 Jess A. Holguin
Jess A. Holguin John L. Margetis1
John L. Margetis1 Anisha Narayan
Anisha Narayan Grant M. Yoneoka
Grant M. Yoneoka Andrei Irimia
Andrei Irimia
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci., 07 July 2022
Sec. Brain Imaging Methods
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.905979
This article is part of the Research TopicBrain Imaging Relations Through Simultaneous RecordingsView all 12 articles
Contemporary stroke assessment protocols have a limited ability to detect vascular cognitive impairment (VCI), especially among those with subtle deficits. This lesser-involved categorization, termed mild stroke (MiS), can manifest compromised processing speed that negatively impacts cognition. From a neurorehabilitation perspective, research spanning neuroimaging, neuroinformatics, and cognitive neuroscience supports that processing speed is a valuable proxy for complex neurocognitive operations, insofar as inefficient neural network computation significantly affects daily task performance. This impact is particularly evident when high cognitive loads compromise network efficiency by challenging task speed, complexity, and duration. Screening for VCI using processing speed metrics can be more sensitive and specific. Further, they can inform rehabilitation approaches that enhance patient recovery, clarify the construct of MiS, support clinician-researcher symbiosis, and further clarify the occupational therapy role in targeting functional cognition. To this end, we review relationships between insult-derived connectome alterations and VCI, and discuss novel clinical approaches for identifying disruptions of neural networks and white matter connectivity. Furthermore, we will frame knowledge translation efforts to leverage insights from cutting-edge structural and functional connectomics research. Lastly, we highlight how occupational therapists can provide expertise as knowledge brokers acting within their established scope of practice to drive substantive clinical innovation.
Stroke is the most frequent cause of disability in the United States (Ovbiagele and Nguyen-Huynh, 2011), a fact that spurs investigation into the nature and variability of infarct-related deficits along a continuum of impairment. The literature is replete with widely accepted functional characterizations of moderate through severe stroke (Murphy et al., 2001; Hodics et al., 2012; Rost et al., 2016), with less clarity available on mild clinical presentations (Brott et al., 1989; Roberts et al., 2020). This uncertainty stems from the absence of a precise taxonomy for characterizing the mild stroke (MiS) population (Roberts et al., 2020). In clinical practice, the lack of a consensus definition precludes consistency in evaluation and treatment approaches and obscures understanding of this population’s needs.
Ongoing work to develop an accord on MiS codification can benefit both research and clinical practice. In their systematic review on downstream effects of inconsistent MiS classification, Roberts et al. (2020) discuss 10 distinct definitions present in the literature. This lack of diagnostic and taxonomic uniformity potentiates knowledge translation efforts targeting the depth and breadth of understanding within this important stroke practice and research area. However, even a robust consensus definition cannot explain mechanisms that drive variation in post-stroke disability, especially regarding shared and distinct underpinnings among each NIH Stroke Scale (NIHSS) severity level (National Institute of Neurological Disorders and Stroke, 2011).
Within this review, we address MiS-relevant associations between vascular cognitive impairment (VCI), processing speed (PS), and neural network efficiency, as informed by insights from neuroimaging and connectomics research. We present evidence suggesting that established norms for key neurocognitive assessments can be used as proxies for detecting potentially overlooked VCI. Infusing emerging theoretical perspectives from multiple academic disciplines, we review approaches that can fuel substantial clinical innovation. In particular, we focus on using proxy-defined, threshold-specific instances of dysfunction that are scalable according to premorbid capacities and inherent daily routine demands. Drawing from neuroimaging-informed models employed to predict and monitor stroke recovery, we argue that performance capacity can be quantified by the degree of dissociation between available and necessary performance skills. Such quantification could empower clinicians and MiS survivors to more strategically consider interrelationships between current abilities and requisite progress along an ecologically valid, individualized recovery timeline.
We also examine three intersecting themes that provide a framework for early MiS care innovation and highlight paths to advance clinical investigation targeting health and wellbeing. After providing background on essential considerations of stroke and associated cognitive sequelae, we first review the problem of MiS-associated-VCI (MiS-VCI) underdetection and clarify the consequences of imprecisely characterizing stroke-derived neurocognitive dysfunction. Secondly, we examine the promise of knowledge translation efforts to improve stroke care and address priorities articulated by healthcare systems and research funding agencies. Thirdly, we overview and delineate knowledge relevant to MiS-VCI rehabilitation that derives from cutting-edge neuroanatomic, structural, and functional connectomics research. These studies employ advanced neuroimaging technologies plus conventional computed tomography (CT) and magnetic resonance imaging (MRI). Importantly, we focus on PS as a proxy for the integrity of neural networks and neurocognitive capacities. Lastly, we highlight clinical implications and future directions by providing evidence and arguments supporting more comprehensive MiS-VCI screening in early stroke care and emphasize the pivotal role of occupational therapy (OT) in addressing functional cognition.
While calling attention to the valuable confluence of contemporary research findings and clinical stroke rehabilitation practices, we will discuss literature ranging from the acute to more chronic phases of recovery. Beyond temporal considerations, foundational links between network theory and neurological insults are influenced by a broad range of factors such as demographic characteristics, lesion laterality, and even mechanisms of injury (e.g., ischemic vs. hemorrhagic stroke vs. traumatic brain injury). Herein, we do not focus on such differentiating factors, as it would far exceed the scope of this endeavor and is the likely purview of future prospective data-analytic studies. We do, however, discuss in detail the findings from conceptual and applied perspectives on an overarching construct poised to drive innovation in clinical practice. Please see Table 1. for a summary of constructs and interrelationships.
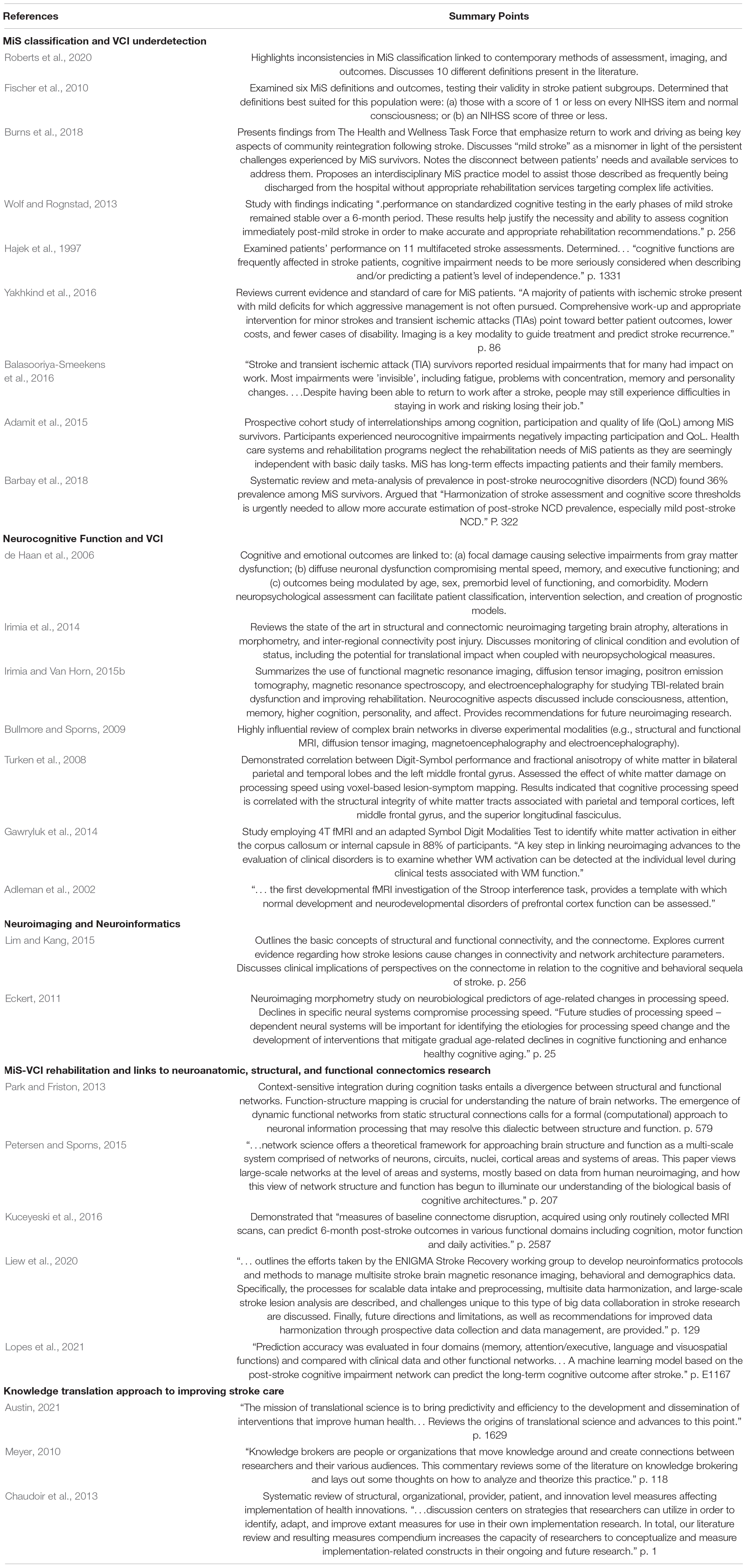
Table 1. Summary of overarching constructs, themes, and seminal works within the reviewed sources.
