 Yuchen Wang
Yuchen Wang Mengqi Li1,2†
Mengqi Li1,2† Qiuhong Ji
Qiuhong Ji- 1Department of Neurology, Affiliated Hospital of Nantong University, Nantong, China
- 2Medical School of Nantong University, Nantong, China
Background: Ischemic stroke is the second leading cause of death and the third leading cause of combined disability and mortality globally. While reperfusion therapies play a critical role in the management of acute ischemic stroke (AIS), their applicability is limited, leaving many patients with significant neurological deficits and poor prognoses. Neuroprotective agents have garnered attention for their potential as adjunct therapies; however, their relative efficacy remains unclear. This study utilized a network meta-analysis (NMA) to systematically compare the efficacy of neuroprotective agents in improving neurological function and prognosis in stroke patients.
Methods: This study adhered to PRISMA guidelines and the Cochrane Handbook for systematic reviews. Randomized controlled trials (RCTs) were identified through comprehensive searches of the PubMed, Embase, and Cochrane Library databases. Two independent reviewers conducted the selection process, data extraction, and quality assessment. Outcomes included 90-day modified Rankin Scale (90d-mRS), change of National Institutes of Health Stroke Scale score from baseline to 90-day/14-day/7-day (90d/14d/7d-NIHSS) and 90-day/14-day Barthel Index (90d/14d-BI). Data analyses were performed using RevMan 5.4 and Stata 14.0.
Results: A total of 42 RCTs involving 12,210 participants were included in this analysis. The interventions assessed included Cerebrolysin, Citicoline, Edaravone, Edaravone Dextranol, Human urinary kallidinogenase, Minocycline, Nerinetide, Butylphthalide, Vinpocetine, and Control. The NMA results demonstrated that NBP ranked highest for the 90d-mRS, 90d-NIHSS, 14d-NIHSS, and 14d-BI outcomes. Edaravone was found to be the most effective intervention for the 7d-NIHSS and 90d-BI outcomes.
Conclusion: The findings of this study indicate that different neuroprotective agents exhibit distinct advantages at specific stages of recovery. NBP showed outstanding performance in improving 90d-mRS and 90d-NIHSS, underscoring its potential in long-term rehabilitation. Edaravone demonstrated significant superiority in 7d-NIHSS scores, highlighting its role in early neuroprotection. These results provide valuable insights for individualized clinical treatment. To further validate the efficacy and safety of neuroprotective agents, future studies should involve larger sample sizes and conduct multicenter, large-scale randomized controlled trials.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=601346, identifier CRD42024601346.
1 Introduction
The 2019 Global Burden of Disease (GBD) study identified stroke as the second leading cause of death and the third leading cause of combined disability and mortality globally (GBD, 2021). Without immediate intervention, the projected global mortality from stroke is expected to rise by 50% by 2050, resulting in approximately 9.7 million deaths annually, and economic losses may reach as high as $2.3 trillion (Feigin et al., 2022). Each year, over 7.6 million new cases of ischemic stroke are reported, with more than 77 million individuals affected globally (GBD, 2021). Acute ischemic stroke (AIS) is an acute medical emergency characterized by a sudden onset of focal neurological deficits due to impaired cerebral blood flow, typically caused by a range of cerebrovascular factors (Walter, 2022). This ischemic disruption triggers a cascade of pathological events, ultimately resulting in neuronal injury. Current treatment options for AIS are primarily limited to reperfusion therapies, such as intravenous thrombolysis and endovascular thrombectomy (Goyal et al., 2016; Menon et al., 2022). However, strict eligibility criteria and time constraints limit these therapies to only a subset of patients. To address this gap, several therapeutic strategies have been developed to target the ischemic pathophysiological cascade, aiming to prevent irreversible tissue damage. Among these, neuroprotective agents have garnered significant attention (Yanık and Yanık, 2024). Clinically, these agents are frequently employed as adjuncts to standard AIS treatments, and additional neurorestorative approaches are being explored. Numerous neuroprotective drugs have demonstrated promising outcomes in preclinical studies; however, despite initial evidence, the comparative efficacy of these agents or their combinations in AIS remains inconclusive.
Several neuroprotective agents, including Citicoline (Agarwal and Patel, 2017; Secades et al., 2016; Shi et al., 2016), Cerebrolysin (Bornstein et al., 2018; Wan et al., 2024), Minocycline (Malhotra et al., 2018), and Vinpocetine (Panda et al., 2022), have demonstrated efficacy in enhancing neurological function and prognosis in stroke patients, as indicated by previous meta-analyses. However, traditional meta-analyses are limited by their focus on pairwise comparisons, thereby restricting the breadth of interventions assessed. In contrast, network meta-analysis (NMA) enables a comprehensive evaluation and ranking of multiple interventions concurrently (Rouse et al., 2017). This study aims to utilize NMA to compare the efficacy of various neuroprotective agents in improving neurological function and prognosis for ischemic stroke patients. Despite the advancements in reperfusion therapies, many stroke patients continue to experience significant neurological impairments. Neuroprotective agents serve as potential adjuncts to these treatments, yet their relative effectiveness remains ambiguous. Accordingly, we conducted a systematic analysis of randomized controlled trial (RCT) data to evaluate the effects of various neuroprotective interventions, including Nerinetide, Human Urinary Kallidinogenase (HUK), Edaravone, Edaravone Dextranol, Vinpocetine, Butylphthalide, Minocycline, Citicoline, and Cerebrolysin, on key early and long-term outcomes such as the modified Rankin Scale (mRS), National Institutes of Health Stroke Scale (NIHSS), and Barthel Index (BI) scores. This study aims to elucidate the relative efficacy of these neuroprotective agents in enhancing neurological function and prognosis at different recovery phases in ischemic stroke patients.
2 Materials and methods
This study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021) and follows the Cochrane Handbook for Systematic Reviews of Interventions to ensure methodological rigor. Furthermore, the network meta-analysis was pre-registered in PROSPERO under the registration number CRD42024601346.
2.1 Search strategy
Two authors independently conducted a comprehensive search of PubMed, Embase, and the Cochrane Library to identify randomized controlled trials (RCTs) and crossover RCTs assessing the efficacy of neuroprotective agents in enhancing neurological function and prognosis in ischemic stroke patients. The search period covered all records from the inception of these databases until September 31, 2024. A combination of Boolean operators, Medical Subject Headings (MeSH), and free-text terms was utilized, incorporating search terms such as “Stroke,” “Cerebrovascular accident,” “Brain Vascular Accident,” “hemiplegia,” “apoplexy,” “CVA,” as well as specific neuroprotective agents including “Nerinetide,” “human urinary kallidinogenase,” “Edaravone,” “Vinpocetine,” “Butylphthalide,” “Minocycline,” “Citicoline,” and “Cerebrolysin.” Detailed search strategies for PubMed are available in Supplementary Table 1.
2.2 Inclusion criteria
The inclusion criteria were established in accordance with the PICOS framework (Population, Interventions, Comparators, Outcomes, and Study Design) (Hutton et al., 2015).
2.2.1 Inclusion criteria
1. Population: Adults (≥18 years) diagnosed with acute ischemic stroke, confirmed through neuroimaging (including CT, MRI, etc.).
2. Interventions: Nerinetide (NA-1), Hman urinary kallidinogenase (HUK), Edaravone, Edaravone Dextranol, Vinpocetine, N-butylphthalide (NBP), Minocycline, Citicoline and Cerebrolysin.
3. Comparators: The control group included placebo or other neuroprotective agents. Both the intervention group and the control group received standard treatment. Standard care is defined as including both non-neuroprotective pharmacological and non-pharmacological treatments. These encompass interventions aimed at improving cerebral blood flow, such as intravenous thrombolysis, endovascular therapy, antiplatelet therapy, anticoagulant therapy, and fibrinolytic therapy, as well as symptomatic treatments. Symptomatic treatments include respiratory support and oxygen supplementation, cardiac monitoring, temperature regulation, blood pressure management, blood glucose control, and lipid level management, among others.
4. Outcomes: The primary outcome indicator was 90-day modified Rankin Scale score (90d-mRS). The secondary outcome indicators included change of National Institutes of Health Stroke Scale score from baseline to 90-day, 14-day, 7-day (90d/14d/7d-NIHSS) and 90-day, 14-day Barthel Index score (90d/14d-BI).
Detailed scoring criteria for mRS, NIHSS and BI are available in Supplementary Tables 2–4.
5. Study designs: RCTs or crossover RCTs.
2.2.2 Exclusion criteria
1. Patients with hemorrhagic stroke or transient ischemic attack (TIA). Pediatric patients or individuals with pre-existing severe neurological deficits.
2. Conference abstracts, study protocols, reviews, meta-analyses, dissertations, and non-randomized controlled trials (e.g., case reports, observational studies, cross-sectional studies, and studies without control groups).
3. Studies lacking any of the primary or secondary outcome measures.
4. Studies where more than 20% of patients discontinued treatment midway.
5. Studies that could not be downloaded.
6. Studies with incomplete outcome data and no response from the authors after three attempts to contact them.
7. Duplicate publications.
2.3 Study selection
First, two authors (Y.C.W and M.Q.L) used Endnote X9 software to remove duplicate articles. Then, they screened titles and abstracts to exclude articles that did not meet the inclusion criteria. Finally, they reviewed the full texts to select articles that met the eligibility criteria. In case of disagreements during the review process, the two authors resolved them through discussion or consultation with a third author (Y.Y.J).
2.4 Data extraction
Two authors independently reviewed all articles and extracted the relevant data. The extracted data encompassed basic publication details, including the first author’s name, year of publication, country of study, participant characteristics (age and sample size), intervention details (type, administration method, dosage, and treatment duration), as well as baseline and final outcome measures (mRS, NIHSS, and BI) for calculating change scores. The collected data were entered into an Excel spreadsheet and subsequently cross-checked by both authors. In cases where discrepancies occurred during data extraction, a third author was consulted to resolve the differences through discussion.
2.5 Quality assessment
Two authors independently evaluated the risk of bias in the included studies using the Cochrane Risk of Bias Tool (Savović et al., 2014). This tool assesses seven key domains: (1) Random sequence generation, (2) Allocation concealment, (3) Blinding of participants and personnel, (4) Blinding of outcome assessment, (5) Incomplete outcome data, (6) Selective reporting, and (7) Other sources of bias. Each domain was classified as having “low risk,” “unclear risk,” or “high risk” based on the available evidence. In instances where disagreements occurred during the assessment, a third author was consulted to facilitate consensus.
