 Jian Huang
Jian Huang Xinping Wang2†
Xinping Wang2† Zhirong Liu
Zhirong Liu- 1Department of Neurology, Xijing Hospital, Airforce Military Medical University, Xi'an, China
- 2Department of Geriatrics, Air Force 986 Hospital, Xi'an, China
- 3Department of Neurology, Xianyang First People's Hospital, Xianyang, China
- 4Department of Neurology, The Second People's Hospital of Shaanxi Province, Xi'an, China
- 5Department of Neurology, Xi'an Daxing Hospital, Xi'an, China
- 6Department of Neurology, Xi'an First Hospital, Xi'an, China
Background and aims: Exponential population aging has led to an increased prevalence of cognitive impairment worldwide. Hand grip strength, which may be associated with physical activity, could be a useful predictor of cognitive impairment. However, few studies have reported the association, if any, between hand grip strength and cognitive function.
Methods: We used data obtained from the National Health and Nutrition Examination Survey between 2011–2012 and 2013–2014 to investigate the association between hand grip strength and cognitive impairment. Cognitive impairment was assessed using the Consortium to Establish a Registry for Alzheimer's Disease (CERAD), animal fluency (AF), and digit symbol substitution test (DSST) scores. Cutoff values of CERAD < 5, AF < 14, and DSST < 34 were used to define cognitive impairment. In this cross-sectional study, we used odds ratios to determine the potential usefulness of hand grip strength for the prediction of cognitive impairment.
Results: This study included 2,623 participants aged ≥60 years. The DSST results showed that hand grip strength was associated with a low risk of cognitive impairment and that subgroup analysis showed that male sex, 60–69 years of age, and the Non-Hispanic (NH)-White, NH Black, and Asian were associated with a significantly low risk of cognitive impairment. The CERAD test results showed that 70–79 years of age and the NH White were significantly associated with a low risk of cognitive impairment. By following full adjustment, we did not observe statistically significant differences between hand grip strength and cognitive impairment based on the CERAD test. The AF test results showed that >80 years of age, female sex, and the NH White were associated with a significantly low risk of cognitive impairment. The most important finding is that a linear association lies between grip strength and cognitive impairment, as well as a sex-based linear association. Machine learning of the XGBoost model suggests that grip strength is one of the top two most important negative predictor variables.
Conclusion: We observed an inverse relationship between hand grip strength and cognitive impairment, which might suggest a shared underlying mechanism that needs to be further investigated using a large-scale prospective clinical trial to validate our findings.
Introduction
Neurological disorders are the leading cause of disability and the second leading cause of death worldwide. Cognitive impairment is prevalent worldwide, particularly in those aged ≥60 years (Feigin et al., 2020). Increases are expected globally as a result of population growth and aging, and cognitive decline warrants urgent attention from policymakers and governments (Carroll, 2019). Reportedly, 6.2 million Americans aged ≥65 years are diagnosed with Alzheimer's disease (AD), and 13.8 million Americans are expected to have AD by 2060 (Warren, 2022). Therefore, AD and cognitive decline are associated with a high socioeconomic burden in the United States (US), and the burden is expected to increase 2-fold to 3.3% of the population by 2060 (Matthews et al., 2019). Unfortunately, currently, early diagnosis and effective treatment of cognitive impairment are relatively limited (Piersol et al., 2018). Therefore, researchers and policymakers consider the prevention of cognitive impairment a more viable strategy (Liss et al., 2021).
Several studies have focused on the role of diet and physical activity (Frith and Loprinzi, 2017, 2018), as well as protective and risk factors in the prevention of cognitive impairment (Li et al., 2019; Dong et al., 2020b; Casagrande et al., 2021; Kim et al., 2021; Pereira et al., 2021). In view of the fact that hand grip strength may associate with physical activity, hand grip strength may also associate with cognitive function (Bohannon, 2019). Previous studies have reported a likely association between hand grip strength and cognitive abilities (Sternäng et al., 2016). However, another study observed no association between hand grip strength and cognitive function (Ritchie et al., 2016). A recent study that included elderly cancer survivors observed an association between hand grip strength and cognitive function in this patient population (Yang et al., 2018).
However, clinical findings that describe the association between hand grip strength and cognitive impairment remain inconsistent. Therefore, we extracted data from the National Health and Nutrition Examination Survey (NHANES) (2011–2012 and 2013–2014) to investigate the association between hand grip strength and cognitive impairment in elderly adults in the US. To the best of our knowledge, this is the first study that confirms the association between grip strength and cognitive impairment based on representative national data.
Materials and methods
Study population
We extracted data from the NHANES across two phases (2011–2012 and 2013–2014). The NHANES included cross-sectional nationally representative health examination surveys that are used to assess the health and nutritional status of the population in the US. The purpose of the information collected by NHANES was for health statistics. Several studies based on the NHANES data have been published in recent years (Flegal et al., 2005; Wong et al., 2019; Appiah et al., 2021). A total of 19,931 participants completed the survey in 2011–2012 (n = 9,756) and 2013–2014 (n = 10,175). Exclusion criteria were as follows: (a) <60 years of age (16,299 individuals), (b) inability to complete cognitive function tests (n = 695), and (c) inability to perform hand grip strength experiments (n = 314). Eventually, data from 2,623 participants were analyzed (Figure 1). Written informed consent was obtained from all participants and by the Research Ethics Review Board of the National Centre for Health Statistics. Informed consent was not required for the second phase of the study for analysis of the public database. This study is reported based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., 2007).
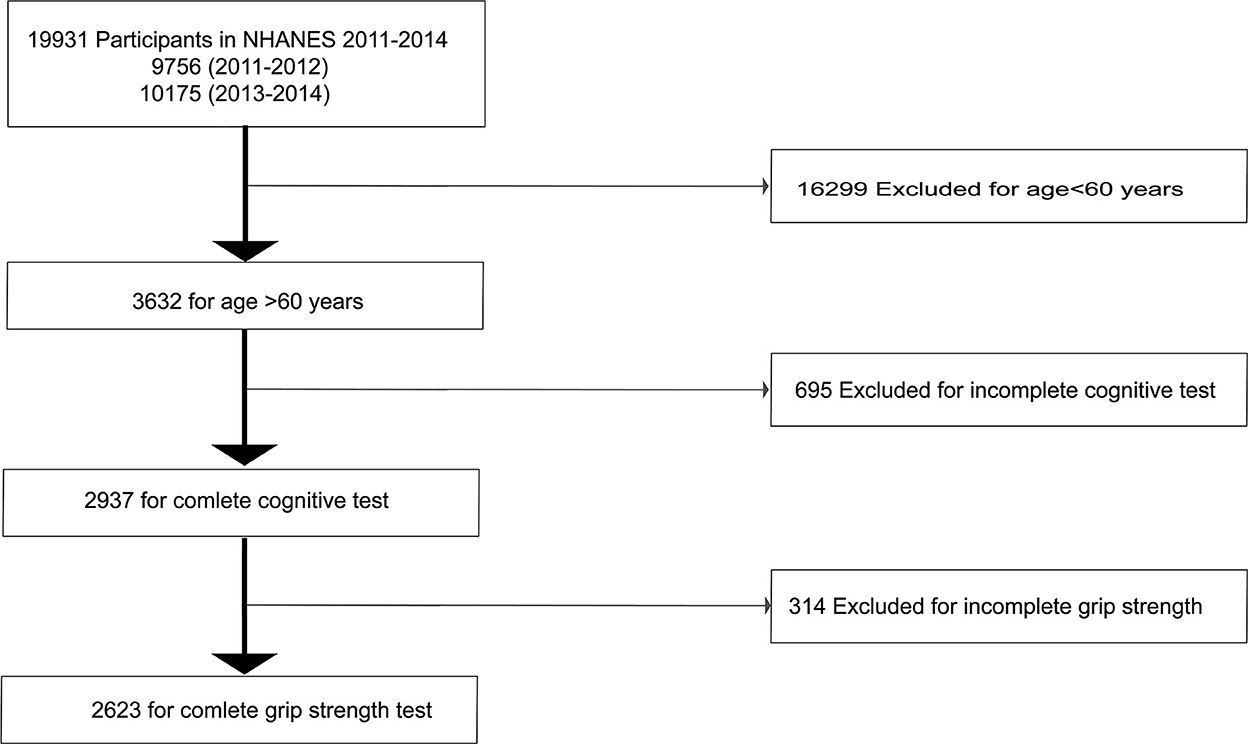
Figure 1. Flow chart showing the selection of study participants.
