
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Neurosci., 18 July 2022
Sec. Neurodegeneration
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.899597
This article is part of the Research TopicThe underlying relationship between sleep and neurodegenerative diseasesView all 9 articles
 Nijole Kazukauskiene1†
Nijole Kazukauskiene1† Naomi A. Fineberg2†
Naomi A. Fineberg2† Aurelija Podlipskyte1†
Aurelija Podlipskyte1† Adomas Bunevicius1†
Adomas Bunevicius1† Nicolás Francisco Narvaez Linares3†
Nicolás Francisco Narvaez Linares3† Marilou Poitras3†
Marilou Poitras3† Hélène Plamondon3†
Hélène Plamondon3† Aiste Pranckeviciene1†
Aiste Pranckeviciene1† Julija Gecaite-Stonciene1†
Julija Gecaite-Stonciene1† Narseta Mickuviene1†
Narseta Mickuviene1† Giedrius Varoneckas1†
Giedrius Varoneckas1† Julius Burkauskas1*†
Julius Burkauskas1*†Introduction: Our exploratory study aimed to determine whether obstructive sleep apnoea (OSA) could affect cognitive functioning in males with coronary artery disease (CAD), and whether such impact could be associated with changes in thyroid hormones and inflammatory marker regulation on cognitive functioning.
Method: We evaluated different endocrine and inflammatory biomarkers, including free triiodothyronine [fT3], free tetraiodothyronine [fT4], N-terminal pro-B-type natriuretic peptide [NT-pro-BNP], and high-sensitivity C-reactive protein [hs-CRP] serum levels in 328 males ( = 57 ± 10 years), undergoing cardiac rehabilitation after an acute coronary event. Participants underwent full-night polysomnography and were classified in mild/non-OSA (n = 253) and OSA (n = 75) according to an apnoea-hypopnoea index ≥ 15 event/h. Cognitive functioning testing included the Digit Span Test, Digit Symbol Test (DSST), and Trail Making Test. Analyses of variance assessed the impact of OSA on cognitive functioning and possible relationships of fT3/fT4, NT-pro-BNP and with hs-CRP on cognitive measures.
Results: Significant group (OSA, mild/non-OSA) × NT-pro-BNP (<157.0 vs. ≥157.0, ng/L) interactions were found for the DSST raw score (F(2,324) = 3.58, p = 0.014). Decomposition of interactions showed that the DSST scores of the OSA group with NT-pro-BNP ≥ 157.0 ng/L (M = 33.2; SD = 8.1) were significantly lower, p = 0.031, than those of the mild/non-OSA with NT-pro-BNP < 157.0 ng/L (M = 37.7; SD = 8.9).
Conclusion: These findings indicate that males with OSA and clinically elevated NT-pro-BNP levels experienced inferior psychomotor performance compared to those without OSA and reduced NT-pro-BNP levels.
Obstructive sleep apnoea (OSA) represents an independent risk factor for adverse cardiac outcomes and impaired cognitive functioning, especially in men (Zhang et al., 2020). Several unfavorable medical conditions have been associated with OSA, for example coronary artery disease (CAD), heart failure, atrial fibrillation, hypertension, stroke (Goudis and Ketikoglou, 2017; Li et al., 2018; Salman et al., 2020; Roderjan et al., 2022), metabolic dysfunction (Bonsignore et al., 2013), and neurocognitive impairment (Seda and Han, 2020). Risk factors for OSA include older age, being male, a family history of OSA, obesity and upper airway anatomical abnormalities (Tishler et al., 2003; Lindberg et al., 2017; Kumar et al., 2021). Data from young and middle-aged individuals show a relationship between OSA and poor cognitive performance, notably in attention, memory, and executive function (Bubu et al., 2020). In older adults, OSA is not associated with a specific type of cognitive impairment at cross-section; however, OSA is linked with the possible development of mild cognitive impairment or Alzheimer’s disease with symptomatic individuals who have a higher likelihood of associated disturbed sleep and cognitive impairment (Bubu et al., 2020).
A meta-analysis on addressing the impact of sleep disruption on inflammation processes, including changes in inflammatory cytokines [i.e., high-sensitivity C-reactive protein (hs-CRP)] found a strong relationship between these factors (Irwin et al., 2016). Indeed, numerous studies have supported inflammation induced by OSA to lead to damage of vascular endothelial cells, which can alter the form and function of arteries (Yu et al., 2018; Orrù et al., 2020; Maniaci et al., 2021). In turn, endothelial dysfunction resulting from such condition has been associated with various comorbidities such as cardiovascular disease, metabolic dysfunction, and most critically neurocognitive impairment (Daulatzai, 2015; Song et al., 2015). Alongside the changes mentioned above, increased concentrations of N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) and hs-CRP commonly observed in individuals with CAD have been associated with impaired cognitive functioning and unfavorable CAD prognosis (Brozaitiene et al., 2016; Burkauskas et al., 2017).
Furthermore, OSA also represents a risk factor for changes in thyroid hormone secretion, with associated reduced concentrations of serum free triiodothyronine (fT3) and free tetraiodothyronine (fT4) themselves increasing the risk of developing CAD (Burkauskas et al., 2018). Examining thyroid function in N = 156 subjects suspected to experience OSA, Takeuchi et al. (2015) found a significant association between the mean apnoea duration and thyroid-stimulating hormone (TSH) secretion.
The consequence of OSA on the endocrine system appears to be mediated mainly by intermittent hypoxaemia, sympathetic activation, elevated blood pressure and increased inflammation and oxidative stress (Lavrentaki et al., 2019). The thyroid hormone is a major physiological regulator of brain development and function (Bernal and Nunez, 1995). Notably, current studies indicate that thyroid hormones have a unique role in the development and functioning of brain regions regulating mood and cognition (Burkauskas et al., 2020; Przybylak et al., 2021).
Studies have indicated a possible association between OSA and hypothyroidism, but the significance of thyroid function screening in individuals with OSA has been controversial. Additionally, while the effect of an interaction between OSA and such hormonal changes on cognitive function have been proposed (Barletta et al., 2019), such contention remains to be thoroughly investigated in a clinical setting.
Therefore, our exploratory study aimed to determine whether OSA interacting with fT3/fT4, NT-pro-BNP and hs-CRP affects specific aspects of cognitive functioning in males with CAD.
