5. doi: 10.1016/j.ophtha.2008.12.049
25. McDowell LJ, Ringash J, Xu W, Chan B, Lu L, Waldron J, et al. A cross sectional study in cognitive and neurobehavioral impairment in long-term nasopharyngeal cancer survivors treated with intensity-modulated radiotherapy. Radiother Oncol J Eur Soc Ther Radiol Oncol. (2019) 131:179–85. doi: 10.1016/j.radonc.2018.09.012
26. Takiar V, Ma D, Garden AS, Li J, Rosenthal DI, Beadle BM, et al. Disease control and toxicity outcomes for T4 carcinoma of the nasopharynx treated with intensity-modulated radiotherapy. Head Neck. (2016) 38 (Suppl. 1):E925–33. doi: 10.1002/hed.24128
27. Meyers CA, Geara F, Wong P-F, Morrison WH. Neurocognitive effects of therapeutic irradiation for base of skull tumors. Int J Radiat Oncol Biol Phys. (2000) 46:51–5. doi: 10.1016/S0360-3016(99)00376-4
28. Hsiao K-Y, Yeh S-A, Chang C-C, Tsai P-C, Wu J-M, Gau J-S. Cognitive function before and after intensity-modulated radiation therapy in patients with nasopharyngeal carcinoma: a prospective study. Int J Radiat Oncol Biol Phys. (2010) 77:722–6. doi: 10.1016/j.ijrobp.2009.06.080
29. Akbaba S, Lang K, Held T, Herfarth K, Rieber J, Plinkert P, et al. Carbon-ion radiotherapy in accelerated hypofractionated active raster-scanning technique for malignant lacrimal gland tumors: feasibility and safety. Cancer Manag Res. (2019) 11:1155–66. doi: 10.2147/CMAR.S190051
Keywords: proton-therapy, cystic adenoid carcinoma, lacrymal carcinoma, adjuvant irradiation, radionecrosis
Citation: Lesueur P, Rapeaud E, De Marzi L, Goudjil F, Levy C, Galatoire O, Jacomet PV, Dendale R and Calugaru V (2020) Adenoid Cystic Carcinoma of the Lacrimal Gland: High Dose Adjuvant Proton Therapy to Improve Patients Outcomes. Front. Oncol. 10:135. doi: 10.3389/fonc.2020.00135
Received: 18 September 2019; Accepted: 27 January 2020;
Published: 18 February 2020.
Edited by:
Steven H. Lin, University of Texas MD Anderson Cancer Center, United StatesReviewed by:
Michael Andrew Samuels, University of Miami, United StatesCopyright © 2020 Lesueur, Rapeaud, De Marzi, Goudjil, Levy, Galatoire, Jacomet, Dendale and Calugaru. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paul Lesueur, UGF1bC5MZXN1ZXVyODlAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.