Primary exposure
We obtained a detailed protocol for the hand grip strength test from the NHANES Muscle Strength Procedures Manual (Yang et al., 2018). Briefly, a dynamometer was used for bilateral hand assessment. Participants were randomly assigned to grasp the dynamometer using the maximal strength possible, and each hand was tested three times. Participants who could not correctly grasp the dynamometer were excluded from the study, and we measured the combined grip strength (kg) (the sum of the largest reading from each hand).
Outcome variables
Cognitive function evaluation was performed at a mobile examination center. A series of tests were performed to assess participants' working memory, delayed recall, and verbal fluency. Participants consented to audio-record the testing throughout the assessment for quality purposes, and the score was approved by all participants.
The Consortium to Establish a Registry for Alzheimer's Disease (CERAD) test battery was used for the assessment of new learning, recognition memory, and delayed recall. Three consecutive learning trials were included in the CERAD-Word Learning test (Morris et al., 1989). After participants read 10 unrelated words aloud, they were required to recall the words. The sum of the three trial scores was 30. During the CERAD-Delayed Recall test (Sotaniemi et al., 2012; Dong et al., 2020a), participants were instructed to recall 10 words in the CERAD-Word Learning test after completing the other trials.
The animal fluency (AF) test, which measures participants' verbal fluency, involves naming as many animals as the participant can in 1 min (Prince et al., 2003). The digit symbol substitution test (DSST) was used to assess working memory, processing speed, and sustained attention. Participants were instructed to copy symbols in 133 boxes after 2 min. The correct matches were included in the total score (Brody et al., 2019).
Unfortunately, cutoffs for cognitive tests that can be used as a gold standard remain unavailable. Based on the historical literature, the 25th percentile of the scores is widely accepted as the cutoff value (Bailey et al., 2020). In the present study, the 25th percentile of the scores was CERAD < 5, AF < 14, and DSST < 34, respectively. Combined CERAD, AF, and DSST tests scores, a score of less than the 25th percentile of the scores on at least one of the CERAD, AF, and DSST tests, is considered as cognitive impairment.
Covariates
We extracted potential confounders, including sociodemographic factors, lifestyle, and health status from the previous literature.
Sociodemographic factors included sex, age, race, educational level, marital status, and the poverty-income ratio. The following age categories were used: 60–69, 70–79, and ≥80 years. Race was categorized into the following groups: Mexican American/other Hispanic, Non-Hispanic (NH)-White, NH-Black, NH-Asian, and other races. Educational level was classified as less than high school, high school, and above high school. The poverty–income ratio was calculated by dividing family (or individual) income by the poverty guidelines specific to the survey year and was categorized into <1 and >1. Marital status was classified into married/living with a partner, widowed/divorced/separated, and never married.
Lifestyle patterns were categorized based on personal habits, including alcohol consumption (12 alcoholic drinks/year), smoking (at least 100 cigarettes), and vigorous work activity (yes or no) (Fan et al., 2021). Health status was evaluated based on history of coronary heart disease, stroke, diabetes, hypertension, and high serum cholesterol levels. The body mass index (BMI) was classified into the following groups: <25, 25–30, and >30 kg/m2. Depression was assessed using the 9-question Patient Health Questionnaire. Based on the reports in the literature, scores ≥10 were defined as depression (Ge et al., 2020). Arm length, arm circumference, and waist circumference, which may be potential confounders of hand grip strength, were considered in the analysis.
Statistical analysis
Continuous variables are expressed as weighted mean ± standard deviation and were compared using an independent t-test. Categorical variables are expressed as weighted percentages and were compared using the chi-square test. A multivariate logistic regression model was established to determine the association between hand grip strength and cognitive impairment. The model was adjusted for sex, age, race, educational level, marital status, poverty-income ratio, alcohol consumption, smoking, vigorous work activity, BMI, depression, and a history of coronary heart disease, stroke, diabetes, hypertension, and high serum cholesterol levels. Furthermore, we performed subgroup analysis based on age, sex, and race. Finally, we constructed the XGBoost algorithm model to predict the relative importance of selected variables (grip strength, arm circumference, waist circumference, and arm length). We performed the XGBoost model to analyze the contribution of each variable to cognitive impairment.
All statistical analyses were performed using the R software (http://www.R-project.org) and Empowerstats (http://www.empowerstats.com, X&Y Solutions, Inc., USA). A full sample 4-year mobile examination center assessment weight was used to represent the survey among older adults. A two-sided test was used, and p < 0.05 was considered statistically significant.
Results
Characteristics of study participants
We analyzed the records of 2,623 participants aged ≥60 years in this study. Table 1 shows the overall characteristics of the study samples represented as quartiles of grip strength. We observed CERAD scores <5 in 20.61%, AF scores <14 in 20.33%, and DSST scores <34 in 13.61% of participants. In addition to a history of diabetes and high serum cholesterol levels, statistically significant differences were observed in most participants through quartiles of hand grip strength (p > 0.05). Furthermore, high hand grip strength was associated with male sex, 60–69 years of age, NH White race, married status/living with a partner, poverty-income ratio >1, higher educational levels, vigorous work activity, BMI > 30 kg/m2, alcohol consumption, smoking (at least 100 cigarettes), and a history of coronary heart disease. In contrast, low hand grip strength was associated with female sex, Asian race, never married status, less vigorous work activity, poverty-income ratio <1, BMI 25–30 kg/m2, a history of stroke, diabetes, hypertension, high serum cholesterol levels, and depression. Notably, arm length, arm circumference, and waist circumference were associated with hand grip strength.
