 Anna Buchheim1*
Anna Buchheim1* Susanne Erk2
Susanne Erk2 Carol George3
Carol George3 Horst Kächele4
Horst Kächele4 Philipp Martius5
Philipp Martius5 Dan Pokorny6
Dan Pokorny6 Manfred Spitzer7
Manfred Spitzer7 Henrik Walter2
Henrik Walter2- 1Institute of Psychology, University of Innsbruck, Innsbruck, Austria
- 2Department of Psychiatry and Psychotherapy, Division of Mind and Brain Research, University Hospital Charité, Berlin, Germany
- 3Department of Psychology, Mills College, Oakland, CA, USA
- 4International Psychoanalytic University Berlin, Berlin, Germany
- 5Psychosomatic Hospital, Höhenried, Berlin, Germany
- 6Department of Psychosomatic Medicine and Psychotherapy, University of Ulm, Ulm, Germany
- 7Department of Psychiatry III, University of Ulm, Ulm, Germany
Individuals with borderline personality disorder (BPD) are characterized by emotional instability, impaired emotion regulation and unresolved attachment patterns associated with abusive childhood experiences. We investigated the neural response during the activation of the attachment system in BPD patients compared to healthy controls using functional magnetic resonance imaging (fMRI). Eleven female patients with BPD without posttraumatic stress disorder (PTSD) and 17 healthy female controls matched for age and education were telling stories in the scanner in response to the Adult Attachment Projective Picture System (AAP), an eight-picture set assessment of adult attachment. The picture set includes theoretically-derived attachment scenes, such as separation, death, threat and potential abuse. The picture presentation order is designed to gradually increase the activation of the attachment system. Each picture stimulus was presented for 2 min. Analyses examine group differences in attachment classifications and neural activation patterns over the course of the task. Unresolved attachment was associated with increasing amygdala activation over the course of the attachment task in patients as well as controls. Unresolved controls, but not patients, showed activation in the right dorsolateral prefrontal cortex (DLPFC) and the rostral cingulate zone (RCZ). We interpret this as a neural signature of BPD patients’ inability to exert top-down control under conditions of attachment distress. These findings point to possible neural mechanisms for underlying affective dysregulation in BPD in the context of attachment trauma and fear.
Introduction
Disturbances in the processing and regulation of emotions are core symptoms of borderline personality disorder (BPD; Leichsenring et al., 2011; Herpertz and Bertsch, 2015; Schulze et al., 2016). Emotional dysregulation is thought to result from increased impulsivity combined with the inability to modulate emotional responses (Linehan et al., 1994; Skodol et al., 2002; Lieb et al., 2004; Putnam and Silk, 2005; Conklin et al., 2006; Viviani et al., 2011; Mitchell et al., 2014; Scherpiet et al., 2014; Schmahl et al., 2014; Herpertz and Bertsch, 2015; van Zutphen et al., 2015).
Attachment theory provides a powerful framework for understanding links between close relationships, mental representations of attachment, and psychopathology (Westen et al., 2006; Bakermans-Kranenburg and van IJzendoorn, 2009). Early experiences of maltreatment, such as sexual and physical abuse and emotional neglect, are implicated in the etiology of BPD (Bandelow et al., 2005; Gunderson et al., 2006; Zanarini et al., 2006; van Dijke et al., 2011; Keinänen et al., 2012; Frías et al., 2016). Adverse attachment experiences, especially relationships trauma, are considered to be risk factors for poor emotion-regulation, functional impairment of mentalization, separation anxiety, and fear (Bowlby, 1973; Milrod et al., 2014; Mosquera et al., 2014; Brüne et al., 2016). The concept of adult attachment concerns an individual’s current representational state with respect to early attachment relationships and their associated modes of defense and affect regulation. A large number of studies in adult attachment research have used the Adult Attachment Interview (AAI) or the Adult Attachment Projective Picture System (AAP) as narrative-based assessments of mental representations of attachment (George et al., 1984/1985/1996; Main and Goldwyn, 1995; George et al., 1999; George and West, 2001, 2012). Attachment classifications are derived from the analysis of narratives with three organized/resolved patterns (also termed attachment status), namely secure, dismissing, preoccupied and unresolved with respect to trauma or loss. Important for our study is the categorization into “resolved” (i.e., either secure, insecure dismissing, insecure-preoccupied) vs. “unresolved” attachment patterns in adults. The narratives of individuals who are unresolved demonstrate their inability to contain or integrate frightening thematic elements. These individuals, overwhelmed by trauma or loss, become dysregulated when attachment is activated during assessment. Dysregulation can be momentary or prolonged, but in either case the individual is unable to use defensive processes to remain organized and recover from conscious thoughts and feelings of frightening distress.
Insecure attachment patterns demonstrate risk for the maladaptive personality traits underlying BPD (Scott et al., 2009). BPD has been associated with increased occurrence of insecure and especially unresolved attachment representations (Agrawal et al., 2004; Bakermans-Kranenburg and van IJzendoorn, 2009; Buchheim and George, 2011). Unresolved attachment has been linked to psychological disorders, impaired cognitive functioning and trauma-related psychopathology (Fearon and Mansell, 2001; Nakash-Eisikovits et al., 2002; Lyons-Ruth and Jacobvitz, 2008; Joubert et al., 2012).
