 Tamara Díaz-Redondo1,2
Tamara Díaz-Redondo1,2 Rocio Lavado-Valenzuela1,3Begoña Jimenez1,2
Rocio Lavado-Valenzuela1,3Begoña Jimenez1,2 Tomas Pascual4Fernando Gálvez5Alejandro Falcón6Maria del Carmen Alamo7
Tomas Pascual4Fernando Gálvez5Alejandro Falcón6Maria del Carmen Alamo7 Cristina Morales8Marta Amerigo9
Cristina Morales8Marta Amerigo9 Javier Pascual10Alfonso Sanchez-Muñoz1,2Macarena González-Guerrero11Luis Vicioso1,12
Javier Pascual10Alfonso Sanchez-Muñoz1,2Macarena González-Guerrero11Luis Vicioso1,12 Aurora Laborda3Maria Victoria Ortega1,12Lidia Perez1,12Aranzazu Fernandez-Martinez13Nuria Chic4Jose Manuel Jerez1,14
Aurora Laborda3Maria Victoria Ortega1,12Lidia Perez1,12Aranzazu Fernandez-Martinez13Nuria Chic4Jose Manuel Jerez1,14 Martina Alvarez1,3,12
Martina Alvarez1,3,12 Aleix Prat4
Aleix Prat4 Nuria Ribelles1,2*Emilio Alba1,2,3
Nuria Ribelles1,2*Emilio Alba1,2,3- 1Instituto de Investigación Biomédica de Málaga (IBIMA), Hospitales Universitarios Regional y Virgen de la Victoria, Málaga, Spain
- 2Unidad de Gestión Clínica Oncología Intercentros, Hospitales Universitarios Regional y Virgen de la Victoria, Málaga, Spain
- 3Laboratorio de Biología Molecular del Cáncer, Centro de Investigaciones Médico-Sanitarias (CIMES), Universidad de Málaga, Málaga, Spain
- 4Translational Genomics and Targeted Therapeutics in Solid Tumors Lab (IDIBAPS), Hospital Clinic de Barcelona, Barcelona, Spain
- 5Hospital Universitario Ciudad de Jaén, Jaén, Spain
- 6Hospital Universitario Virgen del Rocío, Sevilla, Spain
- 7Hospital Universitario Virgen Macarena, Sevilla, Spain
- 8Hospital Reina Sofía, Córdoba, Spain
- 9Hospital Juan Ramón Jiménez, Huelva, Spain
- 10Hospital Costa del Sol, Marbella, Spain
- 11Hospital Universitario Puerta del Mar, Cádiz, Spain
- 12Unidad de Gestión Clínica Anatomía Patológica Intercentros, Hospitales Universitarios Regional y Virgen de la Victoria, Málaga, Spain
- 13Lineberger Comprehensive Cancer Center, University of North Caroina at Chapel Hill, Chapel Hill, NC, United States
- 14Departamento de Lenguajes y Ciencias de la Computación, Universidad de Málaga, Málaga, Spain
Background: Double blockade with pertuzumab and trastuzumab combined with chemotherapy is the standard neoadjuvant treatment for HER2-positive early breast cancer. Data derived from clinical trials indicates that the response rates differ among intrinsic subtypes of breast cancer. The aim of this study is to determine if these results are valid in real-world patients.
Methods: A total of 259 patients treated in eight Spanish hospitals were included and divided into two cohorts: Cohort A (132 patients) received trastuzumab plus standard neoadjuvant chemotherapy (NAC), and Cohort B received pertuzumab and trastuzumab plus NAC (122 patients). Pathological complete response (pCR) was defined as the complete disappearance of invasive tumor cells. Assignment of the intrinsic subtype was realized using the research-based PAM50 signature.
Results: There were more HER2-enriched tumors in Cohort A (70 vs. 56%) and more basal-like tumors in Cohort B (12 vs. 2%), with similar luminal cases in both cohorts (luminal A 12 vs. 14%; luminal B 14 vs. 18%). The overall pCR rate was 39% in Cohort A and 61% in Cohort B. Better pCR rates with pertuzumab plus trastuzumab than with trastuzumab alone were also observed in all intrinsic subtypes (luminal PAM50 41 vs. 11.4% and HER2-enriched subtype 73.5 vs. 50%) but not in basal-like tumors (53.3 vs. 50%). In multivariate analysis the only significant variables related to pCR in both luminal PAM50 and HER2-enriched subtypes were treatment with pertuzumab plus trastuzumab (Cohort B) and histological grade 3.