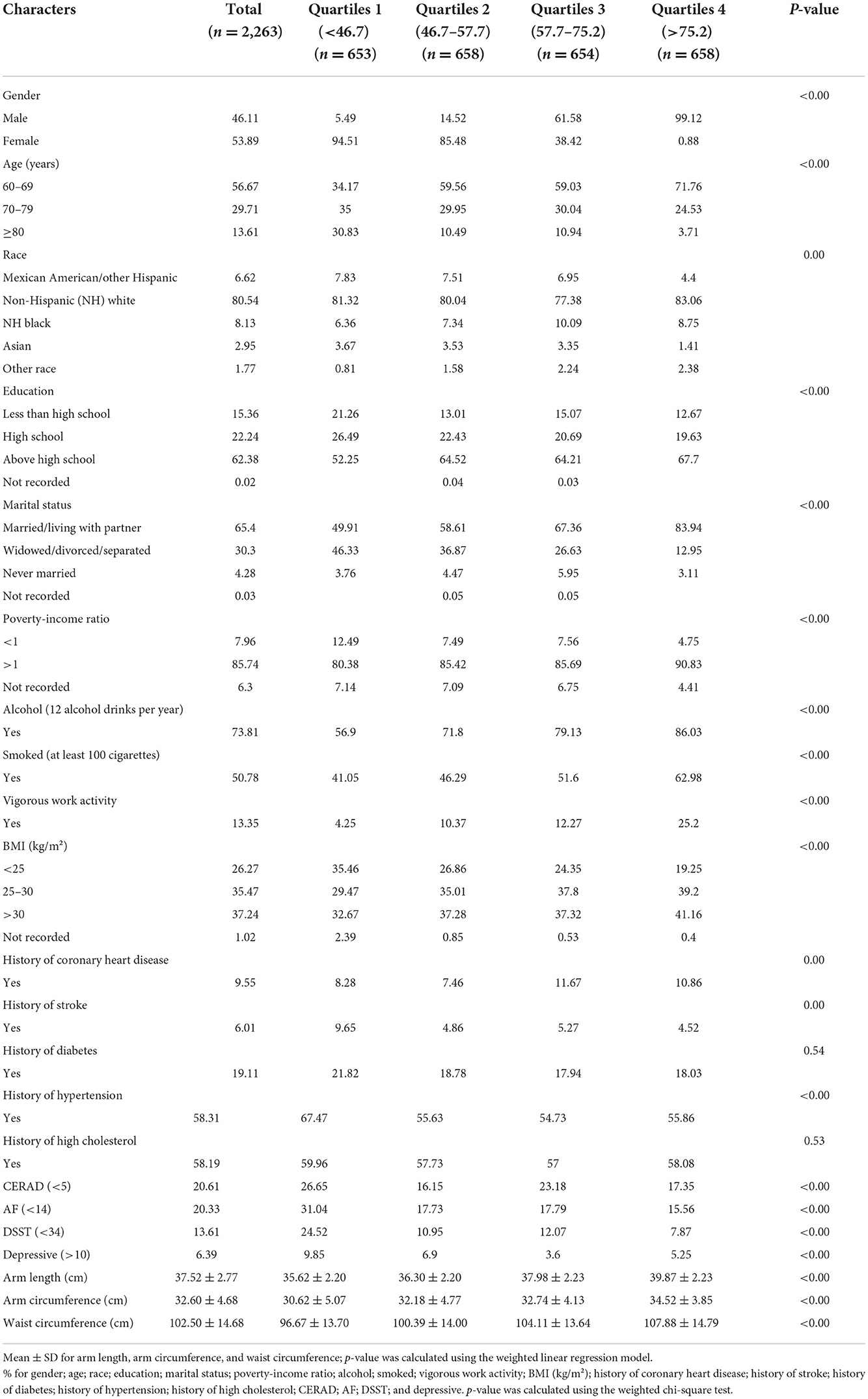
Table 1. General characteristics of participants (n = 2,623) stratified by grip strength (1–4, kg) in the NAHENS 2011–2014.
Association between hand grip strength and cognitive impairment based on the Consortium to Establish a Registry for Alzheimer's Disease test results
Table 2 shows the association between hand grip strength and cognitive impairment measured using the CERAD test. The non-adjusted model showed an odds ratio (OR) of 0.99 [95% confidence interval (CI) 0.99–1.00]. After adjustment for age, sex, and race, a statistically significant difference was observed between hand grip strength and a low risk of cognitive impairment (OR = 0.98, 95% CI 0.97–0.99) and CERAD in Q2–Q4 (Q2: OR = 0.63, 95% CI 0.47–0.85; Q3: OR = 0.68, 95% CI 0.49–0.95; Q4: OR = 0.52, 95% CI 0.35–0.77). However, following full adjustment, we did not observe statistically significant differences between hand grip strength and cognitive impairment.
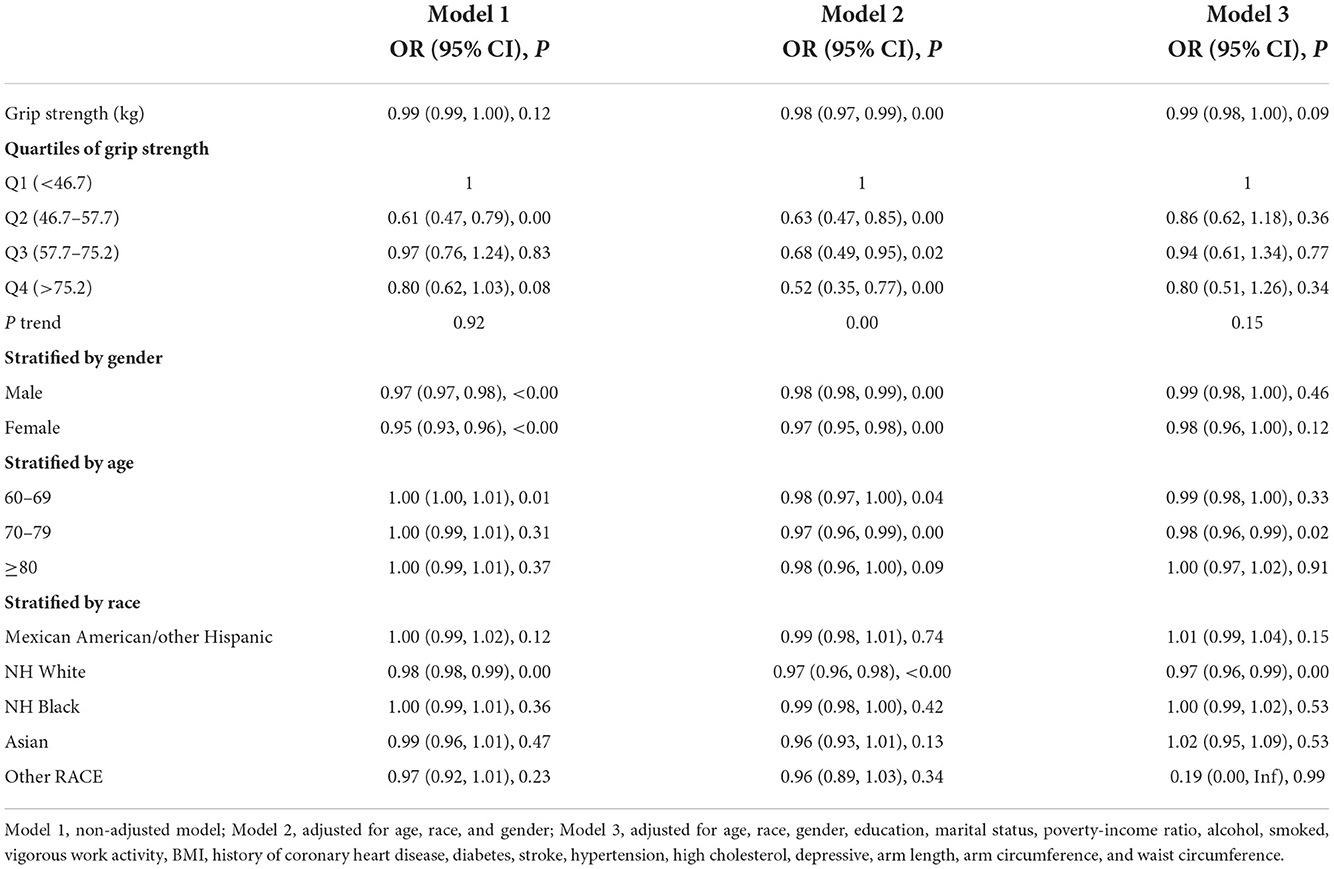
Table 2. Associations between grip strength (kg) and cognitive impairment (CERAD<5) (n = 2,623), NHANES 2011–2014.
