
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Hum. Neurosci. , 10 August 2023
Sec. Brain Imaging and Stimulation
Volume 17 - 2023 | https://doi.org/10.3389/fnhum.2023.1162854
This article is part of the Research Topic Perspectives in Non-Invasive Brain Stimulation and Neuromodulation View all 7 articles
 Bárbara Naeme de Lima Cordeiro1Elizângela Kuster2Aurore Thibaut3Lucas Rodrigues Nascimento2,4Jessica Vaz Gonçalves1
Bárbara Naeme de Lima Cordeiro1Elizângela Kuster2Aurore Thibaut3Lucas Rodrigues Nascimento2,4Jessica Vaz Gonçalves1 Guilherme Peixoto Tinoco Arêas5Wellingson Silva Paiva6
Guilherme Peixoto Tinoco Arêas5Wellingson Silva Paiva6 Fernando Zanela da Silva Arêas2,4*
Fernando Zanela da Silva Arêas2,4*Severe traumatic brain injury (sTBI) is an important cause of disability and mortality and affects people of all ages. Current scientific evidence indicates that motor dysfunction and cognitive impairment are the main limiting factors in patients with sTBI. Transcranial direct current stimulation (tDCS) seems to be a good therapeutic option, but when it comes to patients with sTBI, the results are inconclusive, and some protocols have not yet been tested. In addition, there is still a lack of information on tDCS-related physiological mechanisms, especially during the acute phase. In the present study, based on current evidence on tDCS mechanisms of action, we hypothesized that performing tDCS sessions in individuals with sTBI, especially in the acute and subacute phases, together with conventional therapy sessions, could improve cognition and motor function in this population. This hypothesis presents a new possibility for treating sTBI, seeking to elucidate the extent to which early tDCS may affect long-term clinical outcomes.
Severe traumatic brain injury (sTBI) is a major cause of death and disability affecting all ages worldwide with nearly 70 million new cases each year (Maas et al., 2017). Brain injuries resulting from sTBI typically lead to cognitive, psychological, sensory, behavioral, and motor, including post-traumatic epilepsy, problems that preclude daily activities and social participation (Areas et al., 2019). TBI is largely heterogeneous and the consequences vary according to the complexity and severity of the lesions, as it may affect diverse cortical and sub-cortical brain structures (Zaninotto et al., 2019). In addition, sTBI produces high costs for the government, families, and society (Riggio, 2011).
Physical disability after sTBI (Glasgow Coma Scale 15 to 13 = mild TBI; 12 to 9 = moderate TBI; 8 45 or less = severe TBI) is considerably higher in comparison with able-bodied individuals (Lingsma et al., 2010), leading to sedentary behavior and dependence for performing activities of daily living (Williams et al., 2019). In addition, most individuals remain with cognitive deficits for example attention, memory, executive functions, language, etc. (Alderman and Wood, 2013), which is one of the main limiting factors in post-TBI patients. The diffuse axonal injury in association with secondary injuries and a cascade effect triggered by neurotoxicity explain the high incidence of cognitive impairments (Gupta et al., 2016; Stewan Feltrin et al., 2018). These chronic impairments in cognitive functions (Mcmillan and Wood, 2017; Williams et al., 2019) severely affect patients’ psychosocial recovery and may increase predisposition to neurodegenerative diseases (Alderman and Wood, 2013).
Non-invasive brain stimulation (NBIS) has been recommended for treating cognitive impairments and functional limitations in people with neurological and psychiatric disorders (Fregni and Pascual-Leone, 2007). A widely used technique is transcranial direct current stimulation (tDCS), which has the potential to modify and modulate the polarity of the neuron’s membrane potential (Nitsche et al., 2008). tDCS has been tested in several disorders (Lefaucheur et al., 2017), including TBI, (Villamar et al., 2012) based on the application of a low intensity electric current (generally 1–2 mA) for by means of two electrodes positioned on the patient’s scalp. Previous studies (Nitsche and Paulus, 2000; Boggio et al., 2008) have shown that anodal tDCS increases the excitability of the cerebral cortex and that cathodal stimulation decreases it. On a behavioral level, anodal tDCS can improve motor task performance, language, and memory. In contrast, cathodal tDCS can also increase performance by decreasing the hyperarousal in an area of maladaptive plasticity (Li et al., 2015).