From January 2014 to December 2019, we invited N = 400 males with CAD to participate in this study. All the participants were part of a rehabilitation program at the hospital Palangos Klinika within 7 days after treatment for acute coronary syndrome [ACS, such as myocardial infarction (MI) or angina pectoris (AP)]. Our inclusion criteria were: (a) confirmed CAD diagnosis and recent ACS as identified by a study cardiologist; (b) no history of arrhythmic disorder and/or implantation of a cardioverter defibrillator; (c) comprehension of Lithuanian language; (d) aged 18–80. Our exclusion criteria included: (a) unstable cardiovascular condition (n = 32); (b) severe comorbidities (e.g., kidney failure, musculoskeletal disease) (n = 25); and (c) unwillingness to participate in the study (n = 15). Thus, the final sample consisted of N = 328 males with CAD (mean age 57 ± 10 years, range 33–80). According to the existing guidelines, all participants were subjected to standard evaluation and treatment for the secondary prevention of CAD (Gibbons et al., 2002; Piepoli et al., 2010; Fletcher et al., 2013; O’Gara et al., 2013).
Within 2 days of admission to the rehabilitation program and after providing written consent, all study participants were evaluated for clinical factors [i.e., New York Heart Association (NYHA) functional class, history of ACS, and angina pectoris class], thyroid hormones and other biomarkers (fT3, fT4, NT-pro-BNP, and hs-CRP) as well as demographic information (i.e., age, education, and marital status).
Cognitive functioning testing included the Digit Span Test (DST; Wechsler, 1981), Digit Symbol Test (DSST; Wechsler, 1981), and Trail Making Test Part A (TMTA; Strauss et al., 2006), measuring auditory attention, psychomotor performance and perceptual speed, respectively. These tests were chosen based on the recommendation provided by the National Institute of Neurological Disorders and Stroke-Canadian Stroke Network guidelines for short cognitive testing (Hachinski et al., 2006). They all have been previously validated and used in Lithuania (Bunevicius et al., 1999; Burkauskas et al., 2008). This particular testing battery has also proven to identify cognitive vulnerabilities in individuals with CAD (Burkauskas et al., 2018). Raw scores of each test were converted to a unified T-scores adjusted for age and education level according to the norms provided for a specific testing battery.
Within 3 days, participants underwent full-night polysomnography and were classified as mild/non-OSA (n = 253) and OSA (n = 75) according to an apnoea-hypopnoea index (AHI) ≥ 15 event/h (3% of desaturation or arousal).
Informed consent was obtained. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. The Kaunas Regional Biomedical Research Ethics Committee approved the study protocol (Protocol No. BE-2-21; P1-38/2007; P2-38/2007).
The digit span test (DST) was used to measure participants’ auditory working memory (Wechsler, 1981). The test is divided into two parts: (a) participants are required to repeat numbers using the same numerical order that was previously presented to them; and (b) participants have to repeat digits in reversed order. The results of the DST represent two possible cognitive outcomes with scores ranging from 0 to 14. Higher scores on the first part represent better auditory rehearsal, while higher scores in the second part represent better auditory working memory.
The digit symbol test (DSST; Wechsler, 1981) examines an individual’s psychomotor ability, speed visual-motor coordination and incidental learning. In the first part of this test, participants must quickly assign the correct symbol to a random digit based on the code provided on a separate table. Scores of the test range from 0 to 93. Higher scores on the first part represent better psychomotor performance. On the second part, the code table is no longer provided for participants, and they have to recall which number matches each symbol. The number of pairs correctly recalled is used as a measure of incidental learning.
The main cognitive function measured with the trail making test- part A (TMTA; Strauss et al., 2006) is perceptual speed. In the TMTA version, the participant has to connect randomly displayed numbers in numerical order. Time competition is essential for this task; the faster, the better.
Overnight fully attended polysomnography monitoring was performed with the “Alice 4” polysomnography System (Respironics Inc., Marietta, GA, United States) in the sleep laboratory using standard recording techniques according to the American Academy of Sleep Medicine and precise protocol of polysomnography monitoring (Iber, 2007). Intake of sedative medication was not allowed 48 h before the investigation. Airflow was monitored using a thermistor placed at the nose and mouth, and arterial oxygen saturation (SaO2) was recorded continuously with a pulse oximeter. Apnoea was defined as the disappearance of airflow for over 10 s; hypopnoea was defined as a ≥ 50% decrease in airflow lasting for >10 s associated with arousal or a ≥ 3% decrease in SaO2 from the baseline level. All forms of sleep-disordered breathing were noted, and apnoeas were classified as obstructive, central or mixed where the combination was seen. An OSA is a ≥ 10 s pause in respiration associated with ongoing ventilatory effort. A central apnoea is a ≥ 10 s pause in ventilation with no associated respiratory effort (Iber, 2007; Somers et al., 2008). A central apnoea is particularly common among individuals with heart failure or a stroke (Somers et al., 2008). The most common type of sleep apnoea is OSA, and much of the pathophysiologic understanding of sleep apnoeas relies on studies of OSA (Somers et al., 2008). In our study, the influence of central and obstructive events was not separately analyzed.
The AHI is the most commonly used characteristic of sleep apnoea. Although sleep apnoea syndrome includes both, a polysomnography abnormality and symptoms, its severity is often defined by AHI alone. The AHI was calculated as the total number of apnoea and hypopnoea episodes per hour of sleep. According to the American Academy of Sleep Medicine criteria (Iber, 2007), sleep apnoea was defined with usual clinical AHI thresholds: no sleep disordered breating, <5 event/h; mild, ≥5 to <15 event/h; moderate, ≥15 to <30 event/h; and severe, ≥30 event/h. We used different cut-off levels of AHI to improve comparability with earlier studies on sleep apnoea for adapting a definition of mild-to-severe (AHI ≥ 5) or moderate-to-severe (AHI ≥ 15) sleep apnoea.
All participants had a blood sample collected on the second day after admission to the rehabilitation clinic. Venous blood samples were drawn after a minimum of 12 h overnight fast to evaluate thyroid hormones, NT-pro-BNP and hs-CRP concentrations. Blood was centrifuged, and serum was frozen at −70°C. Serum concentrations of fT3 and fT4 were analyzed using radioimmunoassay kit RIA (R-EW-125, Belgium). Normal fT3 concentrations range from 2.0 to 4.0 pg/mL; fT4, from 7.0 to 17.0 pg/mL. The serum NT-pro-BNP concentrations were determined using a radio-immunoassay method (Roche Cobas analyser, Roche Diagnostics, Switzerland). The normal serum concentration of NT-pro-BNP is considered to be <157 ng/L (Brozaitiene et al., 2016). Serum hs-CRP concentration was assessed using the chemiluminescent immunoassay method (Beckman Coulter Unicel DXC 600) with normal values of ≤0.3 mg/dL.
