
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 26 September 2019
Sec. Women's Cancer
Volume 9 - 2019 | https://doi.org/10.3389/fonc.2019.00918
This article is part of the Research TopicQuality of Life in Breast Cancer Patients and SurvivorsView all 14 articles
 Wanderson Divino Nilo dos Santos1
Wanderson Divino Nilo dos Santos1 Gabriel Dutra de Jesus Siqueira1
Gabriel Dutra de Jesus Siqueira1 Wagner Rodrigues Martins2
Wagner Rodrigues Martins2 Amilton Vieira2
Amilton Vieira2 Raquel Machado Schincaglia3
Raquel Machado Schincaglia3 Paulo Gentil1
Paulo Gentil1 Carlos Alexandre Vieira1*
Carlos Alexandre Vieira1*The aim of this study was to evaluate the reliability and agreement between the test and retest of the 10-repetition maximum (10-RM) test for leg press and bench press in breast cancer survivors (BCS). Thirty-one BCS participated in this study, age 54.87 ± 5.7 years. All performed 10-RM tests and retests for the leg press 45° and the bench press. For reliability analyses, an intraclass coefficient correlation (ICC) and coefficient of variation (CV) were performed. The limits of agreement were calculated using a Bland-Altman plot with 95% CIs. For absolute and relative error of measurement, we used standard error of measurement and minimally detectable change. The result showed a high reliability for the bench press and leg press; ICC of 0.94 and 0.98, respectively. CV was <10% for both exercises. The systematic error were 1.5 kg (10%) and 6.1 (8%) for the bench press and leg press, respectively. The standard errors of measurements were 0.96 kg (6.08%) and 4.11 kg (5.27%) for the bench press and leg press, respectively. The minimally detectable changes were 2.72 kg (17.20%) and 5.62 kg (7.21%) for the bench press and leg press, respectively. In breast cancer survivors, the muscular strength measurement for the 10-RM test showed a high to very high rate of reliability and agreement, with acceptable error of measurement.
The assessment of muscle strength has been used to monitor and prescribe strength training (1). Muscular strength has been associated with high level of functional capacity and to decrease the risk of death from all natural causes (2, 3). The evaluation of muscle strength in breast cancer survivors (BCS) is a significant issue, because breast cancer (BC) treatment could reduce muscle strength after surgery and it may persist over the long-term (4). Therefore, in rehabilitation settings, the assessment of muscular strength is an important strategy to guide exercise prescription in these patients (5, 6).
Muscular strength loss in BCS is one of the side effects of BC treatment (surgery, chemotherapy, and radiotherapy), that could be explained by multiple factors such as: fatigue; lymphedema; decreased in shoulder, elbow, and wrist mobility; pain in the shoulder joint; and psychological changes such as kinesiophobia (7–13). These conditions could interfere with the reliability of maximum force tests and the strength outcomes during resistance training (14). In addition, these side effects of BC treatment pose a challenge for health professionals who work with resistance training for BC patients or survivors.
The one-repetition maximum test (1-RM) is considered the “gold standard” to measure maximum muscle strength in a non-laboratory setting. The 1-RM test is safe and has been applied in studies with BCS and BC patients (15–17). However, there is a lack of data regarding the reliability of this measurement within this population. To our knowledge, a single study presented only the coefficient of variation (CV) data for the bench press and leg press (18). Moreover, the 1-RM receive some criticism during a rehabilitation scenario such as risk of injury (19).
As an alternative to the 1-RM test, some studies with BCS used predictive formulas according to the results of multiple repetition tests (5-10RM) to estimate the maximum strength by 1-RM (20–23). Another method to estimate dynamic muscle strength is the repetition maximum test based on a goal of repetitions, as in the 10-RM test. The 10-RM test has been used to evaluate the load achieved in resistance training (RT) in different populations (24–30). Therefore, taking into consideration the characteristics of BCS, it seems that there is a natural concern with muscular strength tests for upper limbs, and maybe that could interfere on reliability of measurement. For this reason, it is possible that muscular strength for lower limbs could be more reliable than upper limbs. In addition, there is little information on the data of reliability and agreement of muscular strength tests in BCS, thus the performance of reliability studies is necessary.
