 Constantin-Cristian Topriceanu
Constantin-Cristian Topriceanu James C. Moon2,4
James C. Moon2,4 Gabriella Captur
Gabriella Captur Bhathika Perera
Bhathika Perera
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci. , 19 October 2022
Sec. Neuropharmacology
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.1020961
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder with onset usually in childhood characterized by inattention, impulsivity, and hyperactivity causing a functional impairment. Untreated ADHD, or treatment delay is associated with adverse outcomes and poor quality of life. Although conservative management strategies such as behavioral and psychological interventions are important, pharmacological treatment has a strong evidence base with improved outcomes. ADHD medications are broadly divided into stimulant and non-stimulant medications. Stimulant medications are generally more effective than non-stimulants. Cardiovascular safety of ADHD medication has been a matter of debate for decades. Treatment guidelines advise the careful consideration of risks and benefits in people with cardiovascular diseases such as congenital heart disease or cardiomyopathy. Although stimulants can increase systemic blood pressure and heart rate, no significant associations were found between their use and serious cardiovascular events. Concerns regarding QT effects and attendant sudden cardiac death risks deter clinicians from initiating much-needed ADHD medications in patients with heart disease. This overly cautious approach is potentially depriving low-risk individuals from significant benefits associated with timely ADHD drug treatment. This review discusses the cardiovascular risks reportedly associated with ADHD medications, the evidence base for their safe usage in persons with established cardiovascular disease, and highlights future research directions.
Attention-deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder (NDD) affecting around 5% of the population (Polanczyk and Rohde, 2007). Diagnosis of ADHD includes the presence of core symptoms of inattention, and/or hyperactivity/impulsivity. Symptoms manifest from early childhood in all cases and cause a functional impairment in personal, social, academic or occupational functioning (American Psychiatric Association., 2013). Treatment of ADHD is associated with improvements in core symptoms of ADHD along with a reduction in functional impairment in different domains of life. Although psychoeducation and behavioral strategies play a vital role in the management of ADHD, pharmacological treatments have a strong evidence base for their effectiveness (Brown et al., 2018).
It is hypothesized that ADHD is associated with a decrease in pre-frontal cortex and limbic system size and function (Arnsten, 2009). In addition, it is characterized by decreased release of dopamine and norepinephrine in the prefrontal cortex (del Campo et al., 2011). Therefore, pharmacological treatments focus on correcting these neurochemical deficiencies. They can be broadly divided into stimulants (e.g., methylphenidate and dexamfetamine) and non-stimulants (e.g., atomoxetine, clonidine, and guanfacine) (Pliszka, 2003). Dexamfetamine- and methylphenidate-based medications are norepinephrine and dopamine reuptake inhibitors (NDRI) (Briars and Todd, 2016). Dexamfetamine based medications have the added action of increased release of dopamine. Atomoxetine is a selective norepinephrine reuptake inhibitor (SNRI), however, it also increases dopaminergic transmission in the pre-frontal cortex as norepinephrine reuptake is linked to dopamine inactivation (Fu et al., 2022). Clonidine and guanfacine are centrally acting alpha-2-agonists which decrease sympathetic outflow from the central nervous system. In the context of ADHD though their mechanism is not fully understood, the most popular theory is that these agents modulate post-synaptic alpha-2-receptors which translates into an enhanced pre-frontal cortex connectivity (Arnsten, 2010). Generally, stimulant ADHD medications are more effective at reducing the core symptoms of ADHD and are associated with greater effect sizes in terms of positive social and academic outcomes (Habel et al., 2011; Franke et al., 2018).
Starting in the 90s, concerns regarding the cardiovascular (CV) safety of ADHD medications were raised (Gutgesell et al., 1999). As a result, at the first clinic visit, it has become standard practice to take a CV history and, if appropriate, perform a CV examination including a resting 12-lead electrocardiogram (ECG), followed by heart rate (HR) and blood pressure (BP) measurements at the subsequent visits (Brown et al., 2018). Cardiology specialist opinion is often sought before commencing ADHD medications if there is a history of CV disease (CVD), sudden cardiac death (SCD) in a first relative, cardiac murmurs on examination, high heart rate or blood pressure, or abnormal ECG features [e.g., a long corrected QT interval (QTc)]. Although many cardiovascular diagnoses are not contraindications to commencing ADHD medications (e.g., valvular stenosis or regurgitation, atrial or ventricular septal defects etc.), the management in the context of a serious cardiac disease [e.g., hypertrophic cardiomyopathy (HCM)] is still a dilemma as guidelines often vaguely recommend a risk-benefit assessment. This topic is especially relevant since ADHD is more prevalent in patients suffering from congenital heart disease or cardiomyopathy (Mahle et al., 2000; Niarchou et al., 2015). Treating ADHD in these patients has been associated with heighted SCD risk (Vetter et al., 2008), while not treating leads to poor quality of life and other adverse outcomes (Barkley et al., 2006). Thus, there is a need to explore and quantify cardiovascular risks associated with ADHD medications.
The current review summarizes the cardiovascular complications and risks associated with ADHD medication, discusses their use in individuals suffering from cardiomyopathy and congenital heart disease and concludes with future research directions.
In order to identify manuscripts in line with our review aim, a systematic search of Embase, PubMed, and Scopus was used to identify relevant publications published up to 01/10/2022. Search items were defined using the PICO (Patient/Intervention/Comparator/Outcomes) framework: (P) = (“Attention-Deficit Hyperactivity Disorder,” “ADHD”); (I) = (“ADHD medications,” “dexamfetamine,” “methylphenidate,” “atomoxetine,” “clonidine,” “guanfacine”); © = (“cardiovascular disease,” “electrocardiogram/ECG,” “hypertension/blood pressure,” “arrythmia/tachycardia/bradycardia/heart rate/long QT/prolonged QT/malignant ventricular arrythmia/ventricular arrythmia,” “cardiomyopathy,” “cardiac syndrome,” “heat failure,” “myocardial infarction,” “stroke/transient ischemic attack,” “aortic dissection/aneurysm,” “sudden cardiac death/sudden death/cardiac arrest”); (O) = (“outcome,” “risk,” “association”). The PICO framework categories were combined using “AND,” while we grouped the variations within categories via “OR.” Reference lists of included articles were also reviewed to identify further eligible publications.
Inclusion criteria were peer-reviewed, English-written manuscripts available online through electronic indexing fulfilling the following criteria: (1) study participants had diagnosed ADHD formally diagnosed, (2) study participants received pharmacological ADHD treatment, (3) study participants had any form of cardiovascular disease, or the study aimed to highlight an association between ADHD medications and a cardiovascular complication. Non-original research (i.e., lecture notes, book chapters, conference abstracts etc.) were excluded. The quality of studies (e.g., risk of bias) was not formally evaluated through a validated tool, but papers were critically appraised in the discussion.
The cardiovascular effects of medications used to treat ADHD in the general population are summarized in Table 1. Quantitative data relating the effects of ADHD medications on cardiovascular phenotypes based on previous studies and meta-analyses are presented in Table 2.
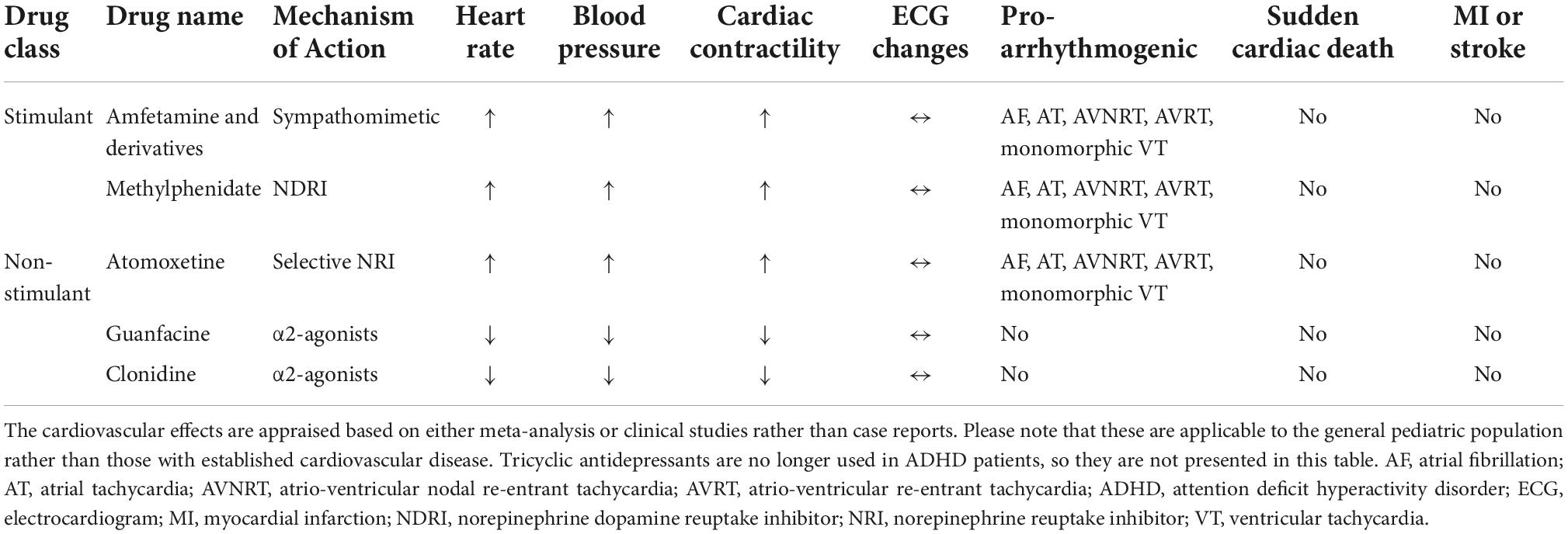
Table 1. The cardiovascular effects of medications used to treat ADHD in the general population.