Conclusions: With data obtained from patients treated in clinical practice, it has been possible to verify that the addition of pertuzumab to trastuzumab and neoadjuvant chemotherapy substantially increases the rate of pCR, especially in the HER2-enriched subtype but also in luminal subtypes, with no apparent benefit in basal-like tumors.
Introduction
The contribution of anti-HER2 therapies to the management of HER2-positive breast cancer patients is undeniable both in metastatic and adjuvant settings (1–6). In the same way, significant benefit was observed with neoadjuvant trastuzumab treatment, obtaining pathological complete response (pCR) rates from 25 to 46% (7–12). These results were improved with the use of pertuzumab combined with trastuzumab, reaching pCR rates between 49 and 69% (8, 13–17).
Several authors have shown that all four intrinsic subtypes can be found in clinically HER2+ tumors. Although the majority of cases are HER2 enriched (40–72%), luminal A (10–27%), luminal B (10–28%), and basal-like tumors (7–14%) are also represented (13, 17–24). This distribution may vary depending on the hormone receptor status. In the hormone-receptor-negative subset, the main intrinsic subtype was HER2 enriched (51–85%), with fewer cases of luminal (luminal A 0.7–24%; luminal B 3–11%), and basal-like subtypes (9–28%) (12, 19, 20, 22, 24, 25). In contrast, in hormone-receptor-positive tumors, luminal subtypes were more frequent (luminal A 28–44%; luminal B 24–48%) than HER2-enriched (8–32%) or basal-like (0.5–2.5%) ones (12, 20, 22, 25, 26).
This heterogeneity is also reflected in the magnitude of the benefit of neoadjuvant anti-HER2 therapies. In the NOAH trial, pCR rate obtained in the trastuzumab arm was higher in the HER2-enriched subtype and in tumors with high ROR scores (18). This association was also observed in patients treated with double HER2 blockade (i.e., trastuzumab plus lapatinib or trastuzumab plus pertuzumab) plus chemotherapy. Neoadjuvant trastuzumab with or without lapatinib shows pCR rates of 50–70% in HER2-enriched tumors, 9–34% in luminal A, 17–36% in luminal B, and 25–38% in basal-like cases (12, 25, 27). Similarly, pCR rates by intrinsic subtype in patients treated with neoadjuvant pertuzumab plus trastuzumab were 70–83% in the HER2-enriched subtype, 16–45% in luminal A, 16–52% in luminal B, and 20–85% in basal-like tumors (13, 17, 22, 23). In a series of patients with BluePrint-defined subtypes, the pCR rate was 76% in the HER2+ type, 31% in the luminal type, and 43% in the basal type (28).
The aim of this work was to evaluate whether the effect of neoadjuvant pertuzumab combined with trastuzumab in comparison with trastuzumab alone varies as a function of PAM50-defined intrinsic subtypes in a real-world cohort of patients with HER2-positive early breast cancer.
Materials and Methods
Patients
A total of 254 patients with HER2+ early breast cancer consecutively treated with standard neoadjuvant chemotherapy (NAC) in eight Spanish hospitals were included in the study. The whole population was divided in two cohorts: Cohort A received trastuzumab plus NAC, and Cohort B was treated with pertuzumab and trastuzumab plus NAC. Standard NAC included taxanes with or without anthracyclines. Adjuvant radiotherapy was performed according local practice. Adjuvant endocrine therapy was administered in all hormone-receptor-positive patients.
Patient data were derived from the patients' clinical records and original pathology reports. Although the analysis was retrospective, the data were collected prospectively.
The study was approved by local ethics committees. Written informed consent was obtained from each participant.
Definition of pCR, Hormone Receptor, HER2 Status, Immunohistochemical Phenotype, and Intrinsic Subtype
pCR was defined as the complete disappearance of invasive tumor cells (ypT0 or ypTis and ypN0). All pathological determinations were performed on diagnostic biopsies. Tumors were classified as estrogen-receptor and progesterone-receptor-positive if ≥1% of tumor cells were stained. HER2+ status was defined by an immunohistochemistry score of 3+ or a HER2 amplification ratio of 2.0 or more by FISH or SISH. Hormone-receptor-positive cases were classified as Luminal-HER2 (luminal immunophenotype) and those with negative hormone receptors such ones as HER2+ (HER2+ immunophenotype).
Assignment of the intrinsic subtype was realized using the research-based PAM50 signature as previously described (29) in order to categorize all cases as one of the following subtypes: luminal A, luminal B, HER2-enriched, basal-like, and normal-like.