The objective of this study was therefore to evaluate the reliability and agreement between the test and retest of the 10-RM test in upper and lower limbs in BCS. Our hypothesis was that the 10-RM test is reliable, and that the reliability is higher for the lower limbs.
In this reliability and agreement study, 31 BCS were included between February and October 2017. The BCS were contacted via phone calls and face-to-face interactions at the Mastology and Oncology Ambulatory of the University Hospital of the Federal University of Goias, Brazil. The eligibility criteria were: (1) confirmed BC stages I to III; (2) between 40 and 65 years old; (3) being in menopause (31); (4) not involved in any regular exercise program for the last 6 months; (5) completed cancer-related therapies including surgery, chemotherapy and/or radiotherapy at least 6 months prior to enrolling; (6) currently undergoing hormone therapy (tamoxifen or aromatase inhibitor); (7) received medical clearance for exercise training. Patients were excluded from the study if they had musculoskeletal limitations that could compromise exercise performance and/or any uncontrolled chronic disease that could represent a risk to their health.
The study was approved by Research Ethics Committee of the Federal University of Goias (CAAE: 50717115.4.0000.5083), and by the Research Ethics Committee of the Clinical Hospital of the Federal University of Goias (CAAE: 50717115.4.3001.5078). All participants provided written consent.
After a measure of body composition, the participants answered medical history and sociodemographic questionnaire and the International Physical Activity Questionnaire (IPAQ—short version) (32). They then performed the 10-RM test at 2 different days within 2– 4 days in between. At day 1, the participants were familiarized with Leg press 45° and Bench press exercises and then performed the 10-RM test (Figure 1).
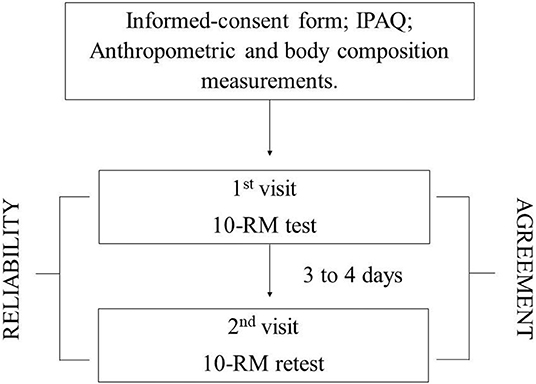
Figure 1. Experimental design. IPAQ, International Physical Activity Questionnaire; 10-RM, 10-repetition maximum.
Body mass index (BMI) was calculated based on body mass and height [BMI = weight (kg)/height squared (m2)]. Fat and lean mass were assessed using dual energy X-ray absorptiometry (DXA) (General Electric Healthcare® model, Madison, WI, USA). Data were analyzed using GE Medical Systems Lunar™ software. A professional technician performed the assessments of DXADuring the DXA, participants remained in a supine position with their lower limbs relaxed, and the upper limbs were positioned along the body with forearms pronated. DXA's were calibrated and tested as recommended by the manufacturer. After analysis of the entire body area, the total body mass, lean body mass and fat mass were registered.
The 10-RM test and retests were performed by the leg press 45° (Rocha, Leg Press 45°, Goias, Brazil) and bench press exercises with free-weight, plate-loaded (Supplementary Material). Both exercises techniques followed the recommendation from the National Strength and Conditioning Association (NSCA) (33). During the 10-RM test and retest, the participants were informed and supervised by two experienced exercise science professionals. The same exercise science professionals supervised the measurements. The participants had three to five 10-RM attempts for each exercise.
The warm-up consisted of one set of 10 repetitions with 50% of the estimated 10-RM load, by rating of perceived exertion 5–6 (0–10) in the first day. For leg press, the warm-up represented ~30–40% of their body mass. For bench press, we chose to use only the weight of the barbell (the barbell weighted 6 kg) to perfume the warm-up on the first day. The load used to perform the warm-up during the 10-RM retest was based on the maximum load achieved on the first day (10-RM test).