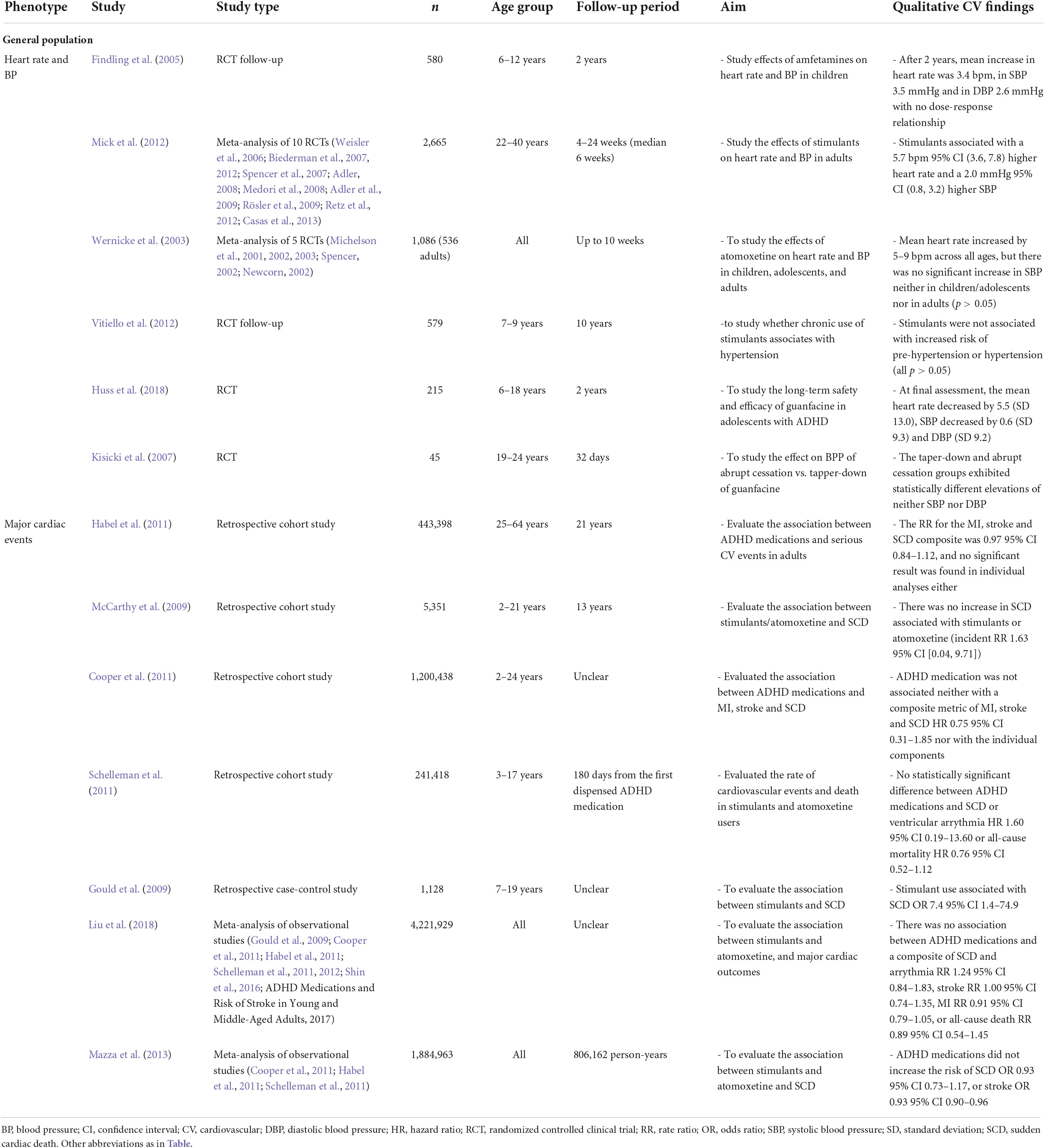
Table 2. Quantitative data relating the effects of ADHD medications on cardiovascular phenotypes.
Stimulant drugs and atomoxetine are positively chronotropic and inotropic, and increase the peripheral systemic vascular resistance as they block the reuptake of norepinephrine and/or dopamine. Thus, they are associated with increases in HR, cardiac contractility, and BP (Tisdale et al., 2020). On the other hand, α2-agonists (clonidine and guanfacine) reduce the sympathetic outflow from the central nervous system having negative chronotropic and inotropic effects which is meditated by the reduced β1 stimulation in the heart. Similarly, the reduced α1 stimulation in the periphery is associated with a reduced peripheral vascular resistance which translates into a reduced blood pressure (Hermiller et al., 1983). Despite this, orthostatic hypotension is unusual (Strange, 2008) as the mean reduction in either systolic or diastolic BP is <5 mmHg (Huss et al., 2018). However, they are associated with a withdrawal syndrome when abruptly discontinued or weaned too fast which is thought to occur due to a rebound sympathetic hyperactivity (Van ZwiEten et al., 1984). This has been shown in approximately half of clonidine users in small sample studies having a total sum totaling less than 200 participants (Geyskes et al., 1979; Weber, 1980; Reid et al., 1984; Leckman et al., 1985), but only in 3% of guanfacine users which might be explained due the longer half-life of the later (Strange, 2008). To date, the risk factors, or the doses at which rebound hypertension can occur are yet to be established. Abrupt withdrawal of guanfacine has been shown to cause an increase from pre-treatment systolic BP values of up to 30 mmHg in adults with already established hypertension (Sorkin and Heel, 1986), but the only clinical trial (involving 45 healthy volunteers aged 19–24 years without hypertension) found no association (Kisicki et al., 2007).
An ECG is highly accessible screening test for CV disease. In certain conditions such as HCM, more than 95% have an ECG abnormality such as repolarization abnormalities (e.g., T-wave inversion, ST depression or elevation) in 80%, left ventricular hypertrophy (e.g., a high Sokolow-Lyon index) in 70%, or QRS-axis deviation in less than 40% (Norrish et al., 2021). However, the negative predictive value of a normal resting ECG is limited by conditions in which abnormalities are subtle (e.g., subclinical HCM; Captur et al., 2014) or only apparent during exertion (Amin et al., 2009). Still, it remains is a cost-effective screening tool (Fuller, 2000) and hence its widespread use (although not mandatory) before starting ADHD medications in clinical practice. However, none of the ADHD medications commonly used in practice bring about any apparent ECG changes (Vetter et al., 2008) besides the faster heart rate as per the scientific statement from the American Heart Association Council on Cardiovascular Disease in the Young Congenital Cardiac Defects Committee (Vetter et al., 2008). It should be noted that this conclusion was based on small clinical trials in stimulants (Dittmann et al., 2001; Findling et al., 2001), atomoxetine (Michelson et al., 2003; Wernicke et al., 2003), clonidine (Hazell and Stuart, 2003), or guanfacine (Hunt et al., 1995). Thus, the value of repeating the ECG for predicting who might develop an arrythmia or who is at risk of SCD is limited.
T-wave inversions in leads III and V4-V6, incomplete right bundle branch block and sinus arrythmia are common in the pediatric population (Norrish et al., 2021) and should not preclude the administration of ADHD medications. Premature atrial or ventricular contractions at low frequency and in the absence of cardiac disease, are also considered benign and should not prevent the initiation of ADHD pharmacological treatment (Picarzo et al., 2020).