Statistical Analysis
Associations between variables and pCR were evaluated by the chi-squared test or Fisher's exact test. Multivariate logistic regression analyses were used to evaluate the association of each intrinsic subtype with pCR and included the variables that showed significant associations in univariate analyses. Cases with unknown data for any of the variables considered were excluded from multivariate analyses.
All the tests were two-sided, and a P-value of < 0.05 was considered to indicate statistical significance. Analyses were carried out using the R system for statistical computing (version 3.5.2).
Results
Patients' Characteristics
A total of 254 patients were included in the study: 132 patients were treated with NAC plus trastuzumab (Cohort A) and 122 patients with NAC plus pertuzumab and trastuzumab (Cohort B). The clinical characteristics are outlined in Table 1. There were more cases with a greater tumor burden in Cohort B than in Cohort A (T3 or T4 tumor size: 33 vs. 19%; stage I: 1 vs. 14%). Slightly more patients were treated with taxanes alone in Cohort B (14 vs. 7%).
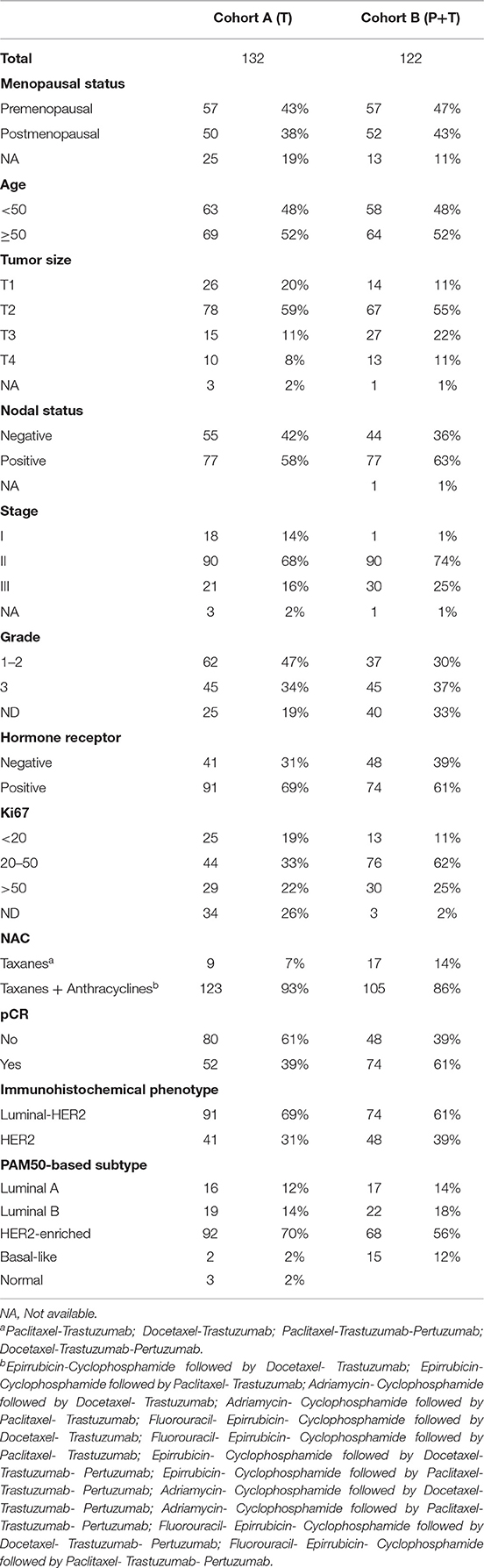
Table 1. Patient characteristics.
The overall pCR rate was 39% in Cohort A and 61% in Cohort B. The immunohistochemical phenotype distribution was similar in both cohorts: luminal-HER2 69 vs. 61% and HER2+ cases 31 vs. 39%. Regarding PAM50-assigned subtypes, there were more HER2-enriched tumors in Cohort A (70 vs. 56%) and more basal-like tumors in Cohort B (12 vs. 2%), with similar luminal case distributions (luminal A 12 vs. 14%; luminal B 14 vs. 18%).
Association Between Variables and pCR
In the whole population (Table 2), pCR was significantly related to the type of treatment (Cohort A 39.4% vs. Cohort B 60.6%; P = 0.0011), histological grade (grade 1 + 2 35.5% vs. grade 3 62.2%; P = 0.0007), Ki67 level (<20% 28.9% vs. 20–50% 60.8% vs. >50% 54.2%; P = 0.003), immunohistochemical phenotype (luminal HER2 38.7% vs. HER2+ 69.6%; P = 0.000005), and PAM50-based subtype (luminal A 21.2% vs. luminal B 31.7% vs. HER-2 enriched 60% vs. basal like 52.9%; P = 0.0004). Similar results were observed in separate analyses of each cohort (Table 2).