Currently, stroke is diagnosed based on neuroimaging and clinical examinations. Aberrant clinical examinations often reflect ischemia-associated fragmentation of neural networks and are highly correlated with abnormal findings on CT or MRI (Jadhav et al., 2020). More severe levels of stroke are typically accompanied by overt motor, sensory, and neurocognitive impairments. By contrast, MiS often involves a small ischemic lesion that may go undetected even when employing standard CT imaging. Detecting subtle deficits is further complicated by an upstream dearth of information concerning MiS-VCI. Lacking a consensus taxonomy for MiS, clinicians often rely on imprecise or inadequate categorizations of symptoms and sequelae. Such conceptualizations are frequently derived from routine neurological assessment protocols which quantify post-stroke severity and functional impairment but fall short of informing rehabilitation approaches (Hajek et al., 1997; Wolf and Rognstad, 2013). Importantly, many of these metrics quantify interrelationships between motor deficits and patients’ daily functioning by focusing on the ability to perform activities of daily living (ADL), bed mobility, transfers, and ambulation, rather than neurocognitive capacities (Wolf and Rognstad, 2013; Lee et al., 2015). Within this review, we use the overarching TREAT definition of MiS (Spokoyny et al., 2015) (i.e., NIHSS 0-5, and the absence of visual field deficits, aphasia, pronounced weakness, or other disabling deficits).
“Neurocognitive” refers to the interrelated domains of perceptual-motor function, language, social cognition, complex attention, executive function (EF), learning, and memory (Ganguli et al., 2011). VCI refers to the broad spectrum of neurocognitive impairment associated with vascular pathology, foregrounding working memory, PS, and EF as sensitive categorical impairment indicators (Hachinski et al., 2006). VCI is arguably a key defining characteristic of MiS and a robust predictor of successful participation in normal daily routines (Khatri et al., 2010; Spokoyny et al., 2015; Overdorp et al., 2016). Nevertheless, VCI is often overlooked in acute clinical settings despite multilevel implications for patients, health care systems, and society (Tellier and Rochette, 2009; Ovbiagele et al., 2013; Adamit et al., 2015). This disconnection stems from insufficient MiS diagnostic criteria, with underdeveloped characterizations impeding deficit identification and remediation (Fischer et al., 2010; Roberts et al., 2020). Even using the term mild, in this context, can inadequately represent the persistent obstacles within post-stroke daily functioning (Burns et al., 2018). Lastly, “functional cognition” relates to OT’s focus on “clients” and their capacity to perform essential tasks given the totality of their abilities, including their use of strategies, habits/routines, and contextual/environmental resources (Giles et al., 2017). Although functional cognition requires looking beyond discrete skills, we contend that initially employing a sound, generalized proxy for network dysfunction can increase access to more specific, comprehensive, and ecologically valid types of intervention currently missing from MiS care.
Neurorehabilitation research and practice are moving toward performance-based assessment tools, such as the Executive Function Performance Test (Baum et al., 2008), the Menu Task (Al-Heizan et al., 2020), and the Kettle Test (Hartman-Maeir et al., 2009). Yet, traditional instruments such as the Trail Making Test (Reitan, 1958), Symbol-Digit Modalities Test (SDMT) (Smith, 1973), and Stroop Color-Word Test (SCWT) (Golden and Freshwater, 2002) remain part of the gold standard for validating newer instruments. Despite newer tools achieving higher ecological validity by evaluating real-world task performance, their administration requirements often strain clinician capacities given time and environmental limitations inherent to practice, especially in fast-paced hospital settings.
In this review, we highlight the use of PS to detect compromised connectome integrity. We further explore how assessing VCI via the select, psychometrically robust instruments discussed herein can significantly improve early stroke care services. In particular, circumscribing and formalizing early MiS-VCI detection protocols can help identify subtle deficits that may be otherwise overlooked. Further, more uniform, sensitive, and specific assessments can potentiate greater access to subsequent performance-based OT evaluations emphasizing functional cognition.
Uncertainty surrounding the concept of MiS-VCI derives in part from inadequate in-place assessment protocols (Roberts et al., 2020). This shortcoming is troubling given that VCI is common among MiS survivors (Chung et al., 2013; Spokoyny et al., 2015; Overdorp et al., 2016) and involves subtle—yet persistent—deficits in working memory and EF. Importantly, PS (i.e., “the rapidity with which a patient processes simple or routine information without making errors of either omission or commission,” Weiss et al., 2010) can sensitively detect MiS-VCI. Improper or inadequate computation within neural networks can significantly impact patients’ ability to undertake daily life tasks, especially when required speed, complexity, and duration amount to high cognitive loads (Khatri et al., 2010; Wolf and Rognstad, 2013; Spokoyny et al., 2015). To offset such potential issues, we wish to extend the scope of care available to the underserved MiS population.
Building on existing literature, we aim to advance MiS-VCI knowledge translation targeting clinical research. To this end, we discuss MiS-relevant scope, implications, and opportunities afforded by structural neuroimaging and connectomics research, though without deeply exploring overarching MiS and VCI associations that are thoroughly reviewed elsewhere (Brodaty et al., 2010; Spitzer et al., 2011; Li et al., 2012; Wolf and Rognstad, 2013; Spokoyny et al., 2015; Sensenbrenner et al., 2020). More concretely, we propose a novel course of action informed by neuroimaging, connectomics, network science, and OT that quantifies covert VCI and highlights the mechanistic link to connectopathies. Our central thesis holds that, in light of technological innovation and advances in neuroimaging and neuroinformatics, PS has emerged as an underutilized—yet essential—indicator of compromised neural network integrity, and thus as a viable MiS-VCI biomarker.
Acute stroke screening protocols lack the ability to consistently detect subtle MiS-VCI. Not having sensitive indicators of potential VCI can potentiate patients being ill-prepared to resume full participation in their daily routine. Being unaware of possible neurocognitive deficits, MiS survivors may prematurely recommence complex tasks such as driving, employment, and caregiving. Therefore, we support using robust capacity indicators to quantify potential discrepancies between pre- and post-stroke levels of functioning.
Mild stroke survivors experience less sensorimotor and VCI than those with moderate-to-severe strokes (Tellier and Rochette, 2009). Yet, they have similar rates of disability (19%, Cucchiara et al., 2019) as all stroke severity classifications as a whole (22%, Mu et al., 2017). Current methodological approaches for understanding and quantifying the nuances of MiS-VCI cannot explain the mechanisms that underlie these findings. Therefore, a critical question is: What is the source of MiS survivors’ documented disability?
Even subtle VCI can manifest a profound functional disconnection between past and present capacities when individuals undertake complex tasks (Stephens et al., 2005). In practice, there are widely accepted measures of motor function such as the Fugl-Meyer assessment (Fugl-Meyer et al., 1975) and the Action Research Arm Test (Lyle, 1981; Santisteban et al., 2016). Yet, uncertainty regarding the measurement and classification of MiS-VCI persists. In this context, focusing on MiS-VCI may yield promising etiological insights (de Haan et al., 2006) via ecologically valid perspectives on daily task proficiency (Stephens et al., 2005).
Profound VCI unquestionably contributes to stroke-associated disability (Spitzer et al., 2011; Wolf and Rognstad, 2013; Sensenbrenner et al., 2020). Yet, there is an absence of research examining the influence of PS thresholds on the likelihood and severity of post-stroke disability. This knowledge gap stems from the widespread practice of classifying stroke by heavily weighting the degree of motor impairment, leading to estimates that 88% of stroke cases acquire notable motor deficiencies, with 71% failing to regain motor function within 6 months of onset (Bonita and Beaglehole, 1988). Among those with TREAT-defined MiS, 29-35.6% reportedly experience residual deficits (Spokoyny et al., 2015). Regarding MiS-VCI, focusing on the degradation of network efficiency to better understand post-stroke disability reveals a path to move beyond the circumscribed utility of primarily motor-driven assessments.