Thus, depending on the size and location of the electrodes applied, tDCS may focally suppress or to modulate neuronal firing after sTBI, which may offer a promising method to minimize damage and promote functional recovery. In addition, cathodal and anodal tDCS can be used to suppress and increase, respectively, the excitability of neurotransmitters such as glutamate and GABA (gamma-aminobutyric acid) that are part of the cascade of neurochemical responses that occurs after brain trauma. Cathodal tDCS can be used to suppress acute glutamatergic hyperexcitability after sTBI. In the subacute phase, high levels of GABA can cause excessive inhibition, making recovery difficult. Therefore, modulation of GABAergic inhibition may be beneficial to minimize the functional impact at this stage. Finally, in the chronic phase of TBI, brain stimulation combined with rehabilitation can improve behavioral recovery, learning of new skills, and cortical plasticity (Demirtas-Tatlidede et al., 2012).
Previous research have demonstrated positive results after stroke (Lefaucheur et al., 2017), such as improved motor and cognitive function, when tDCS was combined with other therapies (Zaninotto et al., 2019). Besides revious studies showed evidence level B to either support the use of tDCS after acute or chronic Stroke (Elsner et al., 2017; Fregni et al., 2021). Factors related to the biological systems and individual variability are the major reasons that underlie some of these inconsistencies (Pruski and Cantarero, 2020). In addition, methodological issues related to the administration of tDCS, such as electrode montage and type, dosage, timing of application, and endpoint measures, prevent conclusions regarding its efficacy after sTBI (Arêas et al., 2022).
Studies showing positive results of tDCS after sTBI were performed in individuals in the chronic phases of trauma (Kang et al., 2012; Ulam et al., 2015; Zaninotto et al., 2019), revealing a lack of studies examining tDCS acutely after sTBI, which would be clinically relevant as studies suggest that early interventions are critical for optimal recovery (Villamar et al., 2012). According to Zaninotto et al. (2019) the combination of tDCS with cognitive and/or physical training may enhance long-term potentiation (LTP), which makes this approach very attractive, especially in acute and subacute rehabilitation settings. Therefore, this study aims to elucidate how tDCS may help improving cognition and motor function in individuals with sTBI in the acute and subacute phases, by presenting a hypothesis model.
The searches were performed in the Medline database and the reference lists of included studies were screened to identify further relevant studies. Seven randomized controlled trials that analyzed the potential effects of tDCS on brain activity in individuals with a disorder of consciousness after sTBI were included. Detailed information was provided in Table 1.
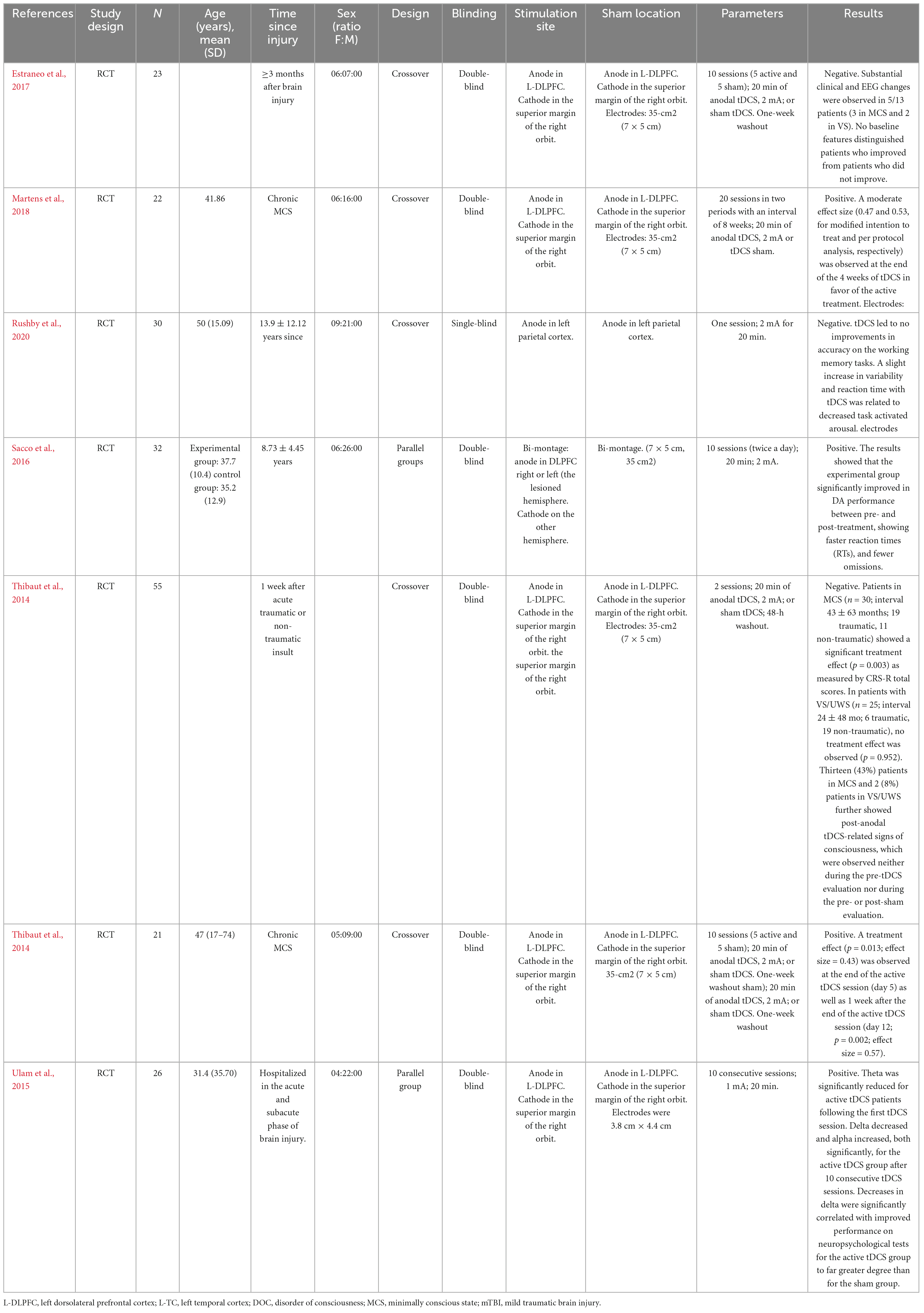
Table 1. Characteristics of included studies.
The first study examined the effects of a single session of tDCS over left DLPFC cortex in 55 participants. The experimental group received 20 min of stimulation at 2 mA. The control group received a sham-stimulation. There was a significant difference in favor of the experimental group on consciousness, in people with severe brain damage (Thibaut et al., 2014).