We performed statistical analysis using the Statistical Package for Social Sciences, SPSS Statistics for Windows, Version 22.0.0.0 (IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp). Data is expressed as a mean ± standard deviation (SD) for continuous variables, as a number (percentage) for qualitative variables, and as medians (25th–75th percentiles) for variables with non-normal distribution. The variable distribution of similarity to normal was assessed visually and using the Kolmogorov–Smirnov test. The data characteristics were compared between groups with OSA and without OSA were using Fisher’s χ2 test, for the parametric two-tailed Student’s t-test test or nonparametric Mann–Whitney U test. Cognitive test scores were converted into demographically adjusted T-scores based on age and education (Joy et al., 2000; Tombaugh, 2004). T-scores are normalized to have an average of 50 and a standard deviation of 10.
Several analyses of variance (ANOVA) were performed on cognitive functioning for (OSA vs. mild/non-OSA) group interaction with fT3/fT4 (≥0.206 vs. <0.206), NT-pro-BNP (<157.0 vs. ≥157.0, ng/L) and with hs-CRP (<0.39 vs. ≥0.39, mg/dL)(Brozaitiene et al., 2016). We used Benjamini-Hochberg adjustment for multiple comparisons in the cognitive function domain, setting the critical value for a false discovery rate at 0.15.
Baseline information on sociodemographic characteristics of the study participants are presented in Table 1, separated according to OSA status. In brief, the mean participants’ age was 57 ± 10, and n = 215 (65.5%) had hypertension. In total, n = 254 (49.0%) participants experienced an acute MI, n = 257 (78.0%) had II NYHA functional class, and the remaining n = 34 (10.0%) were within the III NYHA functional class. No subjects were classified as having IV NYHA functional class. Participants (N = 328) were divided into an OSA group (n = 75) and a non-OSA group (n = 253). Participants with OSA were significantly older (p = 0.002; d = 0.393, had a higher body mass index (p = 0.001; d = 0.487), and a higher number had hypertension (p = 0.017, V = 0.133; see Table 1). The ratio fT3/fT4 was higher in individuals with CAD and OSA (p = 0.001; d = 0.372). Furthermore, individuals with CAD and OSA had lower scores in the psychomotor speed (DSST score; p = 0.011; d = 0.359) domain.
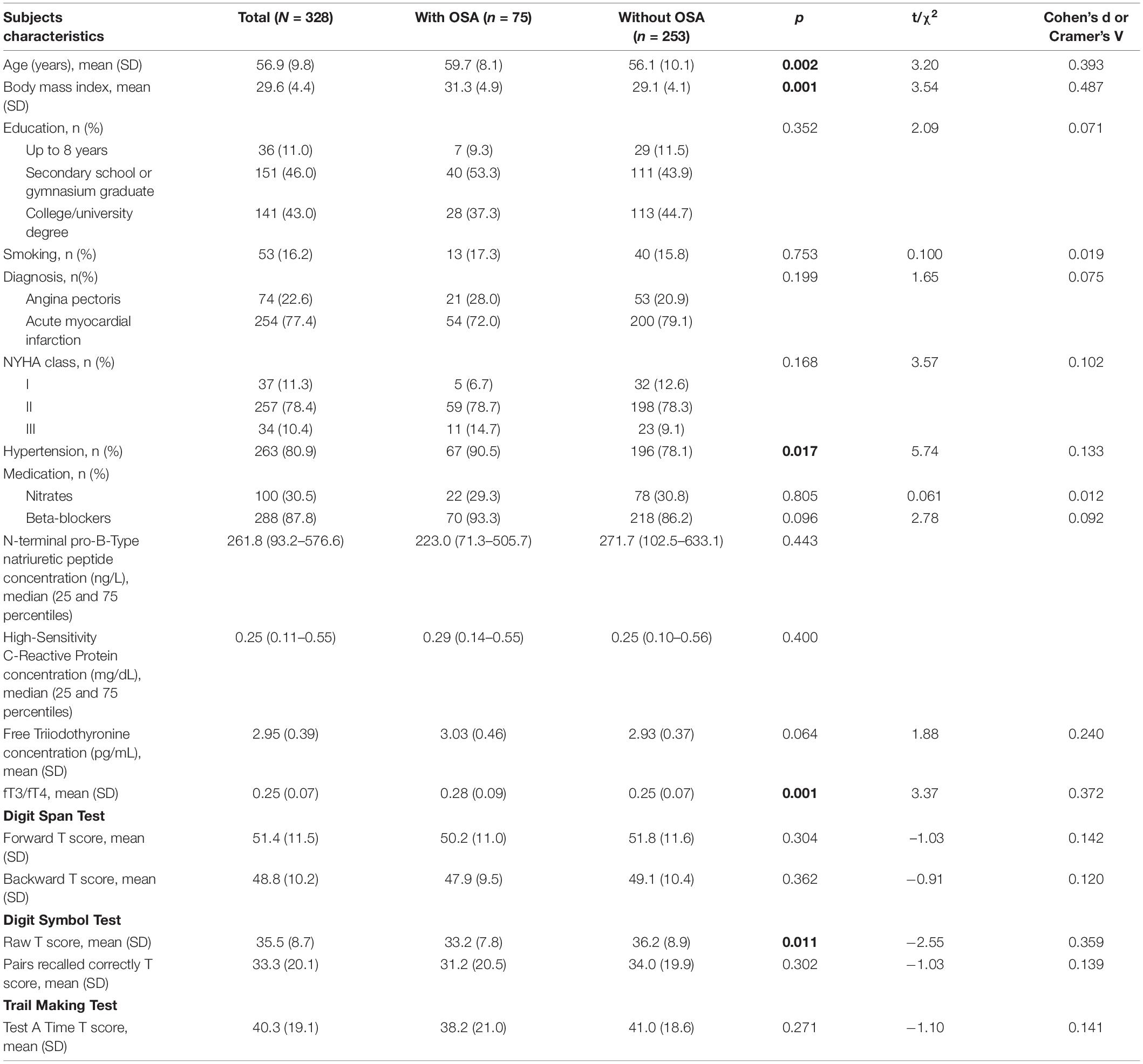
Table 1. Characteristics of the sample (N = 328) and descriptive statistics by presence of obstructive sleep apnoea (OSA).
Univariate ANOVA was used to compare groups’ differences of specific aspects of cognitive functioning. As shown in Table 2, after Benjamini-Hochberg correction significant group (OSA, mild/non-OSA) × NT-pro-BNP (<157.0 vs. ≥157.0 ng/L) interactions were found for the DSST raw score (F(3,324) = 3.58, p = 0.014). Decomposition of interactions showed that DSST score of the OSA group with NT-pro-BNP ≥ 157.0 ng/L (M = 33.2; SD = 8.1) were significantly lower (p = 0.031), than those of the mild/non-OSA with NT-pro-BNP < 157.0 ng/L (M = 37.7; SD = 8.9).
