
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci., 21 February 2020
Sec. Neurodegeneration
Volume 14 - 2020 | https://doi.org/10.3389/fnins.2020.00140
This article is part of the Research TopicOlfactory Biomarkers from Evolution to Sentinel of Neuropathologies and Opportunity for Window TherapeuticsView all 8 articles
 Victoria Van Regemorter1,2*Thomas Hummel3Flora Rosenzweig4André Mouraux2Philippe Rombaux2,4Caroline Huart2,4
Victoria Van Regemorter1,2*Thomas Hummel3Flora Rosenzweig4André Mouraux2Philippe Rombaux2,4Caroline Huart2,4Olfaction is a sense involved in a complex set of tasks, influencing eating behavior, increasing awareness of environmental hazards and affecting social communication. Surprisingly, smell disorders are very frequent, especially in the elderly population. Several recent studies conducted mostly in older subjects have demonstrated a strong association between olfactory impairment and overall mortality risk, with anosmia being even more predictive of 5 years mortality risk than cardiovascular disease. Presently, the underlying pathophysiology linking olfactory impairment to mortality remains unknown and only putative mechanisms are suggested. This review aims to examine the link between olfactory impairment and mortality and to discuss existing ideas on underlying existing mechanisms including, (1) the effect of olfactory loss on nutrition, life-threatening situations and social interactions, (2) associated neurodegenerative diseases, (3) accelerated brain aging, and (4) reflection of general health status being reflected in olfactory function.
Olfactory impairment (OI) is known to occur during the process of aging (odds ratio [OR] = 1.55 for every 5-year increase in age) (Schubert et al., 2012). It is estimated that more than 50% of the population aged between 65 and 80 years old exhibit OI, increasing to 75% above 80 years old (Doty and Kamath, 2014). Several hypotheses are proposed to explain this age-related decline of olfaction.
First, the olfactory nerve, originating from the nasal fossa, is the only cranial nerve directly exposed to the environment, which makes it vulnerable to exposure to toxins, infection, trauma, and airborne pollutants (Huart et al., 2013a, b; Ajmani et al., 2016a, b).
Second, age-related alteration of physiological processes and structural changes within the nose, olfactory epithelium, olfactory bulb and higher brain regions seem to contribute greatly to this deterioration (Cerf-Ducastel and Murphy, 2009; Doty and Kamath, 2014; Attems et al., 2015; Gunzer, 2017; Doty, 2018; Marin et al., 2018).
Third, brain aging or environmental exposure could reduce the cellular regeneration found at the different levels of the olfactory system (Huart et al., 2019).
Fourth, genetic factors could also be involved. For example, it has been shown that carriers of val/val genotype of the brain-derived neurotrophic factor (BDNF) val66met polymorphism present a marked aging-associated decline in olfactory function (Hedner et al., 2010). Apolipoprotein E (ApoE) ε4 allele carriers seem to experience greater olfactory decline than the non-carriers (Wang et al., 2002). ApoE may also contribute to neuronal regenerative processes and to the development of neurodegenerative diseases. Interestingly, the combination of ApoE ε4 allele and OI in a non-demented elderly population predicts a larger decline in global cognitive function (Borenstein Graves et al., 1999; Olofsson et al., 2009). As for cognitively impaired individuals, ApoE ε4 allele carriers also show a more significant decline in cognitive abilities as well as in odor identification (Wang et al., 2002). However, a twin study suggests low heritability coefficients regarding olfactory function (Doty et al., 2011).
Fifth, age-related OI could reflect early involvement of olfactory-related brain areas by the neuropathological processes associated with neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD). Even if the exact mechanisms underlying OI in AD and PD are not completely understood, olfactory brain structures are affected early in their courses (Braak and Del Tredici, 2017; Marin et al., 2018) and OI precedes clinical diagnosis. Regarding AD, OI may already be present in patients with mild cognitive impairment (MCI, cognitive dysfunction exceeding normal “age-related” decline, yet not meeting the criteria for dementia) (Sanford, 2017). It is known that approximately 70% of MCI patients will ultimately convert to AD (Gauthier et al., 2006). Yet, recent data converge toward the idea that olfactory-impaired MCI patients are more prone to develop AD than those without OI (Conti et al., 2013; Devanand, 2016; Adams et al., 2018; Jung et al., 2019). Overall, these findings make OI a potential early predictor for AD development. PD is also marked by early OI, which typically precedes motor symptoms by at least 5 years and thus can be used as a biomarker for the diagnosis of PD (Berardelli et al., 2013; Marin et al., 2018; Haehner et al., 2019). Moreover, a 7-year prospective study conducted in newly diagnosed PD patients reported that hyposmia at diagnosis of PD is associated with further development of cognitive deficits, making OI a predictor of dementia in this setting (Gjerde et al., 2018).
Sixth, OI has been shown to accompany a variety of diseases. In addition to the link to neurodegenerative diseases, OI has been reported to occur in schizophrenia, epilepsy, systemic and endocrine diseases (e.g., hypothyroidism, type 2 diabetes mellitus), chronic kidney or liver failure (Landis et al., 2004; Hummel et al., 2011; Huart et al., 2013a). Of note, a recent study involving type 2 diabetic patients demonstrated not only increased OI in this population compared to controls but also diminished abilities in specific cognitive tests. Besides, once again, they found a strong association between OI and specific memory impairment in this population (Yulug et al., 2019). As for smoking, which is known to interfere with olfactory performance, the effect is equivocal or weak and mostly seen in long-standing heavy smokers (Mackay-Sim et al., 2006). Alcohol’s abuse negative effects on olfaction could be related to alterations in brain areas involved in olfactory processing (Schubert et al., 2012). Higher probability of comorbidities with age comes along with the associated polypharmacy. Despite little evidence-based data, it is commonly thought that medication may affect taste and smell functions (Hummel et al., 2011). Drugs are thought to interact with many different molecular targets of the olfactory pathway from the olfactory receptors to central processes (Lötsch et al., 2012, 2015a,b). A long list of medications might be involved in smell loss, including antibiotics, antidepressant and antipsychotic drugs, antihypertensive drugs (e.g., calcium channel blockers), opioids, sildenafil (Doty and Bromley, 2004; Hummel et al., 2011). However, it is difficult to distinguish drug-induced OI from the effect of the underlying medical issue for which the drug is taken. Landis et al. (2004) did not find a correlation between olfactory function and the number of drugs taken. Nevertheless, a recent study showed a significant correlation between the number of drugs taken and both worse olfactory threshold function and, interestingly, worse MMSE scores (Ottaviano et al., 2018). The authors justified this finding by the fact that these parameters are usually age-related. However, they did not control for comorbidities, which in fact could have explained in part these results.
Until now, seven longitudinal studies have been published on the relationship between olfactory function at baseline and risk of mortality (Wilson et al., 2011; Gopinath et al., 2012; Pinto et al., 2014; Devanand et al., 2015; Schubert et al., 2016; Ekström et al., 2017; Liu et al., 2019). Demographics and methods are summarized in Table 1. Statistics and main results are summarized in Table 2. We deliberately decided to include only studies with psychophysical assessment of olfactory function using well-known validated identification tests since self-assessment of olfactory function is not reliable (Landis et al., 2003; Lötsch and Hummel, 2019; Oleszkiewicz and Hummel, 2019; Oleszkiewicz et al., in press). Together, these studies included a total of 13,366 individuals, male and female, aged 40 and older, with older people representing the majority. In regard to age groups, results vary between studies. Some found a stronger OI-mortality link in older subjects, while others demonstrated a slightly stronger relationship in middle-aged groups (Gopinath et al., 2012; Ekström et al., 2017; Liu et al., 2019). This latter finding may be due to the increased prevalence of anosmia with advancing age. Length of follow-up varied according to studies, mainly ranging from 4–5 years up to 10–13 years. Exclusion criteria, mostly including dementia or neurologic diseases, were found in four studies and are discussed below.
