
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurosci. , 11 March 2024
Sec. Neurodegeneration
Volume 18 - 2024 | https://doi.org/10.3389/fnins.2024.1361832
This article is part of the Research Topic Neurodegeneration and Cognitive Impairment after Traumatic Brain Injury View all 8 articles
 Tao Liu1,2,3†
Tao Liu1,2,3† Shaohui Yu1,2†
Shaohui Yu1,2† Mingqi Liu1,2†
Mingqi Liu1,2† Zhihao Zhao1,2
Zhihao Zhao1,2 Jiangyuan Yuan1,2
Jiangyuan Yuan1,2 Zhuang Sha1,2
Zhuang Sha1,2 Xuanhui Liu1,2Yu Qian1,2Meng Nie1,2*
Xuanhui Liu1,2Yu Qian1,2Meng Nie1,2* Rongcai Jiang1,2*
Rongcai Jiang1,2*Traumatic Brain Injury (TBI) is a prevalent form of neurological damage that may induce varying degrees of cognitive dysfunction in patients, consequently impacting their quality of life and social functioning. This article provides a mini review of the epidemiology in Chinese TBI patients and etiology of cognitive impairment. It analyzes the risk factors of cognitive impairment, discusses current management strategies for cognitive dysfunction in Chinese TBI patients, and summarizes the strengths and limitations of primary testing tools for TBI-related cognitive functions. Furthermore, the article offers a prospective analysis of future challenges and opportunities. Its objective is to contribute as a reference for the prevention and management of cognitive dysfunction in Chinese TBI patients.
Traumatic brain injury (TBI) poses a global health challenge associated with high mortality and disability rates among populations (Maas et al., 2017). As a “silent epidemic,” it is estimated that approximately 70 million people worldwide experience TBI each year, imposing significant economic burdens on both society and families (Ponsford et al., 2022). Despite being a subject of considerable attention, the magnitude of its impact is often underestimated. The patients included in hospital statistics represent only a fraction of the TBI population, and the actual incidence and burden of TBI far exceed public expectations (Jiang et al., 2019).
Mild TBI (m-TBI) is the most common type, accounting for approximately 75–90% of all TBIs. Its symptoms manifest as non-specific, including headaches, anxiety, irritability, fatigue, depression, and cognitive impairment (Fehily and Fitzgerald, 2017; Madhok et al., 2022). Despite clear evidence indicating that m-TBI can lead to long-term physiological changes, the number of individuals with prolonged m-TBI-related symptoms, especially those involving cognitive impairment, is relatively low (McInnes et al., 2017). Cognitive dysfunction in TBI patients not only adversely affects daily life, learning, and work capabilities but also increases psychological stress and a sense of social isolation, significantly reducing the overall quality of life and social functioning (Mac Donald et al., 2017; Schneider et al., 2022). Therefore, the prevention and management of cognitive dysfunction in TBI patients have become a critically important clinical and societal undertaking.
The prevention and management of cognitive dysfunction in Chinese TBI patients face numerous challenges. The primary reason is that the occurrence and recovery of cognitive impairment in TBI patients are influenced by various factors (Jiang et al., 2019; Gao et al., 2020). Evaluating the neurobehavioral sequelae of TBI patients requires a detailed understanding of medical history and a careful assessment of potential risk factors, posing a highly challenging task for frontline clinical physicians burdened with heavy workloads. Currently, our efforts still have many shortcomings, such as a lack of effective early screening and intervention measures, the absence of comprehensive personalized assessment and treatment plans, a shortage of unified epidemiological data, and the need for strengthened multidisciplinary collaboration and tracking management (Jiang et al., 2019). To improve the current situation of cognitive dysfunction in Chinese TBI patients, it is essential to systematically analyze and discuss aspects like epidemiology, etiology, risk factors, and management strategies, providing a basis and guidance for the development of scientifically sound prevention and treatment measures.
Due to differences in factors such as etiology, injury location, type, and severity of TBI, there are significant variations in the occurrence rate and baseline characteristics of cognitive dysfunction among TBI patients. Additionally, it is scientifically unsound to compare epidemiological data across different regions and populations because current studies employ diverse methods and assessment criteria. There is still a lack of standardized tools and criteria for assessing and diagnosing cognitive dysfunction in TBI patients. We are aware that TBI can result in acute neurological deficits during the initial phase and can lead to various complications in the chronic phase, with cognitive dysfunction being the most common and severe. However, the non-specific manifestations of cognitive dysfunction are diverse and challenging to diagnose. These may include declines or losses in cognitive domains such as memory, attention, executive function, language, and visual-spatial abilities, which may impact the daily life, work, study, and social interactions of patients. The relative scarcity of epidemiological studies on cognitive dysfunction in Chinese TBI patients may be attributed to the difficulty in diagnosing these diverse and non-specific manifestations. Furthermore, most studies are single-center, small-sample studies, lacking nationwide large-scale multicenter cohort studies.
To date, the largest-scale clinical characteristics and outcomes study of TBI patients in China, known as CENTER-TBI, was conducted by Gao et al. (2020). This prospective, longitudinal observational study took place across multiple centers in China and included 13,627 cases of TBI from 56 hospitals in 22 provinces. The aim was to depict the epidemiological pattern of contemporary TBI in China. The study revealed that TBI in China predominantly occurs in young and middle-aged males between the ages of 18 and 65, with the primary cause being traffic accidents. The overall mortality rate was 5%, which was lower than the expected value predicted by the CRASH prognostic model (Perel et al., 2008; Lingsma et al., 2011). Furthermore, substantial differences were identified in the treatment methods for TBI across various hospitals and regions. The study suggests that these findings provide an opportunity for comparative effectiveness research to identify optimal practices for TBI treatment and underscore the necessity of improving TBI systems in different regions. Despite the substantial TBI burden, no FDA-approved therapeutics currently exist due to an incomplete understanding of the mechanisms underlying persistent cognitive dysfunction and post-injury degeneration.