Emotional vulnerability in BPD patients may result from a marked sensitivity to emotional stimuli, an impairment of emotion regulation, or both (Gunderson and Lyons-Ruth, 2008). An attentional bias toward negative information in patients with BPD can be seen in neuroimaging data showing increased and prolonged amygdala responses (Herpertz et al., 2001; Donegan et al., 2003; Hazlett et al., 2012; Kamphausen et al., 2013; Schulze et al., 2016), and enhanced activity in the anterior insula (Schulze et al., 2011; Ruocco et al., 2013). Furthermore, study results indicate reductions in amygdala and hippocampal volume in BPD patients (Driessen et al., 2000; Schmahl et al., 2003, 2009; van Elst et al., 2003; Irle et al., 2005; O’Neill and Frodl, 2012; Rossi et al., 2012; O’Neill et al., 2013; Ruocco et al., 2013).
As emotion regulation is dependent on regions exerting cognitive control, like the dorsolateral prefrontal cortex (DLPFC) and medial prefrontal/anterior cingulate cortex (mPFC/ACC; for a review see Ochsner and Gross, 2005), a deficit in emotion regulation should be mediated by reduced activation in these regions in tasks affording emotion control. Studies using Positron emission tomography revealed hypometabolism in PFC of BPD patients compared with healthy controls (De La Fuente et al., 1997; Soloff et al., 2000) and enhanced activation of DLPFC when BPD patients were confronted with individual scripts that evoke personal memories of abandonment and abuse (Schmahl et al., 2003, 2004; Lang et al., 2012). In another study using magnetic resonance spectroscopy (van Elst et al., 2001), BPD patients showed a decreased level of N-acetyl aspartate, which suggests impaired neural functioning in the DLPFC. BPD patients showed metabolic alterations in the amygdala using proton magnetic resonance spectroscopy (Hoerst et al., 2010).
Moreover studies investigated brain activation during processing of autobiographical memory in BPD. One study examining unresolved as compared to resolved life events found, among other regions, increasing activation of amygdala and anterior cingulate cortex (Beblo et al., 2006). A follow up analysis from that study 1 year later reported substantial decrease of temporo-frontal activation during the recall of unresolved negative life, suggesting that these activations were not stable over time (Driessen et al., 2009). Mensebach et al. (2009), comparing episodic and semantic memory retrieval, demonstrated that BPD patients might need to engage larger brain areas to reach a level of performance in episodic and semantic retrieval tasks than comparable healthy controls. A recent study using a stimulus-driven Episodic Memory task showed that negative affective interference with cognitive processing differed in BPD patients compared to healthy controls (Soloff et al., 2015). This pattern was associated with functional abnormalities in brain networks reported to have structural or metabolic abnormalities, like the increased activation of the amygdala (Soloff et al., 2015).
In sum, emotion regulation and their neural correlates are impaired in BPD patients; for example, amygdala responses are prolonged and enhanced in particular during the presentation of emotional stimuli (for a review see Buchheim et al., 2013). Furthermore, traumatic experiences are considered as crucial in these processes. These impairments may be part of the neural mechanisms underlying emotional dysregulation in BPD patients (Kamphausen et al., 2013). Functional anomalies might also have an important impact on cognitive processes. A recent study of Enzi et al. (2013) demonstrated that impaired emotion processing seems to affect the reward system in patients with BPD. Moreover we can conclude, that patients with BPD have been shown to exhibit impaired neuronal activity in areas of the medial and lateral PFC that control and modulate emotional activation, thereby covering topdown processes. Functional neuroimaging studies examined prefrontal hypometabolism during regulatory control processes (O’Neill and Frodl, 2012), and a recent metaanalysis of functional magnetic resonance imaging (fMRI) studies across different stimulation procedures (Ruocco et al., 2013). These studies reported enhanced neuronal activity in the insula but reduced activity in the subgenual ACC and DLPFC in patients with BPD as compared with healthy subjects (O’Neill and Frodl, 2012; Ruocco et al., 2013).
The functional neuroimaging studies summarized above measured brain activation patterns in response to visual stimuli (pictures, faces) or passively presented scripts. Several studies have investigated the neural correlates of “social” attachment (i.e., defined loosely as individuals in intimate relationships) in healthy populations. The main paradigm in these studies is the presentation of pictures of the beloved sexual partner or their own infant by contrasting familiar vs. non-familiar stimuli (Bartels and Zeki, 2000, 2004; Leibenluft et al., 2004; Nitschke et al., 2004; Gillath et al., 2005; Coan et al., 2006; Lenzi et al., 2009; Riem et al., 2012; Wittfoth-Schardt et al., 2012). These studies have used various approaches to identify the neural correlates of distinctive attachment-related systems (caregiving or sexual system). Taking into account the differences in methods and aims, these studies have reported a common neural activity for the romantic and maternal attachment in regions associated with reward and motivation and affective processing. However, much less is known about the neural correlates of attachment representations, for example, when individuals are instructed to tell stories to attachment related pictures while being scanned in an fMRI environment.
Buchheim et al. (2006a,b) developed an fMRI paradigm to investigate the neural correlates of attachment representation while subjects tell stories to attachment pictures using the AAP stimuli (George et al., 1999; George and West, 2012). This validated narrative-based assessment is a set of stimuli and system of analysis that is theoretically derived using attachment theory, and not a traditional open-ended free-response measurement (i.e., subjective interpretation of emotional stimuli). The results of this pilot study showed unresolved attachment to be associated with increasing activation of the right amygdala, the left hippocampus and the right PFC over the course of the attachment task (i.e., from the first to the last attachment pictures).