Stroke survivors with less pronounced impairments are more likely to resume participation in complex activities that offer little margin for error (Hofgren et al., 2007). This tendency may help explain how MiS survivors that lack overt deficits ultimately file for disability at relatively similar rates to those with higher degrees of documented impairment (Mu et al., 2017). To a potentially detrimental degree, decisions regarding activity participation are likely scaled according to patients’ perceived residual capacity. This perspective derives from individuals’ reflections on their lived experience, combined with the degree to which healthcare providers have endorsed their overarching capacities. Though predominantly missing from discussions in contemporary practice, PS provides a sound framework for assessing the integrity of neurocognitive operations in a way that can bridge the gap between actual and perceived abilities. As detailed in subsequent sections, PS can provide a valuable, quantifiable proxy for neurocognitive function. Moreover, it can drive cutting-edge knowledge translation efforts targeting stroke severity characterization and recovery prediction.
Stroke survivors discharging from the acute hospital setting with unrecognized MiS-VCI face considerable challenges in resuming safe and independent daily routine participation (Balasooriya-Smeekens et al., 2016; Camicia et al., 2016). Unfortunately, there is a dearth of literature coalescing clinical evidence to compel early, highly sensitive neurocognitive assessment that could prompt referrals to essential outpatient therapy services following hospitalization. Without improved, neurocognitively focused early stroke care screening protocols, MiS will remain inconsistently detected, incompletely understood, and MiS survivors will continue to struggle in silence (Barbay et al., 2018).
Despite unequivocal evidence linking functional cognition to successful ADL performance (Chung et al., 2013; Fride et al., 2015; Overdorp et al., 2016), widely used stroke assessments lack the sensitivity to detect subtle VCI (Wolf and Rognstad, 2013; Yakhkind et al., 2016; Burns et al., 2018). Concerns about the limited scope of diagnostic instruments are compounded by the frequent suspicion that some MiS patients are incorrectly perceived as lacking deficits (Yakhkind et al., 2016). As a result, MiS patients are often discharged with unrecognized VCI after brief hospital admissions (Balasooriya-Smeekens et al., 2016; Camicia et al., 2016), and are likely to experience threshold-dependent VCI.
Broadly conceived, threshold-dependent VCI involves diminished neurocognitive functioning linked to activity-dependent increases in cognitive load. Daily living involves fluctuating requirements in speed, complexity, and duration inherent to activity engagement. PS metrics can quantify maladaptive responses to variable, multifocal task demands (Leavitt et al., 2011). Thus, increased cognitive load, reflecting greater requisite mental effort during task performance (Calvillo and Irimia, 2020), is linked to diminished task performance quality (Hajek et al., 1997; Fischer et al., 2010). Clinical stroke protocols can benefit from incorporating elements informed by responses to cognitive load and likely individual-specific performance variability.
Entrenched disconnections between research discovery and carry over into clinical practice reinforce a longstanding barrier to mutually beneficial exchanges of ideas (Austin, 2021). Previous efforts targeting top-down, direct-translation of knowledge to end-users have attempted to rectify this issue, with recent trends favoring intricate, multilevel stakeholder collaborations. Within a knowledge translation framework, OT is highly qualified to incorporate innovative approaches into multidisciplinary care collaboratively. Such ends can be accomplished by OT occasionally acting as the knowledge broker, a designation characterizing persons that “facilitate the creation, sharing, and use of knowledge” (Meyer, 2010).
Given OT’s expertise in addressing functional cognition within dynamic, real-world contexts, practitioners can facilitate valuable MiS-VCI research collaborations mobilizing neuroimaging and connectomics-based knowledge. In particular, they can lend insight into the multifaceted nature of patients’ impairments, an essential component of innovative predictive models, patient care delivery, and communications with various stakeholders. Among allied health professions in acute care settings, OT is the only one to have demonstrated a statistically significant association between healthcare spending and lower readmission rates (Rogers et al., 2017). In line with NIH’s emphasis on innovation and developing evidence-based treatment, OT’s established expertise, in-place representation within acute care teams, and cost-effective services provide strong support for its potential to broker knowledge toward those ends effectively (Chaudoir et al., 2013).
Neuroimaging technologies have added unprecedented scope and precision to our understanding of neurological disorders. Unfortunately, current advances in neuroimaging and neuroinformatics outpace translational efforts targeting MiS care. Given the symbiotic nature of translational research and clinical practice, such delays have hindered ongoing innovation in both domains. Although evidence-based protocols guiding early stroke care have improved recovery trajectories, common metrics quantifying MiS characteristics do not reflect recent insights into complex neural processes underlying observable clinical deficits. Instead, contemporary early stroke clinical assessments inordinately focus on motor capacity over cognitive function (Bonita and Beaglehole, 1988; Hodics et al., 2012), endorsing an underdeveloped representation of MiS sequelae.
Connectomics is the field of study concerned with the systematic mapping of neural connections. It provides a unique framework for analyzing neural network disruptions by combining graph theory methodology with neuroimaging (Irimia et al., 2014). Specifically, by conceptualizing brain regions as nodes with structural or functional properties connected by white matter (WM) fibers, connectomics can bridge the gap between mapping neural networks and understanding their functions (Bullmore and Sporns, 2009). Neural network analysis involves focusing on both functional and structural connectivity (Irimia and Van Horn, 2015b). Employing diffusion tensor imaging (DTI) and diffusion spectrum imaging, structural connectomics uses spatial topography data to construct a physical map of neural activity and infer WM anatomic organization along with neurological insult-derived connectivity damage (Irimia et al., 2014).
Using functional MRI (fMRI) (Irimia and Van Horn, 2015b), magnetoencephalography (MEG) (Irimia and Van Horn, 2015a), and electroencephalography (EEG) (Lima et al., 2006; Irimia and Van Horn, 2015a) functional connectomics involves the study of neural network activity via: (a) temporal dynamics; (b) maps representing information exchange between nodes and modules; (c) resting states; and (d) responses to exogenous stimuli (Halgren et al., 2011). Such studies facilitate the measurement of network integrity following neurological insults, including stroke. Additionally, brain activity can be further understood mechanistically through activation patterns identified within the functional connectome. This lens can be useful when cognitive abilities, behavior, or network PS modulate neural responses (Craddock et al., 2015).
Ischemic insults can compromise information processing within and across neural networks. In worst-case scenarios, this ability is lost. In more moderate cases, neuroplasticity can facilitate the preservation of intended operational outputs in a lesioned network. Importantly, this type of recovery has been studied more thoroughly in sensorimotor than neurocognitive domains (Gray et al., 1989; Wang et al., 2010; Lee et al., 2015). With neurocognitive demands, however, negative consequences of ischemic insults may manifest as sub-optimal neural processing, producing operations that are detrimental to the desired outcome or are inadequately timed. Such imprecision gives rise to alternative neural pathway use during network activation sequences to meet specific PS demands (Honey and Sporns, 2008; Wang et al., 2010). By integrating connectomics insights into practice and knowledge translation initiatives, rehabilitation professionals can better identify, isolate, and subsequently target alternative pathways within patient-tailored therapeutic activities.
Consistent with previously discussed trends comparing VCI across stroke severity levels, the ubiquity of WM damage and compromised neurocognitive function is well-documented among severe cases (Zinn et al., 2007), and significantly less so among those with lower degrees of functional impairment (Wolf and Rognstad, 2013). Using innovative PS measures can more sensitively detect MiS-VCI than standard assessment protocols. The following two sections review evidence linking common processing efficiency metrics to emerging insights from connectomics. Such evidence, we propose, can aid the formulation of novel, concrete guidelines for utilizing such knowledge in clinical rehabilitation practice and knowledge translation endeavors.
Previous studies have highlighted relationships between PS and the modulation of WM connections. For example, Turken et al. (2008) demonstrated that damage to the structural integrity of WM axons correlates with diminished performance in PS tasks. Specifically, posterior parietal lesions often lead to compromised PS and associated changes in the integrity of water diffusion anisotropy along WM fibers. Additional evidence suggests that brain activity recruiting temporo-occipital WM structures, such as the inferior longitudinal fasciculi, also modulates PS (Turken et al., 2008). There is robust support for the use of well-studied, psychometrically sound neurocognitive assessments targeting processing efficiency. For example, the SDMT evaluates PS and efficiency and is sensitive to WM disruptions (Gawryluk et al., 2014), whereas the SCWT includes a useful event-related cognitive task that can measure PS sensitively even in the presence of subtle VCI (Adleman et al., 2002).
