
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Hum. Neurosci. , 11 August 2021
Sec. Brain Health and Clinical Neuroscience
Volume 15 - 2021 | https://doi.org/10.3389/fnhum.2021.666468
This article is part of the Research Topic Occupational Neuroscience: Nervous System's Health at the Workplace View all 9 articles
 Salvatore Zaffina1,2†
Salvatore Zaffina1,2† Paola Lanteri3*
Paola Lanteri3* Francesco Gilardi4†
Francesco Gilardi4† Sergio Garbarino5
Sergio Garbarino5 Annapaola Santoro1Maria Rosaria Vinci1,2
Annapaola Santoro1Maria Rosaria Vinci1,2 Rita Carsetti6Alessandro Scorpecci7Massimiliano Raponi8Nicola Magnavita2,9‡Vincenzo Camisa1,2‡
Rita Carsetti6Alessandro Scorpecci7Massimiliano Raponi8Nicola Magnavita2,9‡Vincenzo Camisa1,2‡A case of recurrent coronavirus disease 2019 (COVID-19) with neurovestibular symptoms was reported. In March 2020, a physician working in an Italian pediatric hospital had flu-like symptoms with anosmia and dysgeusia, and following a reverse transcription PCR (RT/PCR) test with a nasopharyngeal swab tested positive for SARS-CoV-2. After home quarantine, 21 days from the beginning of the symptoms, the patient tested negative in two subsequent swabs and was declared healed and readmitted to work. Serological testing showed a low level of immunoglobulin G (IgG) antibody title and absence of immunoglobulin M (IgM). However, 2 weeks later, before resuming work, the patient complained of acute vestibular syndrome, and the RT/PCR test with mucosal swab turned positive. On the basis of the literature examined and reviewed for recurrence cases and vestibular symptoms during COVID-19, to our knowledge this case is the first case of recurrence with vestibular impairment as a neurological symptom, and we defined it as probably a viral reactivation. The PCR retest positivity cannot differentiate re-infectivity, relapse, and dead-viral RNA detection. Serological antibody testing and viral genome sequencing could be always performed in recurrence cases.
In China, in December 2019, the epidemic caused by severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) rapidly diffused all over the world leading to a pandemic. While the coronavirus disease 2019 (COVID-19) typically presents as a self-limiting respiratory disease, and in hospitalized patients, the clinical picture is dominated by respiratory distress (Del Sole et al., 2020), progression to severe illness with multiorgan involvement, including the blood vessels, heart, gut, kidneys, testicles, and brain has been reported (Asadi-Pooya and Simani, 2020; Chen X. et al., 2020; Ibrahim, 2020; Leonardi et al., 2020; Nepal et al., 2020). Patients suffering from COVID-19 can develop acute or long-term neurological sequelae (Ellul et al., 2020). The prevalence of neuro-COVID varies considerably between individual studies ranging from 4.1% (Xiong et al., 2020) to 57.4% (Romero-Sánchez et al., 2020) and even 84% in COVID-19 with acute respiratory distress syndrome (Helms et al., 2020). The onset of nervous system damage can be asynchronous with systemic manifestations and the typically salient severe respiratory disease (Vavougios, 2020).
In our pediatric hospital, between March and May 2020, there were 25 cases of COVID-19 among healthcare workers (HCWs), equal to 1.1% of the total staff. Two of them had at least one symptom, namely, headache, anosmia, and dysgeusia or all the three symptoms at the same time. These neurological symptoms indicate that the virus, like other respiratory viruses (Bohmwald et al., 2018), enters the central nervous system (CNS) through the olfactory bulb causing inflammation. Furthermore, SARS-CoV-2 viruses can spread from the mechano- and chemo-receptors in the lungs and lower respiratory airways to the medullary cardiorespiratory center via a synapse-connected route (Li Y. C. et al., 2020).
In this study, we report a case of recurrent SARS-CoV-2 infection with neurovestibular involvement, review literature cases with vestibular involvement, and discuss the neurotropism of this virus based on literature data.
A 48-year-old female physician in a pediatric hospital presented cough, slight dyspnea, severe myalgia, asthenia, and headache on March, 2020, followed by anosmia and dysgeusia over the following few days (Figure 1) without fever. When symptoms appeared the worker self-isolated at home. The allergic rhinitis the patient suffers from led to a short delay in diagnosis; however, a swab carried out 8 days from the beginning of the symptoms tested positive for SARS-CoV-2 (Allplex™2019-nCoV Assay). In subsequent days, the patient felt better and became asymptomatic. On days 23 and 27 the patient was retested and was negative both times. On day 37, serology was performed by ELISA and a low level of immunoglobulin G (IgG) against SARS-CoV-2 was detected. Immunoglobulin M (IgM) search was negative. She was feeling well and was declared fit to work by the occupational physician of the hospital. However, before returning to work, on day 39 the patient woke up experiencing intensive dizziness, described as subjective vertigo, associated with vomiting and bilateral aural fullness (Figure 1). The dizziness quickly got worse as the patient lied supine on the right side. She was transported by ambulance to the emergency room of a hospital where dizzying syndrome was diagnosed and treated with metoclopramide. Physical examination revealed normal vital signs, while the patient was breathing ambient air. Some relevant auxiliary examinations such as blood routine, coagulation function, liver and renal function, electrolytes, and inflammation indicators were completed, and the results were normal. After 3 h and the improvement of the symptoms, she was discharged home, cared by health public service, and treated with betahistine dihydrochloride for 1 week. The day after, on day 40, a nasal swab was obtained, which tested positive.
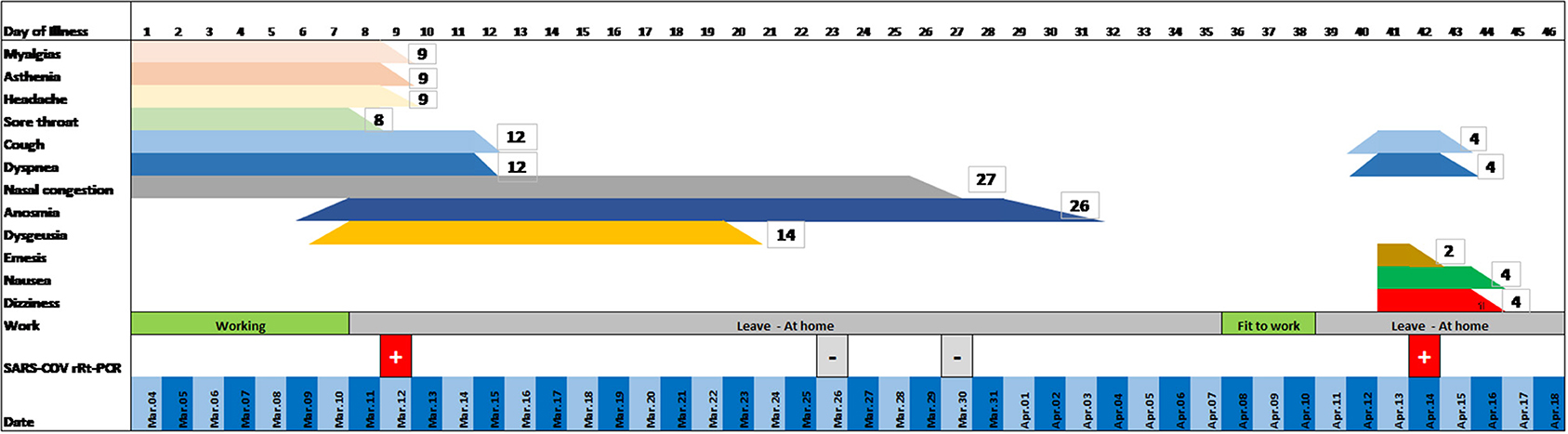
Figure 1. Clinical evolution of the patient: timeline.
In the following days, the dizziness disappeared and only a mild postural instability persisted, whereas aural fullness was unchanged. The only pathology that she suffered from was allergic rhinitis. She had never suffered from dizziness in the past.
An ear, nose, and throat (ENT) visit took place on day 44. Otoscopy was negative. Romberg, Unterberger (March-in-place), and finger-to-nose tests were negative. Neither bedside vestibular examination with Frenzel glasses showed spontaneous nystagmus, nor was nystagmus evoked by supine position, Dix-Hallpike maneuver, lateral head rotation, and Rose position. The head-shaking test was negative. The only relevant finding of the vestibular examination was the patient complaining about slight dizziness during the Dix-Hallpike maneuver on the right side (supine position with the head hyperextended and tilted to the right side). The patient did not develop fever both in the first and in the second phase of the symptoms related to COVID-19. Despite fever being one of the most common symptoms of COVID-19, it may be absent in some individuals. Finally, the patient was completely healed without any deficit and was able to return to work.