Traumatic Brain Injury resulting from external head impact triggers a series of neuroinflammatory and pathophysiological events leading to neuropsychiatric disorders, affecting cognitive function in 15–30% of TBI patients (Jackson et al., 2004; Himanen et al., 2006; Fleminger, 2008; Till et al., 2008; Silver et al., 2009; Wang et al., 2012). Cognitive impairment in TBI patients is a complex, multifactorial process involving several potential mechanisms. Structural damage to brain tissue, especially in functional areas like the frontal lobe and hippocampus, emerges as a primary cause of cognitive dysfunction after brain trauma (Peters et al., 2009). Research showed that damage to the right hemisphere causes more severe cognitive impairment, with damage to the frontal lobe being particularly prominent (Fletcher and Henson, 2001). The neurotransmitter 5-HT, crucial for memory regulation and brain function maintenance, has shown significance in TBI research. Kline et al. discovered that selective 5-HT1A receptor agonists can reduce neuronal damage in the cerebral cortex and hippocampus, suggesting a potential avenue for therapeutic intervention in a rat TBI model (Meneses, 2003). Additionally, Sen et al. (2017) found that endoplasmic reticulum stress-activated PKR-like ER kinase (PERK) phosphorylates CREB and PSD95 proteins, reducing BDNF levels and impairing synaptic structure and function, ultimately affecting memory. This study suggests that inhibiting PERK phosphorylation may protect dendritic spines and synapses, presenting a potential therapeutic strategy. Recently, another team found that aberrant production of TDP-43 is a key factor in promoting AD neuropathology and synaptic and cognitive deterioration in mouse models of mild closed head injury (CHI). They show that excessive production of TDP-43 either resulting from a single mild CHI or from repeated mild CHI in WT mice is an important mechanism common to both AD and TBI-induced AD-like neurodegenerative disease (Gao et al., 2022). This drives our strategy to limit TDP-43 overproduction to potentially provide therapeutic approaches to prevent the development of TBI-induced AD neuropathology. Recent research also has increasingly focused on the significant role of microglia in cognitive impairment post-TBI (Willis et al., 2020; Krukowski et al., 2021; Bray et al., 2022; Packer et al., 2024). Common findings across these studies suggest that regulating microglia can reduce cognitive impairment after TBI, hinting at microglia as a potential breakthrough in future treatments for cognitive dysfunction post-TBI.
Since the first description of the meningeal lymphatic vessels (MLVs), their unique anatomical and physiological features have been gradually revealed (Louveau et al., 2015; Antila et al., 2017). Exciting recent work revealed MLVs play an important drainage pathway in the elimination of neurotoxic substances, including Aβ aggregates, extracellular tau, and alpha-synuclein aggregates in mice. Moreover, Recent studies have also revealed that MLVs play an important role in various neurological diseases, including AD, Parkinson’s disease (PD), and glioblastoma (Da Mesquita et al., 2018; Song et al., 2020; Ding et al., 2021). Great progress has also been made in the critical role of the meningeal lymphatic system in the pathogenesis of TBI (Bolte et al., 2020; Liu et al., 2023). Bolte etc. revealed even mild head trauma can lead to prominent defects in the drainage of fluorescent beads via the meningeal lymphatic system (Bolte et al., 2020). Mouse studies from our group indicate that exogenous IL-33 exert a protective effect on cognitive functions and improve the drainage of MLVs to deep cervical after TBI (Liu et al., 2023). These studies suggest that cognitive impairment after TBI may be closely related to disruption of meningeal lymphatic drainage. This provides new avenues for future intervention in cognitive impairment after brain trauma.
The risk factors for cognitive impairment in TBI patients, that can be divided into two categories: injury-related factors and individual-related factors, are multifaceted, requiring a comprehensive consideration of injury-related and individual-related factors and their interactions (Himanen et al., 2011; Nordström et al., 2013; Mendez, 2017; Kachmar et al., 2018). Research found that early intervention in TBI can significantly improve outcomes (Robertson et al., 2015; Laing et al., 2022). Therefore, this section will introduce the risk factors for cognitive impairment in TBI patients, to timely identify and intervene, and promote patient recovery and improve prognosis.
It includes factors such as the type, severity, location, and frequency of the injury, determining the extent and severity of brain damage as well as secondary damages like bleeding, hypoxia, inflammatory responses, edema, and ischemia following brain injury (Mendez, 2017; Ma et al., 2019).
Types of injuries can be classified into open and closed injuries. Open TBIs are associated with a higher incidence of coagulopathies, which may exacerbate bleeding and further increase the morbidity and mortality rates of TBI (Chen et al., 2021). Compared to open TBIs, closed injuries often result in mild TBI (Nokkari et al., 2015).
The severity of the injury can be assessed based on indicators such as duration of loss of consciousness, increased intracranial pressure, and abnormalities in neuroimaging. Generally, the higher the severity of the injury, the greater the extent and range of brain damage, and the higher the risk and degree of cognitive impairment (Lennon et al., 2023). Cognitive deficits resulting from mild TBI mostly recover completely within 3–6 months (Rabinowitz and Levin, 2014), whereas up to 65% of patients with moderate to severe TBI suffer from long-term cognitive impairments (Whiteneck et al., 2004).
The location of the injury can affect different cognitive domains. Generally, the frontal and temporal lobes are critical structures for cognitive functions, and damage to these areas can lead to cognitive and social dysfunction (Cristofori and Levin, 2015). Lesions in the left temporal lobe can cause a decline in conversational speech and auditory comprehension, lesions in the left frontal lobe can result in reduced verbal fluency, and lesions in the right parietal lobe can lead to decreased auditory comprehension and reasoning abilities (Gauthier et al., 2018).
The frequency of injuries reflects the cumulative effects of brain damage, where multiple TBIs lead to more severe brain damage and cognitive impairment, with slower and more difficult recovery in patients with multiple TBIs (Lennon et al., 2023). An animal study showed that repeated mild TBIs led to cognitive dysfunction in mice during both acute and chronic phases, along with changes in the expression of genes related to inflammation and excitotoxicity. Especially in mice subjected to 15 impacts, compared to the control group, their hippocampal spatial learning and memory abilities were impaired in the acute phase, with this damage persisting into the chronic phase (Hiskens et al., 2021).
Individual-related factors refer to those associated with the patient themselves, such as age, gender, baseline cognitive level, genetic factors, and comorbidities. These factors affect the sensitivity and plasticity of brain injury, as well as the capacity for repair and reorganization post-injury. Different individual-related factors may impact various cognitive domains differently, and there may be interactions between these factors, making the risk and degree of cognitive impairment more difficult to predict and assess (Himanen et al., 2011; Skaansar et al., 2020; Gomez et al., 2021; Mollayeva et al., 2021; Izzy et al., 2022; Kennedy et al., 2022; Mair et al., 2022; Hume et al., 2023).
Age is a significant factor affecting cognitive impairment, generally, the older the age, the higher the risk and degree of cognitive impairment (Hukkelhoven et al., 2006). Elderly patients with TBI, despite higher initial GCS scores, still have higher overall mortality and disability rates. This adverse prognosis may not only stem from the biological aging process and pre-existing comorbidities but also be influenced by medical decision-making biases, such as more conservative or limited diagnostic and therapeutic measures for elderly patients due to anticipated poor treatment outcomes (Skaansar et al., 2020).