DTI techniques like WM tractography facilitate the modeling and visualization of neural pathways (Basser and Pierpaoli, 2011). This method has been used to employ compromised processing efficiency as a metric for impairment magnitude across various neurocognitive domains. Action potentials propagating along WM axons enable information exchange across neural networks, often by synchronizing the firing of neuronal populations (Assaf and Pasternak, 2008; Turken et al., 2008; Basser and Pierpaoli, 2011). Thus, WM insults can substantially alter information processing across network nodes, disrupting neurocognitive capacities (Assaf and Pasternak, 2008; Turken et al., 2008; Basser and Pierpaoli, 2011). At the microscale, such insults often involve dendritic or synaptic loss and inflammation modulated by microglia, both phenomena being able to interfere with local network function (Lim and Kang, 2015).
In addition to applications for MiS-VCI, given DTI’s ability to identify subtle WM abnormalities, it can assist in predicting functional outcomes in other cases involving less severe neurological insults. In particular, there is support for this technology addressing WM changes associated with cerebral hemorrhages and mild traumatic brain injury (Irimia et al., 2014), as well as those linked to the neuro-invasion potential of SARS-CoV-2 during the recovery from COVID-19 (Lu et al., 2020). Importantly, standard structural MRI cannot always detect WM changes (Lim and Helpern, 2002; Assaf and Pasternak, 2008). Thus, DTI can be leveraged to assist the diagnosis and classification of MiS, and help researchers elucidate the relationship between structural WM damage and MiS-VCI. Additionally, because DTI-based network analysis can provide quantitative measures of brain dysfunction, this strategy can complement in-place behavioral diagnostic methods. For these reasons, we propose that insights obtained by combining quantitative descriptions of structural network integrity and insult location can have utility for improving diagnostic accuracy while facilitating MiS characterization and targeted treatment-approach development.
In its own right, functional connectivity can substantially assist MiS diagnosis and classification. Research suggests that the brain can be modeled as a small-world network with extensive local clustering, which facilitates efficient information processing (Lim and Kang, 2015). Global communication, by contrast, relies on long-range connections between network nodes. This ranged approach enables further information processing and integration across neuroanatomically or functionally distinct regions. The extent of network impairment following stroke is highly dependent upon lesion location and can alter both local and global network efficiencies (Wang et al., 2010; Lim and Kang, 2015). For example, Wang et al. (2010) studied patients with focal subcortical motor pathway damage and found that, compared to healthy volunteers, motor execution networks exhibited lower efficiency of local information transfer between homotopic brain network regions. Similarly, reductions in global network efficiency due to nodal damage have been demonstrated by both computational models and MRI studies (Honey and Sporns, 2008; Alstott et al., 2009; Wang et al., 2010). Therefore, interpretations and clinical applications of connectomic measures require careful consideration.
While stroke may compromise local network efficiency, distal network modules can assume the roles of injured regions in response to rehabilitation (Biernaskie et al., 2005; Nomura et al., 2010; Grefkes and Fink, 2011). Given structural redundancies within the brain, these networks can be recruited during recovery from stroke, potentiating functional improvement. Whereas local network efficiency can decrease following stroke, there can also be simultaneous, compensatory functional connectivity increases throughout the brain. Compensation may involve rerouting information between nodes using indirectly connected uninjured regions, increasing the amount of neural processing commensurate with task demands.
Researchers can harness functional connectomics to enhance investigations of cortical information exchange and network integrity since connectomic analysis can sensitively detect subtle MiS-VCI. Furthermore, functional connectivity methods can facilitate the investigation of task-related, inter-regional coupling (Wang et al., 2010), phenomena that are essential considerations in conceptualizing VCI. Incorporating these insights into MiS care can bolster clinical assessment methods and improve the detection of subtle network inefficiencies associated with context-driven impairment.
To assess network processing efficiency and quantify the adequacy of mental operations indelible to neurocognitive function, clinical assessments should account for patient-specific factors that facilitate or hinder performance. Replicating stressors that fuel context-driven impairment can be impractical in acute care settings. In this light, there is utility in identifying a sound proxy to screen core neurocognitive capacities. One crucial factor that varies in response to context-driven cognitive demands is PS. Task-specific demands governing speed, complexity, and duration parameters influence the degree of perceived difficulty associated with any given neurocognitive operation.
Distractions and unexpected changes in the scope of a given task can negatively impact processing efficiency by increasing the cognitive load. Such challenges increase demands upon working memory and EF. Given the nuanced nature of daily living, difficulties may still ensue after reducing competing stimuli and prioritizing task resources. Within the literature, there are examples linking compromised PS to deficient saccadic eye movements and oculomotor impairment to neurocognitive dysfunction (Barnett and Singman, 2015). Similarly, the SCWT and the SDMT are gold-standard assessments of PS (Smith, 1973; Golden and Freshwater, 2002). Importantly, results from these instruments derive from large normative statistical samples and allow subject stratification according to age and educational attainment peers. These tests have also been used to measure neurocognitive function under heightened cognitive load (Siegle et al., 2008) and detect deficits ranging from subtle to profound impairment. In conclusion, using PS as a proxy to assess connectomic integrity and subsequent neurocognitive capacities provides a central organizing principle to inform MiS-VCI detection protocols, drive knowledge translation efforts, and refine treatment approaches.
Building on the Human Connectome Project’s body of knowledge, current conceptualizations of intact network processing (Sporns et al., 2005), generalized linear models of neurocognitive function (Park and Friston, 2013; Petersen and Sporns, 2015), and studies of damaged network integrity due to focal or diffuse injuries (Lim and Kang, 2015), the potential benefit of incorporating connectomic methods into MiS care protocols is compelling. Work toward this end involves creating functional connectivity models, plus calculating network clustering coefficients and characteristic path lengths (Bullmore and Sporns, 2009). Thus, improved MiS-VCI detection could involve quantifying neural network efficiency or the extent of network reorganization following injury. Such strategies offer the potential to stratify MiS presentations with substantial sensitivity and specificity based on the severity of functional network impairments. This approach has already been demonstrated in proof-of-concept studies involving moderate-to-severe stroke (Wang et al., 2010), suggesting that extending this method to more accurately characterize MiS-VCI should be a future research priority.
While clinical neuroimaging modalities critically inform medical management decisions following moderate and severe stroke (Wintermark et al., 2013), multimodal imaging and network theory research have substantially advanced our current understanding of structural and functional connectivity disturbances underlying MiS (Silasi and Murphy, 2014). Such progress has enabled clinicians and researchers to better characterize stroke lesions and their impact on structural and functional connectivity. In practice, neuroimaging localizes lesions topographically to construct a predictive framework for cognitive outcomes after stroke (Hope et al., 2013). However, most topographic models do not account for stroke severity (van Meer et al., 2012; Hope et al., 2013). Thus, aiming beyond topography-based lesion analysis (e.g., studying stroke-driven structural connectome alterations) can potentially help predict MiS-VCI incidence and identify associated biomarkers (Kuceyeski et al., 2016). To improve MiS care, clinician scientists, OT, and other allied health professions should acquire and incorporate findings from standard structural and multimodal imaging technologies. Employing aggregate, atlas-informed (Liew et al., 2020) neuroimaging biomarkers can aid MiS classification, reducing uncertainty stemming from absent consensus on best practices governing detection and diagnosis. Although MiS and brain network heterogeneity may be limiting factors in this respect, incorporating knowledge from VCI-associated deficit atlases can refine clinical evaluations (Wang et al., 2010). Insights from these data-driven approaches may inform the development and selection of MiS-VCI rehabilitation approaches rooted in daily living contexts. However, what is the best way to employ multimodal approaches in quantifying network efficiency and PS while also deriving more sensitive and specific MiS-VCI characterizations? One process could involve the creation or refinement of resting-state fMRI atlases and mapping MiS-associated functional network impairments. This type of development would be akin to MR fingerprinting techniques (Ma et al., 2013) and the Virtual Brain Project, where neuroinformatics drives personalized medical care (Falcon et al., 2016).
Advances in network theory and neuroimaging applications can help clinicians develop innovative, evidence-based, early MiS care. For example, the literature supports the utility of studying compromised network efficiency linked to damaged neuroanatomical structures (Honey and Sporns, 2008). Due to stroke-related increases in average neural network path lengths, information relayed across these structures takes longer to reach intended destinations. This insult-derived change supports screening for MiS-VCI using PS metrics (Turken et al., 2008; Eckert, 2011), as PS is a key variable predicting overall cognition-based stroke outcomes (Su et al., 2015).