The 10-RM load was determined if they were able to complete the 10th repetition but not be able to perform the 11th repetition. If the volunteer were able to performed more than 10 repetitions, the load was increased by 5–10%. The resting interval between each attempt was 3 min, and the resting interval between exercises was 5 min. The cadence was not controlled, but participants were oriented to perform the concentric phase as fast as possible but control the eccentric phase. Leg press 45° was performed first, followed by the bench press. All participants performed the bench press until touching the barbell on the sternum/breast. The 10-RM retest was performed 3–4 days later, using the maximum load achieved on the 10-RM test as reference to perform the first attempt (34).
Descriptive statistics were presented as mean and standard deviation (SD). The intraclass coefficient correlation (ICC) and coefficient of variation (CV = SD divided by mean of test and retest × 100) was used for evaluation of reliability (35). The ICC form used was a two-way mixed effect, mean of k measurements and consistency agreement (36). The ICC and CV are present as mean and 95% of confidential interval (CI). The analyses of measurement error, absolute and relative, of the 10-RM test and retest was also investigated using the standard error of measurement [(SEM); SEM absolute = SD of the mean test-retest score divided by the square root of 1—ICC; SEM relative = SEM absolute score divided by mean test-retest scores and multiplying by 100] and minimally detectable change [(MDC); MDC absolute = 1.96 × the square root of 2 × SEM; MDC relative = MDC absolute score divided by mean of test-retest scores and multiplying by 100] (37). In addition, the limits of agreement were calculated using a Bland–Altman plot with 95% CIs (38). The Munro's classification of reliability was used to interpret the ICC coefficients: 0.50–0.69 reflects moderate correlation; 0.70–0.89 reflects high correlation; and 0.90–1.00 indicates very high correlation. Statistical analyses were performed using MedCalc Software (version 18.11.6) and Statistical Package for the Social Sciences Software (version 22).
The sociodemographic, cancer treatment status, and anthropometric characteristics of the participants are presented in Table 1.
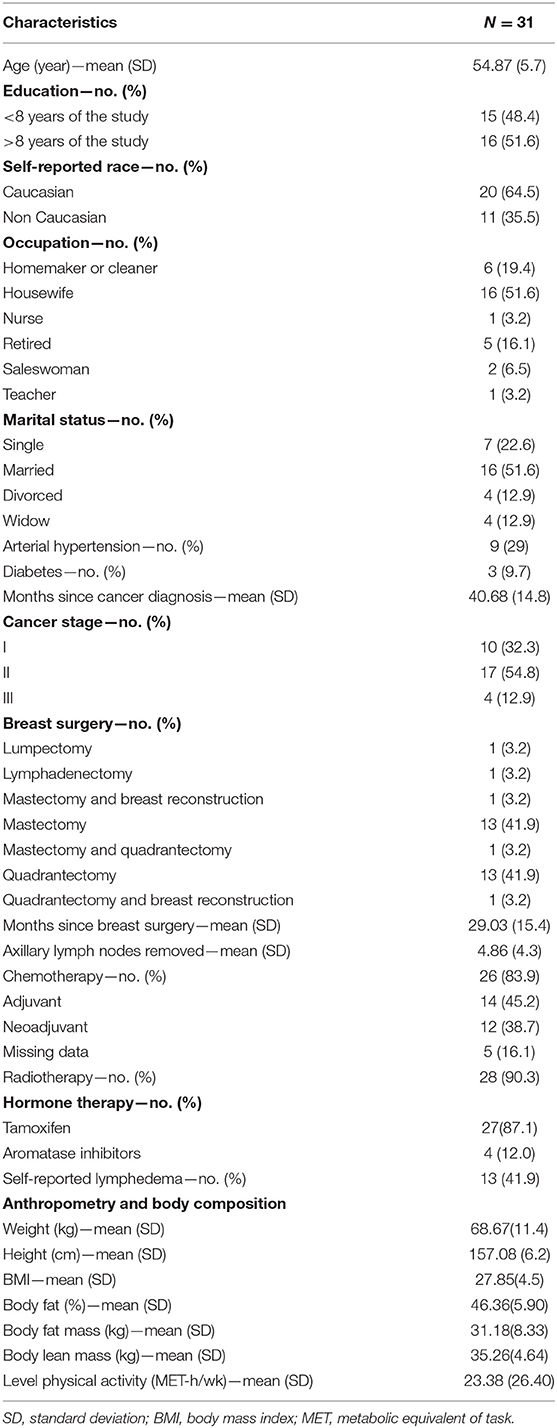
Table 1. Characteristics.
