
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CORRECTION article
Front. Neurosci. , 13 May 2024
Sec. Brain Imaging Methods
Volume 18 - 2024 | https://doi.org/10.3389/fnins.2024.1418734
 Gloria P. Baena-Caldas1,2,3,4
Gloria P. Baena-Caldas1,2,3,4 Juan F. Mier-García4,5*
Juan F. Mier-García4,5* Dylan P. Griswold6,7,8
Dylan P. Griswold6,7,8 Adriana M. Herrera-Rubio3
Adriana M. Herrera-Rubio3 Ximara Peckham9
Ximara Peckham9A corrigendum on
Anatomical variations of the atlas arches: prevalence assessment, systematic review and proposition for an updated classification system
by Baena-Caldas, G. P., Mier-García, J. F., Griswold, D. P., Herrera-Rubio, A. M., and Peckham, X. (2024). Front. Neurosci. 18:1348066. doi: 10.3389/fnins.2024.1348066
In the published article, there was an error in the caption for Figure 4 as published. The legend previously stated:
Recommended enhancements to the Currarino classification of atlas arch variations. Type A – 1 midline posterior cleft in the atlas, Type A – 2 small ossicle within the midline posterior cleft, Type B – 1 partial unilateral posterior cleft, Type B – 2 complete absence of one of the posterior hemiarches, Type C – 1 bilateral partial defect in the posterior arch of the atlas with preservation of the posterior tubercle, Type C – 2 complete absence of one posterior hemiarch, partial defect in the other hemiarch, arm and posterior tubercle are preserved, Type D −1 bilateral complete absence of both posterior hemiarches with a single posterior midline tubercle present, Type D – 2 bilateral absence of both posterior arms, absent posterior tubercle, Type D – 3 unilateral absence of one posterior hemiarch, absence of the contralateral arm and posterior tubercle, Type E – 1 complete absence of the posterior arch and absence of the posterior tubercle, Type E – 2 absence of the posterior arch, both posterior arms are preserved with absence of the posterior tubercle, Type E – 3 absence of the posterior hemiarch, absence of the posterior tubercle and the contralateral arm is preserved, Type F – 1 presence of a cleft in the anterior arch of the atlas, Type F – 2 complete absence of the anterior arch, Type G – 1 combined defects (clefts) in both the anterior and posterior arches of the atlas (bipartite atlas), Type G – 2 combined defects in the anterior and posterior arches (bipartite atlas) that include a cleft in the anterior arch and a unilateral cleft in one of the posterior hemiarches. Arm and posterior tubercle are preserved.
The corrected caption appears below:
Type A – 1 midline posterior cleft in the atlas, Type A – 2 small ossicle within the midline posterior cleft, Type B – 1 partial unilateral posterior cleft, Type B – 2 complete absence of one of the posterior hemiarches, and absence of the posterior tubercle, Type C – 1 bilateral partial defect in the posterior arch of the atlas with preservation of the posterior tubercle, Type C – 2 complete absence of one posterior hemiarch, partial defect in the other hemiarch, arm and posterior tubercle are preserved, Type D – 1 bilateral complete absence of both posterior hemiarches with a single posterior midline tubercle present, Type D – 2 bilateral cleft in both posterior arms and posterior tubercle absent, Type D – 3 unilateral absence of one posterior hemiarch, cleft of the contralateral arm and posterior tubercle absent, Type E – 1 complete absence of the posterior arch and absence of the posterior tubercle, Type E – 2 partial absence of the both posterior hemiarches and absence of the posterior tubercle, Type E – 3 absence of one of the posterior hemiarches, partial absence of the contralateral arm and posterior tubercle absent, Type F – 1 presence of a midline cleft in the anterior arch of the atlas, Type F – 2 complete absence of the anterior arch, Type G – 1 combined midline defects (clefts) in both the anterior and posterior arches of the atlas (bipartite atlas), Type G – 2 combined defects in the anterior and posterior arches (bipartite atlas) that include a midline cleft in the anterior arch and a unilateral cleft in one of the posterior hemiarches, the posterior tubercle is preserved.