As previously discussed, VCI can be reliably measured at the bedside by OT using robust instruments like the SDMT and SCWT (Smith, 1973; Golden and Freshwater, 2002). Additionally, compromised PS can disrupt essential visual-motor skills such as pursuits and saccades. These foundational visual-motor abilities are sensitive to mild cortical insults and can reflect the integrity of core neurocognitive capacities at risk for context-driven impairment (Barnett and Singman, 2015). Therefore, healthcare providers should integrate this information into early stroke care protocols to increase MiS-VCI detection and subsequent access to services (e.g., outpatient OT targeting functional cognition and post-stroke quality of life).
Looking beyond applications within acute MiS care, neuroimaging advances could inform more effective functional cognition protocols for chronic insult recovery. Historically, clinicians have relied heavily upon assessment batteries or subjective measures to determine intervention efficacy (Hajek et al., 1997). However, research suggests that technology such as DTI can be employed to bolster predictions regarding motor responses to restorative stroke therapies (Cassidy et al., 2018). The validity of such approaches targeting MiS-VCI would be further strengthened by in-depth analyses of network disruptions within specific regions of interest, quantified by measures like connectivity strength (Sporns and Zwi, 2004; Park and Friston, 2013).
In addition to improving detection and service provision for stroke patients, emerging practices involving multimodal neuroimaging are being employed to model and predict clinical outcomes. For example, recent studies have successfully predicted aspects of post-stroke cognitive recovery by examining DTI-based connectivity measures and employing machine learning analysis of resting-state network fMRI data (Aben et al., 2021; Lopes et al., 2021). Unfortunately, these studies focus on long-term timelines, using measures acquired 6 months after stroke to predict function at 3-years, or 5 weeks post onset being used to predict 1-year status. We contend that, while such studies are important to advance our overarching understanding of stroke, we must also look pointedly at immediately pressing issues. Specifically, steps should be promptly taken to improve triaging and care for individuals experiencing MiS.
The clinical and neuroimaging communities should undertake sustained knowledge translation efforts to develop theory-driven, practice-based treatment models addressing the paucity of knowledge regarding MiS-VCI. As exemplified in the examples below, integrating neuroimaging protocols with clinical rehabilitation insights can enhance our understanding of this understudied condition. For instance, bolstering functional cognition assessments to consider network strain under high cognitive loads can improve MiS-VCI characterization. Also, positron emission tomography (PET) or MR spectroscopy (MRS) can potentiate improved post-stroke functional mapping and pharmacological targeting of performance-specific neurotransmitters and blood-borne molecules (Schlosser, 2000). Further, evidence supports that incorporating neuroimaging insights into pharmaceutical development protocols can improve early post-stroke medication effectiveness (Faingold and Blumenfeld, 2015). One potentially beneficial general consideration regarding MRI segmentation, as the accuracy of its scheme relies on the ability to differentiate between tissue classes (Madhukumar and Santhiyakumari, 2015) is that the use of fuzzy preprocessors can account for tissue geometry and reduce computational load (Versaci et al., 2015). Lastly, promising MEG/EEG mapping research supports that temporal network patterns reflect resource shifts pre, during, and post task performance (Irimia and Van Horn, 2015b). Studies such as these, examined within large samples, could elucidate high-frequency, time-dependent characteristics of network activity, against which deficient MiS-VCI dynamics can be compared. However, considerable work remains to clarify interrelationships between MiS-driven electrophysiological changes during neural activity and links to clinical parameters.
Subtle stroke-associated neurocognitive impairment is an under-examined condition that impacts patients, health care systems, and society overall (Sun et al., 2014). Though two-thirds of stroke survivors experience minor deficits (Yaghi et al., 2017), and the emerging recognition that VCI is a potential hallmark of MiS (Lim and Kang, 2015), conventional assessments often mischaracterize or inadequately detect MiS. Existing diagnostic and rehabilitation paradigms would benefit from incorporating current perspectives from neuroimaging and connectomics. Such inclusion would illustrate research and practice symbiosis, via knowledge translation efforts, targeting improved MiS-VCI construct clarification and clinical service provision.
Incorporating connectomics and network theory into existing clinical perspectives may require further innovation targeting the acquisition, analysis, and interpretation of neuroimaging data. Nevertheless, structural and functional neuroimaging methods offer unique opportunities for scientific discovery and clinical advances in MiS care whether employed individually or together (Silasi and Murphy, 2014). Available literature supports two key approaches for developing and refining current perspectives: (a) quantify interrelationships between MiS-VCI and network dysfunction via existing neurocognitive assessments; and (b) atlas MiS-derived neural damage to bolster interdependence of MiS research and clinical practice (Liew et al., 2020). These and other strategic knowledge-translation efforts should be pursued in the understudied yet epidemiologically significant area of MiS-VCI.
Finally, considering the MiS-survivor experience, returning to prior routines can be fraught with challenges. Performing complex activities with neurocognitive deficits can be complicated by a narrow margin of error separating success from failure. Consider the prospect of resuming employment with undiagnosed MiS-VCI. A VCI-fueled unsuccessful return to work scenario is easy to envision without access to sensitive assessment and treatment. Despite legal protections available through the Americans with Disabilities Act (n.d.), there is still an inordinate risk for performance-based termination if MiS-VCI has not been identified.
Every day, lapses in judgment and substandard quality of work drives job loss among neurologically intact individuals. In this light, how are MiS-VCI survivors likely to fare given an increased probability of substandard complex task performance in conjunction with potential overestimations of their capacities? Without sensitive MiS-VCI assessments and established access to ecologically valid functional cognition interventions, MiS survivors are often ill-equipped to fully participate in the context of daily living. They are also likely to struggle in negotiating the impact of multifaceted functional disconnections from their baseline capacities. Such deficiencies can be life-changing, significantly altering their ability to perform other complex tasks such as driving and caregiving. In response to such potentialities, clinicians and researchers should proactively infuse cutting-edge neuroimaging technology, neuroinformatics, and connectomics perspectives into rehabilitative approaches to positively influence MiS survivors’ neurocognitive recovery trajectories.