The present study investigated neural correlates of attachment narratives in borderline patients using the same paradigm. In this article, we focus on differences between “unresolved” and “resolved” subjects. Our design permitted analysis related to other linguistic features of the AAP, which were reported elsewhere (Buchheim et al., 2008). Based on research linking BPD to unresolved attachment, we expected that amygdala activation in during the course of administering the attachment task (AAP) would be stronger in the patient group than the control group. We also expected that neural signs of emotion regulation in the cognitive control system (DLPFC and/or anterior cingulate) would decrease or be absent in the patient group.
Materials and Methods
Participants
Thirteen female BPD inpatients were recruited from a psychiatric hospital (Psychosomatic and Psychiatric Hospital, Bad Wiessee, Germany) and compared to 21 healthy female volunteers recruited for the study by an advertisement in a local newspaper and leaflets distributed in the Hospital of the University of Ulm. The sample of the 17 healthy controls in this study included the 11 subjects of our pilot study (Buchheim et al., 2006b). Subjects were matched for age and education. Patients were treated on an average for 114 days (SD: 45.3, range 26–166 days) in the psychiatric hospital and had on an average 1.77 days of inpatient stays (range 1–4, median 1). They were assessed at the beginning of their treatment. All control subjects were physically healthy, without a history of psychiatric disorder and did not use any medication. Clinical diagnoses were assessed by a trained psychiatrist1 using the Structured Clinical Interview for DSM-IV (SCID-I and SCID-II) and the International Personality Disorder Examination (IPDE). Exclusion criteria were left handedness, metal implants, language problems, and serious medical or neurological illness, including comorbid psychotic disorders and bipolar disorder. None of our patients met diagnostic criteria for posttraumatic stress disorder (PTSD) or dissociative disorder. Six subjects had to be excluded from our main analysis. Four controls were excluded for movement in the fMRI apparatus (>2 mm, see below). The only two patients who were classified as resolved were excluded from analysis because two subjects were not enough to allow any substantial group inferences. The final sample consisted of 11 BPD patients and 17 controls. Exclusion of the six subjects did not affect group homogeneity with respect to age (BPD, 27.8 years ± 6.7; controls, 28.4 years ± 7.5) and education (BPD, 10.8 years ± 1.4; controls, 10.9 years ± 1.6). Comorbidity in the final group included depression (n = 6), anxiety or panic disorder (n = 2), and somatoform disorder (n = 3). Five of the eleven patients were treated with psychotropic medication, including serotonin-reuptake inhibitors (n = 2), lithium (n = 1) and low doses of neuroleptics (perazin, promethazine and chlorprothixene, n = 3). After complete description of the study, participants provided written informed consent. The study was conducted in conformance with the Declaration of Helsinki. The protocol was approved by the local institutional ethics committee of the University of Ulm. Clinical characteristics of the sample are shown in Table 1.

Table 1. Two-group-comparison of clinical scales.
Procedure and Measures
Attachment Stimulus Presentation and Attachment Coding
Participants were administered with the fMRI-adapted version of the Adult AAP (Buchheim et al., 2006a), a validated representational adult attachment measure. The measure is comprised of a set of eight drawings, one neutral scene and seven attachment scenes. The picture set includes scenes that depict events associated with attachment activation, such as illness, separation, solitude, death, and threat (Bowlby, 1973). The picture presentation order is designed to gradually increase the activation of the attachment distress (George et al., 1999; George and West, 2003), a methodological feature that has been validated using fMRI analysis (Buchheim et al., 2006b). Pictures are administered in the following sequence: Child at Window—a child looks out a window; Departure—an adult man and woman stand facing each other with suitcases positioned nearby; Bench—a youth sits alone on a bench; Bed—a child and woman sit opposite each other on the child’s bed; Ambulance—a woman and a child watch someone being put on an ambulance stretcher; Cemetery—a man stands by a gravesite head stone; and Child in Corner—a child stands askance in a corner (example picture stimuli are provided in Figure 1).

Figure 1. (A) Picture “Departure” from the Adult Attachment Projective Picture System (AAP) © (George et al., 1999). (B) Picture “Cemetery” from the AAP © (George et al., 1999).
AAP responses are classified on the basis of verbatim transcribed narratives. The coding system defines unresolved attachment as failure to contain frightening or threatening narrative material demonstrated, for example, by story elements representing attachment dysregulation, such as death, attack, abuse, or devastation (George et al., 1999; George and West, 2003; Buchheim and George, 2011). Resolved attachment is designated when the story material either does not include these elements, or if included, the narrative demonstrates emotional integration or mental organization. This requires the story characters to demonstrate the capacity to think through solutions that describe drawing on internalized attachment resources (the “internalized secure base”), seeking out attachment figures, the capacity for positive and constructive action, or others coming to provide comfort, explanation, or assistance to quell frightening distress (Table 2). Resolved attachment status groups include secure, dismissing, and preoccupied. Secure attachment is characterized by story elements that demonstrate the capacity to think about events and feelings, and expectations for comfort from or mutual enjoyment in attachment relationships. Dismissing attachment is characterized by evidence of physical and psychological distance from attachment figures and distress in story themes, often deflecting needs for care and the desire for attachment figures’ comfort to other activities (e.g., achievement, peer relationship). Preoccupied attachment is characterized by representational confusion; the representation of people or events associated with story themes are diffused by vacillation among different and sometimes opposing ideas.