Subgroup analysis revealed that 70–79 years of age (full adjustment: OR = 0.97, 95% CI 0.96–0.99) and NH White race (full adjustment: OR = 0.97, 95% CI 0.96–0.98) were associated with a significantly low risk of cognitive impairment. However, there were no statistically significant differences in sex after full adjustment.
Association between hand grip strength and cognitive impairment based on the AF test results
Table 3 shows the association between hand grip strength and cognitive impairment based on the AF test results. The non-adjusted model showed an OR of 0.98 (95% CI 0.98–0.99). After adjustment for age, sex, and race, a statistically significant difference was observed between hand grip strength and a low risk of cognitive impairment (OR 0.98, 95% CI 0.97–0.99) and AF in Q2–Q4 (Q2: OR = 0.67, 95% CI 0.51–0.86; Q3: OR = 0.63, 95% CI 0.47–0.86; Q4: OR = 0.53, 95% CI 0.36–0.76). However, following full adjustment, we did not observe statistically significant differences between hand grip strength and cognitive impairment.
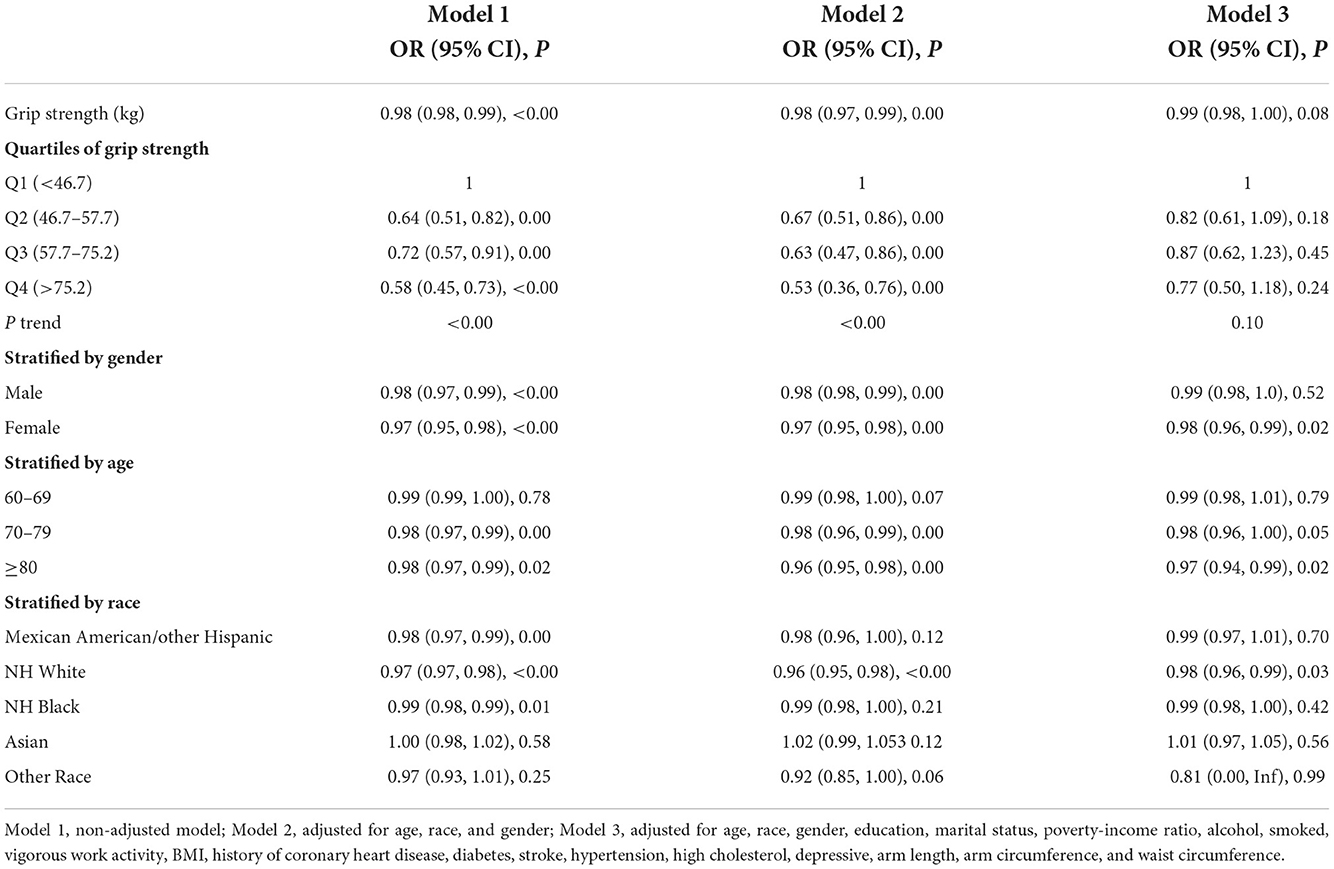
Table 3. Associations between grip strength and cognitive impairment (AF<14) (n = 2,623), NHANES 2011–2014.
Subgroup analysis indicated that >80 years of age (full adjustment: OR = 0.97, 95% CI 0.94–0.99), female sex (OR = 0.98, 95% CI 0.96–0.99), and NH White race (full adjustment: OR = 0.98, 95% CI 0.96–0.99) were associated with a significantly low risk of cognitive impairment.
Association between hand grip strength and cognitive impairment based on the DSST results
Table 4 shows the association between hand grip strength and cognitive impairment based on the DSST results. A statistically significant difference was observed between hand grip strength and a low risk of cognitive impairment in each model (full adjustment: OR = 0.97, 95% CI 0.96–0.98) and DSST in Q2–Q4 (full adjustment: Q2: OR = 0.68, 95% CI 0.48–0.97; Q3: OR = 0.57, 95% CI 0.37–0.87; Q4: OR = 0.34, 95% CI 0.20–0.58).