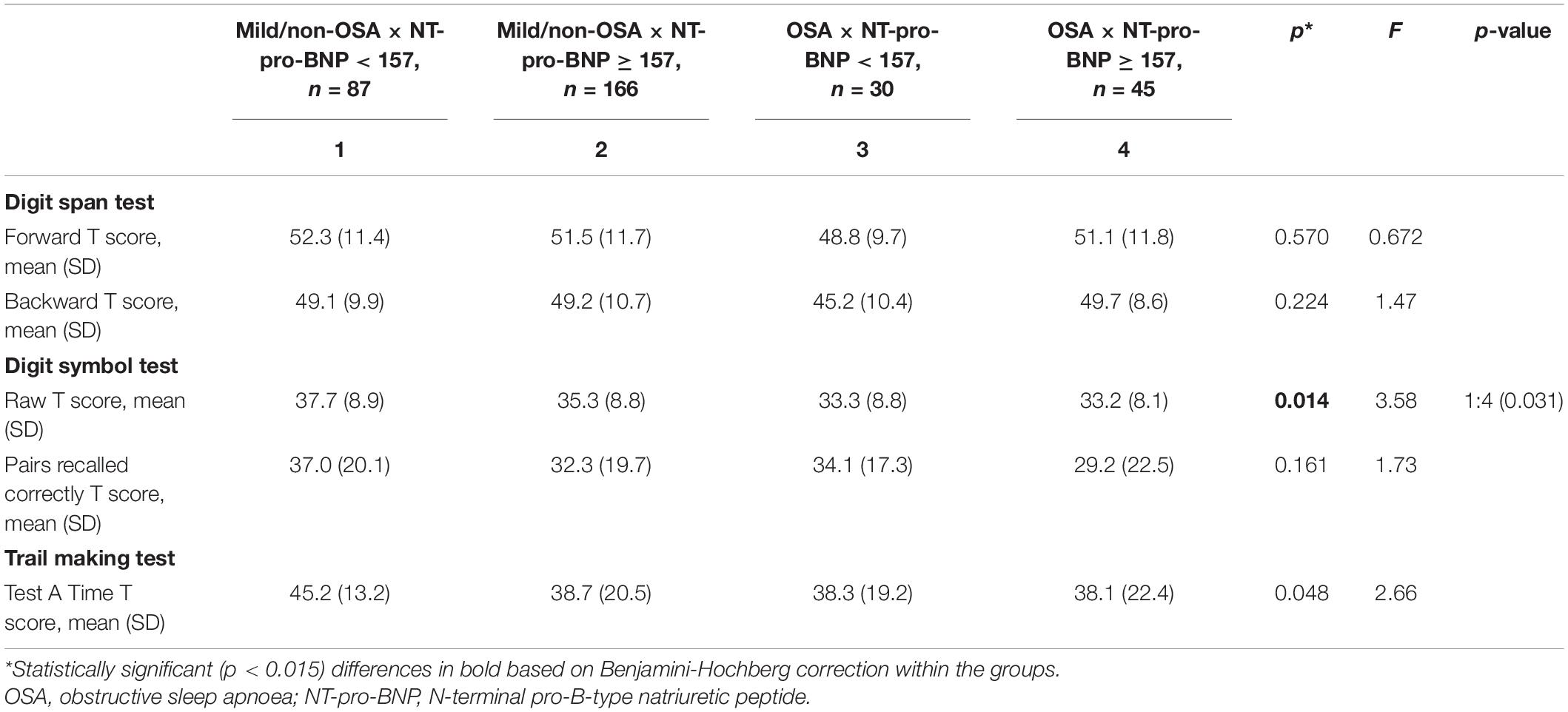
Table 2. Means differences of the cognitive functioning in the four groups stratified according to the presence of obstructive sleep apnoea and the level of NT-pro-BNP (high vs. low).
We found a tendency for group (OSA, mild/non-OSA) × hs-CRP (<0.39 vs. ≥0.39, mg/dL) interaction with the DSST raw score (F(3,323) = 2.93, p = 0.034; see Table 3).
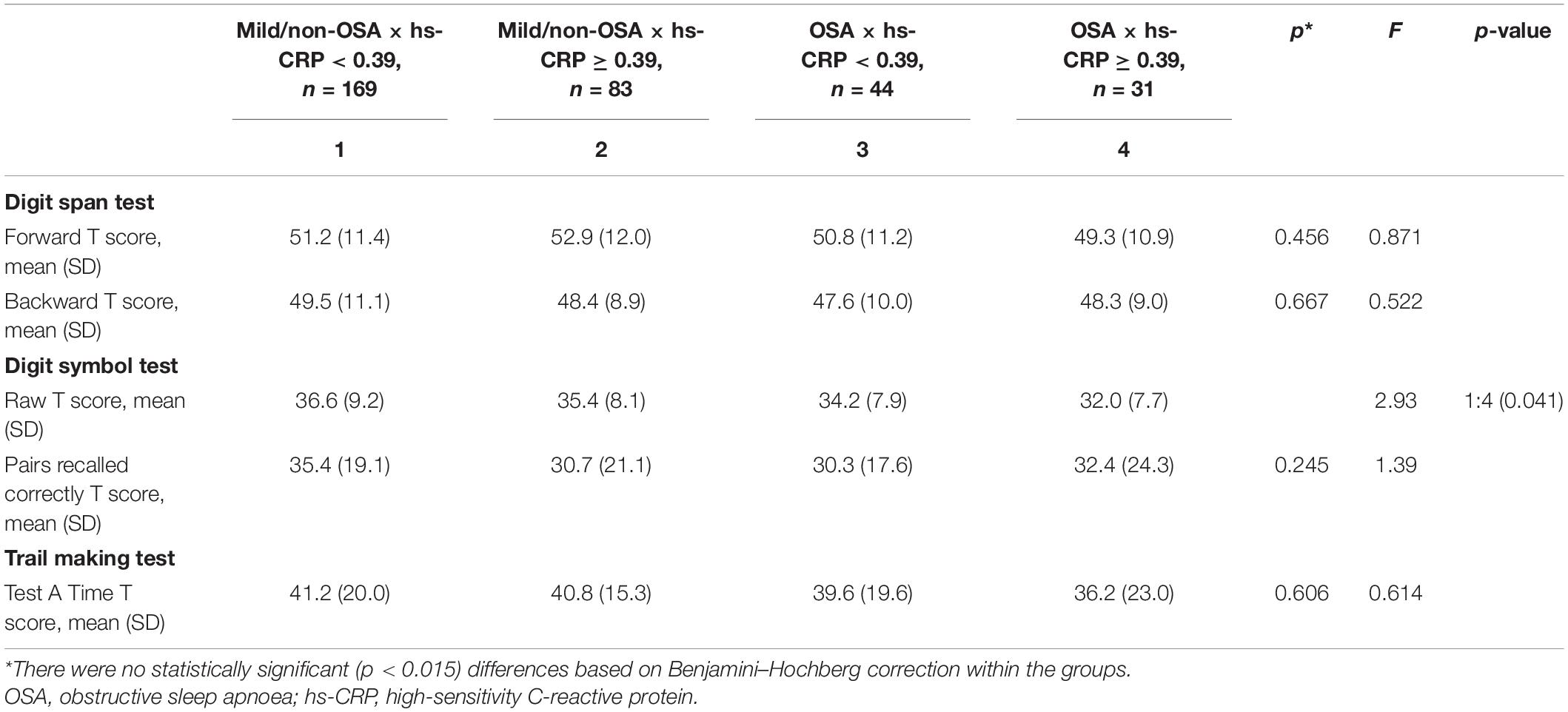
Table 3. Means differences of the cognitive functioning in the four groups stratified according to the presence of obstructive sleep apnoea and the level of hs-CRP (high vs. low).