The case reported presents numerous points of interest. First, the recurring nature of the symptoms must be emphasized along with the neurological origin of the symptoms themselves. Second, the neurotropism and neuroinvasive potential of the virus into recurrence mode should be considered. Finally, the observation that the presence of anti-spike IgG has been followed by a positive PCR test; this feature is rather infrequent, having been found in 0.13 per 10,000 days at risk in HCWs, whereas the probability of having a positive PCR test in the anti-spike–seronegative HCWs is significantly higher (1.09 per 10,000 days at risk) (Lumley et al., 2020).
The presence of at least two consecutive negative RT-PCR tests in respiratory samples (with samples taken at least 24 h apart) and the appearance of specific IgG at serological test, according to the discharge criteria of the European Centre for Disease Prevention and Control (Yahav et al., 2021), permits to classify the case exposed as recurrent COVID-19 with multiple district neurological symptoms (vestibular symptoms, previously anosmia and dysgeusia). Indeed reinfection should be considered during the first 90 days if clinical symptoms of the first episode resolve and two PCR tests were negative before the new episode (Yahav et al., 2021).
Currently, there are numerous reports that a number of patients tested positive again after two consecutive negative PCR tests or after clinical recovery (Table 1) (Falahi and Kenarkoohi, 2020). Nasopharyngeal swabs tend to have a higher sensitivity than the other samples and are the most common method for diagnosis of COVID-19 recurrence, regardless of the clinical disease manifestation. With the progression of SARS-CoV-2 infection, the virus could migrate from the upper respiratory tract to the lower respiratory tract and lungs, resulting in insufficient viral load in the upper respiratory tract, which may explain the negative result of the nasopharyngeal swab test. The detection rate and sensitivity have been improved by multisite specimen collection and serological assays (Table 1). The prevalence of disease recurrence among COVID-19 recovered patients was approximately 14.8%, ranging from 7.35 to 21.4% (Azam et al., 2020; Hoang, 2020). The interval duration from the last negative PCR tests to recurrent positive results ranged from 1 to 123 days (min average 16.16 ± 20.93 ds, max average 25.39 ± 23.00 ds) for 1,038 cases in a selected population of 13,565 patients (Table 1). The case described experienced at the onset two of the three typical symptoms in the first phase of infection, namely, cough (68%) and shortness of breath (66%) without fever (69%). About 92% of the patients experienced at least one of these, less frequently in women (66, 64, 66 respectively; 90% at least one of these; vs. men 70, 67, 71; 93%, each p < 0.001) (ISARIC Clinical Characterisation Group, 2021). She presented symptoms of recurrence 17 days from the last negative PCR tests, in accordance with the literature. True reinfection has criteria that must be considered, including isolation of the complete genome of the virus (and not just genomic fragments) in the second episode (Falahi and Kenarkoohi, 2020), but we did not have this data. In our patient, we could suspect a viral reactivation due to low level of IgG against SARS-CoV-2 detected, even without lymphopenia. It is also possible that the immune responses can suppress, but not completely eradicate, SARS-CoV-2, which may have led to the false-negative results due to lower viral loads (Chen J. et al., 2020). Once the virus starts replicating again, the RT-PCR results reverted to positive and expressed as a new neuroinvasion in the vestibular system. NeuroCovid is now well-known (Whittaker et al., 2020), but recurrence of positive RT-PCR with neurological symptoms is very rare and no further instances of vestibular symptoms are described as recurrence (Table 1). To our knowledge, this is the first case of vestibular symptoms as recurrence of positive RT-PCR SARS-CoV-2. This case shows the neuroinvasive potentials of SARS-CoV-2 and the possibility of disease reactivation after clinical and analytic recovery. SARS-CoV-2 might be latent in some neurons to hide from immune surveillance (Brandt and Dieterich, 2017; Zhang M. et al., 2020). For reasons unclear, after an apparent remission the virus reactivated and was again identifiable in the respiratory tract. At the same time, the multiplication in the nervous system caused recurrence with intense neurological disturbance, clinically highlighted by dizziness associated with slight dyspnea.

Table 1. Recurrent cases reported in literature.
The clinical picture and subsequent ENT are compatible with a diagnosis of the spontaneous acute vestibular syndrome. The most common cause is an acute peripheral vestibulopathy known as vestibular neuritis, affecting the vestibular nerve or “pseudoneuritis” if the acute lesions affect the root entry zone of the eighth nerve or the vestibular nucleus (Wu Y. et al., 2020).
The neuroinvasive potential of SARS-CoV-2 is highlighted by some studies (Baig, 2020; Magnavita et al., 2020).
A relapse of the disease with the involvement of the nervous system may indicate that the virus can be neurotropic since the beginning of the disease or in its recurrence form.
The virus may reach the central nervous system via the olfactory nerve. Olfactory and gustatory dysfunctions without rhinorrhea or nasal obstruction are distinctive of patients with mild-to-moderate COVID-19 infection (Baig, 2020; Cooper et al., 2020; Magnavita et al., 2020; Paniz-Mondolfi et al., 2020; Wu Y. et al., 2020), leading to speculation regarding the olfactory nerve as a possible route of the central nervous system entry.
Dizziness is a common onset symptom of COVID-19 (Table 2). This symptom is often considered a non-specific neurological manifestation and is not actively researched or detailed in the description of the clinical picture. This can lead to variability of prevalence estimates, ranging from 3 to 16% between studies. Dizziness such as headache, fatigue, and myalgia are all likely to be caused by the systemic condition if not well-characterized. Specific vestibular or hearing impairment is rarely reported (Table 2). Vertigo should be investigated in SARS-CoV-2 patients and considered along with neurological signs induced by the invasion of the vestibular pathway from the nerve to the vestibular nuclei complex. It is plausible to hypothesize that if the SARS-CoV-2 can also reach the brain from the lungs through the vagus nerve, the virus will invade the brainstem starting with the vagal nucleus and surrounding sites, including the respiratory control center and more, which can lead to more respiratory dysfunction that further exacerbates the damage caused by the primary infection in the lungs or others neurological symptoms (Lukiw et al., 2020; Yachou et al., 2020), such as vestibular impairment. This hypothesis is supported by the evidence of the presence of a consistent angiotensin-converting enzyme (ACE2) expression across the cerebral cortex. The highest ACE2 expression was found in the pons and the medulla oblongata (Guan et al., 2020). Indeed, SARS-CoV-2 appears to bind exclusively to the ACE2 protein, a single-pass type 1 transmembrane receptor with its enzymatically active domain exposed on the surface of multiple cell types, such as type II alveolar cells of the respiratory system, enterocytes and intestinal epithelial cells, endothelial cells, epithelial cells of the conjunctival epithelium, kidney cells (renal tubules), and certain immune cells, such as the alveolar monocytes/macrophages and certain cells of the CNS including those of the cerebral cortex, especially the brainstem (Zubair et al., 2019; Chigr et al., 2020; Kabbani and Olds, 2020; Li C. et al., 2020; Li M. et al., 2020; Panupattanapong and Brooks, 2020; Zhou L. et al., 2020; 154). The highest levels of ACE2-expression in the brain were found in the pons and medulla oblongata, the breathing centers of the brain, which may in part explain the unusually strong ability of SARS-CoV-2 to disrupt normal respiration and pulmonary manifestations including shortness of breath, impaired breathing, and severe respiratory distress. Significant neuroinvasion involving SARS-CoV-2 has been reported from both patients and experimental animals, where the brainstem was heavily infected from apparent spreading via a synapse-connected route to the medullary cardiorespiratory centers (Panupattanapong and Brooks, 2020).
