 Simon Outram1*
Simon Outram1* Katrina A. Muñoz2
Katrina A. Muñoz2 Kristin Kostick-Quenet2
Kristin Kostick-Quenet2 Clarissa E. Sanchez2Lavina Kalwani2Richa Lavingia3
Clarissa E. Sanchez2Lavina Kalwani2Richa Lavingia3 Laura Torgerson2
Laura Torgerson2 Demetrio Sierra-Mercado2,4Jill O. Robinson2
Demetrio Sierra-Mercado2,4Jill O. Robinson2 Stacey Pereira2Barbara A. Koenig1
Stacey Pereira2Barbara A. Koenig1 Philip A. Starr5
Philip A. Starr5 Aysegul Gunduz6,7
Aysegul Gunduz6,7 Kelly D. Foote6
Kelly D. Foote6 Michael S. Okun6
Michael S. Okun6 Wayne K. Goodman8
Wayne K. Goodman8 Amy L. McGuire2Peter Zuk2
Amy L. McGuire2Peter Zuk2 Gabriel Lázaro-Muñoz2
Gabriel Lázaro-Muñoz2- 1Program in Bioethics, University of California, San Francisco, San Francisco, CA, United States
- 2Center for Medical Ethics and Health Policy, Baylor College of Medicine, Houston, TX, United States
- 3Baylor College of Medicine, Houston, TX, United States
- 4Department of Anatomy and Neurobiology, School of Medicine, University of Puerto Rico, San Juan, Puerto Rico
- 5Department of Neurosurgery, University of California, San Francisco, San Francisco, CA, United States
- 6Fixel Institute for Neurological Diseases, Program for Movement Disorders and Neurorestoration, Department of Neurology, University of Florida, Gainesville, FL, United States
- 7Department of Biomedical Engineering, University of Florida, Gainesville, FL, United States
- 8Department of Psychiatry and Behavioral Sciences, Baylor College of Medicine, Houston, TX, United States
This research study provides patient and caregiver perspectives as to whether or not to undergo adaptive deep brain stimulation (aDBS) research. A total of 51 interviews were conducted in a multi-site study including patients undergoing aDBS and their respective caregivers along with persons declining aDBS. Reasons highlighted for undergoing aDBS included hopes for symptom alleviation, declining quality of life, desirability of being in research, and altruism. The primary reasons for not undergoing aDBS issues were practical rather than specific to aDBS technology, although some persons highlighted a desire to not be the first to trial the new technology. These themes are discussed in the context of “push” factors wherein any form of surgical intervention is preferable to none and “pull” factors wherein opportunities to contribute to science combine with hopes and/or expectations for the alleviation of symptoms. We highlight the significance of study design in decision making. aDBS is an innovative technology and not a completely new technology. Many participants expressed value in being part of research as an important consideration. We suggest that there are important implications when comparing patient perspectives vs. theoretical perspectives on the choice for or against aDBS. Additionally, it will be important how we communicate with patients especially in reference to the complexity of study design. Ultimately, this study reveals that there are benefits and potential risks when choosing a research study that involves implantation of a medical device.
Introduction
Deep brain stimulation (DBS) is a well-established neurosurgical procedure whereby electrodes are surgically implanted into the brain to address common motor symptoms associated with movement disorders. For just over two decades, DBS has had remarkable success in the alleviation of select symptoms relating to Parkinson’s disease (PD) and has become an important therapy for motor symptoms and movement disorders (Hariz, 2017; Hartmann et al., 2019; Artusi et al., 2020). Given the relative success of DBS, there has been considerable interest in whether DBS might be used for treating other brain disorders including Alzheimer’s disease, obsessive compulsive disorder (OCD), and Tourette syndrome. A body of literature has emerged exploring both the likely efficacy and the ethical implications of a broader application of DBS, especially focusing upon the medical and ethical implications of addressing psychological symptomologies as opposed to motor symptoms (Widge et al., 2016a,b; Siegel et al., 2017; Aldehri et al., 2018; Lawrence et al., 2018; Viaña and Gilbert, 2019; Vicheva et al., 2020; Xu et al., 2020; Bonomo and Vetrano, 2021; Smith et al., 2021).
In addition to potentially broadening the scope of DBS usage, an innovative form of DBS is being trialed—known as adaptive deep brain stimulation (aDBS) or closed loop DBS—wherein a sensor electrode is employed to track fluctuations in brain activity possibly associated with clinical symptoms and the system is programmed to deploy or to adjust the level of stimulation (Habets et al., 2018; Swann et al., 2018; Little and Brown, 2020). In part, the development of aDBS was in response to some of the side effects of conventional DBS, including dysarthria, imbalance, hypomania, and dyskinesia as there was an inability to reduce these side effects by adjusting stimulation in real time (Widge et al., 2016b; Habets et al., 2018). By addressing this limitation, aDBS theoretically would be able to provide a more personalized or tailored program of stimulation, thus reducing the likelihood of over- or under-stimulation. Moreover, since this strategy does not employ continuous stimulation, aDBS technology has the potential to increase battery life, decreasing surgeries, and thus reducing morbidities associated with battery replacement surgeries. aDBS does, however, raise philosophical questions about the capacity of the device to stimulate or not stimulate without human input. As Klein et al. (2016) have penned, aDBS is a distinctly novel form of neuromodulation by which “one has effectively constructed a device that autonomously determines what the patient may or may not feel.” This has raised concerns about the impact of aDBS on personal autonomy given that that the algorithm self-directs the stimulation (Goering et al., 2017; Lázaro-Muñoz et al., 2017; Kostick and Lázaro-Muñoz, 2021).
These philosophical concerns may or may not play a role in the decision-making process of prospective DBS surgery patients. Individuals considering aDBS must decide (i) whether they feel brain surgery of any type is their best option, (ii) whether they feel that experimental aDBS is preferable to standard—non-adaptive—DBS (if available for their condition), and (iii) whether they want to be part of a research study (given that aDBS is only offered as part of research rather than as standard clinical practice). The following manuscript provides empirical data on how patients and caregivers reach a decision on accepting or declining aDBS surgery for the alleviation of the symptoms of dystonia, OCD, essential tremor, PD, and Tourette syndrome.
Methods and Analysis
This study was embedded into aDBS clinical trials at Baylor College of Medicine, UCSF, and the University of Florida. Clinicaltrial.gov numbers are as follows: Baylor College of Medicine—NCT03457675, NCT04281134; UCSF—NCT03131817, NCT01934296, and NCT03582891; University of Florida—NCT02649166, NCT02056873. Semi-structured interviews were conducted with trial patients and their caregivers using a similar set of questions, both prior to surgery and approximately 6 months post-surgery. Individuals who decided not to participate in the aDBS trial were interviewed at one time point post-decline. Interviews were conducted in person or via Zoom/phone and lasted an average of 30–35 min for patients and caregivers and 20–25 min for decliners. The interviews were audio recorded and transcribed verbatim, with consent. All transcripts were de-identified prior to analysis. This study was approved by the Baylor College of Medicine Institutional Review Board.