Gender is also a factor affecting cognitive impairment. This may be related to differences in brain structure and function between males and females, as well as the role of sex hormones (Daneshvar et al., 2011). Compared to males, female patients have poorer cognitive recovery at 6 months, and more severe symptoms of depression and anxiety (Moretti et al., 2012).
Baseline cognitive level refers to the cognitive abilities of a patient before the occurrence of TBI. Increasing or maintaining cognitive reserve may help prevent the exacerbation of cognitive decline in the elderly following TBI (Moretti et al., 2012). TBI patients without education have worse cognitive performance compared to those with education, and a higher level of education may help to delay or mitigate the decline in cognitive functions post-TBI (Sharbafshaaer, 2018).
Genetic factors refer to those associated with the genes of TBI patients, which can influence the sensitivity and plasticity of brain injury, as well as the capacity for post-injury repair and reorganization, thereby affecting the risk and severity of cognitive impairments. Studies have shown that certain genetic variations, such as APOE ε4, result in TBI patients carrying the ε4 allele being more prone to adverse outcomes (Zhou et al., 2008; McFadyen et al., 2021). Studies on other genetic variations, like BDNF, indicate that individuals under 45 years old carrying the rs6265 Val (Val66Met) homozygote and rs712444 T allele have the highest survival probabilities in the subacute phase, suggesting that these genes may reduce the risk and severity of cognitive impairments in TBI patients (Failla et al., 2015). The GRIN genotype may affect the plasticity and cognitive function recovery post-TBI, leading to cognitive impairments (Raymont et al., 2008).
Comorbidities refer to other diseases or symptoms that occur concurrently with or subsequent to TBI, such as depression, anxiety, insomnia, pain, diabetes, hypertension, etc. These comorbidities can affect the daily living activities of TBI patients, as well as their abilities in communication, perception, thinking, reasoning, and memory, thereby impacting their overall rehabilitation progress and quality of life (Mollayeva et al., 2017; Hanafy et al., 2021). Additionally, post-concussion syndrome (PCS) that develops after TBI may have lasting effects on cognitive, memory, learning, and executive functions (McInnes et al., 2017).
Cognitive dysfunction is a common complication in TBI patients, significantly impacting their quality of life and social functioning. Therefore, effective cognitive function assessment and rehabilitation intervention are necessary for TBI patients. This section will introduce management strategies for cognitive dysfunction in Chinese TBI patients, including assessment methods, intervention measures.
As the foundation of cognitive dysfunction management, the purpose of cognitive function assessment is to determine the patient’s level of cognitive function, the extent of impairment, and the scope of impact, providing a basis for the formulation of intervention plans and the evaluation of outcomes (Woodford and George, 2007).
Neuropsychological assessment, traditionally used to evaluate the degree of impairment in specific skills and identify potentially affected brain regions, focuses on assessing cognition and behavior, with a crucial emphasis on evaluating the patient’s mental state (Sun et al., 2017). The currently validated cognitive function assessment tools include the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Neurobehavioral Cognitive Status Examination (NCSE), Cognitive Abilities Screening Instrument (CASI), Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) (Mitrushina et al., 1994; Teng et al., 1994; Nasreddine et al., 2005; Mitchell, 2009; Almomani et al., 2018). The main advantages and disadvantages are summarized in Table 1.
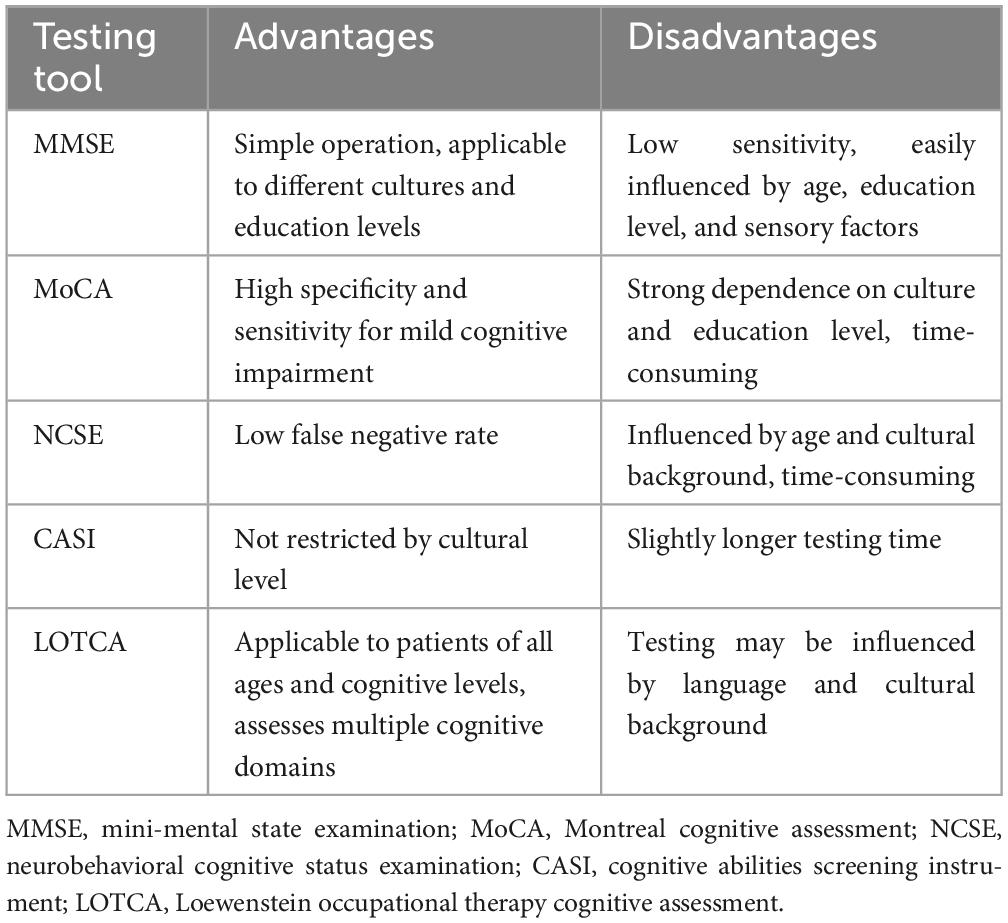
Table 1. Summary of the major cognitive function assessment tools in TBI.
Electrophysiological markers, including electroencephalogram (EEG), sensory-evoked potentials (EPs), and event-related potentials (ERPs), can be used for electrophysiological diagnosis and monitoring of brain function (Amantini et al., 2005; Carrai et al., 2010; Dockree and Robertson, 2011). Valuable indicators such as P300 and mismatch negativity (MMN) are included (Zarza-Luciáñez et al., 2007; Kodama et al., 2010).