2.6 Statistical analysis
Odds ratios (ORs) for binary variables and mean differences (MD) for continuous variables were employed as effect measures, with 95% confidence intervals (CI) provided for each estimate. In cases where different methods or scales were utilized to measure the same outcome, standardized mean differences (SMD) were calculated instead of MD. The differences and standard deviations (SD) for continuous outcome variables before and after treatment were computed according to the guidelines outlined in Section 16.1.3.2 of the Cochrane Handbook version 5.0.2. Statistical analyses were conducted using Stata version 14.0 to perform the network meta-analysis (NMA) and generate various visual representations, including network diagrams for eligible comparisons, Surface Under the Cumulative Ranking (SUCRA) curves, and funnel plots for assessing publication bias (Shim et al., 2017). When loops of evidence existed among interventions, global inconsistency was first evaluated. If p > 0.05, the inconsistency was deemed non-significant, and the consistency model was selected. Local inconsistency was assessed using the node-splitting method. SUCRA values were used to rank the interventions, with higher SUCRA values (closer to 100%) indicating better efficacy.
Subgroup analyses were conducted using RevMan 5.4 software. The 95% confidence interval (CI) was employed to represent the statistical effect size. If no significant heterogeneity was detected between studies (p ≥ 0.1, I2 ≤ 50%), a fixed-effects model was applied. Otherwise, a random-effects model was utilized (p < 0.1, I2 > 50%) (Tufanaru et al., 2015). To assess the robustness of the results, subgroup analyses were performed to identify potential sources of heterogeneity. Funnel plots with adjustments were employed to evaluate publication bias for each outcome measure in the included studies.
3 Results
3.1 Search results
A systematic search of three databases was conducted based on predefined inclusion and exclusion criteria, initially identifying 3,096 articles. After removing duplicates, 2,167 articles remained. Titles and abstracts were then screened, resulting in the exclusion of articles that did not meet the inclusion criteria, reducing the number to 68 articles. Following a full-text review, an additional 26 articles were excluded. Ultimately, 42 randomized controlled trials (RCTs) were included in the final analysis. Figure 1 depicts the screening and selection process of the articles.
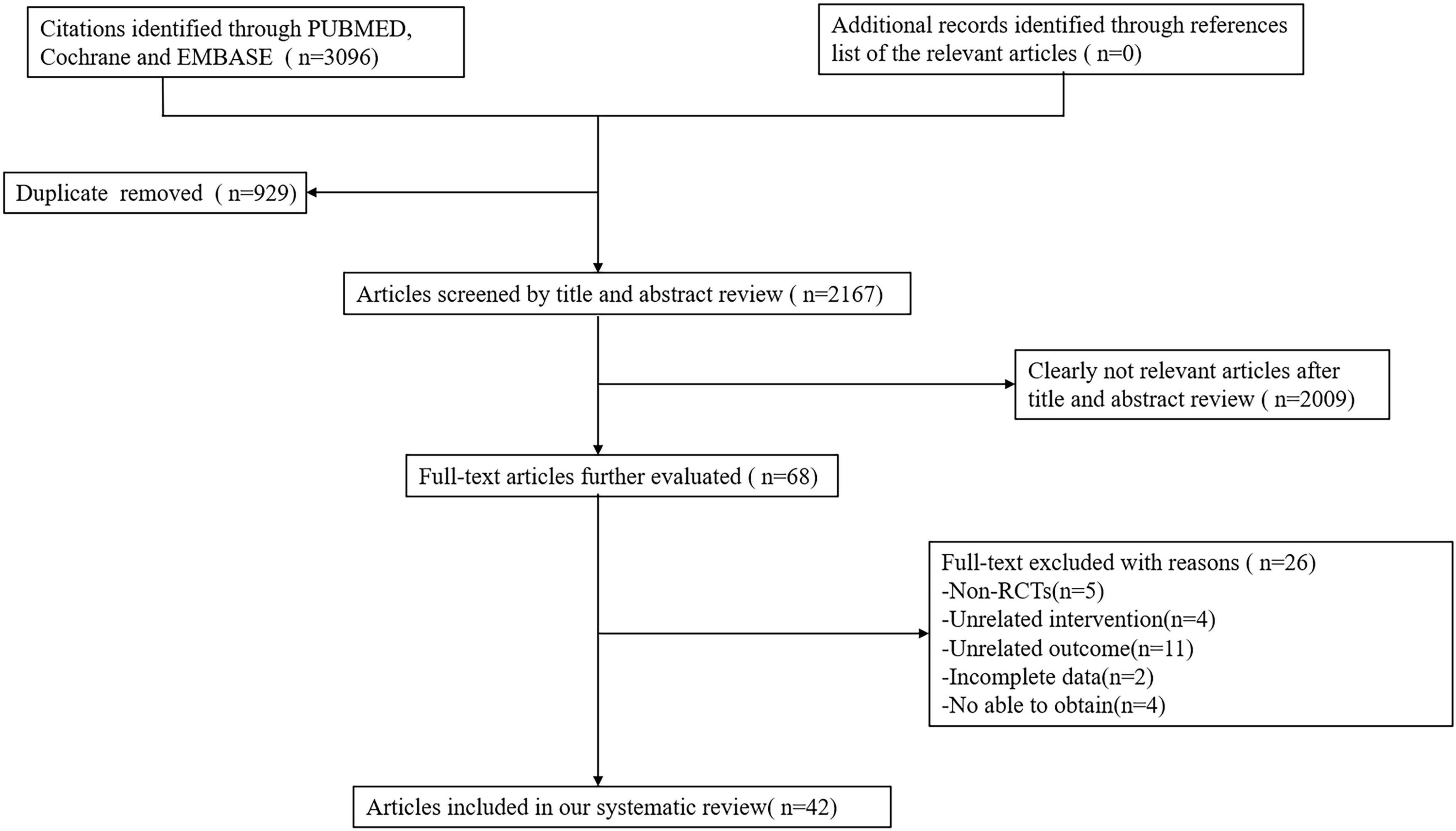
Figure 1. Flow diagram of the eligible studies selection process.
3.2 Characteristics of the included studies
A total of 42 studies published between 2001 and 2023, involving 12,210 patients, were included in this analysis. All studies were randomized controlled trials (RCTs). In terms of geographical distribution, 47.6% of the included studies originated from China, 14.2% from India, 4.8% each from Russia and Iran, and 2.4% each from the United States, Germany, Canada, New Zealand, Australia, Japan, Israel, Iraq, Serbia, Croatia, Romania, and Austria. The majority of studies were conducted in China (20/42), followed by India (6/42), Russia (2/42), Iran (2/42), and one study each from the other aforementioned countries. The outcome measures assessed included: NBP (11 studies), Cerebrolysin (8 studies), Citicoline (7 studies), Edaravone (6 studies), HUK (5 studies), Minocycline (5 studies), Vinpocetine (4 studies), Edaravone Dextranol (2 studies), and NA-1 (1 study). Detailed characteristics of the included studies are provided in Table 1 (Al Mudhafar et al., 2019; Amiri-Nikpour et al., 2014; Amiri-Nikpour et al., 2015; Belova et al., 2017; Chen L. et al., 2019; Cui et al., 2013; Dávalos et al., 2012; Feigin et al., 2001; Fu et al., 2024; Ghosh et al., 2015; Guo et al., 2021; Hill et al., 2020; Imai et al., 2006; Khasanova and Kalinin, 2023; Kohler et al., 2013; Lampl et al., 2007; Lang et al., 2013; Li et al., 2015; Li et al., 2024; Lou et al., 2024; Mehta et al., 2019; Mitrović et al., 2023; Mittal et al., 2012; Ni et al., 2020; Padma Srivastava et al., 2012; Poljakovic et al., 2021; Sharma et al., 2011; Shinohara et al., 2009; Singh et al., 2021; Song et al., 2018; Stan et al., 2017; Tang and Li, 2019; Wang et al., 2023; Wang et al., 2021; Wang and Che, 2022; Xu et al., 2021; Xue et al., 2016; Yan et al., 2017; Zhang et al., 2017; Zhang et al., 2018; Zhang et al., 2016; Zhou et al., 2022).
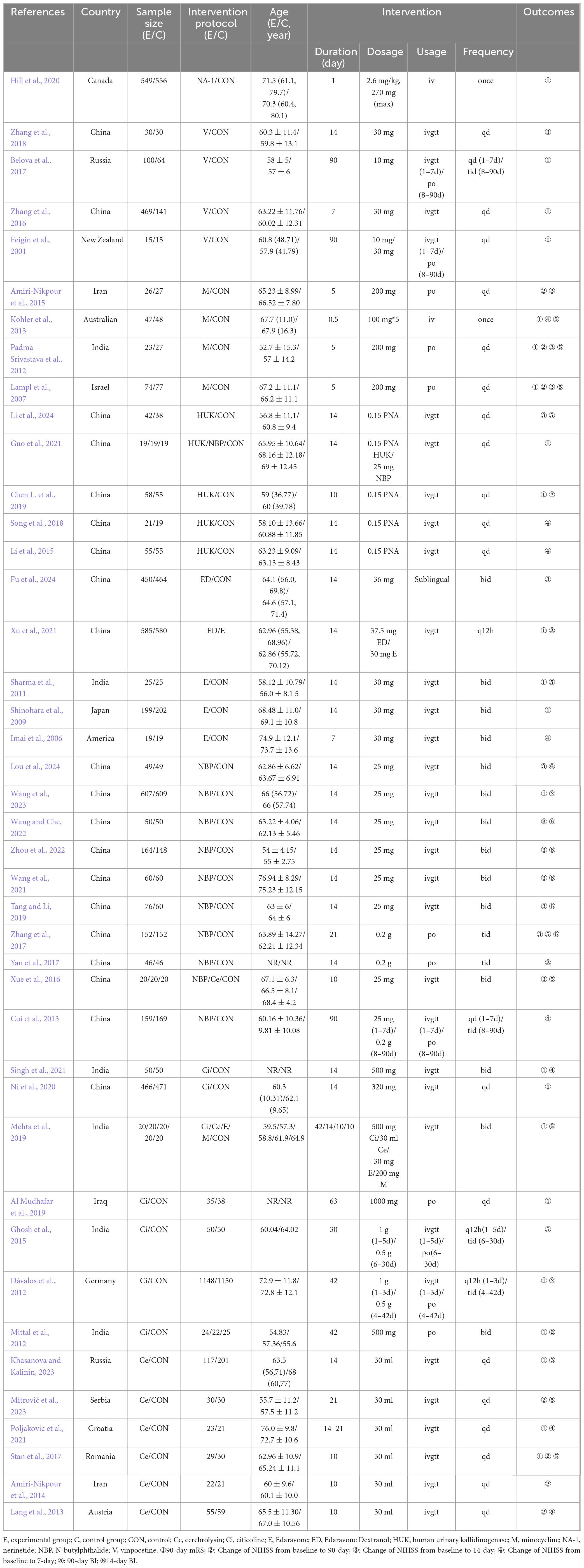
Table 1. Characteristics of included studies.