Each interview cohort (patients, patient caregivers, and study decliners) was asked about the decision to participate or not to participate in a trial which would implant aDBS: Why did you decide to enroll in the study? (patients); what do you think about the patient’s decision to enroll in the study (patient caregivers); why did you decide not to enroll in the study? (study decliners). To identify patient responses to these questions, two members of the research team independently coded each interview transcript using MAXQDA 2018 qualitative data analysis software (Kuckartz). In line with established principles of qualitative research, we conducted interviews until reaching theme saturation, understood as a point at which interviewees were no longer raising novel themes relative to previous interviewees (Saunders et al., 2018). These text segments were then progressively abstracted (SO) utilizing thematic content analysis to identity a set of themes and sub-themes, which were corroborated (KM). The frequencies were not intended to suggest any level of statistical significance but were treated as descriptive data detailing how often a particular theme emerged organically and/or in response to interview questions.
Results
Response rate were as follows: Response rates: 21 out of 23 patients = 91.3%, 20 out of 20 caregivers, and 10 out of 14 decliners = 71.4%. Of the 21 patients who agreed to interview, all but one had a respective caregiver who was also interviewed. One patient did not feel there was anyone who counted as being in a caregiver role for them. Demographic variables are provided to indicate the characteristics of the population interviewed (see Tables 1–3). Although data was reviewed to see if there were any immediately evident differences in population characteristics between patients and decliners, the small size of the population precluded further detailed statistical analysis.
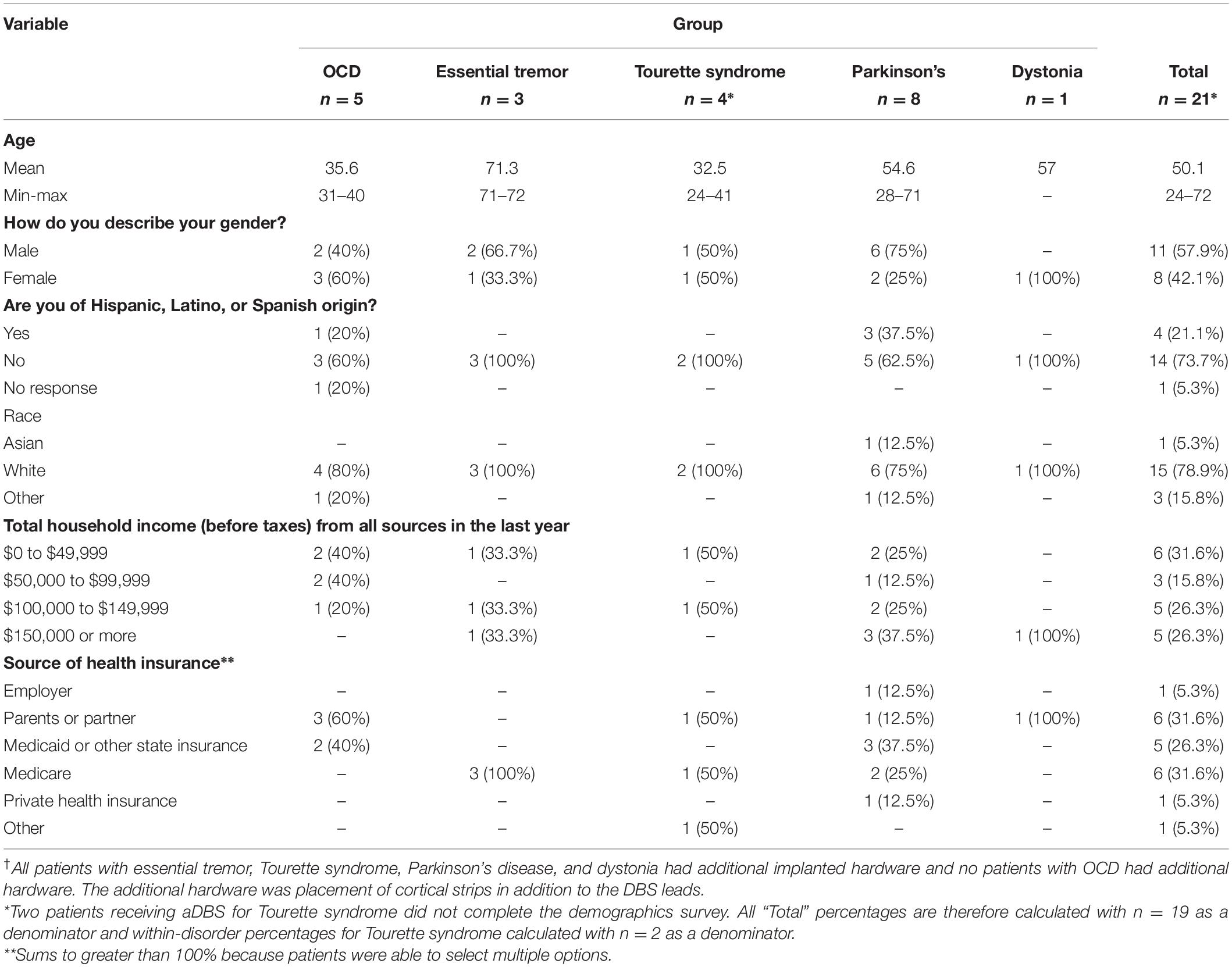
Table 1. Patient demographics†.