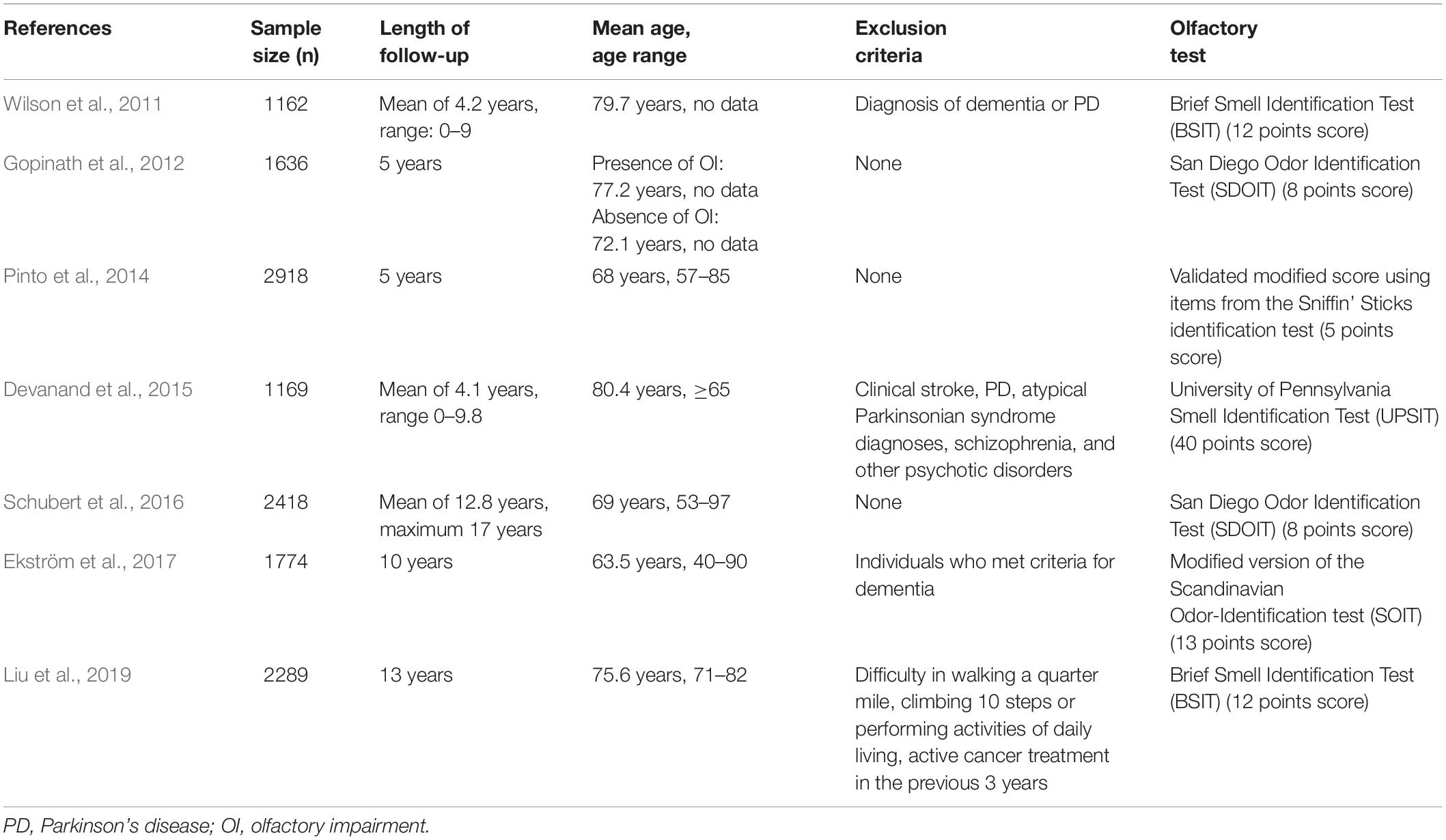
Table 1. Studies linking olfactory impairment and mortality – Demographic data and methods.
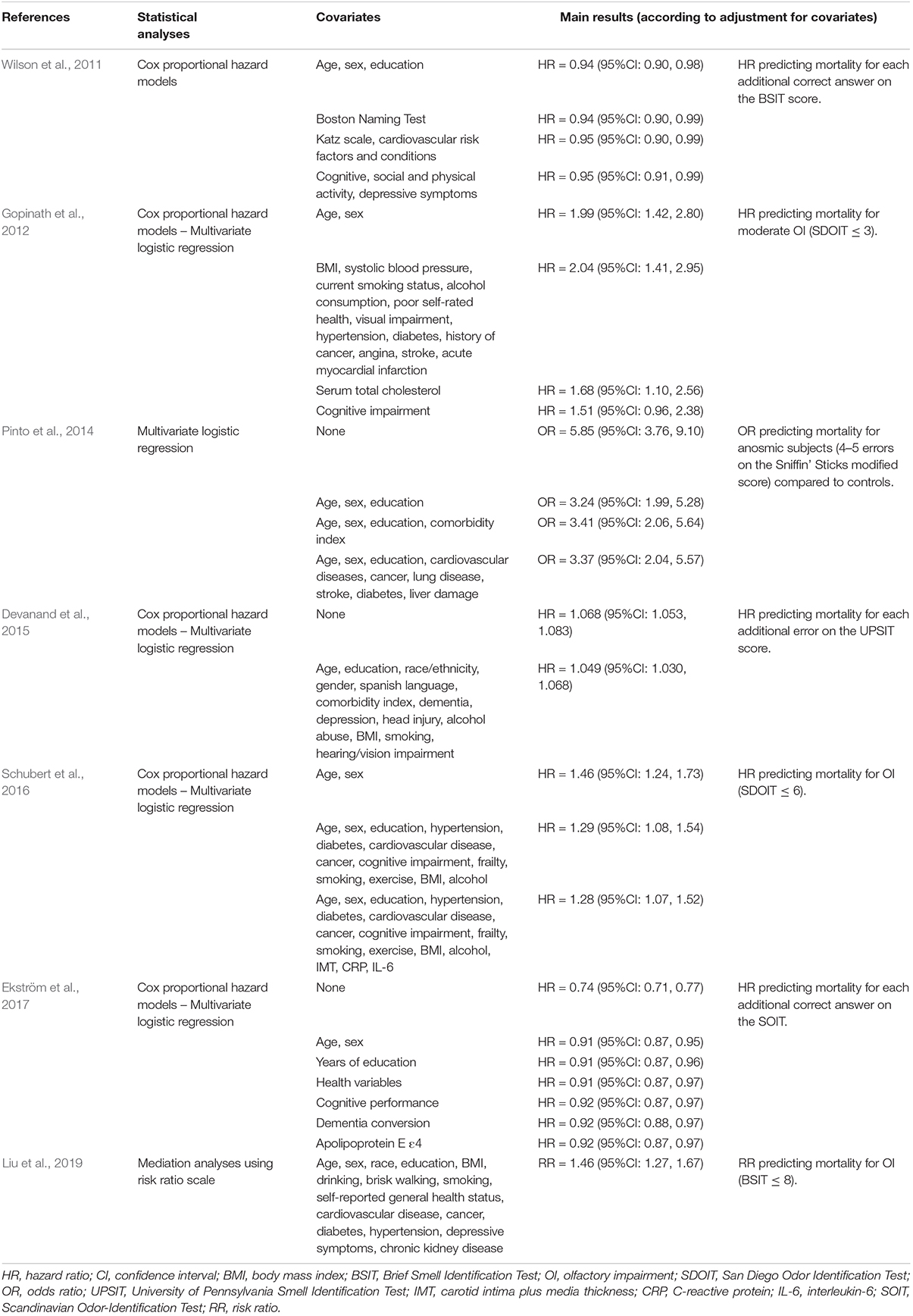
Table 2. Studies linking olfactory impairment and mortality – Statistics and results.