3.3 Quality evaluation
This study included 42 papers. Although the majority of studies provided detailed descriptions of the randomization process, 17 studies (40.5%) did not specify the methods used for random sequence generation. Fifteen studies (35.7%) were classified as having a low risk of bias concerning allocation concealment. Twenty-nine studies (69.0%) demonstrated a low risk of bias in the blinding of participants and personnel, while 35 studies (83.3%) were assessed as having a low risk of bias for outcome assessment. All 42 studies (100%) were considered to have a low risk of bias concerning incomplete outcome data and selective reporting. With regard to other biases, most studies declared no conflicts of interest; however, 10 studies presented an unclear risk for other potential biases. Detailed results of the bias risk assessment are provided in Figure 2.
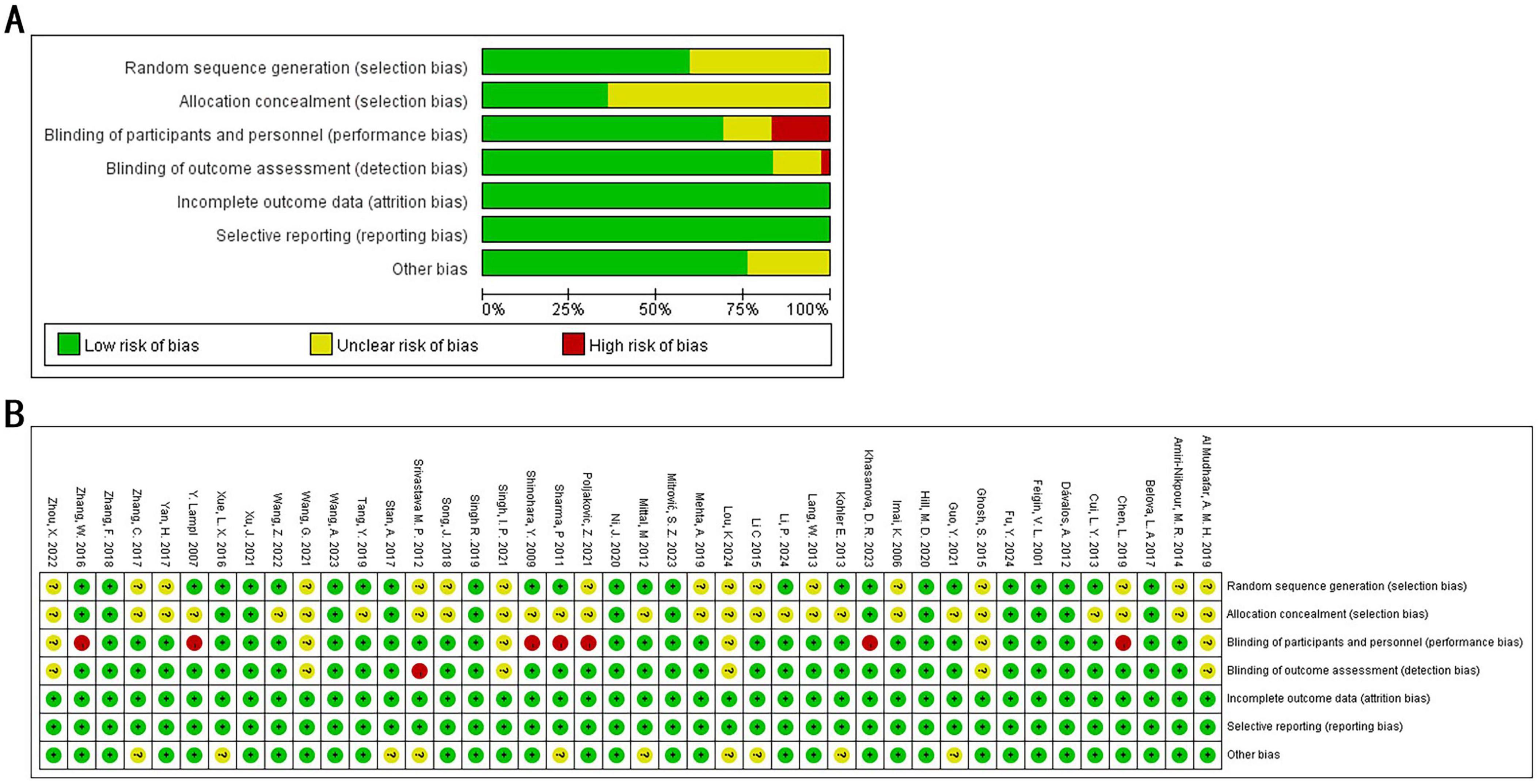
Figure 2. Quality assessment of selected studies by the Cochrane Risk of Bias Tool. (A) Risk of bias graph: each risk of bias item presented as percentages across all included studies. (B) Risk of bias summary: green indicates a low risk of bias, yellow an unclear risk of bias, and red a high risk of bias.
3.4 Pairwise meta-analysis
Pairwise meta-analyses were conducted to comprehensively compare two interventions at a time. Specifically, six distinct pairwise analyses were performed for the following outcomes: 90-day modified Rankin Scale (mRS), 90-day National Institutes of Health Stroke Scale (NIHSS), 14-day NIHSS, 7-day NIHSS, 90-day Barthel Index (BI), and 14-day BI. A summary of the results is provided in Table 2, while the detailed results of the pairwise meta-analyses are available in Supplementary Figures 1–6.
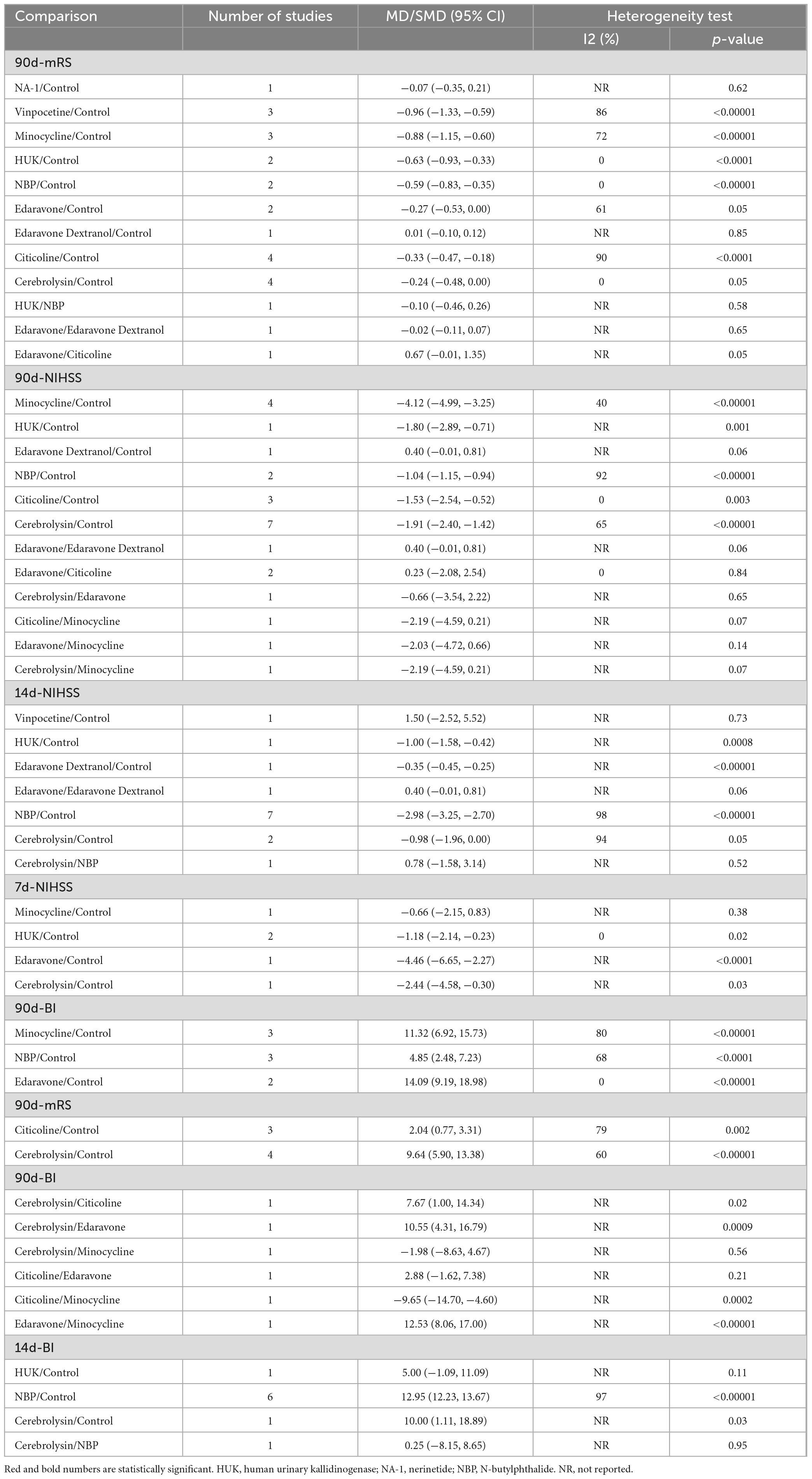
Table 2. Pairwise meta-analysis.
3.5 Network of evidence
A total of 42 randomized controlled trials (RCTs) involving 12,210 participants were included to assess the effects of various neuroprotective agents on neurological function and prognosis in ischemic stroke patients. Figure 3 depicts the network meta-analysis diagram for eligible comparisons. Blue solid circles represent the different interventions, and the size of each circle corresponds to the sample size for that intervention. Black lines connecting the blue circles indicate direct comparisons between two interventions, with the thickness of these lines reflecting the number of studies included in the comparisons. This network visualization provides a comprehensive overview of both direct and indirect comparisons among the included interventions.