The second study examined the effects of 10 consecutive sessions of tDCS over left DLPFC cortex in 36 participants. The experimental group received 20 min of continuous direct current stimulation at 1 mA. The control group received a sham-stimulation. There was a significant difference in favor of the experimental group in the regulation of cortical excitability (Ulam et al., 2015).
The third study examined the effects of 10 sessions of tDCS over the left DLPFC cortex (their specific location depended on participants’ damaged area) combined with computer-assisted training, 2 times per day, in 22 participants. The experimental group received 20 min of tDCS stimulation followed by 30 min of attention training. The control group received a sham-stimulation followed by 30 min of attention training. There was a significant difference in favor of the experimental group on neural reorganization and cognitive effort (Sacco et al., 2016).
The fourth study examined the effects of 5 consecutive sessions of tDCS over left DLPFC cortex in 16 participants. The experimental group received 20 min of stimulation at 2 mA. The control group received a sham-stimulation. There was a significant improvement on the recovery of consciousness in some chronic patients of the experimental group (Thibaut et al., 2017).
The fifth study examined the effects of 5 consecutive sessions of tDCS over left DLPFC cortex in 13 participants. The experimental group received 20 min of stimulation at 2 mA. The control group received a sham-stimulation. There was no difference between-groups on short-term clinical and EEG in patients with prolonged disorders of consciousness (Estraneo et al., 2017).
The sixth study examined the effects of 20 sessions of tDCS over left DLPFC cortex, 5 times per/week, during 4 weeks in 27 participants. The experimental group received 20 min of stimulation at 2 mA. The control group received a sham-stimulation. There was a significant difference in favor of the experimental group on signs of consciousness in chronic minimally conscious state patients (Martens et al., 2018).
The last study examined the effects of a single session of tDCS over left parietal cortex in 30 participants. The experimental group received 20 min of stimulation at 2 mA. The control group received a sham-stimulation. There was no difference between-groups on working memory (Rushby et al., 2020).
Overall, the experimental groups always received stimulation during 20 min at 2 mA; however, the session frequency and program duration varied across trials. The control group always received a sham-stimulation. Most trials reported positive results in favor of the experimental group, which suggests that brain stimulation has a significant effect in outcomes in individuals with disorder of consciousness after TBI. On the other hand, most studies similar methodological limitations: small sample size, heterogeneity regarding participants’ baseline conditions (i.e., diagnosis of consciousness disorders varied from months to years and varied initial level of consciousness) and medical support, lack of follow-up measurements.