Brain imaging methods, such as computerized tomography (CT) and magnetic resonance imaging (MRI), provide essential information, especially for moderate to severe TBI. Diffusion tensor imaging (DTI) can measure changes in brain microstructure and white matter connectivity related to TBI (Hashim et al., 2017; Sun et al., 2017; Königs et al., 2018).
Genetic polymorphisms, such as Brain-derived neurotrophic factor (BDNF), 5-HTTLPR, and the functional catechol-O-methyltransferase genotype (rs4680), are associated with cognitive and social function recovery after TBI (Krueger et al., 2011; Kurowski et al., 2016).
Currently, interventions for cognitive impairment in patients after TBI mainly include the following aspects:
Pharmacological treatment primarily aims to improve brain metabolism, promote the recovery of neuronal function, inhibit apoptosis, and increase neurotrophic factors to enhance cognitive function (Togher et al., 2014). Commonly used medications include acetylcholinesterase inhibitors, serotonin receptor agonists, hormone replacement therapy, but there is a lack of large-scale randomized controlled trials and long-term follow-up studies (Togher et al., 2014; Shih et al., 2019; Ponsford et al., 2022). Therefore, the effectiveness and safety of pharmacological treatment require further validation.
Rehabilitation training refers to stimulating and training the impaired cognitive functions of patients through cognitive tasks, aiming to improve their cognitive levels and adaptability. Currently, several studies have shown significant improvement in cognitive function in TBI patients through rehabilitation training, and the training effects have a certain degree of sustainability and transferability (Jeffay et al., 2023). However, there is no uniform standard or guideline for the optimal timing, frequency, and intensity of rehabilitation training. Therefore, personalized rehabilitation training plans need to be developed based on the specific circumstances of each patient and individual differences.
In addition to pharmacological treatment and rehabilitation training, there are other intervention measures that may have a certain impact on the cognitive function of TBI patients, such as nutritional supplementation, psychological support, and social engagement (Tate et al., 2014; Bayley et al., 2023; Togher et al., 2023). While these interventions may not directly target cognitive function, they could potentially influence cognitive function indirectly by improving the patient’s physical, psychological, and social health (Gómez-de-Regil et al., 2019; Coxe et al., 2021). Currently, more evidence is needed to support the effectiveness and applicability of these intervention measures.
With the development of society and technological progress, the management of cognitive dysfunction in Chinese TBI patients faces new challenges and opportunities. For instance, factors such as population aging and an increase in incidents like traffic accidents, violent events, and sports injuries may contribute to a higher incidence of TBI, leading to a rise in the occurrence of cognitive dysfunction among TBI patients. As medical capabilities improve, the survival rate and lifespan of TBI patients may increase, resulting in a larger population of TBI patients. The advancement of cognitive neuroscience will require a more refined and precise understanding of the pathological mechanisms and classifications of cognitive dysfunction in TBI patients, demanding more sophisticated and specialized diagnostic and assessment tools and methods.
As patient needs become more diverse, the diagnosis and assessment of cognitive dysfunction in TBI patients may require more comprehensive and personalized evaluation metrics and content. With increasing patient expectations, the intervention and management of cognitive dysfunction in TBI patients may necessitate more effective and safe intervention methods and technologies. Additionally, the intervention and management of cognitive dysfunction in TBI patients may face additional challenges and difficulties related to economic, legal, ethical, cultural, and other societal pressures.
However, with the emergence of new technologies and methods, along with the development of information technology, the prevention and intervention of cognitive dysfunction in TBI patients are becoming more personalized and intelligent. The assessment and monitoring of cognitive dysfunction in TBI patients are becoming more convenient and efficient, providing additional avenues and means for the diagnosis and care of cognitive dysfunction in TBI patients.
With the development of society and technological progress, the management of cognitive dysfunction in Chinese TBI patients is facing new challenges and opportunities. Particularly, recent breakthroughs in modern medicine and life sciences have extended people’s lifespan also aggravates aging, potentially increasing the incidence of TBI in the elderly and making cognitive dysfunction issues more prominent. Additionally, the rise in incidents such as traffic accidents, violence, and sports-related activities may contribute to an increased occurrence of TBI, leading to a higher prevalence of cognitive dysfunction in TBI patients. However, limited medical resources may pose challenges to early diagnosis and proactive treatment of cognitive dysfunction in TBI patients. What’s more, as societal pressures increase, interventions and management of cognitive dysfunction in TBI patients may encounter additional economic, legal, ethical, and cultural challenges and difficulties. Nevertheless, these challenges also present opportunities for the management of cognitive dysfunction in TBI. With technological advancements, the emergence of new techniques and methods, the understanding of the pathological mechanisms and classification of cognitive dysfunction in TBI patients has become more refined and precise. Prevention and intervention are becoming more personalized and intelligent.
As patient expectations rise and demands become more diverse, and with clinical physicians focusing on long-term follow-ups and outcomes related to the family and social functions of TBI patients, there is potential to drive the development of comprehensive rehabilitation models and service systems. Furthermore, the development of cognitive neuroscience holds promise in providing new insights and tools for the diagnosis, prediction, and treatment of cognitive dysfunction in TBI patients.
In this article, we have conducted a review and analysis of the epidemiology, underlying mechanisms, influencing factors, assessment methodologies, and management strategies pertaining to cognitive impairment in Chinese patients with TBI. This encompasses a synthesis of the current challenges and future development trends and opportunities in this field. We posit that our article offers substantive guidance for enhancing clinical research and management practices related to cognitive impairment in TBI patients within the Chinese context. Nonetheless, our review acknowledges certain limitations, most notably the absence of large-scale epidemiological surveys on the incidence of cognitive impairment in TBI. This gap is attributed to the lack of standardized research methodologies and assessment criteria, leading to significant variations in study outcomes and the difficulty in drawing uniform conclusions. Future research endeavors should focus on more systematic and standardized investigations to provide a robust foundation for the prevention and treatment of cognitive impairment in TBI patients.
TL: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review and editing. SY: Conceptualization, Investigation, Writing – original draft. ML: Conceptualization, Methodology, Writing – original draft. ZZ: Conceptualization, Investigation, Methodology, Writing – original draft. JY: Conceptualization, Investigation, Methodology, Writing – original draft. ZS: Conceptualization, Investigation, Methodology, Writing – original draft. XL: Investigation, Writing – original draft. YQ: Investigation, Supervision, Writing – original draft. MN: Conceptualization, Investigation, Supervision, Writing – original draft, Writing – review and editing. RJ: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review and editing.