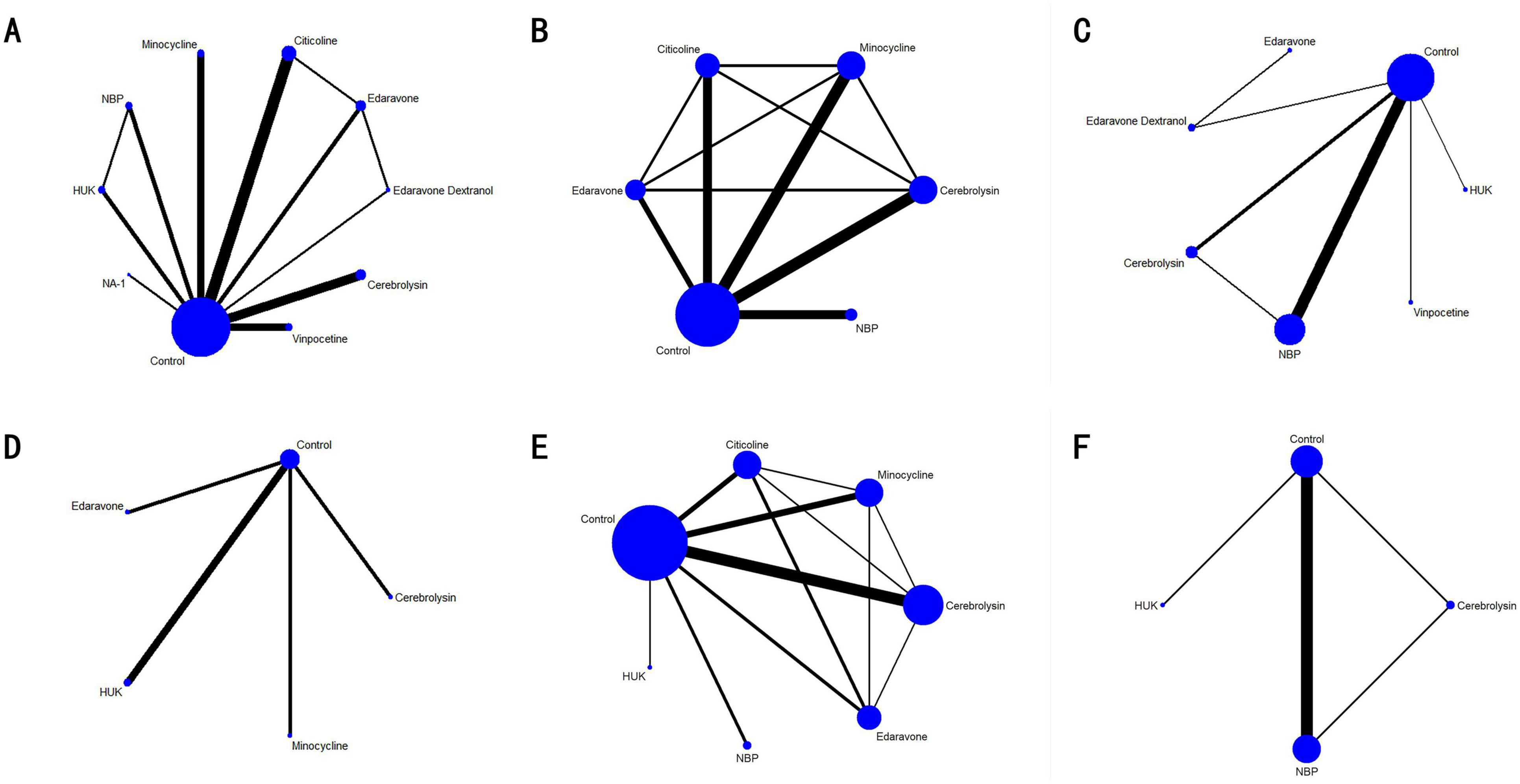
Figure 3. Network meta-analysis diagrams of eligible comparisons. (A) 90d-mRS; (B) 90d-NIHSS; (C) 14d-NIHSS; (D) 7d-NIHSS; (E) 90d-BI; (F) 14d-BI. HUK, human urinary kallidinogenase; NBP, N-butylphthalide.
3.5.1 90-day mRS
A total of 22 studies evaluated the 90-day modified Rankin Scale (mRS), including 10 interventions: Cerebrolysin, Citicoline, Edaravone, Edaravone Dextranol, HUK, Minocycline, NA-1, NBP, Vinpocetine, and a control group, with 10,057 patients included. The inconsistency model showed no significant global inconsistency (p = 0.7085, p > 0.05; Supplementary Figure 7A), so the consistency model was applied. The node-splitting method indicated good local consistency, as all p-values were greater than 0.05 (Supplementary Figure 8). The network meta-analysis (NMA) produced 45 pairwise comparisons. Compared with the control group, Minocycline (SMD = 0.61, 95% CI: 0.22 1.00), HUK (SMD = 0.59, 95% CI: 0.09 1.08), and Vinpocetine (SMD = 0.54, 95% CI: 0.16 0.92) significantly improved 90-day mRS scores for stroke patients. Other pairwise comparisons showed no statistically significant differences (p > 0.05; Figure 4). According to SUCRA analysis and ranking, NBP (SUCRA: 85.0%) was likely the most effective intervention for improving 90-day mRS outcomes in stroke patients (Figure 5A and Table 3).
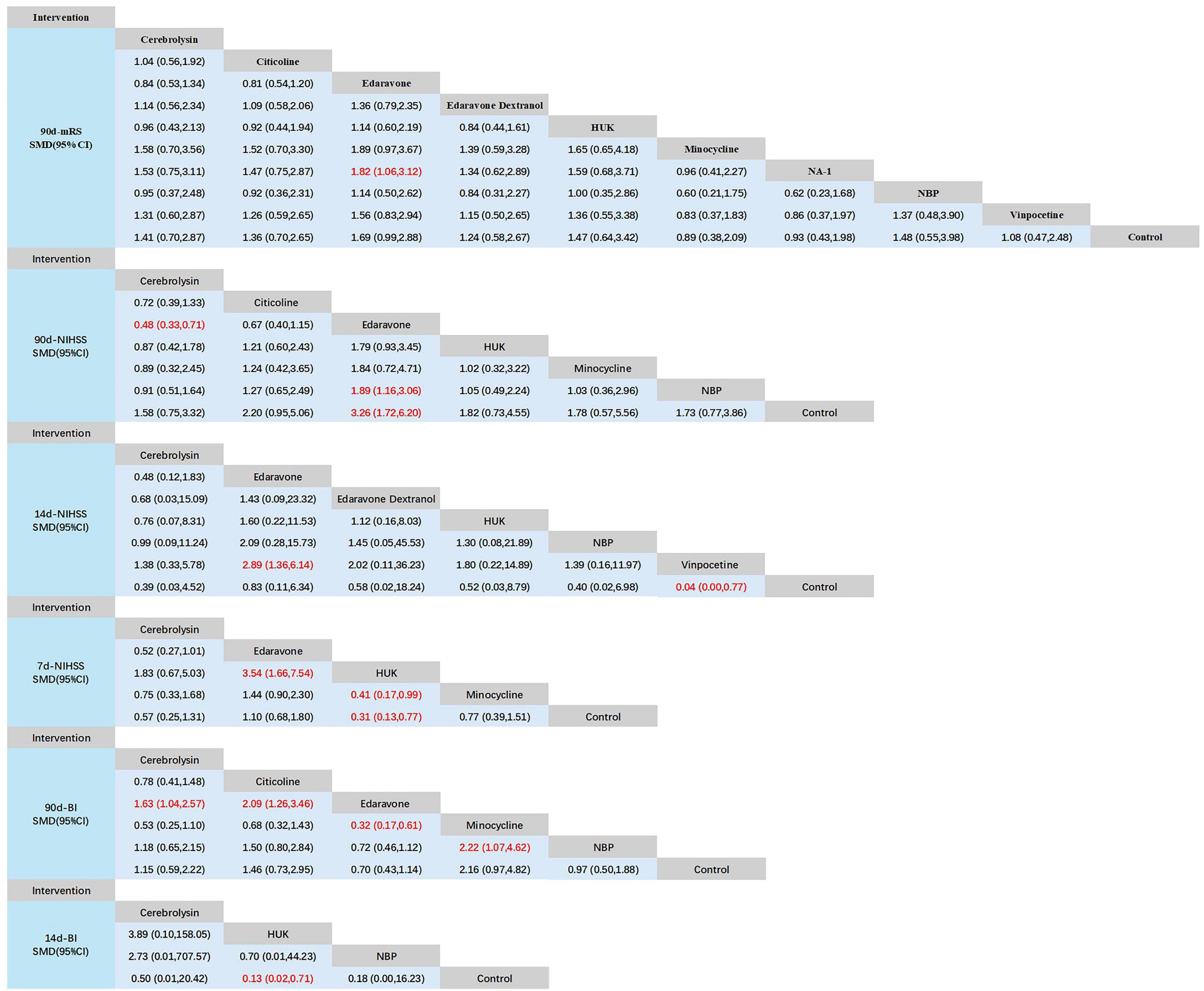
Figure 4. Network meta-analysis of head-to-head comparisons. Red and bold numbers are statistically significant. HUK, human urinary kallidinogenase; NBP, N-butylphthalide.
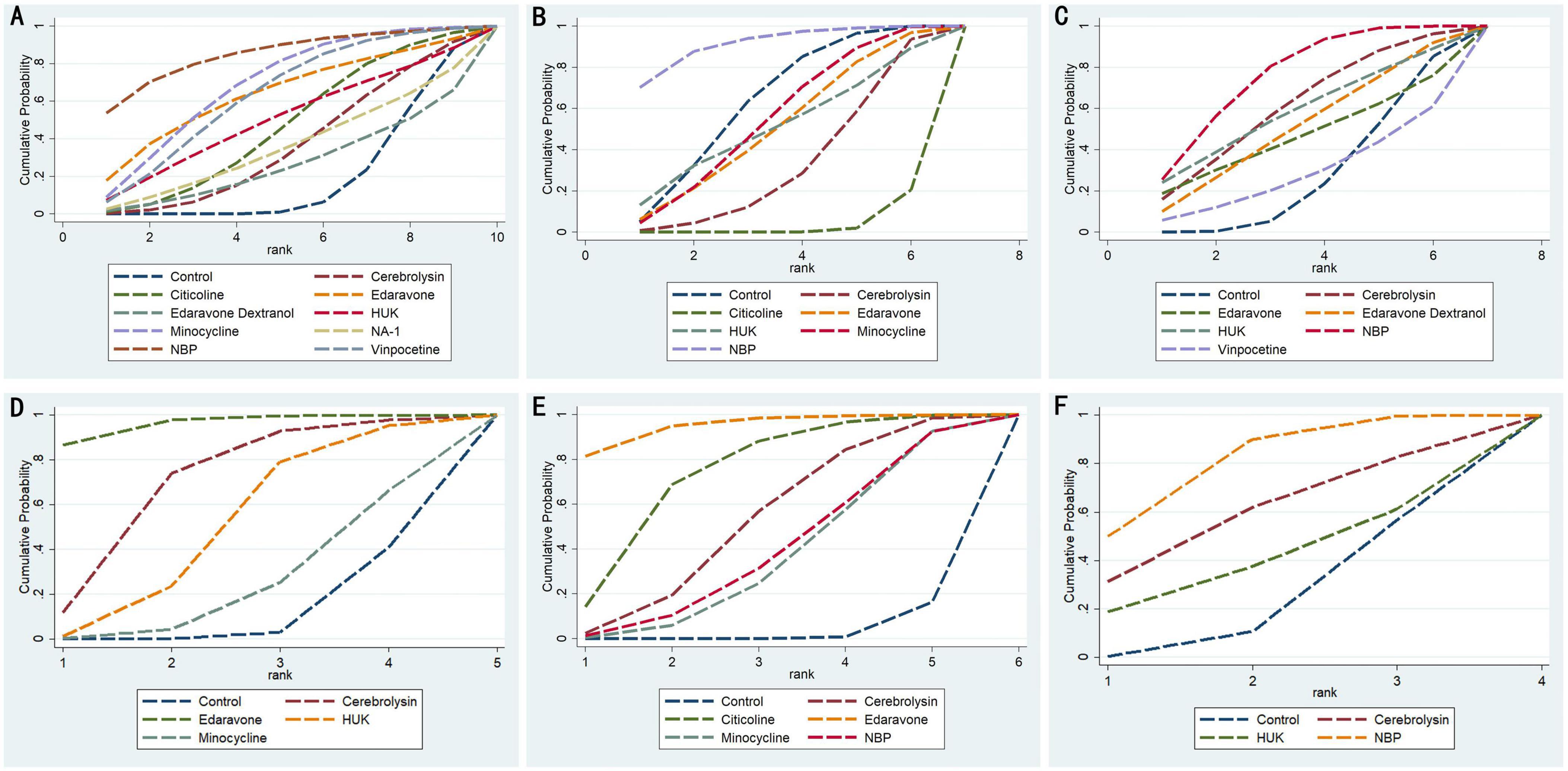
Figure 5. Cumulative probability ranking curve of different interventions. The vertical axis represents cumulative probabilities, while the horizontal axis represents ranks. (A) 90d-mRS; (B) 90d-NIHSS; (C) 14d-NIHSS; (D) 7d-NIHSS; (E) 90d-BI; (F) 14d-BI. HUK, human urinary kallidinogenase; NBP, N-butylphthalide.