As shown in Table 4, there were no statistically significant differences based on Benjamini-Hochberg correction within the groups.
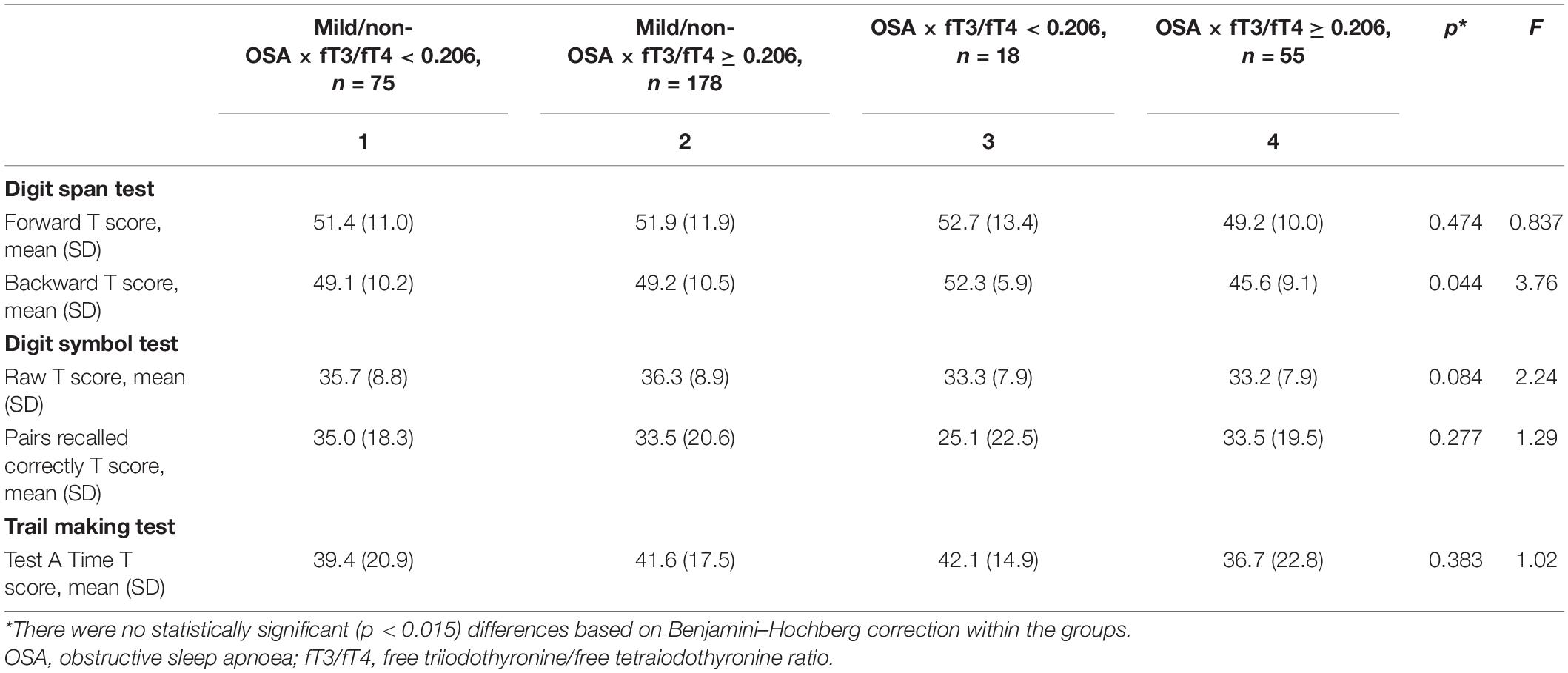
Table 4. Means differences of the cognitive functioning in the four groups stratified according to the presence of obstructive sleep apnoea and the level of fT3/fT4 (high vs. low).
To our knowledge, this exploratory study is the first to identify whether OSA and its interaction with fT3/fT4, NT-pro-BNP and hs-CRP affect specific aspects of cognitive functioning. Our results showed an interaction between OSA and NT-pro-BNP, associated with specific features of cognitive functioning problems in males with CAD. In contrast, the contribution of fT3/fT4 and hs-CRP to specific aspects of cognitive functioning in participants experiencing OSA was not readily apparent.
A recent review from our group supported associations between discrete hormones and biomarkers and impairments in cognitive function in individuals with established CAD (Burkauskas et al., 2018). The most widely studied predictor of long-term outcomes in individuals with CAD having experienced ACS is NT-pro-BNP (Brozaitiene et al., 2016). Other studies have shown higher NT-pro-BNP serum concentrations associated with frequent apnoea or hypoxemia in individuals with sleep apnoea (Strehmel et al., 2016). However, a study by Cifçi et al. (2010) with n = 33 consecutive individuals with OSA did not detect any significant difference between the severity of OSA and serum NT-pro-BNP levels (Cifçi et al., 2010). A review addressing biomarkers of cardiovascular stress supported significant associations between NT-pro-BNP and the presence and severity of OSA, although data remained varied and conflicting (Maeder et al., 2016). In our study, significantly elevated NT-pro-BNP levels in individuals with OSA could support NT-pro-BNP’s role as endogenous marker of heart failure strongly associated with changes in cognitive functioning. Consistent with this, our earlier study found NT-pro-BNP to be negatively related to perceptual speed, independently of clinical risk factors and depressive symptoms in n = 278 individuals with CAD (Burkauskas et al., 2017). In contrast, other studies have considered multiple specific cognitive domains to be affected by OSA (Patel and Chong, 2021). Together, these findings point to NT-pro-BNP as a valuable marker in further elucidating causal factors associated with elevated cardiovascular risk in individuals with OSA.
Numerous studies have also supported serum biomarkers related to inflammation, such as hs-CRP, to be activated in individuals with OSA (Stanek and Brożyna-Tkaczyk, 2021). Inflammation and OSA are strongly related and linked to vascular morbidity (Rocchi et al., 2022). Notably, the observational study by Huang et al. (2016) suggested that elevated cytokines such as hs-CRP, are related to impaired inattention and vigilance abilities in children with OSA. In contrast, we did not find a relationship between OSA and hs-CRP mediating specific cognitive functioning aspects.