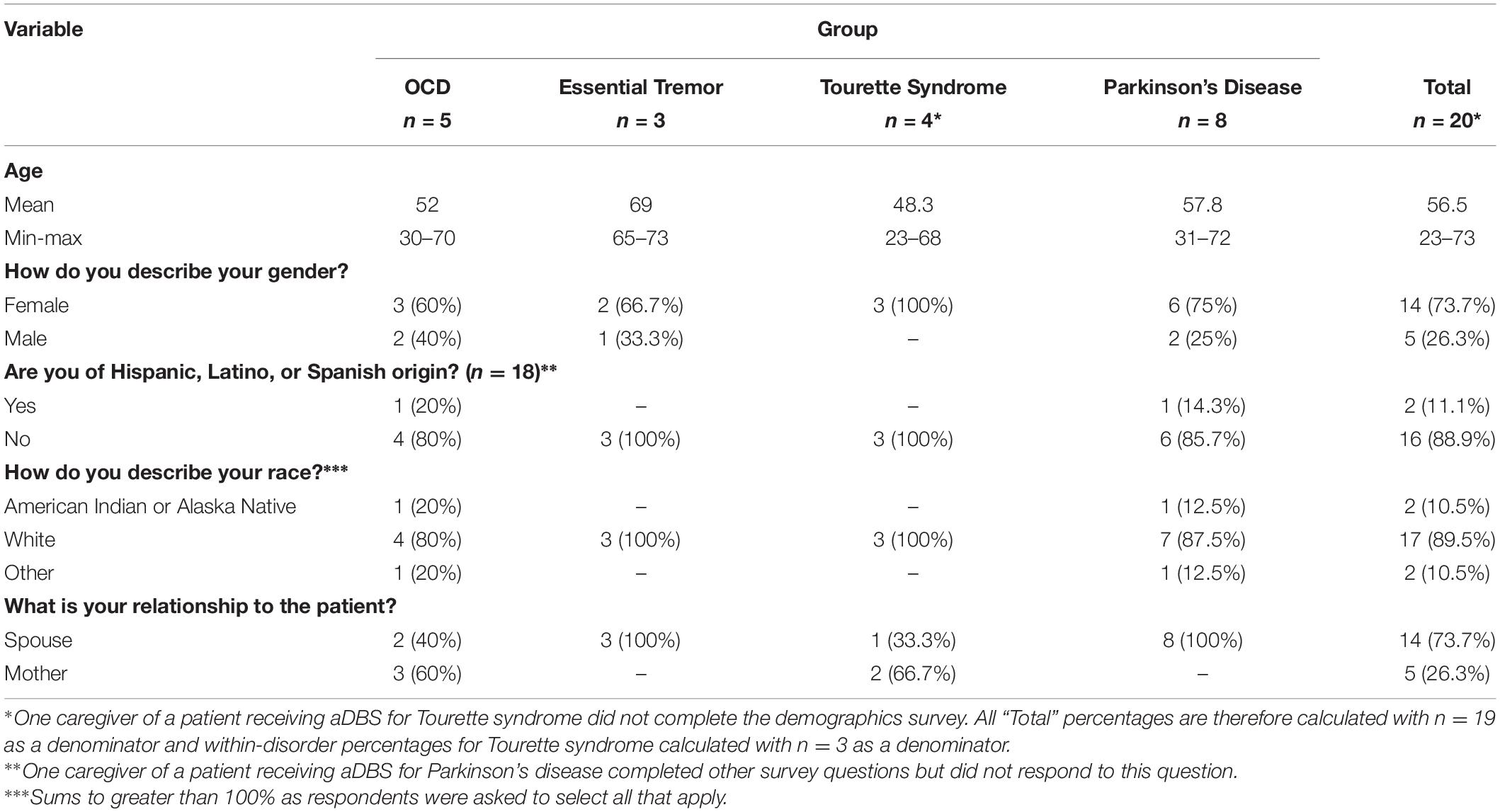
Table 2. Caregiver demographics.
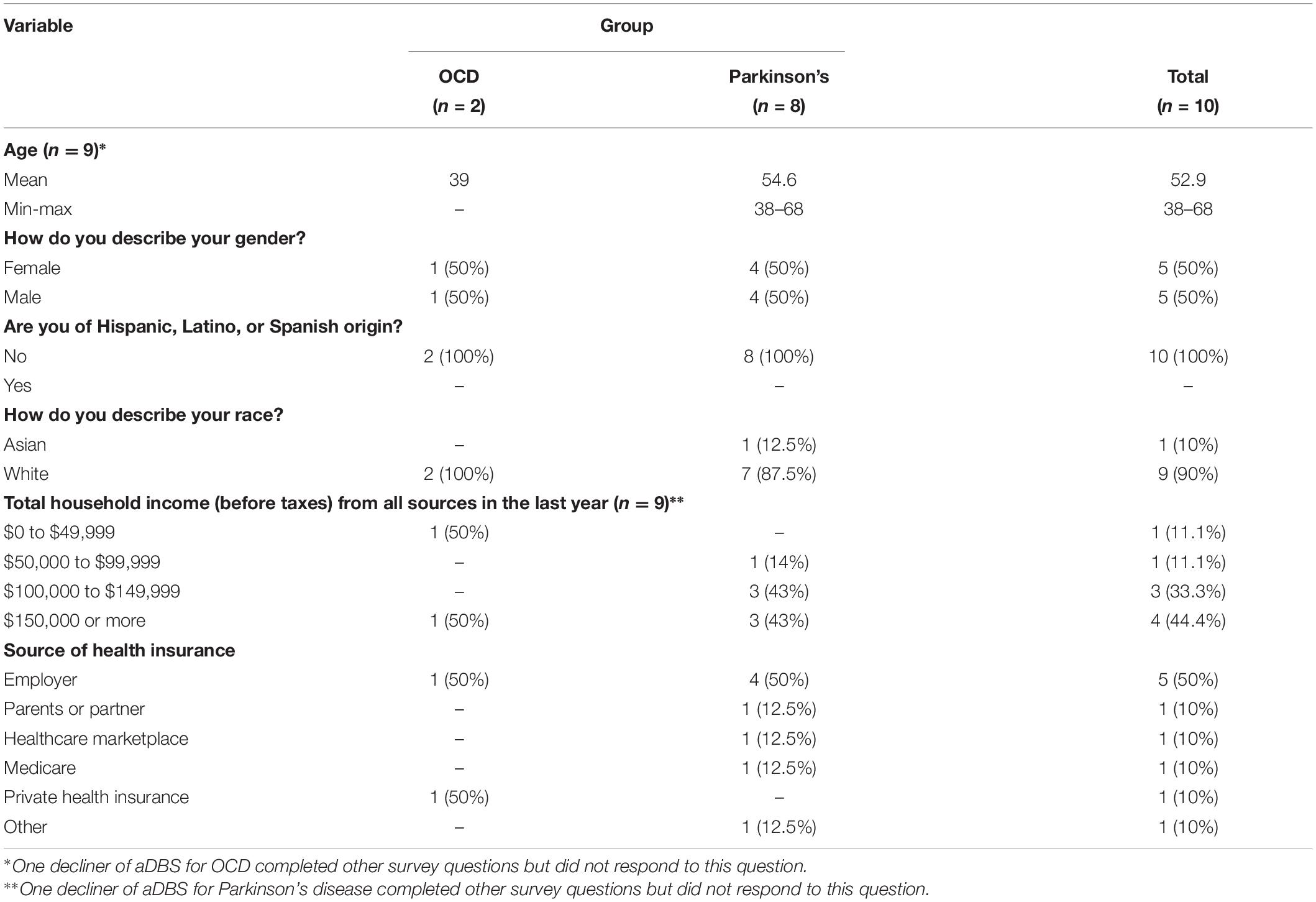
Table 3. Decliner demographics.
