 Mandy Roheger
Mandy Roheger Hannah Liebermann-Jordanidis
Hannah Liebermann-Jordanidis Fabian Krohm2
Fabian Krohm2 Anne Adams
Anne Adams Elke Kalbe
Elke Kalbe
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Hum. Neurosci. , 27 April 2021
Sec. Cognitive Neuroscience
Volume 15 - 2021 | https://doi.org/10.3389/fnhum.2021.636355
Background: Cognitive Training (CT) may contribute to the maintenance and even enhancement of cognitive functions in healthy older adults. However, the question who benefits most from multi-domain CTs is still highly under-investigated.
Objective: The goal is to investigate prognostic factors and models for changes in cognitive test performance in healthy older adults after a multi-domain CT.
Methods: The data bases MEDLINE, Web of Science Core Collection, CENTRAL, and PsycInfo were searched up to July 2019. Studies investigating prognostic factors and/or models on cognitive outcomes (global cognition, memory, attention, executive functions, language, visuo-spatial abilities) after conducting a multi-domain CT in healthy older adults were included. Risk of Bias was assessed using the QUIPS and the PROBAST tool.
Results: 23 prognostic factor and model studies were included. Results indicate a high heterogeneity regarding the conducted multi-domain CTs, the investigated prognostic factors, the investigated outcomes, and the used statistical approaches. Age and neuropsychological performance at study entry were the most investigated predictors, yet they show inconsistent results.
Conclusion: Data on prognostic factors and models of changes after multi-domain CT are still too rare and inconsistent to draw clear conclusions due to statistical shortcomings and low reporting quality. Approaches for future research are outlined.
Registration: https://www.crd.york.ac.uk/prospero/, ID: CRD42020147531
Healthy aging is associated with various functional and structural changes in neural mechanisms leading to a decrease in cognitive functioning (Reuter-Lorenz and Park, 2014). The most vulnerable domains for age-related changes are memory, executive function, and attention (Hughes et al., 2018). Several randomized controlled trials (RCTs) provide evidence that cognitive performance of healthy older individuals can be maintained or even improved by cognitive trainings (CT) (Martin et al., 2011; Reijnders et al., 2013; e.g., Chiu et al., 2017; Shah et al., 2017). A meta-analysis suggested that CT has even long-lasting and persistent protective effects on cognition in healthy older adults (Valenzuela and Sachdev, 2009); therefore, it is increasingly taken into consideration in the prevention of age-associated neurodegenerative diseases as dementia. CTs are defined as non-pharmacological interventions using tasks focusing on memory, executive function, attention, language, and/or visuo-spatial abilities. There are many formats of CTs differing in features such as modality (paper-pencil vs. digital), setting (individual vs. group), intensity or number of trained domains (single- vs. multi-domain training). Furthermore, single-domain trainings focus on one specific cognitive function, whereas multi-domain interventions target two or more cognitive domains. Due to the stimulation of multiple cognitive processes, multi-domain CT is more closely related to real-life demands than single-domain training (Binder et al., 2015). Complementary, the multi-domain approach is frequently applied in commercially available “brain games,” such as Nintendo's Dr Kawashima's Brain Training, which are widely-used in the older population (Simons et al., 2016). Brain games aim to train cognition in a playful way by using various cognitive tasks.
Effects of multi-domain interventions could be observed in trained tasks in healthy older people; transfer effects in untrained tasks are also under discussion, although the results on this topic are heterogeneous (Walton et al., 2015). Notably, a recent meta-analysis by Basak et al. (2020) including n = 215 training studies found that all modules of multicomponent training yielded significant near and far transfer effects (Basak et al., 2020). Besides effects on neuropsychological measures, training-related changes have been found in EEG (Küper et al., 2017) as well as fMRI studies (Li et al., 2016) indicating plastic processes in neural functioning in the healthy aging brain. Even though the effectiveness of multi-domain CTs in healthy older adults has been described systematically in the past (Basak et al., 2020), overviews summarizing the evidence of factors and/or models predicting those training-related gains are lacking. Single studies have revealed that single variables, also called prognostic factors, as for example age (Legault et al., 2011), cognitive baseline performance (Gallen et al., 2016) or genetic markers (Bellander et al., 2015) impact the individual benefit. A prognostic factor is defined as a single factor from which risks can be calculated for a specific endpoint, whereas a prognostic or predictive model is a formal combination of multiple predictors from which risks of a specific endpoint can be calculated for individuals (Steyerberg et al., 2013). Prognostic factors for change in memory test performance after a single-domain memory training have been recently summarized by Roheger et al. (2020a). The authors emphasized methodological heterogeneity of included studies leading to inconsistent findings in prognostic factors and could show that the results vary not only as a function of the type of statistical calculation used to determine prognostic factors, but also of the type of dependent variables used in the calculations: post-test scores, change scores, relative change scores, and residual change scores. A further review on prognostic models for memory training success showed that lower age combined with higher education seems to predict higher improvements after memory training (Roheger et al., 2020b). Yet, both reviews solely focused on memory training as a specific example of a CT.
To date and to the best of our knowledge, there is no systematic review summarizing the evidence of factors and models predicting training success in multi-domain CT. Due to the interventions' broad and frequent use to prevent cognitive decline in the older population, it is in the interest of public health to elaborate who actually benefits from this treatment option. Prognostic factors such as e.g., sociodemographic, neuropsychological or neural parameters can facilitate the process of individual decision-making with regard to interventions preventing cognitive decline. Knowledge in this field would be highly relevant for decision support to realize personalized medicine. Therefore, the aim of the present study is to review specific prognostic factors and models for changes in global cognition, memory, executive function, attention, language, and visuo-spatial function (O) after multi-domain CT (I) compared to an active or passive control (C) in healthy older adults (P) in a non-clinical setting (S).
The present systematic review was preregistered and the review protocol can be assessed at www.crd.york.ac.uk/PROSPERO/ (ID: CRD42020147531). The reporting follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline for systematic reviews and meta-analysis (Moher et al., 2009): “The PRISMA for Abstracts Checklists,” as well as “The PRISMA checklist for systematic reviews” are displayed in Supplementary Tables 1, 2.
MEDLINE (via Ovid), Web of Science Core Collection, CENTRAL and PsycInfo were systematically searched for relevant studies up to July 2019. Furthermore, reference lists of all identified trials, relevant review articles and current treatment guidelines were hand searched for further literature. In cases where no full text could be obtained, we contacted the authors and asked them to provide full text publications within a 2-week time frame. Further information on the systematic search and the full search strategies are presented in the Supplementary Tables 3–6.
Titles and abstracts were screened according to predefined eligibility criteria by two individual review authors (MR and HLJ) with the Covidence Software (https://www.covidence.org/). Full-text articles of the studies that met the inclusion criteria were further reviewed for inclusion in the systematic review. In cases where no consensus could be reached between the two authors MR and HLJ, the case was discussed until a final consensus was reached.
Eligibility criteria were defined in terms of population, interventions, comparators, outcomes and timing (PICOT). The review focused on peer-reviewed studies in English and German which investigated prognostic factors and models of changes in cognitive test performance after multi-domain CT with no limitations regarding publication date. Full study reports needed to be available; abstracts, books, book chapters, study protocols, and conference papers were excluded.
Studies including data on prognostic factors and models for changes after multi-domain CT performance on healthy older participants (age ≥ 55 years) were included (P). We excluded data from participants with diagnosis of cognitive impairment or dementia, neurological and/or psychiatric diseases, assessed at least via self-report.
Regarding the included prognostic factors and models, all prognostic factors (e.g., sociodemographic factors, brain imaging parameters, genetic parameters, blood factors, personality traits, cognitive abilities at the entry of the training, different training characteristics, e.g., intensity of the trainings, etc.) and all prognostic models which investigate changes in cognitive test performance after multi-domain CT were included in the review and meta-analysis. Multi-domain CT was defined as a CT that includes tasks for training of at least two cognitive domains. The training should consist of at least 90% of cognitive exercises (next to e.g., physical exercises, life-style interventions, diets) with a minimum of two sessions in total. Cognitive domains could either be trained separately and sequentially, or several cognitive domains could be trained simultaneously. Furthermore, the training could either include computerized or paper-pencil tasks with clear cognitive rationale, which were administered either on personal devices or in individual- or group settings (I). No pre-assumptions about comparator interventions were made (C). Regarding videogame trainings and brain trainings, we only included those in which cognitive domains trained were explicitly outlined.
Studies including data on prognostic factors and models, which investigate cognitive changes after training as an outcome (global cognition, memory, attention, executive functions, language, visuo-spatial abilities) measured with established objective neuropsychological tests, were included (O). The factor measurement of the included studies had to be conducted before the training started, and there was no limitation regarding post-measurements of outcomes or the length of the follow-ups (T).
Two review authors (MR and HLJ) independently extracted the data according to the Critical appraisal and data extraction for systematic reviews of prediction modeling studies_ prognostic factors (CHARMS_PF) checklist (Moons et al., 2014) to investigate the reporting of prognostic factors.
Two reviewers (MR and HLJ) independently assessed the risk of bias of included studies. For prognostic factor studies, the Quality in Prognosis Studies (QUIPS) checklist, developed by Hayden and colleagues (2013) was used to examine the risk of bias in prognostic factor studies across six domains (Hayden et al., 2013): Study participation, study attrition, prognostic factor measurement, outcome measurement, adjustment for other prognostic factors, statistical analyses, and reporting. Each of the six domains was judged with high, moderate or low risk. A detailed description of the domains included in the tool and the judgement taken by the two reviewers are presented in Supplementary Table 7.
Prognostic model studies were assessed using the “Prediction model Risk of Bias Assessment Tool (PROBAST)” (Wolff et al., 2019) which examines the risk of bias in prognostic model studies across four domains: Participants, Predictors, Outcome, Analysis. Every domain was voted with “yes,” “probably yes,” “no,” “probably no,” and “no information” to rate their risk of bias. To ensure fairness in the ratings, risk of bias assessment of a study conducted by two of the authors of the present review [MR, EK] was done independently by two researchers [HLJ, FK] who were not involved in the former study (Roheger et al., 2020c).