Whereas reduced fT3 concentrations have been associated with worse perceptual speed and inferior efficacy in completing cognitive tasks in individuals with stable CAD and endured ACS (Burkauskas et al., 2017), our study did not indicate OSA-related changes in fT3/fT4 concentrations to affect the investigated aspects of cognitive functioning.
Taken together, our findings support effects of OSA on certain areas of cognitive functioning performance, independently of other sleep disturbances, which may help explain the higher cardiovascular risk associated with sleep-disordered breathing, particularly in males (Marin et al., 2005). Future studies assessing sex-specific effects of OSA on cognitive functioning may offer essential insight on this research topic.
The present study has some strengths and limitations. The strengths of our study include well-validated tests for evaluating culturally free cognitive functioning and an acceptable sample size. Another unique aspect of the current study is the number of biomarkers analyzed. A cross-sectional design is a major limitation of our study, which prevented us from evaluating a causal relationship of fT3, fT4, NT-pro-BNP, and hs-CRP concentrations with cognitive functioning. The inclusion of individuals undergoing cardiac rehabilitation limits the generalizability of our findings to individuals with acute CAD. Also, our findings should not be applied to individuals with CAD above the age of 80, individuals with past cerebrovascular accidents, or individuals with severe somatic illnesses, as these were the study exclusion criteria. We also have to acknowldege that dividing groups by clinical norms of various biomarkers (namely fT3, fT4, NT-pro-BNP, and hs-CRP) might have created uneven distribution of study participants in each group, resulting in some of the groups being underpowered to detect changes. Thus, these results should be treated as preliminary, and have to be replicated in a larger sample size of individuals with CAD.
Despite these limitations, this is the first description of cognitive impairments in patients with OSA and its interaction with biomarkers. More specifically, it would be interesting for future studies to measure specific aspects of cognitive functioning tests a few months after the ACS. Furthermore, by directly addressing the possible underlying causes for the pathological changes seen in patients with OSA, it would also be interesting to assess the effect of continuous positive airway pressure therapy on the variation of biomarkers as well as on the progression of the cognitive function in the medium-long term follow-up. Understanding of other neurocognitive effects of fT3, fT4 NT-pro-BNP and hs-CRP should be elucidated in future studies employing other focused and specific cognitive functioning assessment probes because such knowledge could facilitate the identification of novel therapeutic strategies.
Our results indicate that males with OSA who have clinically elevated NT-pro-BNP levels experienced inferior psychomotor performance, as measured by the DSST, compared to those without OSA and with lower NT-pro-BNP levels. These findings reflect a probable interaction between OSA and NT-pro-BNP, increasing the risk of producing cognitive functioning problems. However, the interaction effect must be confirmed in future studies with larger sample sizes. Our results underscore the importance of referring individuals with CAD and OSA for a comprehensive neuropsychological assessment when a high NT-pro-BNP level is suspected, considering that CAD individuals are more at risk of developing cognitive impairment. Cognitive functioning was not impacted by interaction between OSA and fT3/fT4 as well as hs-CRP.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study involving human participants were reviewed and approved by the Kaunas Regional Biomedical Research Ethics Committee which approved the study protocol (Protocol Nos. BE-2-21; P1-38/2007; P2-38/2007). All participants provided their written informed consent to enter this study.
JB, NM, and GV conceived and designed the study. JG-S, JB, and NK were responsible for the data collection and evaluation. AuP performed the statistical analyses. NK prepared the manuscript. NAF, NFNL, AB, NL, MP, HP, and AiP provided the critical revision and read and approved the final manuscript. All authors contributed to the article and approved the submitted version.
This project was funded by the European Social Fund under the No 09.3.3-LMT-K-712-19-0127 “Development of Competences of Scientists, other Researchers and Students through Practical Research Activities” measure. HP’s research work was supported by a Discovery grant from the Natural Sciences and Engineering Research Council (NSERC) of Canada (RG203596-13).
JG-S works as a consultant at FACITtrans. JB works as a consultant at Cronos. NF reports personal fees from Sun, Otsuka, Abbott, Lundbeck, Taylor and Francis, Oxford University Press, grants and non-financial support from ECNP, Shire, personal fees and non-financial support from College of Mental Health Pharmacists, nonfinancial support from RANZCP, Sun, RCPsych, CINP, Int Society of Behavioral Addiction, WHO, International College of Obsessive Compulsive Spectrum Disorders, BAP, Janssen, Int Forum of Mood and Anxiety Disorders, Wiley, grants from MRC, Wellcome, other from MHRA, outside the submitted work; and non-financial support from the EU COST Action.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Barletta, P., Abreu, A. R., Ramos, A. R., Dib, S. I., Torre, C., and Chediak, A. D. (2019). Role of obstructive sleep apnea in cognitive impairment. Int. J. Head Neck Surg. 10, 57–61. doi: 10.5005/jp-journals-10001-1373
Bernal, J., and Nunez, J. (1995). Thyroid hormones and brain development. Eur. J. Endocrinol. 133, 390–398. doi: 10.1530/eje.0.1330390
Bonsignore, M. R., Borel, A. L., Machan, E., and Grunstein, R. (2013). Sleep apnoea and metabolic dysfunction. Eur. Respir. Rev. 22, 353–364. doi: 10.1183/09059180.00003413
Brozaitiene, J., Mickuviene, N., Podlipskyte, A., Burkauskas, J., and Bunevicius, R. (2016). Relationship and prognostic importance of thyroid hormone and N-terminal pro-B-Type natriuretic peptide for patients after acute coronary syndromes: a longitudinal observational study. BMC Cardiovasc. Disord. 16:45. doi: 10.1186/s12872-016-0226-2
Bubu, O. M., Andrade, A. G., Umasabor-Bubu, O. Q., Hogan, M. M., Turner, A. D., de Leon, M. J., et al. (2020). Obstructive sleep apnea, cognition and Alzheimer’s disease: a systematic review integrating three decades of multidisciplinary research. Sleep Med. Rev. 50:101250. doi: 10.1016/j.smrv.2019.101250
Bunevicius, R., Kazanavicius, G., Zalinkevicius, R., and Prange, A. J. Jr. (1999). Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidism. N. Engl. J. Med. 340, 424–429. doi: 10.1056/NEJM199902113400603
