 Onoufrios Tsavaris1
Onoufrios Tsavaris1 Panagiota Economopoulou1
Panagiota Economopoulou1 Ioannis Kotsantis1
Ioannis Kotsantis1 Lazaros Reppas2
Lazaros Reppas2 Chrysanthi Avgerinou1
Chrysanthi Avgerinou1 Nikolaos Spathas1
Nikolaos Spathas1 Maria Prevezanou1
Maria Prevezanou1 Amanda Psyrri1*
Amanda Psyrri1*
- 1Section of Medical Oncology, Department of Internal Medicine, Faculty of Medicine, National and Kapodistrian University of Athens, Attikon University Hospital, Athens, Greece
- 22nd Radiology Department, University General Hospital “ATTIKON”, Medical School, National and Kapodistrian University of Athens, Athens, Greece
Chondrosarcoma is a rare malignancy characterized by the production of cartilage matrix, displaying heterogeneous histopathology and clinical behavior. Due to lack of effective treatment for advanced disease, the clinical management of metastatic chondrosarcoma is exceptionally challenging. Chondrosarcomas harbor molecular abnormalities, such as overexpression of platelet-derived growth factor receptor (PDGFR)-alpha and PDGFR-beta, which are required for cancer development, progression, and metastasis. Pazopanib is a potent and selective multitargeted tyrosine kinase inhibitor, which co-inhibits stem cell growth factor receptor (c-KIT), fibroblast growth factor receptor (FGFR), PDGFR, and vascular endothelial growth factor receptor (VEGFR) and has demonstrated clinical activity in patients with advanced previously treated soft tissue sarcoma. Herein, we describe the unique case of a patient with metastatic chondrosarcoma who derived clinical benefit from pazopanib after first-line chemotherapy failure.
Introduction
Chondrosarcomas are a heterogeneous group of malignant bone tumors that are commonly characterized by the production of chondroid (cartilaginous) matrix (1). The vast majority is conventional chondrosarcomas; rare subtypes include dedifferentiated, clear cell, and mesenchymal chondrosarcomas (2). Histologic grade is the most important indicator of clinical behavior and prognosis. Grade 3 chondrosarcomas are frequently metastatic, and prognosis is poor with surgical resection alone (3). The main metastatic site is the lung, while regional lymph nodes and liver are much less commonly involved (4).
The cornerstone of treatment for localized chondrosarcoma is surgical resection, which offers the only chance for cure. Chemotherapy is considered ineffective; however, it might be effective in the mesenchymal subtype and is of uncertain value in dedifferentiated chondrosarcoma (5). Several signaling pathways, such as hedgehog, non-receptor tyrosine kinase (Src), phosphatidylinositol-4,5-bisphosphate 3-kinase (PI3K)/serine/threonine-protein kinase (AKT)/mammalian target of rapamycin (mTOR), and angiogenesis are suggested to play an important role in chondrosarcoma (6). Among them, angiogenesis is a key biological phenomenon that plays a critical role in tumor formation, invasion and metastasis.
Pazopanib (Votrient, GW786034, GlaxoSmithKline) is a multi-tyrosine kinase inhibitor (TKI) that targets angiogenesis growth factor receptors, such as stem cell growth factor receptor (c-KIT), fibroblast growth factor receptor (FGFR), platelet-derived growth factor receptor, and vascular endothelial growth factor receptor (VEGFR). It has been shown to suppress chondrosarcoma growth in mice (7). Pazopanib has been approved for the treatment of metastatic soft tissue sarcoma after failure of anthracycline-based chemotherapy, based on a pivotal phase III trial, which demonstrated improved progression-free survival compared with placebo (8). Based on these considerations, we have tested the efficacy of standard pazopanib dose of 800 mg daily in a patient with metastatic chondrosarcoma who had disease progression following anthracycline-based chemotherapy.