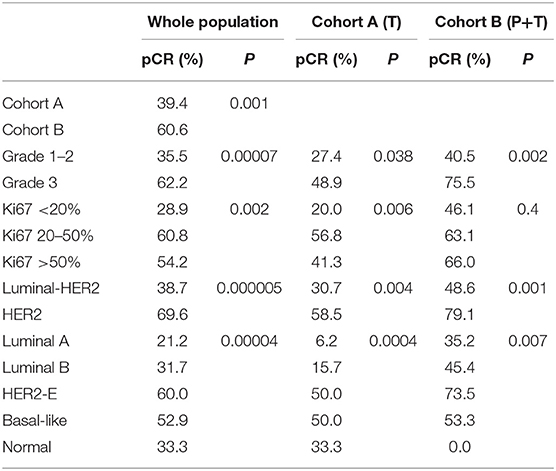
Table 2. Association between variables and pCR.
The better results found in cohort B in the whole population were also observed in an evaluation of different subpopulations (Table 3). Thus, immunohistochemical luminal tumors showed greater pCR with pertuzumab and trastuzumab treatment (48.6 vs. 30.8%; P = 0.03) and also HER2+ patients (58.5 vs. 79.6%; P = 0.06). In addition, in the luminal PAM50-based subtype, a pCR rate of 11.4% was obtained with trastuzumab treatment vs. 41% with combination treatment (P = 0.008) and in the HER2-enriched subtype, these rates were 50 vs. 73.5% (P = 0.004).
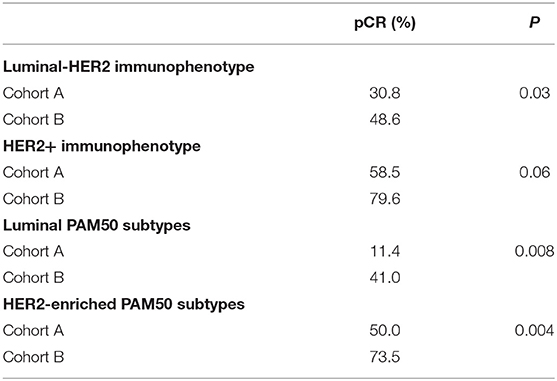
Table 3. Association between variables and pCR in specific subpopulations.
Multivariate Analyses
The variables that remained significantly associated with pCR in the whole population were treatment Cohort B [Odds Ratio (OR) 2.5; 95% CI 1.07–6; P = 0.036], histological grade 3 (OR 3.41; 95% CI 14.48–8.09; P = 0.004), immunophenotype HER2+ (OR 3.82; 95% CI 1.39–11.6; P = 0.01), and PAM50-based HER2-enriched subtype (OR 2.98; 95% CI 1.39–11.6; P = 0.02) (Table 4).
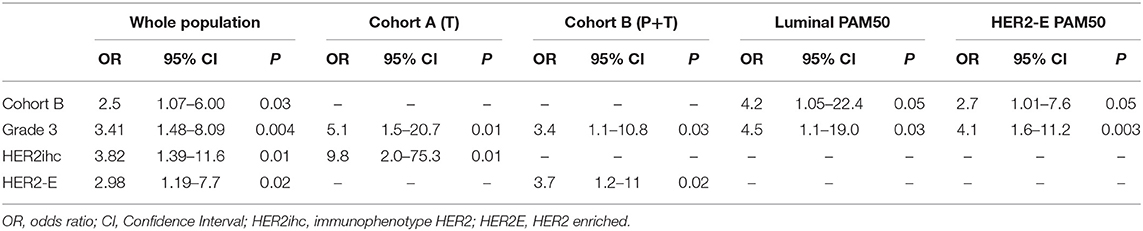
Table 4. Multivariate logistic regression of pCR.
In the cohort of patients treated with trastuzumab alone, grade 3 (OR 5.1; 95% CI 1.5–20.7; P = 0.01) and immunophenotype HER2+ (OR 9.8; 95% CI 2.0–75.3; P = 0.01) were the only variables independently associated with a higher probability of pCR, and in the cohort of patients that received pertuzumab and trastuzumab, these variables were grade 3 (OR 3.4; 95% CI 1.1–10.8; P = 0.03) and PAM50-based HER2-enriched subtype (OR 3.7; 95% CI 1.2–11; P = 0.02) (Table 4).