The extracted data was entered into an electronic database by a review author [MR] and checked by a second review author [HLJ]. All analyses should be conducted with the statistic program R version 3.5.0. Predictors and models of included studies should be examined using meta-analyses (separately for factors and models).
In the preregistration of the present study, it was planned that if clinical and methodological characteristics of the individual studies were sufficiently homogeneous, statistical measures for model performance (e.g., statistics for discrimination and calibration) and model parameters (e.g., regression coefficients) should be pooled meta-analytically across studies and a weighted mean including the corresponding 95% confidence interval should be calculated. Additionally, forest plots were planned to graphically present the results. Multivariable models could only be pooled if the same or at least a very similar set of prognostic factors were used to adapt the model. Random-effects models should be used for meta-analyses.
To evaluate the presence of heterogeneity between studies, heterogeneity statistics I2 und tau2 should be calculated and examined using a chi-squared test (Q-test). Interpretation of the I2 statistic should be made according to chapter 9.5.2 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins, 2008). Relevant heterogeneity should be also examined using meta-regression and subgroup analyses.
However, after data extraction, we found that data on prognostic factors and models of changes after CT were too heterogeneous and too poorly reported to conduct a meta-analysis.
The total number of retrieved references and the numbers of included and excluded studies with reasons for exclusion are documented in a flow chart as recommended in the PRISMA statement (Moher et al., 2009; Figure 1). In total, n = 10,190 studies were identified through the database search. After removing the duplicates, n = 7,559 studies were screened. We assessed n = 446 full-texts for eligibility. Finally, n = 23 studies were included in the present review. All included studies were published in English.
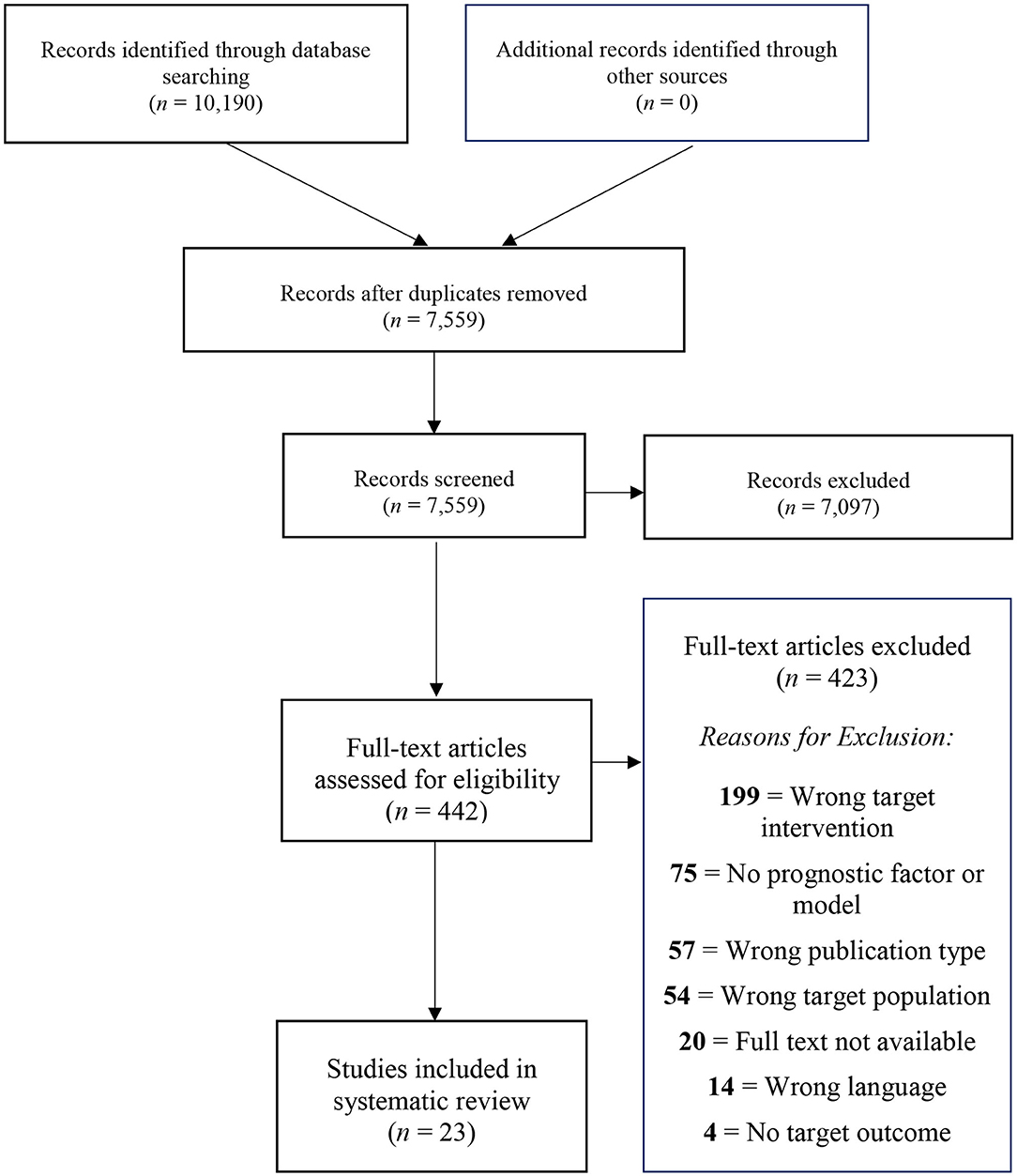
Figure 1. PRISMA diagram showing the study selection process.
An overview of the main characteristics of the included studies [i.e., study type (Prognostic factor vs. prognostic model study), initial sample sizes of the multi-domain CT groups, sample characteristics (age, sex, and education), detailed description of CT] is outlined in Table 1.
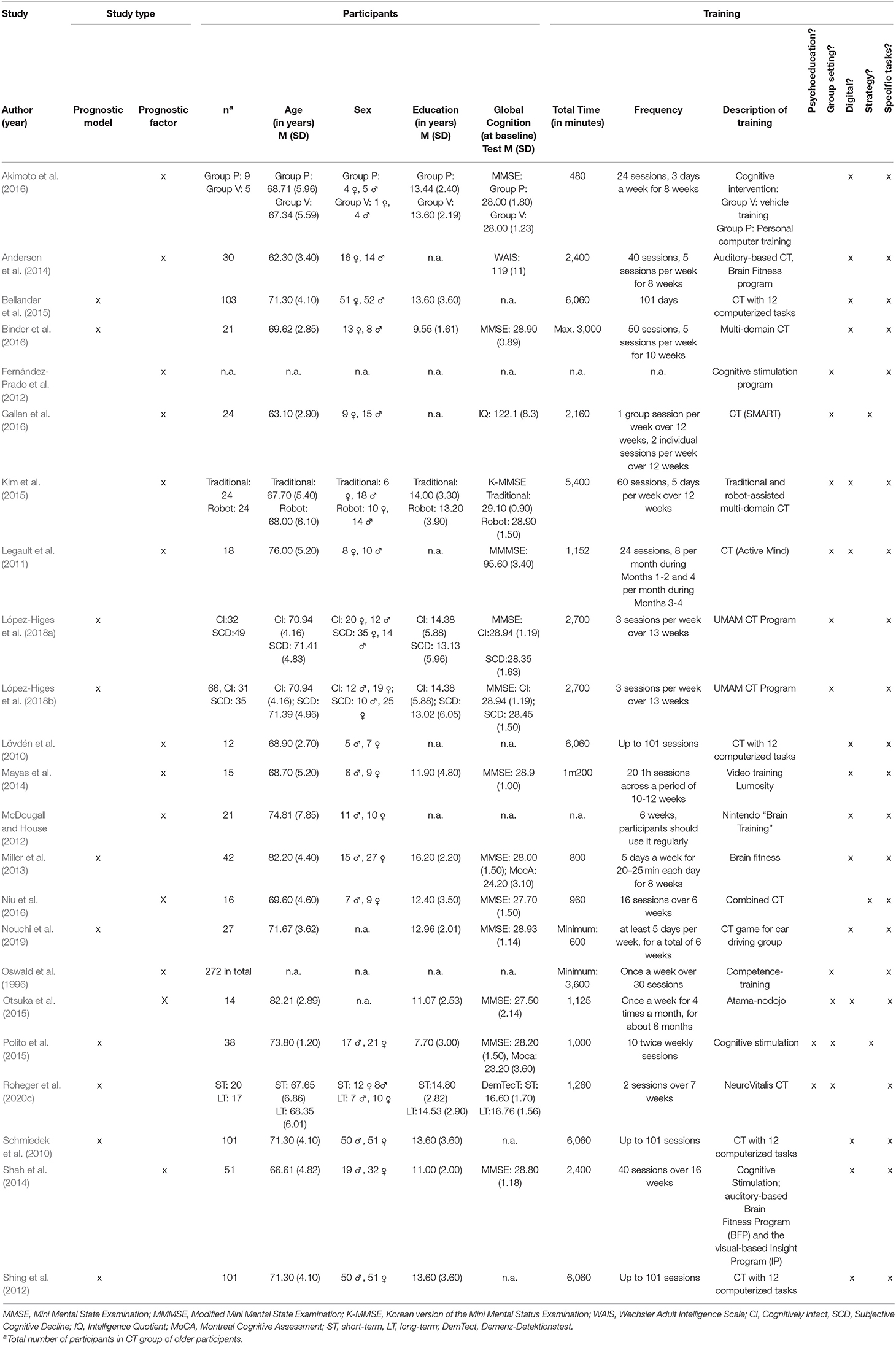
Table 1. Participants' demographics and memory training characteristics.