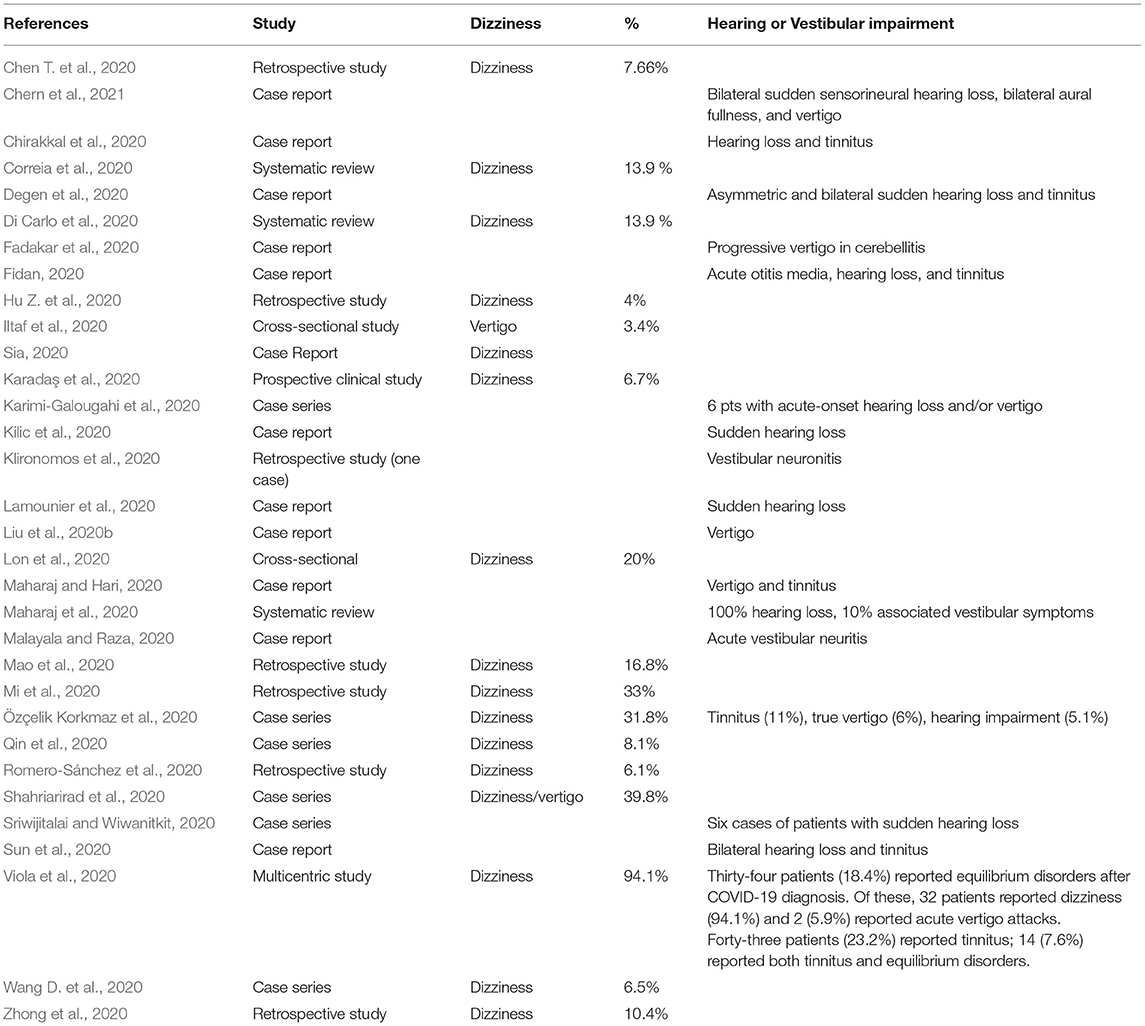
Table 2. Dizziness as clinical onset symptom reported in literature.
A limitation of this case consists of the absence of magnetic resonance documentation of vestibular impairment and the genetic characterization of the viruses at the onset and recurrence of COVID-19. The rapid resolution of clinical symptoms within a few days and the trend of not submitting the non-hospitalized patient to neuroimaging exam above all in patients with low suspicions of CNS disease and plan for outpatient ENT visit in the pandemic period, prompted the emergency physician not to proceed. Several causes for repositive tests for SARS-CoV-2 in COVID-19 patients during the recovery period have been described. They include false RT-PCR results or positive due to traces of the RNA genome, intermittent virus shedding, viral reactivation in people with low antibody levels or immunity, reinfection with another SARS-CoV-2 strain, an acute severe systemic inflammatory response known as cytokine release syndrome (CRS), or exposure to a contaminated environmental surface after discharge (Yang et al., 2020; Dao et al., 2021). Various molecular diagnostic assays have been developed and used worldwide, but the differences in their diagnostic performances remain poorly understood (Matsumura et al., 2020; Liotti et al., 2021; Wang M. et al., 2021). Most of the articles do not report the commercial kit used for RT-PCR, and, where reported, the sensitivity and specificity data for the kit is not often available in the literature (Table 1). All the assays exhibited a specificity of 100%, while sensitivity varied (Table 1). The RT-PCR test cannot distinguish between live and dead viruses, but most recurrence of positive RT-PCR is expressed in an asymptomatic way; therefore likely due to dead viruses. We did not perform a genetic characterization of the viruses in order to distinguish between reinfection and reactivation of SARS-CoV-2 in our repositive patient.
This case is suggestive of colonization of the nervous system that can also result in clinical manifestations in cases of recurrence witnessing the diffusion or permanence of SARS-CoV-2 in the nervous system. It also suggests the neurotrophic hypothesis with the possibility of brainstem invasion (pons and medulla oblongata) and the possibility of recurrence with a SARS-CoV-2 positive RT-PCR test and of clinical recurrence with specific neurological symptoms.
Neurological symptoms should be sought and typified in each SARS-CoV-2 patient.
With the outbreak of COVID-19, to better manage the current phase of the pandemic, we should be vigilant for the presence of any neurological symptoms, both as an onset and as a recurrence of infection.
On the basis of the literature examined and reviewed, for recurrence cases and vestibular symptoms during COVID-19, to our knowledge, this is the first case of recurrence with vestibular impairment as neurological symptom, and we suspect it is likely due to viral reactivation. The PCR retest positivity cannot differentiate between reinfectivity and relapse, and dead-viral RNA detection, serological antibody testing, and viral genome sequencing could be always performed in recurrence cases.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
All authors equally contributed to the conception and design of the study. All the authors agreed on the previous version of the manuscript, read, and approved the final manuscript.