This work was supported by grants from the National Natural Science Foundation of China (Grant No. 82071390 to RJ).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Almomani, F., Avi-Itzhak, T., Demeter, N., Josman, N., and Al-Momani, M. O. (2018). Construct validity and internal consistency reliability of the Loewenstein occupational therapy cognitive assessment (LOTCA). BMC Psychiatry 18:184. doi: 10.1186/s12888-018-1776-x
Amantini, A., Grippo, A., Fossi, S., Cesaretti, C., Piccioli, A., Peris, A., et al. (2005). Prediction of ‘awakening’ and outcome in prolonged acute coma from severe traumatic brain injury: Evidence for validity of short latency SEPs. Clin. Neurophysiol. 116, 229–235. doi: 10.1016/j.clinph.2004.07.008
Antila, S., Karaman, S., Nurmi, H., Airavaara, M., Voutilainen, M. H., Mathivet, T., et al. (2017). Development and plasticity of meningeal lymphatic vessels. J. Exp/Med. 214, 3645–3667. doi: 10.1084/jem.20170391
Bayley, M. T., Janzen, S., Harnett, A., Teasell, R., Patsakos, E., Marshall, S., et al. (2023). INCOG 2.0 guidelines for cognitive rehabilitation following traumatic brain injury: Methods, overview, and principles. J. Head Trauma Rehabil. 38, 7–23. doi: 10.1097/htr.0000000000000838
Bolte, A. C., Dutta, A. B., Hurt, M. E., Smirnov, I., Kovacs, M. A., McKee, C. A., et al. (2020). Meningeal lymphatic dysfunction exacerbates traumatic brain injury pathogenesis. Nat. Commun. 11:4524. doi: 10.1038/s41467-020-18113-4
Bray, C. E., Witcher, K. G., Adekunle-Adegbite, D., Ouvina, M., Witzel, M., Hans, E., et al. (2022). Chronic cortical inflammation, cognitive impairment, and immune reactivity associated with diffuse brain injury are ameliorated by forced turnover of microglia. J. Neurosci. 42, 4215–4228. doi: 10.1523/jneurosci.1910-21.2022
Carrai, R., Grippo, A., Lori, S., Pinto, F., and Amantini, A. (2010). Prognostic value of somatosensory evoked potentials in comatose children: A systematic literature review. Intensive Care Med. 36, 1112–1126. doi: 10.1007/s00134-010-1884-7
Chen, Y., Tian, J., Chi, B., Zhang, S., Wei, L., and Wang, S. (2021). Factors associated with the development of coagulopathy after open traumatic brain injury. J. Clin. Med. 11:185. doi: 10.3390/jcm11010185
Coxe, K. A., Pence, E. K., and Kagotho, N. (2021). Social work care in traumatic brain injury and substance use disorder treatment: A capacity-building model. Health Soc. Work 46, 277–288. doi: 10.1093/hsw/hlab023
Cristofori, I., and Levin, H. S. (2015). Traumatic brain injury and cognition. Handb. Clin. Neurol. 128, 579–611. doi: 10.1016/b978-0-444-63521-1.00037-6
Da Mesquita, S., Louveau, A., Vaccari, A., Smirnov, I., Cornelison, R. C., Kingsmore, K. M., et al. (2018). Functional aspects of meningeal lymphatics in ageing and Alzheimer’s disease. Nature 560, 185–191. doi: 10.1038/s41586-018-0368-8
Daneshvar, D. H., Nowinski, C. J., McKee, A. C., and Cantu, R. C. (2011). The epidemiology of sport-related concussion. Clin. Sports Med. 30, 1–17,vii. doi: 10.1016/j.csm.2010.08.006
Ding, X.-B., Wang, X.-X., Xia, D.-H., Liu, H., Tian, H.-Y., Fu, Y., et al. (2021). Impaired meningeal lymphatic drainage in patients with idiopathic Parkinson’s disease. Nat. Med. 27, 411–418. doi: 10.1038/s41591-020-01198-1
Dockree, P. M., and Robertson, I. H. (2011). Electrophysiological markers of cognitive deficits in traumatic brain injury: A review. Int. J. Psychophysiol. 82, 53–60. doi: 10.1016/j.ijpsycho.2011.01.004
Failla, M. D., Kumar, R. G., Peitzman, A. B., Conley, Y. P., Ferrell, R. E., and Wagner, A. K. (2015). Variation in the BDNF gene interacts with age to predict mortality in a prospective, longitudinal cohort with severe TBI. Neurorehabil. Neural Repair 29, 234–246. doi: 10.1177/1545968314542617
Fehily, B., and Fitzgerald, M. (2017). Repeated mild traumatic brain injury: Potential mechanisms of damage. Cell Transplant 26, 1131–1155. doi: 10.1177/0963689717714092
Fleminger, S. (2008). Long-term psychiatric disorders after traumatic brain injury. Eur. J. Anaesthesiol. Suppl. 42, 123–130. doi: 10.1017/s0265021507003250
Fletcher, P. C., and Henson, R. N. (2001). Frontal lobes and human memory: Insights from functional neuroimaging. Brain 124(Pt 5), 849–881. doi: 10.1093/brain/124.5.849
Gao, F., Hu, M., Zhang, J., Hashem, J., and Chen, C. (2022). TDP-43 drives synaptic and cognitive deterioration following traumatic brain injury. Acta Neuropathol. 144, 187–210. doi: 10.1007/s00401-022-02449-w
Gao, G., Wu, X., Feng, J., Hui, J., Mao, Q., Lecky, F., et al. (2020). Clinical characteristics and outcomes in patients with traumatic brain injury in China: A prospective, multicentre, longitudinal, observational study. Lancet Neurol. 19, 670–677. doi: 10.1016/s1474-4422(20)30182-4
Gauthier, S., LeBlanc, J., Seresova, A., Laberge-Poirier, A., A Correa, J., Alturki, A. Y., et al. (2018). Acute prediction of outcome and cognitive-communication impairments following traumatic brain injury: The influence of age, education and site of lesion. J. Commun. Disord. 73, 77–90. doi: 10.1016/j.jcomdis.2018.04.003
Gomez, A., Batson, C., Froese, L., and Zeiler, F. A. (2021). Genetic variation and impact on outcome in traumatic brain injury: An overview of recent discoveries. Curr. Neurol. Neurosci. Rep. 21:19. doi: 10.1007/s11910-021-01106-1
Gómez-de-Regil, L., Estrella-Castillo, D. F., and Vega-Cauich, J. (2019). Psychological intervention in traumatic brain injury patients. Behav. Neurol. 2019:6937832. doi: 10.1155/2019/6937832