The comparison between 10-RM test and retest showed high to very high reliability for the leg press 45° and bench press. For the leg press 45° and bench press exercises the ICC were 0.98 and 0.94, respectively. CV was below 10% for both exercises. The results of reliability are presented in Table 2.

Table 2. Analysis of reliability and agreement between 10-RM test and retest.
The agreement between the 10-RM test and retest demonstrated that the results from the retest showed higher load than the test situation performed at day 1 (systematic bias values in Figures 2A,B are positives because the analysis were performed with 10-RM retest as first method and 10-RM test as second method for to build the Bland-Altman plots). The Bland-Altman plots (Figure 2) showed the mean difference with 95% IC limits of agreement.
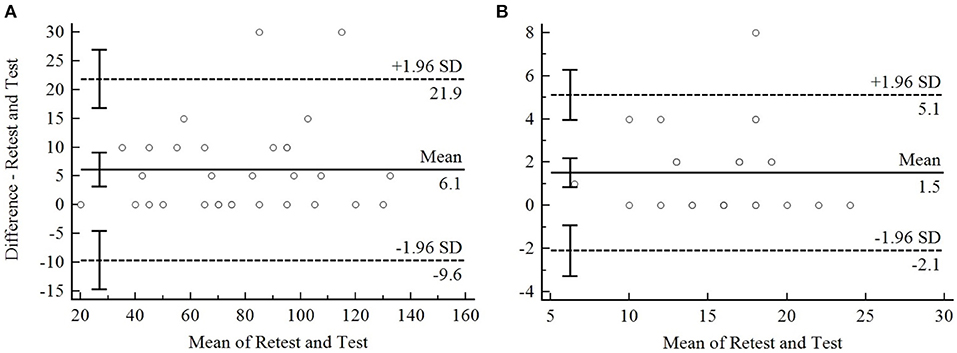
Figure 2. Bland-Altman plot of 10-RM for the leg press 45° (A) and the bench press (B). The dotted line represent the limits of agreement upper and lower boundary. The continue line on the center of plot represent the systematic bias. The continue line on the Y axis represent the mean difference between 10-RM retest and test, and on the X axis represent the mean of 10-RM retest and test.
The relative difference between the test and the retest was predicted in 8.3% (limits of agreement for upper and lower boundary 28 and −11%) and 10.3% (limits of agreement for upper and lower boundary 34 and −13%) for the leg press 45° and the bench press, respectively.
The relative and absolute SEM and MDC are presented in Table 2.
This study aimed to evaluate the reliability and agreement between the 10-RM test and retest for the leg press 45° and bench press exercises in BCS. We found a high to very high rate of reliability and agreement with lower and acceptable CV (CV < 10%), SEM (absolute and relative) and MDC (absolute and relative) between the 10-RM test and retest for both the leg press 45°. and bench press However, a higher value was found in the 10-RM retest situation, for both exercises. To our knowledge, this study is the first to evaluate the 10-RM test reliability in BCS, and the results suggest that 10-RM test could be used to measure muscular strength.
In general, a few studies have previously reported the reliability of test and retest 10-RM. In older people, Farinatti et al. (27) described high reliability of the 10-RM test for the dumbbell bench press (ICC 0.90; typical error 1.61 kg) and knee extension (ICC 0.96; typical error 2.01 kg) in elderly healthy women (68 ± 4 years old). Farinatti et al. (39) reported a high ICC for the barbell bench press in young (22 ± 2 years old) and elderly women (69 ± 7 years old) (0.91 and 0.90, respectively). For the leg press 45°, a high ICC (0.99) was reported in young healthy people (24 ± 3 years old) (40). Monteiro et al. (41) also reported a high ICC for the leg press 45° (0.92) and the bench press (0.90) in adult women (37.6 ± 1.7 years old). Our study found a similar reliability to those studies. Therefore, it seems that the 10-RM test reliability for BCS is similar to that of healthy individuals of different ages.