Burkauskas, J., Bunevicius, A., Brozaitiene, J., Neverauskas, J., Lang, P., Duwors, R., et al. (2017). Cognitive functioning in coronary artery disease patients: associations with thyroid hormones, N-Terminal Pro-B-Type natriuretic peptide and high-sensitivity C-reactive protein. Arch. Clin. Neuropsychol. 32, 245–251. doi: 10.1093/arclin/acx004
Burkauskas, J., Bunevicius, A., Brozaitiene, J., Neverauskas, J., Fineberg, N. A., Wellsted, D., et al. (2008). Exploring cognitive concomitants of mental fatigue in patients with coronary artery disease. Neuropsychobiology. 76, 151–160. doi: 10.1159/000489713
Burkauskas, J., Lang, P., Bunevicius, A., Neverauskas, J., Buciute-Jankauskiene, M., and Mickuviene, N. (2018). Cognitive function in patients with coronary artery disease: a literature review. J. Int. Med. Res. 46, 4019–4031. doi: 10.1177/0300060517751452
Burkauskas, J., Pranckeviciene, A., and Bunevicius, A. (2020). Thyroid Hormones, Brain, and Heart, Thyroid and Heart: A Comprehensive Translational Essay. Cham: Springer International Publishing, 339–360. doi: 10.1007/978-3-030-36871-5_25
Cifçi, N., Uyar, M., Elbek, O., Süyür, H., and Ekinci, E. (2010). Impact of CPAP treatment on cardiac biomarkers and pro-BNP in obstructive sleep apnea syndrome. Sleep Breath. 14, 241–244. doi: 10.1007/s11325-009-0306-y
Daulatzai, M. A. (2015). Evidence of neurodegeneration in obstructive sleep apnea: Relationship between obstructive sleep apnea and cognitive dysfunction in the elderly. J. Neurosci. Res. 93, 1778–1794. doi: 10.1002/jnr.23634
Fletcher, G. F., Ades, P. A., Kligfield, P., Arena, R., Balady, G. J., Bittner, V. A., et al. (2013). Exercise standards for testing and training: a scientific statement from the american heart association. Circulation 128, 873–934. doi: 10.1161/CIR.0b013e31829b5b44
Gibbons, R. J., Balady, G. J., Bricker, J. T., Chaitman, B. R., Fletcher, G. F., Froelicher, V. F., et al. (2002). ACC/AHA 2002 guideline update for exercise testing: summary article. A report of the american college of cardiology/american heart association task force on practice guidelines (committee to update the 1997 exercise testing guidelines). J. Am. Coll. Cardiol. 40, 1531–1540. doi: 10.1016/S0735-1097(02)02164-2
Goudis, C. A., and Ketikoglou, D. G. (2017). Obstructive sleep and atrial fibrillation: pathophysiological mechanisms and therapeutic implications. Int. J. Cardiol. 230, 293–300. doi: 10.1016/j.ijcard.2016.12.120
Hachinski, V., Iadecola, C., Petersen, R. C., Breteler, M. M., Nyenhuis, D. L., Black, S. E., et al. (2006). National institute of neurological disorders and stroke-canadian stroke network vascular cognitive impairment harmonization standards. Stroke 37, 2220–2241. doi: 10.1161/01.STR.0000237236.88823.47
Huang, Y. S., Guilleminault, C., Hwang, F. M., Cheng, C., Lin, C. H., Li, H. Y., et al. (2016). Inflammatory cytokines in pediatric obstructive sleep apnea. Medicine 95, e4944. doi: 10.1097/MD.0000000000004944
Iber, C. (2007). The AASM Manual For The Scoring Of Sleep And Associated Events: Rules. Terminology And Technical Specification. Darien, IL: American Academy of Sleep Medicine.
Irwin, M. R., Olmstead, R., and Carroll, J. E. (2016). Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol. Psychiatry 80, 40–52. doi: 10.1016/j.biopsych.2015.05.014
Joy, S., Fein, D., Kaplan, E., and Freedman, M. (2000). Speed and memory in WAIS-R-NI digit symbol performance among healthy older adults. J. Int. Neuropsychol. Soc. 6, 770–780. doi: 10.1017/s1355617700677044
Kumar, S., Anton, A., and D’Ambrosio, C. M. (2021). Sex differences in obstructive sleep apnea. Clinics Chest Med. 42, 417–425. doi: 10.1016/j.ccm.2021.04.004
Lavrentaki, A., Ali, A., Cooper, B. G., and Tahrani, A. A. (2019). Mechanisms of endocrinology: mechanisms of disease: the endocrinology of obstructive sleep apnoea. Eur. J. Endocrinol. 180, R91–R125. doi: 10.1530/EJE-18-0411
Li, T., Chen, Y., Gua, C., and Wu, B. (2018). Elevated oxidative stress and inflammation in hypothalamic paraventricular nucleus are associated with sympathetic excitation and hypertension in rats exposed to chronic intermittent hypoxia. Front. Physiol. 9:840. doi: 10.3389/fphys.2018.00840
Lindberg, E., Benediktsdottir, B., Franklin, K. A., Holm, M., Johannessen, A., Jögi, R., et al. (2017). Women with symptoms of sleep-disordered breathing are less likely to be diagnosed and treated for sleep apnea than men. Sleep Med. 35, 17–22. doi: 10.1016/j.sleep.2017.02.032
Maeder, M. T., Mueller, C., Schoch, O. D., Ammann, P., and Rickli, H. (2016). Biomarkers of cardiovascular stress in obstructive sleep apnea. Clinica Chim. Acta 460, 152–163. doi: 10.1016/j.cca.2016.06.046
Maniaci, A., Iannella, G., Cocuzza, S., Vicini, C., Magliulo, G., Ferlito, S., et al. (2021). Oxidative stress and inflammation biomarker expression in obstructive sleep apnea patients. J. Clin. Med. 10:277. doi: 10.3390/jcm10020277
Marin, J. M., Carrizo, S. J., Vicente, E., and Agusti, A. G. (2005). Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet (London, England) 365, 1046–1053. doi: 10.1016/S0140-6736(05)71141-7
O’Gara, P. T., Kushner, F. G., Ascheim, D. D., Casey, D. E. Jr., Chung, M. K., de Lemos, J. A., et al. (2013). ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the american college of cardiology foundation/american heart association task force on practice guidelines: developed in collaboration with the american college of emergency physicians and society for cardiovascular angiography and interventions. Catheter. Cardiovasc. Interv. 82, E1–E27. doi: 10.1002/ccd.24776
Orrù, G., Storari, M., Scano, A., Piras, V., Taibi, R., and Viscuso, D. (2020). Obstructive Sleep Apnea, oxidative stress, inflammation and endothelial dysfunction an overview of predictive laboratory biomarkers. Eur. Rev. Med. Pharmacol. Sci. 24, 6939–6948. doi: 10.26355/eurrev_202006_21685
Patel, A., and Chong, D. J. (2021). Obstructive sleep apnea: cognitive outcomes. Clinics Geriatr. Med. 37, 457–467. doi: 10.1016/j.cger.2021.04.007
Piepoli, M. F., Corra, U., Benzer, W., Bjarnason-Wehrens, B., Dendale, P., Gaita, D., et al. (2010). Secondary prevention through cardiac rehabilitation: from knowledge to implementation. A position paper from the cardiac rehabilitation section of the european association of cardiovascular prevention and rehabilitation. Eur. J. Cardiovasc. Prev. Rehabil. 17, 1–17. doi: 10.1097/HJR.0b013e3283313592
Przybylak, M., Grabowski, J., and Bidzan, L. (2021). Cognitive functions and thyroid hormones secretion disorders. Psychiatr. Polska 55, 309–321. doi: 10.12740/PP/112470
Rocchi, C., Valentina, C., Totaro, V., Broggi, S., Lattanzi, S., Viticchi, G., et al. (2022). Inflammation markers in moderate and severe obstructive sleep apnea: the influence of sex. Sleep Breath. 1–7. doi: 10.1007/s11325-021-02537-3
Roderjan, C. N., de Hollanda Cavalcanti, A., and Cortez, A. F. (2022). Association between arterial stiffness and sleep apnoea in patients with resistant hypertension. J. Hum. Hypertens. 1–7.