Studies have shown that tDCS has the potential to regulate brain function by activating the cerebral cortex using electrical current and may, therefore, induce an increase or decrease in motor cortical excitability, depending upon the polarity of tDCS (Groppa et al., 2010). In addition, tDCS increases cerebral blood volume and cerebral blood flow, and decreases the mean transit time, which suggests better oxygen delivery to cerebral tissues (Rango et al., 2008; Trofimov et al., 2018). To support this finding, imaging exams revealed areas of hyperperfusion in the basal nuclei after tDCS application, suggesting a modulatory effect on deep brain areas following tDCS application (Junior et al., 2015). Taken together, these evidences suggest that tDCS may provide benefits related to blood flow, which could help individuals with sTBI by improving hypometabolic areas and regulating those with hyperperfusion.
Our hypothesis is that tDCS applied during the acute phase in individuals with sTBI may facilitate brain plasticity. The anode may promote depolarization of the neuronal membrane and long-term potentiation, which may stimulate hypoactive brain areas. Otherwise, the cathode, which has an inhibitory function, would hyperpolarize the neuronal membrane and promote long-term depression, which may inhibit overactive brain areas (Williams et al., 2009). Because decreased cognition and motor function are the most significant impairments after sTBI, there are plausible reasons for examining the benefits of tDCS in severely disabled individuals with sTBI in the acute phase. In addition, applications focused on the left DLPF cortex in individuals with chronic TBI have already shown improvements in cognition and motor function (Li et al., 2015; O’Neil-Pirozzi et al., 2017; Li L. M. et al., 2019; Li S. et al., 2019; Quinn et al., 2020).
The integrity of white matter–mainly of the stimulated network–in TBI patients may be a factor that positively influences tDCS efficacy in such patients. A study performed by Li and colleagues that anodal stimulation improved response inhibition in control participants, an effect that was not observed in the patient group. The extent of traumatic axonal injury within the salience network strongly influenced the behavioral response to stimulation. Increasing damage to the tract connecting the stimulated right inferior frontal gyrus/anterior insula to the rest of the salience network was associated with reduced beneficial effects of stimulation. In addition, anodal stimulation normalized default mode network activation in patients with poor response inhibition, suggesting that stimulation modulates communication between the networks involved in supporting cognitive control. This is important because can show how patients with TBI can to have positive response to the tDCS approach.
One recommendation is that the severity of encephalopathy following sTBI can be objectified through neurophysiological examinations, such as electroencephalogram. To better characterize the effect of tDCS, a combination of clinical evaluations with electroencephalogram, transcranial magnetic stimulation, and/or other neurophysiological assessments may help in the development of higher quality tDCS studies in sTBI. TMS may be particularly helpful for monitoring motor responses (Zaninotto et al., 2019). In addition, these tools and high-quality imaging examinations can be useful to guide the most appropriate location for placing the electrodes.
Unfortunately, there is a lack of evidence to support or refute the hypothesis of the beneficial effects of tDCS on cognition and motor function in patients with sTBI in the acute/subacute phases (Zaninotto et al., 2019), Although some studies are in progress and show initials results (Leśniak et al., 2014; Boissonnault et al., 2021; De Freitas et al., 2021).
Besides, previous studies have suggested benefits of TMS at chronic stages after TBI (Straudi et al., 2019; Motes et al., 2020; Rushby et al., 2020), the effects of tDCS remain unclear. That is, clinical practice currently follows the do-it-yourself model, based on limited evidence (Lee and Kim, 2018; Pink et al., 2019; Nardone et al., 2020), Estimations emerge from few studies that have showed effective results on motor and cognitive impairments after stroke. We hypothesize that the addition of tDCS to motor, cognitive, or speech therapy early after sTBI would enhance potential benefits on cognition and motor function.
Rehabilitation of individuals after sTBI has major therapeutic challenges influenced by lesion severities, phases, or symptoms. The tDCS applied to individuals with sTBI in the acute phase of the injury may have a facilitating effect on the mechanism of brain plasticity, since the anode electrode promotes depolarization of the neuronal membrane and LTP, and the cathode electrode hyperpolarizes the neuronal membrane and promotes LDP (Williams et al., 2009). In addition, early intervention may help organize the brain recovery and enhance plasticity. Furthermore, the combination of tDCS with cognitive and/or physical training may increase LTP plasticity (Rogers, 2016).
A previous systematic review revealed that new studies are needed to establish tDCS parameters such as electrode positioning, current density, duration, and stimulation intervals, as well as their effects in combination with concomitant therapies. Based on the risks of polypharmacy after sTBI, tDCS may be useful for reducing the need for drugs, or at least counteracting their cognitive side effects. In addition, improved biomarkers of neural damage due to sTBI can help understanding the mechanisms underlying the neurophysiological effects of tDCS and estimating its clinical effects and monitoring therapy. sTBI is a heterogeneous disorder and aids therapists in adapting therapy or identifying those who will most benefit. This becomes particularly challenging as sTBI is typically associated with multiple comorbidities and interventions (Zaninotto et al., 2019).