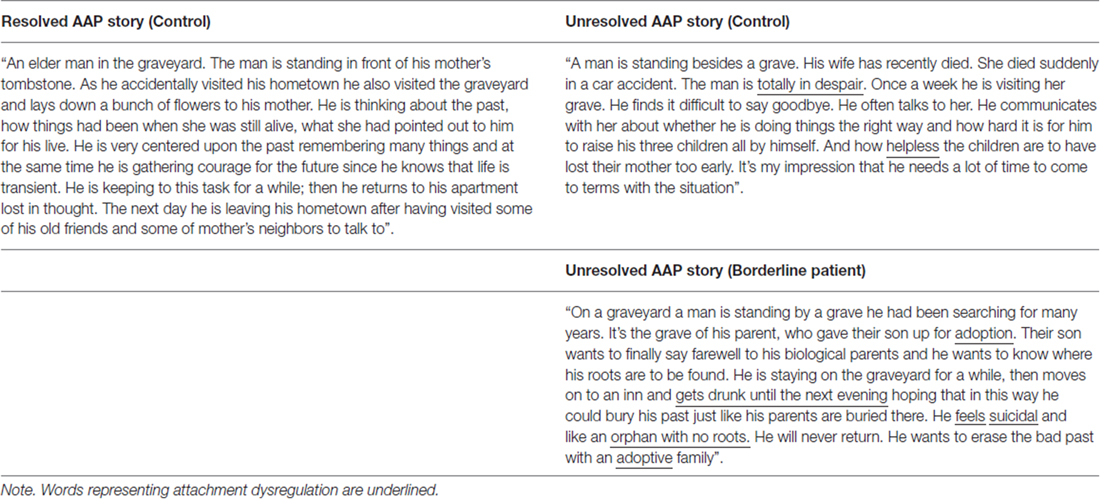
Table 2. Transcript examples of a “resolved” and two “unresolved” stories to the AAP picture “Cemetery”.
The psychometric properties of the AAP were established in an independent validity study with 144 subjects from a healthy community sample of non-patient subjects. This study demonstrated strong psychometric validity, including meeting psychometric standards for inter-judge reliability, test-retest reliability (after 3 months), discriminant validity, and convergent construct validity with another validated developmental attachment narrative assessment, the AAI (George et al., 1984/1985/1996; George and West, 2003, 2012).
In the present study, two blind, reliable AAP judges independently coded the AAP narratives of the stories that participants told in the scanner. There was unresolved-resolved agreement in 27 out of 28 cases (96%). The resulting inter-rater agreement was κ = 0.93, corresponding to “almost perfect agreement” by Landis and Koch (1977). AAP validity for scanner-produced stories was established through convergent classifications with the AAI, which were administered 1 month after fMRI AAP acquisition and classified by a blind trained reliable AAI judge. As also reported in a review on AAP classifications in different clinical groups (Buchheim and George, 2011), the correspondence between the AAP and AAI resolved vs. unresolved categories in this sample was κ = 0.70, corresponding to “substantial agreement” by Landis and Koch (1977).
MRI Acquisition
Experimental procedure
Subjects were instructed in the AAP story telling task before they entered the scanner using two non-AAP “neutral” (i.e., not attachment related scenes) pictures. The pictures were same size and drawn in the same style as the stimuli in the AAP set. The goal was for subjects to understand the scope of the probes normally asked during in-person administration. The training procedure was repeated two more times, as needed to achieve this goal. The fMRI acquisition started with the original AAP picture presentation and instructions. During scanning, subjects were visually presented the standard AAP instruction at the introduction of the stimulus (“what led up to that scene, what are the characters thinking or feeling, and what might happen next?”) for 10 s and a fixation cross for 10 s. Afterwards each AAP picture was presented (120 s) along the original order of the measure (described in the “Materials and Methods” Section). Subjects were asked to talk about the picture for at least 2 min. A fixation cross was shown for 15 s after the picture presentation until beginning a new cycle of instruction and the next picture presentation. The total procedure included nine pictures, the two neutral and seven standard AAP attachment scenes.
Data acquisition
1.5 Tesla Siemens Magnetom Symphony scanner (Siemens, Erlangen, Germany), image size: 64 × 64 voxels, FOV of 192 mm, slice thickness 4 mm with 1 mm gap, 25 slices covering the whole brain, TE/TR 40 ms/2500 ms, total acquisition time 25 min (=598 volumes, one session). Instructions and pictures were shown with fMRI compatible video-goggles (Resonance Technologies, Northridge, CA, USA). Speech was digitally recorded beginning at the onset of each picture using an fMRI compatible microphone and saved digitally on a computer using Cool Edit Pro (Syntrillium Software Cop. Phoenix, Arizona). Head movement was minimized by using padded earphones fixating the head within the gradient insert coil.
Statistical Analysis and Image Analysis
Group differences of the behavioral attachment data were analyzed using the exact Mann-Whitney U-test and the Kruskal-Wallis H-test and (SPSS version 14). We used non-parametric tests because of the non-normal distribution of the dependent variables. Preprocessing and statistical analysis of fMRI data were carried out with SPM22 and MATLAB 6.1 (MathWorks, Natick, MA, USA). The first four functional images were discarded to account for equilibration effects. Individual functional images were corrected for motion artifacts by realignment to the first volume of each session. As noted earlier, we excluded four control subjects because of excessive head movement (>2 mm within a trial cycle) in order to minimize movement effects. Further preprocessing included spatial normalization (3 × 3 × 3 mm) and smoothing (FWHM 8 mm). The regression model for each subject was as follows: each of the nine pictures had three or two individual regressors with variable duration depending on the time of speech: Regressor 1, modeling the time from onset of picture till onset of speech; regressor 2, modeling the picture during speaking; and regressor 3, modeling the time from offset of speech till end of picture presentation (if the subject did talk for less than 2 min). Three more regressors were built, each modeling all nine pictures: Regressor 4, (onset of every single word of all pictures as a stick function); regressor 5, (instructions); and regressor 6, (all fixation crosses = base line). Regressors of interest were convolved with a function that modeled a prototypical hemodynamic response before inclusion into the regression model. A high-pass filter was set at a cutoff frequency of 240 s. Finally, six more regressors modeled residual motion. For each trial the variance of each voxel was estimated according to the General Linear Model Individual regionally specific effects of interest were calculated for each participant using linear contrasts, resulting in a t-statistic for every voxel.