In an analysis of luminal PAM50-based tumors, the variables that remained significantly associated with pCR were treatment Cohort B (OR 4.2; 95% CI 1.05–22.4; P = 0.05), and grade 3 (OR 4.5; 95% CI 1.1–19.0; P = 0.03); this was also true in the HER2-enriched subgroup (Cohort B OR 2.7; 95% CI 1.01–7.6; P = 0.05. Grade 3 OR 4.1; 95% CI 1.6–11.2; P = 0.003) (Table 4).
Discussion
Our study provides valuable information from the real world about neoadjuvant anti-HER2 treatment in early breast cancer, showing that the rate of pCR obtained by double blockade with pertuzumab plus trastuzumab exceeds by 20% that obtained with trastuzumab alone. The pCR rate observed in our series with pertuzumab and trastuzumab treatment (60.6%) is in the range of responses observed in the published phase II-III trials (45.8–69.8%) (8, 13–15, 17, 22). Moreover, the pCR rate found in patients treated with trastuzumab alone (39.4%) is in agreement with previous data (31–46%) (7–12). Interestingly, the greater efficacy shown by the combination of pertuzumab and trastuzumab in our study was despite the fact that the patients in this cohort had worse prognostic characteristics than those who received trastuzumab alone, with a higher percentage of tumors larger than 5 cm or a greater number of cases with nodal involvement. Lower pCR rates were observed in patients with the luminal immunophenotype in both the cohort treated with pertuzumab and trastuzumab and in the one receiving trastuzumab alone. This finding is consistent with previously published data (8, 9, 12, 15, 17, 28).
Although most tumors positive for HER2 by immunohistochemistry or by in situ hybridization correspond to the intrinsic HER2-enriched subtype, it is possible to identify any of the remaining intrinsic subtypes in this type of tumor (19, 29, 30). Surprisingly, the percentage of cases by intrinsic subtype in our two patient cohorts differ to some extent, despite the fact that the processing of the tumor samples was performed in the same laboratory, albeit at different times. In the group of patients treated with pertuzumab and trastuzumab, 56% of the cases corresponded to the HER2-enriched, 14% to the luminal A, 18% to the luminal B, and 12% to the basal-like subtype, and this distribution is in agreement with previously published data (13, 17, 18, 20, 22, 23). However, in the cohort of patients who received trastuzumab alone, there was a higher percentage of HER2-enriched cases (70%), a lower number of basal-like tumors (2%), and a similar amount of luminal tumors (luminal A 12%; luminal B 14%). Similar data were reported by Perez et al. from NCCTG N9831 Trial (21) and more recently by Tolaney et al. from the APT Trial (24).
Anti-HER2 therapies are more beneficial in HER2-enriched tumors, but all intrinsic subtypes benefit from this type of treatment in both the adjuvant (20, 21) and neoadjuvant settings, and the HER2-enriched subtype benefits the most (13, 17, 18, 22, 23, 28). According to these data, our patients with HER2-enriched tumors obtained the highest pCR rate with both treatment schedules. Furthermore, the use of pertuzumab and trastuzumab was the only variable, together with the histological grade, that provided independent predictive information for pCR events in both HER2-enriched tumors (OR 2.7) and patients with luminal subtypes (OR 4.2). Although the number of patients was small, the basal-like subtype shows no benefit with the use of anti-HER2 therapy, achieving nearly the same pCR rate with pertuzumab and trastuzumab as with trastuzumab alone.
To our knowledge, there is no published series of real-world patients with early HER2+ breast cancer treated with NAC plus pertuzumab and trastuzumab or trastuzumab alone, in which the intrinsic subtypes have been established according to the PAM50 definition and their relationship with the pCR rate analyzed. Beitsch et al. (28) published data from patients included in a prospective registry, of whom 178 were treated with NAC plus trastuzumab and 119 with NAC plus pertuzumab and trastuzumab and in which the molecular subtype was defined by BluePrint platform. Their results agree with ours, showing a higher response with double HER2 blockade vs. treatment with trastuzumab alone in the HER2+ type (76% vs. 57%) and the luminal type (31% vs. 8%) and no differences in the basal type (43% vs. 45%). Recently, Fashing et al. (31) published their results from a series of patients included in an ongoing registry comparing two cohorts of patients that received neoadjuvant treatment with chemotherapy plus trastuzumab or chemotherapy plus trastuzumab and pertuzumab. In agreement with our results, there was a greater number of pCR in patients treated with pertuzumab plus trastuzumab with an adjusted OR for double HER2 blockade vs. trastuzumab alone of 2.04 (95% CI 1.24–3.35).