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
This study was supported by the National Institutes of Health grants R01 NS 100973 and RF1 AG 054443 to AI, by the U.S. Department of Defense contract W81XWH-18-1-0413, a Hanson-Thorell Family Research Scholarship, the James J. and Sue Femino Foundation, and the University of Southern California through the Undergraduate Research Associates Program (URAP) and the Center for Undergraduate Research in Viterbi Engineering (CURVE).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Aben, H. P., De Munter, L., Reijmer, Y. D., Spikman, J. M., Visser-Meily, J. M. A., Biessels, G. J., et al. (2021). Prediction of Cognitive Recovery After Stroke: The Value of Diffusion-Weighted Imaging-Based Measures of Brain Connectivity. Stroke 52, 1983–1992. doi: 10.1161/STROKEAHA.120.032033
Adamit, T., Maeir, A., Ben Assayag, E., Bornstein, N. M., Korczyn, A. D., and Katz, N. (2015). Impact of first-ever mild stroke on participation at 3 and 6 month post-event: the TABASCO study. Disabil. Rehabil. 37, 667–673. doi: 10.3109/09638288.2014.923523
Adleman, N. E., Menon, V., Blasey, C. M., White, C. D., Warsofsky, I. S., Glover, G. H., et al. (2002). A developmental fMRI study of the Stroop color-word task. Neuroimage 16, 61–75. doi: 10.1006/nimg.2001.1046
Al-Heizan, M. O., Giles, G. M., Wolf, T. J., and Edwards, D. F. (2020). The construct validity of a new screening measure of functional cognitive ability: The menu task. Neuropsychol. Rehabil. 30, 961–972. doi: 10.1080/09602011.2018.1531767
Alstott, J., Breakspear, M., Hagmann, P., Cammoun, L., and Sporns, O. (2009). Modeling the Impact of Lesions in the Human Brain. PLoS Comput. Biol. 5:e1000408. doi: 10.1371/journal.pcbi.1000408
Assaf, Y., and Pasternak, O. (2008). Diffusion tensor imaging (DTI)-based white matter mapping in brain research: a review. J. Mol. Neurosci. 34, 51–61. doi: 10.1007/s12031-007-0029-0
Austin, C. P. (2021). Opportunities and challenges in translational science. Clin. Transl. Sci. 14, 1629–1647. doi: 10.1111/cts.13055
Balasooriya-Smeekens, C., Bateman, A., Mant, J., and De Simoni, A. (2016). Barriers and facilitators to staying in work after stroke: insight from an online forum. BMJ Open 6:e009974. doi: 10.1136/bmjopen-2015-009974
Barbay, M., Diouf, M., Roussel, M., and Godefroy, O. (2018). Systematic Review and Meta-Analysis of Prevalence in Post-Stroke Neurocognitive Disorders in Hospital-Based Studies. Dement Geriatr. Cogn. Disord. 46, 322–334. doi: 10.1159/000492920
Barnett, B. P., and Singman, E. L. (2015). Vision concerns after mild traumatic brain injury. Curr. Treat. Options Neurol. 17:329. doi: 10.1007/s11940-014-0329-y
Basser, P. J., and Pierpaoli, C. (2011). Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J. Magn. Reson. 213, 560–570. doi: 10.1016/j.jmr.2011.09.022
Baum, C. M., Connor, L. T., Morrison, T., Hahn, M., Dromerick, A. W., and Edwards, D. F. (2008). Reliability, validity, and clinical utility of the Executive Function Performance Test: a measure of executive function in a sample of people with stroke. Am. J. Occup. Ther. 62, 446–455. doi: 10.5014/ajot.62.4.446
Biernaskie, J., Szymanska, A., Windle, V., and Corbett, D. (2005). Bi-hemispheric contribution to functional motor recovery of the affected forelimb following focal ischemic brain injury in rats. Eur. J. Neurosci. 21, 989–999. doi: 10.1111/j.1460-9568.2005.03899.x
Bonita, R., and Beaglehole, R. (1988). Recovery of motor function after stroke. Stroke 19, 1497–1500. doi: 10.1161/01.STR.19.12.1497
Brodaty, H., Altendorf, A., Withall, A., and Sachdev, P. S. (2010). Mortality and institutionalization in early survivors of stroke: the effects of cognition, vascular mild cognitive impairment, and vascular dementia. J. Stroke Cerebrovasc. Dis. 19, 485–493. doi: 10.1016/j.jstrokecerebrovasdis.2009.09.006
Brott, T., Adams, H. P. Jr., Olinger, C. P., Marler, J. R., Barsan, W. G., Biller, J., et al. (1989). Measurements of acute cerebral infarction: a clinical examination scale. Stroke 20, 864–870. doi: 10.1161/01.STR.20.7.864
Bullmore, E., and Sporns, O. (2009). Complex brain networks: graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 10, 186–198. doi: 10.1038/nrn2575
Burns, S. P., Schwartz, J. K., Scott, S. L., Devos, H., Kovic, M., Hong, I., et al. (2018). Interdisciplinary Approaches to Facilitate Return to Driving and Return to Work in Mild Stroke: A Position Paper. Arch. Phys. Med. Rehabil. 99, 2378–2388. doi: 10.1016/j.apmr.2018.01.032
Calvillo, M., and Irimia, A. (2020). Neuroimaging and Psychometric Assessment of Mild Cognitive Impairment After Traumatic Brain Injury. Front. Psychol. 11:1423. doi: 10.3389/fpsyg.2020.01423
Camicia, M., Wang, H., DiVita, M., Mix, J., and Niewczyk, P. (2016). Length of Stay at Inpatient Rehabilitation Facility and Stroke Patient Outcomes. Rehabil. Nurs. 41, 78–90. doi: 10.1002/rnj.218
Cassidy, J. M., Tran, G., Quinlan, E. B., and Cramer, S. C. (2018). Neuroimaging Identifies Patients Most Likely to Respond to a Restorative Stroke Therapy. Stroke 49, 433–438. doi: 10.1161/STROKEAHA.117.018844
Chaudoir, S. R., Dugan, A. G., and Barr, C. H. (2013). Measuring factors affecting implementation of health innovations: a systematic review of structural, organizational, provider, patient, and innovation level measures. Implement. Sci. 8:22. doi: 10.1186/748-5908-8-22
Chung, C., Pollock, A., Campbell, T., Durward, B., and Hagen, S. (2013). Cognitive rehabilitation for executive dysfunction in adults with stroke or other adult nonprogressive acquired brain damage. Stroke. 44:e77–e78. doi: 10.1161/STROKEAHA.113.002049
Craddock, R. C., Tungaraza, R. L., and Milham, M. P. (2015). Connectomics and new approaches for analyzing human brain functional connectivity. Gigascience 4:13. doi: 10.1186/s13742-015-0045-x
Cucchiara, B., George, D. K., Kasner, S. E., Knutsson, M., Denison, H., Ladenvall, P., et al. (2019). Disability after minor stroke and TIA: A secondary analysis of the SOCRATES trial. Neurology 93, e708–e716. doi: 10.1212/WNL.0000000000007936
de Haan, E. H., Nys, G. M., and Van Zandvoort, M. J. (2006). Cognitive function following stroke and vascular cognitive impairment. Curr. Opin. Neurol. 19, 559–564. doi: 10.1097/01.wco.0000247612.21235.d9
Eckert, M. A. (2011). Slowing down: age-related neurobiological predictors of processing speed. Front. Neurosci. 5:25. doi: 10.3389/fnins.2011.00025
Faingold, C. L., and Blumenfeld, H. (2015). Targeting Neuronal Networks with Combined Drug and Stimulation Paradigms Guided by Neuroimaging to Treat Brain Disorders. Neuroscientist 21, 460–474. doi: 10.1177/1073858415592377
Falcon, M. I., Jirsa, V., and Solodkin, A. (2016). A new neuroinformatics approach to personalized medicine in neurology: The Virtual Brain. Curr. Opin. Neurol. 29, 429–436. doi: 10.1097/WCO.0000000000000344
Fischer, U., Baumgartner, A., Arnold, M., Nedeltchev, K., Gralla, J., De Marchis, G. M., et al. (2010). What is a minor stroke? Stroke 41, 661–666. doi: 10.1161/STROKEAHA.109.572883
Fride, Y., Adamit, T., Maeir, A., Ben Assayag, E., Bornstein, N. M., Korczyn, A. D., et al. (2015). What are the correlates of cognition and participation to return to work after first ever mild stroke? Top. Stroke Rehabil. 22, 317–325. doi: 10.1179/1074935714Z.0000000013
Fugl-Meyer, A. R., Jääskö, L., Leyman, I., Olsson, S., and Steglind, S. (1975). The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 7, 13–31.
Ganguli, M., Blacker, D., Blazer, D. G., Grant, I., Jeste, D. V., Paulsen, J. S., et al. (2011). Classification of neurocognitive disorders in DSM-5: a work in progress. Am. J. Geriatr. Psychiatr. 19, 205–210. doi: 10.1097/JGP.0b013e3182051ab4
Gawryluk, J. R., Mazerolle, E. L., Beyea, S. D., and D’Arcy, R. C. (2014). Functional MRI activation in white matter during the Symbol Digit Modalities Test. Front. Hum. Neurosci. 8:589. doi: 10.3389/fnhum.2014.00589
Giles, G. M., Edwards, D. F., Morrison, M. T., Baum, C., and Wolf, T. J. (2017). Screening for Functional Cognition in Postacute Care and the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014. Am. J. Occup. Ther. 71, 7105090010p1–7105090010p6 doi: 10.5014/ajot.2017.715001
Golden, C., and Freshwater, S. M. (2002). The Stroop Color and Word Test: a Manual for Clinical and Experimental Uses. Chicago, IL: Stoelting.