It may be of note that most decliners (7) were high-income (>$100,000), while just under half of patients were. Figures were too small to draw any conclusions from this difference. It should also be noted that income figures are difficult to compare due to major differences between states in respect to cost of living and average income. Nearly all patients received health care through either parents/partner (6), Medicaid (7), or Medicare (6). Only one patient received health care through their employer. By contrast, only half (5) of decliners received health care through their employer, only 1 through parent/partner, only 1 through Medicare, and 0 through Medicaid. Again, figures are too small to draw conclusions about these differences.
A condensed summary providing frequency of themes for undergoing aDBS is provided in Table 4, below.
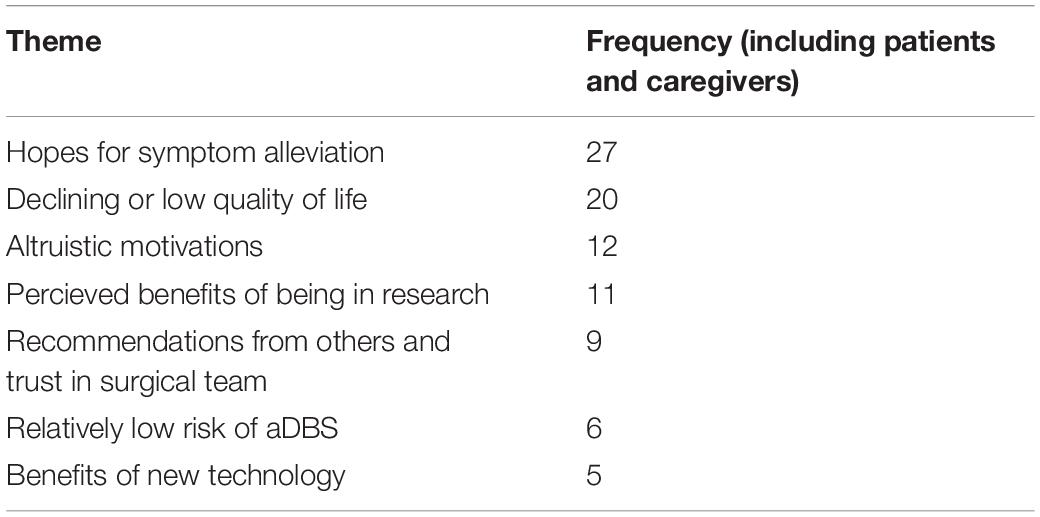
Table 4. Relative frequency of themes for undergoing aDBS.
Patients’ and Caregivers’ Reasons for Trial Participation
Hopes for Symptom Alleviation Through aDBS
Hopes for symptom alleviation from aDBS surgery played a significant role in the decision-making process. In total, 27 out of 41 interviewees (66%) expressed hope for some form of benefit from aDBS. A greater percentage of patients shared that they were hopeful that the surgery would alleviate their symptoms (17/21, 81%) than caregivers (10/20, 50%). As Table 5 indicates, interviewees tended to see aDBS as a good option given the circumstances; they recognized that although it may not work, they felt there was nothing to lose at this point in their disease progression. However, even some patients who self-identified as reasonably healthy decided to enroll in an aDBS trial, hoping that it would prevent their symptoms from getting worse (see final quote in Table 5).
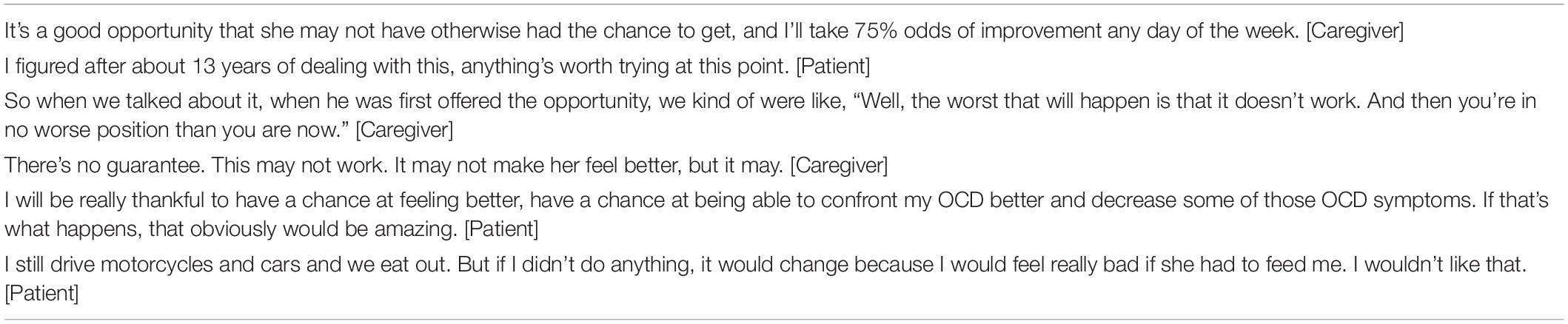
Table 5. Hope for improvement of symptoms.
Quality of Life
Relatedly, about half of the interviewees (20/41, 49%) reported a decline in quality of life as a reason for trial participation, with 14/21 (67%) patients and 6/20 (30%) caregivers raising quality of life issues as a rationale for choosing to have aDBS surgery (see Table 6, below).
