
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurosci. , 18 May 2023
Sec. Neuroprosthetics
Volume 17 - 2023 | https://doi.org/10.3389/fnins.2023.1167244
This article is part of the Research Topic Insights in Neuroprosthetics: 2023 View all 4 articles
 José Damián Carrillo-Ruiz1,2,3*
José Damián Carrillo-Ruiz1,2,3* José Rodrigo Carrillo-Márquez4,5
José Rodrigo Carrillo-Márquez4,5 Jesús Quetzalcóatl Beltrán1
Jesús Quetzalcóatl Beltrán1 Fiacro Jiménez-Ponce1
Fiacro Jiménez-Ponce1 Luis García-Muñoz1
Luis García-Muñoz1 José Luis Navarro-Olvera1
José Luis Navarro-Olvera1 René Márquez-Franco1
René Márquez-Franco1 Francisco Velasco1
Francisco Velasco1Limbic surgery is one of the most attractive and retaken fields of functional neurosurgery in the last two decades. Psychiatric surgery emerged from the incipient work of Moniz and Lima lesioning the prefrontal cortex in agitated patients. Since the onset of stereotactic and functional neurosurgery with Spiegel and Wycis, the treatment of mental diseases gave attention to refractory illnesses mainly with the use of thalamotomies. Neurosis and some psychotic symptoms were treated by them. Several indications when lesioning the brain were included: obsessive-compulsive disorder, depression, and aggressiveness among others with a diversity of targets. The indiscriminately use of anatomical sites without enough scientific evidence, and uncertainly defined criteria for selecting patients merged with a deficiency in ethical aspects, brought a lack of procedures for a long time: only select clinics allowed this surgery around the world from 1950 to the 1990s. In 1999, Nuttin et al. began a new chapter in limbic surgery with the use of Deep Brain Stimulation, based on the experience of pain, Parkinson’s disease, and epilepsy. The efforts were focused on different targets to treat depression and obsessive-compulsive disorders. Nevertheless, other diseases were added to use neuromodulation. The goal of this article is to show the new opportunities to treat neuropsychiatric diseases.
Psychiatric illnesses were treated at the beginning of the 20th century with brain surgery (Freeman and Watts, 1948). No drugs or psychotherapy existed at that time. It was until the 1940s–1950s that brain surgery and psychiatric drugs were utilized. Limbic surgery declined in the 1970s and only few clinics in the world performed these procedures. The arrival of deep brain stimulation (DBS) for neurological and psychiatric diseases brought amelioration of symptoms of obsessive-compulsive disorder (OCD) and depression (Nuttin et al., 1999). This has motivated the scientific community to retake limbic surgery as a discussion topic.
Theoretically, DBS could treat every mental disease, but is important to know the exact mechanism involved in each illness. Moreover, at this moment this proposal is not totally achievable, because of the lack of precision regarding neuroanatomy and neurophysiology of brain circuitries (i.e., connectome and synaptome) and neurotransmitters involved in each mental and neurological disease. After discovering the pathophysiology of every disease, it could be easier to treat specific illnesses and/or modify the nervous system to be more effective.
The criteria to perform psychosurgery includes: (1) The presence of brain nuclei lesions or stimulation in different animal models of mental illness (Oterdoom et al., 2020). (2) The surgical experiences of limbic surgery in patients with psychiatric diseases (Langevin, 2012; García-Muñoz et al., 2019). (3) DBS use in neurological illness to treat mental symptoms and modify them with neuromodulation; based on the experience learned from STN, Thalamus, or GPi in patients with Parkinson’s disease, pain, and epilepsy (Hosobuchi et al., 1973; Benabid et al., 1991; Lee et al., 2019). (4) DBS treatment in OCD and depression symptoms alleviation (Nuttin et al., 1999; Marquez-Franco et al., 2022).
The next lines demonstrated the new indications for DBS treatment in psychiatric pathologies: anxiety, eating disorders (EDs), substance use disorders, aggressiveness, schizophrenia, and Alzheimer’s disease (see Table 1).
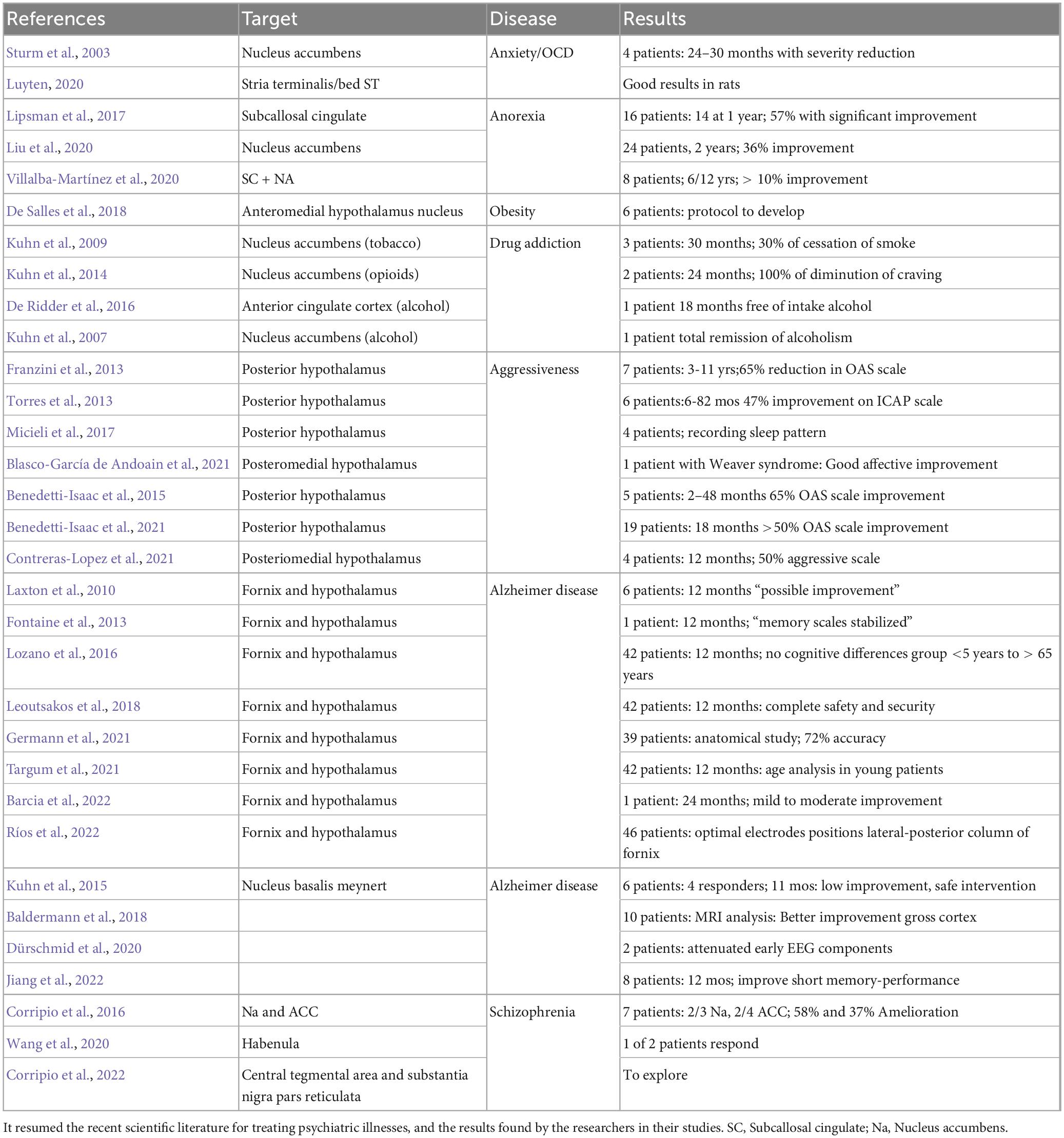
Table 1. New indications of deep brain stimulation in psychosurgery.