Both dexamfetamine and methylphenidate are pro-arrhythmogenic given their direct and indirect sympathomimetic effects. The increase in β-adrenergic stimulation of the heart may cause, precipitate or worsen atrial fibrillation (AF), supraventricular tachycardia [SVT; which includes atrial tachycardia (AT) and atrio-ventricular nodal re-entrant tachycardia (AVNRT)] or monomorphic ventricular tachycardia (VT) as per the American Heart Association consensus statement (Tisdale et al., 2020). The recommendations are based on retrospective cohort studies both in children (Dalsgaard et al., 2014; Shin et al., 2016) and adults (Habel et al., 2011; Schelleman et al., 2012) given the paucity of randomized controlled clinical trials (RCTs). However, this seems to be limited to the exposed time-periods only (Westover and Halm, 2012) with no evidence of long-lasting risks once the medication was stopped (Martinez-Raga et al., 2012). Although generally, increments in resting HR are associated with increased mortality in the general population (Hartaigh et al., 2014), it is unclear whether this holds true for drug-induced HR increases. In adults, although methylphenidate increases the risk of ventricular arrythmias, this effect was not dose-dependent in a cohort of 43,999 methylphenidate users which might suggest that this effect is not causal (Schelleman et al., 2012). In >100,000 person-years of observation using US Medicaid data, although stimulant use was not associated with cardiac death, an increase in emergency room visits but without an increase in hospitalizations was observed (Winterstein et al., 2007). Moreover, an insurance claim review of >150,000 participants found no association between stimulants and clinical symptoms of diagnoses of cardiovascular events (Olfson et al., 2012). Guanfacine and clonidine do not appear to be pro-arrhythmic (Martin et al., 2015; Constantin-Cristian Topriceanu, 2016) and clonidine has historically been shown to have HR-reducing properties in AF (Goodman, 1992) and to reduce the incidence of ventricular arrythmias in adults with heart failure (Zhang and Zhu, 1998). However, the studies which reported these findings are >30 years old with no recent studies replicating or refuting the claims.
Variable drug-response phenotypes can be explained by differences in pharmacokinetics and pharmacodynamics (Yasuda et al., 2008; Schoretsanitis et al., 2019). The differences in pharmacokinetics arise mainly from the genetic variability of drug-metabolizing enzymes (Bjornsson et al., 2003) most of which belong to the CYP superfamily (Guengerich, 2019) which display a considerable inter-ethnic variability (Fricke-Galindo et al., 2016) with copy-number variants (i.e., more than two copies of functional alleles) leading to increased metabolism also being recognized (Ma et al., 2002). Amfetamines and atomoxetine are metabolized via a CYP2D6-mediated hydroxylation (Schoretsanitis et al., 2019), guanfacine is a substrate for CYP3A4 (Verplaetse et al., 2019), while clonidine is metabolized by both but mainly by CYP2D6 (Claessens et al., 2010). Based on the activity of the enzyme isoforms, patients can range from poor (prone to toxicity), intermediate, extensive/normal, rapid to ultrarapid (prone to reduce efficacy) metabolizers. Thus, poor and intermediate metabolizers are more likely to experience side-effects (e.g., tachycardia) (Kam and Jeong, 2020). For CYP2D6, Caucasians are more likely to carry the wild-type CYP2D6*1 allele and be normal (about 40%) rather than intermediate or poor (< 10%) metabolizers (Bradford, 2002; Ingelman-Sundberg et al., 2007). In contrast, CYP2D6*10 is common in Asians meaning that 30–40% are intermediate metabolizers (Gaedigk et al., 1999). In Africans, the percentage of functional alleles is around 50% with reduced function alleles (especially CYP2D6*17) being present in 30–40% of the population (Bradford, 2002). Similarly, there is an ethnicity related polymorphism in CYP3A4 (Guttman et al., 2019). Thus, pharmacogenomic biomarkers are an exciting prospect in the field of precision medicine and personalized pharmacotherapy (Kam and Jeong, 2020).
As dexamfetamine can increase the BP, they are relatively contraindicated in ADHD patients with moderate and severe hypertension (Brown et al., 2018). However, the average increase in systolic and diastolic BP ranged between approximately 3–6 and 2–4 mmHg respectively, in clinical trials with a few hundred participants (Dittmann et al., 2001; Findling et al., 2001) (Michelson et al., 2003; Wernicke et al., 2003) (Samuels et al., 2006). Although some small studies reported an association between stimulant dose and BP effects (Stowe et al., 2002), adequately powered studies did not replicate the findings (Findling et al., 2005). Moreover, some of the acute effects on BP are attenuated with chronic treatment but full tolerance might not develop (Safer, 1992; Wilens et al., 2004; Hammerness et al., 2009). The Multimodal Treatment Study of Children with ADHD (MTA) RCT (NCT: 00000388) found no significant increase in systolic/diastolic BP in 579 children aged 7–9 over 14 months, and also concluded that stimulants were not associated with increased risk of pre-hypertension or hypertension over the 10-year naturalistic follow-up after the trial (Vitiello et al., 2012). Similarly, stimulant ADHD medication increase the heart rate by 4–5 bpm on average (Findling et al., 2005; Mick et al., 2012). The effects of atomoxetine are comparable to psychostimulants (Liang et al., 2018). Given that guanfacine and clonidine decrease the BP, their use in those with cardiac problems associated with hypertension has a double benefit. However, the mean reduction in either systolic or diastolic blood pressure is <5 mmHg in those who are normotensive as shown by clinical trials with a few hundred participants (Huss et al., 2018).
The association between amfetamines and vascular accidents such as myocardial infarction (MI) and hemorrhagic stroke became apparent from population studies based on drug users hospitalized patients (Westover et al., 2007; Huang et al., 2017). Although case reports of both exist, most studies did not find any associations between psychostimulant use and stroke or MI, neither in children and adolescents (Schelleman et al., 2011; Zito and Burcu, 2017) nor in adults (ADHD Medications and Risk of Stroke in Young and Middle-Aged Adults, 2011; Schelleman et al., 2012; Westover and Halm, 2012; Table 2). However, there might be a higher risk of MI but not for stroke in the first 2 months after starting methylphenidate as shown by a small study of 1,224 participants (Shin et al., 2016). In contrast, the increased risk of MI or stroke was not found to be significantly higher in those who recently started stimulants or atomoxetine in half a million participants (Habel et al., 2011). Moreover, most studies did not find any association between atomoxetine and MI or stroke (Holick et al., 2009; Schelleman et al., 2012; Houghton et al., 2020). However, stimulants/atomoxetine might increase the risk of a transient ischemic attack in adults (Holick et al., 2009) which was not observed for children.
Coronary failure is uncommon in children and adolescence. Often the causes include coronary artery anomalies (CAAs), acute Kawasaki disease and vasculitis (Graidis et al., 2015). The increased chronotropy reduces diastole when most blood flow through the coronary artery occurs. Moreover, the positive inotropic effect is associated with higher myocardial oxygen consumption. This is partially counterbalanced by the increased diastolic BP which promotes coronary blood flow. However, given the modest increase in both, neither should be significant in the context of normal physiology. However, in those with coronary failure psychostimulants and atomoxetine can theoretically lead to myocardial supply-demand mismatch which predisposes to a myocardial infarction. As above, this is especially relevant in the period immediately after starting the ADHD medication. Similarly, by decreasing the blood pressure, α2-agonists also reduce coronary perfusion. Thus, all ADHD medications pose theoretical list in those with coronary failure. In acute conditions such as Kawasaki disease and vasculitis, holding the ADHD medications until resolution would be the safest approach. CAAs describe a spectrum from almost normal to completely abnormal coronary blood flow (Graidis et al., 2015). Despite no clinical data, use of sympathomimetic drugs in those with moderate-severe CAAs should be cautious.
Aortic diameter above 3.5 cm is considered to be dilated in adults, but in children normograms with height or body surface area indexation are used. The greater the dilatation, the more likely it is to rupture or to dissect (Erbel and Eggebrecht, 2006). In patients with a dilated proximal aorta, e.g., in the context of Marfan’s syndrome, increases in BP can further exacerbate the dilatation of aorta which might be prone it to rupture (Singh et al., 2021). Thus, psychostimulants and atomoxetine should be avoided, but α2-agonists are safe. Nevertheless, many of those who have aortic dilation are usually already on BP lowering therapy such as β-blockers meaning that they might not tolerate the further drop in BP brought on by the α2-agonists.
Excluding sudden infant death syndrome (SIDS), the commonest causes of sudden cardiac death in children are: (1) structural cardiac disease (e.g., CAAs), (2) cardiomyopathies [HCM, dilated cardiomyopathy (DCM)], (3) arrhythmic cardiomyopathy (AC) and (4) channelopathies (e.g., long QT, Brugada syndrome) with HCM and CAAs being the top two causes (Gajewski and Saul, 2010). In the general pediatric population, studies have obtained mixed effects regarding the association of psychostimulants and atomoxetine with SCD. Some large studies with a combined sample size of almost two million participants found no association (McCarthy et al., 2009; Cooper et al., 2011; Habel et al., 2011) while relatively smaller studies of a quarter of a million participants reported 2–7 times higher odds of SCD (Gould et al., 2009; Schelleman et al., 2011), although they did not adjust for confounders (Schelleman et al., 2011) or failed to address selection bias (Westover and Halm, 2012). These associations were not significant in meta-analyses but the uncertainty arising from the wide confidence intervals of the hazard ratios (Mazza et al., 2013; Liu et al., 2018) highlight the need for more research to understand the association between ADHD medications and SCD.