In total, n = 13 of the included studies investigated prognostic factors, whereas the other n = 10 studies investigated prognostic models to measure changes in cognitive functions after multi-domain CT. The sample sizes of the CT groups varied throughout the prognostic factor studies between n = 5 participants (Akimoto et al., 2016) and n = 272 participants (Oswald et al., 1996, even though no further information on participants is provided in this study report) and between n = 21 participants (Binder et al., 2016) and n = 103 participants (Schmiedek et al., 2010; Shing et al., 2012; Bellander et al., 2015) in the prognostic model studies. Participants were between 62.3 years (Anderson et al., 2014) and 82.21 years old (Otsuka et al., 2015) in the prognostic factor studies, and between 67.65 (Roheger et al., 2020c) and 82.20 years old (Miller et al., 2013) in the prognostic model studies. In both the prognostic factor and prognostic model studies, an almost equal number of male and female participants was investigated (overall: 51% male and 49% female participants; 46% male and 54% female participants, respectively). Three prognostic studies (Oswald et al., 1996; Fernández-Prado et al., 2012; Otsuka et al., 2015) and one prognostic model study (Nouchi et al., 2019) did not report sex distribution among the participants. Years of education varied in the prognostic factor studies between 11.00 (Shah et al., 2014) and 14.00 (Kim et al., 2015), and between 7.70 (Polito et al., 2015) and 14.80 (Roheger et al., 2020c) in the prognostic model studies. N = 7 studies did not report education at all. Global cognitive status was assessed in n = 16 studies with heterogeneous tests. The Mini-Mental Status Examination (MMSE) was assessed in most of them with n = 13.
Characteristics of the multi-domain CTs used in the included studies are depicted in Table 1. It has to be emphasize that it was difficult to determine which specific cognitive domains were trained in the CTs, as often only the used tasks were described without a clear classification to the corresponding domains. Therefore, the review authors classified tasks and tests to their best knowledge. Overall, there was a huge heterogeneity not only in the total time of training in minutes [varying from 480 min (Akimoto et al., 2016) to 6,060 min (Lövdén et al., 2010; Schmiedek et al., 2010; Shing et al., 2012; Bellander et al., 2015)], but also regarding frequency, number of trained domains, and content of the trainings.
CTs were clustered regarding the fact whether they included psychoeducation, were held in individual or group settings, were digital or in paper-pencil-form or whether they included learning of strategies or focused more on specific training tasks. N = 15 studies used a digital CT with tasks training specific functions [prognostic factor studies: n = 9 (Oswald et al., 1996; Lövdén et al., 2010; Legault et al., 2011; McDougall and House, 2012; Anderson et al., 2014; Mayas et al., 2014; Shah et al., 2014; Kim et al., 2015; Akimoto et al., 2016), prognostic model studies: n = 6 (Schmiedek et al., 2010; Shing et al., 2012; Miller et al., 2013; Bellander et al., 2015; Binder et al., 2016; Nouchi et al., 2019)]. A total of n = 10 studies were held in group settings [n = 6 of them prognostic factor studies (Oswald et al., 1996; Legault et al., 2011; Fernández-Prado et al., 2012; Kim et al., 2015; Otsuka et al., 2015; Gallen et al., 2016), n = 4 prognostic model studies (Polito et al., 2015; López-Higes et al., 2018a,b; Roheger et al., 2020c)].
Greyly marked cognitive domains in Table 2 (prognostic factor studies) and Table 3 (prognostic model studies) symbolize the specific domains the participants were trained in the cognitive multi-domain training.
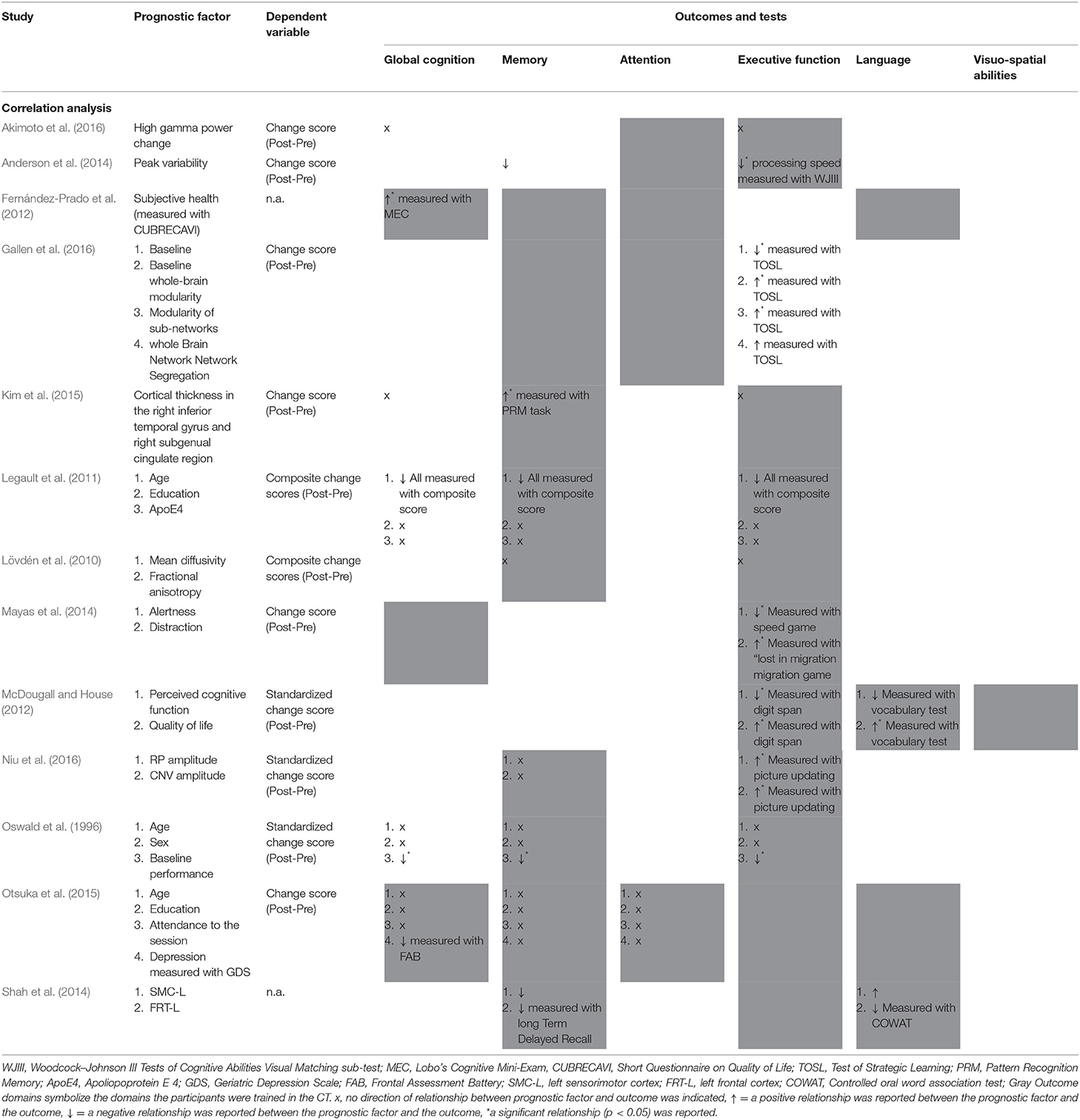
Table 2. Detailed results of prognostic factor studies.
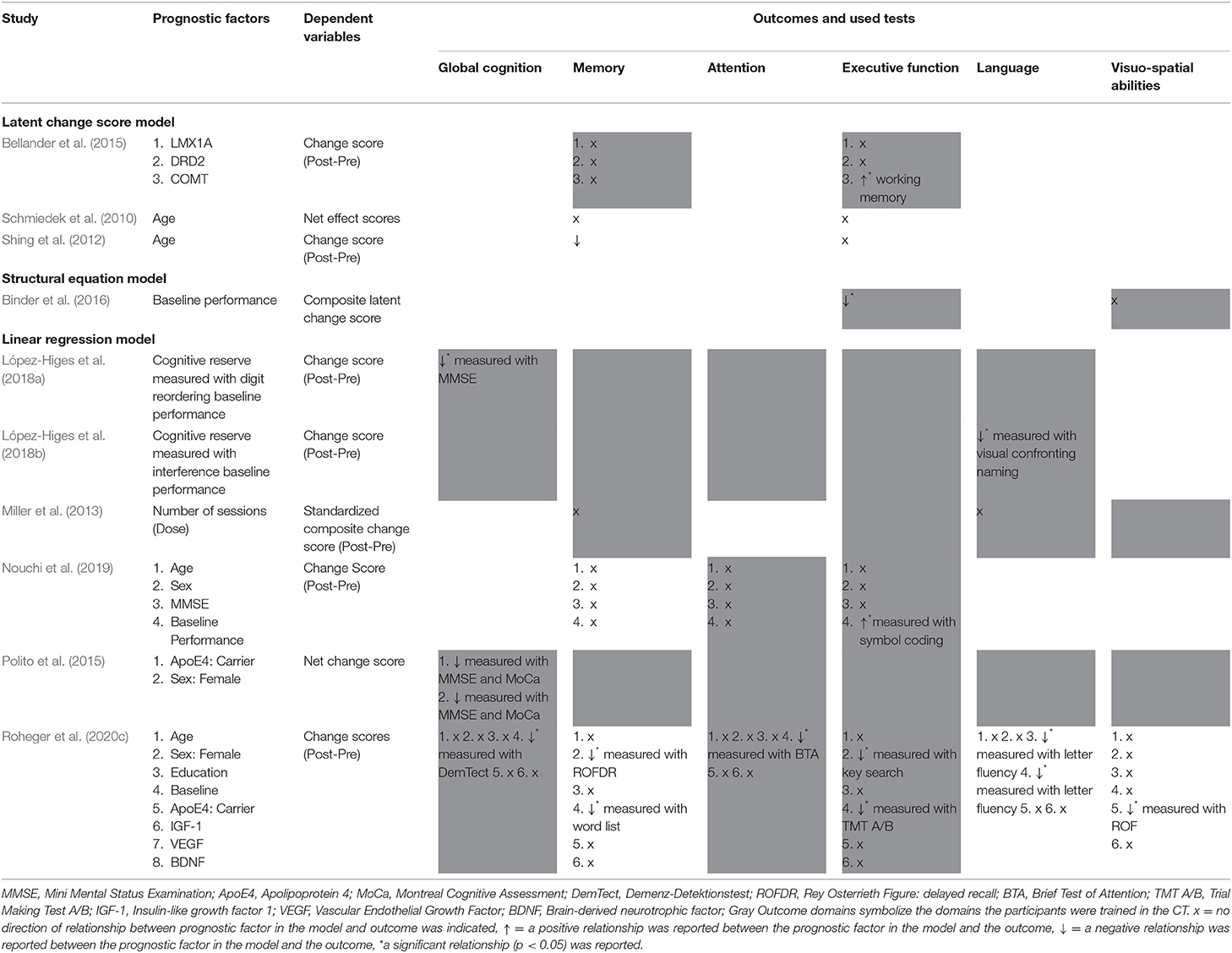
Table 3. Detailed results of prognostic model studies.