In the published article, there was also an error in Figure 3 as published. The image for Figure 3 should be the image that was published as Figure 4. In addition, in Figure 3 there were errors in the n numbers provided. “Registers (n = 6)” should be “Registers (n = 7)”. “Records screened (n = 99)” should be “Records screened (n = 100)”. “Reports sought for retrieval (n = 39)” should be “Reports sought for retrieval (n = 40)”. “Reports assessed for eligibility (n = 39)” should be “Reports assessed for eligibility (n = 40)”. “Studies included in review (n = 6)” should be “Studies included in review (n = 7)”. The corrected Figure 3 and its caption appear below.
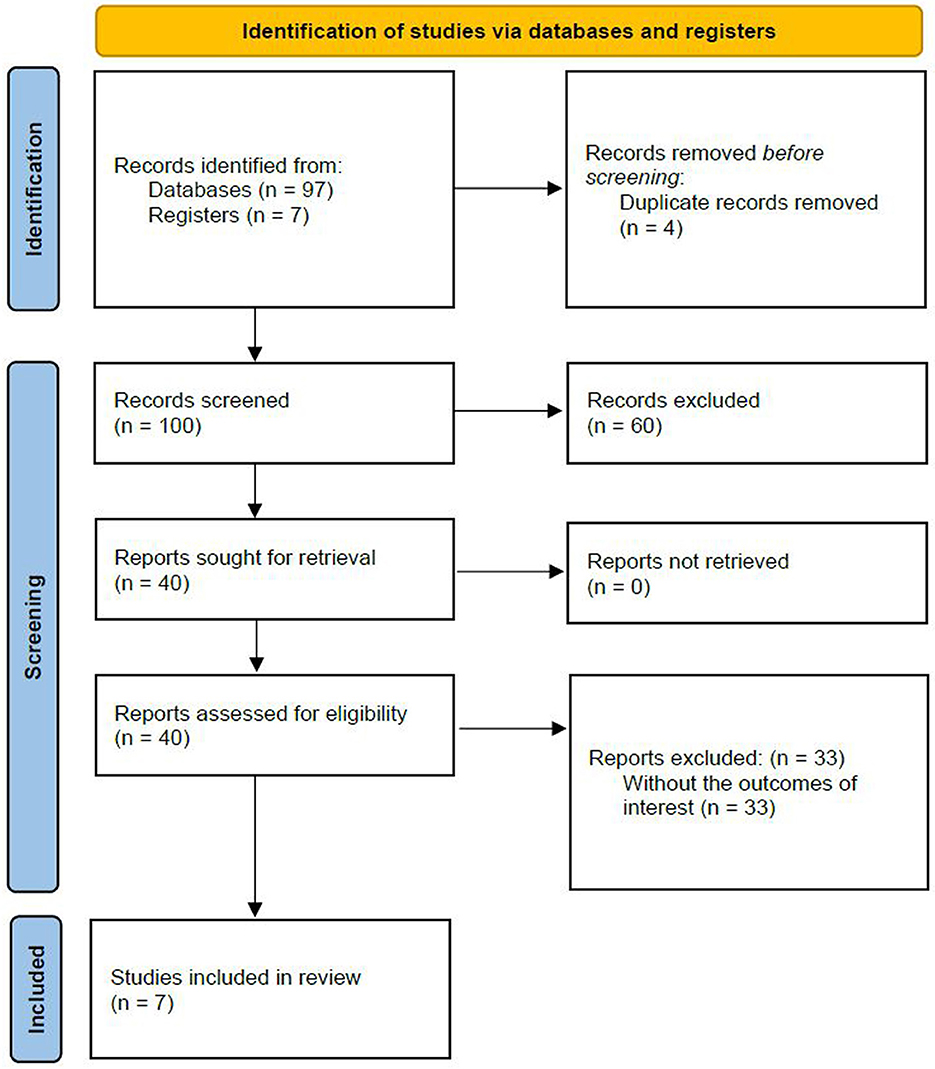
Figure 3. PRISMA diagram.