The CV of 10-RM test showed be <10% for lower and upper limbs. That was similar compare to 1-RM in BCS (18). Winter-Stone et al. (18) reported CV of the 6.6 and 7.5% for the leg press and chest press, respectively. We found a similar CV for the leg press 45° and bench press for 10-RM, 5.87 and 7.27%, respectively. Moreover, our results suggest that lower limbs have a better reliability than upper limb exercise, as we hypothesized. It could be explain by lower capacity of lifting for upper limbs compare to lower limbs, this may be result of sides effects of breast cancer treatments.
The 10-RM retest achieved higher load than 10-RM test situation, which may suggest some training effects either in technique or muscle strength of the first exercise test. A repeated strength measurement could provide a process of the learning of task, improving the ability/skill to perform the movement. Bernardi et al. (42) showed that skill acquisition to perform maximal voluntary contraction allows better control of neuromuscular system which could provide higher force generation through the trials. Grosicki et al. (43) also found higher value of 1-RM in the second trial than the first trial of assessment in young adults and older people, women and men, for leg press, leg extension and biceps curl. The same behavior was observed by Amarante do Nascimento et al. (44). They found that the second day of testing was higher than first day, but similar with the third day in 1-RM load for bench press and leg extension in elderly women (65 ± 4 years old) (44). Thus, the muscle strength values could be reached in the second or third trial of measurement.
The 10-RM test could be useful in the real word for prescribing or monitoring the load of the training. The use of percentage of 1-RM test may present a large variability in the number of repetition performance. Grosicki et al. (43) showed that using 60% and 80% of 1-RM test the participants were able to perform 28.8 (±9.2)/23.3 (± 16.3) and 17 (±6.5)/12.8 (±7.8) repetitions in younger and older women, respectively. Hence, the session of training would be high or low effort, if use the percentage of 1-RM test. Therefore, it seems that using the load reached from 10-RM test could be more precisely to prescribe and monitor the number of repetitions during the training session, and that may be one advantages of 10-RM test compared to 1-RM test. Another advantage of 10RM test could be a better perception of safety and acceptance in BCS, since there have been reported knesiohpobia, fear of movement (11, 45). In addition, repetition to failure as 10-RM might be used to predict 1-RM loads for the bench press/chest press (46–48) and leg press 45°/horizontal (47–49), with a low error of measurement. However, we did not investigate the accuracy of the 10-RM load to predict a 1-RM load in BCS. Future studies could investigate the accuracy of the 10-RM test to predict a 1-RM load in BC patients and BCS.
The study has important strengths. The tests were supervised by two experienced exercise physiologists/professionals that provided better control of the 10-RM test and guaranteed the safety and confidence for the participants to perform higher load, and the homogeneity of the tests. One limitation of the present study included the lack of assessment of shoulder range of motion during the bench press test. However, we think this limitation was eliminated by the experienced physiologists.
In conclusion, muscular strength measurement using 10-RM test has a good to excellent rate of reliability and agreement, with acceptable error of measurement. Due to lack of information about the reliability of 1-RM test in BCS, 10-RM test could be an interesting alternative for diagnosis and prescription in this population. Therefore, the 10-RM test may be used to evaluate the muscular strength in BCS. The new studies with BC patients and BCS could report the reliability of the maximum force production on isoinertial exercises.
The datasets generated for this study are available on request to the corresponding author.
The studies involving human participants were reviewed and approved by Research Ethics Committee of the Federal University of Goias (CAAE: 50717115.4.0000.5083), and by the Research Ethics Committee of the Clinical Hospital of the Federal University of Goias (CAAE: 50717115.4.3001.5078). The patients/participants provided their written informed consent to participate in this study.
WS and CV performed the study concept and design. WS and GS supervised the muscle assessments. WS, RS, and WM conducted the analyses. WS wrote the original draft of the manuscript. AV, WM, PG, and CV wrote, reviewed, and edited the manuscript.