In the prognostic factor studies, all except two CTs (Fernández-Prado et al., 2012; Gallen et al., 2016) mainly focused on executive functions. Memory was the second most trained cognitive domain in the prognostic factor studies in nine out of 13 studies (Oswald et al., 1996; Lövdén et al., 2010; Legault et al., 2011; Fernández-Prado et al., 2012; Shah et al., 2014; Kim et al., 2015; Otsuka et al., 2015; Gallen et al., 2016; Niu et al., 2016). N = 5 studies trained attention (Fernández-Prado et al., 2012; Anderson et al., 2014; Otsuka et al., 2015; Akimoto et al., 2016; Gallen et al., 2016), n = 4 language (Fernández-Prado et al., 2012; McDougall and House, 2012; Kim et al., 2015; Otsuka et al., 2015), n = 3 global cognition (Fernández-Prado et al., 2012; Mayas et al., 2014; Otsuka et al., 2015), and n = 2 visuo-spatial abilities (McDougall and House, 2012; Kim et al., 2015). None of the studies offered a CT that trained all cognitive domains.
In the prognostic model studies, all studies trained the domain executive functions. Memory was trained in n = 8 studies (Lövdén et al., 2010; Schmiedek et al., 2010; Shing et al., 2012; Miller et al., 2013; Bellander et al., 2015; Polito et al., 2015; López-Higes et al., 2018b; Roheger et al., 2020c), attention in n = 5 (Polito et al., 2015; López-Higes et al., 2018a,b; Nouchi et al., 2019; Roheger et al., 2020c), language in n = 4 (Miller et al., 2013; Polito et al., 2015; López-Higes et al., 2018a,b), global cognition in n = 3 (Polito et al., 2015; López-Higes et al., 2018a,b), and visuo-spatial abilities in n = 3 (Miller et al., 2013; Polito et al., 2015; Binder et al., 2016). Only one prognostic model study included a CT targeting all cognitive domains (Polito et al., 2015).
Results of the Risk of Bias Assessment are displayed in Tables 4 and 5. Risk of Bias assessment for prognostic factor studies showed a lack of reporting in the domains “Study Attrition” and “Study Confounders” in most of the studies, probably as a result of the fact that often prognostic factor assessment was not the main goal of the included studies, but more an “add-on”. Overall, prognostic model studies showed a medium reporting quality, yet, several studies were lacking information in the domain “statistical analyses” and especially on model validation.
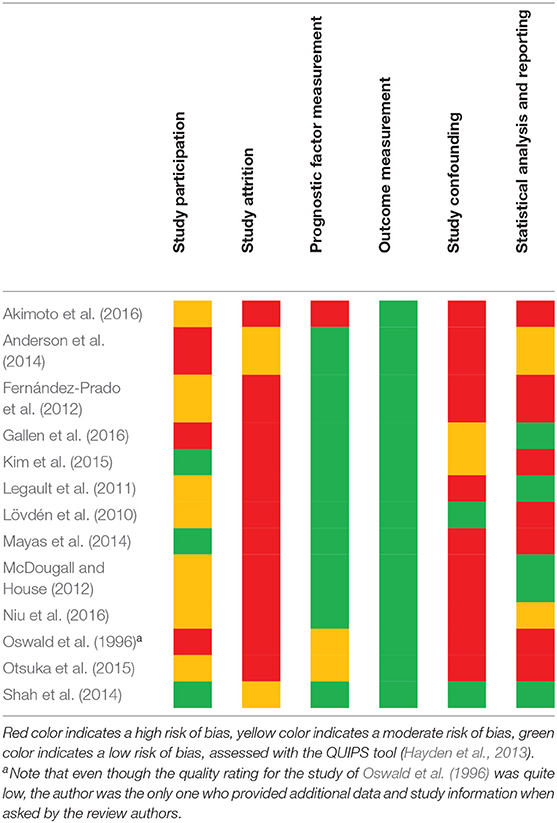
Table 4. Risk of bias assessment for prognostic factor studies.
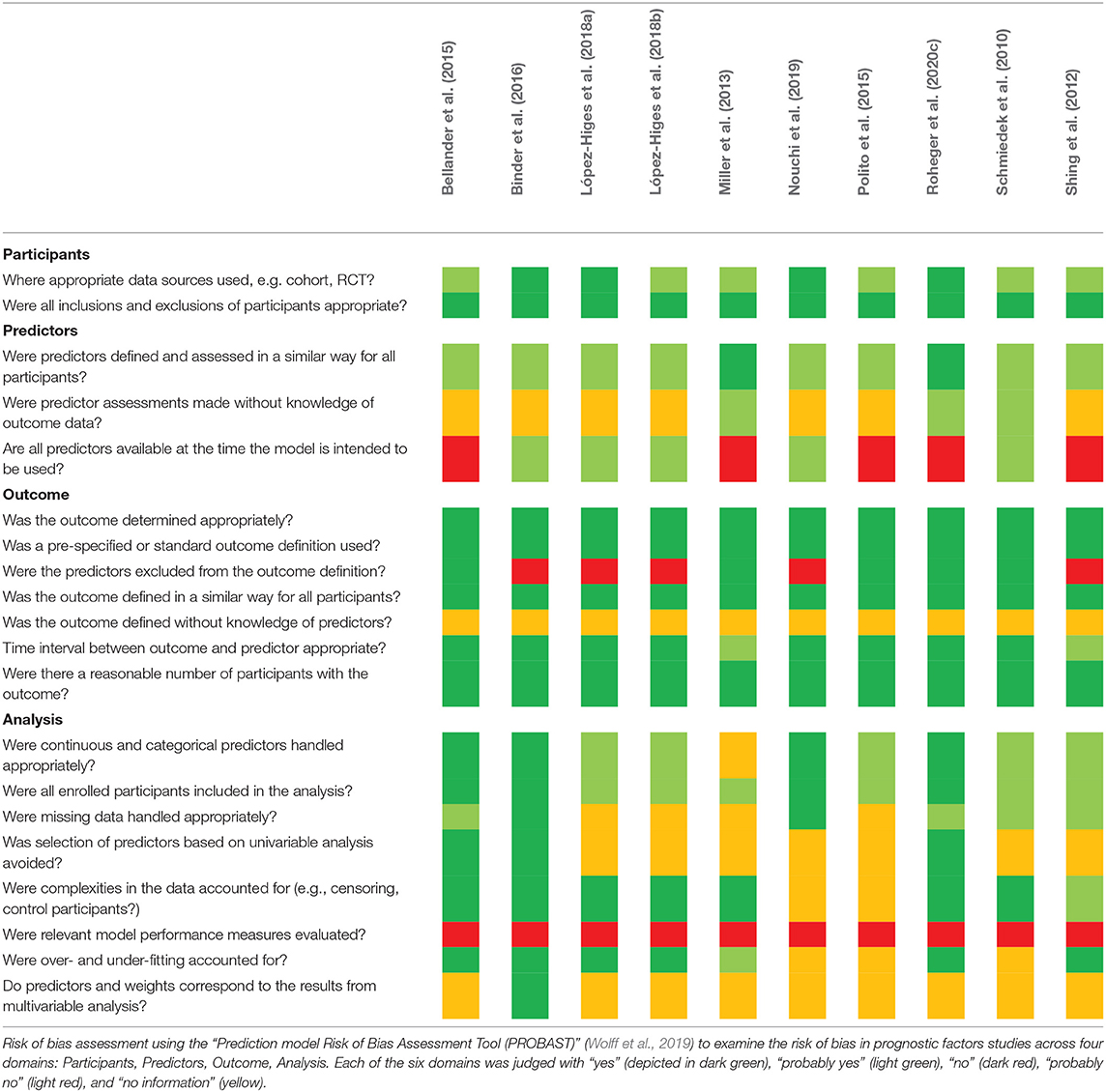
Table 5. Risk of bias assessment for prognostic model studies.
In the present review, we investigated six outcomes: global cognition, memory, attention, executive function, language, visuo-spatial abilities. Outcomes were well-defined in all investigated studies. An overview of the cognitive outcomes investigated in both, prognostic factor and prognostic model studies, can be obtained from Table 6.