Until now, most studies after sTBI were carried out during the chronic phase (Villamar et al., 2012). There are no high-quality studies that explore the applicability of tDCS in the acute/subacute phases of sTBI aiming at improving cognitive and motor outcomes. The results of a Systematic review by Hara et al. (2021) point out that in post-stroke patients with deficits in cognitive function, including attention and memory, NIBS shows promising positive effects but this effect is limited, suggesting that further studies are needed with more precision in stimulation sites and stimulation parameters. However, results of the Systematic Review and Meta-Analysis by Ahorsu et al. (2021) showed that the overall effect of NIBS on cognition in people with TBI was moderately significant, Moreover, predictors of clinical and functional recovery after sTBI are still uncertain. These results would help elucidate the aspects linked to recovery and the use of neuromodulation within this context.
On the other hand, despite the growing interest in developing effective and innovative treatment approaches to improve outcomes after sTBI, the application of tDCS in the acute and subacute phases is challenging due to the high probability of epilepsy, unstable clinical conditions and other procedures such as craniectomy decompression and craniotomy that may limit the application of this technique (Ulam et al., 2015; Neville et al., 2019). It is worth mentioning that when it comes to acute stages of sTBI, patient interventions are very limited in clinical trials, therefore, pre-clinical studies in an animal model of acute-phase TBI as of Yoon et al. (2016) can to point stimulation currents, duration of stimulation location of electrodes and safety, to facilitate decision making from clinical trials to acute stage clinical trials in humans with severe brain injury.
The effects of tDCS isolated or in combination with other therapies, as well as the most appropriate doses and intensities for improving motor and cognitive outcomes early after sTBI need to be elucidated. Although preliminary studies have suggested potential effects of tDCS, the current evidence is insufficient to precisely estimate the size effects of applying tDCS in individuals with sTBI. It would be interesting to show the effects of tDCS or an estimate of its effect sizes only in the treatment of patients with TBI by performing a systematic review with meta-analysis in which a qualitative and quantitative analysis of the RCTS data is performed, we have this gap in the literature. The hypothesis raised in this manuscript by the authors and its applicability in the next studies should be carried out to investigate the effects of tDCS in the rehabilitation of TBI patients in the acute/subacute phase.
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
All authors contributed to the development of the manuscript and read and approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor SC declared a past co-authorship with the author AT.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ahorsu, D. K., Adjaottor, E. S., and Lam, B. Y. H. (2021). Intervention effect of non-invasive brain stimulation on cognitive functions among people with traumatic brain injury: A systematic review and meta-analysis. Brain Sci. 11:840. doi: 10.3390/brainsci11070840
Alderman, N., and Wood, R. L. (2013). Neurobehavioural approaches to the rehabilitation of challenging behaviour. NeuroRehabilitation 32, 761–770. doi: 10.3233/NRE-130900
Arêas, F. Z. S., Cordeiro, B. N. L., and Paiva, W. S. (2022). Neuromodulation in acute traumatic brain injury: A tool in the rehabilitation process that needs to be investigated. Sao Paulo Med. J. 140, 846–847. doi: 10.1590/1516-3180.2021.0988.11052022
Areas, F. Z., Schwarzbold, M. L., Diaz, A. P., Rodrigues, I. K., Sousa, D. S., Ferreira, C. L., et al. (2019). Predictors of hospital mortality and the related burden of disease in severe traumatic brain injury: A prospective multicentric study in Brazil. Front. Neurol. 10:432. doi: 10.3389/fneur.2019.00432
Boggio, P. S., Sultani, N., Fecteau, S., Merabet, L., Mecca, T., Pascual-Leone, A., et al. (2008). Prefrontal cortex modulation using transcranial DC stimulation reduces alcohol craving: A double-blind, sham-controlled study. Drug Alcohol Depend. 92, 55–60. doi: 10.1016/j.drugalcdep.2007.06.011
Boissonnault, È., Higgins, J., LaGarde, G., Barthélemy, D., Lamarre, C., and Dagher, J. H. (2021). Brain stimulation in attention deficits after traumatic brain injury: A literature review and feasibility study. Pilot Feasibility Stud. 7:115. doi: 10.1186/s40814-021-00859-3
De Freitas, D. J., De Carvalho, D., Paglioni, V. M., Brunoni, A. R., Valiengo, L., Thome-Souza, M. S., et al. (2021). Effects of transcranial direct current stimulation (tDCS) and concurrent cognitive training on episodic memory in patients with traumatic brain injury: A double-blind, randomised, placebo-controlled study. BMJ Open. 11:e045285. doi: 10.1136/bmjopen-2020-045285
Demirtas-Tatlidede, A., Vahabzadeh-Hagh, A. M., Bernabeu, M., Tormos, J. M., and Pascual-Leone, A. (2012). Noninvasive brain stimulation in traumatic brain injury. J. Head Trauma Rehabil. 27, 274–292.