As for FG, Medical Director of the Italian Ministry of Health, the opinion and contents expressed in the study are the sole responsibility of the author, and they are not attributable in any way to the institutional and functional positions held by the same at the Italian Ministry of Health (Article 12, paragraph 6, of the Code of Conduct of the Italian Ministry of Health, adopted with DM March 6, 2015 and later).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdullah, M. S., Chong, P. L., Asli, R., Momin, R. N., Mani, B. I., Metussin, D., et al. (2020). Post discharge positive re-tests in COVID-19: common but clinically non-significant. Infect. Dis. 24, 743–7485. doi: 10.1080/23744235.2020.1780309
Alonso, F. O. M., Sabino, B. D., Guimarães, M. A. A. M., and Varella, R. B. (2020). Recurrence of SARS-CoV-2 infection with a more severe case after mild COVID-19, reversion of RT-qPCR for positive and late antibody response: case report. J. Med. Virol. 14:10.1002/jmv.26432. doi: 10.1002/jmv.26432
An, J., Liao, X., Xiao, T., Qian, S., Yuan, J., Ye, H., et al. (2020). Clinical characteristics of recovered COVID-19 patients with re-detectable positive RNA test. Ann. Transl. Med. 8:1084. doi: 10.21037/atm-20-5602
Asadi-Pooya, A. A., and Simani, L. (2020). Central nervous system manifestations of COVID-19: a systematic review. J. Neurol. Sci. 413:116832. doi: 10.1016/j.jns.2020.116832
Azam, M., Sulistiana, R., Ratnawati, M., Fibriana, A. I., Bahrudin, U., Widyaningrum, D., et al. (2020). Recurrent SARS-CoV-2 RNA positivity after COVID-19: a systematic review and meta-analysis. Sci. Rep. 10:20692. doi: 10.1038/s41598-020-77739-y
Baig, A. M. (2020). Neurological manifestations in COVID-19 caused by SARS-CoV-2. CNS Neurosci. Ther. 7, 499–501. doi: 10.1111/cns.13372
Bentivegna, E., Sentimentale, A., Luciani, M., Speranza, M. L., Guerritore, L., and Martelletti, P. (2020). New IgM seroconversion and positive RT-PCR test after exposure to the virus in recovered COVID-19 patient. J. Med. Virol. 2020:10.1002/jmv.26160. doi: 10.1002/jmv.26160
Bohmwald, K., Galvez, N., Ríos, M., and Kalergis, A. M. (2018). Neurologic alterations due to respiratory virus infections. Front. Cell. Neurosci. 12:386. doi: 10.3389/fncel.2018.00386
Bongiovanni, M., Vignati, M., Giuliani, G., Manes, G., Arienti, S., Pelucchi, L., et al. (2020). The dilemma of COVID-19 recurrence after clinical recovery. J. Infect. 81, 979–997. doi: 10.1016/j.jinf.2020.08.019
Brandt, T., and Dieterich, M. (2017). The dizzy patient: don't forget disorders of the central vestibular system. Nat. Rev. Neurol. 13, 352–362. doi: 10.1038/nrneurol.2017.58
Cao, H., Ruan, L., Liu, J., and Liao, W. (2020). The clinical characteristic of eight patients of COVID-19 with positive RT-PCR test after discharge. J. Med. Virol. 92, 2159–2164. doi: 10.1002/jmv.26017
Cento, V., Colagrossi, L., Nava, A., Lamberti, A., Senatore, S., Travi, G., et al. (2020). Persistent positivity and fluctuations of SARS-CoV-2 RNA in clinically-recovered COVID-19 patients. J. Infect. 81, e90–e92. doi: 10.1016/j.jinf.2020.06.024
Chae, K. J., Jin, G. Y., Lee, C. S., Lee, H. B., Lee, J. H., and Kwon, K. S. (2020). Positive conversion of COVID-19 after two consecutive negative RT-PCR results: a role of low-dose CT. Eur. J. Radiol. 129:109122. doi: 10.1016/j.ejrad.2020.109122
Chen, D., Xu, W., Lei, Z., Huang, Z., Liu, J., Gao, Z., et al. (2020). Recurrence of positive SARS-CoV-2 RNA in COVID-19: a case report. Int. J. Infect. Dis. 93, 297–299. doi: 10.1016/j.ijid.2020.03.003
Chen, J., Xu, X., Hu, J., Chen, Q., Xu, F., Liang, H., et al. (2020). Clinical course and risk factors for recurrence of positive SARS-CoV-2 RNA: a retrospective cohort study from Wuhan, China. Aging (Albany NY). 12, 16675–16689. doi: 10.18632/aging.103795
Chen, M., An, W., Xia, F., Yang, P., Li, K., Zhou, Q., et al. (2020). Clinical characteristics of rehospitalized patients with COVID-19 in China. J. Med. Virol. 92, 2146–2151. doi: 10.1002/jmv.26002
Chen, S. L., Xu, H., Feng, H. Y., Sun, J. F., Li, X., Zhou, L., et al. (2020). Epidemiological and clinical findings of short-term recurrence of severe acute respiratory syndrome coronavirus 2 ribonucleic acid polymerase chain reaction positivity in 1282 discharged coronavirus disease 2019 cases: a multicenter, retrospective, observational study. Open Forum Infect. Dis. 7:ofaa432. doi: 10.1093/ofid/ofaa432
Chen, T., Wu, D., Chen, H., Yan, W., Yang, D., Chen, G., et al. (2020). Clinical characteristics of 113 deceased patients with coronavirus disease 2019: retrospective study. BMJ 368:m1091. doi: 10.1136/bmj.m1091
Chen, X., Laurent, S., Onur, O. A., Kleineberg, N. N., Fink, G. R., Schweitzer, F., et al. (2020). A systematic review of neurological symptoms and complications of COVID-19. J. Neurol. 20, 1–11. doi: 10.1007/s00415-020-10067-3
Chen, Y., Bai, W., Liu, B., Huang, J., Laurent, I., Chen, F., et al. (2020). Re-evaluation of retested nucleic acid-positive cases in recovered COVID-19 patients: Report from a designated transfer hospital in Chongqing, China. J. Infect. Public Health. 13, 932–934. doi: 10.1016/j.jiph.2020.06.008
Chern, A., Famuyide, A. O., Moonis, G., and Lalwani, A. K. (2021). Bilateral sudden sensorineural hearing loss and intralabyrinthine hemorrhage in a patient with COVID-19. Otol. Neurotol. 42, e10–e14. doi: 10.1097/MAO.0000000000003233
Chigr, F., Merzouki, M., and Najimi, M. (2020). Autonomic brain centers and pathophysiology of COVID-19. ACS Chem. Neurosci. 11, 1520–1522. doi: 10.1021/acschemneuro.0c00265
Chirakkal, P., Hail, A. N. A., Zada, N., and Vijayakumar, D. S. (2020). COVID-19 and tinnitus. Ear Nose Throat J. 4:145561320974849. doi: 10.1177/0145561320974849
Cooper, K. W., Brann, D. H., Farruggia, M. C., Bhutani, S., Pellegrino, R., Tsukahara, T., et al. (2020). COVID-19 and the chemical senses: supporting players take center stage. Neuron 107, 219–233. doi: 10.1016/j.neuron.2020.06.032
Correia, A. O., Feitosa, P. W. G., Moreira, J. L. S., Nogueira, S. Á. R., Fonseca, R. B., and Nobre, M. E. P. (2020). Neurological manifestations of COVID-19 and other coronaviruses: a systematic review. Neurol. Psychiatry Brain Res. 37, 27–32. doi: 10.1016/j.npbr.2020.05.008
Crouwel, F., Waaijenberg-Warmenhoven, P., Buiter, H. J. C., and de Boer, N. K. (2020). Recurrent COVID-19 in a patient with ulcerative colitis on vedolizumab therapy. J. Crohns Colitis. 22:jjaa259. doi: 10.1093/ecco-jcc/jjaa259
Dao, T. L., Hoang, V. T., and Gautret, P. (2021). Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: a narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 40, 13–25. doi: 10.1007/s10096-020-04088-z
Degen, C., Lenarz, T., and Willenborg, K. (2020). Acute profound sensorineural hearing loss after COVID-19 pneumonia. Mayo Clin. Proc. 95, 1801–1803. doi: 10.1016/j.mayocp.2020.05.034
Del Sole, F., Farcomeni, A., Loffredo, L., Carnevale, R., Menichelli, D., Vicario, T., et al. (2020). Features of severe COVID-19: a systematic review and meta-analysis. Eur. J. Clin. Invest. 50:e13378. doi: 10.1111/eci.13378
Deng, W., Guang, T. W., Yang, M., Li, J. R., Jiang, D. P., Li, C. Y., et al. (2020). Positive results for patients with COVID-19 discharged form hospital in Chongqing, China. BMC Infect. Dis. 20:429. doi: 10.1186/s12879-020-05151-y
Di Carlo, D. T., Montemurro, N., Petrella, G., Siciliano, G., Ceravolo, R., and Perrini, P. (2020). Exploring the clinical association between neurological symptoms and COVID-19 pandemic outbreak: a systematic review of current literature. J. Neurol. 1, 1–9. doi: 10.21203/rs.3.rs-27152/v1