HCM is relatively common affecting 1 in 500 adults and is the leading cause of SCD in the developed world. Current predictors of SCD in HCM include family history of SCD, a left ventricular outflow tract obstruction (LVOTO), high maximal wall thickness (MWT) and non-sustained VT (NSVT) (Norrish et al., 2021). However, these high-risk patients often have implantable cardioverter defibrillations (ICDs) inserted which allows for a more liberal use of ADHD medications (Kantor et al., 2021).
By lowering the blood pressure, α2-agonists increase the LVOT gradient, but this is counterbalanced by their negatively inotropic effect which decreases any LVOTO (Reza et al., 2021). Although the degree of LVOTO is directly related to the risk of SCD (Elliott et al., 2006), minor dynamic increases might not be clinically significant. Moreover, clonidine is considered safe in HCM and is sometimes used to treat hypertension in these patients (Argulian et al., 2013; Sherrid, 2016). The decreased sympathetic outflow brought about by α2-agonists could be beneficial in HCM extrapolating from the use of β-blockers (Hensley et al., 2015).
By increasing adrenergic conduction, psychostimulants and atomoxetine can predispose to NSVT and other atrial and ventricular tachyarrhythmias, and therefore are generally avoided in HCM. Although this is the consensus, it is based mostly on biological plausibility, case reports and retrospective cohort studies (Dalsgaard et al., 2014) with no RCTs being published.
Although in adults, DCM is often secondary to ischemic heart disease, hypertension, and excessive alcohol (Reichart et al., 2019), it is commonly genetic in the pediatric population (Lee et al., 2017) or in those with a positive family history. The association between amfetamines and cocaine use and the developmental of DCM from cardiotoxicity is well established (Lange and Hillis, 2001). As excess catecholamines are toxic to the heart, stimulants could potentially lead to DCM. Although theoretically possible, the association of DCM with psychostimulants at therapeutic doses in ADHD is limited to case reports (Nymark et al., 2008) with no association with heart failure being seen in larger studies (Shin et al., 2016). In those with already established DCM, the use of sympathomimetics is controversial given the increased myocardial workload (Page et al., 2016). However, α2-agonists decrease the heart rate and the afterload and could be beneficial (Hermiller et al., 1983; Girgis et al., 1998) unless the blood pressure is already low. In that scenario, they could cause orthostatic hypotension, syncope, or even hemodynamic collapse.
In the general pediatric population, none of the ADHD medications have been associated with torsade de points (i.e., polymorphic VT) or significant increases in QTc. This also holds true for the use of stimulant medications in patients with long-QT syndrome (n = 144) although higher odds for syncope was demonstrated (Zhang et al., 2015). Extrapolating from use of β-agonists in asthma, the syncope was postulated to be secondary to arrythmias as those with long-QT syndrome have lower threshold to experience them when exposed to sympathomimetic agents (Thottathil et al., 2008). Although atomoxetine reduces K+ efflux from the heart as an antagonist of IKr channel (Scherer et al., 2009), this is not problematic in the general pediatric population at a therapeutic dose as it is not associated with a prolonged QT. However, at supratherapeutic doses the QTc is increased (Martinez-Raga et al., 2012) in a dose dependent fashion (Loghin et al., 2013). As IKr is implicated in long-QT syndrome, use of atomoxetine in those with long-QT syndrome is theoretically problematic, but this has not been evaluated in clinical studies. Although there is a warning from the European Medicines Agency (EMA) regarding the prospect of α2-agonists (e.g., guanfacine) use in those with long-QT syndrome, clinical studies concluded that they do not interfere with cardiac repolarization and are not known to be pro-arrhythmic (Martin et al., 2015; Constantin-Cristian Topriceanu, 2016) and hence this warning might be overly-cautious.
Besides blocking the cardiac IKr channel (Scherer et al., 2009), atomoxetine can also block the hNav1.5 channels at therapeutic levels (Föhr et al., 2021) which makes it a potentially unwise choice for use in children suffering with Brugada syndrome (Brugada et al., 1999) as it can potentially push the heart into ventricular fibrillation (VF). For the same reason the use of TCAs is contraindicated. However, neither stimulants nor α2-agonists were shown to interfere with cardiac Na+ channels. Since the stimulants increase the adrenergic transmission and further increase the risk of arrythmias (Tisdale et al., 2020), there is an argument for avoiding them in Brugada syndrome. However, there are no reported contraindication to α2-agonists based on the literature (Francis and Antzelevitch, 2008). Nevertheless, the use of any ADHD medications continues to be commonly avoided in patients suffering from ADHD and Brugada syndrome (Gundogmus et al., 2018) depriving them from adequate ADHD management.
According to the AHA consensus statement, ADHD medication can be started in those with Wolf-Parkinson-White (WPW) syndrome, but close monitoring is warranted. The prospect of developing atrio-ventricular re-entrant tachycardia (AVRT) is linked to atrio-ventricular node blockade as it is the case with β-blockers (Babayiğit et al., 2020). As psychostimulants and atomoxetine increase the sympathetic drive in the heart, they have not been classically associated with AVRT despite being associated with AVNRT (Tisdale et al., 2020). However, they might promote AF (Tisdale et al., 2020). If that happens, the rate-limiting effects of the AV node are bypassed, and conduction occurs through the accessory pathway potentially leading to VF and cardiac arrest. Although there is no study which reported the incidence of AF in children/adolescents treated with psychostimulants and atomoxetine, it seems to be a rare phenomenon mainly seen in case reports (Gao et al., 2020). Thus, avoiding them in WPW might be overly cautions. However, by decreasing the sympathetic outflow to the heart, α2-agonists can reduce the conduction through the AV node (Kibler and Gazes, 1977) potentially predisposing to AVRT. However, this is more a theoretical risk as no reports of α2-agonists being associated with AVRT or SCD in WPW were found. Furthermore, WPW can be cured through electrophysiological ablation which would allow a more liberal use of ADHD medications in these patients (Shetty et al., 2011).
Attention-deficit hyperactivity disorder treatment has been shown to decrease antisocial behavior, poor academic performance, and mortality but to date, many individuals with cardiovascular disease continue to be deprived of ADHD medications because of overly cautious approaches unsupported by the evidence-base. Review of published evidence shows that stimulant and non-stimulant ADHD medications have generally good cardiovascular safety profiles but given their mechanisms of action, they should be used cautiously in children and adults with pro-arrhythmic cardiovascular diseases. Although α2-agonists are not as effective as stimulants, they are not pro-arrhythmic and therefore safer in those at higher risk of arrhythmias. The increase or decrease in blood pressure associated with stimulants and α2-agonists, respectively, is not usually clinically significant so clinicians should not be deterred from starting them although their abrupt withdrawal, especially of clonidine, can be problematic.
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. As the data used in this manuscript is publicly available, an ethics approval waiver was applied.
C-CT guarantor of this work and attested that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted. All authors contributed significantly to the study design and implementation, data analysis and interpretation, and manuscript writing, involved in critically reviewing and revising the manuscript, approved the final version as submitted, and agree to be accountable for all aspects of the work.
GC was supported by the British Heart Foundation (MyoFit46 Special Programme Grant SP/20/2/34841). JM was directly and indirectly supported by the UCL Hospitals National Institute for Health and Care Research (NIHR) BRC and Biomedical Research Unit at Barts Hospital. GC and JM were supported by the Barts Charity HeartOME1000 project grant (MGU0427 / G-001411).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adler, L. (2008). Double-blind, placebo-controlled study of the efficacy and safety of lisdexamfetamine dimesylate in adults with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 69, 364–373. doi: 10.4088/JCP.v69n0903
Adler, L. A., Zimmerman, B., Starr, H. L., Silber, S., Palumbo, J., Orman, C., et al. (2009). Efficacy and safety of OROS methylphenidate in adults with attention-deficit/hyperactivity disorder: A randomized, placebo-controlled, double-blind, parallel group, dose-escalation study. J. Clin. Psychopharmacol. 29, 239–247. doi: 10.1097/JCP.0b013e3181a390ce
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders : DSM-5, 5th Edn. Arlington, VA: American Psychiatric Association. doi: 10.1176/appi.books.9780890425596
Amin, A. S., de Groot, E. A. A., Ruijter, J. M., Wilde, A. A. M., and Tan, H. L. (2009). Exercise-induced ecg changes in brugada syndrome. Circ. Arrhythm. Electrophysiol. 2, 531–539. doi: 10.1161/CIRCEP.109.862441
Argulian, E., Messerli, F. H., Aziz, E. F., Winson, G., Agarwal, V., Kaddaha, F., et al. (2013). Antihypertensive therapy in hypertrophic cardiomyopathy. Am. J. Cardiol. 111, 1040–1045. doi: 10.1016/j.amjcard.2012.12.026
Arnsten, A. F. T. (2009). The emerging neurobiology of attention deficit hyperactivity disorder: The key role of the prefrontal association cortex. J. Pediatr. 154:S22–S31.
Arnsten, A. F. T. (2010). The use of [alpha]-2A adrenergic agonists for the treatment of attention-deficit/hyperactivity disorder. Exp. Rev. Neurother. 10:1595.