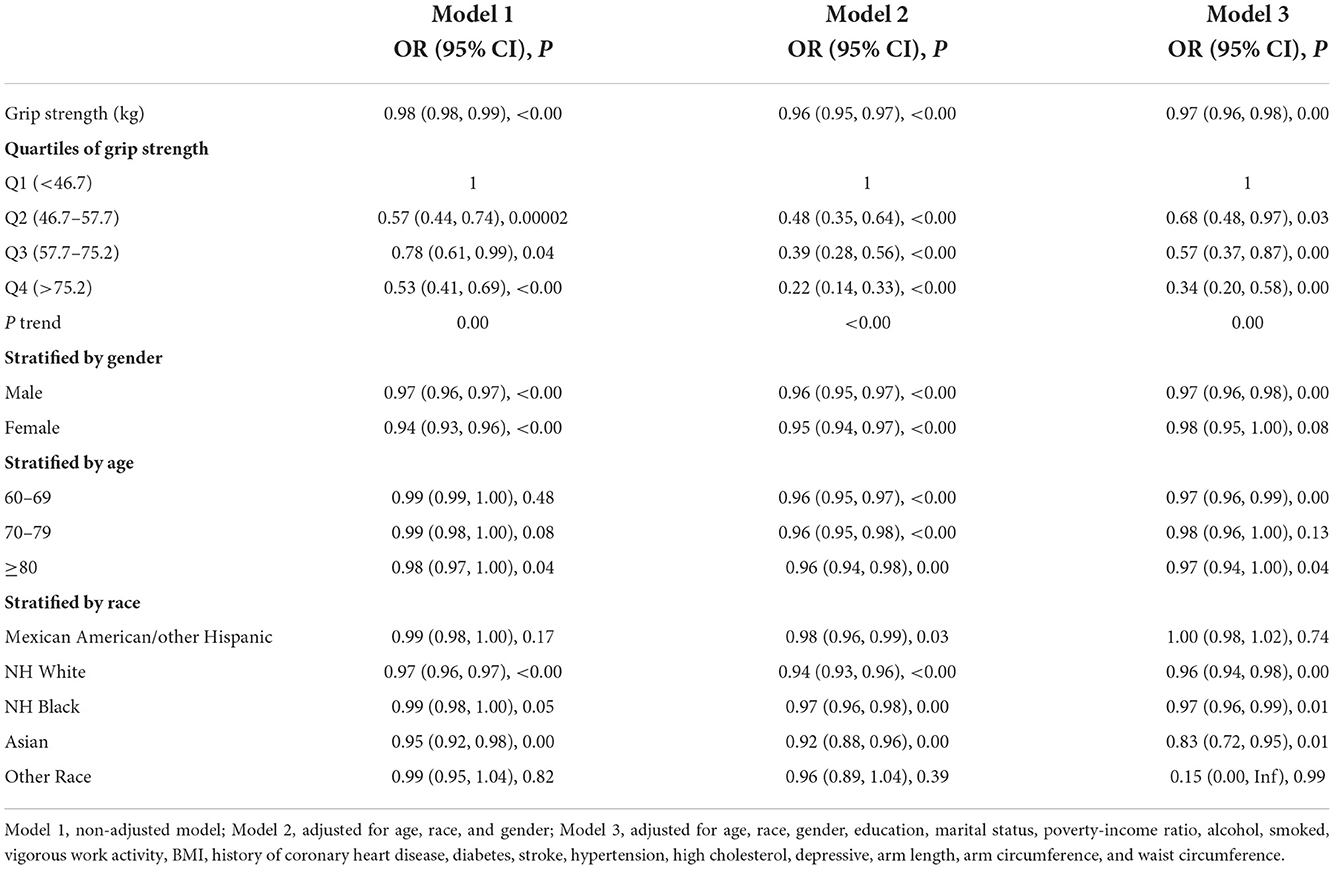
Table 4. Associations between grip strength and cognitive impairment (DSST<34) (n = 2,623), NHANES 2011–2014.
Subgroup analysis revealed that 60–69 years of age (full adjustment: OR = 0.97, 95% CI 0.96–0.99), male sex (full adjustment: OR = 0.97, 95% CI 0.96–0.98), NH White race (full adjustment: OR = 0.96, 95% CI 0.94–0.98), NH Black race (full adjustment: OR = 0.97, 95% CI 0.96–0.99), and Asian race (full adjustment: OR = 0.83, 95% CI 0.72–0.95) were associated with a significantly low risk of cognitive impairment.
Sensitivity analysis outcomes
We used a smooth curve fit model to investigate the possibility of a non-linear association between hand grip strength and cognitive impairment (Figure 2). After full adjustment for covariates (using the aforementioned full adjustment model), our analysis indicated a linear association between hand grip strength and cognitive impairment. Furthermore, the smooth curve fit model was applied to investigate a sex-stratified association between hand grip strength and cognitive impairment (Figure 3). These results were consistent with those obtained using the full adjustment model, which showed a linear association.
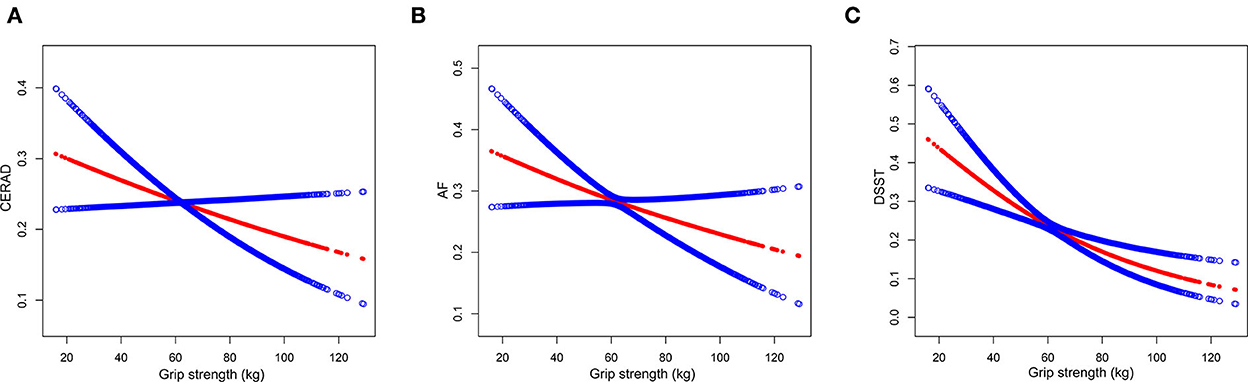
Figure 2. The association between grip strength and cognitive impairment. Consortium to Establish a Registry for Alzheimer's Disease (CERAD) (A), animal fluency (AF) (B), and digit symbol substitution test (DSST) (C) represent cognitive impairment. The red points show a smooth curve fitting line, the blue points show 95% confidence interval. The relationship was adjusted for age, race, gender, education, marital status, poverty-income ratio, alcohol, smoked, vigorous work activity, BMI, history of coronary heart disease, diabetes, stroke, hypertension, high cholesterol, depressive, arm length, arm circumference, and waist circumference.