These studies cannot be directly compared due to methodological differences. However, all yield similar results. Regardless of the statistical method used, the relationship between OI and mortality risk was statistically significant and strong. In addition, the association was found to be dose-dependent, meaning anosmic people have a greater risk of death than hyposmic people.
Unfortunately, while clearly revealing the existence of a link between OI and risk of mortality, these studies leave possible explanations of such a link quite unexplored. Indeed, cause-specific mortality is only explored in one study (Liu et al., 2019) whereas others do not report cause of death. Yet, this parameter could have largely contributed to the understanding of the mechanisms of the OI-mortality relationship. Nevertheless, a large number of covariates were controlled, which certainly adds more data to progress through the current hypotheses. Though being a key feature, the causal involvement of neurodegenerative diseases is still left quite unanswered in these studies.
At the moment, the underlying physiopathology linking olfactory impairment to mortality remains unknown. Based on existing evidence and on data from the mortality studies, we will present an overview of current hypotheses.
Olfaction is known to play a role in eating behavior, danger warning and social interaction (Stevenson, 2010). OI will therefore have various consequences on these three human functions, which might directly or indirectly lead to decreased health.
First, malnutrition may be a direct consequence of OI as taste and smell are intrinsically linked. In fact, OI may lead to a decreased ability to enjoy food, decreased appetite and food intake, as well as change in body weight and increased risk for chronic disease. People suffering from OI might either maintain their weight, or eat less, or on the contrary eat more since food would become tasteless; reasons for this remain unclear (Croy et al., 2014). Interestingly, there is growing evidence that the olfactory system could greatly contribute in the regulation of food intake and energy balance, through its effect on sympathetic and parasympathetic tone (Palouzier-Paulignan et al., 2012; Garrison and Knight, 2017; Mortreux et al., 2019). Indeed, receptors to a variety of orexigenic and anorexigenic molecules (i.e., insulin, leptin, ghrelin, neuropeptide Y, nutrient glucose) were found in the olfactory epithelium and in the olfactory bulb (Palouzier-Paulignan et al., 2012; Min and Min, 2018). It was shown that older women with OI had poorer diet quality over 5 years (Gopinath et al., 2016) and that a population of older United States female and male adults displayed low body mass index (BMI) (Dong et al., 2017). Still, there remain controversies in the literature regarding the association between malnutrition and OI in geriatric patients (Gunzer, 2017). Similarly, the relationship between OI and obesity yield contradictory results, some studies demonstrating a correlation (mainly through increased threshold detection of odors (Richardson et al., 2004; Palouzier-Paulignan et al., 2012), while others did not (Gouveri et al., 2014). Some authors suggest that the wide range of both etiologies and endocrinologic consequences of obesity could explain these conflicting findings (Palouzier-Paulignan et al., 2012). Among our seven reviewed studies, only a few measured BMI of the subjects. One study found that OI was associated with decreased BMI (Gopinath et al., 2012). The other showed that subjects who did not enjoy eating or had a low BMI had increased mortality, whereas those who had a high BMI had decreased mortality (Pinto et al., 2014). Weight loss, as a surrogate marker for malnutrition, was also found to contribute to the association between OI and mortality (Liu et al., 2019). Indeed, their mediation analysis demonstrated that weight loss could account for, respectively, 6 and 11% of the 10-year and 13-year higher mortality linked to poor olfaction.
Olfactory impairment might also increase risk of death as a result of not smelling danger signals in the household environment. A United States survey showed that, respectively, 20.3 and 31.3% of adults older than 70 years were not able to identify the warning odors of smoke and natural gas (Hoffman et al., 2016). OI thus exposes to risks associated with cooking accidents, fires or gas leaks and ingestion of spoiled foods or toxic substances (Santos et al., 2004). Anosmic people experience hazardous events 2 to 3 times more often than normosmic subjects (Pence et al., 2014). Although the seven studies did not take these events into consideration for analysis of cause-specific mortality, death rate from unintentional poisoning or fire (not necessarily related to OI) is actually low (1.7–4.7 per 100,000) (Kramarow et al., 2015).
Olfactory function is known to influence quality of life. Notably, people with OI typically suffer from depressive symptoms (Gopinath et al., 2011; Croy et al., 2012, 2014; Sivam et al., 2016). One proposed explanation is that dysfunction or absence of olfactory bulb might result in the dysfunction of various cellular processes and pathways within the hippocampus (Morales-Medina et al., 2017). Some of the mortality studies reported that the subjects who died showed more depressive signs (Wilson et al., 2011; Ekström et al., 2017). However, the association of OI with mortality persisted after controlling for depressive symptoms (Wilson et al., 2011). OI is associated with reduced social network size (Zou et al., 2016), and recent work showed that reduced in-person physical contact with others might partially mediate the link between OI and mortality in females (Leschak and Eisenberger, 2018).
At present, OI has become a well-known early biomarker for a broad spectrum of neurodegenerative diseases. Therefore, it is not surprising that neurodegenerative diseases have been investigated as a possible mediator in the relationship between OI and mortality. Despite some conflicting results, evidence is progressively increasing that neurodegenerative diseases might partly explain this relationship.
The majority of the reviewed studies included cognitive function at baseline as a covariate. In three studies, controlling for cognitive performance at baseline did not change the results. Nevertheless, Wilson et al. (2011) excluded patients with a diagnosis of dementia or PD at baseline and used a measure of cognitive activity frequency in leisure time, which seems to weakly reflect cognitive function. Schubert et al. (2016) did not adjust the results exclusively for cognitive function but rather included additional covariates for adjustment, so that the precise impact of cognitive function remains unknown. In addition, Ekström et al. (2017) also specifically addressed the question of dementia conversion and found that the OI-mortality relationship was independent from it. On the contrary, three other studies did show a potential mediator effect of cognitive function on mortality (Pinto et al., 2014; Devanand et al., 2015; Liu et al., 2019). Two found that the association between OI and mortality was lowered when controlling for dementia, yet remained statistically significant. Of note, OI was shown to be associated with future cognitive decline in cognitively intact subjects (Devanand, 2016). Moreover, there is evidence of existing post-mortem markers of neurodegenerative disease in the brain of subjects without previous clinical signs of MCI or AD (Wilson et al., 2009). Therefore, one hypothetical explanation for the absence or weak mediating effect of cognitive function on mortality might be that olfaction is altered while clinical cognitive function is not yet affected and thus undiagnosed. Only Gopinath et al. (2012) came to a non-significant association between OI and mortality risk after adjustment for cognitive impairment. This would suggest a mediating role of cognitive function, although the authors clearly state this finding could be due to weak statistical power. More interestingly, the only analysis of cause-specific mortality showed that the strongest causal association found was between OI and death associated with dementia or PD (Liu et al., 2019). Indeed, their mediation analysis showed that dementia or PD could account for 22% of the higher 10-year mortality linked to poor olfaction. Lastly, Devanand et al. (2015) questions the fact that neurodegenerative disorders lead to excess mortality. However, recent evidence suggests otherwise. In 2014, AD was the sixth leading cause of death in the United States, representing 3.6% of total mortality with an age-adjusted death rate of 25.4 per 100,000 citizens (Taylor et al., 2017). As for PD, a meta-analysis showed a pooled mortality ratio of approximately 1.5 compared to controls (Macleod et al., 2014). Also, mean duration until death varies from 6.9 to 14.3 years. This might also partially explain why dementia conversion does not seem to mediate the OI-mortality link despite a 10-year follow-up (Ekström et al., 2017), since death associated with PD may occur after more than 10 years. PD-related mortality was shown to be significantly increased by the presence of MCI at baseline (Hoogland et al., 2019). This finding supports the idea of a correlation between OI, PD and mortality risk.