Babayiğit, E., Ulus, T., and Görenek, B. (2020). What have we learned from the european society of cardiology 2019 guidelines on supraventricular tachycardia. Cardiology 145, 492–503. doi: 10.1159/000508264
Barkley, R. A., Fischer, M., Smallish, L., and Fletcher, K. (2006). Young adult outcome of hyperactive children: Adaptive functioning in major life activities. J. Am. Acad. Child Adolesc. Psychiatry 45, 192–202. doi: 10.1097/01.chi.0000189134.97436.e2
Biederman, J., Fried, R., Hammerness, P., Surman, C., Mehler, B., Petty, C. R., et al. (2012). The effects of lisdexamfetamine dimesylate on the driving performance of young adults with ADHD: A randomized, double-blind, placebo-controlled study using a validated driving simulator paradigm. J. Psychiatr. Res. 46, 484–491. doi: 10.1016/j.jpsychires.2012.01.007
Biederman, J., Mick, E. O., Surman, C., Doyle, R., Hammerness, P., Michel, E., et al. (2007). Comparative acute efficacy and tolerability of OROS and immediate release formulations of methylphenidate in the treatment of adults with attention-deficit/hyperactivity disorder. BMC psychiatry 7:49. doi: 10.1186/1471-244X-7-49
Bjornsson, T. D., Callaghan, J. T., Einolf, H. J., Fischer, V., Gan, L., Grimm, S., et al. (2003). The conduct of in vitro and in vivo drug-drug interaction studies: A pharmaceutical research and manufacturers of America (phrma) perspective. Drug Metab. Dispos. 31, 815–832. doi: 10.1124/dmd.31.7.815
Bradford, L. D. (2002). CYP2D6 allele frequency in European caucasians, Asians, Africans and their descendants. Pharmacogenomics 3, 229–243. doi: 10.1517/14622416.3.2.229
Briars, L., and Todd, T. (2016). A review of pharmacological management of attention-deficit/hyperactivity disorder. J. Pediatr. Pharmacol. Ther. 21, 192–206. doi: 10.5863/1551-6776-21.3.192
Brown, K. A., Samuel, S., and Patel, D. R. (2018). Pharmacologic management of attention deficit hyperactivity disorder in children and adolescents: A review for practitioners. Trans. Pediatr. 7, 36–47. doi: 10.21037/tp.2017.08.02
Brugada, J., Brugada, P., and Brugada, R. (1999). The syndrome of right bundle branch block ST segment elevation in V1 to V3 and sudden death - The Brugada syndrome. Europace 1, 156–166. doi: 10.1053/eupc.1999.0033
Captur, G., Lopes, L. R., Patel, V., Li, C., Bassett, P., Syrris, P., et al. (2014). Abnormal cardiac formation in hypertrophic cardiomyopathy fractal analysis of trabeculae and preclinical gene expression. Circ. Cardiovasc. Genet. 7, 241–248. doi: 10.1161/CIRCGENETICS.113.000362
Habel, L. A., Cooper, W. O., Sox, C. M., Chan, K. A., Fireman, B. H., Arbogast, P. G., et al. (2011). ADHD medications and risk of serious cardiovascular events in young and middle-aged adults. JAMA 306, 2673–2683. doi: 10.1001/jama.2011.1830
Huang, M. C., Yang, S. Y., Lin, S. K., Chen, K. Y., Chen, Y. Y., Kuo, C. J., et al. (2017). Risk of cardiovascular diseases and stroke events in methamphetamine users: A 10-year follow-up study. J. Clin. Psychiatry 77, 1396–1403. doi: 10.4088/JCP.15m09872
Casas, M., Rösler, M., Sandra Kooij, J. J., Ginsberg, Y., Ramos-Quiroga, J. A., Heger, S., et al. (2013). Efficacy and safety of prolonged-release OROS methylphenidate in adults with attention deficit/hyperactivity disorder: A 13-week, randomized, double-blind, placebo-controlled, fixed-dose study. World J. Biol. Psychiatry 14, 268–281. doi: 10.3109/15622975.2011.600333
Claessens, A. J., Risler, L. J., Eyal, S., Shen, D. D., Easterling, T. R., and Hebert, M. F. (2010). CYP2D6 mediates 4-hydroxylation of clonidine in vitro: Implication for pregnancy-induced changes in clonidine clearance. Drug Metab. Dispos. 38, 1393–1396. doi: 10.1124/dmd.110.033878
Constantin-Cristian Topriceanu (2016). Guanfacine for ADHD in children and adolescents. Drug Ther. Bull. 54, 56–60. doi: 10.1136/dtb.2016.5.0402
Cooper, W. O., Habel, L. A., Sox, C. M., Chan, K. A., Arbogast, P. G., Cheetham, T. C., et al. (2011). ADHD drugs and serious cardiovascular events in children and young adults. N. England J. Med. 365, 1896–1904. doi: 10.1056/NEJMoa1110212
Dalsgaard, S., Kvist, A. P., Leckman, J. F., Nielsen, H. S., and Simonsen, M. (2014). Cardiovascular safety of stimulants in children with attention-deficit/hyperactivity disorder: A nationwide prospective cohort study. J. Child Adolesc. Psychopharmacol. 24, 302–310. doi: 10.1089/cap.2014.0020
del Campo, N., Chamberlain, S. R., Sahakian, B. J., and Robbins, T. W. (2011). The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biological psychiatry 69:e145–e157. doi: 10.1016/j.biopsych.2011.02.036
Dittmann, R. W., Fouche, D. S., Kratochvil, C., Heiligenstein, J. H., Spencer, T., and Biederman, J. (2001). Atomoxetine and methylphenidate treatment in children with ADHD: A prospective, randomized, open-label trial. Eur. Neuropsychopharmacol. 11:S318–S319. doi: 10.1016/S0924-977X(01)80448-X
Elliott, P. M., Gimeno, J. R., Tomé, M. T., Shah, J., Ward, D., Thaman, R., et al. (2006). Left ventricular outflow tract obstruction and sudden death risk in patients with hypertrophic cardiomyopathy. Eur. Heart J. 27, 1933–1941. doi: 10.1093/eurheartj/ehl041
Erbel, R., and Eggebrecht, H. (2006). Aortic dimensions and the risk of dissection. Hear 92, 137–142. doi: 10.1136/hrt.2004.055111
Findling, R. L., Biederman, J., Wilens, T. E., Spencer, T. J., McGough, J. J., Lopez, F. A., et al. (2005). Short- and Long-Term Cardiovascular Effects of Mixed Amphetamine Salts Extended Release in Children. J. Pediatr. 147, 348–354. doi: 10.1016/j.jpeds.2005.03.014
Findling, R. L., Short, E. J., and Manos, M. J. (2001). Short-term cardiovascular effects of methylphenidate and adderall. J. Am. Acad. Child Adolesc. Psychiatry 40, 525–529.
