 Tianning Sun
Tianning Sun Maohui Feng2†
Maohui Feng2† Anne Manyande
Anne Manyande Hongbing Xiang
Hongbing Xiang Jun Xiong
Jun Xiong Zhigang He
Zhigang He
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci. , 16 June 2023
Sec. Neuroenergetics and Brain Health
Volume 17 - 2023 | https://doi.org/10.3389/fnins.2023.1206417
This article is part of the Research Topic Insights in Neuroenergetics, Nutrition and Brain Health: 2023 View all 9 articles
Patients with liver disease are prone to various cognitive impairments. It is undeniable that cognitive impairment is often regulated by both the nervous system and the immune system. In this review our research focused on the regulation of mild cognitive impairment associated with liver disease by humoral factors derived from the gastrointestinal tract, and revealed that its mechanisms may be involved with hyperammonemia, neuroinflammation, brain energy and neurotransmitter metabolic disorders, and liver-derived factors. In addition, we share the emerging research progress in magnetic resonance imaging techniques of the brain during mild cognitive impairment associated with liver disease, in order to provide ideas for the prevention and treatment of mild cognitive impairment in liver disease.
Liver disease patients are prone to various cognitive impairments (Sun et al., 2022; Yang et al., 2022; He et al., 2023). Even in healthy populations, plasma transaminase levels are significantly negatively correlated with memory ability (Kamada et al., 2016). Hepatic encephalopathy (HE) is a brain dysfunction caused by acute or chronic liver dysfunction and/or portosystemic shunts, mainly characterized by neurological and psychiatric abnormalities, cognitive and motor function changes (Rose et al., 2020). According to the severity of the patient’s condition, HE can be divided into minimal hepatic encephalopathy (MHE) and overt hepatic encephalopathy (OHE) (Bajaj et al., 2011). MHE occurs during the early stage of HE and is commonly seen in patients with chronic liver cirrhosis. These patients do not have clinical symptoms, but there are cognitive changes indicated by neuropsychological testing (Moran et al., 2021). It has been reported that the incidence of MHE in patients with liver cirrhosis can be as high as 20–80% (Lauridsen et al., 2011; Allampati et al., 2016). MHE seriously affects patients’ work and quality of life, but it especially increases the risk of traffic accidents (Bajaj et al., 2009; Mina et al., 2014). In addition, MHE is prone to progress to OHE (Hartmann et al., 2000), increasing the risk of hospitalization and death of patients (Kim et al., 2019).
As well as MHE, liver diseases such as non-alcoholic fatty liver disease (NAFLD) (Kjaergaard et al., 2021), chronic hepatitis C (Mazzaro et al., 2021), cholestatic liver disease (Phaw et al., 2021), and liver transplantation (Getsuwan et al., 2021) also have mild cognitive impairment. Although current research cannot classify them as MHE, mild cognitive impairment in these liver diseases may be a precursor of OHE and is associated with poor prognosis in patients (Collie, 2005). Once cognitive impairment progresses to OHE, the patient’s mortality rate will greatly increase (Yanny et al., 2019), and permanent central nervous system damage may occur. Even with liver transplantation (LT) treatment, patients will not completely recover cognitive function (Kornerup et al., 2019). Therefore, early understanding of the mechanism of mild cognitive impairment in liver disease is crucial for improving patient quality of life and prognosis by preventing the progression of HE. This review focuses on the changes in the brain during mild cognitive impairment related to liver disease, in order to better understand the mechanism of cognitive impairment and provides new insights for the prevention and treatment of mild cognitive impairment related to liver disease.
In 1970, Zeegen et al. (1970) first reported that 47% of patients undergoing portal decompression surgery experienced brain dysfunction. Subsequently, up until 2011, there has been a gradual increase in research of mild cognitive impairment in chronic liver disease, when Bajaj et al. (2011) described cognitive impairment that appears as MHE before HE symptoms in patients with cirrhosis. In China, the main cause of cirrhosis is viral hepatitis, and the incidence of MHE among hospitalized patients with cirrhosis can reach up to 40% (Xu et al., 2019). It has been reported that cognitive impairment exists in chronic hepatitis C (HCV) patients even before the appearance of cirrhosis (Ibáñez-Samaniego et al., 2022), with more than 50% of HCV patients experiencing cognitive impairment (Mazzaro et al., 2021), antiviral therapy can significantly improve patients’ cognitive function by eradicating HCV (Kraus et al., 2013; Vaghi et al., 2020).
NAFLD is known to be the leading cause of chronic liver disease worldwide, affecting a quarter of the global population (Younossi et al., 2019). Cognitive impairment is also a common extrahepatic complication of NAFLD. According to investigations, up to 70% of NAFLD patients have memory loss and forgetfulness (Kjaergaard et al., 2021). A recent systematic review of 11 observational studies showed that NAFLD patients have cognitive impairments in multiple aspects such as “general cognition” and “mental speed and attention.” An et al. (2019) also found that cognitive impairment in NAFLD patients was related to elevated plasma liver enzymes and abnormal blood lipids. Moreover, Liu Q. et al. (2021) showed that the incidence of cognitive impairment in middle-aged and elderly NAFLD patients was significantly higher than in non-NAFLD patients in a longitudinal cohort study.
In cholestatic liver diseases, primary biliary cholangitis (PBC) patients often have symptoms of cognitive impairment, mainly manifested as memory loss, attention deficit, and psychomotor dysfunction. Newton et al. (2008) ascertained that about 53% of PBC patients have attention or memory impairment, and the severity of cognitive impairment is not related to the severity of the liver disease, such as biochemical indicators and histological damage, indicating that this cognitive impairment is largely unrelated to HE. Liu Y. et al. (2021) also reported that the health-related quality of life of Chinese PBC patients is impaired, and influenced by factors such as gender and age, with women and elderly patients more prone to cognitive impairment.
Liver transplantation (LT) is the ultimate treatment for end-stage liver disease. Previous studies determined that HE is completely reversible after LT, but increasing evidence suggests that patients still have varying degrees of cognitive impairment after the liver function has been restored by transplantation (Teperman and Peyregne, 2010; Kornerup et al., 2019). It has been reported that up to 30% of patients still have neurological sequelae after LT (Weiss and Thabut, 2019), and since the diseased liver has been replaced by a healthy liver, this post-LT cognitive impairment cannot yet be defined as HE. Furthermore, Campagna et al. (2014) showed that post-LT cognitive impairment is influenced by pre-transplant brain disease. Patients with obvious HE before transplantation had poorer overall cognitive function after LT than those without obvious HE, suggesting that post-LT cognitive impairment may be related to permanent brain damage caused by OHE to the central nervous system (Garcia-Martinez et al., 2011). Besides, hepatic ischemia–reperfusion injury (I/R) occurring during the perioperative period also has adverse effects on cognition (He et al., 2023). Many basic research studies have reported cognitive impairments in experimental animals after experiencing hepatic I/R injury (Wu et al., 2019; Wang et al., 2022).
In summary, mild cognitive impairment is very common in liver diseases. Patients not only suffer from impaired personality and activities of daily living ability but also experience a severe decline in their quality of life. Moreover, it creates a significant burden of care and psychological impact on their families (Fabrellas et al., 2020; Shrestha et al., 2020). Although the etiology and clinical manifestations of liver disease-related mild cognitive impairment are not entirely the same, their underlying mechanisms are very similar. The following section summarizes the brain changes in liver disease-related mild cognitive impairment.
Ammonia is a neurotoxic substance primarily produced in the intestine by the metabolism of proteins and amino acids followed by intestinal bacterial degradation. Dysbiosis of the gut microbiota has been shown to increase ammonia production (Kang et al., 2016). Some preclinical studies have demonstrated that dysbiosis is associated with cognitive impairment and hyperammonemia in HE rats (Higarza et al., 2019). Since the elimination of ammonia depends on the liver’s ability to convert ammonia, impairment of liver function due to the lack of glutamine synthetase in the liver can result in the accumulation of ammonia in the body and cognitive changes (Qvartskhava et al., 2015). Elevated blood ammonia can freely pass through the blood–brain barrier, causing inflammation of the nervous system and leading to cognitive impairment (Bobermin et al., 2020; Jaffe et al., 2020), however, treating HE symptoms can be achieved by reducing central ammonia levels and improving inflammation (Jayakumar et al., 2015; Lu et al., 2020). Ammonia is detoxified by converting it into glutamine by astrocytes in the central nervous system (Jayakumar and Norenberg, 2016), but glutamine has permeability, and its accumulation can cause swelling and functional impairment of astrocytes (Rama Rao and Norenberg, 2014) and brain edema (Cudalbu and Taylor-Robinson, 2019). Although high blood ammonia levels are considered a core factor in causing HE (Aldridge et al., 2015; Hadjihambi et al., 2018), their role in mild cognitive impairment associated with liver disease is not significant and is only observed in MHE patients with increased blood ammonia concentration levels and decreased brain ammonia metabolism (Lockwood et al., 1991). In addition, Higarza et al. (2019) showed that cognitive impairment in NAFLD rats was related to increased blood ammonia levels, but only mild ammonia elevation was observed in NAFLD patients (Felipo et al., 2012).