PG receives a Research Grant from CNPq (304435/2018-0).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.00918/full#supplementary-material
1. Kraemer WJ, Ratamess NA. Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc. (2004) 36:674–88. doi: 10.1249/01.MSS.0000121945.36635.61
2. Ruiz JR, Sui X, Lobelo F, Morrow JR, Jackson AW, Sjöström M, et al. Association between muscular strength and mortality in men: prospective cohort study. BMJ. (2008) 337:a439. doi: 10.1136/bmj.a439
3. Tanimoto Y, Watanabe M, Sun W, Sugiura Y, Tsuda Y, Kimura M, et al. Association between sarcopenia and higher-level functional capacity in daily living in community-dwelling elderly subjects in Japan. Arch Gerontol Geriatr. (2012) 55:e9–13. doi: 10.1016/j.archger.2012.06.015
4. Hayes SC, Rye S, Battistutta D, DiSipio T, Newman B. Upper-body morbidity following breast cancer treatment is common, may persist longer-term and adversely influences quality of life. Health Qual Life Outcomes. (2010) 8:92. doi: 10.1186/1477-7525-8-92
5. Feigenbaum MS, Pollock ML. Prescription of resistance training for health and disease. Med Sci Sports Exerc. (1999) 31:38–45. doi: 10.1097/00005768-199901000-00008
6. Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, et al. American college of sports medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. (2010) 42:1409–26. doi: 10.1249/MSS.0b013e3181e0c112
7. Caro-Moran E, Fernandez-Lao C, Diaz-Rodriguez L, Cantarero-Villanueva I, Madeleine P, Arroyo-Morales M. Pressure pain sensitivity maps of the neck-shoulder region in breast cancer survivors. Pain Med. (2016) 17:1942–52. doi: 10.1093/pm/pnw064
8. Ewertz M, Jensen AB. Late effects of breast cancer treatment and potentials for rehabilitation. Acta Oncol. (2011) 50:187–93. doi: 10.3109/0284186X.2010.533190
9. Hayes S, Battistutta D, Newman B. Objective and subjective upper body function six months following diagnosis of breast cancer. Breast Cancer Res Treat. (2005) 94:1–10. doi: 10.1007/s10549-005-5991-z
10. Lee TS, Kilbreath SL, Refshauge KM, Herbert RD, Beith JM. Prognosis of the upper limb following surgery and radiation for breast cancer. Breast Cancer Res Treat. (2008) 110:19–37. doi: 10.1007/s10549-007-9710-9
11. Lee D, Hwang JH, Chu I, Chang HJ, Shim YH, Kim JH. Analysis of factors related to arm weakness in patients with breast cancer-related lymphedema. Support Care Cancer. (2015) 23:2297–304. doi: 10.1007/s00520-014-2584-6
12. Montague ED. Adaptation of irradiation techniques to various types of surgical procedures for breast cancer. Cancer. (1972) 29:557–60. doi: 10.1002/1097-0142(197203)29:3<557::AID-CNCR2820290304>3.0.CO;2-D
13. Nesvold I-L, Dahl AA, Løkkevik E, Marit Mengshoel A, Fosså SD. Arm and shoulder morbidity in breast cancer patients after breast-conserving therapy versus mastectomy. Acta Oncol. (2008) 47:835–42. doi: 10.1080/02841860801961257
14. Nuzzo JL, Taylor JL, Gandevia SC. CORP: Measurement of upper and lower limb muscle strength and voluntary activation. J Appl Physiol. (2019) 126:513–43. doi: 10.1152/japplphysiol.00569.2018
15. Battaglini C, Bottaro M, Dennehy C, Rae L, Shields E, Kirk D, et al. The effects of an individualized exercise intervention on body composition in breast cancer patients undergoing treatment. São Paulo Med J. (2007) 125:22–8. doi: 10.1590/S1516-31802007000100005
16. Schmitz KH, Ahmed RL, Hannan PJ, Yee D, KH S, RL A, et al. Safety and efficacy of weight training in recent breast cancer survivors to alter body composition, insulin, and insulin-like growth factor axis proteins. Cancer Epidemiol Biomarkers Prev. (2005) 14:1672–80. doi: 10.1158/1055-9965.EPI-04-0736
17. Schmitz KH, Troxel AB, Cheville A, Grant LL, Bryan CJ, Gross CR, et al. Physical activity and lymphedema (the PAL trial): assessing the safety of progressive strength training in breast cancer survivors. Contemp Clin Trials. (2009) 30:233–45. doi: 10.1016/j.cct.2009.01.001