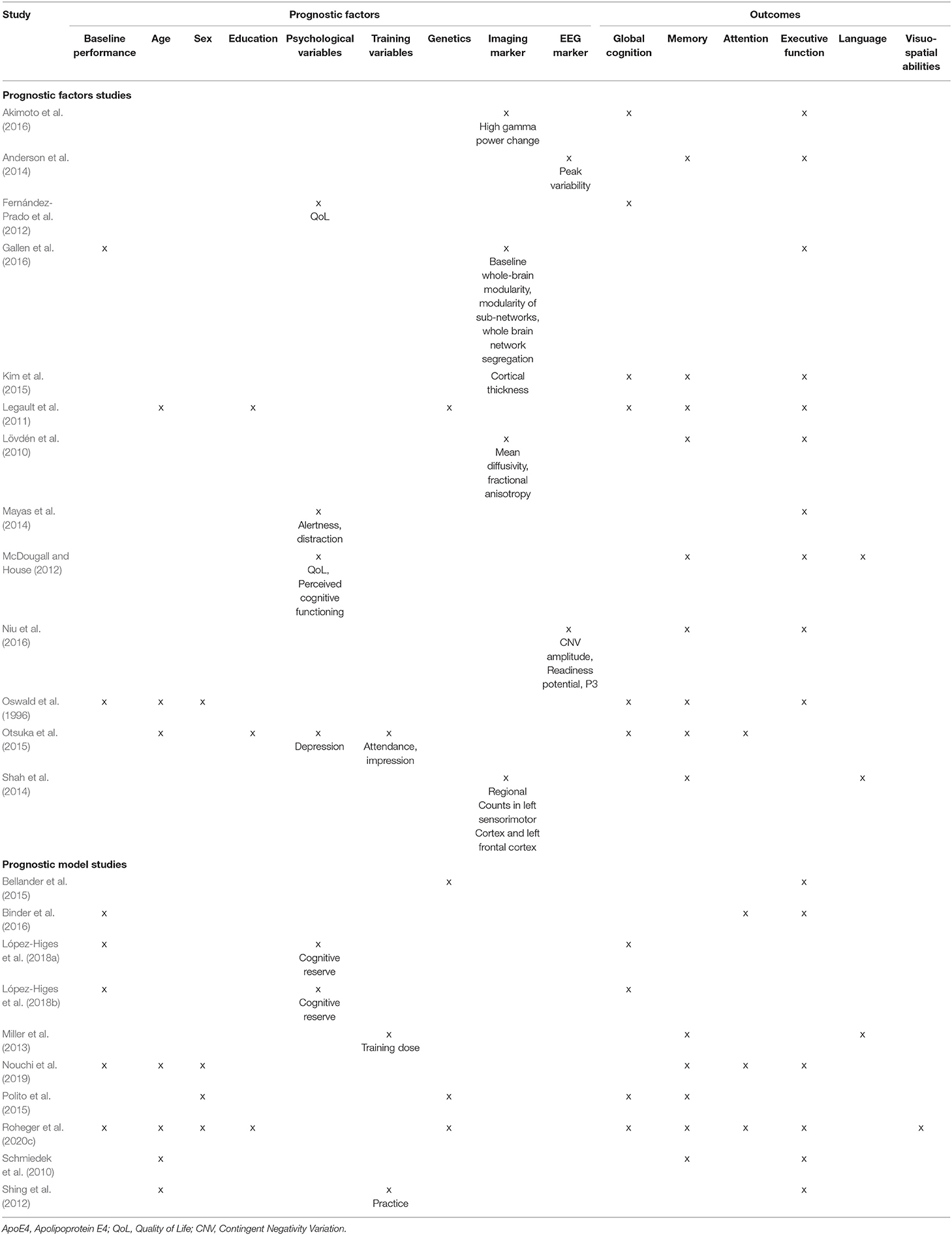
Table 6. Overview of prognostic factors/models and cognitive outcomes of the reviewed studies.
Executive functions was the outcome that was assessed in most studies [n = 10 in prognostic factor studies (Oswald et al., 1996; Lövdén et al., 2010; Legault et al., 2011; McDougall and House, 2012; Anderson et al., 2014; Mayas et al., 2014; Kim et al., 2015; Akimoto et al., 2016; Gallen et al., 2016; Niu et al., 2016), n = 6 in prognostic model studies (Schmiedek et al., 2010; Shing et al., 2012; Bellander et al., 2015; Binder et al., 2016; Nouchi et al., 2019; Roheger et al., 2020c)], followed by memory [n = 9 in prognostic factor studies (Oswald et al., 1996; Lövdén et al., 2010; Legault et al., 2011; McDougall and House, 2012; Anderson et al., 2014; Shah et al., 2014; Kim et al., 2015; Otsuka et al., 2015; Niu et al., 2016), n = 5 in prognostic model studies (Schmiedek et al., 2010; Miller et al., 2013; Polito et al., 2015; Nouchi et al., 2019; Roheger et al., 2020c)]. Global cognition was assessed in n = 6 prognostic factor studies (Oswald et al., 1996; Legault et al., 2011; Fernández-Prado et al., 2012; Kim et al., 2015; Otsuka et al., 2015; Akimoto et al., 2016), but only in two prognostic model studies (Polito et al., 2015; Roheger et al., 2020c), whereas attention was assessed in n = 3 prognostic model studies (Binder et al., 2016; Nouchi et al., 2019; Roheger et al., 2020c), but only in one prognostic factor study (Otsuka et al., 2015). Language and visuo-spatial abilities were the least assessed outcomes in the studies; language was only assessed in two prognostic factor studies (McDougall and House, 2012; Shah et al., 2014) and in one prognostic model study (Miller et al., 2013), visuo-spatial abilities were assessed in none of the prognostic factor studies and only in one of the prognostic model studies as an outcome (Roheger et al., 2020c). None of the studies investigated all cognitive outcome domains.
No detailed description [e.g., a separate paragraph stating not only the name of the predictor and method of measurement, but also blinding, and use in the statistical analysis (e.g. as a continuous or dichotomous factor)] of the candidate predictors was provided in most of the prognostic factor studies, probably as a consequence of the fact that the prediction analysis was mostly not the primary goal of the investigated studies. In prognostic model studies, the descriptions of the statistical analyses were far more detailed.
Investigated predictors include sociodemographic variables (i.e,. age, sex, and education), neuropsychological test status at study entry in different domains, further psychological variables (i.e., quality of life, depression), training characteristics (i.e., modality, intensity), genetic variables (i.e., apolipoprotein E4), brain imaging measures, and EEG markers (for an overview see Table 6, for more details see Table 2 for prognostic factor studies and Table 3 for prognostic model studies).
Prognostic factors in prognostic factor studies were highly heterogeneous. N = 5 studies assessed brain imaging marker (Lövdén et al., 2010; Shah et al., 2014; Kim et al., 2015; Akimoto et al., 2016; Gallen et al., 2016), however, these markers were different over all the studies. Age was assessed in n = 3 prognostic factor studies (Oswald et al., 1996; Legault et al., 2011; Otsuka et al., 2015), cognitive baseline performance (Oswald et al., 1996; Gallen et al., 2016) and education (Legault et al., 2011; Otsuka et al., 2015) were each assessed in n = 2 studies. Sex (Oswald et al., 1996), training variables (Otsuka et al., 2015), and apolipoprotein E4 genotyping (Legault et al., 2011) were each assessed in only one study. Psychological variables were used as predictors in n = 4 studies (Fernández-Prado et al., 2012; McDougall and House, 2012; Mayas et al., 2014; Otsuka et al., 2015), two of them assessing Quality of life (Fernández-Prado et al., 2012; McDougall and House, 2012), one assessing distraction and alertness (Mayas et al., 2014), and one assessing mood (Otsuka et al., 2015). EEG markers were used in two studies as predictors for changes after multi-domain CT (Anderson et al., 2014; Niu et al., 2016).
In all prognostic factor studies, only correlational analyses were conducted. The dependent variables were the raw change score in n = 6 studies (Anderson et al., 2014; Mayas et al., 2014; Kim et al., 2015; Otsuka et al., 2015; Akimoto et al., 2016; Gallen et al., 2016), the standardized change score in n = 3 studies (Oswald et al., 1996; McDougall and House, 2012; Niu et al., 2016), and the composite change score in n = 2 studies (Lövdén et al., 2010; Legault et al., 2011), while n = 2 studies did not clearly report their dependent variable (Fernández-Prado et al., 2012; Shah et al., 2014).
In the prognostic model studies, n = 5 assessed baseline performance of the investigated outcome as a predictor (Binder et al., 2016; López-Higes et al., 2018a,b; Nouchi et al., 2019; Roheger et al., 2020c). N = 4 studies investigated age (Schmiedek et al., 2010; Shing et al., 2012; Nouchi et al., 2019; Roheger et al., 2020c), n = 3 studies investigated sex as possible predictor in the model (Polito et al., 2015; Nouchi et al., 2019; Roheger et al., 2020c). Only one study assessed education (Roheger et al., 2020c), whereas two studies assessed psychological variables (López-Higes et al., 2018a,b), namely cognitive reserve, and two studies integrated training variables (attendance to training, training dose) in their model (Shing et al., 2012; Miller et al., 2013). Apolipoprotein E4, a protein involved in the metabolism of fats in the body and a risk factor for developing Alzheimer's disease, was integrated as prognostic factor in the model in n = 3 studies (Bellander et al., 2015; Polito et al., 2015; Roheger et al., 2020c). Notably, only two studies investigated exact the same model, including baseline performance and cognitive reserve as predictors. Yet, both were conducted by the same research group (López-Higes et al., 2018a,b).
Regarding statistical methods used to calculate prognostic models, our results show that n = 4 studies used multiple regression models (Miller et al., 2013; López-Higes et al., 2018a,b; Roheger et al., 2020c), n = 3 studies used latent change score models (Schmiedek et al., 2010; Shing et al., 2012; Bellander et al., 2015), and one study used structural equation modeling (Binder et al., 2016). All studies used change scores as dependent variable with one exception – a study by Schmiedek et al. (2010) which used net effect scores.
Due to the high heterogeneity of the data and the fact that some data was either missing or not clearly reported, it was difficult to detect a specific pattern of prognostic factors of changes after multi-domain CT (see Tables 2, 3 for a detailed overview of the results).