Table 3. SUCRA values of different interventions for outcomes.
3.5.2 90-day NIHSS
A total of 15 studies evaluated the 90-day NIHSS, involving 7 interventions: Cerebrolysin, Citicoline, Edaravone, HUK, Minocycline, NBP, and placebo. A total of 4,591 patients were included. The inconsistency model showed no significant global inconsistency (p = 0.5899, p > 0.05; Supplementary Figure 7B), so the consistency model was applied. The node-splitting method indicated good local consistency, as all p-values were greater than 0.05 (Supplementary Figure 9). The NMA produced 21 pairwise comparisons. Compared with the control group, Cerebrolysin (SMD = −0.72, 95% CI: −1.10 −0.35), Minocycline (SMD = 0.63, 95% CI: 0.15 1.12), and NBP (SMD = 1.18, 95% CI: 0.54 1.82) significantly improved 90-day NIHSS scores for stroke patients. Other pairwise comparisons showed no statistically significant differences (p > 0.05; Figure 4). According to SUCRA analysis and ranking, NBP (SUCRA: 91.5%) was likely the most effective intervention for improving 90-day NIHSS outcomes in stroke patients (Figure 5B and Table 3).
3.5.3 14-day NIHSS
A total of studies evaluated the 14-day NIHSS, involving 7 interventions: Cerebrolysin, Edaravone, Edaravone Dextranol, HUK, NBP, Vinpocetine, and placebo. A total of 4,591 patients were included. The inconsistency model showed no significant global inconsistency (p = 0.6412, p > 0.05; Supplementary Figure 7C), so the consistency model was applied. The node-splitting method indicated good local consistency, as all p-values were greater than 0.05 (Supplementary Figure 10). The NMA produced 21 pairwise comparisons. Compared with the control group, only NBP (SMD = 1.06, 95% CI: 0.27 1.86) significantly improved 14-day NIHSS scores for stroke patients. Other pairwise comparisons showed no statistically significant differences (p > 0.05; Figure 4). According to SUCRA analysis and ranking, NBP (SUCRA: 75.9%) was likely the most effective intervention for improving 14-day NIHSS outcomes in stroke patients (Figure 5C and Table 3).
3.5.4 7-day NIHSS
A total of studies evaluated the 7-day NIHSS, involving 5 interventions: Cerebrolysin, Edaravone, HUK, Minocycline, and placebo. The total number of patients included was unspecified. There were no loops in the network, so consistency checks were not required. The NMA produced 10 pairwise comparisons. Compared with placebo, Edaravone (SMD = 1.01, 95% CI: 0.64–1.38) significantly improved 7-day NIHSS scores in stroke patients. Additionally, Edaravone showed significantly greater improvement in 7-day NIHSS compared to HUK (SMD = −0.90, 95% CI: −1.75 −0.05) and Minocycline (SMD = −1.09, 95% CI: −1.99 −0.19). No statistically significant differences were found among the other interventions (p > 0.05; Figure 4). According to SUCRA analysis and ranking, Edaravone (SUCRA: 96.1%) was likely the most effective intervention for improving 7-day NIHSS outcomes in stroke patients (Figure 5D and Table 3).
3.5.5 90-day BI
A total of 15 studies evaluated the 90-day Barthel Index (BI), involving 6 interventions: Cerebrolysin, Citicoline, Edaravone, Minocycline, NBP, and placebo, with 4,591 patients included. The inconsistency model showed no significant global inconsistency (p = 0.4253, p > 0.05; Supplementary Figure 7D), so the consistency model was applied. The node-splitting method indicated good local consistency, as all p-values were greater than 0.05 (Supplementary Figure 11). The NMA produced 15 pairwise comparisons. Compared with placebo, Cerebrolysin (SMD = 0.49, 95% CI: 0.06 0.92), Citicoline (SMD = 0.73, 95% CI: 0.26–1.21), and Edaravone (SMD = −1.12, 95% CI: −1.73 −0.52) significantly improved 90-day BI scores in stroke patients. Additionally, Edaravone showed significantly greater improvement in 90-day BI compared to Minocycline (SMD = 0.79, 95% CI: 0.10 1.49) and NBP (SMD = 0.77, 95% CI: 0.01 1.53). No statistically significant differences were found among other pairwise comparisons (p > 0.05; Figure 4). According to SUCRA analysis and ranking, Edaravone (SUCRA: 94.9%) was likely the most effective intervention for improving 90-day BI outcomes in stroke patients (Figures 5B, E, and Table 3).
3.5.6 14-day BI
A total of 7 studies evaluated the 14-day Barthel Index (BI), involving 4 interventions: Cerebrolysin, HUK, NBP, and placebo, with 1,073 patients included. The inconsistency model showed no significant global inconsistency (p = 0.5182, p > 0.05; Supplementary Figure 7E), so the consistency model was applied. The node-splitting method indicated good local consistency, as all p-values were greater than 0.05 (Supplementary Figure 12). The NMA produced 6 pairwise comparisons. Compared with placebo, NBP (SMD = −2.00, 95% CI: −3.00 −0.99) significantly improved 14-day BI scores in stroke patients. No statistically significant differences were found among other pairwise comparisons (p > 0.05; Figure 4). According to SUCRA analysis and ranking, NBP (SUCRA: 79.9%) was likely the most effective intervention for improving 14-day BI outcomes in stroke patients (Figure 5F and Table 3).
3.6 Publication bias
We used STATA 14.0 to create adjusted funnel plots for comparisons of 90-day mRS, 90-day NIHSS, 14-day NIHSS, 7-day NIHSS, 90-day BI, and 14-day BI (Figure 6). The results showed that the studies were generally centered and exhibited good symmetry, indicating a low likelihood of publication bias.
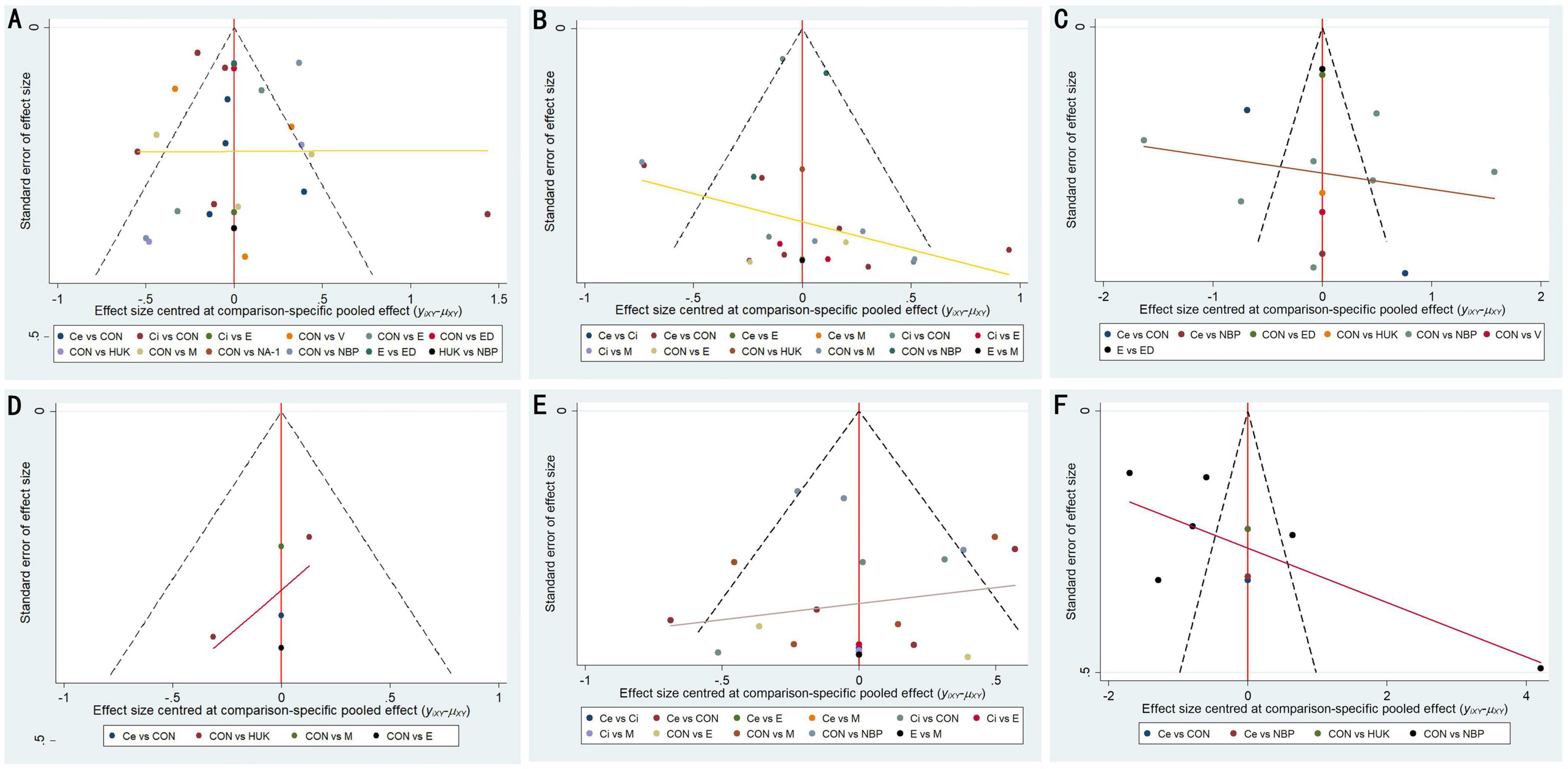
Figure 6. Funnel plot of publication bias. (A) 90d-mRS; (B) 90d-NIHSS; (C) 14d-NIHSS; (D) 7d-NIHSS; (E) 90d-BI; (F) 14d-BI. CON, control; Ce, cerebrolysin; Ci, citicoline; E, Edaravone; ED, Edaravone Dextranol; HUK, human urinary kallidinogenase; M, minocycline; NA-1, nerinetide; NBP, N-butylphthalide; V, vinpocetine.