Dou, C., Xie, X., Peng, Z., Tang, H., Jiang, Z., Zhong, Z., et al. (2020). A case presentation for positive SARS-CoV-2 RNA recurrence in a patient with a history of type 2 diabetes that had recovered from severe COVID-19. Diabetes Res. Clin. Pract. 166:108300. doi: 10.1016/j.diabres.2020.108300
Dou, P., Zhang, S., Wang, C., Cai, L., Liu, Z., Xu, Q., et al. (2020). Serial CT features in discharged COVID-19 patients with positive RT-PCR re-test. Eur. J. Radiol. 127:109010. doi: 10.1016/j.ejrad.2020.109010
Du, H. W., Chen, J.-N., Pan, X. B., Chen, X.-L., Yixian-Zhang Fang, S. F., et al. (2020). Prevalence and outcomes of re-positive nucleic acid tests in discharged COVID-19 patients. Eur. J. Clin. Microbiol. Infect. Dis. 31, 1–5. doi: 10.1007/s10096-020-04024-1
Duggan, N. M., Ludy, S. M., Shannon, B. C., Reisner, A. T., and Wilcox, S. R. (2021). Is novel coronavirus 2019 reinfection possible? Interpreting dynamic SARS-CoV-2 test results. Am. J. Emerg. Med. 39, 256.e1–256.e3. doi: 10.1016/j.ajem.2020.06.079
Ellul, M. A., Benjamin, L., Singh, B., Lant, S., Michael, B. D., Easton, A., et al. (2020). Neurological associations of COVID-19. Lancet Neurol. 19, 767–783. doi: 10.1016/S1474-4422(20)30221-0
Fadakar, N., Ghaemmaghami, S., Masoompour, S. M., Shirazi Yeganeh, B., Akbari, A., Hooshmandi, S., et al. (2020). A first case of acute cerebellitis associated with coronavirus disease (COVID-19): a case report and literature review. Cerebellum 31, 1–4. doi: 10.1007/s12311-020-01177-9
Falahi, S., and Kenarkoohi, A. (2020). COVID-19 reinfection: prolonged shedding or true reinfection? New Microbes New Infect. 38:100812. doi: 10.1016/j.nmni.2020.100812
Fernandes Valente Takeda, C., Moura de Almeida, M., Gonçalves de Aguiar Gomes, R., Cisne Souza, T., Alves de Lima Mota, M., Pamplona de Góes Cavalcanti, L., et al. (2020). Case report: recurrent clinical symptoms of COVID-19 in healthcare professionals: a series of cases from Brazil. Am. J. Trop. Med. Hyg. 103, 1993–1996. doi: 10.4269/ajtmh.20-0893
Fidan, V. (2020). New type of corona virus induced acute otitis media in adult. Am. J. Otolaryngol. 41:102487. doi: 10.1016/j.amjoto.2020.102487
Fu, W., Chen, Q., and Wang, T. (2020). Letter to the Editor: three cases of redetectable positive SARS-CoV-2 RNA in recovered COVID-19 patients with antibodies. J. Med. Virol. 92, 2298–2301. doi: 10.1002/jmv.25968
Gao, G., Zhu, Z., Fan, L., Ye, S., Huang, Z., Shi, Q., et al. (2020). Absent immune response to SARS-CoV-2 in a 3-month recurrence of coronavirus disease 2019 (COVID-19) case. Infection 28, 1–5. doi: 10.1007/s15010-020-01485-6
Geling, T., Huaizheng, G., Ying, C., and Hua, H. (2020). Recurrent positive nucleic acid detection in a recovered COVID-19 patient: a case report and literature review. Respir. Med. Case Rep. 31:101152. doi: 10.1016/j.rmcr.2020.101152
Gidari, A., Nofri, M., Saccarelli, L., Bastianelli, S., Sabbatini, S., Bozza, S., et al. (2021). Is recurrence possible in coronavirus disease 2019 (COVID-19)? Case series and systematic review of literature. Eur. J. Clin. Microbiol. Infect. Dis. 40, 1–12. doi: 10.1007/s10096-020-04057-6
Gousseff, M., Penot, P., Gallay, L., Batisse, D., Benech, N., Bouiller, K., et al. (2020). Clinical recurrences of COVID-19 symptoms after recovery: viral relapse, reinfection or inflammatory rebound? J. Infect. 81, 816–846. doi: 10.1016/j.jinf.2020.06.073
Guan, W. J., Ni, Z. Y., Hu, Y., Liang, W. H., Ou, C. Q., He, J. X., et al. (2020). China Medical Treatment Expert Group for Covid-19. clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382, 1708–1720. doi: 10.1056/NEJMoa2002032
Guo, X., Zeng, L., Huang, Z., He, Y., Zhang, Z., and Zhong, Z. (2020). Longer duration of SARS-CoV-2 infection in a case of mild COVID-19 with weak production of the specific IgM and IgG antibodies. Front. Immunol. 11:1936. doi: 10.3389/fimmu.2020.01936
Habibzadeh, P., Sajadi, M. M., Emami, A., Karimi, M. H., Yadollahie, M., Kucheki, M., et al. (2020). Rate of re-positive RT-PCR test among patients recovered from COVID-19. Biochem. Med. 30:030401. doi: 10.11613/BM.2020.030401
Hao, S., Lian, J., Lu, Y., Jia, H., Hu, J., Yu, G., et al. (2020). Decreased B cells on admission associated with prolonged viral RNA shedding from the respiratory tract in coronavirus disease 2019: a case-control study. J. Infect. Dis. 222, 367–371. doi: 10.1093/infdis/jiaa311
He, F., Luo, Q., Lei, M., Fan, L., Shao, X., Hu, K., et al. (2020). Successful recovery of recurrence of positive SARS-CoV-2 RNA in COVID-19 patient with systemic lupus erythematosus: a case report and review. Clin. Rheumatol. 39, 2803–2810. doi: 10.1007/s10067-020-05230-0
Helms, J., Kremer, S., Merdji, H., Clere-Jehl, R., Schenck, M., Kummerlen, C., et al. (2020). Neurologic features in severe SARS-CoV-2 infection. N. Engl. J. Med. 382, 2268–2270. doi: 10.1056/NEJMc2008597
Hoang, T. (2020). Systematic review and meta-analysis of factors associated with re-positive viral RNA after recovery from COVID-19. J. Med. Virol. 93, 2234–2242. doi: 10.1002/jmv.26648
Hu, R., Jiang, Z., Gao, H., Huang, D., Jiang, D., Chen, F., et al. (2020). Recurrent positive reverse transcriptase-polymerase chain reaction results for coronavirus disease 2019 in patients discharged from a hospital in China. JAMA Netw. Open 3:e2010475. doi: 10.1001/jamanetworkopen.2020.10475
Hu, Z., Song, C., Xu, C., Jin, G., Chen, Y., Yu, X., et al. (2020). Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci. Chi. Life Sci. 63, 706–711. doi: 10.1007/s11427-020-1661-4
Huang, J., Zheng, L., Li, Z., Hao, S., Ye, F., Chen, J., et al. (2020). Recurrence of SARSCoV-2 PCR positivity in COVID-19 patients: a single center experience and potential implications. MedRxiv 2020.05.06.20089573. doi: 10.1101/2020.05.06.20089573
Ibrahim, W. (2020). Neurological manifestations in coronavirus disease 2019 (COVID-19) patients: a systematic review of literature. CNS Spectr. 21, 1–12. doi: 10.1017/S1092852920001935
Iltaf, S. Sr., Fatima, M., Salman, S. Sr., Salam, J. U., and Abbas, S. (2020). Frequency of neurological presentations of coronavirus disease in patients presenting to a tertiary care hospital during the 2019 coronavirus disease pandemic. Cureus 12:e9846. doi: 10.7759/cureus.9846
ISARIC Clinical Characterisation Group (2021). COVID-19 symptoms at hospital admission vary with age and sex: results from the ISARIC prospective multinational observational study. Infection 1–17. doi: 10.1007/s15010-021-01599-5
Jiang, M., Li, Y., Han, M., Wang, Z., Zhang, Y., and Du, X. (2020). Recurrent PCR positivity after hospital discharge of people with coronavirus disease 2019 (COVID-19). J. Infect. 81, 147–178. doi: 10.1016/j.jinf.2020.03.024
Kabbani, N., and Olds, J. L. (2020). Does COVID19 infect the brain? Mol. Pharmacol. 97, 351–353. doi: 10.1124/molpharm.120.000014
Kang, Y.-J. (2020). South Korea's COVID-19 infection status: from the perspective of re-positive test results after viral clearance evidenced by negative test results. Disaster Med. Public Health Prep. 2020, 1–3. doi: 10.1017/dmp.2020.168
Karadaş, Ö., Öztürk, B., and Sonkaya, A. R. (2020). A prospective clinical study of detailed neurological manifestations in patients with COVID-19. Neurol. Sci. 41, 1991–1995. doi: 10.1007/s10072-020-04547-7
Karimi-Galougahi, M., Naeini, A. S., Raad, N., Mikaniki, N., and Ghorbani, J. (2020). Vertigo and hearing loss during the COVID-19 pandemic - is there an association? Acta Otorhinolaryngol. Ital. 40, 463–465. doi: 10.14639/0392-100X-N0820
KCDA. (2020). Findings From Investigation and Analysis of Re-Positive Cases. Available online at: https://www.cdc.go.kr/board/board.es?mid=a30402000000andbid=0030. (accessed September 7, 2020).