The effects of interests in this study were narrative story responses to the seven attachment pictures. We calculated the contrast picture presentation for each subject during speech (regressor 2) + picture presentation before the subjects start to speak (regressor 1) vs. baseline (fixation cross), thereby including potential mental processes before the actual speaking phase starts. For each subject, contrasts for single pictures were calculated, that is, seven contrasts for the attachment pictures ordered 1–7.
A within subject repeated measures ANOVA with three groups (resolved healthy controls, unresolved healthy controls and unresolved BPD patients) and seven repeated measurements was calculated as a second level analysis in order to test for effects of group and attachment classification. The AAP is designed to activate the attachment system increasingly from picture 1–7. The contrast of interest within each group was labeled “AAP effect” (–3 –2 –1 0 1 2 3), in accordance with the results of our pilot study (Buchheim et al., 2006a). t-statistics for each voxel were set at a threshold of p < 0.001 uncorrected for multiple comparisons and a cluster threshold of p < 0.05. We allowed a small volume correction for regions of interest with family wise error correction of p < 0.05 for those regions for which we had a priori hypotheses (amygdala, DLPFC, dorsal anterior cingulate) using a radial sphere of 10 mm (amygdala) and 20 mm (DLPFC, dACC), respectively. Talairach and Tournoux (1988) and Duvernoy (1999) atlases were used to identify all brain areas.
Results
Behavioral Data
Borderline patients differed significantly from controls in all clinical scales (Table 1). As expected, the majority of the BPD patients were judged unresolved (11/13, 85%) in the AAP. Ten of seventeen (59%) controls were judged resolved and seven (41%) were judged as unresolved. In the fMRI data analysis, we included 11 patients (all coded as unresolved) and 17 controls (n = 7 unresolved, n = 10 organized: n = 6 secure, n = 4 dismissing, no preoccupied subjects). The overall distribution of attachment status differed significantly between borderline patients and controls (Fisher’s exact test, p = 0.026).
Neuroimaging Data
Both control and patient groups showed activations in bilateral occipital cortex, bilateral superior medial frontal cortex, bilateral precentral and left inferior frontal gyrus for the main effect of picture presentation and bilateral medial and superior temporal gyrus, bilateral precentral gyrus, medial occipital gyrus and cerebellum for the main effect of speech production.
The goal of the neuroimaging analysis was to examine the AAP effect (increasing attachment activation during the task) in control and borderline subjects. The first analysis examined the AAP effect for the control group. Three regions showed increasing activation during the task: right amygdala, right DLPFC and mPFC in the rostral cingulate zone (RCZ; Table 3). The second analysis compared all controls with all patients. We found a significantly stronger activation of the RCZ in the healthy controls and a significantly stronger activation of the right amygdala in the patient group. The third analysis examined these three regions in order to understand the contribution of attachment status and diagnosis to these activations. This analysis was performed by contrasting the three subgroups of our sample with each other (Figure 2).
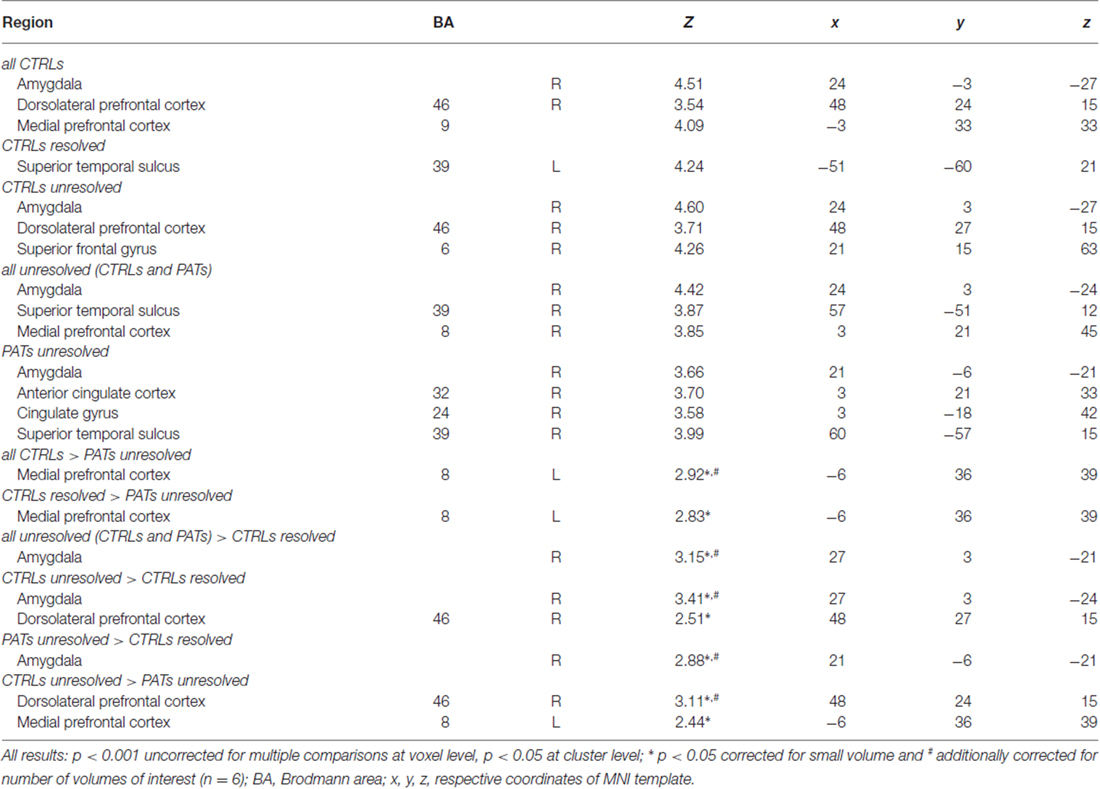
Table 3. fMRI results.