Salman, L. A., Shulman, R., and Cohen, J. B. (2020). Obstructive sleep apnea, hypertension, and cardiovascular risk: epidemiology, pathophysiology, and management. Curr. Cardiol. Rep. 22:6. doi: 10.1007/s11886-020-1257-y
Seda, G., and Han, T. S. (2020). Effect of obstructive sleep apnea on neurocognitive performance. Sleep Med. Clinics 15, 77–85.
Somers, V. K., White, D. P., Amin, R., Abraham, W. T., Costa, F., Culebras, A., et al. (2008). Sleep apnea and cardiovascular disease: an american heart association/american college of cardiology foundation scientific statement from the american heart association council for high blood pressure research professional education committee, council on clinical cardiology, stroke council, and council on cardiovascular nursing. in collaboration with the national heart, lung, and blood institute national center on sleep disorders research (National Institutes of Health). Circulation 118, 1080–1111. doi: 10.1161/CIRCULATIONAHA.107.189375
Song, D., Fang, G., Greenberg, H., and Liu, S. F. (2015). Chronic intermittent hypoxia exposure-induced atherosclerosis: a brief review. Immunol. Res. 63, 121–130. doi: 10.1007/s12026-015-8703-8
Stanek, A., and Brożyna-Tkaczyk, K. (2021). Oxidative stress markers among obstructive sleep apnea patients. Oxid. Med. Cell Longev. 2021:9681595.
Strauss, E., Sherman, E., and Spreen, O. (2006). A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary. New York, NY: Oxford University Press.
Strehmel, R., Valo, M., and Teupe, C. (2016). Natriuretic peptide and high-sensitive troponin T concentrations correlate with effectiveness of short-term CPAP in patients with obstructive sleep apnea and coronary artery disease. Clin. Med. Insights Circ. Respir. Pulm. Med. 10, 33–39. doi: 10.4137/CCRPM.S40939
Takeuchi, S., Kitamura, T., Ohbuchi, T., Koizumi, H., Takahashi, R., Hohchi, N., et al. (2015). Relationship between sleep apnea and thyroid function. Sleep Breath. 19, 85–89. doi: 10.1007/s11325-014-0966-0
Tishler, P. V., Larkin, E. K., Schluchter, M. D., and Redline, S. (2003). Incidence of sleep-disordered breathing in an urban adult population: the relative importance of risk factors in the development of sleep-disordered breathing. JAMA 289, 2230–2237. doi: 10.1001/jama.289.17.2230
Tombaugh, T. N. (2004). Trail making test A and B: normative data stratified by age and education. Arch. Clin. Neuropsychol. 19, 203–214. doi: 10.1016/S0887-6177(03)00039-8
Wechsler, D. (1981). The Wechsler Adult Intelligence Scale-Revised (WAIS-R). San Antonio, TX: Psychological Corporation.
Yu, F. C., Yuan, C. X., Tong, J. Y., Zhang, G. H., Zhou, F. P., and Yang, F. (2018). Protective effect of sphingosine-1-phosphate for chronic intermittent hypoxia-induced endothelial cell injury. Biochem. Biophys. Res. Commun. 498, 1016–1021. doi: 10.1016/j.bbrc.2018.03.106
Keywords: obstructive sleep apnoea, cognitive function, NT-pro-BNP, N-terminal pro-brain natriuretic peptide, free triiodothyronine (fT3), free thyroxine (fT4), high-sensitivity c-reactive protein (hs-CRP)
Citation: Kazukauskiene N, Fineberg NA, Podlipskyte A, Bunevicius A, Narvaez Linares NF, Poitras M, Plamondon H, Pranckeviciene A, Gecaite-Stonciene J, Mickuviene N, Varoneckas G and Burkauskas J (2022) Contribution of Obstructive Sleep Apnoea to Cognitive Functioning of Males With Coronary Artery Disease: A Relationship With Endocrine and Inflammatory Biomarkers. Front. Neurosci. 16:899597. doi: 10.3389/fnins.2022.899597
Received: 18 March 2022; Accepted: 17 June 2022;
Published: 18 July 2022.
Edited by:
Shi-Bin Li, Stanford University, United StatesReviewed by:
Albina Aldoma, University Hospital Arnau de Vilanova, SpainCopyright © 2022 Kazukauskiene, Fineberg, Podlipskyte, Bunevicius, Linares, Poitras, Plamondon, Pranckeviciene, Gecaite-Stonciene, Mickuviene, Varoneckas and Burkauskas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julius Burkauskas, anVsaXVzLmJ1cmthdXNrYXNAbHNtdW5pLmx0
†ORCID: Nijole Kazukauskiene, orcid.org/0000-0003-4268-5303; Naomi A. Fineberg, orcid.org/0000-0003-1158-6900; Aurelija Podlipskyte, orcid.org/0000-0003-1412-6168; Adomas Bunevicius, orcid.org/0000-0003-0446-6898; Nicolás Francisco Narvaez Linares, orcid.org/0000-0002-2077-5159; Marilou Poitras, orcid.org/0000-0002-0786-1466; Hélène Plamondon, orcid.org/0000-0003-1003-2041; Aiste Pranckeviciene, orcid.org/0000-0002-8180-3504; Julija Gecaite-Stonciene, orcid.org/0000-0002-1560-1402; Giedrius Varoneckas, orcid.org/0000-0001-8073-4335; Narseta Mickuviene, orcid.org/0000-0002-7287-2639; Julius Burkauskas, orcid.org/0000-0002-3928-2151
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.