18. Winters-Stone KM, Dobek J, Bennett JA, Nail LM, Leo MC, Schwartz A. The effect of resistance training on muscle strength and physical function in older, postmenopausal breast cancer survivors: a randomized controlled trial. J Cancer Surviv. (2012) 6:189–99. doi: 10.1007/s11764-011-0210-x
19. Pollock ML, Carroll JF, Graves JE, Leggett SH, Braith RW, Limacher M, et al. Injuries and adherence to walk/jog and resistance training programs in the elderly. Med Sci Sports Exerc. (1991) 23:1194–200. doi: 10.1249/00005768-199110000-00014
20. Courneya KS, McKenzie DC, Mackey JR, Gelmon K, Reid RD, Friedenreich CM, et al. Moderators of the effects of exercise training in breast cancer patients receiving chemotherapy: a randomized controlled trial. Cancer. (2008) 112:1845–53. doi: 10.1002/cncr.23379
21. Courneya KS, McKenzie DC, Mackey JR, Gelmon K, Friedenreich CM, Yasui Y, et al. Effects of exercise dose and type during breast cancer chemotherapy: multicenter randomized trial. J Natl Cancer Inst. (2013) 105:1821–32. doi: 10.1093/jnci/djt297
22. Courneya KS, Mckenzie DC, Mackey JR, Gelmon K, Friedenreich CM, Yasui Y, et al. Subgroup effects in a randomised trial of different types and doses of exercise during breast cancer chemotherapy. Br J Cancer. (2014) 111:1718–25. doi: 10.1038/bjc.2014.466
23. De Luca V, Minganti C, Borrione P, Grazioli E, Cerulli C, Guerra E, et al. Effects of concurrent aerobic and strength training on breast cancer survivors: a pilot study. Public Health. (2016) 136:126–32. doi: 10.1016/j.puhe.2016.03.028
24. Barbalho M, Gentil P, Raiol R, Fisher J, Steele J, Coswig V. Influence of adding single-joint exercise to a multijoint resistance training program in untrained young women. J Strength Cond Res. (2018). doi: 10.1519/JSC.0000000000002624. [Epub ahead of print].
25. Barbalho M, Coswig VS, Steele J, Fisher JP, Paoli A, Gentil P. Evidence for an upper threshold for resistance training volume in trained women. Med Sci Sports Exerc. (2019) 51:515–22. doi: 10.1249/MSS.0000000000001818
26. de Salles BF, Maior AS, Polito M, Novaes J, Alexander J, Rhea M, et al. Influence of rest interval lengths on hypotensive response after strength training sessions performed by older men. J Strength Cond Res. (2010) 24:3049–54. doi: 10.1519/JSC.0b013e3181ddb207
27. Farinatti PTV, Geraldes AAR, Bottaro MF, Lima MVIC, Albuquerque RB, Fleck SJ. Effects of different resistance training frequencies on the muscle strength and functional performance of active women older than 60 years. J Strength Cond Res. (2013) 27:2225–34. doi: 10.1519/JSC.0b013e318278f0db
28. Jakobsen TL, Husted H, Kehlet H, Bandholm T. Progressive strength training (10 RM) commenced immediately after fast-track total knee arthroplasty: is it feasible? Disabil Rehabil. (2012) 34:1034–40. doi: 10.3109/09638288.2011.629019
29. Kim H-S, Kim D-G. Effect of long-term resistance exercise on body composition, blood lipid factors, and vascular compliance in the hypertensive elderly men. J Exerc Rehabil. (2013) 9:271–7. doi: 10.12965/jer.130010
30. Pinto CL, Botelho PB, Carneiro JA, Mota JF. Impact of creatine supplementation in combination with resistance training on lean mass in the elderly. J Cachexia Sarcopenia Muscle. (2016) 7:413–21. doi: 10.1002/jcsm.12094
31. WHO. Research on the menopause in the 1990s. Report of a WHO Scientific Group. Geneva World Heal Organ. (1996) 866, 1–107.
32. Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. International Physical Activity Questionnaire (IPAQ): study of validity and reliability in Brazil. Rev Bras Atividade Física Saúde. (2001) 6:5–18.
33. National Strength and Conditioning Association. Exercise Technique Manual for Resistance Training. 3rd ed. Champaign, IL: Human Kineticcs (2016).