Gray, C. S., French, J. M., Bates, D., Cartlidge, N. E., Venables, G. S., and James, O. F. (1989). Recovery of visual fields in acute stroke: homonymous hemianopia associated with adverse prognosis. Age Ageing 18, 419–421. doi: 10.1093/ageing/18.6.419
Grefkes, C., and Fink, G. R. (2011). Reorganization of cerebral networks after stroke: new insights from neuroimaging with connectivity approaches. Brain 134(Pt 5), 1264–1276. doi: 10.1093/brain/awr033
Hachinski, V., Iadecola, C., Petersen, R. C., Breteler, M. M., Nyenhuis, D. L., Black, S. E., et al. (2006). National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 37, 2220–2241. doi: 10.1161/01.STR.0000237236.88823.47
Hajek, V. E., Gagnon, S., and Ruderman, J. E. (1997). Cognitive and functional assessments of stroke patients: an analysis of their relation. Arch. Phys. Med. Rehabil. 78, 1331–1337. doi: 10.1016/S0003-9993(97)90306-3
Halgren, E., Sherfey, J., Irimia, A., Dale, A. M., and Marinkovic, K. (2011). Sequential temporo-fronto-temporal activation during monitoring of the auditory environment for temporal patterns. Hum. Brain Mapp. 32, 1260–1276. doi: 10.1002/hbm.21106
Hartman-Maeir, A., Harel, H., and Katz, N. (2009). Kettle test–a brief measure of cognitive functional performance. Reliability and valdity in stroke rehabilitation. Am. J. Occup. Ther. 63, 592–599. doi: 10.5014/ajot.63.5.592
Hodics, T. M., Nakatsuka, K., Upreti, B., Alex, A., Smith, P. S., and Pezzullo, J. C. (2012). Wolf Motor Function Test for characterizing moderate to severe hemiparesis in stroke patients. Arch. Phys. Med. Rehabil. 93, 1963–1967. doi: 10.1016/j.apmr.2012.05.002
Hofgren, C., Björkdahl, A., Esbjörnsson, E., and Sunnerhagen, K. S. (2007). Recovery after stroke: cognition, ADL function and return to work. Acta Neurol. Scand. 115, 73–80. doi: 10.1111/j.1600-0404.2006.00768.x
Honey, C. J., and Sporns, O. (2008). Dynamical consequences of lesions in cortical networks. Hum. Brain Mapp. 29, 802–809. doi: 10.1002/hbm.20579
Hope, T. M., Seghier, M. L., Leff, A. P., and Price, C. J. (2013). Predicting outcome and recovery after stroke with lesions extracted from MRI images. Neuroimage Clin. 2, 424–433. doi: 10.1016/j.nicl.2013.03.005
Irimia, A., and Van Horn, J. D. (2015b). Functional neuroimaging of traumatic brain injury: advances and clinical utility. Neuropsychiatr. Dis. Treat. 11, 2355–2365. doi: 10.2147/NDT.S79174
Irimia, A., and Van Horn, J. D. (2015a). Epileptogenic focus localization in treatment-resistant post-traumatic epilepsy. J. Clin. Neurosci. 22, 627–631. doi: 10.1016/j.jocn.2014.09.019
Irimia, A., Goh, S. Y., Torgerson, C. M., Vespa, P., and Van Horn, J. D. (2014). Structural and connectomic neuroimaging for the personalized study of longitudinal alterations in cortical shape, thickness and connectivity after traumatic brain injury. J. Neurosurg. Sci. 58, 129–144.
Jadhav, A. P., Desai, S. M., Liebeskind, D. S., and Wechsler, L. R. (2020). Neuroimaging of Acute Stroke. Neurol. Clin. 38, 185–199. doi: 10.1016/j.ncl.2019.09.004
Khatri, P., Kleindorfer, D. O., Yeatts, S. D., Saver, J. L., Levine, S. R., Lyden, P. D., et al. (2010). Strokes with minor symptoms: an exploratory analysis of the National Institute of Neurological Disorders and Stroke recombinant tissue plasminogen activator trials. Stroke 41, 2581–2586. doi: 10.1161/STROKEAHA.110.593632
Kuceyeski, A., Navi, B. B., Kamel, H., Raj, A., Relkin, N., Toglia, J., et al. (2016). Structural connectome disruption at baseline predicts 6-months post-stroke outcome. Hum. Brain Mapp. 37, 2587–2601. doi: 10.1002/hbm.23198
Leavitt, V. M., Lengenfelder, J., Moore, N. B., Chiaravalloti, N. D., and DeLuca, J. (2011). The relative contributions of processing speed and cognitive load to working memory accuracy in multiple sclerosis. J. Clin. Exp. Neuropsychol. 33, 580–586. doi: 10.1080/13803395.2010.541427
Lee, K. B., Lim, S. H., Kim, K. H., Kim, K. J., Kim, Y. R., Chang, W. N., et al. (2015). Six-month functional recovery of stroke patients: a multi-time-point study. Int. J. Rehabil. Res. 38, 173–180. doi: 10.1097/MRR.0000000000000108
Li, W., Cheng, Y. H., and Yu, X. G. (2012). [Observation on therapeutic effect of acupuncture combined with medicine on mild cognition disorders in patients with post-stroke]. Zhongguo Zhen Jiu 32, 3–7.
Liew, S. L., Zavaliangos-Petropulu, A., Jahanshad, N., Lang, C. E., Hayward, K. S., Lohse, K. R., et al. (2020). The ENIGMA Stroke Recovery Working Group: Big data neuroimaging to study brain-behavior relationships after stroke. Hum. Brain Mapp. 43, 129–148. doi: 10.1002/hbm.25015
Lim, J. S., and Kang, D. W. (2015). Stroke Connectome and Its Implications for Cognitive and Behavioral Sequela of Stroke. J. Stroke 17, 256–267. doi: 10.5853/jos.2015.17.3.256
Lim, K. O., and Helpern, J. A. (2002). Neuropsychiatric applications of DTI-a review. NMR Biomed. 15, 587–593. doi: 10.1002/nbm.789
Lima, E. A., Irimia, A., and Wikswo, J. P. (2006). “The magnetic inverse problem”. The SQUID Handbook: Applications of SQUIDs and SQUID Systems.(eds) J. Clarke and A. I. Braginski (Hoboken, NJ: John Wiley & Sons) doi: 10.1002/9783527609956.ch10
Lopes, R., Bournonville, C., Kuchcinski, G., Dondaine, T., Mendyk, A. M., Viard, R., et al. (2021). Prediction of Long-term Cognitive Functions after Minor Stroke, Using Functional Connectivity. Neurology. [Epub ahead of print] doi: 10.1212/WNL.0000000000011452
Lu, Y., Li, X., Geng, D., Mei, N., Wu, P. Y., Huang, C. C., et al. (2020). Cerebral Micro-Structural Changes in COVID-19 Patients-An MRI-based 3-month Follow-up Study. EClin. Med. 25:100484. doi: 10.1016/j.eclinm.2020.100484
Lyle, R. C. (1981). A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 4, 483–492. doi: 10.1097/00004356-198112000-00001
Ma, D., Gulani, V., Seiberlich, N., Liu, K., Sunshine, J. L., Duerk, J. L., et al. (2013). Magnetic resonance fingerprinting. Nature 495, 187–192. doi: 10.1038/nature11971
Madhukumar, S., and Santhiyakumari, N. (2015). Evaluation of k-Means and fuzzy C-means segmentation on MR images of brain. Egyptian J. Radiol. Nuclear Med. 46, 475–479. doi: 10.1016/j.ejrnm.2015.02.008
Meyer, M. (2010). The rise of the knowledge broker. Sci. Commun. 32, 118–127. doi: 10.1177/1075547009359797
Mu, F., Hurley, D., Betts, K. A., Messali, A. J., Paschoalin, M., Kelley, C., et al. (2017). Real-world costs of ischemic stroke by discharge status. Curr. Med. Res. Opin. 33, 371–378. doi: 10.1080/03007995.2016.1257979
Murphy, R., Sackley, C. M., Miller, P., and Harwood, R. H. (2001). Effect of experience of severe stroke on subjective valuations of quality of life after stroke. J. Neurol. Neurosurg. Psychiatr. 70, 679–681. doi: 10.1136/jnnp.70.5.679
National Institute of Neurological Disorders and Stroke (2011). NIH stroke scale. Bethesda, Md.?: National Institute of Neurological Disorders and Stroke. Washington, DC: Dept. of Health and Human Services.