4 Discussion
Stroke is a prevalent acute condition worldwide, leading to significant neurological impairments and poor prognoses for patients. Current treatment strategies for ischemic stroke are primarily limited to vascular recanalization therapies, which benefit only a small subset of patients. Concurrently, the pathophysiological cascade of irreversible tissue damage initiated by cerebral ischemia has become increasingly well understood (Chamorro et al., 2016; Lyden, 2021). As a result, a growing number of neuroprotective agents are under development. Despite these efforts, no neuroprotective strategy has yet been translated into a universally accepted clinical approach (Haupt et al., 2023). Although certain neuroprotective methods have demonstrated promise in preclinical settings, their clinical application largely depends on the experience of clinicians and region-specific treatment practices. There is insufficient evidence to definitively identify the most suitable neuroprotective method for AIS patients. This study utilized a network meta-analysis (NMA) to compare the efficacy of various neuroprotective agents, including Nerinetide, HUK, Edaravone, Edaravone Dextranol, Vinpocetine, NBP, Minocycline, Citicoline, and Cerebrolysin. The analysis incorporated data from 42 RCTs involving 3,017 participants and examined the efficacy of 9 neuroprotective agents. The modified Rankin Scale (mRS), a tool for assessing functional recovery following stroke or neurological injury (Bamford et al., 1989), was selected to evaluate outcomes at 90 days. The National Institutes of Health Stroke Scale (NIHSS), a standardized tool for measuring stroke-related neurological deficits (with higher scores indicating more severe damage)(Yoo et al., 2010), was used to assess changes in NIHSS scores from baseline to days 7, 14, and 90 to evaluate both early and long-term neurological improvements. Additionally, the Barthel Index (BI), which measures a person’s ability to perform activities of daily living (ADL) independently (with higher scores reflecting greater functional independence)(Wade and Collin, 1988), was used to evaluate the impact of neuroprotective agents on early and long-term daily life functions, specifically at 14 and 90 days post-stroke.
The findings of this study revealed significant differences in the efficacy of various neuroprotective agents in enhancing neurological function and prognosis for ischemic stroke patients across different recovery stages. Specifically, NBP showed notable improvements in 90-day mRS, 90-day NIHSS, and 7-day BI compared to conventional treatments, suggesting its broad applicability across different stages of recovery. Evidence suggests that the mechanism of NBP involves enhancing cerebral blood flow and exerting antioxidative effects to protect neurons and delay neuronal death (Chen X.-Q. et al., 2019; Huang et al., 2018), emphasizing its potential clinical significance for the long-term rehabilitation of AIS patients. Edaravone demonstrated notable efficacy in improving 90-day BI scores and 7-day NIHSS. Its significant effect on the 7-day NIHSS suggests its potential role in early neuroprotection, which may be attributed to its antioxidative properties, as Edaravone scavenges free radicals, reduces brain cell damage, and promotes early neurological recovery (Cao et al., 2023; Yamashita and Abe, 2024). Minocycline also showed significant improvements in 90-day modified Rankin Scale (mRS) scores, indicating its potential suitability for long-term intervention. The mechanism of action of Minocycline may involve inhibiting neuroinflammation and protecting the vascular endothelium, thereby mitigating neural damage during the chronic phase (Zhao et al., 2023). Notably, Cerebrolysin demonstrated less efficacy than NBP and Edaravone in improving 90-day and 14-day NIHSS scores, potentially due to its mechanism being more focused on enhancing short-term memory and cognitive function rather than motor function recovery in ischemic stroke patients (Mureşanu et al., 2022; Rejdak et al., 2023). Furthermore, Citicoline has been reported in some studies to effectively improve functional outcomes in patients with AIS. However, two studies reported no significant differences compared to standard treatments (Al Mudhafar et al., 2019; Dávalos et al., 2012). This study found that Citicoline’s efficacy in improving 90-day mRS scores was inferior to that of other neuroprotective agents, suggesting that its application in AIS requires further research and validation.
The findings of this study hold significant clinical value for the treatment of AIS patients. Considering the differences in short- and long-term effects of various drugs, it is recommended that clinicians tailor the choice of neuroprotective agents based on the patient’s specific condition and stage of recovery. First, NBP and Edaravone demonstrated excellent performance in long-term follow-up scores, indicating their potential to improve long-term prognosis after stroke. These agents may be particularly suitable for maintenance therapy following early intervention. Second, Edaravone exhibited superior efficacy in NIHSS scores within the first 7 days compared to other drugs, suggesting its potential for providing rapid neuroprotective effects in acute stroke treatment. Therefore, during the acute phase—especially in the early stages following stroke onset—the use of Edaravone may help maximize neuroprotection and reduce early disability rates (Kimura et al., 2012). Additionally, the results of this study suggest that neuroprotective agents are more effective when administered as early interventions in stroke patients. This observation aligns with the physiological characteristics of brain tissue, which are more responsive to treatment and exhibit greater recovery potential during the early stages. Furthermore, preliminary findings from existing studies indicate that the efficacy of neuroprotective strategies often surpasses that of single-drug approaches in achieving better long-term outcomes (Li et al., 2022; Tran et al., 2022). Given the complexity of neurological recovery and the substantial individual variability observed in stroke patients, future clinical applications should incorporate factors such as stroke type, onset timing, lesion location, and the severity of neurological damage. Such an approach would facilitate the selection of the most suitable drug combinations or individualized treatment plans, thereby maximizing the potential for optimal clinical outcomes.
This study provides preliminary evidence regarding the comparative efficacy of neuroprotective agents through NMA, including improvements in 90-day mRS and NIHSS; however, several limitations remain. First, the included studies exhibited imbalanced sample sizes, with many being small-scale trials, potentially compromising the stability and generalizability of the findings. Second, although NMA facilitates the comparison of multiple interventions, it predominantly relies on indirect comparisons across studies rather than direct head-to-head comparisons among all drugs. Third, this study was unable to fully eliminate potential biases present in the included trials, particularly those related to random sequence generation and allocation concealment. The low methodological quality of certain studies—such as a lack of blinding, high dropout rates, and inadequate randomization—may have influenced the final outcomes. Finally, this study did not conduct a detailed analysis of the long-term safety and adverse effects of neuroprotective agents. Although some trials reported mild adverse effects, such as dizziness and headache, systematic evaluations of adverse events were lacking. Future research should incorporate safety data to further validate the risk-benefit profiles of neuroprotective agents, thereby providing more comprehensive guidance for their safe clinical use. To address the aforementioned limitations, future research should prioritize expanding sample sizes and including multicenter, highly heterogeneous populations to enhance the representativeness and generalizability of findings. Designing head-to-head comparative studies is crucial for clarifying the relative efficacy priorities of different drugs. Additionally, further exploration of the effects of various drug combinations is warranted to evaluate their potential synergistic effects in improving neurological function. While some evidence suggests that early combination therapy with neuroprotective agents may yield superior long-term outcomes compared to monotherapy, the potential side effects and higher costs associated with prolonged combination regimens must be carefully considered. The demand for neuroprotective agents may vary across different recovery stages, making stratified treatment strategies tailored to specific phases a promising avenue for future research. For instance, acute-phase drugs such as Edaravone may be more effective in mitigating early damage, whereas medications like NBP might better support long-term functional recovery during rehabilitation. Finally, given the significant impact of neuroprotective agents on the long-term quality of life for stroke patients, future studies should incorporate more comprehensive assessments of quality of life, including factors such as depression, anxiety, and social participation. Such evaluations would provide a more holistic understanding of the effects of neuroprotective agents on stroke recovery and contribute to the development of optimized post-stroke rehabilitation strategies.
5 Conclusion
This network meta-analysis offers a comprehensive comparison of the efficacy of various neuroprotective agents in enhancing neurological function and prognosis for patients with ischemic stroke. The evidence from this study indicates that different drugs provide distinct benefits at specific stages of recovery. NBP demonstrated notable efficacy in improving 90d-mRS and 90d-NIHSS, highlighting its potential in long-term rehabilitation. Edaravone exhibited significant superiority in improving 7d-NIHSS scores, suggesting its potential role in early neuroprotection. These findings offer valuable insights for individualized clinical treatment. To further validate the efficacy and safety of different neuroprotective agents, future research should include larger sample sizes, involve multicenter and large-scale randomized controlled trials, and assess the effects of combination therapies. Such efforts will help confirm and strengthen the findings of this study. In conclusion, this research underscores the substantial value of neuroprotective agents in enhancing neurological function and prognosis for patients with ischemic stroke.