We followed the National Library of Medicine standard search protocol, using PubMed and Google Scholar metasearch engines which are free and public. The search was conducted using Boolean Operators with the following Medical Subject Headings (MeSH): “psychosurgery,” “limbic surgery,” “deep brain stimulation,” “brain stimulation,” “stereotactic lesion,” “neuromodulation,” “depression,” “aggressiveness,” “drug usage,” “addiction,” “anxiety,” “eating disorders,” “electrodes,” “Alzheimer’s disease,” “Schizophrenia,” “transhumanism,” and “neuroethics.”
The inclusion criteria for the selected papers were: (1) new studies focused on limbic surgery in humans, and/or (2) animal studies that propose new targets for treating psychiatric illnesses, and (3) neuroethics regarding the implementation of new technologies for treating psychiatric pathologies. The exclusion criteria were: (1) articles written in another language than English, Spanish, or French and (2) articles that were not found as full-text articles. The results were synthesized and presented as a mini-review describing the new tendencies.
Galvani’s work on animal electricity was a milestone in understanding the nature of the nerve impulse and led to the founding of electrophysiology (Piccolino, 1998; Bennett, 1999). This is focused on the clinical application for the management of various neurological diseases, and promoting laboratory research to expand the knowledge of biophysical neuronal functioning (Bennett, 1999; Feindel, 2007).
In the clinical field, this led to understanding the electrical stimulation of the nervous system. It helped to create more accurate diagnoses and treatments for neurological patients. Penfield, in the first half of the 20th century, mapped the topographic organization of motor and sensory homunculi in patients with epilepsy (Penfield and Boldrey, 1937). Later on, based on this experience Hassler et al. (1960), Benabid et al. (1991), Hosobuchi et al. (1973), Mundinger (1977), and other researchers developed DBS with chronically implanted devices for the management of various pathologies including Parkinson’s disease, essential tremor, pain, epilepsy, and neuropsychiatric disorders (Hosobuchi et al., 1973; Benabid et al., 1991; Lee et al., 2019; Marquez-Franco et al., 2022). More recently, responsive neurostimulation (RNS) has been used as a system that monitors brain waves and applies different voltages according to brain activity in a specific brain area (Albright et al., 2000).
Basic neuroscience research has helped to understand the cellular and molecular mechanisms of neural communication (Piccolino, 1998; Bennett, 1999). Emile du Bois-Reymond in the second half of the 20th century demonstrated the correlation between nervous tissue and bioelectricity. Researchers such as Dale, Loewi, Eccles, Katz, Miledi, Neher, Sakmann, and Kandel, unveiled the basic mechanisms involved in the transmission of information, processing, and neuronal communication (Albright et al., 2000). Hodgkin and Huxley described the biophysics of the electrical activity in neurons (Piccolino, 1998; Albright et al., 2000).
The convergence of basic and clinical neurophysiology in the last decades has created outstanding achievements. Undoubtedly, previous advances, like the development of dynamic and adaptable brain implants, are the prelude to developing correct DBS techniques and brain–machine interfaces (BMI) as a possibility for understanding the brain and treating illnesses (Hochberg et al., 2012; Raspopovic, 2021).
Currently, EDs are a major health problem worldwide, and the reality is that humans must obtain energy and biochemical precursors from food (Hauck et al., 2020). In this way, in the feeding and nourishing mechanisms pleasure should be felt to assure survival. The activation of the reward system of dopamine circuitry (Thalamus Ventrolateral Tegmental nucleus) is involved in this process. The discovery of the activation of endocannabinoids and opioid peptides are some of the new contributions to functional neuroscience (Al Massadi et al., 2019). It has been proven in animal models that treating EDS with DBS can bring changes (Oterdoom et al., 2020). Therefore, surgeons should be very selective in the techniques implemented to assure a good outcome because it is translated to a better quality of life for patients. The last reports determined DBS is still an emerging treatment, yet human trials suggest two treatment possibilities: anorexia nervosa and obesity.
In the case of anorexia nervosa, DBS has been acknowledged as well as inserting electrodes in some key areas (Lipsman et al., 2013; Wu et al., 2013), including these anatomical targets: Rostromedial tegmental nucleus (Melse et al., 2016), Subcallosal cingulate (Sc) (Lipsman et al., 2017), Na (Nucleus accumbens) (Liu et al., 2020), and a combination of Sc + Na (Villalba-Martínez et al., 2020). Although promising results were published, further research should be made (Sobstyl et al., 2019; Treasure et al., 2020).
Regarding obesity, scientific evidence has determined some anatomical sites of the brain that could be modulated (Halpern et al., 2011; Torres et al., 2011; McClelland et al., 2013; Ho et al., 2015). After theoretical analysis, surgery was performed in humans by a few groups over the world. The possibility of treating EDs with anteromedial hypothalamus nucleus stimulation to promote the satiety effect is an option (De Salles et al., 2018). Another possible treatment was demonstrated by stimulating Na in a patient with obesity and depression using DBS to generate weight loss (Tronnier et al., 2018).
Is DBS an answer? Acknowledging and investigating dopaminergic reinforcement pathways must be discussed by neurosurgeons, neurologists, psychiatrists, and researchers to correctly treating these illnesses (Volkow et al., 2019). DBS has been utilized to treat substance addictions according to scientific literature (Chang et al., 2022).
In most animal models focused on drug usage, results tend to prove that the implementation of this technology helps to reduce addictions (Guercio et al., 2020). Although clinical trials provide encouraging results, the complex approach of creating human models has diminished in the last years (Wang et al., 2018). Moreover, Polyakov and Kholyavin (2022) reported crio-cyngulotomies as a possible safe treatment for psychological dependence in drug addiction.
Fattahi et al. (2022) described that opioid dependence can be treated by stimulating Na with high-frequency stimulation. Also, Kuhn et al. (2009, 2014) proposed treating opioid dependence with DBS in Na as well. DBS might be an answer to treat patients that require surgical intervention due to the failure of previous therapies and/or other treatments. Shallow to moderate addiction can be treated with psychiatric drugs, and intensive substance abuse opens the possibility to use neuromodulation and DBS.
Nowadays, tobacco addiction could be ameliorated after the stimulation of Na (Kuhn et al., 2009), and alcohol abuse disorder decreased with anterior cingulate cortex implantation (De Ridder et al., 2016), or with the use of Na stimulation (Kuhn et al., 2007). On the other hand, DBS in non-substance addictions has been poorly described, excluding EDs. This is a promising work based on results established by the scientific community (Volkow et al., 2019; Oterdoom et al., 2020).