Finally, adjusting for ApoE ε4 genotype, associated with cognitive decline and OI (Wang et al., 2002), did not attenuate the association between OI and mortality (Devanand et al., 2015; Ekström et al., 2017).
In conclusion, even if available data remain controversial, there seems to be growing evidence that neurodegenerative diseases, through cognitive dysfunction, may be a potential mediator in the relationship connecting OI to mortality risk.
One of the special features of the olfactory system is its extraordinary plasticity and continuing neurogenesis through adulthood, at least at the level of the olfactory epithelium (for recent review see Huart et al., 2019). Mechanisms underlying these neural abilities have been largely investigated mainly in rodents; indeed, the paucity of human data remains controversial. Adult neurogenesis is thought to occur both peripherally and centrally, in three different locations. First, proliferating stem cells, located within the olfactory epithelium differentiate into olfactory receptor neurons. Secondly, neural stem cells coming from the walls of the lateral ventricle could migrate following the rostral migratory stream toward the olfactory bulb (OB) to give rise to olfactory interneurons (Curtis et al., 2007). Thirdly, some animal data suggest the presence of progenitor cells lying directly within the OB (Huart et al., 2019). For now, however, all this remains somewhat hypothetical in adult human brains. Yet, clinical findings support the idea of high plasticity of the olfactory system. For instance, it is widely acknowledged that the OB is subject to significant volume changes, as a function of olfactory performance. Indeed, OI is associated with reduced OB volume, while recovery of olfactory function correlates with OB volume (Rombaux et al., 2006a, b; Hummel et al., 2013; Yaldizi et al., 2016; Rottstädt et al., 2018). These volume fluctuations probably depend on bottom-up (Negoias et al., 2017) and top-down processes (Cavazzana et al., 2018). In addition, structural brain modifications could also occur beyond the OB (Reichert and Schöpf, 2018). Finally, olfactory plasticity has also been recently highlighted by olfactory training, which was found to improve significantly olfactory skills regardless of baseline olfactory function (Sorokowska et al., 2017) and to lead to increased cortical thickness of certain brain areas (Al Aïn et al., 2019). Interestingly, olfactory training was also shown to improve verbal function and subjective well-being in older people (Wegener et al., 2018).
Importantly, vision and hearing impairment were not associated with mortality nor did they alter the OI-mortality relationship, suggesting that death could not be explained by sensory loss more broadly (Devanand et al., 2015; Schubert et al., 2016). Still, some previous studies have shown a possible link between vision and/or hearing impairment and mortality, evidence for the impact of vision impairment alone remaining weaker (Fisher et al., 2014; Schubert et al., 2016; Lin et al., 2019). It is also important to underline the fact that all humans do not age equally. That is why physiological age might be more relevant than the chronological age. It may be hypothesized that decline in olfactory function could indicate a more advanced physiological age. Indeed, it was found that idiopathic age-related decline in olfactory function was much smaller in the healthy, non-medicated, non-smoking population (Mackay-Sim et al., 2006). On the contrary, it was shown that taste and smell disorders were associated with an increased risk of frailty in the older population (Somekawa et al., 2017; Harita et al., 2019). Among the mortality studies, controlling for performance in activities of daily living or frailty score did not attenuate the effect (Pinto et al., 2014; Schubert et al., 2016). Global sensory impairment (including the five classical senses: smell, taste, hearing, vision and touch) predicts 5-year mortality, but also major components of physical frailty (e.g., slow gait, weight loss, low activity) (Pinto et al., 2017). The same authors developed the concept that multisensory loss of function could reflect a common underlying aging process (Correia et al., 2016).
To summarize, we hypothesize that OI reflects a decline in brain plasticity, and could be seen more globally as an indicator of lowered physiologic repair function. This could explain, at least partly, the pathway toward increased mortality. Brain aging could make the olfactory system as well as other brain structures more vulnerable and less capable of recovering from insults. This highlights the current need to think in terms of physiological age and frailty status. Whether frailty mediates the relationship between OI and mortality still requires more evidence.
Olfactory impairment is known to be associated with a wide range of illnesses and is thought to be a marker of poor health. Landis et al. (2004) showed a negative correlation between olfactory function and the number of comorbid conditions. Self-reported poor health status was associated with OI in one study (Liu et al., 2019). However, the association between OI and mortality risk was mostly driven by the subjects with baseline excellent to good health, which might question the idea of OI being merely a marker of poor health. The authors hypothesized either that OI in healthy older people might hide an underneath life-threatening condition or that the cumulative effect of multiple comorbid conditions might outweigh the effect of OI on death. Moreover, half of the analyzed studies adjusted their results for comorbid conditions, with either little or no effect on the OI-mortality link (Pinto et al., 2014; Devanand et al., 2015; Schubert et al., 2016; Ekström et al., 2017). Controlling for smoking or alcohol abuse did not attenuate the link between OI and mortality (Pinto et al., 2014; Devanand et al., 2015). Some authors also suggested that high levels of inflammatory markers (interleukin-6, C-reactive protein) could be associated with frailty, atherosclerosis and also with OI (Schubert et al., 2011; Henkin et al., 2013; Laudisio et al., 2019). However, adjusting for these variables did not attenuate the link between OI and mortality (Schubert et al., 2016). Hence, whether OI is a marker of poor health remains doubtful. The only assertion that can be made is that OI is a strong and independent risk factor for death, regardless of health status.
Since controlling for comorbid conditions had little or no effect on the OI-mortality link, this would then suggest a weak impact of cardiovascular diseases or metabolic disorders (being part of the comorbidity indexes used in the studies).
However, analysis of cause-specific mortality revealed that OI was modestly associated with death from cardiovascular disease, but not from cancer or respiratory diseases (Liu et al., 2019). Furthermore, the association between OI and mortality did not remain significant after adjusting for total serum cholesterol, though potentially explained by reduced statistical power (Gopinath et al., 2012). Physical exercise and use of statins were found to decrease the incidence of OI (Schubert et al., 2011). Indeed, both are known to improve cardiovascular health and to lower the risk of atherosclerosis, which is the main hallmark of cardiovascular diseases. Additionally, statins may also directly provide to the brain (and thereby to the olfactory system) their positive pleiotropic effects on endothelial function, oxidative stress and vascular inflammation. This would be consistent with the reduced risk of OI being specific to statins crossing well the blood-brain barrier in the study from Schubert et al. (2011). However, in a mouse model, administration of atorvastatin (classified as not crossing the blood-brain barrier) could still enhance the recovery of olfactory function, likely through the promotion of cellular proliferation and neural regeneration of the olfactory epithelium (Kim et al., 2010, 2012). Carotid artery intima media thickness (IMT), a biomarker of generalized atherosclerosis, was shown to be associated with a decline in odor identification performance at 5 years, but only before 60 years old (Schubert et al., 2015a, b). Nevertheless, the association between OI and mortality remained statistically significant after adjusting for IMT (Schubert et al., 2016). Also, OI could be associated to the intake of antihypertensive drugs (Doty and Bromley, 2004). Therefore, cardiovascular diseases might be somehow connected to OI. Yet, evidence remains sparse and further studies are needed.