Regarding prognostic factor studies, 13 studies were investigated. Two studies found that lower baseline performance in the trained task predicted improvements in executive functions (Oswald et al., 1996; Gallen et al., 2016). One study showed that lower age predicted improvements in global cognition, memory, and executive functions (Legault et al., 2011), whereas the other study investigating age in these domains did not find significant results (Oswald et al., 1996). Yet, no more patterns could be detected over the prognostic factor studies. N = 2 studies did not report the directions of the results at all (Lövdén et al., 2010; Akimoto et al., 2016), n = 5 studies only reported the directions of the significant correlations (Oswald et al., 1996; Legault et al., 2011; Kim et al., 2015; Otsuka et al., 2015; Niu et al., 2016), and did not report directions of non-significant results (results of all studies are depicted in more detail in Table 2).
Four models that included age as a prognostic factor [two using a latent change score model (Schmiedek et al., 2010; Shing et al., 2012), two using multiple regression analyses (Nouchi et al., 2019; Roheger et al., 2020c)] did not find a significant relation between age and changes after multi-domain CT in the domains global cognition (Roheger et al., 2020c), memory (Schmiedek et al., 2010; Nouchi et al., 2019; Roheger et al., 2020c), attention (Nouchi et al., 2019; Roheger et al., 2020c), executive function (Schmiedek et al., 2010; Shing et al., 2012; Niu et al., 2016; Roheger et al., 2020c), language (Roheger et al., 2020c), or visuo-spatial abilities (Roheger et al., 2020c). Only Shing et al. (2012) found a negative correlation in the domain memory, indicating younger participants to benefit more from the training. Baseline performance was integrated as a prognostic factor in three prognostic model studies [one using a structural equation model (Binder et al., 2016), two using multiple regression models (Nouchi et al., 2019; Roheger et al., 2020c)], showing contradictory results: while in one study participants with higher baseline performance benefited most in executive functions (Nouchi et al., 2019), results of the two other studies showed that participants with lower baseline performance benefited in this domain (Binder et al., 2016; Roheger et al., 2020c). Only two studies used exact the same prognostic factors in their model (López-Higes et al., 2018a,b), but investigated different outcome domains, therefore not serving as a validation of their results. They found that lower cognitive reserve leads to more benefit in global cognition (López-Higes et al., 2018a), and that lower cognitive reserve leads to more benefit scores in the language domain (López-Higes et al., 2018b).
The aim of the present review was to identify prognostic factors and models for predicting changes after multi-domain CT in healthy older adults. Our main results are that (i) there is a high heterogeneity not only regarding the conducted multi-domain CT, but also regarding the investigated prognostic factors, the investigated outcomes, and the used statistical approaches, and that (ii) there is a poor reporting of prognostic factor and model studies. Further, (iii) investigated predictors include sociodemographic variables (i.e., age, sex, education), neuropsychological performance at study entry in different tasks and domains, further psychological variables (i.e., quality of life, depression), training characteristics (i.e., modality, intensity), genetic variables (i.e., apolipoprotein E4), brain imaging measures, and EEG markers. Age and baseline performance were the most investigated predictors, but results are inconsistent.
The present review shows that most prognostic factor and model studies show strong methodological shortcomings and therefore conclusions are difficult. Several guidelines for the adequate conduction and reporting of prognostic factor and model studies exist (Moons et al., 2009, 2015; Riley et al., 2013; Steyerberg et al., 2013). Yet, none of the included studies used any of the guidelines designed for the reporting of prognostic models and factors; only two studies (Mayas et al., 2014; Nouchi et al., 2019) stated that they used the CONSORT reporting guideline for RCTs (Cuschieri, 2019). The present review underlines the need to use these guidelines in order to generate evidence-based, reproducible and reliable results as it is not possible to generate these from studies without a clear reporting of predictors or statistical analysis used. In the Supplementary Material, we provide the TRIPOD Statement Checklist (Moons et al., 2015) as an example guideline to demonstrate which aspects are important when reporting prognostic research. Specific explanations and examples can be obtained in the original publication and go beyond the scope of the present review. Furthermore, validation of the results of prognostic research is essential as performance in “a validation study is arguably all that matters, and how a model was derived is of little importance if it performs well” (Steyerberg et al., 2013). However, validation is missing in most of the conducted studies. In the field of non-pharmacological—and more specific, cognitive–interventions, it seems important that the perception of prognostic research changes: from being a solely “add-on analysis” of a present study to the own research methodology with its challenges and obstacles that it is. Without this change of perception and a change in the conduction of prognostic research according to the present guidelines, further development in this research field will not be achieved.
However, keeping the limitations named above in mind, some study results should still be discussed. Regarding sociodemographic predictors, one prognostic factor study and one prognostic model study found younger participants to benefit more from multi-domain CT in the domain memory, while four prognostic model studies could not show a significant relationship between age and performance change after multi-domain CT. While these results are conflicting, they are also not in line with the results found in a recent systematic review on prognostic factors of solely memory training on memory outcomes (Roheger et al., 2020a), in which older participants benefited most from the training. Yet, one possible reason might be that multi-domain trainings challenge a larger variety of domains than a single-domain memory training, so that the multi-domain training might be more complex, and effects are harder to achieve due to the lower intensity of training of specific domains. As a result, it may be easier for younger participants to train in a multi-domain training than older participants. So far, results on prognostic factors on single and multi-domain CT performance have been discussed in the context of the magnification and the compensation account (Lövdén et al., 2012). The magnification account is prominent for interpreting the increase in adult age differences after trainings as it suggests that individual and age-related differences in gains from CT can be explained by initial differences in cognitive resources available to acquire, implement, and sharpen effortful cognitive strategies. In adult lifespan samples cognitive abilities and possible gains from mnemonic training seem to decline with age (Verhaeghen and Marcoen, 1996; Rönnlund et al., 2005). The magnification account predicts that group differences will magnify after the training (Lövdén et al., 2012). On the contrary, the compensation account states that individuals who are already functioning at optimal levels have less room for changes in memory training performance. Older participants may then have more room for cognitive improvement as younger adults. Gains from CT should correlate negatively with cognitive abilities and age differences are reduced after training. Both accounts are still under debate regarding the conditions under which they occur (Karbach and Unger, 2014). Yet, a recent methodological assessment of the existing and potential evidence in favor of the compensation account of CT shows that most of the evidence is highly questionable due to the incorrect use of statistics (Smoleń et al., 2018). Smolen and colleagues showed that a negative correlation of pre-test score and training gain occurs naturally when gain (treated as the dependent variable) is the linear function of the independent variable (pre-test). This is a special example of a general statistical artifact called regression to the mean. Therefore, the authors suggest using graphical and structural equation models when investigating prognostic factors of CT gains, which is also emphasized in the previous cited guidelines on prognostic factor and model research. Notably, while we did not find education to be predictive for changes in multi-domain CT, education is also a factor that should be investigated in more detail in further studies on prognostic factors and models of changes after multi-domain CT. Educational attainment moderated training effects on cognitive outcomes in healthy older adults in the recent meta-analysis by Basak et al. (2020), indicating that participants with less formal education benefitted more from CT (Basak et al., 2020).
Regarding possible neuropsychological predictors, results are also inconsistent. In two prognostic factor and also two prognostic model studies, lower neuropsychological performance at study entry predicted gains in the investigated cognitive outcomes, while one other prognostic model study found higher baseline performance to be predictive for training benefit. Yet, as prognostic model studies included different types of possible predictors additionally to neuropsychological performance at study entry, it is not possible to detect why different results were found. For such an analysis, identical prognostic models in different study samples would be needed to draw clearer conclusions. Again, for the explanation of differences in neuropsychological performance at study entry, the magnification and compensation accounts can be consulted (with consideration of the already outlined methodological critique and the awareness that it is still not clear under which circumstances these two accounts occur). Future research about these two explanation approaches and linked statistical methods is needed to draw clearer conclusions.
In the present review, investigated predictors include sociodemographic variables (i.e., age, sex, education), neuropsychological performance at study entry in different tasks and domains, further psychological variables (i.e., quality of life, depression), training characteristics (i.e., modality, intensity), genetic variables (i.e., apolipoprotein E4), brain imaging measures, and EEG markers. Age and baseline cognitive performance were most used as these are standard covariates used in most studies. However, one has to take into account that there are of course several other potential predictors that might have an influence on CT and that should be considered in future studies on prognostic factors and/or models for changes after CT. Examples are psychological variables including intelligence (Lee et al., 2015), personality traits (Hill et al., 2014), or locus of control (Wolinsky et al., 2010), as well as social factors such as isolation and networking (Evans et al., 2018).
In the present review, studies that used structural equation modeling did not find significant effects when investigating age and multi-domain CT gain, and mixed effects when investigating baseline neuropsychological performance and multi-domain CT gain. Therefore, it has to be emphasized again that more research with adequate statistical analysis and reporting is needed to gather robust evidence on this topic. As a consequence of the methodological shortcomings and the heterogeneity of the studies, no further results on prognostic models can be discussed meaningfully.
There are some limitations that have to be taken into account when reading this review. First, as outlined, data was too rare and heterogeneous to perform a meta-analysis (as we registered in our pre-registration). However, important methodological shortcomings regarding the statistics and reporting could be identified, so that suggestions to improve the data quality can be outlined for future research. Second, as only German and English articles were included in the present review, this implies a possible limitation of the present review due to the fact that we might have missed information of articles in other languages. As a more general limitation regarding research on multi-domain trainings, they are in some cases more complex than single-domain trainings and aim at emphasizing complex cognitive interactions by simultaneously engaging either multiple lower-level mental processes (e.g., attention, memory, etc.) or higher-level executive functions (e.g,. inhibition, flexibility of thinking) (Tagliabue et al., 2018). Consequently, the trained domains of the included studies are naturally highly heterogeneous and it is difficult to pinpoint which aspect of the training actually brings benefit. In addition to that, the optimal amount of different trained modalities will likely differ on an individual basis; therefore, a personalized approach to CTs as it is addressed in this review with the aim to identify possible predictors, might lead to more sustained and significant outcomes (Ball et al., 2007). Furthermore, we decided to exclude videogames and brain trainings, that did not specifically state which cognitive domains they target. Therefore, we might have missed some studies that could potentially be included in the systematic review. Yet, we made this decision as an explicit outline of trained domains was a prerequisite to be able to clearly include multi-domain trainings. Future studies should explicitly investigate effects and responsiveness to videogames and brain trainings, but will have to access more detailed information that goes beyond those available in the manuscripts published.