Although research on substance use disorders is beginning, it is possible to get targets to treat addictions. Research in dependency problems is complicated because drug abuse can cause exclusion from studies (i.e., secondary pathologies and death) in subjects. The comorbidities can bring many mental disorders (e.g., OCD, depression, dementia), so it is important to create models of drug dependence in these subjects as well.
Limbic surgery began to treat psychiatric patient’s suffering. The procedure consisted in lesioning the frontal lobe as proposed by Freeman and Watts (1948). It was possible to diminish all the symptoms of anxiety, but with unwished secondary effects (Lichterman et al., 2022). At that time, it existed neither consensus of psychiatrists nor the Diagnostic and Statistical Manual of Mental Disorders (DSM). After several decades, anxiety patients were treated with psychiatric drugs and/or therapy. Brain surgical procedures were practically abandoned and reduced to lesions of the following structures: anterior cingulate circumvolution (ACC), subcaudate nuclei, and anterior capsule (Leiphart and Valone, 2010; Patel et al., 2013). Nevertheless, Nuttin et al. (1999) referred to the possibility of neuromodulating the internal capsule to treat OCD. Some of these patients had anxiety alleviation.
Diverse authors reported benefits in treating OCD, and nervousness with DBS (Sturm et al., 2003; Patel et al., 2013; Velasques et al., 2014; Freire et al., 2020; Ganz, 2022). For anxiety, some targets have been reported lately, including Na (Sturm et al., 2003), Papez ring (Hescham et al., 2015), and the Bed Nucleus of Stria Terminalis (BNST) (Luyck and Luyten, 2015; Luyten, 2020). The results indicated an amelioration of OCD symptoms, but also a decrease in fretfulness and fear. Li et al. (2022) described that hypothalamic DBS can be used in brief periods to treat anxiety and arrest relapse in a mice model. Further basic and clinical research should be done to prove efficacy (Li et al., 2022).
One of the most important indications to perform limbic surgery is the presence of aggressiveness in individuals with psychiatric illnesses. Symptoms by themselves are not a disorder. Brain lesioning surgery has been performed in patients with good results in diverse clinical studies (García-Muñoz et al., 2019; Marquez-Franco et al., 2022). The most frequent target used in surgery is the hypothalamus (Rizzi et al., 2017; Marquez-Franco et al., 2022), then the cingulum and amygdala (Langevin, 2012). These specific lesions brought good results, so the next step was to perform DBS.
Italians Franzini et al. (2013) and Rizzi et al. (2017) proposed the posterior hypothalamus to treat neuropathic pain, and it was transferred to patients with violent behavior with good outcomes. They were followed by the Spaniards with hypothalamic DBS (Torres et al., 2013, 2020; Blasco-García de Andoain et al., 2021), and by Colombian and Brazilian neurosurgeon groups with the same methods in clinical trials (Benedetti-Isaac et al., 2015, 2021; Micieli et al., 2017; Contreras-Lopez et al., 2021).
A very recent point is neuromodulation to treat amnesia and forgetting in patients with dementia and Alzheimer’s disease. The idea to stimulate sites where memory and learning is located is not new because murine models were made. After, Laxton et al. (2010) introduced electrodes in the limbic system, fornix and hypothalamus in individuals with moderate Alzheimer’s disease. Three aspects were evaluated: brain mapping with conventional tomography, metabolic changes in regional neurons evaluated with PET, so as cognitive function. Results showed entorhinal and hippocampal zones had modifications after stimulation. The amnesia was ameliorated, using a neuropsychological battery, posterior to modulation of these targets for 12 months (Laxton et al., 2010). Based on the findings, other researchers have followed this method, obtaining similar results to the ones first published (Fontaine et al., 2013; Sankar et al., 2015; Ponce et al., 2016; Leoutsakos et al., 2018; Germann et al., 2021; Targum et al., 2021; Barcia et al., 2022; Ríos et al., 2022).
Two more sites of stimulation to treat amnesia have been proposed: Nucleus Basalis Meynert (NBM) and Ventral Capsule/Ventral Striatum. Laxton and Lozano (2013) proposed the first target explaining that: “the study of dementia is preliminary and limited.” They showed evidence of the use of DBS in NBM for Alzheimer’s disease and dementia in Parkinson’s disease with initially hopeless results (Laxton and Lozano, 2013). Later on, Kuhn et al. (2015) implanted six patients with good responses and four of them with no side effects. In the last years, other studies reported positive results as well (Baldermann et al., 2018; Dürschmid et al., 2020; Jiang et al., 2022).
On the other side, the Ventral Capsule/Ventral Striatum stimulation produced modifications of the frontotemporal circuits involved in learning and memory formation. At this moment there is a lack of experience in this area (Scharre et al., 2018).
Schizophrenia is an illness with controversial use of surgery, based on the molecular, genetic, and cellular changes with animal models (Heath, 1975; Ma and Leung, 2014; Schwabe and Krauss, 2018). The most important question is what part of the brain should be modified. It is necessary to known which circuits are involved in negative and positive symptoms.
The first attempt to use DBS in schizophrenia was performed by Heath, on patients with other comorbidities including sexual disturbances. Back then, they were different scientific and ethical views compared with today’s standards, so Dr. Heath was severely criticized (Heath, 1975).
Corripio et al. (2020) published the first paper with a stronger methodology to evaluate patients with schizophrenia. The article was focused on the Na or subgenual ACC bilateral neuromodulation (Corripio et al., 2020). They performed a randomized, double-blind crossover phase lasting 24 weeks, showing 25% of symptoms amelioration. Wang et al. (2020) performed DBS in the habenula in two patients, founding only a response in one of them, after 12 months of follow-up. Later, Corripio et al. (2022) described the possibility of two targets: the ventral tegmental area and the substantia nigra pars reticulata, but the experience at the moment is poor to get conclusions (see Figure 1).