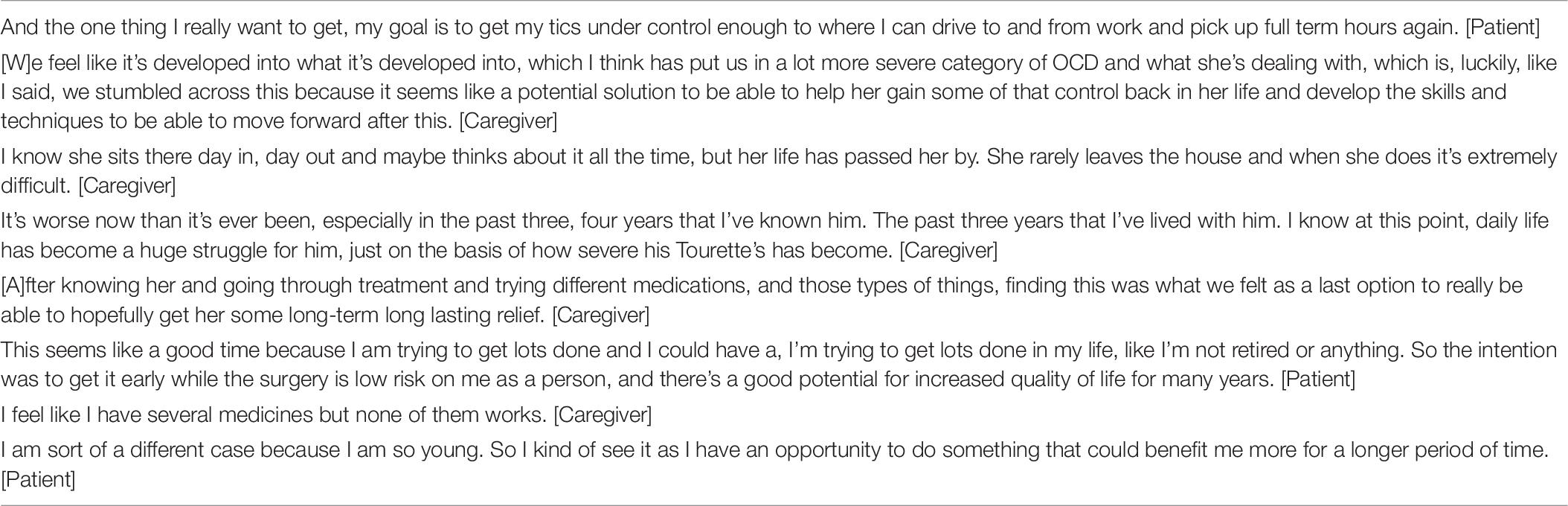
Table 6. Quality of life.
The Desirability of Being in Research
A number of patients 11/41 (27%; including nine patients and two caregivers) referred to being in a research trial—rather than specific benefits of aDBS—as being an important consideration in choosing to enter the respective study. These considerations were largely centered upon the benefits of being closely monitored as a research patient and a generalizable technological enthusiasm. Finally, receiving treatment free of charge due to being in research was specifically raised by two patients (see Table 7, below).
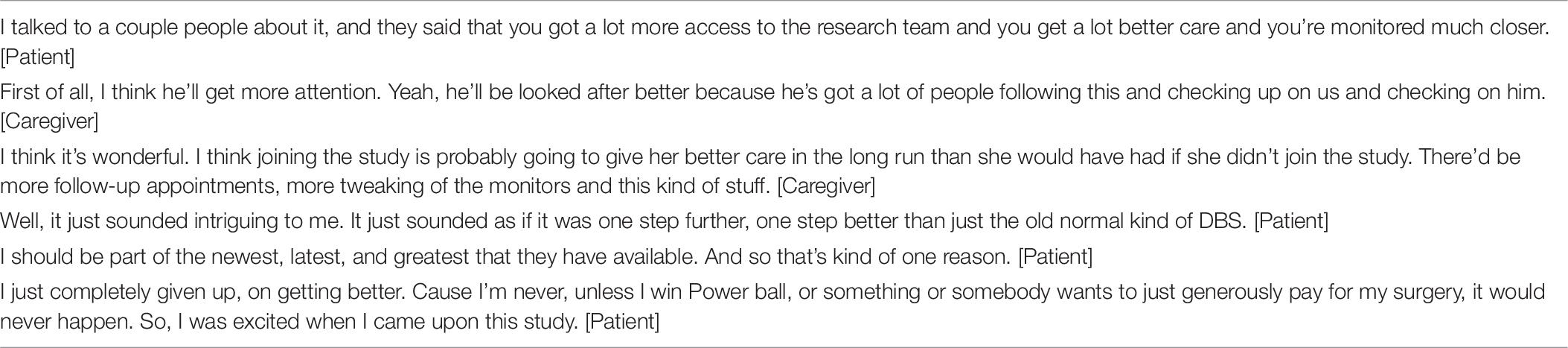
Table 7. Benefits of being in research.
Altruism and Helping Oneself
Altruism was another of the more frequently occurring rationales for electing to participate in an aDBS trial, with 12/41 (29%) of interviewees referring to one or more forms of altruistic rationale. As summarized in Table 8, the expression of altruism varied significantly, from hoping to contribute to science, to helping others with the same condition, to potentially helping future patients or family members. Often, the distinction between each was blurred or different expressions of altruism were referred to by the same interviewee. It is notable that altruism was expressed far more often by patients (11/21) than caregivers (1/20), suggesting patients might see themselves as directly giving or contributing more often than caregivers. It is possible that patients felt more justified in deciding to undergo brain surgery on themselves for altruistic reasons, while caregivers primarily thought about benefits and risks to the patient rather than the general population (see Table 8, below).

Table 8. Expressions of altruism.
It is important to note that for several interviewees, altruism was not an exclusive motivation but instead was combined with the hope that the technology would improve their own lives, as illustrated in the following quotes:
From a selfish standpoint I want to try it, but also from a standpoint of helping me, helping the research, I felt that it would be good to participate. [Patient]
If I can add on a little bit that could possibly help down the road for myself or other people, great. That to me is worth it. [Patient]
At first, I really liked the idea that it could help further OCD research, just that of course, first and foremost, I will be really thankful to have a chance at feeling better. [Patient]
Recommendations From Others
Although perhaps relatively non-controversial, an important consideration among interviewees was the advice of others that undertaking to have aDBS would be a good choice. This particularly related to advice from a patient’s primary care provider. A total of nine interviewees (22%) including seven patients and two caregivers indicated that this was important in their decision making. Table 9 provides illustrative excerpts from interviews on this subject.

Table 9. Recommendations from others.
Study Decliners’ Reasons for Not Enrolling in an aDBS Trial
Study decliners provided a range of rationales for why they chose to decline aDBS (Table 10). The primary rationale for declining was practical, with 7 out of 10 (70%) highlighting that they declined aDBS because the study was located inconveniently, involved too much time in follow-up, or was not scheduled in manner that was convenient to them. Other factors were more specific and include not being able to have an MRI (20% of decliners), people seeing the wires (20% of decliners), and concerns over health insurance (20%).

Table 10. Specific reasons not to have aDBS.
Balancing the Risks and Benefits of aDBS Surgery as Novel Technology
The status of aDBS as a novel form of technology was a key consideration for both patients and individuals declining aDBS. Patients tended to view the novelty of the technology as a positive, or opportunity to offer a more personalized and improved treatment system (newer = better), while study decliners saw it more negatively, as simply too experimental and risky (hesitancy to be among the first). It may be interesting to highlight that of total number of patients and caregivers interviewed, only 5 out of 41 (12%) referred specifically to the new technology as reason for choosing to have aDBS. A far greater percentage, 5 out of 10 decliners (50%) referred to concerns over new technology as one of the reasons for not undertaking to have aDBS (see Table 11, below).

Table 11. Evaluation of aDBS’s novelty.