Kilic, O., Kalcioglu, M. T., Cag, Y., et al. (2020). Could sudden sensorineural hearing loss be the sole manifestation of COVID-19? An investigation into SARS-COV-2 in the etiology of sudden sensorineural hearing loss. Int. J. Infect. Dis. 97, 208–211 doi: 10.1016/j.ijid.2020.06.023
Klironomos, S., Tzortzakakis, A., Kits, A., Öhberg, C., Kollia, E., Ahoromazdae, A., et al. (2020). Nervous system involvement in coronavirus disease 2019: results from a retrospective consecutive neuroimaging cohort. Radiology 297, E324–E334. doi: 10.1148/radiol.2020202791
Lamounier, P., Franco Gonçalves, V., Ramos, H. V. L., Gobbo, D. A., Teixeira, R. P., Dos Reis, P. C., et al. (2020). A 67-year-old woman with sudden hearing loss associated with SARS-CoV-2 infection. Am. J. Case Rep. 21:e927519. doi: 10.12659/AJCR.927519
Lan, L., Xu, D., Ye, G., Xia, C., Wang, S., Li, Y., et al. (2020). Positive RT-PCR test results in patients recovered from COVID-19. JAMA 323, 1502–1503. doi: 10.1001/jama.2020.2783
Landi, F., Gremese, E., Rota, E., Carfi, A., Benvenuto, F., Ciciarello, F., et al. (2020). Positive RT-PCR nasopharyngeal swab in patients recovered from COVID-19 disease: when does quarantine really end? J. Infect. 81, e1–e3. doi: 10.1016/j.jinf.2020.08.034
Leonardi, M., Padovani, A., and McArthur, J. C. (2020). Neurological manifestations associated with COVID-19: a review and a call for action. J. Neurol. 267, 1573–1576. doi: 10.1007/s00415-020-09896-z
Li, C., Luo, F., Xie, L., Gao, Y., Zhang, N., and Wu, B. (2020). Chest CT study of fifteen COVID-19 patients with positive RT-PCR retest results after discharge. Quant. Imaging Med. Surg. 10, 1318–1324. doi: 10.21037/qims-20-530
Li, J., Long, X., Fang, X., Zhang, Q., Hu, S., Lin, Z., et al. (2020). SARS-CoV-2 positivity in a discharged COVID-19 patient: a case report. Clin. Microbiol. Infect. 26, 1115–1117. doi: 10.1016/j.cmi.2020.04.032
Li, M. Y., Li, L., Zhang, Y., and Wang, X. S. (2020). Expression of the SARSCoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty 9:45. doi: 10.1186/s40249-020-00662-x
Li, Y., Hu, Y., Yu, Y., Zhang, X., Li, B., Wu, J., et al. (2020). Positive result of Sars-Cov-2 in faeces and sputum from discharged patients with COVID-19 in Yiwu, China. J. Med. Virol. 92, 1938–1947. doi: 10.1002/jmv.25905
Li, Y. C., Bai, W. Z., and Hashikawa, T. (2020). The neuroinvasive potential of SARSCoV2 may be at least partially responsible for the respiratory failure of COVID-19 patients. J. Med. Virol. 92, 552–555. doi: 10.1002/jmv.25824
Ling, Y., Xu, S. B., Lin, Y. X., Tian, D., Zhu, Z. Q., Dai, F. H., et al. (2020). Persistence and clearance of viral RNA in 2019 novel coronavirus disease rehabilitation patients. Chin. Med. J. (Engl.). 133, 1039–1043. doi: 10.1097/CM9.0000000000000774
Liotti, F. M., Menchinelli, G., Marchetti, S., Morandotti, G. A., Sanguinetti, M., Posteraro, B., et al. (2021). Evaluation of three commercial assays for SARS-CoV-2 molecular detection in upper respiratory tract samples. Eur. J. Clin. Microbiol. Infect. Dis. 40, 269–277. doi: 10.1007/s10096-020-04025-0
Liu, B., Shi, Y., Zhang, W., Li, R., He, Z., Yang, X., et al. (2020). Recovered COVID-19 patients with recurrent viral RNA exhibit lower levels of anti-RBD antibodies. Cell. Mol. Immunol. 17, 1098–1100. doi: 10.1038/s41423-020-00528-0
Liu, C., Ye, L., Xia, R., Zheng, X., Yuan, C., Wang, Z., et al. (2020a). Chest CT and clinical follow-up of discharged patients with COVID-19 in Wenzhou City, Zhejiang, China. Ann. Am. Thorac. Soc. 17, 1231–1237. doi: 10.1513/AnnalsATS.202004-324OC
Liu, C., Zhou, J., Xia, L., Cheng, X., and Lu, D. (2020b). 18F-FDG PET/CT and serial chest CT findings in a COVID-19 patient with dynamic clinical characteristics in different period. Clin. Nucl. Med. 45, 495–496. doi: 10.1097/RLU.0000000000003068
Liu, F., Cai, Z. B., Huang, J. S., Yu, W. Y., Niu, H. Y., Zhang, Y., et al. (2020). Positive SARS-CoV-2 RNA recurs repeatedly in a case recovered from COVID-19: dynamic results from 108 days of follow-up. Pathog Dis. 78:ftaa031. doi: 10.1093/femspd/ftaa031
Liu, J., Lian, R., Zhang, G., Hou, B., Wang, C., Dong, J., et al. (2020). Changes in serum virus-specific IgM/IgG antibody in asymptomatic and discharged patients with reoccurring positive COVID-19 nucleic acid test (RPNAT). Ann. Med. 53, 34–42. doi: 10.1080/07853890.2020.1811887
Liu, T., Wu, S., Zeng, G., Zhou, F., Li, Y., Guo, F., et al. (2020). Recurrent positive SARS-CoV-2: immune certificate may not be valid. J. Med. Virol. 29:10.1002/jmv.26074. doi: 10.1002/jmv.26074
Loconsole, D., Passerini, F., Palmieri, V. O., Centrone, F., Sallustio, A., Pugliese, S., et al. (2020). Recurrence of COVID-19 after recovery: a case report from Italy. Infection 16, 1–3. doi: 10.1007/s15010-020-01444-1
Lon, I. L., Lio, C. F., Cheong, H. H., Lei, C. I., Cheong, T. H., Zhong, X., et al. (2020). Evolution of SARS-CoV-2 RNA shedding in clinical specimens and clinical characteristics of 10 patients with COVID-19 in Macau. Int. J. Biol. Sci. 16, 1698–1707. doi: 10.7150/ijbs.45357
Lu, J., Peng, J., Xiong, Q., Liu, Z., Lin, H., Tan, X., et al. (2020). Clinical, immunological and virological characterization of COVID-19 patients that test re-positive for SARS-CoV-2 by RT-PCR. EBio Med. 59:102960. doi: 10.1016/j.ebiom.2020.102960
Luciani, M., Bentivegna, E., Spuntarelli, V., Lamberti, P. A., Cacioli, G., Del Porto, F., et al. (2020). Recurrent COVID-19 pneumonia in the course of chemotherapy: consequence of a weakened immune system? J. Med. Virol. 28:10.1002/jmv.26701. doi: 10.1002/jmv.26701
Lukiw, W. J., Pogue, A., and Hill, J. M. (2020). SARS-CoV-2 infectivity and neurological targets in the brain. Cell Mol. Neurobiol. 2020, 1–8. doi: 10.1007/s10571-020-00947-7
Lumley, S. F., O'Donnell, D., Stoesser, N. E., Matthews, P. C., Howarth, A., Hatch, S. B., et al. (2020). Antibody status and incidence of SARS-CoV-2 infection in health care workers. N. Engl. J. Med. 384, 533–540. doi: 10.1056/NEJMoa2034545
Magnavita, N., Tripepi, G., and Di Prinzio, R. R. (2020). Symptoms in health care workers during the COVID-19 epidemic. a cross-sectional survey. Int. J. Environ. Res. Public Health. 17:5218. doi: 10.3390/ijerph17145218
Maharaj, S., Bello Alvarez, M., Mungul, S., and Hari, K. (2020). Otologic dysfunction in patients with COVID-19: a systematic review. Laryngos. Investig. Otolaryngol. 5, 1192–1196. doi: 10.1002/lio2.498
Maharaj, S., and Hari, K. (2020). Congenital inner ear abnormalities and COVID-19-related ear infections. Ear Nose Throat J. 23:145561320968934. doi: 10.1177/0145561320968934
Malayala, S. V., and Raza, A. (2020). A case of COVID-19-induced vestibular neuritis. Cureus 12:e8918. doi: 10.7759/cureus.8918
Mao, L., Wang, M., Chen, S., He, Q., Chang, J., Hong, C., et al. (2020). Neurological manifestations of hospitalized patients with COVID-19 in Wuhan, China: a retrospective case series study. medRxiv 2020.02.22.20026500. doi: 10.1101/2020.02.22.20026500