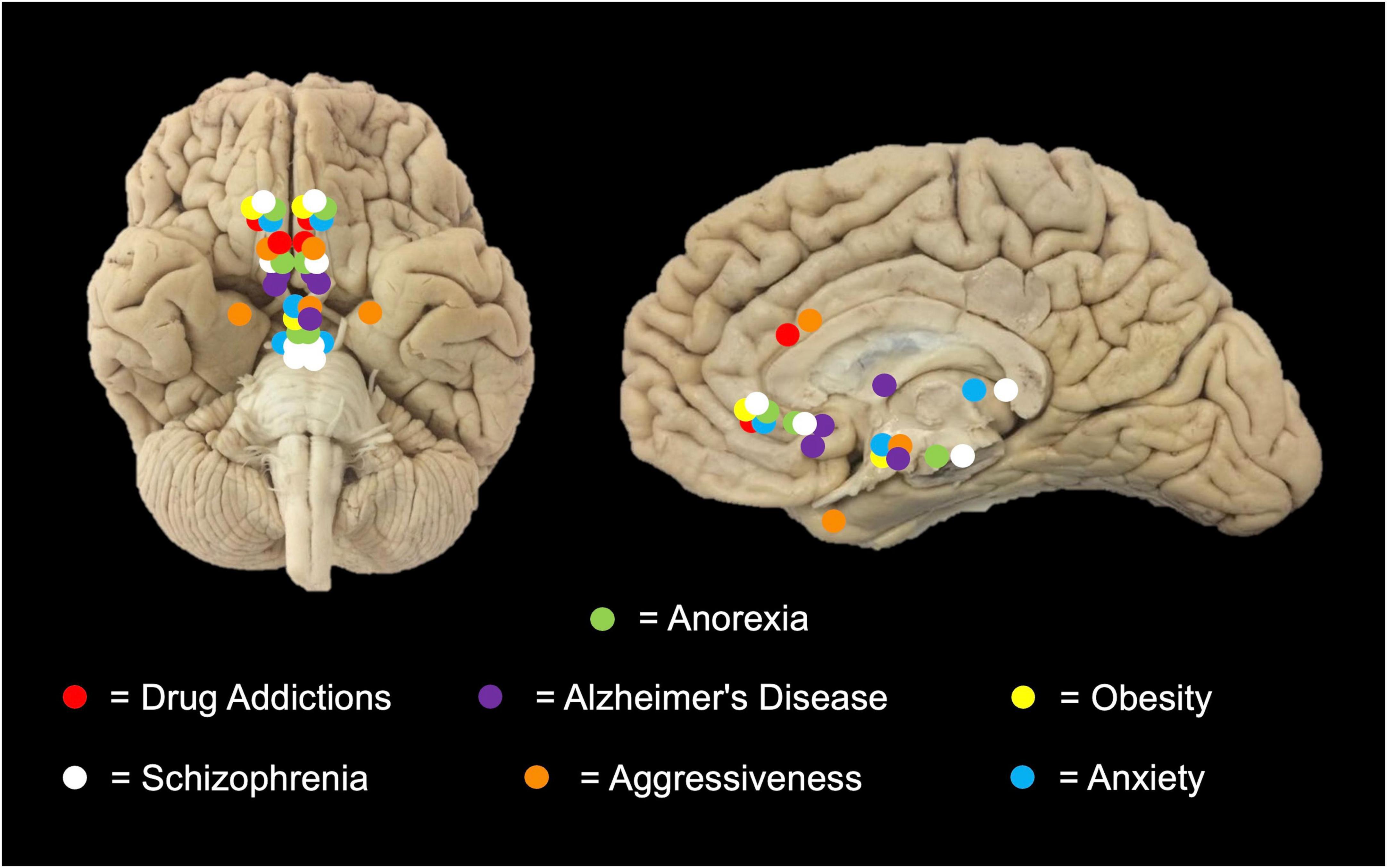
Figure 1. Targets of new indications for DBS. In this representative scheme, different anatomical DBS sites are shown according to pathologies: Addictions (Cingulum, Nucleus accumbens [Na]); Anorexia (Rostromedial Tegmental Nucleus, Subcallosal cingulate [Sc]); Anxiety (Na, Bed Nucleus of Stria Terminalis, Hypothalamus); Aggressiveness (Posterior hypothalamus, cingulum and amygdala); Alzheimer’s disease (Fornix/hypothalamus, Nucleus Basalis of Meynert; Ventral capsule/ventral Striatum); Schizophrenia (Na, anterior Corpus callosum, Habenula); and Obesity (Anteromedial Hypothalamus, Na) for performing DBS therapy.
Another important aspect of this review is that DBS can be used to enhance human capacities and not just overcome psychiatric disorders, using electrophysiological theory and neuroprosthetics. It will be explained on the neurological, technical, philosophical, and ethical levels the implications of computer sciences with neurosciences.
BMIs, also known as brain-computer interfaces or neuroprosthetics, are devices that record signals from the nervous system and control external devices or hybrid systems to help restore communication or movement (Benabid et al., 1991; Albright et al., 2000; Hochberg et al., 2012). Neuroprosthetics have three parts: (1) a sensor that detects the electrical activity of the brain, (2) a signal processor that decodes the movement in the neural activity through algorithms, and (3) an effector that carries out the desired action using digital systems (i.e., cursor, computer), electromechanical prostheses and/or direct neuromuscular reactivation (Benabid et al., 1991; Raspopovic, 2021).
Nowadays, the use of BMI is emerging, and it is expected that it will eventually have a specific clinical application (Kansaku, 2021). For this purpose, closed-loop systems, fast and efficient algorithms, the development of better models of movement, sensory-motor feedback, miniaturized hardware, and wireless broadband systems are required (Ajiboye et al., 2017; Savage, 2018; Schwemmer et al., 2018; Simeral et al., 2021; Yadav et al., 2021). Findings such as the increment in spatial memory in epileptic patients with entorhinal electrical stimulation (Topalovic et al., 2020) have questioned the potential use of DBS and BMI in people with age-related cognitive deficits, and people without neurological pathologies (Suthana et al., 2012; Zimerman et al., 2013).
Neuroenhancement that uses chemicals, artifacts, or techniques on the brain to increase neurological capabilities—especially cognitive functions—is a new and complex issue with various positions (Hochberg et al., 2012; Suthana et al., 2012; Zimerman et al., 2013). Humans can receive diverse focal modifications in their bodies, which could be accumulative. In the long term, this could theoretically modify beings from current humans into transhumans. Even more, it is possible to use technology not only to extend human cognitive capabilities to a superhuman level, but also to transcend the biological limits of the mind and consciousness. The idea is to merge neural biological networks with artificial neural networks in order to end psychiatric diseases.
All of the aforementioned have profound ethical and philosophical issues that concern human survival as individuals and humanity (Koch, 2010; Zimerman et al., 2013; Clark and Parasuraman, 2014). A possible artificial selection of transhumans (with neuroprosthetics and/or genetic engineering), could lead to a hyperspecialized human race directed by them. Mental illnesses and limbic malfunctioning could be abolished completely. Psychiatric diseases will be a topic from the past, but mind afflictions such as biohacking might be a concern in these “new neural networks composed of cells and inorganic technology” (Yetisen, 2018).
On the other hand, the biological transcendence of consciousness upgraded to digital systems implies virtually non-mortal entities, a situation that could break the status quo and stagnation of human civilizations (Hochberg et al., 2012; Raspopovic, 2021). Undoubtedly the horizons of neuroenhancement are far and surely deep, speculation about issues allows us to imagine some possible contexts, but it is in our hands to define the results. It is important to discuss these topics from now on from different perspectives, including psychiatric diseases and their obliteration: it is important to understand what the concept attributed to the person means, and what is the exact role of neuroprosthetics in the essence of the human being (Carrillo-Ruiz et al., 2020, 2022).
Limbic surgery has new indications to treat anxiety, eating disorders, addictions, aggressiveness, schizophrenia, and Alzheimer’s disease. It is important to take into consideration the anatomical sites of DBS use, as well ethical and scientific committees should be present when approaching each patient. Transhumanism is a contemporary option for DBS use in treating or enhancing some cognitive abilities, and a possible technology to abolish psychiatric diseases in the future.