Summarized, this is the first systematic review on prognostic factors and models of multi-domain CT. Prognostic research is of high importance in informing prevention decisions (either directly or as part of prognostic models for an individualized prediction), and also in improving the design of intervention trials and in targeting new interventions to strengthen cognitive function in older adults (Riley et al., 2013). By fostering knowledge in this field, we will not only be able to state that multi-domain CT is effective in strengthening cognition in healthy older adults (Basak et al., 2020) as a group (which is a highly important message due to the aging population and the related risk for cognitive decline and dementia), but who—with which profile of characteristics—benefits from which CT. Yet, the present review showed that prognostic research in multi-domain CT is still at the beginning: even though clear guidelines exist, most studies have statistical shortcomings and/ or are poorly reported, and results are therefore not reliable. Future prognostic research should focus on using registered study protocols, large sample sizes, appropriate statistical methods, and transparent reporting. Sociodemographic variables (i.e., age, sex, and education), neuropsychological test status at study entry in different domains, further psychological variables (i.e., quality of life, depression), training characteristics (i.e., modality, intensity), genetic variables (i.e., apolipoprotein E4), brain imaging measures, and EEG markers may be possible predictors that influence multi-domain CT gains.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
MR, HLJ, and EK contributed to conception of the study. FK organized the database. MR wrote the first draft of the manuscript. HLJ and AA wrote sections of the manuscript. AA advised statistical analysis. All authors contributed to manuscript revision, read, and approved the submitted version.
This study was funded by the Brandau-Laibach foundation of the University Hospital of Cologne, Germany.
MR has received a grant from the Brandau-Laibach Stiftung, and a grant from the German Ministry of Education and Research. AA has received a grant from the Brandau-Laibach Stiftung. EK has received grants from the German Ministry of Education and Research, ParkinsonFonds Deutschland GmbH, the German Parkinson Society; honoraria from: Oticon GmbH, Hamburg, Germany; Lilly Pharma GmbH, Bad Homburg, Germany; Bernafon AG, Bern, Switzerland; Desitin GmbH, Hamburg, Germany. EK is author of the CT program NEUROvitalis but receives no corresponding honoraria.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnhum.2021.636355/full#supplementary-material
Akimoto, Y., Nozawa, T., Kanno, A., Kambara, T., Ihara, M., Ogawa, T., et al. (2016). High-gamma power changes after cognitive intervention: preliminary results from twenty-one senior adult subjects. Brain Behav. 6:e00427. doi: 10.1002/brb3.427
Anderson, S., White-Schwoch, T., Choi, H. J., and Kraus, N. (2014). Partial maintenance of auditory-based cognitive training benefits in older adults. Neuropsychologia 62, 286–296. doi: 10.1016/j.neuropsychologia.2014.07.034
Ball, K., Edwards, J. D., and Ross, L. A. (2007). The impact of speed of processing training on cognitive and everyday functions. J. Gerontol. B Psychol. Sci. Soc. Sci. 62, 19–31. doi: 10.1093/geronb/62.special_issue_1.19
Basak, C., Qin, S., and O'Connell, M. A. (2020). Differential effects of cognitive training modules in healthy aging and mild cognitive impairment: a comprehensive meta-analysis of randomized controlled trials. Psychol. Aging 35, 220–249. doi: 10.1037/pag0000442
Bellander, M., Bäckman, L., Liu, T., Schjeide, B.-M. M., Bertram, L., Schmiedek, F., et al. (2015). Lower baseline performance but greater plasticity of working memory for carriers of the val allele of the COMT Val58Met polymorphism. Neuropsychology 29, 247–254. doi: 10.1037/neu0000088
Binder, J. C., Martin, M., Zöllig, J., Röcke, C., Mérillat, S., Eschen, A., et al. (2016). Multi-domain training enhances attentional control. Psychol. Aging 31, 390–408. doi: 10.1037/pag0000081
Binder, J. C., Zöllig, J., Eschen, A., Mérillat, S., Röcke, C., Schoch, S. F., et al. (2015). Multi-domain training in healthy old age: hotel Plastisse as an iPad-based serious game to systematically compare multi-domain and single-domain training. Front. Aging Neurosci. 7:137. doi: 10.3389/fnagi.2015.00137
Chiu, H.-L., Chu, H., Tsai, J.-C., Liu, D., Chen, Y.-R., Yang, H.-L., et al. (2017). The effect of cognitive-based training for the healthy older people: a meta-analysis of randomized controlled trials. PLoS ONE 12:e0176742. doi: 10.1371/journal.pone.0176742
Cuschieri, S. (2019). The STROBE guidelines. Saudi J Anaesth. 13(Suppl 1), S31–S34. doi: 10.4103/sja.SJA_543_18
Evans, I. E. M., Llewellyn, D. J., Matthews, F. E., Woods, R. T., Brayne, C., and Clare, L. (2018). Social isolation, cognitive reserve, and cognition in healthy older people. PLoS ONE 13:e0201008. doi: 10.1371/journal.pone.0201008
Fernández-Prado, S., Conlon, S., Mayán-Santos, J. M., and Gandoy-Crego, M. (2012). The influence of a cognitive stimulation program on the quality of life perception among the elderly. Arch. Gerontol. Geriatr. 54, 181–184. doi: 10.1016/j.archger.2011.03.003
Gallen, C. L., Baniqued, P. L., Chapman, S. B., Aslan, S., Keebler, M., Didehbani, N., et al. (2016). Modular brain network organization predicts response to cognitive training in older adults. PLoS ONE 11:e0169015. doi: 10.1371/journal.pone.0169015
Hayden, J. A., van der Windt, D. A., Cartwright, J. L., Côté, P., and Bombardier, C. (2013). Assessing bias in studies of prognostic factors. Ann. Intern. Med. 158, 280–286. doi: 10.7326/0003-4819-158-4-201302190-00009
Higgins, J. (2008). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1. The Cochrane Collaboration. Available online at: http://www.cochrane-handbook.org
Hill, N. L., Kolanowski, A. M., Fick, D., Chinchilli, V. M., and Jablonski, R. A. (2014). Personality as a moderator of cognitive stimulation in older adults at high risk for cognitive decline. Res. Gerontol. Nurs. 7, 159–170. doi: 10.3928/19404921-20140311-01
Hughes, M. L., Agrigoroaei, S., Jeon, M., Bruzzese, M., and Lachman, M. E. (2018). Change in cognitive performance from midlife into old age: findings from the midlife in the United States (MIDUS) study. J. Int. Neuropsychol. Soc. 24, 805–820. doi: 10.1017/S1355617718000425
Karbach, J., and Unger, K. (2014). Executive control training from middle childhood to adolescence. Front. Psychol. 5:390. doi: 10.3389/fpsyg.2014.00390
Kim, G. H., Jeon, S., Im, K., Kwon, H., Lee, B. H., Kim, G. Y., et al. (2015). Structural brain changes after traditional and robot-assisted multi-domain cognitive training in community-dwelling healthy elderly. PLoS ONE 10:e0123251. doi: 10.1371/journal.pone.0123251
Küper, K., Gajewski, P. D., Frieg, C., and Falkenstein, M. (2017). A randomized controlled ERP study on the effects of multi-domain cognitive training and task difficulty on task switching performance in older adults. Front. Hum. Neurosci. 11:184. doi: 10.3389/fnhum.2017.00184
Lee, H., Boot, W. R., Baniqued, P. L., Voss, M. W., Prakash, R. S., Basak, C., et al. (2015). The relationship between intelligence and training gains is moderated by training strategy. PLoS ONE 10:e0123259. doi: 10.1371/journal.pone.0123259
Legault, C., Jennings, J. M., Katula, J. A., Dagenbach, D., Gaussoin, S. A., Sink, K. M., et al. (2011). Designing clinical trials for assessing the effects of cognitive training and physical activity interventions on cognitive outcomes: the Seniors Health and Activity Research Program Pilot (SHARP-P) study, a randomized controlled trial. BMC Geriatr. 11:27. doi: 10.1186/1471-2318-11-27
Li, T., Yao, Y., Cheng, Y., Xu, B., Cao, X., Waxman, D., et al. (2016). Cognitive training can reduce the rate of cognitive aging: a neuroimaging cohort study. BMC Geriatr. 16:12. doi: 10.1186/s12877-016-0194-5
López-Higes, R., Martín-Aragoneses, M. T., Rubio-Valdehita, S., Delgado-Losada, M. L., Montejo, P., Montenegro, M., et al. (2018a). Efficacy of cognitive training in older adults with and without subjective cognitive decline is associated with inhibition efficiency and working memory span, not with cognitive reserve. Front. Aging Neurosci. 10:23. doi: 10.3389/fnagi.2018.00023
López-Higes, R., Prados, J. M., Rubio-Valdehita, S., Rodríguez-Rojo, I., Frutos-Lucas, J., de, Montenegro, M., et al. (2018b). Factors explaining language performance after training in elders with and without subjective cognitive decline. Front. Aging Neurosci. 10:264. doi: 10.3389/fnagi.2018.00264
Lövdén, M., Bodammer, N. C., Kühn, S., Kaufmann, J., Schütze, H., Tempelmann, C., et al. (2010). Experience-dependent plasticity of white-matter microstructure extends into old age. Neuropsychologia 48, 3878–3883. doi: 10.1016/j.neuropsychologia.2010.08.026