Another theme that emerged was how for several participants aDBS was considered a relatively low additional risk in comparison to DBS. Six interviewees (five study participants and two caregivers) referred to their decision being influenced by this perception of relatively minimal extra risk of having aDBS, as compared to conventional DBS (see Table 12). It was notable that of the six interviewees referring to this issue, all but one were from the PD cohort.

Table 12. Additional risk of aDBS over conventional DBS.
Discussion
Of those issues considered important in decision-making by persons who enrolled in aDBS, hopes for alleviation of symptoms and declining quality of life often arose together as reasons to have aDBS surgery. Another of the more frequently cited rationales for having aDBS was that being in research would provide access to a team of experts that might not otherwise be made available in standard clinical practice. Altruism also featured as an important rationale and was often combined with a hope that surgery might benefit the patient. Finally, personal recommendations from physicians or friends featured reasons to undergo aDBS surgery. Persons declining aDBS cited inconvenience, time commitments, and concerns about health insurance coverage as reasons not to undertake aDBS surgery. Finally, it was notable how relative risk featured in these deliberations in respect to the technology on offer. For some, the offer of a novel, experimental technology was considered a positive attribute and thus inclined them toward choosing aDBS. For others, the experimental nature of the technology concerned them and was a reason (among others) not to have aDBS. For a third group, the additional risk of being part of trial was counterbalanced by the knowledge that the adaptive element of aDBS, if ineffective, could be de-activated, allowing them to revert to standard DBS technology; as such, they saw the additional risk of aDBS over DBS as minimal compared to the overall risk of brain surgery itself. Notably absent from the decision making process was either an explicit enthusiasm or concern regarding the automaticity of the adaptive system. This is interesting both because automaticity (i.e., automatic change in stimulation using aDBS) has been raised in respect to potential concerns about aDBS (as seen above—Goering et al., 2017; Lázaro-Muñoz et al., 2017; Kostick and Lázaro-Muñoz, 2021) and that trust in automaticity has been seen as important factor in public enthusiasm (or otherwise) for other forms of automated technology such as automated cars (Jian et al., 2000; Hoff and Bashir, 2015; Schaefer et al., 2016). In part, this may be an artifact of the study question design wherein the purpose was to find the primary reason or reasons for entry into the study or non-enrollment. One could speculate that the enthusiasm or distrust of automaticity might still be part of the decision making process, but it did not appear high on agenda when considering the decision to have aDSB or decline aDBS. In a study being conducted at present, the research team is exploring interviewees’ understandings of the specific features of aDBS including automatic stimulation.
This study provides much needed empirical data on reasons for and against electing to surgically implant a neural device that is both innovative and potential ethically complex due to software algorithm-based control of an individual’s brain stimulation treatment in real time. It highlights the depth and breadth of considerations made in choosing whether to enter or decline aDBS research trials, and brings to the fore those elements of the decision that are important to persons themselves making this decision. These empirical decision-making factors include “push” factors wherein any form of surgical intervention is preferable to none and “pull” factors wherein opportunities to contribute to science combine with hopes and/or expectations for the alleviation of symptoms. Interviewee responses highlight that, regardless of whether they decided to participate in an aDBS trial or now, this was a decision made after considerable deliberation and often in consultation with others; as seen in respect to the number of people considering recommendations from others. No single issue determined whether someone elected to have aDBS or chose to decline. This depth of consideration reflects similar findings by Lawrence et al. (2018), who write in the context of conventional DBS that “participants seemed very aware of the risks, and very aware of their own difficulties processing information, and there was no indication that participants would make quick decisions to undergo DBS.”
Our findings suggest that those who chose to undergo aDBS often did so through either by reason of wanting to help others or a combination of altruism and a desire to help oneself. As similar complex interplay is found in a study by Locock and Smith (2011) in their own study of who takes part in such trials, whereby they conclude “While altruistic motivations were undoubtedly present in our participants’ decisions, potential personal benefit emerged as the prime motivator in this group of respondents. Where altruistic reasons were expressed, they tended to be in combination with personal reasons, or to be founded more on notions of ‘social exchange,’ than any purely selfless motivation.” In an additional complexity, altruism was expressed through a broad spectrum of rationales for having aDBS ranging from helping to forward scientific and human progress to a much closer identification of the community of persons suffering from the same or similar symptoms and even to personal identification of other persons who may benefit as a result of the individual joining the research. McCann et al. (2010) suggest that the term “conditional altruism” can be helpful when characterizing the decision to enter randomized control trials and “trial participation seemed to be something of a ‘win: win’ situation—one in which they [trial participants] could both help others and benefit (or at least not be harmed) personally.” The incorporation of scientific objectives as part of the individuals’ altruistic thinking may well have enabled the sort of win/win expectation, or at the very least one win out of a potential two.
The data also highlight the degree to which participants do not conceptualize their participation in terms of a clear boundary between research and clinical objectives. Rather than constituting a therapeutic misconception (see Appelbaum et al., 1987; McConville, 2017 for discussion of this term), we suggest that this blurred line of distinction reflects study designs wherein aDBS is an extension of existing technology that can be switched off if it proves to be ineffective or associated with undesirable side effects. Persons considering whether to have aDBS surgery as part of research weighed the advantages and disadvantages and chose accordingly; they did not deny the possibility of disadvantages in entering into the research process, but factored this into their decision-making. It is argued that interviewees were aware of the research vs. clinical distinction but, when choosing to undertake aDBS surgery, explicitly combined the scientific objective of creating generalizable knowledge with at least a hope that aDBS would alleviate their symptoms. In doing so, they blended the scientific objective—which some incorporated as their own motivation—with what might be referred to as qualified expectation of clinical benefit.
It is important to highlight—as some participants articulated—that if participant enrolls in the trial and gets aDBS, there still an option to turn off the adaptive component and treat them with conventional DBS. Mergenthaler et al. (2021) have referred to “opportunity studies” vs. “experimental trials.” In the former, there is likely to be only “a marginal increase in risk over the risk associated with the clinical intervention itself,” while in the case of experimental trials, investigators test devices as “stand-alone procedures” and subjects are “unlikely to receive neurosurgery if not for enrollment in research.” These offer very different contexts for choice and perceptions of risk. These considerations influence not only decision making about entering into a trial but also post-trial concerns about continued access to experimental technology or removal of such technology (the subject of a forthcoming manuscript by the team). In some cases, interviewees appear to express a clear understanding that they were entering into what Mergenthaler refers to as an “opportunity” study but it remains unclear as to the degree to which others fully understood this complex research/clinical relationship and the possibility of switching from aDBS to DBS.