JC-R originated the idea and abstract. JC-M made the figure. JB created the table. FJ-P and LG-M contributed with psychosurgery indications in the manuscript. JN-O checked anatomical functional details as well as correcting style. RM-F added information regarding neuroprosthetics, neuroenhancement, and transhumanism. FV reviewed the text and contributed with expertise in the field. All authors participated in the creation of this manuscript by writing evenly.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ajiboye, A., Willett, F., Young, D., Memberg, W., Murphy, B., Miller, J., et al. (2017). Restoration of reaching and grasping movements through brain-controlled muscle stimulation in a person with tetraplegia: A proof-of-concept demonstration. Lancet 389, 1821–1830. doi: 10.1016/S0140-6736(17)30601-3
Al Massadi, O., Nogueiras, R., Dieguez, C., and Girault, J. (2019). Ghrelin and food reward. Neuropharmacology 148, 131–138. doi: 10.1016/j.neuropharm.2019.01.001
Albright, T., Jessell, T., Kandel, E., and Posner, M. (2000). Neural science: A century of progress and the mysteries that remain. Neuron 25, S1–S55.
Baldermann, J. C., Hardenacke, K., Hu, X., Köster, P., Horn, A., Freund, H., et al. (2018). Neuroanatomical characteristics associated with response to deep brain stimulation of the nucleus basalis of meynert for Alzheimer’s disease. Neuromodulation 21, 184–190. doi: 10.1111/ner.12626
Barcia, J. A., Viloria, M. A., Yubero, R., Sanchez-Sanchez-Rojas, L., López, A., Strange, B. A., et al. (2022). Directional DBS of the fornix in Alzheimer’s disease achieves long-term benefits: A case report. Front. Aging Neurosci. 14:809972. doi: 10.3389/fnagi.2022.809972
Benabid, A., Pollak, P., Hoffmann, D., Gervason, C., Hommel, M., Perret, J., et al. (1991). Long-term suppression of tremor by chronic stimulation of the ventral intermediate thalamic nucleus. Lancet 337, 403–406.
Benedetti-Isaac, J., Camargo, L., Gargiulo, P., and López, N. (2021). Deep brain stimulation in the posteromedial hypothalamic nuclei in refractory aggressiveness: Post-surgical results of 19 cases. Int. J. Neuropsych. 24, 977–978. doi: 10.1093/ijnp/pyab059
Benedetti-Isaac, J., Torres-Zambrano, M., Vargas-Toscano, A., Perea-Castro, E., Alcalá-Cerra, G., Furlanetti, L., et al. (2015). Seizure frequency reduction after posteromedial hypothalamus deep brain stimulation in drug-resistant epilepsy associated with intractable aggressive behavior. Epilepsia 56, 1152–1161. doi: 10.1111/epi.13025
Bennett, M. R. (1999). The early history of the synapse: From Plato to Sherrington. Brain Res. Bull. 50, 95–118. doi: 10.1016/s0361-9230(99)00094-5
Blasco-García de Andoain, G., Navas-García, M., González-Aduna, Ó, Bocos-Portillo, A., Ezquiaga-Terrazas, E., Ayuso-Mateos, J., et al. (2021). Posteromedial hypothalamic deep brain stimulation for refractory aggressiveness in a patient with weaver syndrome: Clinical, technical report and operative video. Oper. Neurosurg. 21, 165–171. doi: 10.1093/ons/opab149
Carrillo-Ruiz, J., Carrillo-Márquez, J., Jiménez-Ponce, F., García-Muñoz, L., Navarro-Olvera, J., and Beltrán, J. (2020). Neurobioética personalista: Su consideración en la psicocirugía. Neurocir. Neurosur. Demo Flanc. 29, 117–135.
Carrillo-Ruiz, J., Carrillo-Márquez, J., and Kalkach-Aparicio, M. (2022). “Utilización de implantes cerebrales en la persona en el Transhumanismo,” in Riesgos y desafíos del transhumanismo. Perspectivas antropológicas y bioéticas, eds J. Alexánder, G. Echeverri, and V. H. Yepes (Argentina: Universidad Católica Argentina).
Chang, R., Peng, J., Chen, Y., Liao, H., Zhao, S., Zou, J., et al. (2022). Deep brain stimulation in drug addiction treatment: Research progress and perspective. Front. Psychiatr. 13:858638. doi: 10.3389/fpsyt.2022.858638
Clark, V., and Parasuraman, R. (2014). Neuroenhancement: Enhancing brain and mind in health and in disease. Neuroimage 15, 889–894. doi: 10.1016/j.neuroimage.2013.08.071
Contreras-Lopez, W., Navarro, P., Gouveia, F., Fonoff, E., Lebrun, I., Auada, A., et al. (2021). Directional deep brain stimulation of the posteromedial hypothalamus for refractory intermittent explosive disorder: A case series using a novel neurostimulation device and intraoperative microdialysis. World Neurosurg. 155, e19–e33. doi: 10.1016/j.wneu.2021.07.086
Corripio, I., Roldán, A., McKenna, P., Sarr, S., Alonso-Solís, A., Salgado, L., et al. (2022). Target selection for deep brain stimulation in treatment resistant schizophrenia. Prog. Neuropsychopharmacol. Biol. Psychiatry 112:110436. doi: 10.1016/j.pnpbp.2021.11043
Corripio, I., Roldán, A., Sarr, S., McKenna, P. J., Alonso-Solís, A., Rabella, M., et al. (2020). Deep brain stimulation in treatment resistant schizophrenia: A pilot randomized cross-over clinical trial. Ebiomedicine 51:102568. doi: 10.1016/j.ebiom.2019.11.029
Corripio, I., Sarró, S., McKenna, P. J., Molet, J., Álvarez, E., Pomarol-Clotet, E., et al. (2016). Clinical improvement in a treatment-resistant patient with schizophrenia treated with deep brain stimulation. Biol. Psychiatry 80, e69–e70. doi: 10.1016/j.biopsych.2016.03.1049
De Ridder, D., Manning, P., Glue, P., Cape, G., Langguth, B., and Vanneste, S. (2016). Anterior cingulate implant for alcohol dependence: Case report. Neurosurgery 78, E883–E893. doi: 10.1227/NEU.0000000000001248
De Salles, A., Barbosa, D., Fernandes, F., Abucham, J., Nazato, D., Oliveira, J. D., et al. (2018). An open-label clinical trial of hypothalamic deep brain stimulation for human morbid obesity: Bless study protocol. Neurosurgery 83, 800–809. doi: 10.1093/neuros/nyy024
Dürschmid, S., Reichert, C., Kuhn, J., Freund, H., Hinrichs, H., and Heinze, H. (2020). Deep brain stimulation of the nucleus basalis of Meynert attenuates early EEG components associated with defective sensory gating in patients with Alzheimer disease - a two-case study. Eur. J. Neurosci. 51, 1201–1209. doi: 10.1111/ejn.13749