In the published article, there was also an error in Figure 4 as published. The image for Figure 4 should be the image that was published as Figure 3. The corrected Figure 4 and its caption appear below.
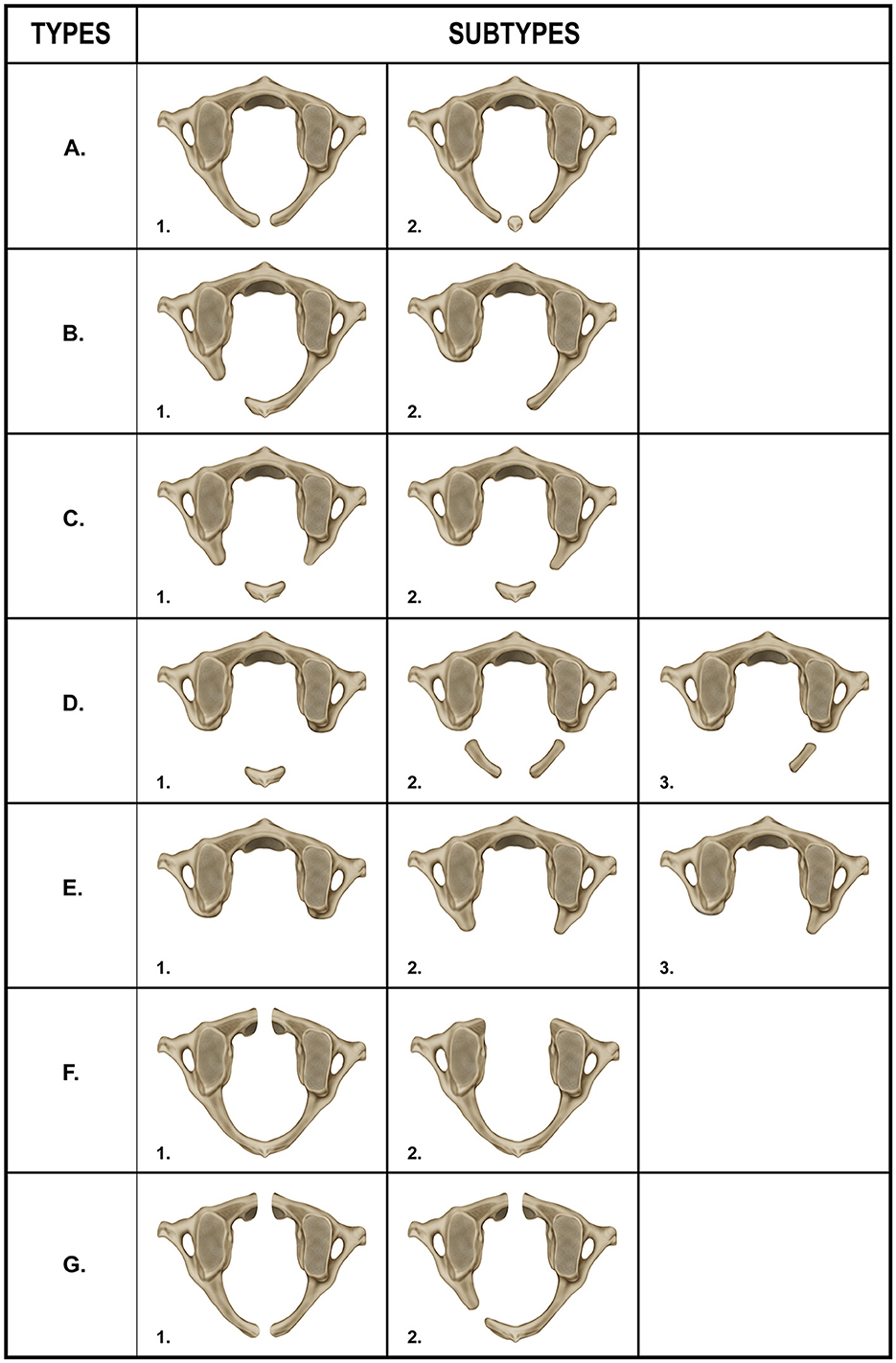
Figure 4. Recommended enhancements to the Currarino classification of atlas arch variations. Type A – 1 midline posterior cleft in the atlas, Type A – 2 small ossicle within the midline posterior cleft, Type B – 1 partial unilateral posterior cleft, Type B – 2 complete absence of one of the posterior hemiarches, and absence of the posterior tubercle, Type C – 1 bilateral partial defect in the posterior arch of the atlas with preservation of the posterior tubercle, Type C – 2 complete absence of one posterior hemiarch, partial defect in the other hemiarch, arm and posterior tubercle are preserved, Type D – 1 bilateral complete absence of both posterior hemiarches with a single posterior midline tubercle present, Type D – 2 bilateral cleft in both posterior arms and posterior tubercle absent, Type D – 3 unilateral absence of one posterior hemiarch, cleft of the contralateral arm and posterior tubercle absent, Type E – 1 complete absence of the posterior arch and absence of the posterior tubercle, Type E – 2 partial absence of the both posterior hemiarches and absence of the posterior tubercle, Type E – 3 absence of one of the posterior hemiarches, partial absence of the contralateral arm and posterior tubercle absent, Type F – 1 presence of a midline cleft in the anterior arch of the atlas, Type F – 2 complete absence of the anterior arch, Type G – 1 combined midline defects (clefts) in both the anterior and posterior arches of the atlas (bipartite atlas), Type G – 2 combined defects in the anterior and posterior arches (bipartite atlas) that include a midline cleft in the anterior arch and a unilateral cleft in one of the posterior hemiarches, the posterior tubercle is preserved.
In the published article, there was also an error in Table 3 as published.