Our results confirm the data obtained from clinical trials in patients treated in clinical practice, showing that the addition of pertuzumab to trastuzumab and neoadjuvant chemotherapy increase the pCR rate substantially, especially in the HER2-enriched subtype but also in luminal subtypes, with no apparent benefit in basal-like tumors.
Data Availability Statement
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité de Ética de la Investigación Provincial de Málag, Servicio Andaluz de Salud, Consejería de Salud, Junta de Andalucía. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
EA, TD-R, and AP made substantial contributions to the conception of the work. TD-R, RL-V, BJ, TP, FG, AF, MCA, CM, MAl, JP, AS-M, MG-G, LV, AL, MO, LP, AF-M, NC, and MAm contributed to the acquisition of the data. EA, JJ, TD-R, and NR contributed to the analysis of data. NR and EA drafting the work. All authors approved the final version of the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors acknowledge support through grant TIN2017-88728-C2-1-R from MICINN SPAIN.
References
1. Slamon DJ, Leyland-Jones B, Shak S, Fuchs H, Paton V, Bajamonde A, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. (2001) 344:783–92. doi: 10.1056/NEJM200103153441101
2. Cameron D, Piccart-Gebhart MJ, Gelber RD, Procter M, Goldhirsch A, de Azambuja E, et al. 11 years' follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive early breast cancer: final analysis of the HERceptin Adjuvant (HERA) trial. Lancet. (2017) 389:1195–205. doi: 10.1016/S0140-6736(16)32616-2
3. Perez EA, Romond EH, Suman VJ, Jeong JH, Sledge G, Geyer CE Jr, et al. Trastuzumab plus adjuvant chemotherapy for human epidermal growth factor receptor 2-positive breast cancer: planned joint analysis of overall survival from NSABP B-31 and NCCTG N9831. J Clin Oncol. (2014) 32:3744–52. doi: 10.1200/JCO.2014.55.5730
4. Slamon D, Eiermann W, Robert N, Pienkowski T, Martin M, Press M, et al. Ten year follow-up of the BCIRG-006 trial comparing doxorubicin plus cyclophosphamide followed by docetaxel (AC-.T) with doxorubicin plus cyclophosphamide followed by docetaxel and trastuzumab (AC-.TH) with docetaxel, carboplatin and trastuzumab (TCH) in HER2+ early breast cancer patients. Cancer Res. (2015) 76. doi: 10.1158/1538-7445.SABCS15-S5-04
5. Swain SM, Kim SB, Cortes J, Ro J, Semiglazov V, Campone M, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA study): overall survival results from a randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. (2013) 14:461–71. doi: 10.1016/S1470-2045(13)70130-X
6. Bachelot T, Ciruelos E, Schneeweiss A, Puglisi F, Peretz-Yablonski T, Bondarenko I, et al. Preliminary safety and efficacy of first-line pertuzumab combined with trastuzumab and taxane therapy for HER2-positive locally recurrent or metastatic breast cancer (PERUSE). Ann Oncol. (2019) 30:766–73. doi: 10.1093/annonc/mdz061
7. Gianni L, Eiermann W, Semiglazov V, Manikhas A, Lluch A, Tjulandin S, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. (2010) 375:377–84. doi: 10.1016/S0140-6736(09)61964-4
8. Gianni L, Pienkowski T, Im YH, Roman L, Tseng LM, Liu MC, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. (2012) 13:25–32. doi: 10.1016/S1470-2045(11)70336-9
9. Baselga J, Bradbury I, Eidtmann H, Di Cosimo S, de Azambuja E, Aura C, et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): a randomised, open-label, multicentre, phase 3 trial. Lancet. (2012) 379:633–40. doi: 10.1016/S0140-6736(11)61847-3
10. Guarneri V, Frassoldati A, Bottini A, Cagossi K, Bisagni G, Sarti S, et al. Preoperative chemotherapy plus trastuzumab, lapatinib, or both in human epidermal growth factor receptor 2-positive operable breast cancer: results of the randomized phase II CHER-LOB study. J Clin Oncol. (2012) 30:1989–95. doi: 10.1200/JCO.2011.39.0823