Neuroinflammation is a common feature of various liver disease-related mild cognitive impairments. The immune cells of the central nervous system are microglia (Sheeler et al., 2020), which can monitor synaptic activity, pathogens, and injuries in the local environment and have phagocytic and synaptic remodeling-promoting functions. Microglial activation is a significant feature of neuroinflammation and is accompanied by an increase in cytokines and chemokines (Sheeler et al., 2020; Woodburn et al., 2021). It has been reported that MHE patients have significantly higher levels of inflammation, such as IL-6 and C-reactive protein, compared to normal individuals (Shawcross et al., 2007). Nonetheless, Shawcross et al. (2004) found that hyperammonemia in cirrhotic patients could only induce cognitive impairment when an inflammatory response occurred. Patients did not have cognitive impairment after the inflammation subsided, indicating that inflammation plays an important role in cognitive impairment in MHE patients. Neuroinflammation is also an important cause of cognitive impairment in NAFLD patients (Kjaergaard et al., 2021). Balzano et al. (2018) showed that NASH patients had neuroinflammatory manifestations such as neuronal loss, microglial and astrocytic activation, and lymphocyte infiltration in the cerebellum. Animal experiments have indicated that the neurological dysfunction of NAFLD is related to neuroinflammation (Veniaminova et al., 2020). Similarly, Bokemeyer et al. (2011) and Pflugrad et al. (2016) observed microglial and astrocytic activation and other neuroinflammatory manifestations in HCV patients. Although there is no evidence of cholestatic liver disease-associated neuropathy, it has been reported that NF-KB is activated in cholestatic liver disease, and NF-KB is associated with neuropathic inflammation and cognitive impairment (Phaw et al., 2021).
The brain has a high energy demand, consuming 20% of the body’s energy despite accounting for only 2% of its weight (Magistretti and Allaman, 2018). Glucose is the brain’s primary source of energy, providing over 95% of its energy needs through the tricarboxylic acid (TCA) cycle in neurons under physiological conditions (Bordone et al., 2019). However, the astrocyte-neuron lactate shuttle hypothesis (Magistretti and Allaman, 2018) suggests that glucose is mainly metabolized to lactate in astrocytes. When neuronal activity increases, the released glutamate can trigger astrocytes to uptake glucose and produce lactate as a supplemental energy source for neurons (Pellerin et al., 2007; Huang et al., 2019).
Elevated brain lactate levels in hepatic encephalopathy (HE) patients are typically regarded as a sign of cerebral energy failure (Bosoi and Rose, 2014). The accumulation of lactate in brain cells can cause cell swelling and brain edema, and interfere with communication, metabolism, and neurotransmission between astrocytes and neurons (Bosoi and Rose, 2014). Jiménez et al. (2010) compared the serum 1H-NMR metabolome of healthy controls (n = 69), cirrhotic patients without minimal hepatic encephalopathy (MHE) (n = 62), and cirrhotic patients with MHE (n = 39), and found that MHE patients had increased glucose and lactate concentration levels. Basic research also suggests that bile duct ligation (BDL) induced HE in rats which results in significant lactate accumulation in the cerebellum, hippocampus, and striatum (Simicic et al., 2019). Additionally, Hadjihambi et al. (2017) demonstrated that hyperammonemia induced by BDL in HE rats can impair the function of lactate transporters and astrocyte-neuron lactate shuttle, leading to neuronal energy metabolism disorders.
Apart from metabolic substrates, adequate oxygen supply is needed for the normal functioning of the brain. The energy metabolism of the brain is regulated by the neurovascular unit (NVU), which consists of neurons, glial cells, and vascular cells (Ahmad et al., 2020). Astrocytes strictly regulate cerebral blood flow through the NVU, thereby regulating the nutrition and oxygen supply of the central nervous system to meet the needs of local neurons (Bélanger et al., 2011). Structural and functional damage to the blood–brain barrier and astrocyte dysfunction can lead to NVU dysfunction, resulting in inadequate oxygen and energy metabolism in brain tissue. Nakanishi et al. (2014) ascertained that non-MHE cirrhotic patients exhibited a sharp and repetitive increase in cerebral oxyhemoglobin during task execution, while MHE patients showed a relatively slow increase, indicating poor task responsiveness to cerebral oxygen concentration levels in MHE patients. Sunil et al. (2012) also reported abnormal cerebral blood flow perfusion in multiple brain regions of MHE patients, and that regional cerebral blood flow in some brain regions was related to patients’ cognitive impairment. Near-infrared spectroscopy measurements of NAFLD (Takahashi et al., 2017) and PBC (Duszynski et al., 2020) patients illustrated cerebral hypoxia in these patients. Moreover, significant decreases in glucose, lactate, and tissue oxygen concentration levels were observed in the cortex of BDL-induced MHE rats (Hadjihambi et al., 2022). In conclusion, these findings indicate that there is energy metabolic dysfunction in mild cognitive impairment associated with liver disease.
Impaired glucose metabolism in the brain not only causes damage to brain energy metabolism but also affects neurotransmitter synthesis. In neuronal cells, glucose generated from glycolysis can not only be metabolized into ATP through the TCA cycle, but its product alpha-ketoglutarate (α-KG) can be synthesized into glutamate (Glu) via aspartate transaminase. Glu released into the synaptic cleft can be retaken up by astrocytes and converted into glutamine (Gln) via glutamine synthetase, and then transferred back to neurons where it is reconverted to Glu via glutaminase, a process known as the glutamate-glutamine cycle (Schousboe et al., 2014). Gln generated by astrocytes is also an important pathway for GABA replenishment. Impairment of the glutamate-glutamine cycle is a major cause of hepatic encephalopathy (Limón et al., 2021).
Magnetic resonance spectroscopy (MRS) of 13C-labeled metabolic substrates can provide insights into energy and neurotransmitter metabolism in neurons and astrocytes (Sonnay et al., 2017). Zwingmann et al. (2003) used [1-13C] glucose labeling to track neurotransmitter metabolism in rats with acute liver failure (ALF) induced by portacaval anastomosis (PCA), from the early stages of hepatic encephalopathy (HE) to the coma stage. The results showed that, compared to the control group, the total Gln and lactate concentrations in the brains of rats in the early stages of HE increased by 2 to 4.5 times, lactate synthesis (13C-labeled lactate enrichment) increased by 2.5 times in rats in the coma stage, Gln synthesis (Gln2) increased by 10 times in the precoma stage, and Glu synthesis (Glu4) decreased in the coma stage, while GABA synthesis did not show significant differences at any stage. Furthermore, Bosoi et al. (2014) used [1-13C] glucose and lactate labeling to trace neurotransmitter metabolism in the brains of rats with minimal hepatic encephalopathy (MHE) induced by bile duct ligation (BDL) and found that the de novo synthesis of lactate and Gln significantly increased in the brains of MHE rats. These results indicate the presence of neurotransmitter metabolism defects in MHE.
Neuroinflammation can affect the transmission of glutamatergic and GABAergic neurotransmitters (Cabrera-Pastor et al., 2019). Changes in glutamatergic and GABAergic neurotransmission are closely related to cognitive and motor changes in MHE patients (Llansola et al., 2015), and an increase in GABAergic tone in the brain is considered a characteristic of HE. Hassan et al. (2019) used transcranial magnetic stimulation to compare cerebellar inhibition (CBI) in 15 HE patients at different stages with 15 healthy controls. The results showed that CBI was reduced in HE patients at a stimulus interval of 5–7 ms, but the degree of CBI in patients at a stimulus interval of 7 ms was significantly correlated with the severity of HE, indicating an increase in GABAergic neurotransmission in the cerebellum of HE patients and a decrease in GABAergic neurotransmission in the motor cortex. Zöllner et al. (2023) study of 16 healthy controls and 19 MHE patients used edited MRS to measure GABA levels in the right cerebellum, left thalamus, and left motor cortex. The results showed that Gln levels were elevated in all three brain regions in MHE patients, whereas GABA levels were elevated in the cerebellum, and significantly decreased in the motor cortex and highly correlated with the severity of MHE. A clinical study also reported that the GABA-A receptor modulating steroid antagonist golexanolone improved cognition in MHE patients (Montagnese et al., 2021). Overall, these study results imply the important role of changes in the GABAergic system in the cerebellum and motor cortex in MHE.
Besides, neurotransmitter metabolic changes have been reported in patients with liver disease-related mild cognitive impairment. In NASH, rats with cognitive impairment, had decreased dopamine levels in the frontal cortex and the cerebellum and reduced norepinephrine levels in the striatum (Higarza et al., 2019). In patients with chronic hepatitis C cognitive impairment, the choline/creatine ratio in the basal ganglia and posterior cingulate gyrus was significantly increased, while the N-acetylaspartate/creatine ratio was significantly decreased. Cognitive impairment was also significantly negatively correlated with the choline/creatine ratio and positively correlated with the N-acetylaspartate/creatine ratio in the basal ganglia (Abo Hagar et al., 2018). Furthermore, Pflugrad et al. (2019) compared the brain MRS of healthy individuals with LT-related cognitive impairment patients before and after LT and found that after LT, there was an increase in myo-inositol in the thalamus, putamen, and white matter in LT cognitive impairment patients, and a decrease in glutamine/glutamate ratio in the putamen. Patients without cognitive impairment after LT only showed an increase in myo-inositol in the thalamus after LT, and there was no significant difference in brain MRS between transplant-related cognitive impairment patients and those without cognitive impairment.
The liver’s condition is closely intertwined with brain function. A study by Seo et al. (2016) revealed that elevated levels of liver enzymes, specifically aspartate aminotransferase (AST) and alanine aminotransferase (ALT), in patients with NAFLD are associated with impaired cognitive performance. Interestingly, in healthy individuals, plasma levels of ALT and AST not only display a significant negative correlation with memory capacity (Kamada et al., 2016), but also exhibit a noteworthy positive correlation with plasma Glu levels. AST and ALT serve as crucial indicators for assessing liver function biochemically, while also acting as vital enzymes involved in hepatic gluconeogenesis and the regulation of tissue glutamate production (Sookoian and Pirola, 2015). ALT facilitates a reversible transamination reaction between alanine and α-ketoglutarate, leading to the formation of pyruvate and glutamate. Conversely, AST catalyzes the reversible reaction between aspartate and α-ketoglutarate, resulting in the production of oxaloacetate and glutamate (Ellinger et al., 2011).