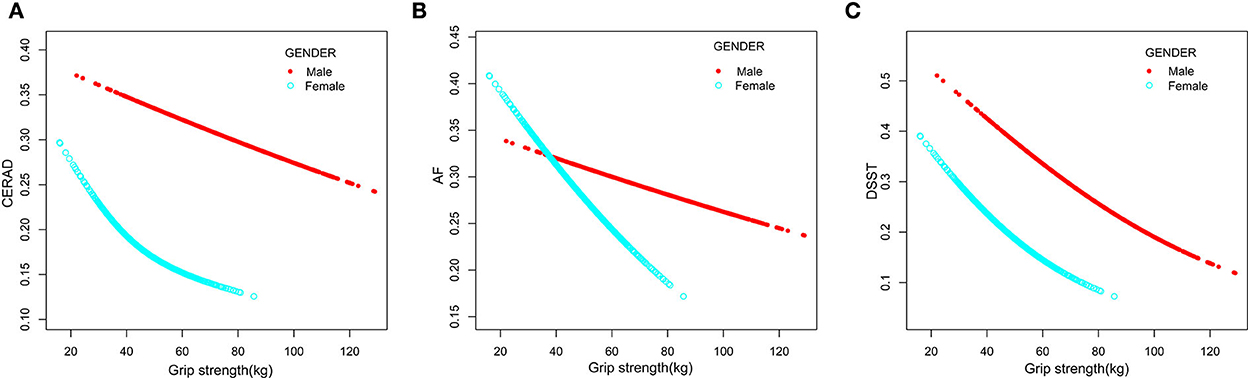
Figure 3. The association between grip strength and cognitive impairment for male sex (red line) and female sex (blue line). CERAD (A), AF (B), and DSST (C) represent cognitive impairment. The relationship was adjusted for age, race, gender, education, marital status, poverty-income ratio, alcohol, smoked, vigorous work activity, BMI, history of coronary heart disease, diabetes, stroke, hypertension, high cholesterol, depressive, arm length, arm circumference, and waist circumference.
Machine learning using the XGBoost algorithm model
We used the machine learning of the XGBoost model to determine the relative importance of variables associated with cognitive impairment. Variables included grip strength, arm circumference, waist circumference, and arm length. Data showed that each variable's contribution by the XGBoost model, arm circumference, and grip strength was the topmost important negative variables of the dataset based on AF and DSST. Arm length was the most important positive variable of the dataset based on cognitive function tests (Figure 4).
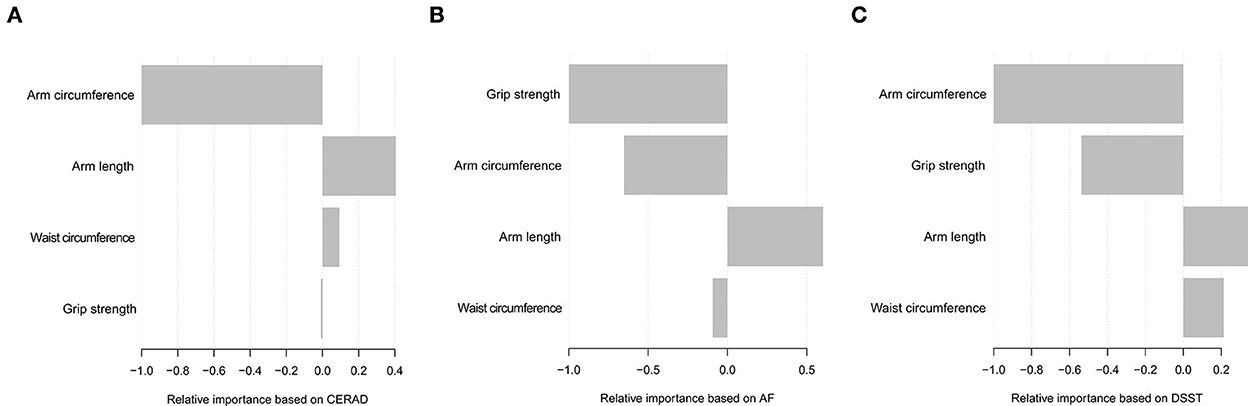
Figure 4. Relative importance of the selected variables using XGBoost and the corresponding variable importance score based on CERAD (A), AF (B), and DSST (C). The X-axis indicates the importance score, which is the relative number of a variable that is used to distribute the data, and Y-axis indicates the selected variable.
Discussion
In the present study, we analyzed the data of 2,623 elderly American adults to investigate the association between grip strength and cognitive impairment. After adjustment for all potential confounders, our results showed an association between growth hand grip strength and cognitive impairment, and statistically significant differences were observed in NH White, NH Black, Asian, male sex, and individuals aged 60–69 years throughout subgroup analyses. Furthermore, a linear correlation was observed between hand grip strength and cognitive impairment. Finally, machine learning of the XGBoost model shows that grip strength is one of the top two most important negative predictor variables.
Several previous studies have investigated the association between hand grip strength and cognitive function. In 2000, Christensen et al. reported that grip strength could not predict future changes in memory or IQ (Christensen et al., 2000). Deary et al. (2011) also observed no association between grip strength and cognitive function. In 2016, Ritchie et al. (2016) reported no association between an increase or decrease in grip strength and cognitive impairment. Nevertheless, some researchers who used the horizontal linear mixed growth model have confirmed a clear association between cognitive impairment and a decline in grip strength (Macdonald et al., 2011). Another study indicated that grip strength did not predict cognitive impairment in individuals aged < 65 years; however, it could predict a decline in all cognitive domains in individuals aged >65 years (Sternäng et al., 2016). A study that included cancer survivors and used information from the NHANES database reported an association between cognitive impairment and hand grip strength (Yang et al., 2018). Several studies have investigated the association between cognitive functioning and hand grip strength (Firth et al., 2018; Robitaille et al., 2018; Yoon et al., 2018; Ahrenfeldt et al., 2019; Imaoka et al., 2019; Kim and Kim, 2019; Liu et al., 2019, 2020; Hooyman et al., 2021; Watermeyer et al., 2021). Our results were consistent with those reported by previous studies; we observed that cognitive impairment was associated with grip strength in older American adults.
High hand grip strength was associated with male sex, vigorous work activity, alcohol consumption, smoking, and a history of coronary heart disease. However, low hand grip strength was associated with female sex, never married status, a history of stroke, diabetes, hypertension, high serum cholesterol levels, and depression. The mechanism under the interesting results may involve the basal metabolic rate and blood flow to the upper extremities. Regular exercise and a healthy lifestyle are also important factors. Of course, the exact mechanism needs to be confirmed by more animal and clinical trials.
The following are the strengths of the present study. (a) The large sample size (2,623 participants) is a strength because an increase in sample size improves the statistical power of the study, and our results are statistically more significant. (b) In this study, we sorted different categories of missing data, which minimized the effect of missing data on bias in our results. (c) We eliminated as many confounders as possible, including a history of chronic disease and depressive status, and used the three most common tests performed in clinical practice for the assessment of cognitive function. (d) The linear association between grip strength and cognitive impairment was supported by the use of a smooth curve fit model and further confirmed using subgroup and sensitivity analyses.