Lövdén, M., Brehmer, Y., Li, S.-C., and Lindenberger, U. (2012). Training-induced compensation versus magnification of individual differences in memory performance. Front. Hum. Neurosci. 6:141. doi: 10.3389/fnhum.2012.00141
Martin, M., Clare, L., Altgassen, A. M., Cameron, M. H., and Zehnder, F. (2011). Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database Syst Rev. 19:CD006220. doi: 10.1002/14651858.CD006220.pub2
Mayas, J., Parmentier, F. B. R., Andrés, P., and Ballesteros, S. (2014). Plasticity of attentional functions in older adults after non-action video game training: a randomized controlled trial. PLoS ONE 9:e92269. doi: 10.1371/journal.pone.0092269
McDougall, S., and House, B. (2012). Brain training in older adults: evidence of transfer to memory span performance and pseudo-Matthew effects. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 19, 195–221. doi: 10.1080/13825585.2011.640656
Miller, K. J., Dye, R. V., Kim, J., Jennings, J. L., O'Toole, E., Wong, J., et al. (2013). Effect of a computerized brain exercise program on cognitive performance in older adults. Am. J. Geriatr. Psychiatry 21, 655–663. doi: 10.1016/j.jagp.2013.01.077
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. doi: 10.1371/journal.pmed.1000097
Moons, K. G. M., Altman, D. G., Reitsma, J. B., Ioannidis, J. P. A., Macaskill, P., Steyerberg, E. W., et al. (2015). Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): explanation and elaboration. Ann. Intern. Med. 162, W1–73. doi: 10.7326/M14-0698
Moons, K. G. M., Groot, J. A. H., de, Bouwmeester, W., Vergouwe, Y., Mallett, S., Altman, D. G., et al. (2014). Critical appraisal and data extraction for systematic reviews of prediction modelling studies: the CHARMS checklist. PLoS Med 11:e1001744. doi: 10.1371/journal.pmed.1001744
Moons, K. G. M., Royston, P., Vergouwe, Y., Grobbee, D. E., and Altman, D. G. (2009). Prognosis and prognostic research: what, why, and how? BMJ 338:b375. doi: 10.1136/bmj.b375
Niu, Y.-N., Zhu, X., Li, J., and Fu, J.-N. (2016). The ERP effects of combined cognitive training on intention-based and stimulus-based actions in older Chinese adults. Front. Psychol. 7:1670. doi: 10.3389/fpsyg.2016.01670
Nouchi, R., Kobayashi, A., Nouchi, H., and Kawashima, R. (2019). Newly developed TV-based cognitive training games improve car driving skills, cognitive functions, and mood in healthy older adults: evidence from a randomized controlled trial. Front. Aging Neurosci. 11:99. doi: 10.3389/fnagi.2019.00099
Oswald, W. D., Rupprecht, R., Gunzelmann, T., and Tritt, K. (1996). The SIMA-project: effects of 1 year cognitive and psychomotor training on cognitive abilities of the elderly. Behav. Brain Res. 78, 67–72. doi: 10.1016/0166-4328(95)00219-7
Otsuka, T., Tanemura, R., Noda, K., Nagao, T., Sakai, H., and Luo, Z.-W. (2015). Development of computer-aided cognitive training program for elderly and its effectiveness through a 6 months group intervention study. Curr. Alzheimer Res. 12, 553–562. doi: 10.2174/1567205012666150530202335
Polito, L., Abbondanza, S., Vaccaro, R., Valle, E., Davin, A., Degrate, A., et al. (2015). Cognitive stimulation in cognitively impaired individuals and cognitively healthy individuals with a family history of dementia: short-term results from the “Allena-Mente” randomized controlled trial. Int. J. Geriatr. Psychiatry 30, 631–638. doi: 10.1002/gps.4194
Reijnders, J., van Heugten, C., and van Boxtel, M. (2013). Cognitive interventions in healthy older adults and people with mild cognitive impairment: a systematic review. Ageing Res. Rev. 12, 263–275. doi: 10.1016/j.arr.2012.07.003
Reuter-Lorenz, P. A., and Park, D. C. (2014). How does it STAC up? Revisiting the scaffolding theory of aging and cognition. Neuropsychol. Rev. 24, 355–370. doi: 10.1007/s11065-014-9270-9
Riley, R. D., Hayden, J. A., Steyerberg, E. W., Moons, K. G. M., Abrams, K., Kyzas, P. A., et al. (2013). Prognosis Research Strategy (PROGRESS) 2: prognostic factor research. PLoS Med. 10:e1001380. doi: 10.1371/journal.pmed.1001380
Roheger, M., Folkerts, A.-K., Krohm, F., Skoetz, N., and Kalbe, E. (2020a). Prognostic factors for change in memory test performance after memory training in healthy older adults: a systematic review and outline of statistical challenges. Diagn Progn Res. 4:7. doi: 10.1186/s41512-020-0071-8
Roheger, M., Meyer, J., Kessler, J., and Kalbe, E. (2020c). Predicting short- and long-term cognitive training success in healthy older adults: who benefits? Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 27, 351–369. doi: 10.1080/13825585.2019.1617396
Roheger, M., Folkerts, A.-K., Krohm, F., Skoetz, N., and Kalbe, E. (2020b). Prognostic models for changes in memory performance after memory training in healthy older adults: a systematic review. J. Cogn. Enhanc. 1–14. doi: 10.1007/s41465-020-00194-0
Rönnlund, M., Nyberg, L., Bäckman, L., and Nilsson, L.-G. (2005). Stability, growth, and decline in adult life span development of declarative memory: cross-sectional and longitudinal data from a population-based study. Psychol. Aging 20, 3–18. doi: 10.1037/0882-7974.20.1.3
Schmiedek, F., Lövdén, M., and Lindenberger, U. (2010). Hundred days of cognitive training enhance broad cognitive abilities in adulthood: findings from the COGITO study. Front Aging Neurosci. 2:27. doi: 10.3389/fnagi.2010.00027
Shah, T., Verdile, G., Sohrabi, H., Campbell, A., Putland, E., Cheetham, C., et al. (2014). A combination of physical activity and computerized brain training improves verbal memory and increases cerebral glucose metabolism in the elderly. Transl. Psychiatry 4:e487. doi: 10.1038/tp.2014.122
Shah, T. M., Weinborn, M., Verdile, G., Sohrabi, H. R., and Martins, R. N. (2017). Enhancing cognitive functioning in healthly older adults: a systematic review of the clinical significance of commercially available computerized cognitive training in preventing cognitive decline. Neuropsychol. Rev. 27, 62–80. doi: 10.1007/s11065-016-9338-9
Shing, Y. L., Schmiedek, F., Lövdén, M., and Lindenberger, U. (2012). Memory updating practice across 100 days in the COGITO study. Psychol. Aging 27, 451–461. doi: 10.1037/a0025568
Simons, D. J., Boot, W. R., Charness, N., Gathercole, S. E., Chabris, C. F., Hambrick, D. Z., et al. (2016). Do “brain-training” programs work? Psychol. Sci. Public Interest 17, 103–186. doi: 10.1177/1529100616661983
Smoleń, T., Jastrzebski, J., Estrada, E., and Chuderski, A. (2018). Most evidence for the compensation account of cognitive training is unreliable. Mem. Cognit. 46, 1315–1330. doi: 10.3758/s13421-018-0839-z
Steyerberg, E. W., Moons, K. G. M., van der Windt, D. A., Hayden, J. A., Perel, P., Schroter, S., et al. (2013). Prognosis research strategy (PROGRESS) 3: prognostic model research. PLoS Med. 10:e1001381. doi: 10.1371/journal.pmed.1001381
Tagliabue, C. F., Guzzetti, S., Gualco, G., Boccolieri, G., Boccolieri, A., Smith, S., et al. (2018). A group study on the effects of a short multi-domain cognitive training in healthy elderly Italian people. BMC Geriatr. 18:321. doi: 10.1186/s12877-018-1014-x
Valenzuela, M., and Sachdev, P. (2009). Can cognitive exercise prevent the onset of dementia? Systematic review of randomized clinical trials with longitudinal follow-up. Am. J. Geriatr. Psychiatry 17, 179–187. doi: 10.1097/JGP.0b013e3181953b57
Verhaeghen, P., and Marcoen, A. (1996). On the mechanisms of plasticity in young and older adults after instruction in the method of loci: evidence for an amplification model. Psychol. Aging 11, 164–178. doi: 10.1037/0882-7974.11.1.164
Walton, C. C., Kavanagh, A., Downey, L. A., Lomas, J., Camfield, D. A., and Stough, C. (2015). Online cognitive training in healthy older adults: a preliminary study on the effects of single versus multi-domain training. Transl. Neurosci. 6, 13–19. doi: 10.1515/tnsci-2015-0003
Wolff, R. F., Moons, K. G. M., Riley, R. D., Whiting, P. F., Westwood, M., Collins, G. S., et al. (2019). PROBAST: a tool to assess the risk of bias and applicability of prediction model studies. Ann. Intern. Med. 170, 51–58. doi: 10.7326/M18-1376
Keywords: prognostic factors, prognostic model, cognitive training, prediction, cognition, memory
Citation: Roheger M, Liebermann-Jordanidis H, Krohm F, Adams A and Kalbe E (2021) Prognostic Factors and Models for Changes in Cognitive Performance After Multi-Domain Cognitive Training in Healthy Older Adults: A Systematic Review. Front. Hum. Neurosci. 15:636355. doi: 10.3389/fnhum.2021.636355
Received: 01 December 2020; Accepted: 26 March 2021;
Published: 27 April 2021.
Edited by:
Chandramallika Basak, The University of Texas at Dallas, United StatesReviewed by:
Mike Martin, University of Zurich, SwitzerlandCopyright © 2021 Roheger, Liebermann-Jordanidis, Krohm, Adams and Kalbe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elke Kalbe, ZWxrZS5rYWxiZUB1ay1rb2Vsbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.