Obesity, insulin resistance and type 2 diabetes mellitus constitute a well-known continuum which represents a major burden in terms of public health and mortality. In rodent obesity models, the olfactory bulb developed insulin resistance which could then be responsible for the disruption of olfactory function (Palouzier-Paulignan et al., 2012). Human data also support the fact that insulin resistance could affect negatively olfactory function. Indeed, a recent study found that older adults with high insulin resistance (quantified by the HOMA-IR test) had an approximately 2-fold increased odds of OI compared with subjects with low insulin resistance (Min and Min, 2018). This could explain, at least in part, the independent association found between type 2 diabetes mellitus (in which insulin resistance represents the key mechanism) and OI (Gopinath et al., 2012; Gouveri et al., 2014; Yulug et al., 2019). OI in type 2 diabetes mellitus might also be due to microvascular injury since OI was mainly found in diabetic patients already suffering from the microvascular complications of this disease (Gouveri et al., 2014). Regarding mortality studies, diabetes mellitus was associated with OI in one study (Gopinath et al., 2012) but was not in another one more recent (Liu et al., 2019). Three studies included diabetes mellitus in their controlled variables, but the correlation between OI and mortality remained unchanged, thus also suggesting a weak impact of diabetes mellitus. Regarding the link of obesity, insulin resistance and type 2 diabetes mellitus with OI, controversies thus persist on many points.
Finally, due to its direct contact to the outside, the olfactory system may be an easy target for environmental insults. Indeed, olfaction is altered by air pollutants and by exposure to a variety of toxic agents (e.g., metallic compounds) (Ajmani et al., 2016a, b; Genter and Doty, 2019). The airborne toxicants may also make their way to the brain directly through the olfactory pathway, leading to neuronal damage. Of note, it was shown that high levels of air pollution could result in neurodegenerative diseases-related pathology within the olfactory bulb (Calderon-Garciduenas et al., 2018). Pollution and toxic exposure have been linked to poor health and might thus constitute a potential mediator in the relationship between OI and mortality (Fuller-Thomson and Fuller-Thomson, 2019).
Studies agree that OI is an indicator of increased mortality risk in the older population. Several hypothetical mechanisms are suggested, yet the extent to which they contribute to this association remains an open question. To our opinion, the effects of olfactory impairment on eating behavior, danger warning and social interaction do exist, although their importance in this context seems minor. Olfactory impairment and poor health status seem to be linked in some ways, though the exact relationship remains poorly understood. On the contrary, based on current evidence, neurodegenerative diseases and advanced physiological brain aging appear to us as the most likely involved. The olfactory system plays a determinant role and further attention should be given to these potential mechanisms underlying the robust OI-mortality association. In the future, we should also address the question whether the recovery of olfactory function could have beneficial effects on outcome.
VV and CH were the major contributors in writing the manuscript. All authors were involved in manuscript preparation and approved the final version of the manuscript.
VV and CH were supported by the Fund for Scientific Research (FRS-FNRS) of the French Speaking Community of Belgium.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank Jayant M. Pinto for his help in improving the manuscript.
Adams, D. R., Kern, D. W., Wroblewski, K. E., McClintock, M. K., Dale, W., and Pinto, J. M. (2018). Olfactory dysfunction predicts subsequent dementia in older U.S. adults. J. Am. Geriatr. Soc. 66, 140–144. doi: 10.1111/jgs.15048
Ajmani, G. S., Suh, H. H., and Pinto, J. M. (2016a). Effects of ambient air pollution exposure on olfaction: a review. Environ. Health Perspect. 124, 1683–1693. doi: 10.1289/ehp136
Ajmani, G. S., Suh, H. H., Wroblewski, K. E., Kern, D. W., Schumm, L. P., McClintock, M. K., et al. (2016b). Fine particulate matter exposure and olfactory dysfunction among urban-dwelling older US adults. Environ. Res. 151, 797–803. doi: 10.1016/j.envres.2016.09.012
Al Aïn, S., Poupon, D., Hétu, S., Mercier, N., Steffener, J., and Frasnelli, J. (2019). Smell training improves olfactory function and alters brain structure. Neuroimage 189, 45–54. doi: 10.1016/j.neuroimage.2019.01.008
Attems, J., Walker, L., and Jellinger, K. A. (2015). Olfaction and aging: a mini-review. Gerontology 61, 485–490. doi: 10.1159/000381619
Berardelli, A., Wenning, G. K., Antonini, A., Berg, D., Bloem, B. R., and Bonifati, V. (2013). EFNS/MDS-ES recommendations for the diagnosis of Parkinson’s disease. Eur. J. Neurol. 20, 16–34. doi: 10.1111/ene.12022
Borenstein Graves, A., Bowen, J. D., Rajaram, L., McCormick, W. C., McCurry, S. M., Schellenberg, G. D., et al. (1999). Impaired olfaction as a marker for cognitive decline. Interaction with apolipoprotein E 4 status. Neurology 53, 1480–1487.
Braak, H., and Del Tredici, K. (2017). Neuropathological staging of brain pathology in sporadic Parkinson’s disease: separating the wheat from the chaff. J. Parkinsons Dis. 7, S71–S85.
Calderon-Garciduenas, L., Gonzalez-Maciel, A., Reynoso-Robles, R., Kulesza, R. J., Mukherjee, P. S., Torres-Jardon, R., et al. (2018). Alzheimer’s disease and alpha-synuclein pathology in the olfactory bulbs of infants, children, teens and adults ≤40 years in metropolitan mexico city. APOE4 carriers at higher risk of suicide accelerate their olfactory bulb pathology. Environ. Res. 166, 348–362. doi: 10.1016/j.envres.2018.06.027
Cavazzana, A., Poletti, S. C., Guducu, C., Larsson, M., and Hummel, T. (2018). Electro-olfactogram responses before and after aversive olfactory conditioning in humans. Neuroscience 373, 199–206. doi: 10.1016/j.neuroscience.2018.01.025
Cerf-Ducastel, B., and Murphy, C. (2009). Age-related differences in the neural substrates of cross-modal olfactory recognition memory: an fMRI investigation. Brain Res. 88, 1285–1288. doi: 10.1016/j.brainres.2009.05.086
Conti, M. Z., Vicini-Chilovi, B., Riva, M., Zanetti, M., Liberini, P., Padovani, A., et al. (2013). Odor identification deficit predicts clinical conversion from mild cognitive impairment to dementia due to Alzheimer’s disease. Arch. Clin. Neuropsychol. 28, 391–399. doi: 10.1093/arclin/act032
Correia, C., Lopez, K. J., Wroblewski, K. E., Huisingh-Scheetz, M., Kern, D. W., Chen, R. C., et al. (2016). Global sensory impairment in older adults in the United States. J. Am. Geriatr. Soc. 64, 306–313. doi: 10.1111/jgs.13955
Croy, I., Negoias, S., Novakova, L., Landis, B. N., and Hummel, T. (2012). Learning about the functions of the olfactory system from people without a sense of smell. PLoS One 7:e33365. doi: 10.1371/journal.pone.0033365
Croy, I., Nordin, S., and Hummel, T. (2014). Olfactory disorders and quality of life – An updated review. Chem. Senses 39, 185–194. doi: 10.1093/chemse/bjt072
Curtis, M. A., Kam, M., Nannmark, U., Anderson, M. F., Zetterstrom Axell, M., Wikkelso, C., et al. (2007). Human neuroblasts mograte to the olfactory bulb via a lateral ventricular extension. Science 315, 1243–1249. doi: 10.1126/science.1136281
Devanand, D. P. (2016). Olfactory identification deficits, cognitive decline, and dementia in older adults. Am. J. Geriatr. Psychiatry 24, 1151–1157. doi: 10.1016/j.jagp.2016.08.010
Devanand, D. P., Lee, S., Manly, J., Andrews, H., Schupf, N., Masurkar, A., et al. (2015). Olfactory identification deficits and increased mortality in the community. Ann. Neurol. 78, 401–411. doi: 10.1002/ana.24447
Dong, J., Pinto, J. M., Guo, X., Alonso, A., Tranah, G., Cauley, J. A., et al. (2017). The prevalence of anosmia and associated factors among U.S. black and white older adults. J. Gerontol. A. Biol. Sci. med. Sci. 72, 1080–1086. doi: 10.1093/gerona/glx081
Doty, R. L. (2018). Age-related deficits in taste and smell. Otolaryngol. Clin. North Am. 51, 815–825. doi: 10.1016/j.otc.2018.03.014
Doty, R. L., and Bromley, S. M. (2004). Effects of drugs on olfaction and taste. Otolaryngol. Clin. N. Am. 37, 1229–1254.