Case Presentation
In May 2011, a 41-year-old Caucasian male was referred to the orthopedic department of our institution for evaluation of a 6-month left proximal humeral pain, increasing in severity over the last 2–3 weeks. His medical history was unremarkable and was under no medications at the time. He was an ex smoker and a social drinker and worked in constructions. Family history was notable for a grandfather with lung cancer and an aunt with breast cancer.
Upon physical examination, a limited range of motion of the left shoulder was noted (decreased flexion, extension, abduction, and external rotation). Plain radiograph of the left shoulder demonstrated a lytic lesion with intralesional calcifications and cortical remodeling, suggestive of a chondrosarcoma. MRI of the left shoulder confirmed this finding. Biopsy of the lesion was positive for grade 2–3 chondrosarcoma. A full diagnostic workup was carried out, including a CT of the chest and upper abdomen and a bone scan, which demonstrated increased uptake in the left upper arm but no additional bone lesions. Hematological and biochemical investigations were within normal limits.
In June 2011, the patient underwent a limb sparing surgical operation, and pathology was positive for conventional chondrosarcoma grade 2–3, that had destroyed the medullary and cortical portions of bone reaching into adjacent soft tissue. Distal bony resection margin and skin were both free of tumor infiltration. The patient did not receive any adjuvant therapy.
The patient remained free of disease for 4 years following surgery. In 2015, the patient complained of increasing pain in his left resected arm and shoulder. Imaging confirmed local recurrence. The patient subsequently underwent amputation of his left arm with resection of scapula. Pathology confirmed diagnosis of a grade 2/3 conventional chondrosarcoma. In August 2016, he started to experience significant substernal chest pain with shortness of breath and was admitted to the hospital. A CT scan of the chest revealed multiple pulmonary lesions compatible with metastases. The patient was discussed at the oncology tumor board and it was decided that chemotherapy should be administered. He was treated with chemotherapy combination of doxorubicin 20 mg/m2, Ifosfamide 2.5 g/m2, and Mesna 2.5 g/m2 IV on days 1–3 every 3 weeks. After 3 months of treatment, chemotherapy was discontinued due to disease progression, which included presence of new pulmonary nodules.
At that time, we decided to treat the patient with pazopanib as second-line treatment. The drug was well tolerated and after 6 months of treatment, the patient had partial response on imaging according to RECIST criteria (Figure 1), with improvement of symptoms. At the last follow-up in August 2017, clinical, biochemical, and imaging evaluation showed no evidence of disease progression. The patient continues to be on treatment with pazopanib. Written informed consent was obtained from the participant for the publication of this case report.
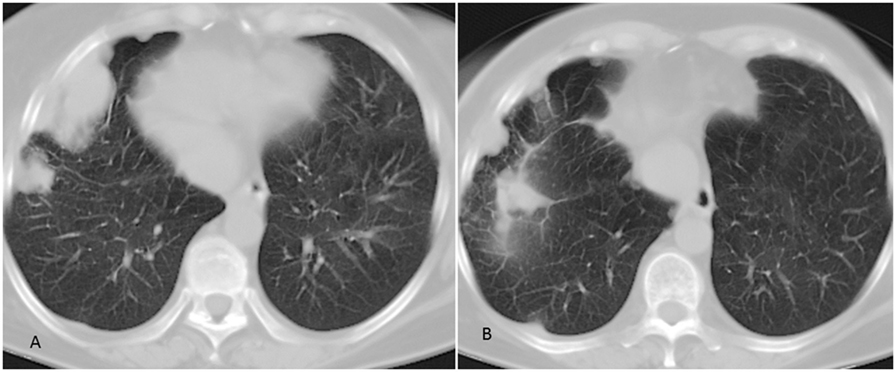
Figure 1. Chest CT scan of the patient. (A) Pulmonary lesions of the right lung. (B) Partial response of pulmonary lesions following 6 months of treatment with pazopanib.
Discussion
Due to limited efficacy of available treatment strategies, management of metastatic chondrosarcoma is intriguing. During the last decades, there has been no significant improvement in survival; furthermore, rarity of the disease hampers the conduction of large randomized trials. New therapeutic approaches are urgently needed, and current research focuses on elucidation of molecular events underlying the pathogenesis of this rare malignancy.