Notably, decreased ALT levels signify reduced liver metabolic activity and have been linked to a higher risk of dementia (Lu et al., 2021; He et al., 2022). Furthermore, a study by Nho et al. (2019) demonstrated demonstrated that lower serum ALT levels and an elevated AST/ALT ratio in individuals with Alzheimer’s disease (AD) are associated with poorer cognitive abilities, reduced brain glucose metabolism, and the deposition of amyloid-beta (Aβ). These findings suggest that reduced ALT levels may contribute to decreased pyruvate levels, leading to disrupted energy balance, compromised glutamate metabolism, and impaired synaptic transmission in the central nervous system. However, it’s important to note that Ferri et al. (2022) only observed lower serum ALT levels and higher AST/ALT ratios in elderly male dementia patients compared to cognitively normal individuals, with no significant differences observed in elderly females. In contrast, a study by Yokokawa et al. (2022) found a significant correlation between serum levels of brain-derived neurotrophic factor (BDNF) and liver enzymes in middle-aged and elderly females, along with a negative correlation between BDNF and liver fibrosis measured by the Fibrosis-4 (FIB-4) index. Although cognitive function was not assessed in this particular study, previous research has established a link between liver fibrosis and an increased risk of dementia (Weinstein et al., 2019; Solfrizzi et al., 2020; Jeong et al., 2022). Moreover, serum BDNF has been identified as a biomarker not only for cognitive function in elderly females (Komulainen et al., 2008) but also for the decline in cognitive abilities associated with mild cognitive impairment and dementia (Nikolac Perkovic et al., 2023). In addition, a study by Chen et al. (2020) reported that short-term exposure to bilirubin can induce AD-like brain pathology. In summary, while gender differences exist, liver enzymes play a significant role in the underlying mechanisms of dementia.
The liver, as the largest organ responsible for metabolite clearance in the bloodstream, plays a critical role in the peripheral clearance of plasma Aβ. Peripheral clearance of Aβ by the liver potentially facilitates the removal of Aβ from the brain, thus contributing to the treatment of AD (Liu et al., 2015). Impairment in liver function leading to reduced peripheral Aβ clearance is a significant factor in the accumulation of Aβ in the brain and the development of AD (Bassendine et al., 2020). A study by Cheng et al. (2023) revealed elevated plasma Aβ levels in patients with liver cirrhosis, and chronic impairment in hepatic Aβ clearance was found to increase brain Aβ deposition in APP/PS1 transgenic mice, resulting in neurodegeneration and cognitive deficits. These findings suggest that a decrease in hepatic Aβ clearance rate may be a potential factor in AD development. Additionally, Li et al. (2013) reported postoperative cognitive dysfunction in 44% of patients who underwent liver transplantation, which was associated with an increase in postoperative serum biomarkers of dementia, including Aβ, within 24 h after surgery. Moreover, NAFLD exacerbates Aβ plaque accumulation in transgenic AD mice, promoting the progression of AD (Kim et al., 2016). Furthermore, the clearance of peripheral Aβ relies on the transportation of circulating proteins such as albumin and apolipoprotein E, highlighting the significance of lipid metabolism disorders in the liver as contributing factors to Aβ accumulation and cognitive impairment (Cheng et al., 2020).
Furthermore, certain liver-derived factors have the potential to regulate cognition. For instance, Horowitz et al. (2020) reported that an elevated concentration of liver-derived glycosylphosphatidylinositol (GPI)-specific phospholipase D1 in the plasma of mice after exercise can improve hippocampal function and alleviate cognitive impairment in elderly mice. Yan et al. (2022) found that aerobic exercise increases the synthesis of liver methyl donors, leading to enhanced brain RNA N6-methyladenosine levels and exhibiting anti-anxiety effects. These research findings collectively suggest that liver-derived factors play a significant role in mild cognitive impairment associated with liver disease.
Recently, the development of Magnetic Resonance Spectroscopy (MRS) and Magnetic Resonance Imaging (MRI) techniques has provided non-invasive detection methods for exploring changes in brain structure and function in cognitive impairment (Chavarria and Cordoba, 2015). MRS detects the proton signals of metabolites and can distinguish the concentration of metabolites such as lactate, Glu, Gln, and GABA in the brain. Further, by adding substrates with special radioactive labeling such as 13C, it is possible to track the metabolic processes of compounds, and MRS related to neurotransmitter metabolism has been discussed in previous reviews. Brain MRI mainly images water proton signals in brain tissue. Conventional MRI images include T1 and T2-weighted images, which can provide information on the anatomy, metabolism, and water content of the brain. Moreover, functional Magnetic Resonance Imaging (fMRI) can assess the function of brain regions based on changes in blood oxygen signals generated by neuronal activity in brain functional areas and establish brain functional networks. Numerous studies have shown that the progress in mechanism research on mild cognitive impairment related to liver disease is closely related to the application of magnetic resonance brain imaging technology (see Table 1).
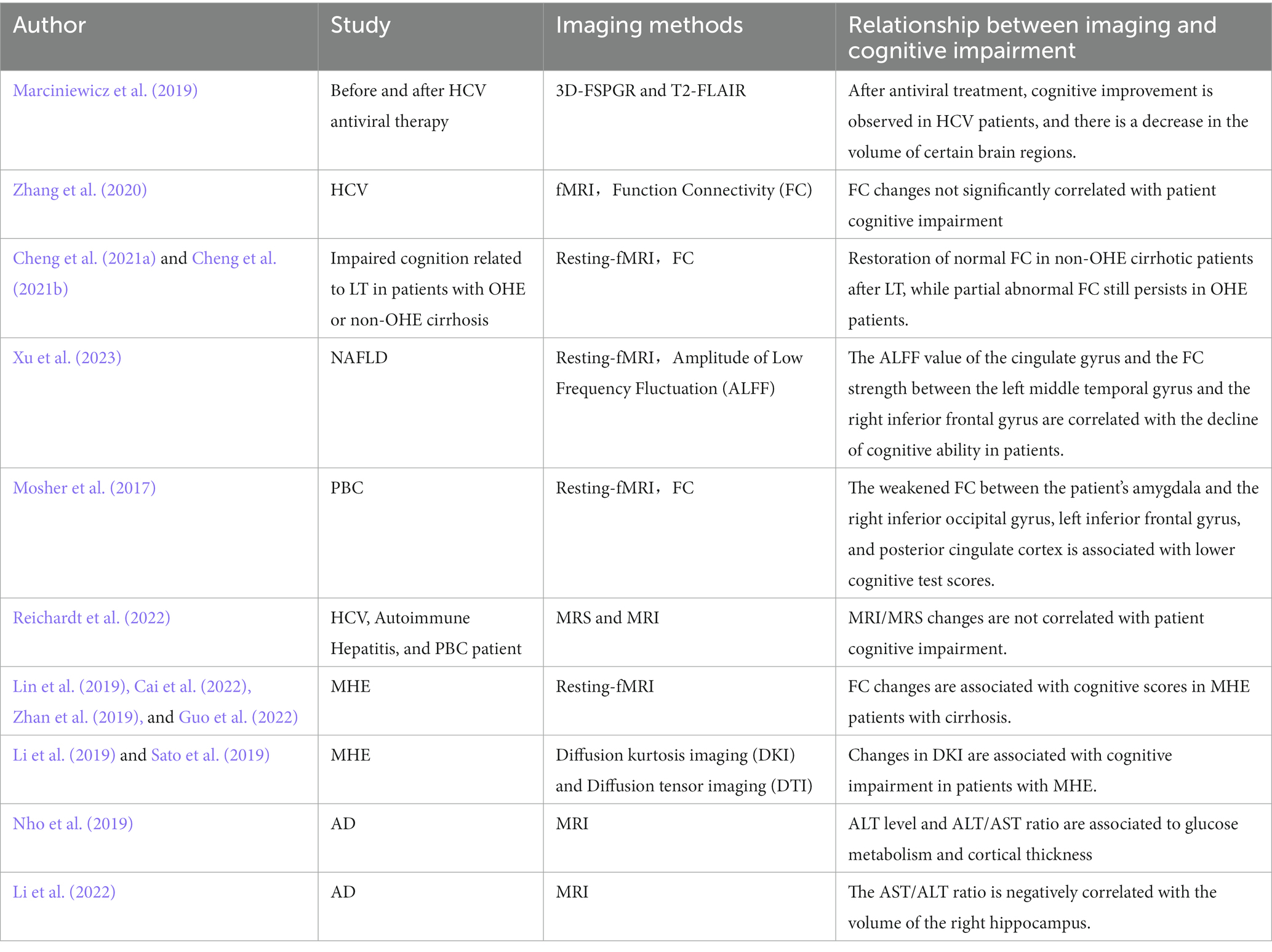
Table 1. Advances in magnetic resonance imaging for mild cognitive impairment in liver disease.
In the healthy population, there is a significant relationship between serum liver function markers and brain structure and function. Chen et al. (2021) discovered a positive correlation between serum proteins and gray matter volume (GMV) in the parahippocampal gyrus and amygdala. The levels of globulin and the albumin/globulin ratio were associated with GMV in the olfactory cortex and parahippocampal gyrus. Higher bilirubin levels were linked to increased regional homogeneity (ReHo) in the precentral gyrus, middle cingulate gyrus, and inferior frontal gyrus, while ReHo decreased in the caudate nucleus. Furthermore, elevated ALT levels were found to be correlated with increased cerebral blood flow (CBF) in the superior frontal gyrus and decreased CBF in the occipital gyrus, angular gyrus, precentral gyrus, and middle temporal gyrus.