Elsner, B., Kwakkel, G., Kugler, J., and Mehrholz, J. (2017). Transcranial direct current stimulation (tDCS) for improving capacity in activities and arm function after stroke: A network meta-analysis of randomised controlled trials. J. Neuroeng. Rehabil. 14:95. doi: 10.1186/s12984-017-0301-7
Estraneo, A., Pascarella, A., Moretta, P., Masotta, O., Fiorenza, S., Chirico, G., et al. (2017). Repeated transcranial direct current stimulation in prolonged disorders of consciousness: A double-blind cross-over study. J. Neurol. Sci. 375, 464–470. doi: 10.1016/j.jns.2017.02.036
Fregni, F., and Pascual-Leone, A. (2007). Technology insight: Noninvasive brain stimulation in neurology-perspectives on the therapeutic potential of rTMS and tDCS. Nat. Clin. Pract. Neurol. 3, 383–393. doi: 10.1038/ncpneuro0530
Fregni, F., El-Hagrassy, M. M., Barrios, K. P., Carvalho, S., Leite, J., Simis, M., et al. (2021). Evidence-based guidelines and secondary meta-analysis for the use of transcranial direct current stimulation (tDCS) in neurological and psychiatric disorders. Int. J. Neuropsychopharmacol. 24, 256–313. doi: 10.1093/ijnp/pyaa051
Groppa, S., Bergmann, T. O., Siems, C., Molle, M., Marshall, L., and Siebner, H. R. (2010). Slow-oscillatory transcranial direct current stimulation can induce bidirectional shifts in motor cortical excitability in awake humans. Neuroscience 166, 1219–1225. doi: 10.1016/j.neuroscience.2010.01.019
Gupta, D., Sharma, D., Kannan, N., Prapruettham, S., Mock, C., Wang, J., et al. (2016). Guideline adherence and outcomes in severe adult traumatic brain injury for the CHIRAG (collaborative head injury and guidelines) study. World Neurosurg. 89, 169–179. doi: 10.1016/j.wneu.2015.12.097
Hara, H., Shanmugalingam, A., McIntyre, A., and Burhan, A. M. (2021). The effect of non-invasive brain stimulation (NIBS) on attention and memory function in stroke rehabilitation patients: A systematic review and meta-analysis. Diagnostics 11:227. doi: 10.3390/diagnostics11020227
Junior, L. H. J., Costa, M. D. D. L., Neto, L. H. J., Ribeiro, J. P. M., Freitas, W. J. S. D. N., and Teixeira, M. J. (2015). Estimulação elétrica transcraniana por corrente contínua em fibromialgia: Efeitos sobre a dor e a qualidade de vida, avaliados clinicamente e por cintilografia de perfusão cerebral. Rev. São Paulo 16, 37–42.
Kang, E. K., Kim, D. Y., and Paik, N. J. (2012). Transcranial direct current stimulation of the left prefrontal cortex improves attention in patients with traumatic brain injury: A pilot study. J. Rehabil. Med. 44, 346–350. doi: 10.2340/16501977-0947
Lee, S. A., and Kim, M. K. (2018). Effect of low frequency repetitive transcranial magnetic stimulation on depression and cognition of patients with traumatic brain injury: A randomized controlled trial. Med. Sci. Monit. 24, 8789–8794.
Lefaucheur, J. P., Antal, A., Ayache, S. S., Benninger, D. H., Brunelin, J., Cogiamanian, F., et al. (2017). Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 128, 56–92.
Leśniak, M., Polanowska, K., Seniów, J., and Członkowska, A. (2014). Effects of repeated anodal tDCS coupled with cognitive training for patients with severe traumatic brain injury: A pilot randomized controlled trial. J. Head Trauma Rehabil. 29, E20–E29. doi: 10.1097/HTR.0b013e318292a4c2
Li, L. M., Violante, I. R., Zimmerman, K., Leech, R., Hampshire, A., Patel, M., et al. (2019). Traumatic axonal injury influences the cognitive effect of non-invasive brain stimulation. Brain 142, 3280–3293. doi: 10.1093/brain/awz252
Li, S., Dong, X., Sun, W., Zhao, N., Yu, G., and Shuai, L. (2019). Effects of transcranial direct current stimulation on patients with disorders of consciousness after traumatic brain injury: Study protocol for a randomized, double-blind controlled trial. Trials 20:596.