Mardani, M., Nadji, S. A., Sarhangipor, K. A., Sharifi-Razavi, A., and Baziboroun, M. (2020). COVID-19 infection recurrence presenting with meningoencephalitis. New Microbes New Infect. 37:100732. doi: 10.1016/j.nmni.2020.100732
Matsumura, Y., Shimizu, T., Noguchi, T., Nakano, S., Yamamoto, M., and Nagao, M. (2020). Comparison of 12 molecular detection assays for SARS-CoV-2. bioRxiv 2020: 06.24.170332. doi: 10.1101/2020.06.24.170332
Mei, Q., Li, J., Du, R., Yuan, X., Li, M., and Li, J. (2020). Assessment of patients who tested positive for COVID-19 after recovery. Lancet Infect. Dis. 20, P1004–P1005. doi: 10.1016/S1473-3099(20)30433-3
Mi, B., Chen, L., Xiong, Y., Xue, H., Zhou, W., Liu, G., et al. (2020). Characteristics and early prognosis of COVID-19 infection in fracture patients. J. Bone Joint Surg. 102, 750–758. doi: 10.2106/JBJS.20.00390
Nepal, G., Rehrig, J. H., Shrestha, G. S., Shing, Y. K., Yadav, J. K., Ojha, R., et al. (2020). Neurological manifestations of COVID-19: a systematic review. Crit. Care. 24:421. doi: 10.1186/s13054-020-03121-z
Özçelik Korkmaz, M., Egilmez, O. K., Özçelik, M. A., and Güven, M. (2020). Otolaryngological manifestations of hospitalised patients with confirmed COVID-19 infection. Eur. Arch. Otorhinolaryngol. 3, 1–11. doi: 10.1007/s00405-020-06396-8
Paniz-Mondolfi, C., Bryce, Z., Grimes, R. E., Gordon, J., Reidy, J., Lednicky, E., et al. (2020). Central nervous system involvement by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). J. Med. Virol. 92, 699–702. doi: 10.1002/jmv.25915
Panupattanapong, S., and Brooks, E. B. (2020). New spectrum of COVID-19 manifestations in children: Kawasaki-like syndrome and hyperinflammatory response. Cleve Clin. J. Med. 1–7 doi: 10.3949/ccjm.87a.ccc039
Peng, J., Wang, M., Zhang, G., and Lu, E. (2020). Seven discharged patients turning positive again for SARS-CoV-2 on quantitative RT-PCR. Am. J. Infect. Control. 48, 725–726. doi: 10.1016/j.ajic.2020.03.017
Qiao, X.-M., Xu, X.-F., Zi, H., Liu, G.-X., Li, B.-H., Du, X., et al. (2020). Re- positive cases of nucleic acid tests in discharged patients with COVID-19: a follow-up study. Front. Med. 7:349. doi: 10.3389/fmed.2020.00349
Qin, C., Zhou, L., Hu, Z., Zhang, S., Yang, S., Tao, Y., et al. (2020). Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 71, 762–768. doi: 10.1093/cid/ciaa248
Ravioli, S., Ochsner, H., and Lindner, G. (2020). Reactivation of COVID-19 pneumonia: a report of two cases. J. Inf. Secur. 81, e72–e73. doi: 10.1016/j.jinf.2020.05.008
Romero-Sánchez, C. M., Díaz-Maroto, I., Fernández-Díaz, E., Sánchez-Larsen, Á., Layos-Romero, A., García-García, J., et al. (2020). Neurologic manifestations in hospitalized patients with COVID-19: the ALBACOVID registry. Neurology 95, e1060–e1070. doi: 10.1212/WNL.0000000000009937
Salcin, S., and Fontem, F. (2020). Recurrent Sars-Cov-2 infection resulting in acute respiratory distress syndrome and development of pulmonary hypertension: a case report. Respir. Med. Case Rep. 5:101314. doi: 10.1016/j.rmcr.2020.101314
Sen, M. K., Gupta, N., Yadav, S. R., Kumar, R., Singh, B., and Ish, P. (2020). Contentious issue in recurrent COVID-19 infection: reactivation or reinfection. Turk Thorac. J. 21, 463–466. doi: 10.5152/TurkThoracJ.2020.20164
Shahriarirad, R., Khodamoradi, Z., Erfani, A., Hosseinpour, H., Ranjbar, K., Emami, Y., et al. (2020). Epidemiological and clinical features of 2019 novel coronavirus diseases (COVID-19) in the South of Iran. BMC Infect. Dis. 20:427. doi: 10.1186/s12879-020-05128-x
Sharma, R., Sardar, S., Mohammad Arshad, A., Ata, F., Zara, S., and Munir, W. (2020). A patient with asymptomatic SARS-CoV-2 infection who presented 86 days later with COVID-19 pneumonia possibly due to reinfection with SARS-CoV-2. Am. J. Case Rep. 21:e927154. doi: 10.12659/AJCR.927154
Sia, J. (2020). Dizziness can be an early sole clinical manifestation for COVID-19 infection: a case report. J. Am. Coll. Emerg. Physicians Open. 23:10.1002/emp2.12185. doi: 10.1002/emp2.12185
Sriwijitalai, W., and Wiwanitkit, V. (2020). Hearing loss and COVID-19: a note. Am. J. Otolaryngol. 41:102473. doi: 10.1016/j.amjoto.2020.102473
Sun, R., Liu, H., and Wang, X. (2020). Mediastinal emphysema, giant bulla, and pneumothorax developed during the course of COVID-19 pneumonia. Korean J. Radiol. 21, 541–544. doi: 10.3348/kjr.2020.0180
Tian, M., Long, Y., Hong, Y., Zhang, X., and Zha, Y. (2020). The treatment and follow-up of 'recurrence' with discharged COVID-19 patients: data from Guizhou, China. Environ. Microbiol. 22, 3588–3592. doi: 10.1111/1462-2920.15156
To, K. K.-W., Hung, I. F.-N., Ip, J. D., Chu, A. W.-H., Chan, W.-M., Tam, A. R., et al. (2020). COVID-19 re-infection by a phylogenetically distinct SARS-coronavirus-2 strain confirmed by whole genome sequencing. Clin. Infect. Dis. 2020:ciaa1275. doi: 10.1093/cid/ciaa1275
Vavougios, G. D. (2020). SARS-CoV-2 dysregulation of PTBP1 and YWHAE/Z gene expression: a primer of neurodegeneration. Med. Hypotheses. 144:110212. doi: 10.1016/j.mehy.2020.110212
Viola, P., Ralli, M., Pisani, D., Malanga, D., Sculco, D., Messina, L., et al. (2020). Tinnitus and equilibrium disorders in COVID-19 patients: preliminary results. Eur. Arch. Otorhinolaryngol. 23, 1–6. doi: 10.1007/s00405-020-06440-7
Wang, D., Hu, B., Hu, C., Zhu, F., Liu, X., Zhang, J., et al. (2020). Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus – infected pneumonia in Wuhan – China. J. Am. Med. Assoc. 323, 1061–1069. doi: 10.1001/jama.2020.1585
Wang, H., Li, Y., Wang, F., Du, H., and Lu, X. (2020). Rehospitalization of a recovered coronavirus disease 19 (COVID-19) child with positive nucleic acid detection. Pediatr. Infect. Dis. J. 39:e69. doi: 10.1097/INF.0000000000002690
Wang, M., Chen, D., Wu, W., Tang, H., Kan, L., Zong, Z., et al. (2021). Analytical performance evaluation of five RT-PCR kits for severe acute respiratory syndrome coronavirus 2. J. Clin. Lab. Anal. 2021:e23643. doi: 10.1002/jcla.23643
Wang, X., Xu, H., Jiang, H., Wang, L., Lu, C., Wei, X., et al. (2020). Clinical features and outcomes of discharged coronavirus disease 2019 patients: a prospective cohort study. QJM. 113, 657–665. doi: 10.1093/qjmed/hcaa178
Whittaker, A., Anson, M., and Harky, A. (2020). Neurological manifestations of COVID-19: a systematic review and current update. Acta Neurol. Scand. 142, 14–22. doi: 10.1111/ane.13266
Wong, J., Koh, W. C., Momin, R. N., Alikhan, M. F., Fadillah, N., and Naing, L. (2020). Probable causes and risk factors for positive SARS-CoV-2 test in recovered patients: evidence from Brunei Darussalam. J. Med. Virol. 92, 2847–2851. doi: 10.1002/jmv.26199
Wu, F., Zhang, W., Zhang, L., Wang, D., and Wan, Y. (2020). Discontinuation of antiviral drugs may be the reason for recovered COVID-19 patients testing positive again. Br. J. Hosp. Med. 81, 1–2. doi: 10.12968/hmed.2020.0156