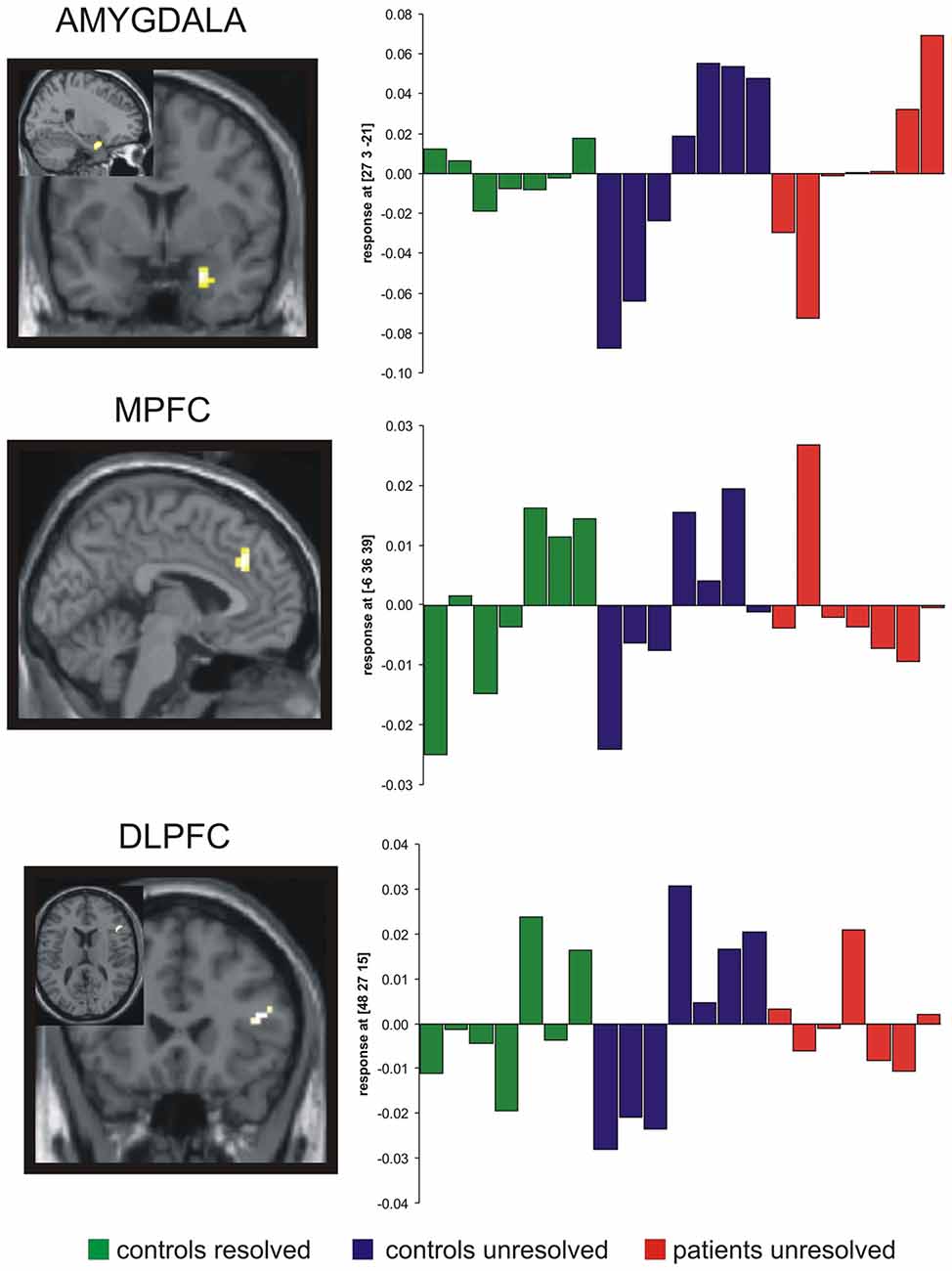
Figure 2. Results of the functional magnetic resonance imaging (fMRI) analysis. A significant AAP effect (increasing activation along the task) was found in the amygdala for both, unresolved controls and patients, but not in the resolved controls. A significant AAP effect in the medial PFC was observed in both control groups, whereas the dorsolateral prefrontal cortex (DLPFC) exhibits an AAP effect only in the group of unresolved controls. All regions were significant in the respective interaction analyses (see Table 3). Images of statistic parametric mapping are projected onto sections of the standard T1 template of SPM 2. Plots of contrast estimates for each condition were shown on the right. Green bars, resolved controls; blue bars, unresolved controls; red bars, unresolved patients.