Fattahi, M., Eskandari, K., Sayehmiri, F., Kuhn, J., and Haghparast, A. (2022). Deep brain stimulation for opioid use disorder: A systematic review of preclinical and clinical evidence. Brain Res. Bull. 187, 39–48. doi: 10.1016/j.brainresbull.2022.06.015
Feindel, W. (2007). The physiologist and the neurosurgeon: The enduring influence of Charles Sherrington on the career of Wilder Penfield. Brain 130, 2758–2765. doi: 10.1093/brain/awm098
Fontaine, D., Deudon, A., Lemaire, J. J., Razzouk, M., Viau, P., Darcourt, J., et al. (2013). Symptomatic treatment of memory decline in Alzheimer’s disease by deep brain stimulation: A feasibility study. J. Alzheimers Dis. 34, 315–323. doi: 10.3233/JAD-121579
Franzini, A., Broggi, G., Cordella, R., Dones, I., and Messina, G. (2013). Deep-brain stimulation for aggressive and disruptive behavior. World Neurosurg. 80, S29.e11–4. doi: 10.1016/j.wneu.2012.06.038
Freire, R., Cabrera-Abreu, C., and Milev, R. (2020). Neurostimulation in anxiety disorders, post-traumatic stress disorder, and obsessive-compulsive disorder. Adv. Exp. Med. Biol. 1191, 331–346. doi: 10.1007/978-981-32-9705-0_18
Ganz, J. (2022). Behavioral disorders. Prog. Brain Res. 268, 385–392. doi: 10.1016/bs.pbr.2021.10.043
García-Muñoz, L., Picazo-Picazo, O., Carrillo-Ruíz, J., Favila-Bojórquez, J., Corona-García, F., Meza-Bautista, M., et al. (2019). Effect of unilateral amygdalotomy and hypothalamotomy in patients with refractory aggressiveness. Gac. Med. Mex. 155, S49–S55. doi: 10.24875/GMM.M19000290
Germann, J., Elias, G. J., Boutet, A., Narang, K., Neudorfer, C., Horn, A., et al. (2021). Brain structures and networks responsible for stimulation-induced memory flashbacks during forniceal deep brain stimulation for Alzheimer’s disease. Alzheimers Dement. 17, 777–787. doi: 10.1002/alz.12238
Guercio, L., Wimmer, M., Schmidt, H., Swinford-Jackson, S., Pierce, R., and Vassoler, F. (2020). Deep brain stimulation of the infralimbic cortex attenuates cocaine priming-induced reinstatement of drug seeking. Brain Res. 1746:147011. doi: 10.1016/j.brainres.2020.147011
Halpern, C., Torres, N., Hurtig, H., Wolf, J., Stephen, J., Oh, M., et al. (2011). Expanding applications of deep brain stimulation: A potential therapeutic role in obesity and addiction management. Acta Neurochir. 153, 2293–2306. doi: 10.1007/s00701-011-1166-3
Hassler, R., Riechert, T., Mundinger, F., Umbach, W., and Ganglberger, J. (1960). Physiological observations in stereotaxic operations in extrapyramidal motor disturbances. Brain 83, 337–350. doi: 10.1093/brain/83.2.337
Hauck, C., Cook, B., and Ellrott, T. (2020). Food addiction, eating addiction and eating disorders. Proc. Nutr. Soc. 79, 103–112. doi: 10.1017/S0029665119001162
Heath, R. (1975). Brain function and behavior. I. Emotion and sensory phenomena in psychotic patients and in experimental animals. J. Nerv. Ment. Dis. 160, 159–175.
Hescham, S., Jahanshahi, A., Meriaux, C., Lim, L., Blokland, A., and Temel, Y. (2015). Behavioral effects of deep brain stimulation of different areas of the Papez circuit on memory- and anxiety-related functions. Behav. Brain Res. 292, 353–360. doi: 10.1016/j.bbr.2015.06.032
Ho, A., Sussman, E., Pendharkar, A., Azagury, D., Bohon, C., and Halpern, C. (2015). Deep brain stimulation for obesity: Rationale and approach to trial design. Neurosurg. Focus 38:E8. doi: 10.3171/2015.3
Hochberg, L., Bacher, D., Jarosiewicz, B., Masse, N., Simeral, J., Vogel, J., et al. (2012). Reach and grasp by people with tetraplegia using a neurally controlled robotic arm. Nature 485, 372–375.
Hosobuchi, Y., Adams, J., and Rutkin, B. (1973). Chronic thalamic stimulation for the control of facial anesthesia dolorosa. Arch. Neurol. 29, 158–161.
Jiang, Y., Yuan, T., Chen, Y., Guo, P., Lian, T., Liu, Y., et al. (2022). Deep brain stimulation of the nucleus basalis of Meynert modulates hippocampal-frontoparietal networks in patients with advanced Alzheimer’s disease. Transl. Neurodegener. 11:51. doi: 10.1186/s40035-022-00327-9
Kansaku, K. (2021). Neuroprosthetics in systems neuroscience and medicine. Sci. Rep. 11:5404. doi: 10.1038/s41598-021-85134-4
Koch, T. (2010). Enhancing who? Enhancing what? Ethics, bioethics, and transhumanism. J. Med. Phil. 35, 685–699.
Kuhn, J., Bauer, R., Pohl, S., Lenartz, D., Huff, W., and Kim, E. (2009). Observations on unaided smoking cessation after deep brain stimulation of the nucleus accumbens. Eur. Addict. Res. 15, 196–201. doi: 10.1159/000228930
Kuhn, J., Hardenacke, K., Lenartz, D., Gruendler, T., Ullsperger, M., Bartsch, C., et al. (2015). Deep brain stimulation of the nucleus basalis of Meynert in Alzheimer’s dementia. Mol. Psychiatry 20, 353–360. doi: 10.1038/mp.2014.32
Kuhn, J., Lenartz, D., Huff, W., Lee, S., Koulousakis, A., and Klosterkoetter, J. (2007). Remission of alcohol dependency following deep brain stimulation of the nucleus accumbens: Valuable therapeutic implications? J. Neurol. Neurosurg. Psychiatr. 78, 1152–1153. doi: 10.1136/jnnp.2006.113092
Kuhn, J., Möller, M., Treppmann, J., Bartsch, C., Lenartz, D., and Gruendler, T. (2014). Deep brain stimulation of the nucleus accumbens and its usefulness in severe opioid addiction. Mol. Psychiatr. 19, 145–146. doi: 10.1038/mp.2012.196
Langevin, J. (2012). The amygdala as a target for behavior surgery. Surg. Neurol. Int. 3, S40–S46. doi: 10.4103/2152-7806.9160
Laxton, A., and Lozano, A. (2013). Deep brain stimulation for the treatment of Alzheimer disease and dementias. World Neurosurg. 80, e1–e28. doi: 10.1016/j.wneu.2012.06.028
Laxton, A. W., Tang-Wai, D. F., McAndrews, M. P., Zumsteg, D., Wennberg, R., Keren, R., et al. (2010). A phase I trial of deep brain stimulation of memory circuits in Alzheimer’s disease. Ann. Neurol. 68, 521–534. doi: 10.1002/ana.22089
Lee, D., Lozano, C., Dallapiazza, R., and Lozano, A. (2019). Current and future directions of deep brain stimulation for neurological and psychiatric disorders. J. Neurosurg. 131, 333–342.