Wu, J., Liu, X., Liu, J., Liao, H., Long, S., Zhou, N., et al. (2020). Coronavirus disease 2019 test results after clinical recovery and hospital discharge among patients in China. JAMA Netw. Open. 3:e209759. doi: 10.1001/jamanetworkopen.2020.9759
Wu, Y., Xu, X., Chen, Z., Duan, J., Hashimoto, K., Yang, L., et al. (2020). Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 87, 18–22. doi: 10.1016/j.bbi.2020.03.031
Xiao, A. T., Tong, Y. X., and Zhang, S. (2020). False negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: rather than recurrence. J. Med. Virol. 9:10.1002/jmv.25855. doi: 10.1002/jmv.25855
Xiao, Y., Shi, X., She, Q., Chen, Q., Pan, H., Zhang, J., et al. (2020). Exploration of turn-positive RT-PCR results and factors related to treatment outcome in COVID-19: a retrospective cohort study. Virulence 11, 1250–1256. doi: 10.1080/21505594.2020.1816076
Xie, C., Lu, J., Wu, D., Zhang, L., Zhao, H., Rao, B., et al. (2020). False negative rate of COVID-19 is eliminated by using nasal swab test. Travel Med. Infect. Dis. 37:101668. doi: 10.1016/j.tmaid.2020.101668
Xing, Y., Mo, P., Xiao, Y., Zhao, O., Zhang, Y., and Wang, F. (2020). Post-discharge surveillance and positive virus detection in two medical staff recovered from coronavirus disease 2019 (COVID-19), China, January to February 2020. Euro Surveill. 25:2000191. doi: 10.2807/1560-7917.ES.2020.25.10.2000191
Xiong, W., Mu, J., Guo, J., Lu, L., Liu, D., Luo, J., et al. (2020). New onset neurologic events in people with COVID-19 in 3 regions in China. Neurology 95, e1479–e1487. doi: 10.1212/WNL.0000000000010034
Yachou, Y., El Idrissi, A., Belapasov, V., and Ait Benali, S. (2020). Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2, understanding the neurological manifestations in COVID-19 patients. Neurol. Sci. 41, 2657–2669. doi: 10.1007/s10072-020-04575-3
Yahav, D., Yelin, D., Eckerle, I., et al. (2021). Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 27, 315–318. doi: 10.1016/j.cmi.2020.11.028
Yang, C., Jiang, M., Wang, X., Tang, X., Fang, S., Li, H., et al. (2020). Viral RNA level, serum antibody responses, and transmission risk in recovered COVID-19 patients with recurrent positive SARS-CoV-2 RNA test results: a population-based observational cohort study. Emerg. Microbes Infect. 9, 2368–2378. doi: 10.1080/22221751.2020.1837018
Ye, G., Pan, Z., Pan, Y., Deng, Q., Chen, L., Li, J., et al. (2020). Clinical characteristics of severe acute respiratory syndrome coronavirus 2 reactivation. J. Infect. 80, e14–e17. doi: 10.1016/j.jinf.2020.03.001
Yoo, S. Y., Lee, Y., Lee, G. H., and Kim, D. H. (2020). Reactivation of SARSCoV-2 after recovery. Pediatr. Int. 62, 879–881. doi: 10.1111/ped.14312
Yuan, B., Liu, H. Q., Yang, Z. R., Chen, Y. X., Liu, Z. Y., Zhang, K., et al. (2020). Recurrence of positive SARS-CoV-2 viral RNA in recovered COVID-19 patients during medical isolation observation. Sci. Rep. 10:11887. doi: 10.1038/s41598-020-68782-w
Yuan, J., Kou, S., Liang, Y., Zeng, J., Pan, Y., and Liu, L. (2020). PCR assays turned positive in 25 discharged COVID-19 patients. Clin. Infect. Dis. 8:ciaa398. doi: 10.1093/cid/ciaa398
Zhang, B., Liu, S., Dong, Y., Zhang, L., Zhong, Q., Zou, Y., et al. (2020). Positive rectal swabs in young patients recovered from coronavirus disease 2019 (COVID-19). J. Infect. 81:e49–e52. doi: 10.1016/j.jinf.2020.04.023
Zhang, J.-F., Yan, K., Ye, H.-H., Lin, J., Zheng, J.-J., and Cai, T. (2020). SARS-CoV-2 turned positive in a discharged patient with COVID-19 arouses concern regarding the present standards for discharge. Int. J. Infect. Dis. 97, 212–214. doi: 10.1016/j.ijid.2020.03.007
Zhang, M., Zhou, L., Wang, J., Wang, K., Wang, Y., Pan, X., et al. (2020). The nervous system-A new territory being explored of SARS-CoV-2. J. Clin. Neurosci. 82(Pt A):87–92. doi: 10.1016/j.jocn.2020.10.056
Zhang, R. Z., Deng, W., He, J., Song, Y. Y., Qian, C. F., Yu, Q., et al. (2020). Case Report: recurrence of positive SARS-CoV-2 results in patients recovered from COVID-19. Front. Med. 7:585485. doi: 10.3389/fmed.2020.585485
Zhao, W., Wang, Y., Tang, Y., Zhao, W., Fan, Y., Liu, G., et al. (2020). Characteristics of children with reactivation of SARS-CoV-2 infection after hospital discharge. Clin. Pediatr. (Phila). 59, 929–932. doi: 10.1177/0009922820928057
Zheng, K. I., Wang, X. B., Jin, X. H., Liu, W. Y., Gao, F., Chen, Y. P., et al. (2020). A case series of recurrent viral RNA positivity in recovered COVID-19 Chinese patients. J. Gen. Intern. Med. 35, 2205–2206. doi: 10.1007/s11606-020-05822-1
Zhong, Z. F., Huang, J., Yang, X., Peng, J. L., Zhang, X. Y., Hu, Y., et al. (2020). Epidemiological and clinical characteristics of COVID-19 patients in Hengyang, Hunan Province, China. World J. Clin. Cases 8, 2554–2565. doi: 10.12998/wjcc.v8.i12.2554
Zhou, H., Fu, L., Jin, Y., Shao, J., Zhang, S., Zheng, N., et al. (2020). Clinical features of COVID-19 convalescent patients with re-positive nucleic acid detection. J. Clin. Lab. Anal. 34:e23392. doi: 10.1002/jcla.23392
Zhou, L., Xu, Z., Castiglione, G. M., Soiberman, U. S., Eberhart, C. G., and Duh, E. J. (2020). ACE2 and TMPRSS2 are expressed on the human ocular surface, suggesting susceptibility to SARS-CoV-2 infection. Ocul. Surf. 18, 537–544. doi: 10.1016/j.jtos.2020.06.007
Zhou, X., Zhou, J., and Zhao, J. (2020). Recurrent pneumonia in a patient with new coronavirus infection after discharge from hospital for insufficient antibody production: a case report. BMC Infect. Dis. 20:500. doi: 10.1186/s12879-020-05231-z
Zhou, Y., Fu, B., Zheng, X., et al. (2020). Pathogenic T cells and inflammatory monocytes incite inflammatory storm in severe COVID-19 patients. Natl. Sci. Rev. 13:nwaa041. doi: 10.1093/nsr/nwaa041
Keywords: recurrence, occupational medicine, neuroCOVID, neurologic symptoms, vestibular syndrome, healthcare workers, case report
Citation: Zaffina S, Lanteri P, Gilardi F, Garbarino S, Santoro A, Vinci MR, Carsetti R, Scorpecci A, Raponi M, Magnavita N and Camisa V (2021) Recurrence, Reactivation, or Inflammatory Rebound of SARS-CoV-2 Infection With Acute Vestibular Symptoms: A Case Report and Revision of Literature. Front. Hum. Neurosci. 15:666468. doi: 10.3389/fnhum.2021.666468
Received: 10 February 2021; Accepted: 15 July 2021;
Published: 11 August 2021.
Edited by:
Björn H. Schott, Leibniz Institute for Neurobiology (LG), GermanyReviewed by:
Naoto Kuroda, Wayne State University, United StatesCopyright © 2021 Zaffina, Lanteri, Gilardi, Garbarino, Santoro, Vinci, Carsetti, Scorpecci, Raponi, Magnavita and Camisa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paola Lanteri, cGFvbGEubGFudGVyaUBpc3RpdHV0by1iZXN0YS5pdA==
†These authors share first authorship
‡These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.