Hanafy, S., Xiong, C., Chan, V., Sutton, M., Escobar, M., Colantonio, A., et al. (2021). Comorbidity in traumatic brain injury and functional outcomes: A systematic review. Eur. J. Phys. Rehabil. Med. 57, 535–550. doi: 10.23736/s1973-9087.21.06491-1
Hashim, E., Caverzasi, E., Papinutto, N., Lewis, C. E., Jing, R., Charles, O., et al. (2017). Investigating microstructural abnormalities and Neurocognition in sub-acute and chronic traumatic brain injury patients with normal-appearing white matter: A preliminary diffusion tensor imaging study. Front. Neurol. 8:97. doi: 10.3389/fneur.2017.00097
Himanen, L., Portin, R., Hämäläinen, P., Hurme, S., Hiekkanen, H., and Tenovuo, O. (2011). Risk factors for reduced survival after traumatic brain injury: A 30-year follow-up study. Brain Inj. 25, 443–452. doi: 10.3109/02699052.2011.556580
Himanen, L., Portin, R., Isoniemi, H., Helenius, H., Kurki, T., and Tenovuo, O. (2006). Longitudinal cognitive changes in traumatic brain injury: A 30-year follow-up study. Neurology 66, 187–192. doi: 10.1212/01.wnl.0000194264.60150.d3
Hiskens, M. I., Schneiders, A. G., Vella, R. K., and Fenning, A. S. (2021). Repetitive mild traumatic brain injury affects inflammation and excitotoxic mRNA expression at acute and chronic time-points. PLoS One 16:e0251315. doi: 10.1371/journal.pone.0251315
Hukkelhoven, C. W., Rampen, A. J., Maas, A. I., Farace, E., Habbema, J. D., Marmarou, A., et al. (2006). Some prognostic models for traumatic brain injury were not valid. J. Clin. Epidemiol. 59, 132–143. doi: 10.1016/j.jclinepi.2005.06.009
Hume, C., Mitra, B., Wright, B., and Kinsella, G. J. (2023). Cognitive performance in older people after mild traumatic brain injury: Trauma effects and other risk factors. J. Int. Neuropsychol. Soc. 29, 651–661. doi: 10.1017/s1355617722000674
Izzy, S., Chen, P. M., Tahir, Z., Grashow, R., Radmanesh, F., Cote, D. J., et al. (2022). Association of traumatic brain injury with the risk of developing chronic cardiovascular, endocrine, neurological, and psychiatric disorders. JAMA Netw. Open 5:e229478. doi: 10.1001/jamanetworkopen.2022.9478
Jackson, J. C., Gordon, S. M., Hart, R. P., Hopkins, R. O., and Ely, E. W. (2004). The association between delirium and cognitive decline: A review of the empirical literature. Neuropsychol, Rev. 14, 87–98. doi: 10.1023/b:nerv.0000028080.39602.17
Jeffay, E., Ponsford, J., Harnett, A., Janzen, S., Patsakos, E., Douglas, J., et al. (2023). INCOG 2.0 guidelines for cognitive rehabilitation following traumatic brain injury, part III: Executive functions. J. Head Trauma Rehabil. 38, 52–64. doi: 10.1097/htr.0000000000000834
Jiang, J. Y., Gao, G. Y., Feng, J. F., Mao, Q., Chen, L. G., Yang, X. F., et al. (2019). Traumatic brain injury in China. Lancet Neurol. 18, 286–295. doi: 10.1016/s1474-4422(18)30469-1
Kachmar, A. G., Irving, S. Y., Connolly, C. A., and Curley, M. A. Q. (2018). A systematic review of risk factors associated with cognitive impairment after Pediatric critical illness. Pediatr. Crit Care Med. 19, e164–e171. doi: 10.1097/pcc.0000000000001430
Kennedy, L., Nuno, M., Gurkoff, G. G., Nosova, K., and Zwienenberg, M. (2022). Moderate and severe TBI in children and adolescents: The effects of age, sex, and injury severity on patient outcome 6 months after injury. Front. Neurol. 13:741717. doi: 10.3389/fneur.2022.741717
Kodama, T., Morita, K., Doi, R., Shoji, Y., and Shigemori, M. (2010). Neurophysiological analyses in different color environments of cognitive function in patients with traumatic brain injury. J. Neurotrauma 27, 1577–1584. doi: 10.1089/neu.2009.1119
Königs, M., Pouwels, P. J., Ernest van Heurn, L. W., Bakx, R., Jeroen Vermeulen, R., Goslings, J. C., et al. (2018). Relevance of neuroimaging for neurocognitive and behavioral outcome after pediatric traumatic brain injury. Brain Imaging Behav. 12, 29–43. doi: 10.1007/s11682-017-9673-3
Krueger, F., Pardini, M., Huey, E. D., Raymont, V., Solomon, J., Lipsky, R. H., et al. (2011). The role of the Met66 brain-derived neurotrophic factor allele in the recovery of executive functioning after combat-related traumatic brain injury. J. Neurosci. 31, 598–606. doi: 10.1523/jneurosci.1399-10.2011
Krukowski, K., Nolan, A., Becker, M., Picard, K., Vernoux, N., Frias, E. S., et al. (2021). Novel microglia-mediated mechanisms underlying synaptic loss and cognitive impairment after traumatic brain injury. Brain Behav. Immun, 98, 122–135. doi: 10.1016/j.bbi.2021.08.210
Kurowski, B. G., Backeljauw, B., Zang, H., Zhang, N., Martin, L. J., Pilipenko, V., et al. (2016). Influence of catechol-O-methyltransferase on executive functioning longitudinally after early childhood traumatic brain injury: Preliminary findings. J. Head Trauma Rehabil. 31, E1–E9. doi: 10.1097/htr.0000000000000162
Laing, J., Gabbe, B., Chen, Z., Perucca, P., Kwan, P., and O’Brien, T. J. (2022). Risk factors and prognosis of early posttraumatic seizures in moderate to severe traumatic brain injury. JAMA Neurol. 79, 334–341. doi: 10.1001/jamaneurol.2021.5420
Lennon, M. J., Brooker, H., Creese, B., Thayanandan, T., Rigney, G., Aarsland, D., et al. (2023). Lifetime traumatic brain injury and cognitive domain deficits in late life: The PROTECT-TBI cohort study. J. Neurotrauma 40, 1423–1435. doi: 10.1089/neu.2022.0360
Lingsma, H. F., Roozenbeek, B., Li, B., Lu, J., Weir, J., Butcher, I., et al. (2011). Large between-center differences in outcome after moderate and severe traumatic brain injury in the international mission on prognosis and clinical trial design in traumatic brain injury (IMPACT) study. Neurosurgery 68, 601–607. doi: 10.1227/NEU.0b013e318209333b