34. Heyward VH, Gibson AL. Advanced Fitness Assessment and Exercise Prescription. 7th ed. Champaign, IL: Human Kineticcs (2014).
35. Atkinson G, Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sport Med. (1998) 26:217–38. doi: 10.2165/00007256-199826040-00002
36. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. (2016) 15:155–63. doi: 10.1016/j.jcm.2016.02.012
37. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. (2005) 19:231. doi: 10.1519/15184.1
38. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. (1999) 8:135–60. doi: 10.1177/096228029900800204
39. Farinatti PTV, da Silva NSL, Monteiro WD. Influence of exercise order on the number of repetitions, oxygen uptake, and rate of perceived exertion during strength training in younger and older women. J Strength Cond Res. (2013) 27:776–85. doi: 10.1519/JSC.0b013e31825d9bc1
40. Lattari E, Rosa Filho BJ, Fonseca Junior SJ, Murillo-Rodriguez E, Rocha N, Machado S, et al. Effects on volume load and ratings of perceived exertion in individuals advanced weight-training after transcranial direct current stimulation. J Strength Cond Res. (2018). doi: 10.1519/JSC.0000000000002434. [Epub ahead of print].
41. Monteiro WD, Simão R, Polito MD, Santana CA, Chaves RB, Bezerra E, et al. Influence of strength training on adult women's flexibility. J Strength Cond Res. (2008) 22:672–7. doi: 10.1519/JSC.0b013e31816a5d45
42. Bernardi M, Solomonow M, Nguyen G, Smith A, Baratta R. Motor unit recruitment strategy changes with skill acquisition. Eur J Appl Physiol Occup Physiol. (1996) 74:52–9. doi: 10.1007/BF00376494
43. Grosicki GJ, Miller ME, Marsh AP. Resistance exercise performance variability at submaximal intensities in older and younger adults. Clin Interv Aging. (2014) 9:209–18. doi: 10.2147/CIA.S55719
44. Amarante do Nascimento M, Borges Januário RS, Gerage AM, Mayhew JL, Cheche Pina FL, Cyrino ES. Familiarization and reliability of one repetition maximum strength testing in older women. J Strength Cond Res. (2013) 27:1636–42. doi: 10.1519/JSC.0b013e3182717318
45. Karadibak D, Yavuzsen T, Saydam S. Prospective trial of intensive decongestive physiotherapy for upper extremity lymphedema. J Surg Oncol. (2008) 97:572–7. doi: 10.1002/jso.21035
46. Dohoney P, Chromiak JA, Lemire D, Abadie BR, Kovacs C. Prediction of one repetition maximum (1-rm) strength from a 4-6 RM and a 7-10 RM submaximal strength test in healthy young adult males. J Exerc Physiol Online. (2002) 5:54–9.
47. Mayhew JL, Johnson BD, Lamonte MJ, Lauber D, Kemmler W. Accuracy of prediction equations for determining one repetition maximum bench press in women before and after resistance training. J Strength Cond Res. (2008) 22:1570–7. doi: 10.1519/JSC.0b013e31817b02ad
48. Reynolds JM, Gordon TJ, Robergs RA. Prediction of one repetition maximum strength from multiple repetition maximum testing and anthropometry. J Strength Cond Res. (2006) 20:584–92. doi: 10.1519/R-15304.1
Keywords: muscle strength, muscular measurement, strength training, resistance training, cancer
Citation: Santos WDNd, Siqueira GDdJ, Martins WR, Vieira A, Schincaglia RM, Gentil P and Vieira CA (2019) Reliability and Agreement of the 10-Repetition Maximum Test in Breast Cancer Survivors. Front. Oncol. 9:918. doi: 10.3389/fonc.2019.00918
Received: 26 June 2019; Accepted: 03 September 2019;
Published: 26 September 2019.
Edited by:
Jisun Kim, University of Ulsan, South KoreaReviewed by:
Justin Y. Jeon, Yonsei University, South KoreaCopyright © 2019 Santos, Siqueira, Martins, Vieira, Schincaglia, Gentil and Vieira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Alexandre Vieira, dmllaXJhY2ExMUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.