Nomura, E. M., Gratton, C., Visser, R. M., Kayser, A., Perez, F., and D’Esposito, M. (2010). Double dissociation of two cognitive control networks in patients with focal brain lesions. Proc. Natl. Acad. Sci. U.S.A. 107, 12017–12022. doi: 10.1073/pnas.1002431107
Ovbiagele, B., and Nguyen-Huynh, M. N. (2011). Stroke epidemiology: advancing our understanding of disease mechanism and therapy. Neurotherapeutics 8, 319–329. doi: 10.1007/s13311-011-0053-1
Ovbiagele, B., Goldstein, L. B., Higashida, R. T., Howard, V. J., Johnston, S. C., Khavjou, O. A., et al. (2013). Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association. Stroke 44, 2361–2375. doi: 10.1161/STR.0b013e31829734f2
Overdorp, E. J., Kessels, R. P., Claassen, J. A., and Oosterman, J. M. (2016). The Combined Effect of Neuropsychological and Neuropathological Deficits on Instrumental Activities of Daily Living in Older Adults: a Systematic Review. Neuropsychol. Rev. 26, 92–106. doi: 10.1007/s11065-015-9312-y
Park, H. J., and Friston, K. (2013). Structural and functional brain networks: from connections to cognition. Science 342:1238411. doi: 10.1126/science.1238411
Petersen, S. E., and Sporns, O. (2015). Brain Networks and Cognitive Architectures. Neuron 88, 207–219. doi: 10.1016/j.neuron.2015.09.027
Reitan, R. M. (1958). Validity of the Trail Making Test as an Indicator of Organic Brain Damage. Perceptual. Motor Skills 8, 271–276. doi: 10.2466/pms.1958.8.3.271
Roberts, P. S., Krishnan, S., Burns, S. P., Ouellette, D., and Pappadis, M. R. (2020). Inconsistent Classification of Mild Stroke and Implications on Health Services Delivery. Arch. Phys. Med. Rehabil. 101, 1243–1259. doi: 10.1016/j.apmr.2019.12.013
Rogers, A. T., Bai, G., Lavin, R. A., and Anderson, G. F. (2017). Higher Hospital Spending on Occupational Therapy Is Associated With Lower Readmission Rates. Med. Care Res. Rev. 74, 668–686. doi: 10.1177/1077558716666981
Rost, N. S., Bottle, A., Lee, J. M., Randall, M., Middleton, S., Shaw, L., et al. (2016). Stroke Severity Is a Crucial Predictor of Outcome: An International Prospective Validation Study. J. Am. Heart Assoc. 5:e002433. doi: 10.1161/JAHA.115.002433
Santisteban, L., Térémetz, M., Bleton, J. P., Baron, J. C., Maier, M. A., and Lindberg, P. G. (2016). Upper Limb Outcome Measures Used in Stroke Rehabilitation Studies: A Systematic Literature Review. PLoS One 11:e0154792.
Schlosser, R. (2000). [Detection of neurotransmitter interactions with PET and SPECT by pharmacological challenge paradigms]. Nervenarzt 71, 9–18. doi: 10.1007/s001150050002
Sensenbrenner, B., Rouaud, O., Graule-Petot, A., Guillemin, S., Piver, A., Giroud, M., et al. (2020). High Prevalence of Social Cognition Disorders and Mild Cognitive Impairment Long Term After Stroke. Alzheimer Dis. Assoc. Dis. 34, 72–78. doi: 10.1097/WAD.0000000000000355
Siegle, G. J., Ichikawa, N., and Steinhauer, S. (2008). Blink before and after you think: blinks occur prior to and following cognitive load indexed by pupillary responses. Psychophysiology 45, 679–687. doi: 10.1111/j.1469-8986.2008.00681.x
Silasi, G., and Murphy, T. H. (2014). Stroke and the connectome: how connectivity guides therapeutic intervention. Neuron 83, 1354–1368. doi: 10.1016/j.neuron.2014.08.052
Smith, A. (1973). Symbol Digit Modalities Test (SDMT), Manual. Los Angeles, CA: Western Psychological Services.
Spitzer, J., Tse, T., Baum, C. M., and Carey, L. M. (2011). Mild impairment of cognition impacts on activity participation after stroke in a community-dwelling Australian cohort. OTJR 31, S8–S15.
Spokoyny, I., Raman, R., Ernstrom, K., Khatri, P., Meyer, D. M., Hemmen, T. M., et al. (2015). Defining mild stroke: outcomes analysis of treated and untreated mild stroke patients. J. Stroke Cerebrovasc. Dis. 24, 1276–1281. doi: 10.1016/j.jstrokecerebrovasdis.2015.01.037
Sporns, O., and Zwi, J. D. (2004). The small world of the cerebral cortex. Neuroinformatics 2, 145–162. doi: 10.1385/NI:2:2:145
Sporns, O., Tononi, G., and Kotter, R. (2005). The human connectome: A structural description of the human brain. PLoS Comput. Biol. 1:e42. doi: 10.1371/journal.pcbi.0010042
Stephens, S., Kenny, R. A., Rowan, E., Kalaria, R. N., Bradbury, M., Pearce, R., et al. (2005). Association between mild vascular cognitive impairment and impaired activities of daily living in older stroke survivors without dementia. J. Am. Geriatr. Soc. 53, 103–107. doi: 10.1111/j.1532-5415.2005.53019.x
Su, C. Y., Wuang, Y. P., Lin, Y. H., and Su, J. H. (2015). The role of processing speed in post-stroke cognitive dysfunction. Arch. Clin. Neuropsychol. 30, 148–160. doi: 10.1093/arclin/acu057
Sun, J. H., Tan, L., and Yu, J. T. (2014). Post-stroke cognitive impairment: epidemiology, mechanisms and management. Ann. Transl. Med. 2:80.
Tellier, M., and Rochette, A. (2009). Falling through the cracks: a literature review to understand the reality of mild stroke survivors. Top. Stroke Rehabil. 16, 454–462. doi: 10.1310/tsr1606-454
Turken, A., Whitfield-Gabrieli, S., Bammer, R., Baldo, J. V., Dronkers, N. F., and Gabrieli, J. D. (2008). Cognitive processing speed and the structure of white matter pathways: convergent evidence from normal variation and lesion studies. Neuroimage 42, 1032–1044. doi: 10.1016/j.neuroimage.2008.03.057
van Meer, M. P., Otte, W. M., van der Marel, K., Nijboer, C. H., Kavelaars, A., van der Sprenkel, J. W., et al. (2012). Extent of bilateral neuronal network reorganization and functional recovery in relation to stroke severity. J. Neurosci. 32, 4495–4507. doi: 10.1523/JNEUROSCI.3662-11.2012
Versaci, M., Calcagno, S., and Morabito, F. C. (2015). Image Contrast Enhancement by Distances Among Points in Fuzzy Hyper-Cubes. Computer Analysis of Images and Patterns. Berlin: Springer International Publishing.
Wang, L., Yu, C., Chen, H., Qin, W., He, Y., Fan, F., et al. (2010). Dynamic functional reorganization of the motor execution network after stroke. Brain 133, 1224–1238. doi: 10.1093/brain/awq043
Weiss, L., Saklofske, D. H., Coalson, D. L., and Raiford, S. E. (2010). Theoretical, empirical and clinical foundations of the WAIS-IV index scores. WAIS IV Clin. Use Interp. 61–94. doi: 10.1016/B978-0-12-375035-8.10003-5
Wintermark, M., Sanelli, P. C., Albers, G. W., Bello, J. A., Derdeyn, C. P., Hetts, S. W., et al. (2013). Imaging recommendations for acute stroke and transient ischemic attack patients: a joint statement by the American Society of Neuroradiology, the American College of Radiology and the Society of NeuroInterventional Surgery. J. Am. Coll. Radiol. 10, 828–832. doi: 10.1016/j.jacr.2013.06.019
Wolf, T. J., and Rognstad, M. C. (2013). Changes in cognition following mild stroke. Neuropsychol. Rehabil. 23, 256–266. doi: 10.1080/09602011.2012.748672
Yaghi, S., Herber, C., Boehme, A. K., Andrews, H., Willey, J. Z., Rostanski, S. K., et al. (2017). The Association between Diffusion MRI-Defined Infarct Volume and NIHSS Score in Patients with Minor Acute Stroke. J. Neuroimaging 27, 388–391. doi: 10.1111/jon.12423
Yakhkind, A., McTaggart, R. A., Jayaraman, M. V., Siket, M. S., Silver, B., and Yaghi, S. (2016). Minor Stroke and Transient Ischemic Attack: Research and Practice. Front. Neurol. 7:86. doi: 10.3389/fneur.2016.00086
Keywords: stroke, neuroimaging, occupational therapy, neurorehabilitation, cognitive dysfunction, neurocognitive function, translational medical research, connectomics
Citation: Holguin JA, Margetis JL, Narayan A, Yoneoka GM and Irimia A (2022) Vascular Cognitive Impairment After Mild Stroke: Connectomic Insights, Neuroimaging, and Knowledge Translation. Front. Neurosci. 16:905979. doi: 10.3389/fnins.2022.905979
Received: 28 March 2022; Accepted: 20 June 2022;
Published: 07 July 2022.
Edited by:
Aleksandra Dagmara Kawala-Sterniuk, Opole University of Technology, PolandReviewed by:
Mario Versaci, Mediterranea University of Reggio Calabria, ItalyCopyright © 2022 Holguin, Margetis, Narayan, Yoneoka and Irimia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jess A. Holguin, amVzcy5ob2xndWluQG1lZC51c2MuZWR1; Andrei Irimia, aXJpbWlhQHVzYy5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.