Liu, M., Huang, J., Liu, T., Yuan, J., Lv, C., Sha, Z., et al. (2023). Exogenous interleukin 33 enhances the brain’s lymphatic drainage and toxic protein clearance in acute traumatic brain injury mice. Acta Neuropathol. Commun. 11:61. doi: 10.1186/s40478-023-01555-4
Louveau, A., Smirnov, I., Keyes, T. J., Eccles, J. D., Rouhani, S. J., Peske, J. D., et al. (2015). Structural and functional features of central nervous system lymphatic vessels. Nature 523, 337–341. doi: 10.1038/nature14432
Ma, X., Aravind, A., Pfister, B. J., Chandra, N., and Haorah, J. (2019). Animal models of traumatic brain injury and assessment of injury severity. Mol. Neurobiol, 56, 5332–5345. doi: 10.1007/s12035-018-1454-5
Maas, A. I. R., Menon, D. K., Adelson, P. D., Andelic, N., Bell, M. J., Belli, A., et al. (2017). Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16, 987–1048. doi: 10.1016/s1474-4422(17)30371-x
Mac Donald, C. L., Barber, J., Jordan, M., Johnson, A. M., Dikmen, S., Fann, J. R., et al. (2017). Early clinical predictors of 5-year outcome after concussive blast traumatic brain injury. JAMA Neurol, 74, 821–829. doi: 10.1001/jamaneurol.2017.0143
Madhok, D. Y., Rodriguez, R. M., Barber, J., Temkin, N. R., Markowitz, A. J., Kreitzer, N., et al. (2022). Outcomes in patients with mild traumatic brain injury without acute intracranial traumatic injury. JAMA Netw. Open 5:e2223245. doi: 10.1001/jamanetworkopen.2022.23245
Mair, O., Greve, F., Lefering, R., Biberthaler, P., and Hanschen, M. (2022). The outcome of severely injured patients following traumatic brain injury is affected by gender-A retrospective, multicenter, matched-pair analysis utilizing data of the TraumaRegister DGU(®). Front. Neurosci. 16:974519. doi: 10.3389/fnins.2022.974519
McFadyen, C. A., Zeiler, F. A., Newcombe, V., Synnot, A., Steyerberg, E., Gruen, R. L., et al. (2021). Apolipoprotein E4 polymorphism and outcomes from traumatic brain injury: A living systematic review and meta-analysis. J. Neurotrauma 38, 1124–1136. doi: 10.1089/neu.2018.6052
McInnes, K., Friesen, C. L., MacKenzie, D. E., Westwood, D. A., and Boe, S. G. (2017). Mild traumatic brain injury (mTBI) and chronic cognitive impairment: A scoping review. PLoS One 12:e0174847. doi: 10.1371/journal.pone.0174847
Mendez, M. F. (2017). What is the relationship of traumatic brain injury to dementia? J. Alzheimers Dis, 57, 667–681. doi: 10.3233/jad-161002
Meneses, A. (2003). A pharmacological analysis of an associative learning task: 5-HT(1) to 5-HT(7) receptor subtypes function on a pavlovian/instrumental autoshaped memory. Learn Mem. 10, 363–372. doi: 10.1101/lm.60503
Mitchell, A. J. (2009). A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J. Psychiatr. Res. 43, 411–431. doi: 10.1016/j.jpsychires.2008.04.014
Mitrushina, M., Abara, J., and Blumenfeld, A. (1994). Aspects of validity and reliability of the neurobehavioral cognitive status examination (NCSE) in assessment of psychiatric patients. J. Psychiatr. Res. 28, 85–95. doi: 10.1016/0022-3956(94)90037-x
Mollayeva, T., Mollayeva, S., Pacheco, N., and Colantonio, A. (2021). Systematic review of sex and gender effects in traumatic brain injury: Equity in clinical and functional outcomes. Front. Neurol. 12:678971. doi: 10.3389/fneur.2021.678971
Mollayeva, T., Xiong, C., Hanafy, S., Chan, V., Hu, Z. J., Sutton, M., et al. (2017). Comorbidity and outcomes in traumatic brain injury: Protocol for a systematic review on functional status and risk of death. BMJ Open 7:e018626. doi: 10.1136/bmjopen-2017-018626
Moretti, L., Cristofori, I., Weaver, S. M., Chau, A., Portelli, J. N., and Grafman, J. (2012). Cognitive decline in older adults with a history of traumatic brain injury. Lancet Neurol. 11, 1103–1112. doi: 10.1016/s1474-4422(12)70226-0
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., et al. (2005). The montreal cognitive assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699. doi: 10.1111/j.1532-5415.2005.53221.x
Nokkari, A., Mouhieddine, T. H., Itani, M. M., Abou-Kheir, W., Daoud, G., Zhu, R., et al. (2015). Characterization of the Kallikrein-Kinin system post chemical neuronal injury: An in vitro biochemical and Neuroproteomics assessment. PLoS One 10:e0128601. doi: 10.1371/journal.pone.0128601
Nordström, A., Edin, B. B., Lindström, S., and Nordström, P. (2013). Cognitive function and other risk factors for mild traumatic brain injury in young men: Nationwide cohort study. Bmj 346:f723. doi: 10.1136/bmj.f723
Packer, J. M., Bray, C. E., Beckman, N. B., Wangler, L. M., Davis, A. C., Goodman, E. J., et al. (2024). Impaired cortical neuronal homeostasis and cognition after diffuse traumatic brain injury are dependent on microglia and type I interferon responses. Glia 72, 300–321. doi: 10.1002/glia.24475
Perel, P., Arango, M., Clayton, T., Edwards, P., Komolafe, E., Poccock, S., et al. (2008). Predicting outcome after traumatic brain injury: Practical prognostic models based on large cohort of international patients. Bmj 336, 425–429. doi: 10.1136/bmj.39461.643438.25
Peters, J., Daum, I., Gizewski, E., Forsting, M., and Suchan, B. (2009). Associations evoked during memory encoding recruit the context-network. Hippocampus 19, 141–151. doi: 10.1002/hipo.20490
Ponsford, J., Spitz, G., and Hicks, A. J. (2022). Highlights in traumatic brain injury research in 2021. Lancet Neurol. 21, 5–6. doi: 10.1016/s1474-4422(21)00424-5
Rabinowitz, A. R., and Levin, H. S. (2014). Cognitive sequelae of traumatic brain injury. Psychiatr. Clin. North Am. 37, 1–11. doi: 10.1016/j.psc.2013.11.004