The following are the weaknesses of the present study that may have affected our results. (a) Owing to the cross-sectional study design, it is difficult to distinguish causality between grip strength and cognitive impairment owing to its internal characteristics. (b) The study population was limited to Americans; therefore, our results may not be generalizable. (c) Cognitive function evaluation was based on the cognitive level of the interviewee; therefore, some cognitive functions that did not meet the interview requirements may have been excluded inadvertently.
In conclusion, our study highlights an inverse relationship between hand grip strength and cognitive impairment, which might suggest a shared underlying mechanism that needs to be further investigated using a large-scale prospective clinical trial to validate our findings.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: Centers for Disease Control and Prevention (CDC) National Health and Nutrition Examination Survey (NHANES), https://wwwn.cdc.gov/nchs/nhanes/Default.aspx. Further inquiries can be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
JH and ZL planned and executed the studies and data analysis and drafted the manuscript. XW processed and analyzed the data. HZ and DH made great efforts to revise the manuscript. WL conceived the item. JW facilitated the design and analysis of the experiments. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the National Natural Science Foundation of China (81471197 and 81070950).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ahrenfeldt, L. J., Scheel-Hincke, L. L., Kjærgaard, S., Möller, S., Christensen, K., and Lindahl-Jacobsen, R. (2019). Gender differences in cognitive function and grip strength: a cross-national comparison of four European regions. Eur. J. Public Health 29, 667–674. doi: 10.1093/eurpub/cky266
Appiah, D., Nwabuo, C. C., Ebong, I. A., Wellons, M. F., and Winters, S. J. (2021). Trends in age at natural menopause and reproductive life span among US women, 1959-2018. JAMA 325, 1328–1330. doi: 10.1001/jama.2021.0278
Bailey, R. L., Jun, S., Murphy, L., Green, R., Gahche, J. J., Dwyer, J. T., et al. (2020). High folic acid or folate combined with low vitamin B-12 status: potential but inconsistent association with cognitive function in a nationally representative cross-sectional sample of US older adults participating in the NHANES. Am. J. Clin. Nutr 112, 1547–1557. doi: 10.1093/ajcn/nqaa239
Bohannon, R. W. (2019). Grip strength: an indispensable biomarker for older adults. Clin. Interv. Aging 14, 1681–1691. doi: 10.2147/CIA.S194543
Brody, D. J., Kramarow, E. A., Taylor, C. A., and Mcguire, L. C. (2019). Cognitive performance in adults aged 60 and over: National Health and Nutrition Examination Survey, 2011-2014. Natl. Health Stat. Report. 126, 1–23.
Carroll, W. M. (2019). The global burden of neurological disorders. Lancet Neurol. 18, 418–419. doi: 10.1016/S1474-4422(19)30029-8
Casagrande, S. S., Lee, C., Stoeckel, L. E., Menke, A., and Cowie, C. C. (2021). Cognitive function among older adults with diabetes and prediabetes, NHANES 2011-2014. Diabetes Res. Clin. Pract. 178, 108939. doi: 10.1016/j.diabres.2021.108939
Christensen, H., Korten, A. E., Mackinnon, A. J., Jorm, A. F., Henderson, A. S., and Rodgers, B. (2000). Are changes in sensory disability, reaction time, and grip strength associated with changes in memory and crystallized Intelligence? A longitudinal analysis in an elderly community sample. Gerontology 46, 276–292. doi: 10.1159/000022172
Deary, I. J., Johnson, W., Gow, A. J., Pattie, A., Brett, C. E., Bates, T. C., et al. (2011). Losing one's grip: a bivariate growth curve model of grip strength and nonverbal reasoning from age 79 to 87 years in the Lothian Birth Cohort 1921. J. Gerontol. B Psychol. Sci. Soc. Sci. 66, 699–707. doi: 10.1093/geronb/gbr059
Dong, X., Li, S., Chen, J., Li, Y., Wu, Y., and Zhang, D. (2020a). Association of dietary ω-3 and ω-6 fatty acids intake with cognitive performance in older adults: National Health and nutrition examination Survey (NHANES) 2011-2014. Nutr. J. 19, 25. doi: 10.1186/s12937-020-00547-7
Dong, X., Li, S., Sun, J., Li, Y., and Zhang, D. (2020b). Association of coffee, decaffeinated coffee and caffeine intake from coffee with cognitive performance in older adults: National Health and Nutrition Examination Survey (NHANES) 2011-2014. Nutrients 12, 840. doi: 10.3390/nu12030840
Fan, Y., Zhang, Y., Li, J., Liu, Y., Chang, H., Jiang, Y., et al. (2021). Association between healthy eating index-2015 and various cognitive domains in US adults aged 60 years or older: the National Health and Nutrition Examination Survey (NHANES) 2011-2014. BMC Public Health 21, 1862. doi: 10.1186/s12889-021-11914-2
Feigin, V. L., Vos, T., Nichols, E., Owolabi, M. O., Carroll, W. M., Dichgans, M., et al. (2020). The global burden of neurological disorders: translating evidence into policy. Lancet Neurol. 19, 255–265. doi: 10.1016/S1474-4422(19)30411-9
Firth, J., Stubbs, B., Vancampfort, D., Firth, J. A., Large, M., Rosenbaum, S., et al. (2018). Grip strength is associated with cognitive performance in schizophrenia and the general population: a UK biobank study of 476559 participants. Schizophr. Bull 44, 728–736. doi: 10.1093/schbul/sby034
Flegal, K. M., Graubard, B. I., Williamson, D. F., and Gail, M. H. (2005). Excess deaths associated with underweight, overweight, and obesity. JAMA 293, 1861–1867. doi: 10.1001/jama.293.15.1861
Frith, E., and Loprinzi, P. D. (2017). The association between physical activity and cognitive function with considerations by social risk status. Eur. J. Psychol. 13, 767–775. doi: 10.5964/ejop.v13i4.1471
Frith, E., and Loprinzi, P. D. (2018). Physical activity and cognitive function among older adults with an elevated gamma gap. Med. Princ. Pract. 27, 531–536. doi: 10.1159/000493732
Ge, H., Yang, T., Sun, J., and Zhang, D. (2020). Associations between dietary carotenoid intakes and the risk of depressive symptoms. Food Nutr. Res. 64, 3920 doi: 10.29219/fnr.v64.3920
Hooyman, A., Malek-Ahmadi, M., Fauth, E. B., and Schaefer, S. Y. (2021). Challenging the relationship of grip strength with cognitive status in older adults. Int. J. Geriatr. Psychiatry 36, 433–442. doi: 10.1002/gps.5441