In MHE patients, T1-weighted images mainly show high signal intensity in the globus pallidus and thalamic edema. Taylor-Robinson et al. (1995) compared the MRI findings of MHE patients, OHE patients, and patients with chronic liver cirrhosis but without cognitive impairment, and found that the signal intensity of the globus pallidus was significantly higher in patients with cognitive impairment than in those without, and that the T1 signal intensity of the globus pallidus was correlated with blood ammonia levels. However, this increased magnetic resonance signal intensity in the globus pallidus is believed to be caused by manganese deposition, as the T1 high signal is related to blood manganese concentration levels in patients with liver cirrhosis (Taylor-Robinson et al., 1995), and the manganese content in the globus pallidus was also shown to be significantly increased in HE patients on autopsy (Butterworth et al., 1995). Lin et al. (2022) also compared brain T1-weighted images of healthy individuals and patients with hepatitis B-related cirrhosis and illustrated that patients with cirrhosis had significant thalamic swelling even before the onset of MHE, which further extended to bilateral basal ganglia and the cortex. Cerebellar swelling occurred during the MHE stage, and thalamic swelling was significantly negatively correlated with cognitive ability in MHE patients. Winterdahl et al. (2019) likewise found increased water content in the brain white matter and thalamic edema in patients with mild HE, that can lead to damage to the basal ganglia-thalamus-cortex loop. Brain edema and increased water content were observed in MHE patients on T2-weighted images. Diffusion-weighted imaging (DWI) can be used to evaluate the diffusion ability of water molecules in tissues using the apparent diffusion coefficient (ADC). Sugimoto et al. (2008) demonstrated that the brain ADC value increased in MHE patients with liver cirrhosis, indicating significant brain edema in MHE patients, and that the ADC value of the frontal and parietal lobes could predict the progression of HE.
The high signal intensity of the globus pallidus in liver disease patients can recover within 5 months after liver transplantation (LT) (Long et al., 2009). Compared with LT patients without cognitive impairment, LT patients with cognitive impairment showed high signal intensity in the bilateral insular cortex and cingulate gyrus and extensive brain edema. MRI findings in non-alcoholic fatty liver disease (NAFLD) patients indicate white matter lesions (Petta et al., 2016) and reduced brain volume (Weinstein et al., 2018), and the relationship between decrease in brain volume and cognitive impairment (Filipović et al., 2018). In chronic hepatitis C, Thames et al. (2015) found that fractional anisotropy scores in the striatum of HCV patients with cognitive impairment increased as well as the mean diffusion coefficients in the cingulum and external capsule, and that the diffusion coefficient in the superior longitudinal fasciculus was significantly correlated with patient cognitive performance. Prell et al. (2019) also reported that compared with the control group, HCV patients with cognitive impairment had gray matter atrophy in the bilateral insular cortex and thalamus, increased gray matter volume in the cerebellum, and that gray matter atrophy in the left amygdala and left parahippocampal area worsened during the 7-year disease progression.
Additionally, changes in functional connectivity (FC) of the brain are also important causes of mild cognitive impairment (MCI) related to liver disease. Ye et al. (2020) compared interhemispheric functional connectivity and the corpus callosum volume between healthy controls, patients with minimal hepatic encephalopathy (MHE), and those with cirrhosis without MHE, and reported that patients with MHE showed corpus callosum degeneration and interhemispheric connectivity disorders. At the global level of the brain, Gou et al. (2020) determined that the small-worldness of the brain structural network was significantly reduced in patients with MHE, and the network integration and module separation were decreased. Brain functional connectivity significantly improved after LT treatment in patients with HE (Ahluwalia et al., 2016). However, Cheng et al. (2018) showed that after LT treatment, most of the abnormal functional connectivity strength in patients without HE returned to normal levels, but HE patients still retained most of the abnormal functional connectivity strength, including brain areas related to advanced cognition such as the frontal and parietal lobes. This suggests that the recovery of brain functional connectivity after LT is influenced by the history of HE before transplantation. In summary, magnetic resonance imaging can provide a non-invasive method for studying brain metabolism, structure, and function in patients with liver disease-related MCI, which is helpful for exploring the mechanisms related to cognitive impairment and for diagnosing and treating liver disease-related MCI in clinical practice.
Liver diseases such as MHE, NAFLD, cholestatic liver disease, and mild cognitive impairment in liver transplant recipients are very common. Cognitive impairment not only seriously reduces the quality of life of patients but can also progress to overt hepatic encephalopathy, leading to poor prognosis for patients. This review summarized the mechanisms underlying mild cognitive impairment in liver disease, including high blood ammonia, neuroinflammation, brain energy metabolic disorders, and neurotransmitter metabolic disorders, liver-derived factors, as well as the emerging research progress in magnetic resonance imaging of the brain, in order to provide ideas for the prevention and treatment of mild cognitive impairment in liver disease.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
This work was supported by the National Natural Science Foundation of China (Nos. 82070302 and 81873467).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abo Hagar, A., Ashour, Y., Negm, M., Abdelfatah, M., Gad, K. A., and Hashish, E. (2018). Brain magnetic resonance spectroscopy and cognitive impairment in chronic hepatitis C patients. Egypt. J. Neurol. Psychiatr. Neurosurg. 54:43. doi: 10.1186/s41983-018-0046-7
Ahluwalia, V., Wade, J. B., White, M. B., Gilles, H. S., Heuman, D. M., Fuchs, M., et al. (2016). Liver transplantation significantly improves global functioning and cerebral processing. Liver Transpl. 22, 1379–1390. doi: 10.1002/lt.24498
Ahmad, A., Patel, V., Xiao, J., and Khan, M. M. (2020). The role of neurovascular system in neurodegenerative diseases. Mol. Neurobiol. 57, 4373–4393. doi: 10.1007/s12035-020-02023-z
Aldridge, D. R., Tranah, E. J., and Shawcross, D. L. (2015). Pathogenesis of hepatic encephalopathy: role of ammonia and systemic inflammation. J. Clin. Exp. Hepatol. 5, S7–s20. doi: 10.1016/j.jceh.2014.06.004
Allampati, S., Duarte-Rojo, A., Thacker, L. R., Patidar, K. R., White, M. B., Klair, J. S., et al. (2016). Diagnosis of minimal hepatic encephalopathy using stroop EncephalApp: a multicenter US-based, norm-based study. Am. J. Gastroenterol. 111, 78–86. doi: 10.1038/ajg.2015.377
An, K., Starkweather, A., Sturgill, J., Salyer, J., and Sterling, R. K. (2019). Association of CTRP13 with liver enzymes and cognitive symptoms in nonalcoholic fatty liver disease. Nurs. Res. 68, 29–38. doi: 10.1097/nnr.0000000000000319
Bajaj, J. S., Cordoba, J., Mullen, K. D., Amodio, P., Shawcross, D. L., Butterworth, R. F., et al. (2011). Review article: the design of clinical trials in hepatic encephalopathy--an International Society for Hepatic Encephalopathy and Nitrogen Metabolism (ISHEN) consensus statement. Aliment. Pharmacol. Ther. 33, 739–747. doi: 10.1111/j.1365-2036.2011.04590.x
Bajaj, J. S., Saeian, K., Schubert, C. M., Hafeezullah, M., Franco, J., Varma, R. R., et al. (2009). Minimal hepatic encephalopathy is associated with motor vehicle crashes: the reality beyond the driving test. Hepatology 50, 1175–1183. doi: 10.1002/hep.23128
Balzano, T., Forteza, J., Molina, P., Giner, J., Monzó, A., Sancho-Jiménez, J., et al. (2018). The cerebellum of patients with steatohepatitis shows lymphocyte infiltration, microglial activation and loss of Purkinje and granular neurons. Sci. Rep. 8:3004. doi: 10.1038/s41598-018-21399-6