Data availability statement
The original contributions presented in this study are included in this article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
YW: Data curation, Methodology, Writing – original draft, Writing – review and editing. ML: Data curation, Methodology, Writing – original draft, Writing – review and editing. YJ: Data curation, Methodology, Supervision, Writing – review and editing. QJ: Funding acquisition, Supervision, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the National Natural Science Foundation of China (Nos. 82071553, 81201016, and 81272027), the Natural Science Foundation of Jiangsu Province (BK20151277), Jiangsu Provincial Medical Innovation Center (CXZX202212), and Jiangsu Provincial Research Hospital (YJXYY202204).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2024.1530987/full#supplementary-material
References
Agarwal, S., and Patel, B. M. (2017). Is aura around citicoline fading? A systemic review. Indian J. Pharmacol. 49, 4–9. doi: 10.4103/0253-7613.201037
Al Mudhafar, A. M. H., Hassoun, H. K., Sameer, A., Hadi, N. R., and Allebban, Z. (2019). Effect of citicoline on cerebral hemodynamics and vasoreactivity using transcranial Doppler in acute ischemic stroke patients: clinical trial. Int. J. Pharm. Res. 11, 262–269. doi: 10.31838/ijpr/2019.11.02.045
Amiri-Nikpour, M. R., Nazarbaghi, S., Ahmadi-Salmasi, B., Mokari, T., Tahamtan, U., and Rezaei, Y. (2014). Cerebrolysin effects on neurological outcomes and cerebral blood flow in acute ischemic stroke. Neuropsychiatr. Dis. Treat. 10, 2299–2306. doi: 10.2147/ndt.S75304
Amiri-Nikpour, M. R., Nazarbaghi, S., Hamdi-Holasou, M., and Rezaei, Y. (2015). An open-label evaluator-blinded clinical study of minocycline neuroprotection in ischemic stroke: gender-dependent effect. Acta Neurol. Scand. 131, 45–50. doi: 10.1111/ane.12296
Bamford, J. M., Sandercock, P. A., Warlow, C. P., and Slattery, J. (1989). Interobserver agreement for the assessment of handicap in stroke patients. Stroke 20:828. doi: 10.1161/01.str.20.6.828
Belova, L. A., Mashin, V. V., Proshin, A. N., Ovsyannicova, A. N., and Kostishko, B. B. (2017). Possibilities of cavinton therapy regimen for infusions and cavinton comforte in acute and early recovery periods after ischemic stroke. Zh. Nevrol. Psihiatr. Im. S S Korsakova 117, 51–58. doi: 10.17116/jnevro20171179151-58
Bornstein, N. M., Guekht, A., Vester, J., Heiss, W.-D., Gusev, E., Hömberg, V., et al. (2018). Safety and efficacy of Cerebrolysin in early post-stroke recovery: a meta-analysis of nine randomized clinical trials. Neurol. Sci. 39, 629–640. doi: 10.1007/s10072-017-3214-0
Cao, Y., Yue, X., Jia, M., and Wang, J. (2023). Neuroinflammation and anti-inflammatory therapy for ischemic stroke. Heliyon 9:e17986. doi: 10.1016/j.heliyon.2023.e17986
Chamorro, Á, Dirnagl, U., Urra, X., and Planas, A. M. (2016). Neuroprotection in acute stroke: targeting excitotoxicity, oxidative and nitrosative stress, and inflammation. Lancet Neurol. 15, 869–881. doi: 10.1016/s1474-4422(16)00114-9
Chen, L., Geng, L., Chen, J., Yan, Y., Yang, L., Zhao, J., et al. (2019). Effects of Urinary Kallidinogenase on NIHSS score, mRS score, and fasting glucose levels in acute ischemic stroke patients with abnormal glucose metabolism: a prospective cohort study. Medicine (United States) 98:e17008. doi: 10.1097/MD.0000000000017008
Chen, X.-Q., Qiu, K., Liu, H., He, Q., Bai, J.-H., and Lu, W. (2019). Application and prospects of butylphthalide for the treatment of neurologic diseases. Chinese Med. J. 132, 1467–1477. doi: 10.1097/cm9.0000000000000289
Cui, L. Y., Zhu, Y. C., Gao, S., Wang, J. M., Peng, B., Ni, J., et al. (2013). Ninety-day administration of dl-3-n-butylphthalide for acute ischemic stroke: a randomized, double-blind trial. Chinese Med. J. 126, 3405–3410. doi: 10.3760/cma.j.issn.0366-6999.20123240
Dávalos, A., Alvarez-Sabín, J., Castillo, J., Díez-Tejedor, E., Ferro, J., Martínez-Vila, E., et al. (2012). Citicoline in the treatment of acute ischaemic stroke: an international, randomised, multicentre, placebo-controlled study (ICTUS trial). Lancet 380, 349–357. doi: 10.1016/S0140-6736(12)60813-7
Feigin, V. L., Brainin, M., Norrving, B., Martins, S., Sacco, R. L., Hacke, W., et al. (2022). World Stroke Organization (WSO): global stroke fact sheet 2022. Int. J. Stroke 17, 18–29. doi: 10.1177/17474930211065917
Feigin, V. L., Doronin, B. M., Popova, T. F., Gribatcheva, E. V., and Tchervov, D. V. (2001). Vinpocetine treatment in acute ischaemic stroke: a pilot single-blind randomized clinical trial. Eur. J. Neurol. 8, 81–85. doi: 10.1046/j.1468-1331.2001.00181.x
Fu, Y., Wang, A., Tang, R., Li, S., Tian, X., Xia, X., et al. (2024). Sublingual edaravone dexborneol for the treatment of acute ischemic stroke: the TASTE-SL randomized clinical trial. JAMA Neurol. 81, 319–326. doi: 10.1001/jamaneurol.2023.5716
GBD (2021). Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 20, 795–820. doi: 10.1016/s1474-4422(21)00252-0
Ghosh, S., Ghosh, K. C., Bhattacharyya, R., and Mondal, G. P. (2015). The effect of citicoline in stroke: a comparative study from eastern part of India. Ann. Indian Acad. Neurol. 18, S36–S37.
Goyal, M., Menon, B. K., Zwam, W. H., Dippel, D. W. J., Mitchell, P. J., Demchuk, A. M., et al. (2016). Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet (London, England) 387, 1723–1731. doi: 10.1016/s0140-6736(16)00163-x
Guo, Y., Abdoulaye, I. A., Liu, F., Wang, J., Tian, X., Yu, D., et al. (2021). N-Butylphthalide vs. human urinary kallidinogenase for the treatment of acute ischemic stroke: functional outcome and impact on serum VEGF and TNF-α expressions. Ann. Clin. Lab. Sci. 51, 503–511.
Haupt, M., Gerner, S. T., Bähr, M., and Doeppner, T. R. (2023). Neuroprotective strategies for ischemic stroke-future perspectives. Int. J. Mol. Sci. 24:4334. doi: 10.3390/ijms24054334
Hill, M. D., Goyal, M., Menon, B. K., Nogueira, R. G., McTaggart, R. A., Demchuk, A. M., et al. (2020). Efficacy and safety of nerinetide for the treatment of acute ischaemic stroke (ESCAPE-NA1): a multicentre, double-blind, randomised controlled trial. Lancet 395, 878–887. doi: 10.1016/S0140-6736(20)30258-0
Huang, L., Wang, S., Ma, F., Zhang, Y., Peng, Y., Xing, C., et al. (2018). From stroke to neurodegenerative diseases: the multi-target neuroprotective effects of 3-n-butylphthalide and its derivatives. Pharmacol. Res. 135, 201–211. doi: 10.1016/j.phrs.2018.08.007
Hutton, B., Salanti, G., Caldwell, D. M., Chaimani, A., Schmid, C. H., Cameron, C., et al. (2015). The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann. Intern. Med. 162, 777–784. doi: 10.7326/m14-2385
Imai, K., Mori, T., Izumoto, H., Takabatake, N., Kunieda, T., and Watanabe, M. (2006). Hyperbaric oxygen combined with intravenous edaravone for treatment of acute embolic stroke: a pilot clinical trial. Neurol. Med. Chir. 46, 373–378. doi: 10.2176/nmc.46.373
Khasanova, D. R., and Kalinin, M. N. (2023). Cerebrolysin as an Early Add-on to Reperfusion Therapy: Risk of Hemorrhagic Transformation after Ischemic Stroke (CEREHETIS), a prospective, randomized, multicenter pilot study. BMC Neurol. 23:121. doi: 10.1186/s12883-023-03159-w
Kimura, K., Aoki, J., Sakamoto, Y., Kobayashi, K., Sakai, K., Inoue, T., et al. (2012). Administration of edaravone, a free radical scavenger, during t-PA infusion can enhance early recanalization in acute stroke patients–a preliminary study. J. Neurol. Sci. 313, 132–136. doi: 10.1016/j.jns.2011.09.006
Kohler, E., Prentice, D. A., Bates, T. R., Hankey, G. J., Claxton, A., Van Heerden, J., et al. (2013). Intravenous minocycline in acute stroke: a randomized, controlled pilot study and meta-analysis. Stroke 44, 2493–2499. doi: 10.1161/STROKEAHA.113.000780
Lampl, Y., Boaz, M., Gilad, R., Lorberboym, M., Dabby, R., Rapoport, A., et al. (2007). Minocycline treatment in acute stroke: an open-label, evaluator-blinded study. Neurology 69, 1404–1410. doi: 10.1212/01.wnl.0000277487.04281.db
Lang, W., Stadler, C. H., Poljakovic, Z., and Fleet, D. (2013). A prospective, randomized, placebo-controlled, double-blind trial about safety and efficacy of combined treatment with alteplase (rt-PA) and Cerebrolysin in acute ischaemic hemispheric stroke. Int. J. Stroke 8, 95–104. doi: 10.1111/j.1747-4949.2012.00901.x
Li, C., Zha, O. G., He, Q. Y., Wu, Y. Z., Wang, T. S., and Teng, J. F. (2015). Study on the clinical efficacy of Human Urinary Kalllikrein in the treatment of acute cerebral infarction according to TOAST classification. Pak. J. Pharm. Sci. 28, 1505–1510.
Li, K., Zhang, Q., Lu, X., and Yao, S. (2022). Effects of butylphthalide sodium chloride injection combined with edaravone dexborneol on neurological function and serum inflammatory factor levels in sufferers having acute ischemic stroke. J. Healthc. Eng. 2022:1509407. doi: 10.1155/2022/1509407
Li, P., Lu, H., Shi, X., Yan, J., Zhou, L., Yang, J., et al. (2024). Protective effects of human urinary kallidinogenase against corticospinal tract damage in acute ischemic stroke patients. Neuroreport 35, 431–438. doi: 10.1097/WNR.0000000000002028
Lou, K., Lu, D., Pan, Y., Le, Y., Yan, H., Fu, H., et al. (2024). Effects of Shuxuetong combined with butylphthalide on neurological function and inflammatory response in patients with acute ischemic stroke. J. Chin. Pharm. Sci. 33, 241–247. doi: 10.5246/jcps.2024.03.019
Lyden, P. D. (2021). Cerebroprotection for acute ischemic stroke: looking ahead. Stroke 52, 3033–3044. doi: 10.1161/strokeaha.121.032241
Malhotra, K., Chang, J. J., Khunger, A., Blacker, D., Switzer, J. A., Goyal, N., et al. (2018). Minocycline for acute stroke treatment: a systematic review and meta-analysis of randomized clinical trials. J. Neurol. 265, 1871–1879. doi: 10.1007/s00415-018-8935-3
Mehta, A., Mahale, R., Buddaraju, K., Javali, M., Acharya, P., and Srinivasa, R. (2019). Efficacy of neuroprotective drugs in acute ischemic stroke: is it helpful? J. Neurosci. Rural Pract. 10, 576–581. doi: 10.1055/s-0039-1700790
Menon, B. K., Buck, B. H., Singh, N., Deschaintre, Y., Almekhlafi, M. A., Coutts, S. B., et al. (2022). Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet (London, England) 400, 161–169. doi: 10.1016/s0140-6736(22)01054-6
Mitrović, S. Z., Konstantinović, L. M., Miler Jerković, V., Dedijer-Dujović, S., and Djordjević, O. C. (2023). Extended poststroke rehabilitation combined with cerebrolysin promotes upper limb motor recovery in early subacute phase of rehabilitation: a randomized clinical study. Medicina (Kaunas, Lithuania) 59:291. doi: 10.3390/medicina59020291
Mittal, M., Goel, D., Bansal, K. K., and Puri, P. (2012). Edaravone - Citicoline comparative study in acute ischemic stroke (ECCS- AIS). J. Assoc. Phys. India 60, 36–38.