Angiogenesis is a hallmark pathway involved in cancer evolution, evasion, and metastasis and has been introduced as an important therapeutic target in the last two decades (9). Preclinical data have supported a role of angiogenesis in the pathogenesis of chondrosarcoma. Early studies have demonstrated production of VEGF in human chondrosarcoma cell lines (10). Chemokine CCL5 has been shown to mediate VEGF angiogenesis via inhibition of miR-200b through PI3K/Akt pathway in chondrosarcoma cells (11). In another study, protein hormone adiponectin promoted VEGF-A expression in human chondrosarcoma cell lines via PI3k, Akt, mTOR, and hypoxia-inducible factor-1a signaling cascades (12). In chondrosarcoma animal models, treatment with VEGFR2/PFGF-β/FGFR1 inhibitor SU668 resulted in tumor growth inhibition (7). On the other hand, combination of chemotherapeutic agent ET-743 and antiangiogenic protein plasminogen-related protein B has shown to be effective in reducing tumor necrosis in chondrosarcoma animal models (13).
In the case of our patient, angiogenesis TKI pazopanib resulted in objective response for more than 6 months, which was associated with clear improvement of the patient’s symptoms and general condition. Of note, the patient had received prior chemotherapy without any clinical benefit. In a recent report by Jones et al., among eight patients with chondrosarcoma who were treated with pazopanib in the context of a clinical trial, seven patients achieved prolonged disease stabilization for over 6 months (14).
There are two ongoing trials evaluating the efficacy of pazopanib in patients with chondrosarcomas. A phase II study that investigates the efficacy and safety of pazopanib in patients with unresectable or metastatic chondrosarcoma has completed recruitment, and results are eagerly awaited (NCT01330966). In addition, a phase II trial is evaluating pazopanib in patients with unresectable or metastatic solitary fibrous tumor and extraskeletal myxoid chondrosarcoma (NCT02066285). Regorafenib is another oral multikinase inhibitor, which targets angiogenic, stromal, and oncogenic RTKs and is currently being tested in a phase II study in patients with metastatic bone sarcomas (NCT02389244).
Concluding Remarks
In conclusion, chondrosarcoma is a rare bone malignancy with a diverse pattern of clinical behavior and remarkable resistance to chemotherapy or radiation. Current research focuses on elucidation of molecular events during tumorigenesis, with the ultimate goal to develop effective molecular targeted treatments. Herein, we describe the unusual case of a patient with metastatic chondrosarcoma who derived clinical benefit from pazopanib. Large randomized trials are warranted to confirm a role of pazopanib in chondrosarcoma treatment.
Author Contributions
OT reviewed the literature and wrote the paper. PE and IK collected the data and contributed in the preparation of the manuscript. CA, NS, and MP contributed in revision of the literature. LR prepared the figure. AP carried out critical interpretations and contributed in the final version of the paper. All the authors read and approved the final manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rozeman LB, Hogendoorn PC, Bovee JV. Diagnosis and prognosis of chondrosarcoma of bone. Expert Rev Mol Diagn (2002) 2(5):461–72. doi:10.1586/14737159.2.5.461
2. Angelini A, Guerra G, Mavrogenis AF, Pala E, Picci P, Ruggieri P. Clinical outcome of central conventional chondrosarcoma. J Surg Oncol (2012) 106(8):929–37. doi:10.1002/jso.23173