Imaoka, M., Nakao, H., Nakamura, M., Tazaki, F., Maebuchi, M., Ibuki, M., et al. (2019). Effect of multicomponent exercise and nutrition support on the cognitive function of older adults: a randomized controlled trial. Clin. Interv. Aging 14, 2145–2153. doi: 10.2147/CIA.S229034
Kim, J. H., and Kim, J. M. (2019). Association of cognitive impairment and grip strength trajectories with mortality among middle-aged and elderly adults. Int. Psychogeriatr. 31, 723–734. doi: 10.1017/S1041610218001175
Kim, U. J., Hong, M., and Choi, Y. H. (2021). environmental pyrethroid exposure and cognitive dysfunction in U.S. older adults: the NHANES 2001-2002. Int. J. Environ. Res. Public Health 18, 12005. doi: 10.3390/ijerph182212005
Li, S., Sun, W., and Zhang, D. (2019). Association of zinc, iron, copper, and selenium intakes with low cognitive performance in older adults: a cross-sectional study from National Health and Nutrition Examination Survey (NHANES). J. Alzheimers Dis. 72, 1145–1157. doi: 10.3233/JAD-190263
Liss, J. L., Seleri Assunção, S., Cummings, J., Atri, A., Geldmacher, D. S., Candela, S. F., et al. (2021). Practical recommendations for timely, accurate diagnosis of symptomatic Alzheimer's disease (MCI and dementia) in primary care: a review and synthesis. J. Intern. Med. 290, 310–334. doi: 10.1111/joim.13244
Liu, X., Chen, J., Geng, R., Wei, R., Xu, P., Chen, B., et al. (2020). Sex- and age-specific mild cognitive impairment is associated with low hand grip strength in an older Chinese cohort. J. Int. Med. Res. 48, 300060520933051. doi: 10.1177/0300060520933051
Liu, Y., Cao, X., Gu, N., Yang, B., Wang, J., and Li, C. (2019). A prospective study on the association between grip strength and cognitive function among middle-aged and elderly Chinese participants. Front. Aging Neurosci. 11, 250. doi: 10.3389/fnagi.2019.00250
Macdonald, S. W., Decarlo, C. A., and Dixon, R. A. (2011). Linking biological and cognitive aging: toward improving characterizations of developmental time. J. Gerontol. B Psychol. Sci. Soc. Sci. 66(Suppl. 1):i59–70. doi: 10.1093/geronb/gbr039
Matthews, K. A., Xu, W., Gaglioti, A. H., Holt, J. B., Croft, J. B., Mack, D., et al. (2019). Racial and ethnic estimates of Alzheimer's disease and related dementias in the United States (2015-2060) in adults aged ≥65 years. Alzheimers Dement. 15, 17–24. doi: 10.1016/j.jalz.2018.06.3063
Morris, J. C., Heyman, A., Mohs, R. C., Hughes, J. P., Van Belle, G., Fillenbaum, G., et al. (1989). The Consortium to Establish a Registry for Alzheimer's Disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer's disease. Neurology 39, 1159–1165. doi: 10.1212/WNL.39.9.1159
Pereira, L. C. R., Shannon, O. M., Mazidi, M., Babateen, A. M., Ashor, A. W., Stephan, B. C. M., et al. (2021). Relationship between urinary nitrate concentrations and cognitive function in older adults: findings from the NHANES survey. Int. J. Food Sci. Nutr. 72, 805–815. doi: 10.1080/09637486.2020.1868411
Piersol, C. V., Jensen, L., Lieberman, D., and Arbesman, M. (2018). Occupational therapy interventions for people with Alzheimer's disease. Am. J. Occup. Ther. 72, 7201390010p7201390011–6. doi: 10.5014/ajot.2018.721001
Prince, M., Acosta, D., Chiu, H., Scazufca, M., and Varghese, M. (2003). Dementia diagnosis in developing countries: a cross-cultural validation study. Lancet 361, 909–917. doi: 10.1016/S0140-6736(03)12772-9
Ritchie, S. J., Tucker-Drob, E. M., Starr, J. M., and Deary, I. J. (2016). Do cognitive and physical functions age in concert from age 70 to 76? Evidence from the Lothian birth cohort 1936. Span J. Psychol. 19, E90. doi: 10.1017/sjp.2016.85
Robitaille, A., Piccinin, A. M., Hofer, S. M., Johansson, B., and Muniz Terrera, G. (2018). An examination of the heterogeneity in the pattern and association between rates of change in grip strength and global cognition in late life. A multivariate growth mixture modelling approach. Age Ageing 47, 692–697. doi: 10.1093/ageing/afy048
Sotaniemi, M., Pulliainen, V., Hokkanen, L., Pirttil,ä, T., Hallikainen, I., Soininen, H., et al. (2012). CERAD-neuropsychological battery in screening mild Alzheimer's disease. Acta Neurol. Scand. 125, 16–23. doi: 10.1111/j.1600-0404.2010.01459.x
Sternäng, O., Reynolds, C. A., Finkel, D., Ernsth-Bravell, M., Pedersen, N. L., and Dahl Aslan, A. K. (2016). Grip strength and cognitive abilities: associations in old age. J. Gerontol. B Psychol. Sci. Soc. Sci. 71, 841–848. doi: 10.1093/geronb/gbv017
Vandenbroucke, J. P., Von Elm, E., Altman, D. G., Gøtzsche, P. C., Mulrow, C. D., Pocock, S. J., et al. (2007). Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. 4, e297. doi: 10.1371/journal.pmed.0040297
Warren, A. (2022). Behavioral and psychological symptoms of dementia as a means of communication: considerations for reducing stigma and promoting person-centered care. Front. Psychol. 13, 875246. doi: 10.3389/fpsyg.2022.875246
Watermeyer, T., Massa, F., Goerdten, J., Stirland, L., Johansson, B., and Muniz-Terrera, G. (2021). Cognitive dispersion predicts grip strength trajectories in men but not women in a sample of the oldest old without dementia. Innovat. Aging 5, igab025. doi: 10.1093/geroni/igab025
Wong, T., Dang, K., Ladhani, S., Singal, A. K., and Wong, R. J. (2019). Prevalence of alcoholic fatty liver disease among adults in the United States, 2001-2016. JAMA 321, 1723–1725. doi: 10.1001/jama.2019.2276
Yang, L., Koyanagi, A., Smith, L., Hu, L., Colditz, G. A., Toriola, A. T., et al. (2018). Hand grip strength and cognitive function among elderly cancer survivors. PLoS ONE 13, e0197909. doi: 10.1371/journal.pone.0197909
Keywords: grip strength, cognitive impairment, Consortium to Establish a Registry for Alzheimer's Disease (CERAD), animal fluency (AF), digit symbol substitution test (DSST), smooth curve fit, machine learning
Citation: Huang J, Wang X, Zhu H, Huang D, Li W, Wang J and Liu Z (2022) Association between grip strength and cognitive impairment in older American adults. Front. Mol. Neurosci. 15:973700. doi: 10.3389/fnmol.2022.973700
Received: 20 June 2022; Accepted: 07 November 2022;
Published: 30 November 2022.
Edited by:
James Cheng-Chung Wei, Chung Shan Medical University Hospital, TaiwanReviewed by:
Galya Bigman, United States Department of Veterans Affairs, United StatesMuddanna Sakkattu Rao, Kuwait University, Kuwait
Copyright © 2022 Huang, Wang, Zhu, Huang, Li, Wang and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhirong Liu, bGl1emhpcjgwMTlAMTI2LmNvbQ==
†These authors have contributed equally to this work