In row “Type D”, “2. A bilateral absence encompassing both posterior arms, coupled with the absence of the posterior tubercle. 3. The unilateral absence of one posterior hemiarch, along with the absence of the contralateral arm and the posterior tubercle.”, should be amended to “2. A bilateral cleft in both posterior hemiarches, coupled with the absence of the posterior tubercle. 3. The unilateral absence of one posterior hemiarch, cleft of the contralateral arm and cleft of the contralateral arm and absence of the posterior tubercle.”
In row “Type E”, “2. The absence of the posterior arch, while both posterior arms are preserved. In this configuration, the posterior tubercle is notably absent. 3. The absence of an entire posterior hemiarch, including the posterior tubercle, with the preservation of the contralateral arm.”, should be amended to “2. The partial absence of both posterior hemiarches, while both posterior arms are preserved. In this configuration, the posterior tubercle is notably absent. 3. The absence of an entire posterior hemiarch, including the posterior tubercle, with the partial preservation of the contralateral arm.”
In row “Type F”, “1. The presence of a cleft in the anterior arch of the atlas.”, should be amended to: “1. The presence of a midline cleft in the anterior arch of the atlas.”
In row “Type G”, “1. Combined defects in both the anterior and posterior arches of the atlas, characteristic of a bipartite atlas. This includes a cleft in the anterior arch and a midline cleft in the posterior arch. 2. Combined defects in the anterior and posterior arches, indicative of a bipartite atlas, encompassing a cleft in the anterior arch and a unilateral cleft in one of the posterior hemiarches, with the preservation of its arm and the posterior tubercle.”, should be amended to: “1. Combined defects in both the anterior and posterior arches of the atlas, characteristic of a bipartite atlas. This includes a midline cleft in the anterior arch, as well as a midline cleft in the posterior arch. 2. Combined defects in the anterior and posterior arches, indicative of a bipartite atlas, encompassing a midline cleft in the anterior arch and a unilateral cleft in one of the posterior hemiarches, with the preservation of the posterior tubercle.”
The corrected Table 3 and its caption appear below.