Raymont, V., Greathouse, A., Reding, K., Lipsky, R., Salazar, A., and Grafman, J. (2008). Demographic, structural and genetic predictors of late cognitive decline after penetrating head injury. Brain 131(Pt 2), 543–558. doi: 10.1093/brain/awm300
Robertson, M., Seaton, A., and Whalley, L. J. (2015). Can we reduce the risk of dementia? Qjm 108, 93–97. doi: 10.1093/qjmed/hcu072
Schneider, A. L. C., Huie, J. R., Boscardin, W. J., Nelson, L., Barber, J. K., Yaffe, K., et al. (2022). Cognitive outcome 1 year after mild traumatic brain injury: Results from the TRACK-TBI Study. Neurology 98, e1248–e1261. doi: 10.1212/wnl.0000000000200041
Sen, T., Gupta, R., Kaiser, H., and Sen, N. (2017). Activation of PERK elicits memory impairment through inactivation of CREB and downregulation of PSD95 after traumatic brain injury. J. Neurosci. 37, 5900–5911. doi: 10.1523/jneurosci.2343-16.2017
Sharbafshaaer, M. (2018). Impacts of cognitive impairment for different levels and causes of traumatic brain injury, and education status in TBI patients. Dement Neuropsychol. 12, 415–420. doi: 10.1590/1980-57642018dn12-040012
Shih, C. C., Yeh, C. C., Yang, J. L., Lane, H. L., Huang, C. J., Lin, J. G., et al. (2019). Reduced use of emergency care and hospitalization in patients with post-stroke cognitive impairment treated with traditional Chinese medicine. Qjm 112, 437–442. doi: 10.1093/qjmed/hcz044
Silver, J. M., McAllister, T. W., and Arciniegas, D. B. (2009). Depression and cognitive complaints following mild traumatic brain injury. Am. J. Psychiatry 166, 653–661. doi: 10.1176/appi.ajp.2009.08111676
Skaansar, O., Tverdal, C., Rønning, P. A., Skogen, K., Brommeland, T., Røise, O., et al. (2020). Traumatic brain injury-the effects of patient age on treatment intensity and mortality. BMC Neurol. 20:376. doi: 10.1186/s12883-020-01943-6
Song, E., Mao, T., Dong, H., Boisserand, L. S. B., Antila, S., Bosenberg, M., et al. (2020). VEGF-C-driven lymphatic drainage enables immunosurveillance of brain tumours. Nature 577, 689–694. doi: 10.1038/s41586-019-1912-x
Sun, H., Luo, C., Chen, X., and Tao, L. (2017). Assessment of cognitive dysfunction in traumatic brain injury patients: A review. Forensic. Sci. Res. 2, 174–179. doi: 10.1080/20961790.2017.1390836
Tate, R., Kennedy, M., Ponsford, J., Douglas, J., Velikonja, D., Bayley, M., et al. (2014). INCOG recommendations for management of cognition following traumatic brain injury, part III: Executive function and self-awareness. J. Head Trauma Rehabil. 29, 338–352. doi: 10.1097/htr.0000000000000068
Teng, E. L., Hasegawa, K., Homma, A., Imai, Y., Larson, E., Graves, A., et al. (1994). The Cognitive Abilities Screening Instrument (CASI): A practical test for cross-cultural epidemiological studies of dementia. Int. Psychogeriatr. 6, 45–58. doi: 10.1017/s1041610294001602
Till, C., Colella, B., Verwegen, J., and Green, R. E. (2008). Postrecovery cognitive decline in adults with traumatic brain injury. Arch. Phys. Med. Rehabil. 89(12 Suppl.), S25–S34. doi: 10.1016/j.apmr.2008.07.004
Togher, L., Douglas, J., Turkstra, L. S., Welch-West, P., Janzen, S., Harnett, A., et al. (2023). INCOG 2.0 guidelines for cognitive rehabilitation following traumatic brain injury, part IV: Cognitive-communication and social cognition disorders. J. Head Trauma Rehabil. 38, 65–82. doi: 10.1097/htr.0000000000000835
Togher, L., Wiseman-Hakes, C., Douglas, J., Stergiou-Kita, M., Ponsford, J., Teasell, R., et al. (2014). INCOG recommendations for management of cognition following traumatic brain injury, part IV: Cognitive communication. J. Head Trauma Rehabil. 29, 353–368. doi: 10.1097/htr.0000000000000071
Wang, H. K., Lin, S. H., Sung, P. S., Wu, M. H., Hung, K. W., Wang, L. C., et al. (2012). Population based study on patients with traumatic brain injury suggests increased risk of dementia. J. Neurol. Neurosurg. Psychiatry 83, 1080–1085. doi: 10.1136/jnnp-2012-302633
Whiteneck, G. G., Gerhart, K. A., and Cusick, C. P. (2004). Identifying environmental factors that influence the outcomes of people with traumatic brain injury. J. Head Trauma Rehabil. 19, 191–204. doi: 10.1097/00001199-200405000-00001
Willis, E. F., MacDonald, K. P. A., Nguyen, Q. H., Garrido, A. L., Gillespie, E. R., Harley, S. B. R., et al. (2020). Repopulating microglia promote brain repair in an IL-6-dependent manner. Cell 180, 833.e16–846.e16. doi: 10.1016/j.cell.2020.02.013
Woodford, H. J., and George, J. (2007). Cognitive assessment in the elderly: A review of clinical methods. Qjm 100, 469–484. doi: 10.1093/qjmed/hcm051
Zarza-Luciáñez, D., Arce-Arce, S., Bhathal, H., and Sanjuán-Martín, F. (2007). [Mismatch negativity and conscience level in severe traumatic brain injury]. Rev. Neurol. 44, 465–468.
Keywords: traumatic brain injury, cognitive impairment, dysfunction, epidemiology, risk factors, challenges, opportunities
Citation: Liu T, Yu S, Liu M, Zhao Z, Yuan J, Sha Z, Liu X, Qian Y, Nie M and Jiang R (2024) Cognitive impairment in Chinese traumatic brain injury patients: from challenge to future perspectives. Front. Neurosci. 18:1361832. doi: 10.3389/fnins.2024.1361832
Received: 27 December 2023; Accepted: 27 February 2024;
Published: 11 March 2024.
Edited by:
Mohammad Badruzzaman Khan, Augusta University, United StatesReviewed by:
Mohammed Sikander, The University of Texas Rio Grande Valley, United StatesCopyright © 2024 Liu, Yu, Liu, Zhao, Yuan, Sha, Liu, Qian, Nie and Jiang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rongcai Jiang, amlhbmdyb25nY2FpQHRtdS5lZHUuY24=; Meng Nie, bjE3MzU0MjgxODExQDE2My5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.