One of the more notable expectations of aDBS was that rather than specifically alleviating symptoms, some saw aDBS surgery as an opportunity to maintain their existing quality of life by preventing decline, sometimes specifically identifying having a number of high-quality years still available to them if aDBS is successful (Schuepbach et al., 2019 for recent discussion of early stage intervention and quality of life). While these were patients with diagnosed disease who have symptoms and diagnosed condition, to a limited extent their comments raise a number of questions regarding the timing of surgical intervention. It is important to note that we do not have a clear understanding of whether DBS or aDBS can reverse symptoms for all conditions or slow the progression of the disease.
Finally, arguably, the most provocative and significant finding is that some people perceive the experimental aspect of their participation as positive (where they are first in line to receive a promising new treatment), while others perceive it as negative (that they are first in line to be “guinea pigs” for a treatment with potentially negative down-the-road consequences). As such, our findings suggest a strong need to re-address the theoretical perception of research as being largely one of additional risk, over and above clinical practice (see Lantos, 2014). As our interviews suggest, a considerable number of persons were drawn toward having aDBS because they felt that being part of research would be advantageous to them. In doing so, they often merged technological enthusiasm, wanting the best and newest technology, and an expectation of greater care and attention. These expectations are well worth considering in respect to broader literature on patient perspectives on entering into research (McCann et al., 2010, 2013; Locock and Smith, 2011; Jenkins et al., 2013; Hughes-Morley et al., 2015).
Limitations
These in-depth interviews were intended to identify the range of responses that were offered by interviewees when discussing their choice to enter or decline aDBS trial participation. This approach is limited in the sense that it cannot provide generalizable results as it is restricted to these specific responses. Though we reached theme saturation in all three interviewee cohorts—participants, caregivers, and decliners—substantially more people interviewed were patients and respective caregivers, which biases our analysis to this perspective in respect to the depth of analysis.
Conclusion
Our study highlights the requirement to improve our understanding of the considerations made in choosing whether to undergo aDBS surgery as part of research. Looking in detail at this choice making process is strongly suggestive of the need to reflect upon some of the more theoretically based concerns about aDBS raised and compare these to rationales expressed by patients, caregivers, and decliners about their choice to enter or decline aDBS. In addition, the study highlights the need for further research into how prospective study enrollees come to understand complex study protocols wherein an innovative technology is overlaid with an established clinical procedure. By improving our empirical knowledge of choice-making within this context, we should be able to improve our communication strategies, thus minimizing the likelihood of unwarranted expectations and misunderstandings of what is an inherently complex study protocol. Finally, in the light our findings that many participants viewed research as positive, the study highlights that we need to pay close attention to what patients believe are the benefits of being in research. In doing so, we can be better placed to make sure that such expectations are met.
Data Availability Statement
The datasets presented in this article are not readily available as raw data will not be shared outside of the research team. Upon request, sections of the data may be provided for specific requests after the permissions of participants are requested and received.
Ethics Statement
The studies involving human participants were reviewed and approved by the Baylor College of Medicine Institutional Review Board. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
SO wrote the first draft. GL-M, PZ, AM, WG, BK, LT, SP, JR, and KK-Q contributed to conception and design. KM, KK-Q, CS, LK, RL, LT, DS-M, JR, BK, PS, AG, KF, MO, WG, AM, PZ, and GL-M contributed to recruitment and implementation. SO, KK-Q, KM, CS, LK, RL, LT, and PZ analyzed the data. PZ, KK-Q, AM, SP, and GL-M wrote sections of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version of the manuscript.
Funding
This research for this article was funded by the BRAIN Initiative-National Institutes of Health (NIH), parent grant R01MH114854 and supplemental grant R01MH114854-01S1 (GL-M, AM, and WG).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor declared a shared affiliation with three of the authors, SO, BK, and PS, at the time of review.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aldehri, M., Temel, Y., Alnaami, I., Jahanshahi, A., and Hescham, S. (2018). Deep brain stimulation for Alzheimer’s Disease: an update. Surg. Neurol. Int. 9:58.
Appelbaum, P. S., Roth, L. H., Lidz, C. W., Benson, P., and Winslade, W. (1987). False hopes and best data: consent to research and the therapeutic misconception. Hastings Cent. Rep. 17, 20–24. doi: 10.2307/3562038
Artusi, C. A., Dwivedi, A., Romagnolo, A., Bortolani, S., Marsili, L., Imbalzano, G., et al. (2020). Differential response to pallidal deep brain stimulation among monogenic dystonias: systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 91, 426–433. doi: 10.1136/jnnp-2019-322169
Bonomo, G., and Vetrano, I. G. (2021). A systematic review of deep brain stimulation targets for obsessive-compulsive disorder. Neurosurgery 88, E456–E457.
Goering, S., Klein, E., Dougherty, D. D., and Widge, A. S. (2017). Staying in the loop: relational agency and identity in next-generation DBS for psychiatry. AJOB Neurosci. 8, 59–70. doi: 10.1080/21507740.2017.1320320
Habets, J. G., Heijmans, M., Kuijf, M. L., Janssen, M. L., Temel, Y., and Kubben, P. L. (2018). An update on adaptive deep brain stimulation in Parkinson’s disease. Mov. Disord. 33, 1834–1843.
Hariz, M. (2017). My 25 stimulating years with DBS in Parkinson’s disease. J. Parkinsons Dis. 7, S33–S41.
Hartmann, C. J., Fliegen, S., Groiss, S. J., Wojtecki, L., and Schnitzler, A. (2019). An update on best practice of deep brain stimulation in Parkinson’s disease. Ther. Adv. Neurol. Disord. 12:1756286419838096.
Hoff, K. A., and Bashir, M. (2015). Trust in automation: integrating empirical evidence on factors that influence trust. Hum. Factors 57, 407–434. doi: 10.1177/0018720814547570
Hughes-Morley, A., Young, B., Waheed, W., Small, N., and Bower, P. (2015). Factors affecting recruitment into depression trials: systematic review, meta-synthesis and conceptual framework. J. Affect. Disord. 172, 274–290. doi: 10.1016/j.jad.2014.10.005
Jenkins, V., Farewell, V., Farewell, D., Darmanin, J., Wagstaff, J., Langridge, C., et al. (2013). Drivers and barriers to patient participation in RCTs. Br. J. Cancer 108, 1402–1407. doi: 10.1038/bjc.2013.113
Jian, J. Y., Bisantz, A. M., and Drury, C. G. (2000). Foundations for an empirically determined scale of trust in automated systems. Int. J. Cogn. Ergon. 4, 53–71. doi: 10.1207/s15327566ijce0401_04
Klein, E., Goering, S., Gagne, J., Shea, C. V., Franklin, R., Zorowitz, S., et al. (2016). Brain-computer interface-based control of closed-loop brain stimulation: attitudes and ethical considerations. Brain Comput. Interfaces 3, 140–148. doi: 10.1080/2326263x.2016.1207497
Kostick, K. M., and Lázaro-Muñoz, G. (2021). Neural safeguards against global impacts of memory modification on identity: ethical and practical considerations. AJOB Neurosci. 12, 45–48. doi: 10.1080/21507740.2020.1866111
Lantos, J. D. (2014). Lessons from the controversy over the SUPPORT study. Arch. Dis. Child. Fetal Neonatal Ed. 99:F4.