Doty, R. L., and Kamath, V. (2014). The influences of age on olfaction: a review. Front. Psychol. 5:20. doi: 10.3389/fpsyg.2014.00020
Doty, R. L., Petersen, I., Mensah, N., and Christensen, K. (2011). Genetic and environmental influences on odor identification ability in the very old. Psychol. Aging 26, 864–871. doi: 10.1037/a0023263
Ekström, I., Sjölund, S., Nordin, S., Nordin Adolfsson, A., Adolfsson, R., Nilsson, L.-G., et al. (2017). Smell loss predicts mortality risk regardless of dementia conversion. J. Am. Geriatr. Soc. 65, 1238–1243. doi: 10.1111/jgs.14770
Fisher, D., Li, C. M., Chiu, M. S., Themann, C. L., Petersen, H., Jonasson, F., et al. (2014). Impairments in hearing and vision impact on mortality in older people: the AGES-Reykjavik Study. Age. Ageing 43, 69–76. doi: 10.1093/ageing/aft122
Fuller-Thomson, E. R., and Fuller-Thomson, E. G. (2019). Relationship between poor olfaction and mortality. Ann. Intern. Med. 171, 525–526. doi: 10.7326/L19-0467
Garrison, J. L., and Knight, Z. A. (2017). Linking smell to metabolism and aging. Science 358, 718–719. doi: 10.1126/science.aao5474
Gauthier, S., Reisberg, B., Zaudig, M., Petersen, R. C., Ritchie, K., Broich, K., et al. (2006). Mild cognitive impairment. Lancet 367, 1262–1270.
Genter, M., and Doty, R. L. (2019). Toxic exposures and the senses of taste and smell. Handb. Clin. Neurol. 164, 389–408. doi: 10.1016/B978-0-444-63855-7.00022-8
Gjerde, K. V., Müller, B., Skeie, G. O., Assmus, J., Alves, G., and Tysnes, O.-B. (2018). Hyposmia in a simple smell test is associated with accelerated cognitive decline in early Parkinson’s disease. Acta Neurol. Scand. 138, 508–514. doi: 10.1111/ane.13003
Gopinath, B., Anstey, K. J., Sue, C. M., Kifley, A., and Mitchell, P. (2011). Olfactory impairment in older adults is associated with depressive symptoms and poorer quality of life scores. Am. J. Geriatr. Psychiatry 19, 830–834. doi: 10.1097/JGP.0b013e318211c205
Gopinath, B., Russel, J., Sue, C. M., Flood, V. M., Burlutsky, G., and Mitchell, P. (2016). Olfactory impairment in older adults is associated with poorer diet quality over 5 years. Eur. J. Nutr. 55, 1081–1087. doi: 10.1007/s00394-015-0921-2
Gopinath, B., Sue, C. M., Kifley, A., and Mitchell, P. (2012). The association between olfactory impairment and total mortality in older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 67, 204–209. doi: 10.1093/gerona/glr165
Gouveri, E., Katotomichelakis, M., Gouveris, H., Danielides, V., Maltezos, E., and Papanas, N. (2014). Olfactory dysfunction in type 2 diabetes mellitus: an additional manifestation of microvascular disease? Angiology 65, 869–876. doi: 10.1177/0003319714520956
Gunzer, W. (2017). Changes of olfactory performance during the process of aging – Psychophysical testing and its relevance in the fight against malnutrition. J. Nutr. Health Aging 21, 1010–1015. doi: 10.1007/s12603-017-0873-8
Haehner, A., Masala, C., Walter, S., Reichmann, H., and Hummel, T. (2019). Incidence of Parkinson’s disease in a large patient cohort with idiopathic smell and taste loss. J. Neurol. 266, 339–345. doi: 10.1007/s00415-018-9135-x
Harita, M., Miwa, T., Shiga, H., Yamada, K., Sugiyama, E., Okabe, Y., et al. (2019). Association of olfactory impairment with indexes of sarcopenia and frailty in community-dwelling older adults. Geriatr. Gerontol. Int. 19, 384–391. doi: 10.1111/ggi.1362
Hedner, M., Nilsson, L.-G., Olofsson, J. K., Bergman, O., Eriksson, E., Nyberg, L., et al. (2010). Age-related olfactory decline is associated with the BDNF val66met polymorphism: evidence from a population-based study. Front. Aging Neurosci. 2:24. doi: 10.3389/fnagi.2010.00024
Henkin, R. I., Schmidt, L., and Velicu, I. (2013). Interleukin 6 in hyposmia. JAMA Otolaryngol. Head Neck Surg. 139, 728–734. doi: 10.1001/jamaoto.2013.3392
Hoffman, H. J., Rawal, S., Li, C.-M., and Duffy, V. B. (2016). New chemosensory component in the U.S. national health and nutrition examination survey (NHANES): first-year results for measured olfactory dysfunction. Rev. Endocr. Metab. Disord. 17, 221–240. doi: 10.1007/s11154-016-9364-1
Hoogland, J., Post, B., and de Bie, R. M. A. (2019). Overall and disease related mortality in Parkinson’s disease – a longitudinal cohort study. J. Parkinsons Dis. 9, 767–774. doi: 10.3233/JPD-191652
Huart, C., Eloy, P., and Rombaux, P. (2013a). “Olfaction,” in Nasal Physiology and Pathophysiology of Nasal Disorders, ed. T. M. Önerci, (Berlin: Springer), 113–137.