3. Fiorenza F, Abudu A, Grimer RJ, Carter SR, Tillman RM, Ayoub K, et al. Risk factors for survival and local control in chondrosarcoma of bone. J Bone Joint Surg Br (2002) 84(1):93–9. doi:10.1302/0301-620X.84B1.11942
4. Giuffrida AY, Burgueno JE, Koniaris LG, Gutierrez JC, Duncan R, Scully SP. Chondrosarcoma in the United States (1973 to 2003): an analysis of 2890 cases from the SEER database. J Bone Joint Surg Am (2009) 91(5):1063–72. doi:10.2106/JBJS.H.00416
5. Gelderblom H, Hogendoorn PC, Dijkstra SD, van Rijswijk CS, Krol AD, Taminiau AH, et al. The clinical approach towards chondrosarcoma. Oncologist (2008) 13(3):320–9. doi:10.1634/theoncologist.2007-0237
6. Bovee JV, Cleton-Jansen AM, Taminiau AH, Hogendoorn PC. Emerging pathways in the development of chondrosarcoma of bone and implications for targeted treatment. Lancet Oncol (2005) 6(8):599–607. doi:10.1016/S1470-2045(05)70282-5
7. Klenke FM, Abdollahi A, Bertl E, Gebhard MM, Ewerbeck V, Huber PE, et al. Tyrosine kinase inhibitor SU6668 represses chondrosarcoma growth via antiangiogenesis in vivo. BMC Cancer (2007) 7:49. doi:10.1186/1471-2407-7-49
8. van der Graaf WT, Blay JY, Chawla SP, Kim DW, Bui-Nguyen B, Casali PG, et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet (2012) 379(9829):1879–86. doi:10.1016/S0140-6736(12)60651-5
9. Ellis LM, Liu W, Ahmad SA, Fan F, Jung YD, Shaheen RM, et al. Overview of angiogenesis: biologic implications for antiangiogenic therapy. Semin Oncol (2001) 28(5 Suppl 16):94–104. doi:10.1016/S0093-7754(01)90287-8
10. Furumatsu T, Nishida K, Kawai A, Namba M, Inoue H, Ninomiya Y. Human chondrosarcoma secretes vascular endothelial growth factor to induce tumor angiogenesis and stores basic fibroblast growth factor for regulation of its own growth. Int J Cancer (2002) 97(3):313–22. doi:10.1002/ijc.1607
11. Liu GT, Chen HT, Tsou HK, Tan TW, Fong YC, Chen PC, et al. CCL5 promotes VEGF-dependent angiogenesis by down-regulating miR-200b through PI3K/Akt signaling pathway in human chondrosarcoma cells. Oncotarget (2014) 5(21):10718–31. doi:10.18632/oncotarget.2532
12. Lee HP, Lin CY, Shih JS, Fong YC, Wang SW, Li TM, et al. Adiponectin promotes VEGF-A-dependent angiogenesis in human chondrosarcoma through PI3K, Akt, mTOR, and HIF-alpha pathway. Oncotarget (2015) 6(34):36746–61. doi:10.18632/oncotarget.5479
13. Morioka H, Weissbach L, Vogel T, Nielsen GP, Faircloth GT, Shao L, et al. Antiangiogenesis treatment combined with chemotherapy produces chondrosarcoma necrosis. Clin Cancer Res (2003) 9(3):1211–7.
Keywords: pazopanib, metastatic chondrosarcoma, angiogenesis, vascular endothelial growth factor receptor, platelet-derived growth factor receptor
Citation: Tsavaris O, Economopoulou P, Kotsantis I, Reppas L, Avgerinou C, Spathas N, Prevezanou M and Psyrri A (2018) Clinical Benefit of Pazopanib in a Patient with Metastatic Chondrosarcoma: A Case Report and Review of the Literature. Front. Oncol. 8:45. doi: 10.3389/fonc.2018.00045
Received: 03 December 2017; Accepted: 13 February 2018;
Published: 01 March 2018
Edited by:
Anna Rita Migliaccio, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Antonio Rozzi, Istituto Neurotraumatologico Italiano Grottaferrata (Roma), ItalyDhiraj Kumar, University of Texas MD Anderson Cancer Center, United States
Copyright: © 2018 Tsavaris, Economopoulou, Kotsantis, Reppas, Avgerinou, Spathas, Prevezanou and Psyrri. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amanda Psyrri, cHN5cnJpMjM3JiN4MDAwNDA7eWFob28uY29t