Bassendine, M. F., Taylor-Robinson, S. D., Fertleman, M., Khan, M., and Neely, D. (2020). Is Alzheimer's disease a liver disease of the brain? J. Alzheimers Dis. 75, 1–14. doi: 10.3233/jad-190848
Bélanger, M., Allaman, I., and Magistretti, P. J. (2011). Brain energy metabolism: focus on astrocyte-neuron metabolic cooperation. Cell Metab. 14, 724–738. doi: 10.1016/j.cmet.2011.08.016
Bobermin, L. D., Roppa, R. H. A., Gonçalves, C. A., and Quincozes-Santos, A. (2020). Ammonia-induced glial-inflammaging. Mol. Neurobiol. 57, 3552–3567. doi: 10.1007/s12035-020-01985-4
Bokemeyer, M., Ding, X. Q., Goldbecker, A., Raab, P., Heeren, M., Arvanitis, D., et al. (2011). Evidence for neuroinflammation and neuroprotection in HCV infection-associated encephalopathy. Gut 60, 370–377. doi: 10.1136/gut.2010.217976
Bordone, M. P., Salman, M. M., Titus, H. E., Amini, E., Andersen, J. V., Chakraborti, B., et al. (2019). The energetic brain – a review from students to students. J. Neurochem. 151, 139–165. doi: 10.1111/jnc.14829
Bosoi, C. R., and Rose, C. F. (2014). Elevated cerebral lactate: implications in the pathogenesis of hepatic encephalopathy. Metab. Brain Dis. 29, 919–925. doi: 10.1007/s11011-014-9573-9
Bosoi, C. R., Zwingmann, C., Marin, H., Parent-Robitaille, C., Huynh, J., Tremblay, M., et al. (2014). Increased brain lactate is central to the development of brain edema in rats with chronic liver disease. J. Hepatol. 60, 554–560. doi: 10.1016/j.jhep.2013.10.011
Butterworth, R. F., Spahr, L., Fontaine, S., and Layrargues, G. P. (1995). Manganese toxicity, dopaminergic dysfunction and hepatic encephalopathy. Metab. Brain Dis. 10, 259–267. doi: 10.1007/bf02109357
Cabrera-Pastor, A., Llansola, M., Montoliu, C., Malaguarnera, M., Balzano, T., Taoro-Gonzalez, L., et al. (2019). Peripheral inflammation induces neuroinflammation that alters neurotransmission and cognitive and motor function in hepatic encephalopathy: underlying mechanisms and therapeutic implications. Acta Physiol. 226:e13270. doi: 10.1111/apha.13270
Cai, L. M., Shi, J. Y., Dong, Q. Y., Wei, J., and Chen, H. J. (2022). Aberrant stability of brain functional architecture in cirrhotic patients with minimal hepatic encephalopathy. Brain Imaging Behav. 16, 2258–2267. doi: 10.1007/s11682-022-00696-9
Campagna, F., Montagnese, S., Schiff, S., Biancardi, A., Mapelli, D., Angeli, P., et al. (2014). Cognitive impairment and electroencephalographic alterations before and after liver transplantation: what is reversible? Liver Transpl. 20, 977–986. doi: 10.1002/lt.23909
Chavarria, L., and Cordoba, J. (2015). Magnetic resonance imaging and spectroscopy in hepatic encephalopathy. J. Clin. Exp. Hepatol. 5, S69–S74. doi: 10.1016/j.jceh.2013.10.001
Chen, H., Liang, L., Xu, H., Xu, J., Yao, L., Li, Y., et al. (2020). Short term exposure to bilirubin induces encephalopathy similar to Alzheimer's disease in late life. J. Alzheimers Dis. 73, 277–295. doi: 10.3233/jad-190945
Chen, J., Liu, S., Wang, C., Zhang, C., Cai, H., Zhang, M., et al. (2021). Associations of serum liver function markers with brain structure, function, and perfusion in healthy young adults. Front. Neurol. 12:606094. doi: 10.3389/fneur.2021.606094
Cheng, Y., He, C. Y., Tian, D. Y., Chen, S. H., Ren, J. R., Sun, H. L., et al. (2023). Physiological β-amyloid clearance by the liver and its therapeutic potential for Alzheimer's disease. Acta Neuropathol. 145, 717–731. doi: 10.1007/s00401-023-02559-z
Cheng, Y., Li, J. L., Zhou, J. M., Zhang, G. Y., Shen, W., and Zhang, X. D. (2021a). Renormalization of thalamic sub-regional functional connectivity contributes to improvement of cognitive function after liver transplantation in cirrhotic patients with overt hepatic encephalopathy. Korean J. Radiol. 22, 2052–2061. doi: 10.3348/kjr.2020.1432
Cheng, Y., Shen, W., Xu, J., Amey, R. C., Huang, L. X., Zhang, X. D., et al. (2021b). Neuromarkers from whole-brain functional connectivity reveal the cognitive recovery scheme for overt hepatic encephalopathy after liver transplantation. eNeuro 8. doi: 10.1523/eneuro.0114-1521.2021
Cheng, Y., Tian, D. Y., and Wang, Y. J. (2020). Peripheral clearance of brain-derived Aβ in Alzheimer's disease: pathophysiology and therapeutic perspectives. Transl. Neurodegener. 9:16. doi: 10.1186/s40035-020-00195-1
Cheng, Y., Zhang, G., Shen, W., Huang, L. X., Zhang, L., Xie, S. S., et al. (2018). Impact of previous episodes of hepatic encephalopathy on short-term brain function recovery after liver transplantation: a functional connectivity strength study. Metab. Brain Dis. 33, 237–249. doi: 10.1007/s11011-017-0155-5
Collie, A. (2005). Cognition in liver disease. Liver Int. 25, 1–8. doi: 10.1111/j.1478-3231.2005.01012.x
Cudalbu, C., and Taylor-Robinson, S. D. (2019). Brain edema in chronic hepatic encephalopathy. J. Clin. Exp. Hepatol. 9, 362–382. doi: 10.1016/j.jceh.2019.02.003
Duszynski, C. C., Avati, V., Lapointe, A. P., Scholkmann, F., Dunn, J. F., and Swain, M. G. (2020). Near-infrared spectroscopy reveals brain hypoxia and cerebrovascular dysregulation in primary biliary cholangitis. Hepatology 71, 1408–1420. doi: 10.1002/hep.30920
Ellinger, J. J., Lewis, I. A., and Markley, J. L. (2011). Role of aminotransferases in glutamate metabolism of human erythrocytes. J. Biomol. NMR 49, 221–229. doi: 10.1007/s10858-011-9481-9
Fabrellas, N., Moreira, R., Carol, M., Cervera, M., de Prada, G., Perez, M., et al. (2020). Psychological burden of hepatic encephalopathy on patients and caregivers. Clin. Transl. Gastroenterol. 11:e00159. doi: 10.14309/ctg.0000000000000159
Felipo, V., Urios, A., Montesinos, E., Molina, I., Garcia-Torres, M. L., Civera, M., et al. (2012). Contribution of hyperammonemia and inflammatory factors to cognitive impairment in minimal hepatic encephalopathy. Metab. Brain Dis. 27, 51–58. doi: 10.1007/s11011-011-9269-3
Ferri, E., Rossi, P. D., Scichilone, M., Lucchi, T. A., and Arosio, B. (2022). Liver enzymes in a cohort of community-dwelling older persons: focus on sex contribution. Nutrients 14:4973. doi: 10.3390/nu14234973
Filipović, B., Marković, O., Đurić, V., and Filipović, B. (2018). Cognitive changes and brain volume reduction in patients with nonalcoholic fatty liver disease. Can. J. Gastroenterol. Hepatol. 2018:9638797. doi: 10.1155/2018/9638797
Garcia-Martinez, R., Rovira, A., Alonso, J., Jacas, C., Simón-Talero, M., Chavarria, L., et al. (2011). Hepatic encephalopathy is associated with posttransplant cognitive function and brain volume. Liver Transpl. 17, 38–46. doi: 10.1002/lt.22197
Getsuwan, S., Chuthapisith, J., Treepongkaruna, S., Butsriphum, N., Prabpram, W., Charoenthanakit, C., et al. (2021). Behavior problems and cognitive function in pediatric liver transplant recipients. Transplant. Proc. 53, 649–655. doi: 10.1016/j.transproceed.2020.10.041
Gou, L. B., Zhang, W., Guo, D. J., Zhong, W. J., Wu, X. J., and Zhou, Z. M. (2020). Aberrant brain structural network and altered topological organization in minimal hepatic encephalopathy. Diagn. Interv. Radiol. 26, 255–261. doi: 10.5152/dir.2019.19216
Guo, J. R., Shi, J. Y., Dong, Q. Y., Cao, Y. B., Li, D., and Chen, H. J. (2022). Altered dynamic spontaneous neural activity in minimal hepatic encephalopathy. Front. Neurol. 13:963551. doi: 10.3389/fneur.2022.963551
Hadjihambi, A., Arias, N., Sheikh, M., and Jalan, R. (2018). Hepatic encephalopathy: a critical current review. Hepatol. Int. 12, 135–147. doi: 10.1007/s12072-017-9812-3
Hadjihambi, A., Cudalbu, C., Pierzchala, K., Simicic, D., Donnelly, C., Konstantinou, C., et al. (2022). Abnormal brain oxygen homeostasis in an animal model of liver disease. JHEP Rep. 4:100509. doi: 10.1016/j.jhepr.2022.100509
Hadjihambi, A., De Chiara, F., Hosford, P. S., Habtetion, A., Karagiannis, A., Davies, N., et al. (2017). Ammonia mediates cortical hemichannel dysfunction in rodent models of chronic liver disease. Hepatology 65, 1306–1318. doi: 10.1002/hep.29031
Hartmann, I. J., Groeneweg, M., Quero, J. C., Beijeman, S. J., de Man, R. A., Hop, W. C., et al. (2000). The prognostic significance of subclinical hepatic encephalopathy. Am. J. Gastroenterol. 95, 2029–2034. doi: 10.1111/j.1572-0241.2000.02265.x