Li, S., Zaninotto, A. L., Neville, I. S., Paiva, W. S., Nunn, D., and Fregni, F. (2015). Clinical utility of brain stimulation modalities following traumatic brain injury: Current evidence. Neuropsychiatr. Dis. Treat. 11, 1573–1586. doi: 10.2147/NDT.S65816
Lingsma, H. F., Roozenbeek, B., Steyerberg, E. W., Murray, G. D., and Maas, A. I. (2010). Early prognosis in traumatic brain injury: From prophecies to predictions. Lancet Neurol. 9, 543–554.
Maas, A. I. R., Menon, D. K., Adelson, P. D., Andelic, N., Bell, M. J., Belli, A., et al. (2017). Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 16, 987–1048.
Martens, G., Lejeune, N., O’brien, A. T., Fregni, F., Martial, C., Wannez, S., et al. (2018). Randomized controlled trial of home-based 4-week tDCS in chronic minimally conscious state. Brain Stimul. 11, 982–990. doi: 10.1016/j.brs.2018.04.021
Mcmillan, T. M., and Wood, R.L. (eds.) (2017). Neurobehavioural disability and social handicap following traumatic brain injury, 2nd Edn. London: Routledge.
Motes, M. A., Spence, J. S., Yeatman, K., Jones, P. M., Lutrell, M., O’hair, R., et al. (2020). High-definition transcranial direct current stimulation to improve verbal retrieval deficits in chronic traumatic brain injury. J. Neurotrauma 37, 170–177.
Nardone, R., Sebastianelli, L., Versace, V., Brigo, F., Golaszewski, S., Manganotti, P., et al. (2020). Repetitive transcranial magnetic stimulation in traumatic brain injury: Evidence from animal and human studies. Brain Res. Bull. 159, 44–52.
Neville, I. S., Zaninotto, A. L., Hayashi, C. Y., Rodrigues, P. A., Galhardoni, R., Ciampi de Andrade, D., et al. (2019). Repetitive TMS does not improve cognition in patients with TBI: A randomized double-blind trial. Neurology 93, 190–199.
Nitsche, M. A., and Paulus, W. (2000). Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 527(Pt 3), 633–639.
Nitsche, M. A., Cohen, L. G., Wassermann, E. M., Priori, A., Lang, N., Antal, A., et al. (2008). Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 1, 206–223. doi: 10.1016/j.brs.2008.06.004
O’Neil-Pirozzi, T. M., Doruk, D., Thomson, J. M., and Fregni, F. (2017). Immediate memory and electrophysiologic effects of prefrontal cortex transcranial direct current stimulation on neurotypical individuals and individuals with chronic traumatic brain injury: A pilot study. Int. J. Neurosci. 127, 592–600. doi: 10.1080/00207454.2016.1216415
Pink, A. E., Williams, C., Alderman, N., and Stoffels, M. (2019). The use of repetitive transcranial magnetic stimulation (rTMS) following traumatic brain injury (TBI): A scoping review. Neuropsychol. Rehabil. 31, 479–505.
Pruski, A., and Cantarero, G. (2020). Transcranial direct current stimulation for motor recovery following brain injury. Curr. Phys. Med. Rehabil. Rep. 8, 268–279.
Quinn, D. K., Upston, J., Jones, T., Brandt, E., Story-Remer, J., Fratzke, V., et al. (2020). Cerebral perfusion effects of cognitive training and transcranial direct current stimulation in mild-moderate TBI. Front. Neurol. 11:545174. doi: 10.3389/fneur.2020.545174
Rango, M., Cogiamanian, F., Marceglia, S., Barberis, B., Arighi, A., Biondetti, P., et al. (2008). Myoinositol content in the human brain is modified by transcranial direct current stimulation in a matter of minutes: A 1H-MRS study. Magn. Reson. Med. 60, 782–789. doi: 10.1002/mrm.21709
Riggio, S. (2011). Traumatic brain injury and its neurobehavioral sequelae. Neurol. Clin. 29, 35–47.
Rogers, L. (2016). Transcranial direct current stimulation (tDCS): Emerging uses, safety and neurobiological effects. Neurosci. Res. Prog. 104.