Föhr, K. J., Nastos, A., Fauler, M., Zimmer, T., Jungwirth, B., and Messerer, D. A. C. (2021). Block of voltage-gated sodium channels by atomoxetine in a state- and use-dependent manner. Front. Pharmacol. 12:622489. doi: 10.3389/fphar.2021.622489
Francis, J., and Antzelevitch, C. (2008). Atrial fibrillation and brugada syndrome. J. Am. Coll. Cardiol. 51, 1149–1153. doi: 10.1016/j.jacc.2007.10.062
Franke, B., Michelini, G., Asherson, P., Banaschewski, T., Bilbow, A., Buitelaar, J. K., et al. (2018). Live fast, die young? A review on the developmental trajectories of ADHD across the lifespan. Eur. Neuropsychopharmacol. 28, 1059–1088. doi: 10.1016/j.euroneuro.2018.08.001
Fricke-Galindo, I., Céspedes-Garro, C., Rodrigues-Soares, F., Naranjo, M. E. G., Delgado, Á, De Andrés, F., et al. (2016). Interethnic variation of CYP2C19 alleles, ‘predicted’ phenotypes and ‘measured’ metabolic phenotypes across world populations. Pharmacogenomics J. 16, 113–123. doi: 10.1038/tpj.2015.70
Fu, D., Wu, D.-D., Guo, H.-L., Hu, Y.-H., Xia, Y., Ji, X., et al. (2022). The mechanism, clinical efficacy, safety, and dosage regimen of atomoxetine for ADHD therapy in children: A narrative review. Front. Psychiatry 12:780921. doi: 10.3389/fpsyt.2021.780921
Fuller, C. M. (2000). Cost effectiveness analysis of screening of high school athletes for risk of sudden cardiac death. Med. Sci. Sports Exerc. 32, 887–890. doi: 10.1097/00005768-200005000-00002
Gaedigk, A., Gotschall, R. R., Forbes, N. S., Simon, S. D., Kearns, G. L., and Leeder, J. S. (1999). Optimization of cytochrome P4502D6 (CYP2D6) phenotype assignment using a genotyping algorithm based on allele frequency data. Pharmacogenetics 9, 669–682. doi: 10.1097/01213011-199912000-00002
Gajewski, K. K., and Saul, J. P. (2010). Sudden cardiac death in children and adolescents (excluding Sudden Infant Death Syndrome). Ann. Pediatr. Cardiol. 3, 107–112. doi: 10.4103/0974-2069.74035
Gao, M., Chin, J., Nagendiram, G., Chen, D., Rajyaguru, P., and Lomiguen, C. (2020). New onset atrial fibrillation in health profession student with newly diagnosed Adhd: A case report on wellness and cardiovascular consequences of burnout. Int. J. Clin. Cardiol. 7:175. doi: 10.23937/2378-2951/1410175
Geyskes, G. G., Boer, P., and Mees, D. E. J. (1979). Clonidine withdrawal. Mechanism and frequency of rebound hypertension. Br. J. Clin. Pharmacol. 7, 55–62. doi: 10.1111/j.1365-2125.1979.tb00897.x
Girgis, I., Chakko, S., de Marchena, E., Jara, C., Diaz, P., Castellanos, A., et al. (1998). Effect of clonidine on heart rate variability in congestive heart failure. Am J. Cardiol. 82, 335–337. doi: 10.1016/S0002-9149(98)00329-4
Goodman, T. (1992). Clonidine for patients with rapid atrial fibrillation. Ann. Emergency Med. 21, 1012–1013. doi: 10.1016/S0196-0644(05)82954-3
Gould, M. S., Walsh, B. T., Munfakh, J. L., Kleinman, M., Duan, N., Olfson, M., et al. (2009). Sudden death and use of stimulant medications in youths. Am. J. Psychiatry 166, 992–1001. doi: 10.1176/appi.ajp.2009.09040472
Graidis, C., Dimitriadis, D., Karasavvidis, V., Dimitriadis, G., Argyropoulou, E., Economou, F., et al. (2015). Prevalence and characteristics of coronary artery anomalies in an adult population undergoing multidetector-row computed tomography for the evaluation of coronary artery disease. BMC Cardiovasc. Disord. 15:112. doi: 10.1186/s12872-015-0098-x
Guengerich, F. P. (2019). Cytochrome P450 research and The Journal of Biological Chemistry. J. Biol. Chem. 294, 1671–1680. doi: 10.1074/jbc.TM118.004144
Gundogmus, P. D., Gundogmus, I., Karagoz, A., Kiyancicek, M., Yasar, A. B., and Algul, A. (2018). Treatment of ADHD in a patient with Brugada syndrome: A case report and a brief review. Psychiatry Clin. Psychopharmacol. 28, 339–342. doi: 10.1080/24750573.2017.1338821
Gutgesell, H., Atkins, D., Barst, R., Buck, M., Franklin, W., Humes, R., et al. (1999). Cardiovascular monitoring of children and adolescents receiving psychotropic drugs: A statement for healthcare professionals from the committee on congenital cardiac defects, council on cardiovascular disease in the young, American Heart Association. Circulation 99, 979–982. doi: 10.1161/01.cir.99.7.979
Guttman, Y., Nudel, A., and Kerem, Z. (2019). Polymorphism in cytochrome P450 3A4 is ethnicity related. Front. Genet. 10:224. doi: 10.3389/fgene.2019.00224
Habel, L. A., Cooper, W. O., Sox, C. M., Chan, K. A., Fireman, B. H., Arbogast, P. G., et al. (2011). ADHD medications and risk of serious cardiovascular events in young and middle-aged adults. JAMA 306, 2673–2683. doi: 10.1001/jama.2011.1830
Hammerness, P. M. D., Wilens, T. M. D., Mick, E. S., Spencer, T. M. D., Doyle, R. M. D., McCreary, M. B. A., et al. (2009). Cardiovascular effects of longer-term, high-dose oros methylphenidate in adolescents with attention deficit hyperactivity disorder. J. Pediatr. 155:84–9, 89.e1. doi: 10.1016/j.jpeds.2009.02.008
Hartaigh, B. O., Gill, T. M., Shah, I., Hughes, A. D., Deanfield, J. E., Kuh, D., et al. (2014). Association between resting heart rate across the life course and all-cause mortality: Longitudinal findings from the Medical Research Council (MRC) National Survey of Health and Development (NSHD). J. Epidemiol. Community Health 68, 883–889. doi: 10.1136/jech-2014-203940
Hazell, P. L., and Stuart, J. E. A. (2003). Randomized controlled trial of clonidine added to psychostimulant medication for hyperactive and aggressive children. J. Am. Acad. Child Adolesc. Psychiatry 42, 886–894. doi: 10.1097/01.CHI.0000046908.27264.00
Hensley, N., Dietrich, J., Nyhan, D., Mitter, N., Yee, M.-S., and Brady, M. (2015). Hypertrophic cardiomyopathy: A review. Anesth. Analg. 120, 554–569. doi: 10.1213/ANE.0000000000000538
Hermiller, J. B., Magorien, R. D., Leithe, M. E., Unverferth, D. V., and Leier, C. V. (1983). Clonidine in congestive heart failure: A vasodilator with negative inotropic effects. Am. J. Cardiol. 51, 791–795. doi: 10.1016/s0002-9149(83)80135-0
Holick, C. N., Turnbull, B. R., Jones, M. E., Chaudhry, S., Bangs, M. E., and Seeger, J. D. (2009). Atomoxetine and cerebrovascular outcomes in adults. J. Clin. Psychopharmacol. 29, 453–460. doi: 10.1097/JCP.0b013e3181b2b828
Houghton, R., de Vries, F., and Loss, G. (2020). Psychostimulants/atomoxetine and serious cardiovascular events in children with adhd or autism spectrum disorder. CNS Drugs. 34, 93–101. doi: 10.1007/s40263-019-00686-4
Hunt, R. D., Arnsten, A. F. T., and Asbell, M. D. (1995). An open trial of guanfacine in the treatment of attention-deficit hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 34, 50–54. doi: 10.1097/00004583-199501000-00013
Huss, M., Dirks, B., Gu, J., Robertson, B., Newcorn, J. H., and Ramos-Quiroga, J. A. (2018). Long-term safety and efficacy of guanfacine extended release in children and adolescents with ADHD. Eur. Child Adolesc. Psychiatry 27, 1283–1294. doi: 10.1007/s00787-018-1113-4
Ingelman-Sundberg, M., Sim, S. C., Gomez, A., and Rodriguez-Antona, C. (2007). Influence of cytochrome P450 polymorphisms on drug therapies: Pharmacogenetic, pharmacoepigenetic and clinical aspects. Pharmacol. Ther. 116, 496–526. doi: 10.1016/j.pharmthera.2007.09.004
Kam, H., and Jeong, H. (2020). Pharmacogenomic biomarkers and their applications in psychiatry. Genes. 11, 1–22. doi: 10.3390/genes11121445
Kantor, P. F., Casarez, T. W., and Bar-Cohen, Y. (2021). Hypertrophic cardiomyopathy in adolescence: Application of guidelines. JACC Case Rep. 3, 10–15. doi: 10.1016/j.jaccas.2020.11.006
Kibler, L., and Gazes, P. (1977). Effect of clonidine on atrioventricular conduction. JAMA 238, 1930–1932. doi: 10.1001/jama.1977.03280190032022
Kisicki, J. C. M. D., Fiske, K. M. P. H., and Lyne, A. M. C. (2007). Phase I, double-blind, randomized, placebo-controlled, dose-escalation study of the effects on blood pressure of abrupt cessation versus taper down of guanfacine extended-release tablets in adults aged 19 to 24 years. Clin. Ther. 29, 1967–1979. doi: 10.1016/j.clinthera.2007.09.020
Lange, R. A., and Hillis, L. D. (2001). Cardiovascular Complications of Cocaine Use. N. England J. Med. 345, 351–358. doi: 10.1056/NEJM200108023450507
Leckman, J. F., Detlor, J., Harcherik, D. F., Ort, S., Shaywitz, B. A., and Cohen, D. J. (1985). Short- and long-term treatment of Tourette’s syndrome with clonidine: A clinical perspective. Neurology 35, 343–351. doi: 10.1212/wnl.35.3.343
Lee, T. M., Hsu, D. T., Kantor, P., Towbin, J. A., Ware, S. M., Colan, S. D., et al. (2017). Pediatric cardiomyopathies. Circ. Res. 121, 855–873. doi: 10.1161/CIRCRESAHA.116.309386
Liang, E. F., Lim, S. Z., Tam, W. W., Ho, C. S., Zhang, M. W., McIntyre, R. S., et al. (2018). The effect of methylphenidate and atomoxetine on heart rate and systolic blood pressure in young people and adults with attention-deficit hyperactivity disorder (ADHD): Systematic review, meta-analysis, and meta-regression. Int. J. Environ. Res. Public Health. 15:1789. doi: 10.3390/ijerph15081789
Liu, H., Feng, W., and Zhang, D. (2018). Association of ADHD medications with the risk of cardiovascular diseases: A meta-analysis. Eur. Child Adolesc. Psychiatry 28, 1283–1293. doi: 10.1007/s00787-018-1217-x