Lawrence, R. E., Kaufmann, C. R., DeSilva, R. B., and Appelbaum, P. S. (2018). Patients’ beliefs about deep brain stimulation for treatment-resistant depression. AJOB Neurosci. 9, 210–218. doi: 10.1080/21507740.2018.1553897
Lázaro-Muñoz, G., McGuire, A. L., and Goodman, W. K. (2017). Should we be concerned about preserving agency and personal identity in patients with Adaptive Deep Brain Stimulation systems? AJOB Neurosci. 8, 73–75. doi: 10.1080/21507740.2017.1320337
Little, S., and Brown, P. (2020). Debugging adaptive deep brain stimulation for Parkinson’s Disease. Mov. Disord. 35, 555–561. doi: 10.1002/mds.27996
Locock, L., and Smith, L. (2011). Personal benefit, or benefiting others? Deciding whether to take part in clinical trials. Clin. Trials 8, 85–93. doi: 10.1177/1740774510392257
McCann, S. K., Campbell, M. K., and Entwistle, V. A. (2010). Reasons for participating in randomised controlled trials: conditional altruism and considerations for self. Trials 11:31.
McCann, S., Campbell, M., and Entwistle, V. (2013). Recruitment to clinical trials: a meta-ethnographic synthesis of studies of reasons for participation. J. Health Serv. Res. Policy 18, 233–241. doi: 10.1177/1355819613483126
McConville, P. (2017). Presuming patient autonomy in the face of therapeutic misconception. Bioethics 31, 711–715. doi: 10.1111/bioe.12384
Mergenthaler, J. V., Chiong, W., Dohan, D., Feler, J., Lechner, C. R., Starr, P. A., et al. (2021). A qualitative analysis of ethical perspectives on recruitment and consent for human intracranial electrophysiology studies. AJOB Neurosci. 12, 57–67. doi: 10.1080/21507740.2020.1866098
Saunders, B., Sim, J., Kingstone, T., Baker, S., Waterfield, J., Bartlam, B., et al. (2018). Saturation in qualitative research: exploring its conceptualization and operationalization. Qual. Quant. 52, 1893–1907. doi: 10.1007/s11135-017-0574-8
Schaefer, K. E., Chen, J. Y., Szalma, J. L., and Hancock, P. A. (2016). A meta-analysis of factors influencing the development of trust in automation: implications for understanding autonomy in future systems. Hum. Factors 58, 377–400. doi: 10.1177/0018720816634228
Schuepbach, W. M., Tonder, L., Schnitzler, A., Krack, P., Rau, J., Hartmann, A., et al. (2019). Quality of life predicts outcome of deep brain stimulation in early Parkinson disease. Neurology 92, e1109–e1120.
Siegel, A. M., Barrett, M. S., and Bhati, M. T. (2017). Deep brain stimulation for Alzheimer’s disease: ethical challenges for clinical research. J. Alzheimers Dis. 56, 429–439. doi: 10.3233/jad-160356
Smith, A. H., Choi, K. S., Waters, A. C., Aloysi, A., Mayberg, H. S., Kopell, B. H., et al. (2021). Replicable effects of deep brain stimulation for obsessive-compulsive disorder. Brain Stimul. 14, 1–3. doi: 10.1016/j.brs.2020.10.016
Swann, N. C., de Hemptinne, C., Thompson, M. C., Miocinovic, S., Miller, A. M., Ostrem, J. L., et al. (2018). Adaptive deep brain stimulation for Parkinson’s disease using motor cortex sensing. J. Neural Eng. 15:046006. doi: 10.1088/1741-2552/aabc9b
Viaña, J. N. M., and Gilbert, F. (2019). Deep brain stimulation for people with Alzheimer’s disease: anticipating potential effects on the tripartite self. Dementia 18, 2836–2855. doi: 10.1177/1471301218761147
Vicheva, P., Butler, M., and Shotbolt, P. (2020). Deep brain stimulation for obsessive-compulsive disorder: a systematic review of randomised controlled trials. Neurosci. Biobehav. Rev. 109, 129–138. doi: 10.1016/j.neubiorev.2020.01.007
Widge, A. S., Deckersbach, T., Eskandar, E. N., and Dougherty, D. D. (2016a). Deep brain stimulation for treatment-resistant psychiatric illnesses: what has gone wrong and what should we do next? Biol. Psychiatry 79, e9–e10.
Widge, A. S., Licon, E., Zorowitz, S., Corse, A., Arulpragasam, A. R., Camprodon, J. A., et al. (2016b). Predictors of hypomania during ventral capsule/ventral striatum deep brain stimulation. J. Neuropsychiatry Clin. Neurosci. 28, 38–44. doi: 10.1176/appi.neuropsych.15040089
Keywords: aDBS, altruism, decision-making, interviews, quality of life, research, study design, symptoms
Citation: Outram S, Muñoz KA, Kostick-Quenet K, Sanchez CE, Kalwani L, Lavingia R, Torgerson L, Sierra-Mercado D, Robinson JO, Pereira S, Koenig BA, Starr PA, Gunduz A, Foote KD, Okun MS, Goodman WK, McGuire AL, Zuk P and Lázaro-Muñoz G (2021) Patient, Caregiver, and Decliner Perspectives on Whether to Enroll in Adaptive Deep Brain Stimulation Research. Front. Neurosci. 15:734182. doi: 10.3389/fnins.2021.734182
Received: 30 June 2021; Accepted: 16 August 2021;
Published: 07 October 2021.
Edited by:
Doris D. Wang, University of California, San Francisco, United StatesReviewed by:
Ignacio Delgado Martinez, Hospital del Mar Medical Research Institute (IMIM), SpainBrent Winslow, Design Interactive, United States
Copyright © 2021 Outram, Muñoz, Kostick-Quenet, Sanchez, Kalwani, Lavingia, Torgerson, Sierra-Mercado, Robinson, Pereira, Koenig, Starr, Gunduz, Foote, Okun, Goodman, McGuire, Zuk and Lázaro-Muñoz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Simon Outram, c2ltb24ub3V0cmFtQHVjc2YuZWR1