Leiphart, J., and Valone, F. III (2010). Stereotactic lesions for the treatment of psychiatric disorders. J. Neurosurg. 113, 1204–1211. doi: 10.3171/2010.5.JNS091277
Leoutsakos, J. S., Yan, H., Anderson, W. S., Asaad, W. F., Baltuch, G., Burke, A., et al. (2018). Deep Brain Stimulation Targeting the Fornix for Mild Alzheimer Dementia (the ADvance Trial): A Two Year Follow-up Including Results of Delayed Activation. J. Alzheimers Dis. 64, 597–606. doi: 10.3233/JAD-180121
Li, H., Donegan, D., Peleg-Raibstein, D., and Burdakov, D. (2022). Hypothalamic deep brain stimulation as a strategy to manage anxiety disorders. Proc. Natl. Acad. Sci. U. S. A. 119:e2113518119. doi: 10.1073/pnas.2113518119
Lichterman, B., Schulder, M., Liu, B., Yang, X., and Taira, T. (2022). A comparative history of psychosurgery. Prog. Brain Res. 270, 1–31. doi: 10.1016/bs.pbr.2021.12.003
Lipsman, N., Lam, E., Volpini, M., Sutandar, K., Twose, R., and Giacobbe, P. (2017). Deep brain stimulation of the subcallosal cingulate for treatment-refractory anorexia nervosa: 1 year follow-up of an open-label trial. Lancet Psychiatr. 4, 285–294. doi: 10.1016/S2215-0366(17)30076-7
Lipsman, N., Woodside, B., and Lozano, A. (2013). Evaluating the potential of deep brain stimulation for treatment-resistant anorexia nervosa. Hand. Clin. Neurol. 116, 271–276. doi: 10.1016/B978-0-444-53497-2.00022-X
Liu, W., Zhan, S., Li, D., Lin, Z., Zhang, C., Wang, T., et al. (2020). Deep brain stimulation of the nucleus accumbens for treatment-refractory anorexia nervosa: A long-term follow-up study. Brain Stimul. 13, 643–649. doi: 10.1016/j.brs.2020.02.004
Lozano, A., Fosdick, L., Chakravarty, M., Leoutsakos, J., Munro, C., Oh, E., et al. (2016). A Phase II Study of Fornix Deep Brain Stimulation in Mild Alzheimer’s Disease. J. Alzheimer Dis. 54, 777–787. doi: 10.3233/JAD-160017
Luyck, K., and Luyten, L. (2015). Can electrical stimulation of the human bed nucleus of the stria terminalis reduce contextual anxiety? An unanswered question. Front. Behav. Neurosci. 9:69. doi: 10.3389/fnbeh.2015.00069
Luyten, L. (2020). The bed nucleus of the stria terminalis: Translational deep brain stimulation to reduce anxiety. Neuroscientist 26, 278–284. doi: 10.1177/1073858419898381
Ma, J., and Leung, L. (2014). Deep brain stimulation of the medial septum or nucleus accumbens alleviates psychosis-relevant behavior in ketamine-treated rats. Behav. Brain Res. 266, 174–182. doi: 10.1016/j.bbr.2014.03.010
Marquez-Franco, R., Carrillo-Ruiz, J., Velasco, A., and Velasco, F. (2022). Deep brain stimulation neuromodulation for the treatment of mood disorders: Obsessive compulsive disorder and treatment resistant depression. Front. Psychiatry 12:764776. doi: 10.3389/fpsyt.2021.764776
McClelland, J., Bozhilova, N., Campbell, I., and Schmidt, U. (2013). A systematic review of the effects of neuromodulation on eating and body weight: Evidence from human and animal studies. Eur. Eat. Disord. Rev. 21, 436–455. doi: 10.1002/erv.2256
Melse, M., Temel, Y., Tan, S., and Jahanshahi, A. (2016). Deep brain stimulation of the rostromedial tegmental nucleus: An unanticipated, selective effect on food intake. Brain Res. Bull. 127, 23–28. doi: 10.1016/j.brainresbull.2016.08.004
Micieli, R., Rios, A., Aguilar, R., Posada, L., and Hutchison, W. (2017). Single-unit analysis of the human posterior hypothalamus and red nucleus during deep brain stimulation for aggressivity. J. Neurosurg. 126, 1158–1164. doi: 10.3171/2016.4
Mundinger, F. (1977). New stereotactic treatment of spasmodic torticollis with a brain stimulation system. Medizinische Klinik 72, 1982–1986.
Nuttin, B., Cosyns, P., Demeulemeester, H., Gybels, J., and Meyerson, B. (1999). Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet 354:1526. doi: 10.1016/S0140-6736(99)02376-4
Oterdoom, D., Lok, R., van Beek, A., den Dunnen, W., Emous, M., van Dijk, J., et al. (2020). Deep brain stimulation in the nucleus accumbens for binge eating disorder: A study in rats. Obes. Surg. 30, 4145–4148. doi: 10.1007/s11695-020-04697-9
Patel, S., Aronson, J., Sheth, S., and Eskandar, E. (2013). Lesion procedures in psychiatric neurosurgery. World Neurosurg. 80, e9–e16. doi: 10.1016/j.wneu.2012.11.038
Penfield, W., and Boldrey, E. (1937). Somatic motor and sensory representation in the cerebral cortex of man as studied by electrical stimulation. Brain 60, 389–443.