Loghin, C., Haber, H., Beasley, C. M., Kothare, P. A., Kauffman, L., April, J., et al. (2013). Effects of atomoxetine on the QT interval in healthy CYP2D6 poor metabolizers: Effect of atomoxetine on cardiac repolarization. Br. J. Clin. pharmacol. 75, 549–564. doi: 10.1111/j.1365-2125.2012.04382.x
Ma, M. K., Woo, M. H., and McLeod, H. L. (2002). Genetic basis of drug metabolism. Am. J. Health Syst. Pharmacy 59, 2061–2069. doi: 10.1093/ajhp/59.21.2061
Mahle, W. T., Clancy, R. R., Moss, E. M., Gerdes, M., Jobes, D. R., and Wernovsky, G. (2000). Neurodevelopmental outcome and lifestyle assessment in school-aged and adolescent children with hypoplastic left heart syndrome. Pediatrics 105, 1082–1089. doi: 10.1542/peds.105.5.1082
Martin, P., Satin, L., Kahn, R., Robinson, A., Corcoran, M., Pulakayastha, J., et al. (2015). A thorough QT study of guanfacine. Int. J. Clin. Pharmacol. Ther. 53, 301–316. doi: 10.5414/CP202065
Martinez-Raga, J., Knecht, C., Szerman, N., and Martinez, M. I. (2012). Risk of Serious Cardiovascular Problems with Medications for Attention-Deficit Hyperactivity Disorder. CNS Drugs 27, 15–30. doi: 10.1007/s40263-012-0019-9
Mazza, M., D’Ascenzo, F., Davico, C., Biondi-Zoccai, G., Frati, G., Romagnoli, E., et al. (2013). Drugs for attention deficit–hyperactivity disorder do not increase the mid-term risk of sudden death in children: A meta-analysis of observational studies. Int. J. Cardiol. 168, 4320–4321. doi: 10.1016/j.ijcard.2013.04.169
McCarthy, S., Cranswick, N., Potts, L., Taylor, E., and Wong, I. C. K. (2009). Mortality Associated with Attention-Deficit Hyperactivity Disorder (ADHD) Drug Treatment: A retrospective cohort study of children, adolescents and young adults using the general practice research database. Drug Safe. 32, 1089–1096. doi: 10.2165/11317630-000000000-00000
Medori, R., Ramos-Quiroga, J. A., Casas, M., Kooij, J. J. S., Niemelä, A., Trott, G.-E., et al. (2008). A randomized, placebo-controlled trial of three fixed dosages of prolonged-release OROS methylphenidate in adults with attention-deficit/hyperactivity disorder. Biol. Psychiatry 63, 981–989. doi: 10.1016/j.biopsych.2007.11.008
Michelson, D., Adler, L., Spencer, T., Reimherr, F. W., West, S. A., Allen, A. J., et al. (2003). Atomoxetine in adults with ADHD: Two randomized, placebo-controlled studies. Biol. Psychiatry 53, 112–120. doi: 10.1016/S0006-3223(02)01671-2
Michelson, D., Allen, A. J., Busner, J., Casat, C., Dunn, D., Kratochvil, C., et al. (2002). Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: A randomized, placebo-controlled study. Am. J. Psychiatry 159, 1896–1901. doi: 10.1176/appi.ajp.159.11.1896
Michelson, D., Faries, D., Wernicke, J., Kelsey, D., Kendrick, K., Sallee, F. R., et al. (2001). Atomoxetine in the treatment of children and adolescents with attention-deficit/hyperactivity disorder: A randomized, placebo-controlled, dose-response study. Pediatrics 108:e83. doi: 10.1542/peds.108.5.e83
Mick, E., McManus, D. D., and Goldberg, R. J. (2012). Meta-analysis of increased heart rate and blood pressure associated with CNS stimulant treatment of ADHD in adults. Eur. Neuropsychopharmacol. 23, 534–541. doi: 10.1016/j.euroneuro.2012.06.011
Newcorn, J. (2002). “Efficacy trials of atomoxetine for ADHD in children, adolescents and adults [abstract 40B],” in Proceedings of the 49th annual meeting American Academy of Child and Adolescent Psychiatry, San Francisco, CA, 66.
Niarchou, M., Martin, J., Thapar, A., Owen, M. J., and van den Bree, M. B. M. (2015). The clinical presentation of attention deficit-hyperactivity disorder (ADHD) in children with 22q11.2 deletion syndrome. Am. J. Med. Genet. Part B 168B:730–738. doi: 10.1002/ajmg.b.32378
Norrish, G., Topriceanu, C., Qu, C., Field, E., Walsh, H., Ziółkowska, L., et al. (2021). The role of the electrocardiographic phenotype in risk stratification for sudden cardiac death in childhood hypertrophic cardiomyopathy. Eur. J. Prev. Cardiol. 29, 645–653. doi: 10.1093/eurjpc/zwab046
Nymark, T.-B., Hovland, A., Bjørnstad, H., and Nielsen, E. W. (2008). A young man with acute dilated cardiomyopathy associated with methylphenidate. Vasc. Health Risk Manag. 4, 477–479. doi: 10.2147/VHRM.S2410
Olfson, M. M. D. M. P. H., Huang, C. P. D., Gerhard, T. P. D., Winterstein, A. G. P. D., Crystal, S. P. D., Allison, P. D. P. D., et al. (2012). Stimulants and cardiovascular events in youth with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 51, 147–156. doi: 10.1016/j.jaac.2011.11.008
Page, R. L., O’Bryant, C. L., Cheng, D., Dow, T. J., Ky, B., Stein, C. M., et al. (2016). Drugs that may cause or exacerbate heart failure: A scientific statement from the american heart association. Circulation 134:e32–e69. doi: 10.1161/CIR.0000000000000426
Picarzo, J. P.-L., Malfaz, F. C., Marcos, D. C., Hernández, R. C., Soria, T. F., García, B. M., et al. (2020). Recommendations of the Spanish Society of Paediatric Cardiology and Congenital Heart Disease as regards the use of drugs in attention deficit hyperactivity disorder in children and adolescents with a known heart disease, as well as in the general paediatric population: Position statement by the Spanish Paediatric Association. Anales Pediatría 92, .e1–.e7. doi: 10.1016/j.anpedi.2019.09.002
Pliszka, S. R. (2003). Non-stimulant treatment of attention-deficit/hyperactivity disorder. CNS Spectrums 8, 253–258. doi: 10.1017/S1092852900018460
Polanczyk, G., and Rohde, L. A. (2007). Epidemiology of attention-deficit/hyperactivity disorder across the lifespan. Curr. Opin. Psychiatry 20, 386–392. doi: 10.1097/YCO.0b013e3281568d7a
Reichart, D., Magnussen, C., Zeller, T., and Blankenberg, S. (2019). Dilated cardiomyopathy: From epidemiologic to genetic phenotypes: A translational review of current literature. J. Intern. Med. 286, 362–372. doi: 10.1111/joim.12944
Reid, J. L., Campbell, B. C., and Hamilton, C. A. (1984). Withdrawal reactions following cessation of central α-adrenergic receptor agonists. Hypertension 6:II–71–II–5. doi: 10.1161/01.hyp.6.5_pt_2.ii71
Retz, W., Rösler, M., Ose, C., Scherag, A., Alm, B., Philipsen, A., et al. (2012). Multiscale assessment of treatment efficacy in adults with ADHD: A randomized placebo-controlled, multi-centre study with extended-release methylphenidate. World J. Biol. Psychiatry 13, 48–59. doi: 10.3109/15622975.2010.540257
Reza, S., Mohammad Nasrollahzadeh, M., Ahmad, A., and Saied, B. (2021). Effect of medetomidine on left ventricular outflow tract velocity in cats: A Doppler echocardiography study. Vet. Res. Forum 12, 383–386. doi: 10.30466/vrf.2020.113899.2710
Rösler, M., Fischer, R., Ammer, R., Ose, C., and Retz, W. (2009). A randomised, placebo-controlled, 24-week, study of low-dose extended-release methylphenidate in adults with attention-deficit/hyperactivity disorder. Eur. Arch. Psychiatry Clin. Neurosci. 259:368. doi: 10.1007/s00406-008-0845-4
Safer, D. J. (1992). Relative cardiovascular safety of psychostimulants used to treat attention-deficit hyperactivity disorder. J. Child Adolesc. Psychopharmacol. 2, 279–290. doi: 10.1089/cap.1992.2.279
Samuels, J. A., Franco, K., Wan, F., and Sorof, J. M. (2006). Effect of stimulants on 24-h ambulatory blood pressure in children with ADHD: A double-blind, randomized, cross-over trial. Pediatr. Nephrol. 21, 92–95. doi: 10.1007/s00467-005-2051-1
Schelleman, H., Bilker, W. B., Kimmel, S. E., Daniel, G. W., Newcomb, C., Guevara, J. P., et al. (2012). Methylphenidate and risk of serious cardiovascular events in adults. Am. J. Psychiatry 169, 178–185. doi: 10.1176/appi.ajp.2011.11010125
Schelleman, H., Bilker, W. B., Strom, B. L., Kimmel, S. E., Newcomb, C., Guevara, J. P., et al. (2011). Cardiovascular events and death in children exposed and unexposed to ADHD agents. Pediatrics 127, 1102–1110. doi: 10.1542/peds.2010-3371
Scherer, D., Hassel, D., Bloehs, R., Zitron, E., von Lowenstern, K., Seyler, C., et al. (2009). Selective noradrenaline reuptake inhibitor atomoxetine directly blocks hERG currents. Br. J. Pharmacol. 156, 226–236. doi: 10.1111/j.1476-5381.2008.00018.x
Schoretsanitis, G., de Leon, J., Eap, C. B., Kane, J. M., and Paulzen, M. (2019). Clinically significant drug–drug interactions with agents for attention-deficit/hyperactivity disorder. CNS Drugs. 33, 1201–1222. doi: 10.1007/s40263-019-00683-7
Sherrid, M. V. (2016). Drug therapy for hypertrophic cardiomypathy: Physiology and practice. Curr. Cardiol. Rev. 12, 52–65. doi: 10.2174/1573403x1201160126125403
Shetty, I., Silver, E. S., Hordof, A. J., Goldberg, P. H., and Liberman, L. (2011). Ablation of supraventricular tachycardia allows more liberal therapy in some children with attention-deficit-hyperactivity disorder. Pediatr. Int. 53, 715–717. doi: 10.1111/j.1442-200X.2011.03326.x
Shin, J. Y., Roughead, E. E., Park, B. J., and Pratt, N. L. (2016). Cardiovascular safety of methylphenidate among children and young people with attention-deficit/hyperactivity disorder (ADHD): Nationwide self controlled case series study. BMJ 353:i2550.