The results of these analyses are shown in Table 3. An AAP effect was found in the amygdala in both unresolved groups (unresolved controls and unresolved BPD patients). An AAP effect in the RCZ was found only in the controls (resolved and unresolved). An AAP effect in the right DLPFC was found only in the unresolved controls.
In order to check that our results are not solely due to medication effects, we performed an additional analysis including only patients taking no psychotropic drugs (n = 6). Results were the same: all CTRLs > unmedicated PATs unresolved: mPFC (−9, 36, −39, Z = 3.63); CTRLs resolved > unmedicated PATs unresolved: mPFC (−9, 36, −39, Z = 3.54); unmedicated PATs unresolved > CTRLs resolved: Amygdala (21, −6, −21, Z = 3.39); CTRLs unresolved > unmedicated PATs unresolved: DLPFC (48, 24, 15, z = 2.53).
Discussion
The present study examined the neural correlates of attachment dysregulation in a group of BPD patients compared to controls. This study used a paradigm that evaluated neural response patterns while subjects told attachment stories in response to AAP stimuli in the fMRI scanner. The fMRI analysis model followed the logic of the design of the attachment measure. According to this logic, the picture presentation sequence increasingly activates the attachment distress. We labeled this increasing activation over the course of task as “AAP effect.” Due to the fact that almost all BDP patients were classified as unresolved, we investigated only three classification groups: resolved controls, unresolved controls and unresolved BDP patients. There were three main imaging finding. First, all unresolved subjects (borderline and controls), but not the resolved controls, showed the AAP effect reflected in an increasing amygdala activation. Second, all controls (resolved and unresolved), but not the unresolved patients, showed the AAP effect in relation to increasing activation of the RCZ. Third, only the unresolved controls showed an AAP effect of increasing activation of the right DLPFC. This effect was not found in the resolved controls or the unresolved patients. We now discuss these results in the context of attachment research.
The predominant unresolved classification in the BPD patients was consistent with previous research (Fonagy et al., 2000; Agrawal et al., 2004; Bakermans-Kranenburg and van IJzendoorn, 2009; Buchheim and George, 2011). This was found using two independent attachment measures (AAI and AAP). How are these attachment findings related to the neural patterns found in the three groups (unresolved patients, unresolved and resolved controls)?
As shown in Figure 2, the AAP effect was present in the right amygdala in both unresolved groups. This finding strengthens the results of our pilot study with healthy subjects (Buchheim et al., 2006a). Amygdala activation has been found in other studies to be associated with a range of negative and positive emotional stimuli (Davis and Whalen, 2001). A recent study by White et al. (2014) demonstrated that the amygdala is responsive to animate and emotional stimuli. Moreover, the authors consider that the interaction between the various functions of the amygdala may need to be taken into account simultaneously to fully understand how they interact. Although amygdala activity has been suggested to be modulated by affective and non-affective factors, there is considerable controversy regarding its specific functional nature. Costafreda et al. (2008) examined the effects of experimental characteristics on the probability of detecting amygdala activity in a meta-analysis of 385 functional neuroimaging studies of emotional processing. The authors reported that all emotional stimuli were related to higher probability of amygdala activity than neutral stimuli. Comparable effects were detected for most negative and positive emotions, however there was a higher probability of activation for fear and disgust as compared to happiness (Costafreda et al., 2008). The stimuli used in the present study were not general emotional stimuli. The AAP picture stimuli were selected specifically because of their ability to activate attachment distress by introducing themes like, e.g., separation, loneliness, danger or loss. Therefore, we interpret this amygdala activation as a neural correlate of negative emotional arousal that is associated with dysregulated attachment fear that is evident in the unresolved verbatim narratives. In contrast, resolved controls do not show the AAP effect in the amygdala. Resolved attachment is defined by the ability to re-organize attachment related fearful and threatening themes emerging in their stories. This re-organization appears to have blocked the AAP effect in the amygdala. Attachment activation of resolved controls, therefore, is not dysregulated by the negative emotions associated with distress.
Increased amygdala activation in BPD patients has been found in a variety of passive stimulation paradigms and these findings are interpreted as heightened emotional sensitivity to aversive stimuli (Davis and Whalen, 2001; Herpertz et al., 2001; Donegan et al., 2003; Silbersweig et al., 2007; Hazlett et al., 2012; Kamphausen et al., 2013; Schulze et al., 2016). Our results are consistent with these findings. Moreover, they provide an empirical link to the frequently reported unresolved attachment found in BPD samples, as mentioned before (Agrawal et al., 2004; Bakermans-Kranenburg and van IJzendoorn, 2009; Buchheim and George, 2011). As the amygdala activation AAP effect was found in both our BPD and unresolved controls, the effect is likely to be related to adverse early experiences that are not necessarily specific to BPD diagnosis. In order to disentangle the contribution of attachment and diagnosis, it would be desirable to include a resolved BPD group. This was not possible in the current study because the small number of resolved BDP patients precluded such an analysis.
The RCZ showed the AAP effect in both control groups, resolved or unresolved. Studies in humans showed that the RCZ (the posterior MFC border zone between the medial areas BA8, BA6 and BA32’ with some extension into BA24’) is involved in monitoring for unfavorable outcomes, performance and conflict monitoring, and decision uncertainty (Carter et al., 1998; Botvinick et al., 1999; Ridderinkhof et al., 2004; Fan et al., 2008; Nee et al., 2011). A recent comprehensive review discussed the diverse functions of the RCZ and proposed that this diversity can be understood in terms of the allocation of control based on monitoring the expected value of control (Shenhav et al., 2013). Although a subgroup of the healthy participants showed the failure to reorganize their attachment distress in their narratives on a behavioral level (unresolved), they demonstrated the ability to control their distress on a neural level. As the attachment stories in our study include distressing and potentially threatening themes, one possible interpretation of this activation is that all control subjects monitored their stories for unfavorable outcomes, that is, how the story might continue (part of the instruction). This monitoring function seems to be impaired in the BPD patients of our sample. An alternative interpretation is that activation in this region simply reflects emotional involvement. However, this is unlikely given that the three groups showed a different pattern.