Hassan, S. S., Baumgarten, T. J., Ali, A. M., Füllenbach, N. D., Jördens, M. S., Häussinger, D., et al. (2019). Cerebellar inhibition in hepatic encephalopathy. Clin. Neurophysiol. 130, 886–892. doi: 10.1016/j.clinph.2019.02.020
He, X. Y., Kuo, K., Yang, L., Zhang, Y. R., Wu, B. S., Chen, S. D., et al. (2022). Serum clinical laboratory tests and risk of incident dementia: a prospective cohort study of 407,190 individuals. Transl. Psychiatry 12:312. doi: 10.1038/s41398-022-02082-x
He, Z., Liu, Y., Li, Z., Sun, T., Li, Z., Manyande, A., et al. (2023). Gut microbiota regulates circadian oscillation in hepatic ischemia-reperfusion injury-induced cognitive impairment by interfering with hippocampal lipid metabolism in mice. Hepatol. Int. doi: 10.1007/s12072-023-10509-w
Higarza, S. G., Arboleya, S., Gueimonde, M., Gómez-Lázaro, E., Arias, J. L., and Arias, N. (2019). Neurobehavioral dysfunction in non-alcoholic steatohepatitis is associated with hyperammonemia, gut dysbiosis, and metabolic and functional brain regional deficits. PLoS One 14:e0223019. doi: 10.1371/journal.pone.0223019
Horowitz, A. M., Fan, X., Bieri, G., Smith, L. K., Sanchez-Diaz, C. I., Schroer, A. B., et al. (2020). Blood factors transfer beneficial effects of exercise on neurogenesis and cognition to the aged brain. Science 369, 167–173. doi: 10.1126/science.aaw2622
Huang, L., Nakamura, Y., Lo, E. H., and Hayakawa, K. (2019). Astrocyte signaling in the neurovascular unit after central nervous system injury. Int. J. Mol. Sci. 20, 282. doi: 10.3390/ijms20020282
Ibáñez-Samaniego, L., Rapado-Castro, M., Cabrero, L., Navarrete, C., García-Mulas, S., Ahumada, A., et al. (2022). Hepatitis C eradication improves cognitive function in patients with or without cirrhosis: a prospective real-life study. Eur. J. Neurol. 29, 400–412. doi: 10.1111/ene.15138
Jaffe, A., Lim, J. K., and Jakab, S. S. (2020). Pathophysiology of hepatic encephalopathy. Clin. Liver Dis. 24, 175–188. doi: 10.1016/j.cld.2020.01.002
Jayakumar, A. R., and Norenberg, M. D. (2016). Glutamine Synthetase: role in neurological disorders. Adv. Neurobiol. 13, 327–350. doi: 10.1007/978-3-319-45096-4_13
Jayakumar, A. R., Rama Rao, K. V., and Norenberg, M. D. (2015). Neuroinflammation in hepatic encephalopathy: mechanistic aspects. J. Clin. Exp. Hepatol. 5, S21–S28. doi: 10.1016/j.jceh.2014.07.006
Jeong, S., Oh, Y. H., Choi, S., Chang, J., Kim, S. M., Son, J. S., et al. (2022). Association of non-alcoholic fatty liver disease with incident dementia later in life among elder adults. Clin. Mol. Hepatol. 28, 510–521. doi: 10.3350/cmh.2021.0332
Jiménez, B., Montoliu, C., MacIntyre, D. A., Serra, M. A., Wassel, A., Jover, M., et al. (2010). Serum metabolic signature of minimal hepatic encephalopathy by (1)H-nuclear magnetic resonance. J. Proteome Res. 9, 5180–5187. doi: 10.1021/pr100486e
Kamada, Y., Hashimoto, R., Yamamori, H., Yasuda, Y., Takehara, T., Fujita, Y., et al. (2016). Impact of plasma transaminase levels on the peripheral blood glutamate levels and memory functions in healthy subjects. BBA Clin. 5, 101–107. doi: 10.1016/j.bbacli.2016.02.004
Kang, D. J., Betrapally, N. S., Ghosh, S. A., Sartor, R. B., Hylemon, P. B., Gillevet, P. M., et al. (2016). Gut microbiota drive the development of neuroinflammatory response in cirrhosis in mice. Hepatology 64, 1232–1248. doi: 10.1002/hep.28696
Kim, D. G., Krenz, A., Toussaint, L. E., Maurer, K. J., Robinson, S. A., Yan, A., et al. (2016). Non-alcoholic fatty liver disease induces signs of Alzheimer's disease (AD) in wild-type mice and accelerates pathological signs of AD in an AD model. J. Neuroinflammation 13:1. doi: 10.1186/s12974-015-0467-5
Kim, M., Liotta, E. M., Zee, P. C., Ganger, D. R., Ladner, D. P., Karmarkar, A., et al. (2019). Impaired cognition predicts the risk of hospitalization and death in cirrhosis. Ann. Clin. Transl. Neurol. 6, 2282–2290. doi: 10.1002/acn3.50924
Kjaergaard, K., Mikkelsen, A. C. D., Wernberg, C. W., Gronkjaer, L. L., Eriksen, P. L., Damholdt, M. F., et al. (2021). Cognitive dysfunction in non-alcoholic fatty liver disease-current knowledge, mechanisms and perspectives. J. Clin. Med. 10, 673. doi: 10.3390/jcm10040673
Komulainen, P., Pedersen, M., Hänninen, T., Bruunsgaard, H., Lakka, T. A., Kivipelto, M., et al. (2008). BDNF is a novel marker of cognitive function in ageing women: the DR's EXTRA study. Neurobiol. Learn. Mem. 90, 596–603. doi: 10.1016/j.nlm.2008.07.014
Kornerup, L. S., Pflugrad, H., Weissenborn, K., Vilstrup, H., and Dam, G. (2019). Cognitive impairment after liver transplantation: residual hepatic encephalopathy or posttransplant encephalopathy? Hepat. Med. 11, 41–46. doi: 10.2147/hmer.S144667
Kraus, M. R., Schäfer, A., Teuber, G., Porst, H., Sprinzl, K., Wollschläger, S., et al. (2013). Improvement of neurocognitive function in responders to an antiviral therapy for chronic hepatitis C. Hepatology 58, 497–504. doi: 10.1002/hep.26229
Lauridsen, M. M., Jepsen, P., and Vilstrup, H. (2011). Critical flicker frequency and continuous reaction times for the diagnosis of minimal hepatic encephalopathy: a comparative study of 154 patients with liver disease. Metab. Brain Dis. 26, 135–139. doi: 10.1007/s11011-011-9242-1
Li, J. L., Jiang, H., Zhang, X. D., Huang, L. X., Xie, S. S., Zhang, L., et al. (2019). Microstructural brain abnormalities correlate with neurocognitive dysfunction in minimal hepatic encephalopathy: a diffusion kurtosis imaging study. Neuroradiology 61, 685–694. doi: 10.1007/s00234-019-02201-4
Li, X., Wen, D. X., Zhao, Y. H., Hang, Y. N., and Mandell, M. S. (2013). Increase of beta-amyloid and C-reactive protein in liver transplant recipients with postoperative cognitive dysfunction. Hepatobiliary Pancreat. Dis. Int. 12, 370–376. doi: 10.1016/s1499-3872(13)60058-2
Li, W., Yue, L., Sun, L., and Xiao, S. (2022). An increased aspartate to alanine aminotransferase ratio is associated with a higher risk of cognitive impairment. Front. Med. (Lausanne) 9:780174. doi: 10.3389/fmed.2022.780174
Limón, I. D., Angulo-Cruz, I., Sánchez-Abdon, L., and Patricio-Martínez, A. (2021). Disturbance of the glutamate-glutamine cycle, secondary to hepatic damage, compromises memory function. Front. Neurosci. 15:578922. doi: 10.3389/fnins.2021.578922
Lin, W., Chen, X., Gao, Y. Q., Yang, Z. T., Yang, W., and Chen, H. J. (2019). Hippocampal atrophy and functional connectivity disruption in cirrhotic patients with minimal hepatic encephalopathy. Metab. Brain Dis. 34, 1519–1529. doi: 10.1007/s11011-019-00457-6
Lin, S., Guo, Z., Chen, S., Lin, X., Ye, M., and Qiu, Y. (2022). Progressive brain structural impairment assessed via network and causal analysis in patients with hepatitis B virus-related cirrhosis. Front. Neurol. 13:849571. doi: 10.3389/fneur.2022.849571
Liu, Q., Liu, C., Hu, F., Deng, X., and Zhang, Y. (2021). Non-alcoholic fatty liver disease and longitudinal cognitive changes in middle-aged and elderly adults. Front. Med. (Lausanne) 8:738835. doi: 10.3389/fmed.2021.738835
Liu, Y., Tian, S., Jia, G., Han, Z., Guo, C., Shang, Y., et al. (2021). Symptoms burden and health-related quality of life in Chinese patients with primary biliary cholangitis. J. Clin. Transl. Hepatol. 9, 860–867. doi: 10.14218/jcth.2020.00119
Liu, Y. H., Wang, Y. R., Xiang, Y., Zhou, H. D., Giunta, B., Mañucat-Tan, N. B., et al. (2015). Clearance of amyloid-beta in Alzheimer's disease: shifting the action site from center to periphery. Mol. Neurobiol. 51, 1–7. doi: 10.1007/s12035-014-8694-9
Llansola, M., Montoliu, C., Agusti, A., Hernandez-Rabaza, V., Cabrera-Pastor, A., Gomez-Gimenez, B., et al. (2015). Interplay between glutamatergic and GABAergic neurotransmission alterations in cognitive and motor impairment in minimal hepatic encephalopathy. Neurochem. Int. 88, 15–19. doi: 10.1016/j.neuint.2014.10.011
Lockwood, A. H., Yap, E. W., and Wong, W. H. (1991). Cerebral ammonia metabolism in patients with severe liver disease and minimal hepatic encephalopathy. J. Cereb. Blood Flow Metab. 11, 337–341. doi: 10.1038/jcbfm.1991.67
Long, L. L., Li, X. R., Huang, Z. K., Jiang, Y. M., Fu, S. X., and Zheng, W. (2009). Relationship between changes in brain MRI and (1)H-MRS, severity of chronic liver damage, and recovery after liver transplantation. Exp. Biol. Med. (Maywood) 234, 1075–1085. doi: 10.3181/0903-rm-118