Huart, C., Rombaux, P., and Hummel, T. (2013b). Plasticity of the human olfactory system: the olfactory bulb. Molecules 18, 11586–11600. doi: 10.3390/molecules180911586
Huart, C., Rombaux, P., and Hummel, T. (2019). Neural plasticity in developing and adult olfactory pathways – focus on the human olfactory bulb. J. Bioernerg. Biomembr. 51, 77–87. doi: 10.1007/s10863-018-9780-x
Hummel, T., Henkel, S., Negoias, S., Galvan, J. R. B., Bogdanov, V., Hopp, P., et al. (2013). Olfactory bulb volume in patients with temporal lobe epilepsy. J. Neurol. 260, 1004–1008. doi: 10.1007/s00415-012-6741-x
Hummel, T., Landis, B. N., and Hüttenbrink, K.-B. (2011). Smell and taste disorders. GMS Curr. Top. Otorhinolaryngol. Head Neck Surg. 10:Doc04. doi: 10.3205/cto000077
Jung, H. J., Shin, I.-S., and Lee, J.-E. (2019). Olfactory function in mild cognitive impairment and Alzheimer’s disease: a meta-analysis. Laryngoscope 129, 362–369. doi: 10.1002/lary.27399
Kim, H. Y., Dhong, H. J., Min, Y. G., Jung, Y. G., and Chung, S. K. (2010). Effects of statins on regeneration of olfactory epithelium. Am. J. Rhinol. Allergy. 24, 121–125. doi: 10.2500/ajra.2010.24.3455
Kim, H. Y., Kim, J. H., Dhong, H. J., Kim, K. R., Chung, S. K., Chung, S. C., et al. (2012). Effects of statins on the recovery of olfactory function in a 3-methylindole-induced anosmia mouse model. Am. J. Rhinol. Allergy. 26, e81–e84. doi: 10.2500/ajra.2012.26.3719
Kramarow, E., Chen, L.-H., Hedegaard, H., and Warner, M. (2015). Deaths from unintentional injury among adults aged 65 and over: United States, 2000-2013. NCHS Data Brief 199,
Landis, B. N., Konnerth, C. G., and Hummel, T. (2004). A study on the frequency of olfactory dysfunction. Laryngoscope 114, 1764–1769. doi: 10.1097/00005537-200410000-00017
Landis, B. N., Hummel, T., Hugentobler, M., Giger, R., and Lacroix, J. S. (2003). Ratings of overall olfactory function. Chem. Senses 28, 691–694. doi: 10.1093/chemse/bjg061
Laudisio, A., Navarini, L., Margiotta, D. P. E., Fontana, D. O., Chiarella, I., Spitaleri, D., et al. (2019). The association of olfactory dysfunction, frailty, and mortality is mediated by inflammation: result from the InCHIANTI study. J. Immunol. Res. 2019:3128231. doi: 10.1155/2019/3128231
Leschak, C. J., and Eisenberger, N. I. (2018). The role of social relationships in the link between olfactory dysfunction and mortality. PLoS One 13:e0196708. doi: 10.1371/journal.pone.0196708
Lin, H. W., Mahboubi, H., and Bhattacharyya, N. (2019). Hearing difficulty and risk of mortality. Ann. Otol. Rhinol. Laryngol. 128, 614–618. doi: 10.1177/0003489419834948
Liu, B., Luo, Z., Pinto, J. M., Shiroma, E. J., Tranah, G. J., Wirdefeldt, K., et al. (2019). Relationship between poor olfaction and mortality among community-dwelling older adults. Ann. Intern. Med. 170, 673–681. doi: 10.7326/M18-0775
Lötsch, J., Daiker, H., Hähner, A., Ultsch, A., and Hummel, T. (2015a). Drug-target based cross-sectional analysis of olfactory drug effects. Eur. J. Clin. Pharmacol. 71, 461–471. doi: 10.1007/s00228-015-1814-2
Lötsch, J., Geisslinger, G., and Hummel, T. (2012). Sniffing out pharmacology: interactions of drugs with human olfaction. Trends Pharmacol. Sci. 33, 193–199. doi: 10.1016/j.tips.2012.01.004
Lötsch, J., and Hummel, T. (2019). Clinical usefulness of self-rated olfactory performance – A data science-based assessment of 6000 patients. Chem. Senses 44, 357–364. doi: 10.1093/chemse/bjz029
Lötsch, J., Knothe, C., Lippman, C., Ultsch, A., Hummel, T., and Walter, C. (2015b). Olfactory drug effects approached from human-derived data. Drug Discov. Today 20, 1398–1406. doi: 10.1016/j.drudis.2015.06.012
Mackay-Sim, A., Johnston, A. N. B., Owen, C., and Burne, T. H. J. (2006). Olfactory ability in the healthy population: reassessing prebyosmia. Chem. Senses 31, 763–771. doi: 10.1093/chemse/bjl019
Macleod, A. D., Taylor, K. S. M., and Counsell, C. E. (2014). Mortality in Parkinson’s disease: a systematic review and meta-analysis. Mov. Disord. 29, 1615–1622. doi: 10.1002/mds.25898
Marin, C., Vilas, D., Langdon, C., Alobid, I., Lopez-Chacon, M., Haehner, A., et al. (2018). Olfactory dysfunction in neurodegenerative diseases. Curr. Allergy Asthma Rep. 18:42. doi: 10.1007/s11882-018-0796-4
Min, J. Y., and Min, K. B. (2018). Insulin resistance and the increased risk for smell dysfunction in US adults. Laryngoscope 129, 1992–1996. doi: 10.1002/lary.27093
Morales-Medina, J. C., Ianitti, T., Freeman, A., and Caldwell, H. K. (2017). The olfactory bulbectomized rat as a model of depression: the hippocampal pathway. Behav. Brain Res. 317, 562–575. doi: 10.1016/j.bbr.2016.09.029
Mortreux, M., Foppen, E., Denis, R. G., Montaner, M., Kassis, N., Denom, J., et al. (2019). New roles for prokineticin 2 in feeding behavior, insulin resistance and type 2 diabetes: studies in mice and humans. Mol. Metab. 29, 182–196. doi: 10.1016/j.molmet.2019.08.016
Negoias, S., Pietsch, K., and Hummel, T. (2017). Changes in olfactory bulb volume following lateralized olfactory training. Brain Imaging Behav. 11, 998–1005. doi: 10.1007/s11682-016-9567-9
Oleszkiewicz, A., Kunkel, F., Larsson, M., and Hummel, T. (in press). Consequences of undetected olfactory loss on human chemosensory communication and well-being. Prof. Royal Acad. Sci. Phil. Trans. B.