11. Untch M, Loibl S, Bischoff J, Eidtmann H, Kaufmann M, Blohmer JU, et al. Lapatinib versus trastuzumab in combination with neoadjuvant anthracycline-taxane-based chemotherapy (GeparQuinto, GBG 44): a randomised phase 3 trial. Lancet Oncol. (2012) 13:135–44. doi: 10.1016/S1470-2045(11)70397-7
12. Carey LA, Berry DA, Cirrincione CT, Barry WT, Pitcher BN, Harris LN, et al. Molecular heterogeneity and response to neoadjuvant human epidermal growth factor receptor 2 targeting in CALGB 40601:a randomized phase III trial of paclitaxel plus trastuzumab with or without lapatinib. J Clin Oncol. (2016) 34:542–9. doi: 10.1200/JCO.2015.62.1268
13. Gavila J, Oliveira M, Pascual T, Pérez J, Canes J, González X, et al. Association of intrinsic subtype and immune genes with pathological complete response in the OPTIHER-HEART phase II clinical trial following neoadjuvant trastuzumab/pertuzumab-based chemotherapy in HER2-positive breast cancer. Cancer Res. (2018) 78. doi: 10.1158/1538-7445.SABCS17-P2-09-04
14. Schneeweiss A, Chia S, Hickish T, Harvey V, Eniu A, Hegg R, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. (2013) 24:2278–84. doi: 10.1093/annonc/mdt182
15. Untch M, Jackisch C, Schneeweiss A, Conrad B, Aktas B, Denkert C, et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trial. Lancet Oncol. (2016) 17:345–56. doi: 10.1016/S1470-2045(15)00542-2
16. Hurvitz SA, Martin M, Symmans WF, Jung KH, Huang CS, Thompson AM, et al. Neoadjuvant trastuzumab, pertuzumab, and chemotherapy versus trastuzumab emtansine plus pertuzumab in patients with HER2-positive breast cancer (KRISTINE): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. (2018) 19:115–26. doi: 10.1016/S1470-2045(17)30716-7
17. Swain SM, Ewer MS, Viale G, Delaloge S, Ferrero JM, Verrill M, et al. Pertuzumab, trastuzumab, and standard anthracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive localized breast cancer (BERENICE): a phase II, open-label, multicenter, multinational cardiac safety study. Ann Oncol. (2018) 29:646–53. doi: 10.1093/annonc/mdx773
18. Prat A, Bianchini G, Thomas M, Belousov A, Cheang MC, Koehler A, et al. Research-based PAM50 subtype predictor identifies higher responses and improved survival outcomes in HER2-positive breast cancer in the NOAH study. Clin Cancer Res. (2014) 20:511–21. doi: 10.1158/1078-0432.CCR-13-0239
19. Prat A, Carey LA, Adamo B, Vidal M, Tabernero J, Cortes J, et al. Molecular features and survival outcomes of the intrinsic subtypes within HER2-positive breast cancer. J Natl Cancer Inst. (2014) 106:dju152. doi: 10.1093/jnci/dju152
20. Pogue-Geile KL, Song N, Jeong JH, Gavin PG, Kim SR, Blackmon NL, et al. Intrinsic subtypes, PIK3CA mutation, and the degree of benefit from adjuvant trastuzumab in the NSABP B-31 trial. J Clin Oncol. (2015) 33:1340–7. doi: 10.1200/JCO.2014.56.2439
21. Perez EA, Ballman KV, Mashadi-Hossein A, Tenner KS, Kachergus JM, Norton N, et al. Intrinsic subtype and therapeutic response among HER2-positive breaty st tumors from the NCCTG (Alliance) N9831 trial. J Natl Cancer Inst. (2017) 109:djw207. doi: 10.1093/jnci/djw207
22. Prat A, Slamon D, Hurvitz S, Press MF, Lewis Phillips G, Valverde VL, et al. Association of intrinsic subtypes with pathological complete response (pCR) in the KRISTINE neoadjuvant phase 3 clinical trial in HER2-positive early breast cancer (EBC). Abstract PD3–06. Cancer Res. (2017) 78. doi: 10.1158/1538-7445.SABCS17-PD3-06