Singh, V., Wander, G., Mohan, B., Aslam, N., Tandon, R., Chhabra, S., et al. (2021). Hypertension and Size of Aortic Root – Cause-and-Effect Relationship. J. Indian Coll. Cardiol. 11:13.
Sorkin, E., and Heel, R. (1986). Guanfacine: A review of its pharmacodynamics and pharmacokinectic properties, and therapeutic efficacy in the treatment of hypertension. Drugs 31, 301–336.
Spencer, T. (2002). Results from 2 proof-of-concept, placebo-controlled studies of atomoxetine in children with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 63, 1140–1147. doi: 10.4088/jcp.v63n1209
Spencer, T. J., Adler, L. A., McGough, J. J., Muniz, R., Jiang, H., and Pestreich, L. (2007). Efficacy and safety of dexmethylphenidate extended-release capsules in adults with attention-deficit/hyperactivity disorder. Biol. Psychiatry 61, 1380–1387.
Stowe, C. D., Gardner, S. F., Gist, C. C., Schulz, E. G., and Wells, T. G. (2002). 24-hour ambulatory blood pressure monitoring in male children receiving stimulant therapy. Ann. Pharmacother. 36, 1142–1149. doi: 10.1345/aph.1A367
Strange, B. C. (2008). Once-daily treatment of ADHD with guanfacine: Patient implications. Neuropsychiatr. Dis. Treat. 4, 499–506. doi: 10.2147/ndt.s1711
Thottathil, P. B. A., Acharya, J. B. A., Moss, A. J. M. D., Jons, C. M. D., McNitt, S. M. S., Goldenberg, I. M. D., et al. (2008). Risk of Cardiac Events in Patients With Asthma and Long-QT Syndrome Treated With Beta2 Agonists. Am. J. Cardiol. 102, 871–874. doi: 10.1016/j.amjcard.2008.05.029
Tisdale, J. E., Chung, M. K., Campbell, K. B., Hammadah, M., Joglar, J. A., Leclerc, J., et al. (2020). Drug-induced arrhythmias: A scientific statement from the american heart association. Circulation 142:e214–e233.
Van ZwiEten, P. A., Ti-Ioolen, M. J., and Timmermans, P. B. (1984). The Hypotensive Activity and Side Effects Of Methyldopa, Clonidine, And Guanfacine. Hypertension 6:II–28–II–33.
Verplaetse, T. L., Roberts, W., Moore, K. E., Peltier, M. R., Oberleitner, L. M., and McKee, S. A. (2019). Pharmacokinetics and pharmacodynamics of immediate-release versus extended-release guanfacine in adult daily smokers. J. Clin. Psychopharmacol. 39, 124–128. doi: 10.1097/JCP.0000000000001004
Vetter, V. L., Elia, J., Erickson, C., Berger, S., Blum, N., Uzark, K., et al. (2008). Cardiovascular monitoring of children and adolescents with heart disease receiving stimulant drugs: A scientific statement from the american heart association council on cardiovascular disease in the young congenital cardiac defects committee and the council on cardiovascular nursing. Circulation 117, 2407–2423. doi: 10.1161/CIRCULATIONAHA.107.189473
Vitiello, B. B., Elliott, G. R. G. R., Swanson, J. M. J. M., Arnold, L. E. L. E., Hechtman, L. L., Abikoff, H. H., et al. (2012). Blood pressure and heart rate in the multimodal treatment of attention deficit/hyperactivity disorder study over 10 years. Am. J. Psychiatry 169, 167–177. doi: 10.1176/appi.ajp.2011.10111705
Weber, M. A. (1980). Discontinuation syndrome following cessation of treatment with clonidine and other antihypertensive agents. J. Cardiovasc. pharmacol 2:S73–S. doi: 10.1097/00005344-198000021-00008
Weisler, R. H., Biederman, J., Spencer, T. J., Wilens, T. E., Faraone, S. V., Chrisman, A. K., et al. (2006). Mixed amphetamine salts extended-release in the treatment of adult adhd: A randomized. controlled trial. CNS Spectr. 11, 625–639.
Wernicke, J. F., Faries, D., Girod, D., Brown, J. W., Gao, H., Kelsey, D., et al. (2003). Cardiovascular effects of atomoxetine in children, adolescents, and adults. Drug Safe. 26, 729–740.
Westover, A. N., and Halm, E. A. (2012). Do prescription stimulants increase the risk of adverse cardiovascular events?: A systematic review. BMC Cardiovasc. Disord. 12:41. doi: 10.1186/1471-2261-12-41
Westover, A. N., McBride, S., and Haley, R. W. (2007). Stroke in young adults who abuse amphetamines or cocaine: A population-based study of hospitalized patients. Arch. General Psychiatry 64, 495–502.
Wilens, T. E., Biederman, J., and Lerner, M. (2004). Effects of once-daily osmotic-release methylphenidate on blood pressure and heart rate in children with attention-deficit/hyperactivity disorder: Results from a one-year follow-up study. J. Clin. Psychopharmacol. 24, 36–41. doi: 10.1097/01.jcp.0000106223.36344.df
Winterstein, A. G., Gerhard, T., Shuster, J., Johnson, M., Zito, J. M., and Saidi, A. (2007). Cardiac safety of central nervous system stimulants in children and adolescents with attention-deficit/hyperactivity disorder. Pediatrics 120:e1494–e1501.
Yasuda, S. U., Zhang, L., and Huang, S. M. (2008). The role of ethnicity in variability in response to drugs: focus on clinical pharmacology studies. Clin. Pharmacol. Ther. 84, 417–423.
Zhang, C., Kutyifa, V., Moss, A. J., McNitt, S., Zareba, W., and Kaufman, E. S. (2015). Long-QT syndrome and therapy for attention deficit/hyperactivity disorder. J. Cardiovasc. Electrophysiol. 26, 1039–1044.
Zhang, Y.-H., and Zhu, J. (1998). Suppressing sympathetic activation with clonidine on ventricular arrhythmias in congestive heart failure. Int. J. Cardiol. 65, 233–238. doi: 10.1016/s0167-5273(98)00127-2
Keywords: ADHD (attention deficit and hyperactivity disorder), cardiovascular disease, stimulant medications for ADHD, non-stimulant medications for ADHD, electrocardiogram (ECG), blood pressure, cardiomyopathies, aortopathies
Citation: Topriceanu C-C, Moon JC, Captur G and Perera B (2022) The use of attention-deficit hyperactivity disorder medications in cardiac disease. Front. Neurosci. 16:1020961. doi: 10.3389/fnins.2022.1020961
Received: 16 August 2022; Accepted: 03 October 2022;
Published: 19 October 2022.
Edited by:
William Davies, Cardiff University, United KingdomReviewed by:
Yuyang Luo, Massachusetts Eye and Ear Infirmary and Harvard Medical School, United StatesCopyright © 2022 Topriceanu, Moon, Captur and Perera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Constantin-Cristian Topriceanu, emNoYXRvcEB1Y2wuYWMudWs=
†These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.