Oleszkiewicz, A., and Hummel, T. (2019). Whose nose does not know? Demographical characterization of people unaware of ansomia. Eur. Arch. Otorhinolaryngol. 276, 1849–1852. doi: 10.1007/s00405-019-05414-8
Olofsson, J. K., Rönnlund, M., Nordin, S., Nyberg, L., Nilsson, L.-G., and Larsson, M. (2009). Odor identification deficit as a predictor of five-year global cognitive change: interactive effects with age and ApoE-(4). Behav. Genet. 39, 496–503. doi: 10.1007/s10519-009-9289-5
Ottaviano, G., Savietto, E., Scarpa, B., Bertocco, A., Maculan, P., Sergi, G., et al. (2018). Influence of number of drugs on olfaction in the elderly. Rhinology 56, 351–357. doi: 10.4193/Rhin17.152
Palouzier-Paulignan, B., Lacroix, M. C., Aimé, P., Baly, C., Caillol, M., Congar, P., et al. (2012). Olfaction under metabolic influences. Chem. Senses 37, 769–797. doi: 10.1093/chemse/bjs059
Pence, T. S., Reiter, E. R., DiNardo, L. J., and Costanzo, R. M. (2014). Risk factors for hazardous events in olfactory-impaired patients. JAMA Otolayrngol. Head Neck Surg. 140, 951–955. doi: 10.1001/jamaoto.2014.1675
Pinto, J. M., Wroblewski, K. E., Huisingh-Scheetz, M., Correia, C., Lopez, K. J., Chen, R. C., et al. (2017). Global sensory impairment predicts morbidity and mortality in older U.S. adults. J. Am. Geriatr. Soc. 65, 2587–2595. doi: 10.1111/jgs.15031
Pinto, J. M., Wroblewski, K. E., Kern, D. W., Schumm, L. P., and McClintock, M. K. (2014). Olfactory dysfunction predicts 5-year mortality in older adults. PLoS One 9:e107541. doi: 10.1371/journal.pone.0107541
Reichert, J. L., and Schöpf, V. (2018). Olfactory loss and regain: lessons for neuroplasticity. Neuroscientist 24, 22–35. doi: 10.1177/1073858417703910
Richardson, B. E., Vander Woude, E. A., Sudan, R., Thompson, J. S., and Leopold, D. A. (2004). Altered olfactory acuity in the morbidly obese. Obes. Surg. 7, 967–969. doi: 10.1381/0960892041719617
Rombaux, P., Mouraux, A., Bertrand, B., Nicolas, G., Duprez, T., and Hummel, T. (2006a). Olfactory function and olfactory bulb volume in patients with postinfectious olfactory loss. Laryngoscope 116, 436–439. doi: 10.1097/01.mlg.0000195291.36641.1e
Rombaux, P., Mouraux, A., Bertrand, B., Nicolas, G., Duprez, T., and Hummel, T. (2006b). Retronasal and orthonasal olfactory function in relation to olfactory bulb volume in patients with posttraumatic loss of smell. Laryngosope 116, 901–905. doi: 10.1097/01.mlg.0000217533.60311.e7
Rottstädt, F., Han, P., Weidner, K., Schellong, J., Wolff-Stephan, S., and Strauß, T. (2018). Reduced olfactory bulb in depression – A structural moderator analysis. Hum. Brain Mapp. 39, 2573–2582. doi: 10.1002/hbm.24024
Sanford, A. M. (2017). Mild cognitive impairment. Clin. Geriatr. Med. 33, 325–337. doi: 10.1016/j.cger.2017.02.005
Santos, D. V., Reiter, E. R., DiNardo, L. J., and Costanzo, R. M. (2004). Hazardous events associated with impaired olfactory function. Arch. Otolaryngol. Head Neck Surg. 130, 317–319.
Schubert, C. R., Cruickshanks, K. J., Fischer, M. E., Huang, G.-H., Klein, B. E. K., Klein, R., et al. (2012). Olfactory impairment in an adult population: the beaver dam offspring study. Chem. Senses 37, 325–334. doi: 10.1093/chemse/bjr102
Schubert, C. R., Cruickshanks, K. J., Fischer, M. E., Huang, G.-H., Klein, R., Tsai, M. Y., et al. (2015a). Carotid intima media thickness, atherosclerosis, and 5-year decline in odor identification: the beaver dam offspring study. J. Geron. A. Biol. Sci. Med. Sci. 70, 879–884. doi: 10.1093/gerona/glu15
Schubert, C. R., Cruickshanks, K. J., Fischer, M. E., Klein, E. K., Klein, R., and Pinto, A. A. (2015b). Inflammatory and vascular markers and olfactory impairment in older adults. Age. Ageing 44, 878–882. doi: 10.1093/ageing/afv075
Schubert, C. R., Cruickshanks, K. J., Klein, B. E. K., Klein, R., and Nondahl, D. M. (2011). Olfactory impairment in older adults: 5-year incidence and risk factors. Laryngoscope 121, 873–878. doi: 10.1002/lary.21416
Schubert, C. R., Fischer, M. E., Pinto, A. A., Klein, B. E. K., Klein, R., Tweed, T. S., et al. (2016). Sensory impairments and risk of mortality in older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 72, 710–715. doi: 10.1093/gerona/glw036
Sivam, A., Wroblewski, K. E., Alkorta-Aranburu, G., Barnes, L. L., Wilson, R. S., Bennett, D. A., et al. (2016). Olfactory dysfunction in older adults is associated with feelings of depression and loneliness. Chem. Senses 41, 293–299. doi: 10.1093/chemse/bjv088
Somekawa, S., Mine, T., Ono, K., Hayashi, N., Obuchi, S., Yoshida, H., et al. (2017). Relationship between sensory perception and frailty in a community-dwelling elderly population. J. Nutr. Health Aging 21, 710–714. doi: 10.1007/s12603-016-0836-5
Sorokowska, A., Drechsler, E., Karwowski, M., and Hummel, T. (2017). Effects of olfactory training: a meta-analysis. Rhinology 55, 17–26. doi: 10.4193/Rhin16.195
Stevenson, R. J. (2010). An initial evaluation of the functions of human olfaction. Chem. Senses 35, 3–20. doi: 10.1093/chemse/bjp083
Taylor, C. A., Greenlund, S. E., McGuire, L. C., Lu, H., and Croft, J. B. (2017). Deaths from Alzheimer’s disease – United States, 1999-2014. MMWR Morb. Mortal. Wkly. Rep. 66, 521–526. doi: 10.15585/mmwr.mm6620a1
Wang, Q.-S., Tian, L., Huang, Y.-L., Qin, S., He, L.-Q., and Zhou, J.-N. (2002). Olfactory identification and apolipoprotein E (4 allele in mild cognitive impairment. Brain Res. 951, 77–81. doi: 10.1016/s0006-8993(02)03137-2
Wegener, B.-A., Croy, I., Hähner, A., and Hummel, T. (2018). Olfactory training with older people. Int. J. Geriatr. Psychiatry 33, 212–220. doi: 10.1002/gps.4725
Wilson, R. S., Arnold, S. E., Schneider, J. A., Boyle, P. A., Buchman, A. S., and Bennett, D. A. (2009). Olfactory impairment in presymptomatic Alzheimer’s disease. Ann. N. Y. Acad. Sci. 1170, 730–735. doi: 10.1111/j.1749-6632.2009.04013.x
Wilson, R. S., Yu, L., and Bennett, D. A. (2011). Odor identification and mortality in old age. Chem. Senses 36, 63–67. doi: 10.1093/chemse/bjq098
Yaldizi, O., Penner, I.-K., Yonekawa, T., Naegelin, Y., Kuhle, J., Pardini, M., et al. (2016). The association between olfactory bulb volume, cognitive dysfunction, physical disability and depression in multiple sclerosis. Eur. J. Neurol. 23, 510–519. doi: 10.1111/ene.12891
Yulug, B., Saatci, O., Isiklar, A., Hanoglu, L., Kilic, U., Ozansoy, M., et al. (2019). The association between HbA1c levels, olfactory memory and cognition in normal, pre-diabetic and diabetic persons. Endocr. Metab. Immune Disord. Drug Targets. doi: 10.2174/1871530319666190614121738 [Epub ahead of print],
Keywords: olfactory impairment, mortality, neurodegenerative diseases, cognitive function, plasticity, aging
Citation: Van Regemorter V, Hummel T, Rosenzweig F, Mouraux A, Rombaux P and Huart C (2020) Mechanisms Linking Olfactory Impairment and Risk of Mortality. Front. Neurosci. 14:140. doi: 10.3389/fnins.2020.00140
Received: 15 November 2019; Accepted: 04 February 2020;
Published: 21 February 2020.
Edited by:
Hamid R. Sohrabi, Murdoch University, AustraliaReviewed by:
Viviana Triaca, Italian National Research Council, ItalyCopyright © 2020 Van Regemorter, Hummel, Rosenzweig, Mouraux, Rombaux and Huart. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victoria Van Regemorter, victoria.vanregemorter@uclouvain.be
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.