Piccolino, M. (1998). Animal electricity and the birth of electrophysiology: The legacy of Luigi Galvani. Brain Res. Bull. 46, 381–407. doi: 10.1016/s0361-9230(98)00026-4
Polyakov, Y., and Kholyavin, A. (2022). Stereotactic surgeries for abuse syndromes: Patient selection and results. Prog. Brain Res. 272, 85–103. doi: 10.1016/bs.pbr.2022.03.006
Ponce, F. A., Asaad, W. F., Foote, K. D., Anderson, W. S., Cosgrove, G. R., Baltuch, G. H., et al. (2016). Bilateral deep brain stimulation of the fornix for Alzheimer’s disease: Surgical safety in the advance trial. J. Neurosurg. 125, 75–84. doi: 10.3171/2015.6.JNS15716
Ríos, A. S., Oxenford, S., Neudorfer, C., Butenko, K., Li, N., Rajamani, N., et al. (2022). Optimal deep brain stimulation sites and networks for stimulation of the fornix in Alzheimer’s disease. Nat. Commun. 13:7707. doi: 10.1038/s41467-022-34510-3
Rizzi, M., Trezza, A., Messina, G., De Benedictis, A., Franzini, A., and Marras, C. (2017). Exploring the brain through posterior hypothalamus surgery for aggressive behavior. Neurosurg. Focus 43:E14. doi: 10.3171/2017.6
Sankar, T., Chakravarty, M. M., Bescos, A., Lara, M., Obuchi, T., Laxton, A. W., et al. (2015). Deep Brain stimulation influences brain structure in Alzheimer’s disease. Brain Stimul. 8, 645–654. doi: 10.1016/j.brs.2014.11.020
Scharre, D. W., Weichart, E., Nielson, D., Zhang, J., Agrawal, P., Sederberg, P. B., et al. (2018). Deep brain stimulation of frontal lobe networks to treat Alzheimer’s disease. J. Alzheimers Dis. 62, 621–633. doi: 10.3233/JAD-170082
Schwabe, K., and Krauss, J. (2018). What rodent models of deep brain stimulation can teach us about the neural circuit regulation of prepulse inhibition in neuropsychiatric disorders. Schizophr. Res. 198, 45–51. doi: 10.1016/j.schres.2017.06.033
Schwemmer, M. A., Skomrock, N. D., Sederberg, P. B., Ting, J. E., Sharma, G., Bockbrader, M. A., et al. (2018). Meeting brain–computer interface user performance expectations using a deep neural network decoding framework. Nat. Med. 24, 1669–1676. doi: 10.1038/s41591-018-0171-y
Simeral, J. D., Hosman, T., Saab, J., Flesher, S. N., Vilela, M., Franco, B., et al. (2021). Home use of a percutaneous wireless intracortical brain-computer interface by individuals with tetraplegia. IEEE Trans. Biomed. Eng. 68, 2313–2325. doi: 10.1109/TBME.2021.3069119
Sobstyl, M., Stapiñska-Syniec, A., Sokół-Szawłowska, M., and Kupryjaniuk, A. (2019). Deep brain stimulation for the treatment of severe intractable anorexia nervosa. Br. J. Neurosurg. 33, 601–607. doi: 10.1080/02688697.2019.1667484
Sturm, V., Lenartz, D., Koulousakis, A., Treuer, H., Herholz, K., Klein, J., et al. (2003). The nucleus accumbens: A target for deep brain stimulation in obsessive-compulsive- and anxiety-disorders. J. Chem. Neuroanat. 26, 293–299. doi: 10.1016/j.jchemneu.2003.09.003
Suthana, N., Haneef, Z., Stern, J., Mukamel, R., Behnke, E., Knowlton, B., et al. (2012). Memory enhancement and deep-brain stimulation of the entorhinal area. New Engl. J. Med. 366, 502–510.
Targum, S. D., Fosdick, L., Drake, K. E., Rosenberg, P. B., Burke, A. D., Wolk, D. A., et al. (2021). Effect of Age on Clinical Trial Outcome in Participants with Probable Alzheimer’s Disease. J. Alzheimers Dis. 82, 1243–1257. doi: 10.3233/JAD-210530
Topalovic, U., Aghajan, Z., Villaroman, D., Hiller, S., Christov-Moore, L., Wishard, T., et al. (2020). Wireless programmable recording and stimulation of deep brain activity in freely moving humans. Neuron 108, 322–334.e9. doi: 10.1016/j.neuron.2020.08.021
Torres, C., Blasco, G., Navas García, M., Ezquiaga, E., Pastor, J., and Vega-Zelaya, L. (2020). Deep brain stimulation for aggressiveness: Long-term follow-up and tractography study of the stimulated brain areas. J. Neurosurg. 7, 1–10. doi: 10.3171/2019.11
Torres, C., Sola, R., Pastor, J., Pedrosa, M., Navas, M., García-Navarrete, E., et al. (2013). Long-term results of posteromedial hypothalamic deep brain stimulation for patients with resistant aggressiveness. J. Neurosurg. 119, 277–287. doi: 10.3171/2013.4.JNS121639
Torres, N., Chabardès, S., and Benabid, A. (2011). Rationale for hypothalamus-deep brain stimulation in food intake disorders and obesity. Adv. Tech. Stand. Neurosurg. 36, 17–30. doi: 10.1007/978-3-7091-0179-7_2
Treasure, J., Duarte, T., and Schmidt, U. (2020). Eating disorders. Lancet 395, 899–911. doi: 10.1016/S0140-6736(20)30059-3
Tronnier, V., Rasche, D., Thorns, V., Alvarez-Fischer, D., Münte, T., and Zurowski, B. (2018). Massive weight loss following deep brain stimulation of the nucleus accumbens in a depressed woman. Neurocase 24, 49–53. doi: 10.1080/13554794.2018.1431678
Velasques, B., Diniz, C., Teixeira, S., Cartier, C., Peressutti, C., Silva, F., et al. (2014). Deep brain stimulation: A new treatment in mood and anxiety disorders. CNS Neurol. Disord. Drug Targets 13, 961–971. doi: 10.2174/1871527313666140612122929
Villalba-Martínez, G., Justicia, A., Salgado, P., Ginés, J., Guardiola, R., Cedrón, C., et al. (2020). A randomized trial of deep brain stimulation to the subcallosal cingulate and nucleus accumbens in patients with treatment-refractory, chronic, and severe anorexia nervosa: Initial results at 6 months of follow up. J. Clin. Med. 9:1946. doi: 10.3390/jcm9061946
Volkow, N., Michaelides, M., and Baler, R. (2019). The neuroscience of drug reward and addiction. Physiol. Rev. 99, 2115–2140. doi: 10.1152/physrev.00014.2018
Wang, T., Moosa, S., Dallapiazza, R., Elias, W., and Lynch, W. (2018). Deep brain stimulation for the treatment of drug addiction. Neurosurg. Focus 45:E11. doi: 10.3171/2018.5.FOCUS18163
Wang, Y., Zhang, C., Zhang, Y., Gong, H., Li, J., Jin, H., et al. (2020). Habenula deep brain stimulation for intractable schizophrenia: A pilot study. Neurosurg. Focus 49:E9. doi: 10.3171/2020.4.FOCUS20174
Wu, H., Van Dyck-Lippens, P., Santegoeds, R., Van Kuyck, K., Gabriëls, L., Lin, G., et al. (2013). Deep-brain stimulation for anorexia nervosa. World Neurosurg. 80, S29.e1–e10. doi: 10.1016/j.wneu.2012.06.039
Yadav, A., Li, S., Krucoff, M., Lebedev, M., Abd-El-Barr, M., and Nicolelis, M. (2021). Generating artificial sensations with spinal cord stimulation in primates and rodents. Brain Stim. 14, 825–836. doi: 10.1016/j.brs.2021.04.024
Keywords: limbic surgery, psychosurgery, aggressiveness, anxiety, drug usage, eating disorders, dementia, transhumanism
Citation: Carrillo-Ruiz JD, Carrillo-Márquez JR, Beltrán JQ, Jiménez-Ponce F, García-Muñoz L, Navarro-Olvera JL, Márquez-Franco R and Velasco F (2023) Innovative perspectives in limbic surgery using deep brain stimulation. Front. Neurosci. 17:1167244. doi: 10.3389/fnins.2023.1167244
Received: 16 February 2023; Accepted: 24 April 2023;
Published: 18 May 2023.
Edited by:
Kenji Kansaku, Dokkyo Medical University, JapanReviewed by:
Maria Rosaria Scala, University of Naples Federico II, ItalyCopyright © 2023 Carrillo-Ruiz, Carrillo-Márquez, Beltrán, Jiménez-Ponce, García-Muñoz, Navarro-Olvera, Márquez-Franco and Velasco. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Damián Carrillo-Ruiz, ZGFtaWFuLmNhcnJpbGxvQGFuYWh1YWMubXg=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.