Lu, Y., Pike, J. R., Selvin, E., Mosley, T., Palta, P., Sharrett, A. R., et al. (2021). Low liver enzymes and risk of dementia: the atherosclerosis risk in communities (ARIC) study. J. Alzheimers Dis. 79, 1775–1784. doi: 10.3233/jad-201241
Lu, L., Wu, C., Lu, B. J., Xie, D., Wang, Z., Bahaji Azami, N. L., et al. (2020). BabaoDan cures hepatic encephalopathy by decreasing ammonia levels and alleviating inflammation in rats. J. Ethnopharmacol. 249:112301. doi: 10.1016/j.jep.2019.112301
Magistretti, P. J., and Allaman, I. (2018). Lactate in the brain: from metabolic end-product to signalling molecule. Nat. Rev. Neurosci. 19, 235–249. doi: 10.1038/nrn.2018.19
Marciniewicz, E., Podgórski, P., Pawłowski, T., Małyszczak, K., Fleischer-Stępniewska, K., Knysz, B., et al. (2019). Evaluation of brain volume alterations in HCV-infected patients after interferon-free therapy: a pilot study. J. Neurol. Sci. 399, 36–43. doi: 10.1016/j.jns.2019.02.002
Mazzaro, C., Quartuccio, L., Adinolfi, L. E., Roccatello, D., Pozzato, G., Nevola, R., et al. (2021). A review on extrahepatic manifestations of chronic hepatitis C virus infection and the impact of direct-acting antiviral therapy. Viruses 13, 2249. doi: 10.3390/v13112249
Mina, A., Moran, S., Ortiz-Olvera, N., Mera, R., and Uribe, M. (2014). Prevalence of minimal hepatic encephalopathy and quality of life in patients with decompensated cirrhosis. Hepatol. Res. 44, E92–E99. doi: 10.1111/hepr.12227
Montagnese, S., Lauridsen, M., Vilstrup, H., Zarantonello, L., Lakner, G., Fitilev, S., et al. (2021). A pilot study of golexanolone, a new GABA-A receptor-modulating steroid antagonist, in patients with covert hepatic encephalopathy. J. Hepatol. 75, 98–107. doi: 10.1016/j.jhep.2021.03.012
Moran, S., López-Sánchez, M., Milke-García, M. D. P., and Rodríguez-Leal, G. (2021). Current approach to treatment of minimal hepatic encephalopathy in patients with liver cirrhosis. World J. Gastroenterol. 27, 3050–3063. doi: 10.3748/wjg.v27.i22.3050
Mosher, V. A. L., Swain, M. G., Pang, J. X. Q., Kaplan, G. G., Sharkey, K. A., MacQueen, G. M., et al. (2017). Primary biliary cholangitis alters functional connections of the Brain's deep gray matter. Clin. Transl. Gastroenterol. 8:e107. doi: 10.1038/ctg.2017.34
Nakanishi, H., Kurosaki, M., Nakanishi, K., Tsuchiya, K., Noda, T., Tamaki, N., et al. (2014). Impaired brain activity in cirrhotic patients with minimal hepatic encephalopathy: evaluation by near-infrared spectroscopy. Hepatol. Res. 44, 319–326. doi: 10.1111/hepr.12127
Newton, J. L., Hollingsworth, K. G., Taylor, R., El-Sharkawy, A. M., Khan, Z. U., Pearce, R., et al. (2008). Cognitive impairment in primary biliary cirrhosis: symptom impact and potential etiology. Hepatology 48, 541–549. doi: 10.1002/hep.22371
Nho, K., Kueider-Paisley, A., Ahmad, S., Mahmoudian Dehkordi, S., Arnold, M., Risacher, S. L., et al. (2019). Association of Altered Liver Enzymes with Alzheimer Disease Diagnosis, cognition, neuroimaging measures, and cerebrospinal fluid biomarkers. JAMA Netw. Open 2:e197978. doi: 10.1001/jamanetworkopen.2019.7978
Nikolac Perkovic, M., Borovecki, F., Filipcic, I., Vuic, B., Milos, T., Nedic Erjavec, G., et al. (2023). Relationship between brain-derived neurotrophic factor and cognitive decline in patients with mild cognitive impairment and dementia. Biomol. Ther. 13, 570. doi: 10.3390/biom13030570
Pellerin, L., Bouzier-Sore, A. K., Aubert, A., Serres, S., Merle, M., Costalat, R., et al. (2007). Activity-dependent regulation of energy metabolism by astrocytes: an update. Glia 55, 1251–1262. doi: 10.1002/glia.20528
Petta, S., Tuttolomondo, A., Gagliardo, C., Zafonte, R., Brancatelli, G., Cabibi, D., et al. (2016). The presence of White matter lesions is associated with the fibrosis severity of nonalcoholic fatty liver disease. Medicine 95:e3446. doi: 10.1097/md.0000000000003446
Pflugrad, H., Meyer, G. J., Dirks, M., Raab, P., Tryc, A. B., Goldbecker, A., et al. (2016). Cerebral microglia activation in hepatitis C virus infection correlates to cognitive dysfunction. J. Viral Hepat. 23, 348–357. doi: 10.1111/jvh.12496
Pflugrad, H., Tryc, A. B., Goldbecker, A., Barg-Hock, H., Strassburg, C., Klempnauer, J., et al. (2019). Cerebral metabolite alterations in patients with posttransplant encephalopathy after liver transplantation. PLoS One 14:e0221626. doi: 10.1371/journal.pone.0221626
Phaw, N. A., Leighton, J., Dyson, J. K., and Jones, D. E. (2021). Managing cognitive symptoms and fatigue in cholestatic liver disease. Expert Rev. Gastroenterol. Hepatol. 15, 235–241. doi: 10.1080/17474124.2021.1844565
Prell, T., Dirks, M., Arvanitis, D., Braun, D., Peschel, T., Worthmann, H., et al. (2019). Cerebral patterns of neuropsychological disturbances in hepatitis C patients. J. Neurovirol. 25, 229–238. doi: 10.1007/s13365-018-0709-2
Qvartskhava, N., Lang, P. A., Görg, B., Pozdeev, V. I., Ortiz, M. P., Lang, K. S., et al. (2015). Hyperammonemia in gene-targeted mice lacking functional hepatic glutamine synthetase. Proc. Natl. Acad. Sci. U. S. A. 112, 5521–5526. doi: 10.1073/pnas.1423968112
Rama Rao, K. V., and Norenberg, M. D. (2014). Glutamine in the pathogenesis of hepatic encephalopathy: the trojan horse hypothesis revisited. Neurochem. Res. 39, 593–598. doi: 10.1007/s11064-012-0955-2
Reichardt, J. L., Dirks, M., Wirries, A. K., Pflugrad, H., Nösel, P., Haag, K., et al. (2022). Brain metabolic and microstructural alterations associated with hepatitis C virus infection, autoimmune hepatitis and primary biliary cholangitis. Liver Int. 42, 842–852. doi: 10.1111/liv.15093
Rose, C. F., Amodio, P., Bajaj, J. S., Dhiman, R. K., Montagnese, S., Taylor-Robinson, S. D., et al. (2020). Hepatic encephalopathy: novel insights into classification, pathophysiology and therapy. J. Hepatol. 73, 1526–1547. doi: 10.1016/j.jhep.2020.07.013
Sato, T., Endo, K., Kakisaka, K., Suzuki, Y., Kooka, Y., Sawara, K., et al. (2019). Decreased mean kurtosis in the putamen is a diagnostic feature of minimal hepatic encephalopathy in patients with cirrhosis. Intern. Med. 58, 1217–1224. doi: 10.2169/internalmedicine.2116-18
Schousboe, A., Scafidi, S., Bak, L. K., Waagepetersen, H. S., and McKenna, M. C. (2014). Glutamate metabolism in the brain focusing on astrocytes. Adv. Neurobiol. 11, 13–30. doi: 10.1007/978-3-319-08894-5_2
Seo, S. W., Gottesman, R. F., Clark, J. M., Hernaez, R., Chang, Y., Kim, C., et al. (2016). Nonalcoholic fatty liver disease is associated with cognitive function in adults. Neurology 86, 1136–1142. doi: 10.1212/wnl.0000000000002498
Shawcross, D. L., Davies, N. A., Williams, R., and Jalan, R. (2004). Systemic inflammatory response exacerbates the neuropsychological effects of induced hyperammonemia in cirrhosis. J. Hepatol. 40, 247–254. doi: 10.1016/j.jhep.2003.10.016
Shawcross, D. L., Wright, G., Olde Damink, S. W., and Jalan, R. (2007). Role of ammonia and inflammation in minimal hepatic encephalopathy. Metab. Brain Dis. 22, 125–138. doi: 10.1007/s11011-006-9042-1
Sheeler, C., Rosa, J. G., Ferro, A., McAdams, B., Borgenheimer, E., and Cvetanovic, M. (2020). Glia in neurodegeneration: the housekeeper, the defender and the perpetrator. Int. J. Mol. Sci. 21, 9188. doi: 10.3390/ijms21239188
Shrestha, D., Rathi, S., Grover, S., Taneja, S., Duseja, A., Chawla, Y. K., et al. (2020). Factors affecting psychological burden on the informal caregiver of patients with cirrhosis: looking beyond the patient. J. Clin. Exp. Hepatol. 10, 9–16. doi: 10.1016/j.jceh.2019.06.002
Simicic, D., Pierzchala, K., Rackayová, V., Braissant, O., Mitrea, S.-O., Sessa, D., et al. (2019). P: 33in vivo longitudinal 1H MRS study of hippocampal, cereberal and striatal metabolic changes in the adult brain using an animal model of chronic hepatic encephalopathy. Offic. J. Am. Coll. Gastroenterol. 114:S17. doi: 10.14309/01.ajg.0000582108.29364.13
Solfrizzi, V., Scafato, E., Custodero, C., Loparco, F., Ciavarella, A., Panza, F., et al. (2020). Liver fibrosis score, physical frailty, and the risk of dementia in older adults: the Italian longitudinal study on aging. Alzheimers Dement. 6:e12065. doi: 10.1002/trc2.12065