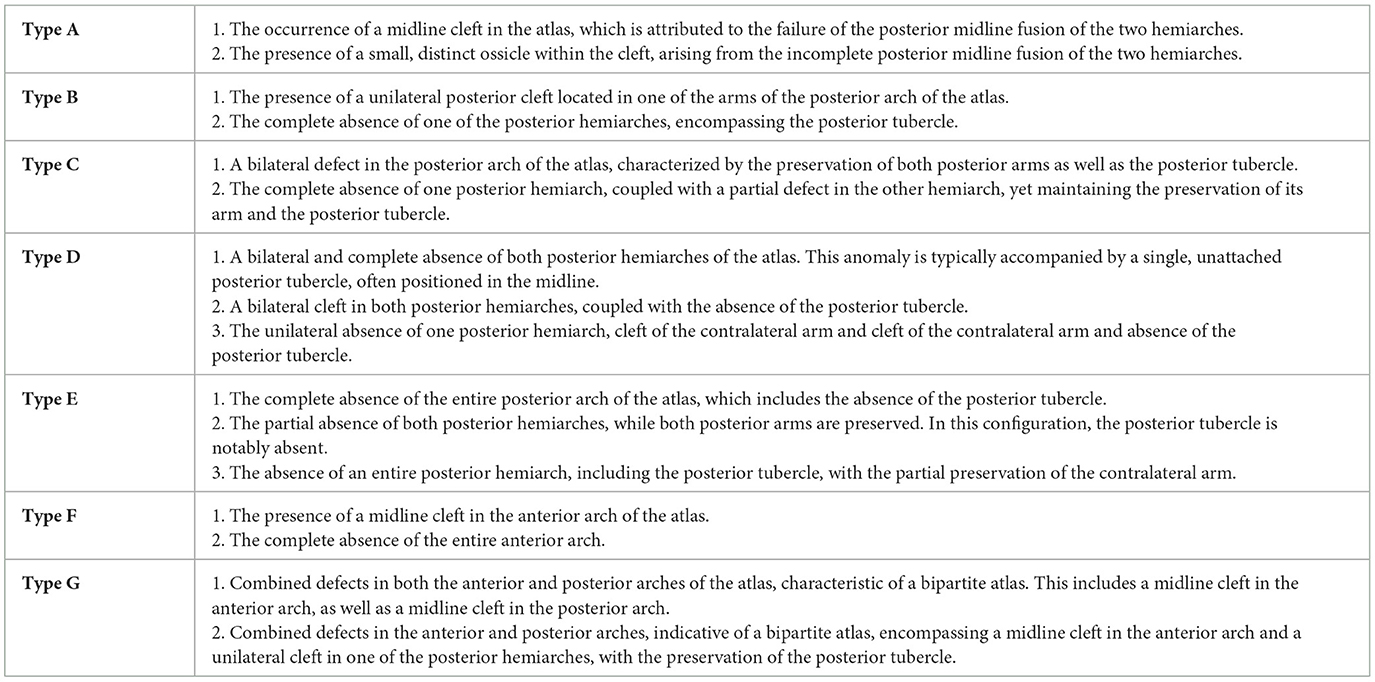
Table 3. Enhanced currarino classification: revised typology of atlas arches variations.
In the published article, the Acknowledgment statement was mistakenly not included in the publication. The missing Acknowledgment statement appears below:
The authors would like to thank the graphic designer, Fabian Cabrera, professor at Universidad del Valle, for his contribution to the illustrations of this manuscript.
The authors apologize for these errors and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: atlas (C1 vertebra), anatomical variation, vertebral arch, cone-beam computed tomography (CBCT), congenital abnormalities, cervical instability
Citation: Baena-Caldas GP, Mier-García JF, Griswold DP, Herrera-Rubio AM and Peckham X (2024) Corrigendum: Anatomical variations of the atlas arches: prevalence assessment, systematic review and proposition for an updated classification system. Front. Neurosci. 18:1418734. doi: 10.3389/fnins.2024.1418734
Received: 17 April 2024; Accepted: 22 April 2024;
Published: 13 May 2024.
Edited and reviewed by: Mauro Palmieri, Sapienza University of Rome, Italy
Copyright © 2024 Baena-Caldas, Mier-García, Griswold, Herrera-Rubio and Peckham. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan F. Mier-García, anVhbi5taWVyQGNvcnJlb3VuaXZhbGxlLmVkdS5jbw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.