23. Ignatiadis M, Van den Eynden G, Roberto S, Fornili M, Bareche Y, Desmedt C, et al. Tumor-infiltrating lymphocytes in patients receiving trastuzumab/pertuzumab-based chemotherapy: a TRYPHAENA substudy. J Natl Cancer Inst. (2019) 111:69–77. doi: 10.1093/jnci/djy076
24. Tolaney SM, Guo H, Pernas S, Barry WT, Dillon DA, Ritterhouse L, et al. Seven-year follow-up analysis of adjuvant paclitaxel and trastuzumab trial for node-negative, human epidermal growth factor receptor 2-positive breast cancer. J Clin Oncol. (2019) 37:1868–75. doi: 10.1200/JCO.19.00066
25. Dieci MV, Prat A, Tagliafico E, Pare L, Ficarra G, Bisagni G, et al. Integrated evaluation of PAM50 subtypes and immune modulation of pCR in HER2-positive breast cancer patients treated with chemotherapy and HER2-targeted agents in the CherLOB trial. Ann Oncol. (2016) 27:1867–73. doi: 10.1093/annonc/mdw262
26. Cejalvo JM, Pascual T, Fernandez-Martinez A, Braso-Maristany F, Gomis RR, Perou CM, et al. Clinical implications of the non-luminal intrinsic subtypes in hormone receptor-positive breast cancer. Cancer Treat Rev. (2018) 67:63–70. doi: 10.1016/j.ctrv.2018.04.015
27. Fumagalli D, Venet D, Ignatiadis M, Azim HA Jr, Maetens M, Rothe F, et al. RNA sequencing to predict response to neoadjuvant anti-HER2 therapy: a secondary analysis of the NeoALTTO randomized clinical trial. JAMA Oncol. (2016) 3:227–34. doi: 10.1001/jamaoncol.2016.3824
28. Beitsch P, Whitworth P, Baron P, Rotkis MC, Mislowsky AM, Richards PD, et al. Pertuzumab/trastuzumab/CT versus trastuzumab/CT therapy for HER2+ breast cancer: results from the prospective neoadjuvant breast registry symphony trial (NBRST). Ann Surg Oncol. (2017) 24:2539–46. doi: 10.1245/s10434-017-5863-x
29. Parker JS, Mullins M, Cheang MC, Leung S, Voduc D, Vickery T, et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol. (2009) 27:1160–7. doi: 10.1200/JCO.2008.18.1370
30. The Cancer Genome Atlas N, Koboldt DC, Fulton RS, McLellan MD, Schmidt H, Kalicki-Veizer J, et al. Comprehensive molecular portraits of human breast tumours. Nature. (2012) 490:61. doi: 10.1038/nature11412
31. Fasching PA, Hartkopf AD, Gass P, Haberle L, Akpolat-Basci L, Hein A, et al. Efficacy of neoadjuvant pertuzumab in addition to chemotherapy and trastuzumab in routine clinical treatment of patients with primary breast cancer: a multicentric analysis. Breast Cancer Res Treat. (2019) 173:319–28. doi: 10.1007/s10549-018-5008-3
Keywords: breast cancer, real-world data, neoadjuvant, pertuzumab, trastuzumab
Citation: Díaz-Redondo T, Lavado-Valenzuela R, Jimenez B, Pascual T, Gálvez F, Falcón A, Alamo MdC, Morales C, Amerigo M, Pascual J, Sanchez-Muñoz A, González-Guerrero M, Vicioso L, Laborda A, Ortega MV, Perez L, Fernandez-Martinez A, Chic N, Jerez JM, Alvarez M, Prat A, Ribelles N and Alba E (2019) Different Pathological Complete Response Rates According to PAM50 Subtype in HER2+ Breast Cancer Patients Treated With Neoadjuvant Pertuzumab/Trastuzumab vs. Trastuzumab Plus Standard Chemotherapy: An Analysis of Real-World Data. Front. Oncol. 9:1178. doi: 10.3389/fonc.2019.01178
Received: 14 May 2019; Accepted: 18 October 2019;
Published: 05 November 2019.
Edited by:
Takayuki Ueno, Cancer Institute Hospital of Japanese Foundation for Cancer Research, JapanReviewed by:
Alessandro Igor Cavalcanti Leal, Johns Hopkins Medicine, United StatesShigehira Saji, Fukushima Medical University, Japan
Copyright © 2019 Díaz-Redondo, Lavado-Valenzuela, Jimenez, Pascual, Gálvez, Falcón, Alamo, Morales, Amerigo, Pascual, Sanchez-Muñoz, González-Guerrero, Vicioso, Laborda, Ortega, Perez, Fernandez-Martinez, Chic, Jerez, Alvarez, Prat, Ribelles and Alba. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nuria Ribelles, bnVyaWFyaWJlbGxlc0B1bWEuZXM=