Sonnay, S., Gruetter, R., and Duarte, J. M. N. (2017). How energy metabolism supports cerebral function: insights from (13)C magnetic resonance studies in vivo. Front. Neurosci. 11:288. doi: 10.3389/fnins.2017.00288
Sookoian, S., and Pirola, C. J. (2015). Liver enzymes, metabolomics and genome-wide association studies: from systems biology to the personalized medicine. World J. Gastroenterol. 21, 711–725. doi: 10.3748/wjg.v21.i3.711
Sugimoto, R., Iwasa, M., Maeda, M., Urawa, N., Tanaka, H., Fujita, N., et al. (2008). Value of the apparent diffusion coefficient for quantification of low-grade hepatic encephalopathy. Am. J. Gastroenterol. 103, 1413–1420. doi: 10.1111/j.1572-0241.2008.01788.x
Sun, T., Du, H., Li, Z., Xiong, J., Liu, Y., Li, Y., et al. (2022). Decoding the contributions of gut microbiota and cerebral metabolism in acute liver injury mice with and without cognitive dysfunction. CNS Neurosci. Ther. doi: 10.1111/cns.14069
Sunil, H. V., Mittal, B. R., Kurmi, R., Chawla, Y. K., and Dhiman, R. K. (2012). Brain perfusion single photon emission computed tomography abnormalities in patients with minimal hepatic encephalopathy. J. Clin. Exp. Hepatol. 2, 116–121. doi: 10.1016/s0973-6883(12)60099-1
Takahashi, A., Kono, S., Wada, A., Oshima, S., Abe, K., Imaizumi, H., et al. (2017). Reduced brain activity in female patients with non-alcoholic fatty liver disease as measured by near-infrared spectroscopy. PLoS One 12:e0174169. doi: 10.1371/journal.pone.0174169
Taylor-Robinson, S. D., Oatridge, A., Hajnal, J. V., Burroughs, A. K., McIntyre, N., and deSouza, N. M. (1995). MR imaging of the basal ganglia in chronic liver disease: correlation of T1-weighted and magnetisation transfer contrast measurements with liver dysfunction and neuropsychiatric status. Metab. Brain Dis. 10, 175–188. doi: 10.1007/bf01991864
Teperman, L. W., and Peyregne, V. P. (2010). Considerations on the impact of hepatic encephalopathy treatments in the pretransplant setting. Transplantation 89, 771–778. doi: 10.1097/TP.0b013e3181d2fe66
Thames, A. D., Castellon, S. A., Singer, E. J., Nagarajan, R., Sarma, M. K., Smith, J., et al. (2015). Neuroimaging abnormalities, neurocognitive function, and fatigue in patients with hepatitis C. Neurol. Neuroimmunol. Neuroinflamm. 2:e59. doi: 10.1212/nxi.0000000000000059
Vaghi, G., Gori, B., Strigaro, G., Burlone, M., Minisini, R., Barbaglia, M. N., et al. (2020). Direct antivirals and cognitive impairment in hepatitis C: a clinical-neurophysiologic study. J. Neurovirol. 26, 870–879. doi: 10.1007/s13365-020-00904-6
Veniaminova, E., Oplatchikova, M., Bettendorff, L., Kotenkova, E., Lysko, A., Vasilevskaya, E., et al. (2020). Prefrontal cortex inflammation and liver pathologies accompany cognitive and motor deficits following Western diet consumption in non-obese female mice. Life Sci. 241:117163. doi: 10.1016/j.lfs.2019.117163
Wang, Y., Qiu, G., and Li, Y. (2022). The effects of hepatic ischemia/reperfusion injury on postoperative cognitive function in aged rats. Arch. Med. Sci. 18, 1357–1363. doi: 10.5114/aoms.2019.90335
Weinstein, G., Davis-Plourde, K., Himali, J. J., Zelber-Sagi, S., Beiser, A. S., and Seshadri, S. (2019). Non-alcoholic fatty liver disease, liver fibrosis score and cognitive function in middle-aged adults: the Framingham Study. Liver Int. 39, 1713–1721. doi: 10.1111/liv.14161
Weinstein, G., Zelber-Sagi, S., Preis, S. R., Beiser, A. S., DeCarli, C., Speliotes, E. K., et al. (2018). Association of nonalcoholic fatty liver disease with lower brain volume in healthy middle-aged adults in the framingham study. JAMA Neurol. 75, 97–104. doi: 10.1001/jamaneurol.2017.3229
Weiss, N., and Thabut, D. (2019). Neurological complications occurring after liver transplantation: role of risk factors, hepatic encephalopathy, and acute (on chronic) brain injury. Liver Transpl. 25, 469–487. doi: 10.1002/lt.25420
Winterdahl, M., Abbas, Z., Noer, O., Thomsen, K. L., Gras, V., Nahimi, A., et al. (2019). Cerebral water content mapping in cirrhosis patients with and without manifest HE. Metab. Brain Dis. 34, 1071–1076. doi: 10.1007/s11011-019-00427-y
Woodburn, S. C., Bollinger, J. L., and Wohleb, E. S. (2021). The semantics of microglia activation: neuroinflammation, homeostasis, and stress. J. Neuroinflammation 18:258. doi: 10.1186/s12974-021-02309-6
Wu, W., Wu, Y., Cheng, G., Zhang, C., Wang, H., and Li, Y. (2019). A mouse model of hepatic ischemia-reperfusion injury demonstrates potentially reversible effects on hippocampal neurons and postoperative cognitive function. Med. Sci. Monit. 25, 1526–1536. doi: 10.12659/msm.912658
Xu, X. Y., Ding, H. G., Li, W. G., Jia, J. D., Wei, L., Duan, Z. P., et al. (2019). Chinese guidelines on management of hepatic encephalopathy in cirrhosis. World J. Gastroenterol. 25, 5403–5422. doi: 10.3748/wjg.v25.i36.5403
Xu, J. L., Gu, J. P., Wang, L. Y., Zhu, Q. R., You, N. N., Li, J., et al. (2023). Aberrant spontaneous brain activity and its association with cognitive function in non-obese nonalcoholic fatty liver disease: a resting-state fMRI study. J. Integr. Neurosci. 22:8. doi: 10.31083/j.jin2201008
Yan, L., Wei, J. A., Yang, F., Wang, M., Wang, S., Cheng, T., et al. (2022). Physical exercise prevented stress-induced anxiety via improving brain RNA methylation. Adv. Sci. 9:e2105731. doi: 10.1002/advs.202105731
Yang, B., Sun, T., Chen, Y., Xiang, H., Xiong, J., and Bao, S. (2022). The role of gut microbiota in mice with bile duct ligation-evoked Cholestatic liver disease-related cognitive dysfunction. Front. Microbiol. 13:909461. doi: 10.3389/fmicb.2022.909461
Yanny, B., Winters, A., Boutros, S., and Saab, S. (2019). Hepatic encephalopathy challenges, burden, and diagnostic and therapeutic approach. Clin. Liver Dis. 23, 607–623. doi: 10.1016/j.cld.2019.07.001
Ye, M., Guo, Z., Li, Z., Lin, X., Li, J., Jiang, G., et al. (2020). Aberrant inter-hemispheric coordination characterizes the progression of minimal hepatic encephalopathy in patients with HBV-related cirrhosis. Neuroimage Clin. 25:102175. doi: 10.1016/j.nicl.2020.102175
Yokokawa, T., Sasaki, S., Sase, K., Yoshii, N., Yasuda, J., Hayashi, T., et al. (2022). Association of serum brain-derived neurotrophic factor with hepatic enzymes, AST/ALT ratio, and FIB-4 index in middle-aged and older women. PLoS One 17:e0273056. doi: 10.1371/journal.pone.0273056
Younossi, Z., Tacke, F., Arrese, M., Chander Sharma, B., Mostafa, I., Bugianesi, E., et al. (2019). Global perspectives on nonalcoholic fatty liver disease and nonalcoholic steatohepatitis. Hepatology 69, 2672–2682. doi: 10.1002/hep.30251
Zeegen, R., Drinkwater, J. E., and Dawson, A. M. (1970). Method for measuring cerebral dysfunction in patients with liver disease. Br. Med. J. 2, 633–636. doi: 10.1136/bmj.2.5710.633
Zhan, C., Chen, H. J., Gao, Y. Q., and Zou, T. X. (2019). Functional network-based statistics reveal abnormal resting-state functional connectivity in minimal hepatic encephalopathy. Front. Neurol. 10:33. doi: 10.3389/fneur.2019.00033
Zhang, X. H., Shi, J. Y., Zhan, C., Zhang, L., and Chen, H. J. (2020). Intrinsic brain abnormalities in patients with hepatitis C virus infection with cognitive impairment: a preliminary resting-state fMRI study. Biomed. Res. Int. 2020:1693043. doi: 10.1155/2020/1693043
Zöllner, H. J., Thiel, T. A., Füllenbach, N. D., Jördens, M. S., Ahn, S., Wilms, L. M., et al. (2023). J-difference GABA-edited MRS reveals altered cerebello-thalamo-cortical metabolism in patients with hepatic encephalopathy. Metab. Brain Dis. 38, 1221–1238. doi: 10.1007/s11011-023-01174-x
Keywords: cognitive impairment, liver disease, humoral factor, MRI research, brain
Citation: Sun T, Feng M, Manyande A, Xiang H, Xiong J and He Z (2023) Regulation of mild cognitive impairment associated with liver disease by humoral factors derived from the gastrointestinal tract and MRI research progress: a literature review. Front. Neurosci. 17:1206417. doi: 10.3389/fnins.2023.1206417
Edited by:
David Mokler, University of New England, United StatesReviewed by:
Alena Sidenkova, Ural State Medical University, RussiaCopyright © 2023 Sun, Feng, Manyande, Xiang, Xiong and He. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongbing Xiang, eGhidGoyMDA0QDE2My5jb20=; Jun Xiong, b2xkeGlvbmdAcXEuY29t; Zhigang He, MTA5NzY4NTgwN0BxcS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.