Mureşanu, D. F., Popa, L. L., Chira, D., Dăbală, V., Hapca, E., Vlad, I., et al. (2022). Role and impact of cerebrolysin for ischemic stroke care. J. Clin. Med. 11:1273. doi: 10.3390/jcm11051273
Ni, J., Chen, H., Chen, G., Ji, Y., Yi, F., Zhang, Z., et al. (2020). Efficacy and safety of cinepazide maleate injection in patients with acute ischemic stroke: a multicenter, randomized, double-blind, placebo-controlled trial. BMC Neurol. 20:282. doi: 10.1186/s12883-020-01844-8
Padma Srivastava, M. V., Bhasin, A., Bhatia, R., Garg, A., Gaikwad, S., Prasad, K., et al. (2012). Efficacy of minocycline in acute ischemic stroke: a single-blinded, placebo-controlled trial. Neurol. India 60, 23–28. doi: 10.4103/0028-3886.93584
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. doi: 10.1136/bmj.n71
Panda, P. K., Ramachandran, A., Panda, P., and Sharawat, I. K. (2022). Safety and efficacy of vinpocetine as a neuroprotective agent in acute ischemic stroke: a systematic review and meta-analysis. Neurocrit. Care 37, 314–325. doi: 10.1007/s12028-022-01499-y
Poljakovic, Z., Supe, S., Ljevak, J., Starcevic, K., Peric, I., Blazevic, N., et al. (2021). Efficacy and safety of Cerebrolysin after futile recanalisation therapy in patients with severe stroke. Clin. Neurol. Neurosurg. 207:106767. doi: 10.1016/j.clineuro.2021.106767
Rejdak, K., Sienkiewicz-Jarosz, H., Bienkowski, P., and Alvarez, A. (2023). Modulation of neurotrophic factors in the treatment of dementia, stroke and TBI: effects of cerebrolysin. Med. Res. Rev. 43, 1668–1700. doi: 10.1002/med.21960
Rouse, B., Chaimani, A., and Li, T. (2017). Network meta-analysis: an introduction for clinicians. Intern. Emerg. Med. 12, 103–111. doi: 10.1007/s11739-016-1583-7
Savović, J., Weeks, L., Sterne, J. A. C., Turner, L., Altman, D. G., Moher, D., et al. (2014). Evaluation of the Cochrane Collaboration’s tool for assessing the risk of bias in randomized trials: focus groups, online survey, proposed recommendations and their implementation. Syst. Rev. 3:37. doi: 10.1186/2046-4053-3-37
Secades, J. J., Alvarez-Sabín, J., Castillo, J., Díez-Tejedor, E., Martínez-Vila, E., Ríos, J., et al. (2016). Citicoline for acute ischemic stroke: a systematic review and formal meta-analysis of randomized, double-blind, and placebo-controlled trials. J. Stroke Cerebrovasc. Dis. 25, 1984–1996. doi: 10.1016/j.jstrokecerebrovasdis.2016.04.010
Sharma, P., Sinha, M., Shukla, R. K., Garg, R., Verma, R., and Singh, M. K. (2011). A randomized controlled clinical trial to compare the safety and efficacy of edaravone in acute ischemic stroke. Ann. Indian Acad. Neurol. 14, 103–106. doi: 10.4103/0972-2327.82794
Shi, P.-Y., Zhou, X.-C., Yin, X.-X., Xu, L.-L., Zhang, X.-M., and Bai, H.-Y. (2016). Early application of citicoline in the treatment of acute stroke: a meta-analysis of randomized controlled trials. J. Huazhong Univ. Sci. 36, 270–277. doi: 10.1007/s11596-016-1579-6
Shim, S., Yoon, B.-H., Shin, I.-S., and Bae, J.-M. (2017). Network meta-analysis: application and practice using Stata. Epidemiol. Health 39:e2017047. doi: 10.4178/epih.e2017047
Shinohara, Y., Saito, I., Kobayashi, S., and Uchiyama, S. (2009). Edaravone (Radical Scavenger) versus sodium ozagrel (Antiplatelet Agent) in acute noncardioembolic ischemic stroke (EDO Trial). Cerebrovasc. Dis. 27, 485–492. doi: 10.1159/000210190
Singh, I. P., Kaur, K., Bhatia, L., and Pal, A. (2021). Defining outcome in acute stroke patients using barthel index and modified rankin scale treated with neuroprotective agents. Asian J. Pharm. Clin. Res. 14, 59–61. doi: 10.22159/ajpcr.2021.v14i8.40959
Song, J., Lyu, Y., Wang, M., Zhang, J., Gao, L., and Tong, X. (2018). treatment of human urinary Kallidinogenase combined with Maixuekang capsule promotes good functional outcome in ischemic stroke. Front. Physiol. 9:84. doi: 10.3389/fphys.2018.00084
Stan, A., Birle, C., Blesneag, A., and Iancu, M. (2017). Cerebrolysin and early neurorehabilitation in patients with acute ischemic stroke: a prospective, randomized, placebo-controlled clinical study. J. Med. Life 10, 216–222.
Tang, Y., and Li, N. (2019). Effect of combination of ganglioside and butylphthalide on serum tau protein content and prognosis in stroke patients. Chin. J. Pharm. Biotechnol. 26, 494–497. doi: 10.19526/j.cnki.1005-8915.20190606
Tran, L., Alvarez, X. A., Le, H.-A., Nguyen, D.-A., Le, T., Nguyen, N., et al. (2022). Clinical efficacy of cerebrolysin and cerebrolysin plus nootropics in the treatment of patients with acute ischemic stroke in Vietnam. CNS Neurol. Disord. Drug Targets 21, 621–630. doi: 10.2174/1871527320666210820091655
Tufanaru, C., Munn, Z., Stephenson, M., and Aromataris, E. (2015). Fixed or random effects meta-analysis? Common methodological issues in systematic reviews of effectiveness. Int. J. Evid. Based Healthc. 13, 196–207. doi: 10.1097/xeb.0000000000000065
Wade, D. T., and Collin, C. (1988). The Barthel ADL index: a standard measure of physical disability? Int. Disabil. Stud. 10, 64–67. doi: 10.3109/09638288809164105
Wan, M., Yang, K., Zhang, G., Yang, C., Wei, Y., He, Y., et al. (2024). Efficacy, safety, and cost-effectiveness analysis of Cerebrolysin in acute ischemic stroke: a rapid health technology assessment. Medicine 103:e37593. doi: 10.1097/md.0000000000037593
Wang, A., Jia, B., Zhang, X., Huo, X., Chen, J., Gui, L., et al. (2023). Efficacy and safety of butylphthalide in patients with acute ischemic stroke: a randomized clinical trial. JAMA Neurol. 80, 851–859. doi: 10.1001/jamaneurol.2023.1871
Wang, G., Ma, D., and Wang, R. (2021). Effect of butylphthalide on serum CRP, PARK7, NT-3 and neurological function in patients with acute cerebral infarction. Am. J. Transl. Res. 13, 10388–10395.
Wang, Z., and Che, J. (2022). Effectiveness of alteplase intravenous thrombolysis combined with butylphthalide in patients with acute severe cerebral infarction. Folia Neuropathol. 60, 421–426. doi: 10.5114/fn.2022.118787
Xu, J., Wang, A., Meng, X., Yalkun, G., Xu, A., Gao, Z., et al. (2021). Edaravone dexborneol versus edaravone alone for the treatment of acute ischemic stroke: a phase III, randomized, double-blind, comparative trial. Stroke 52, 772–780. doi: 10.1161/STROKEAHA.120.031197
Xue, L. X., Zhang, T., Zhao, Y. W., Geng, Z., Chen, J. J., and Chen, H. (2016). Efficacy and safety comparison of DL-3-n-butylphthalide and cerebrolysin: effects on neurological and behavioral outcomes in acute ischemic stroke. Exp. Ther. Med. 11, 2015–2020. doi: 10.3892/etm.2016.3139
Yamashita, T., and Abe, K. (2024). Update on antioxidant therapy with edaravone: expanding applications in neurodegenerative diseases. Int. J. Mol. Sci. 25:2945. doi: 10.3390/ijms25052945
Yan, H., Xi, H., Wang, H., Zhang, F., and Cao, D. (2017). Clinical application of butylphthalide in massive cerebral infarction treatment. Int. J. Clin. Exp. Med. 10, 3757–3761.
Yanık, T., and Yanık, B. (2024). Current neuroprotective agents in stroke. Tur. J. Phys. Med. Rehabil. 70, 157–163. doi: 10.5606/tftrd.2024.15287
Yoo, A. J., Romero, J., Hakimelahi, R., Nogueira, R. G., Rabinov, J. D., Pryor, J. C., et al. (2010). Predictors of functional outcome vary by the hemisphere of involvement in major ischemic stroke treated with intra-arterial therapy: a retrospective cohort study. BMC Neurol. 10:25. doi: 10.1186/1471-2377-10-25
Zhang, C., Zhao, S., Zang, Y., Gu, F., Mao, S., Feng, S., et al. (2017). The efficacy and safety of Dl-3n-butylphthalide on progressive cerebral infarction: a randomized controlled STROBE study. Medicine 96:e7257. doi: 10.1097/MD.0000000000007257
Zhang, F., Yan, C., Wei, C., Yao, Y., Ma, X., Gong, Z., et al. (2018). Vinpocetine inhibits NF-κB-dependent inflammation in acute ischemic stroke patients. Transl. Stroke Res. 9, 174–184. doi: 10.1007/s12975-017-0549-z
Zhang, W., Huang, Y., Li, Y., Tan, L., Nao, J., Hu, H., et al. (2016). Efficacy and safety of vinpocetine as part of treatment for acute cerebral infarction: a randomized, open-label, controlled, multicenter CAVIN (Chinese Assessment for Vinpocetine in Neurology) trial. Clin. Drug Investig. 36, 697–704. doi: 10.1007/s40261-016-0415-x
Zhao, K., Wang, P., Tang, X., Chang, N., Shi, H., Guo, L., et al. (2023). The mechanisms of minocycline in alleviating ischemic stroke damage and cerebral ischemia-reperfusion injury. Eur. J. Pharmacol. 955:175903. doi: 10.1016/j.ejphar.2023.175903
Keywords: neuroprotective agents, network meta-analysis, N-butylphthalide, Edaravone, neurological function, stroke rehabilitation
Citation: Wang Y, Li M, Jiang Y and Ji Q (2025) Comparative efficacy of neuroprotective agents for improving neurological function and prognosis in acute ischemic stroke: a network meta-analysis. Front. Neurosci. 18:1530987. doi: 10.3389/fnins.2024.1530987
Received: 19 November 2024; Accepted: 13 December 2024;
Published: 06 January 2025.
Edited by:
Magdalena Sowa-Kućma, University of Rzeszów, PolandReviewed by:
Marcin Siwek, Jagiellonian University, PolandDhriti Majumder, Alliance University, India
Copyright © 2025 Wang, Li, Jiang and Ji. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qiuhong Ji, amlxaXVob25nQG50dS5lZHUuY24=
†These authors have contributed equally to this work