Rushby, J. A., De Blasio, F. M., Logan, J. A., Wearne, T., Kornfeld, E., Wilson, E. J., et al. (2020). tDCS effects on task-related activation and working memory performance in traumatic brain injury: A within group randomized controlled trial. Neuropsychol. Rehabil. 31, 814–836. doi: 10.1080/09602011.2020.1733620
Sacco, K., Galetto, V., Dimitri, D., Geda, E., Perotti, F., Zettin, M., et al. (2016). Concomitant use of transcranial direct current stimulation and computer-assisted training for the rehabilitation of attention in traumatic brain injured patients: Behavioral and neuroimaging results. Front. Behav. Neurosci. 10:57. doi: 10.3389/fnbeh.2016.00057
Stewan Feltrin, F., Zaninotto, A. L., Guirado, V. M. P., Macruz, F., Sakuno, D., Dalaqua, M., et al. (2018). Longitudinal changes in brain volumetry and cognitive functions after moderate and severe diffuse axonal injury. Brain Inj. 32, 1208–1217. doi: 10.1080/02699052.2018.1494852
Straudi, S., Bonsangue, V., Mele, S., Craighero, L., Montis, A., Fregni, F., et al. (2019). Bilateral M1 anodal transcranial direct current stimulation in post traumatic chronic minimally conscious state: A pilot EEG-tDCS study. Brain Inj. 33, 490–495. doi: 10.1080/02699052.2019.1565894
Thibaut, A., Bruno, M. A., Ledoux, D., Demertzi, A., and Laureys, S. (2014). tDCS in patients with disorders of consciousness: Sham-controlled randomized double-blind study. Neurology 82, 1112–1118.
Thibaut, A., Wannez, S., Donneau, A. F., Chatelle, C., Gosseries, O., Bruno, M. A., et al. (2017). Controlled clinical trial of repeated prefrontal tDCS in patients with chronic minimally conscious state. Brain Inj. 31, 466–474. doi: 10.1080/02699052.2016.1274776
Trofimov, A. O., Kalentiev, G., Karelsky, M., Ksenofontova, C., Ruzavina, A., Yuriev, M., et al. (2018). Cerebral hemodynamics after transcranial direct current stimulation (tDCS) in patients with consequences of traumatic brain injury. Adv. Exp. Med. Biol. 1072, 59–62. doi: 10.1007/978-3-319-91287-5_10
Ulam, F., Shelton, C., Richards, L., Davis, L., Hunter, B., Fregni, F., et al. (2015). Cumulative effects of transcranial direct current stimulation on EEG oscillations and attention/working memory during subacute neurorehabilitation of traumatic brain injury. Clin. Neurophysiol. 126, 486–496. doi: 10.1016/j.clinph.2014.05.015
Villamar, M. F., Santos Portilla, A., Fregni, F., and Zafonte, R. (2012). Noninvasive brain stimulation to modulate neuroplasticity in traumatic brain injury. Neuromodulation 15, 326–338.
Williams, C., Wood, R. L., and Howe, H. (2019). Alexithymia is associated with aggressive tendencies following traumatic brain injury. Brain Inj. 33, 69–77. doi: 10.1080/02699052.2018.1531302
Williams, J., Imamura, M., and Fregni, F. (2009). Updates on the use of non-invasive brain stimulation in physical and rehabilitation medicine. Rehabil. Med. 41, 305–311.
Yoon, K. J., Lee, Y. T., Chae, S. W., Park, C. R., and Kim, D. Y. (2016). Effects of anodal transcranial direct current stimulation (tDCS) on behavioral and spatial memory during the early stage of traumatic brain injury in the rats. J. Neurol. Sci. 362, 314–320. doi: 10.1016/j.jns.2016.02.005
Keywords: traumatic brain injury, neuromodulation, transcranial direct current stimulation, cognition, functionality, rehabilitation
Citation: Cordeiro BNL, Kuster E, Thibaut A, Rodrigues Nascimento L, Gonçalves JV, Arêas GPT, Paiva WS and Arêas FZS (2023) Is transcranial direct current stimulation (tDCS) effective to improve cognition and functionality after severe traumatic brain injury? A perspective article and hypothesis. Front. Hum. Neurosci. 17:1162854. doi: 10.3389/fnhum.2023.1162854
Received: 10 February 2023; Accepted: 27 July 2023;
Published: 10 August 2023.
Edited by:
Sandra Carvalho, University of Aveiro, PortugalReviewed by:
Maíra Izzadora Souza Carneiro, Federal University of Pernambuco, BrazilCopyright © 2023 Cordeiro, Kuster, Thibaut, Rodrigues Nascimento, Gonçalves, Arêas, Paiva and Arêas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernando Zanela da Silva Arêas, ZmVybmFuZG96YW5lbGFAaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.