The AAP effect in the DLPFC was found only in the unresolved control group; it was not observed in the resolved controls or the unresolved patients. The right DLPFC has been described as being involved in cognitive control (Duncan and Owen, 2000), emotion regulation (Ochsner and Gross, 2005), and more generally in executive functions, regulatory mechanisms that help individuals cope with extraordinary affordances. Recent research findings suggested a regulatory hierarchy, whereby the DLPFC and areas of the anterior medio-PFC modulate the cingulate, which in turn modulates the amygdala and further subcortical areas (Meyer-Lindenberg et al., 2005; Buckholtz et al., 2007). Several neuroimaging studies described a dysfunction of the right DLPFC in BPD patients (De La Fuente et al., 1997; Soloff et al., 2000; Schmahl et al., 2003). One recent study reported that cortical thickness in the DLPFC of female BPD patients without PTSD correlated positively with emotion regulation scores, which was also positively associated with amygdala volume, as well as cortical thickness of the insula (Bruehl et al., 2013). These findings suggested possible compensatory mechanisms for the impaired emotion regulation. Resolved subjects in the present study demonstrated a low incidence of threatening situations in their narratives, suggesting that the cognitive control system was not increasingly engaged over the course of the task. Unresolved controls, however, had increasing affective involvement. We, therefore, interpret the accompanying right DLPFC activation as an effort in this group to cope with this increasing affective involvement.
BPD patients were showing the highest proportion of unresolved attachment patterns in this sample. The fMRI findings suggest that they were neither able to recruit the DLPFC (cognitive control) nor the RCZ (conflict monitoring) while being emotionally overwhelmed, as reflected in the enhanced amygdala activation. However this finding contrasts with some published neuroimaging studies of affective dysregulation in BPD, which used passive stimulation. Studies on functional correlates of response inhibition have demonstrated further evidence for functional impairments of prefrontal areas, particularly of the DLPFC, the rostral ACC, and the orbitofrontal cortex (OFC). Minzenberg et al. (2007) used for example an implicit affect regulation task (responses to threatening vs. neutral faces) and found specifically enhanced neural activation of the right amygdala in BPD along with attenuated activations of the rostral ACC. Although our interpretation of the different activation patterns shown in Figure 2 cannot be directly proven, we suggest that we provided a novel and interesting approach to understanding emotional instability in BPD patients with respect to attachment on a neural basis. The participants in our task were actively talking about their subjective perception of attachment scenes reflecting their individual mental organization of these crucial topics in relation to their history of abuse, maltreatment and emotional neglect.
Limitations
There are several limitations to our study that need to be taken into account when interpreting our findings. First, the number of resolved BPD patients (n = 2) was too small to include in our analysis and moreover we were not able to recruit a larger sample of BPD patients willing to participate in such a demanding paradigm (talking in the fMRI scanner), which limits the generalization of our results. The attachment literature suggests, that unresolved attachment is the predominant classification group, therefore future research would require a substantially large sample in order to include resolved BPD subjects. Although this limits the interpretation of our data to a certain extent, we were able to meaningfully evaluate the results using the three-group designations afforded by the participant attachment distribution in the current study.
Second, we did not include a clinical control group. This leads to questions as to whether our results may also be present in patients with other psychiatric disorders and not specific to BPD.
Third, 5 out of 11 of the BPD subjects were under low dose medication. This could be a confounding factor in comparing patients and controls, although our control analyses of medication-free patients only speaks against this assumption.
Fourth, this study aimed to characterize differences between healthy participants and BPD patients using an attachment paradigm along the AAP system focusing on attachment related pictures only. Since this study has identified differences between controls and patients, it is rather difficult to interpret the data univocally in the absence of an adequate control stimulus set, which is the focus of a recent study with healthy controls (Labek et al., 2016). Moreover, it would have been appropriate to add an established emotion-inducing paradigm for comparing neural responses to attachment plus to emotional involvement and/or emotional regulation capacities. Strictly spoken without this contrasting paradigm we may not directly conclude that we have investigated emotional dysregulation in BPD patients compared to controls.
Fifth, all results were derived from the three group analyses. However, this might have inflated statistical results. Therefore, we also calculated separate analyses for those contrasts where only two groups were involved. All results remain significant, showing that increased degrees of freedom did not generally inflate our results. Only mPFC activation in the contrast comparing resolved controls and unresolved patients does not surpass additional small volume correction.
Finally, overt speech in the scanner always is accompanied with head movements. The head movement in this study was less than 2 mm, and we took steps to eliminate residual influences. These included dropping subjects, including movement parameters as a covariate of no interest, and modeling the onset of every spoken word.
Conclusions
Unresolved controls, but not patients, showed activation in the right DLPFC and the RCZ. We interpreted this as a neural signature of BPD patients’ inability to exert top-down control under conditions of attachment distress. These findings point to possible neural mechanisms for underlying affective dysregulation in BPD in the context of attachment trauma and fear. We found that both increased emotional sensitivity, as well as impaired emotion regulation, may have contributed to affective dysregulation in unresolved BPD patients. Increased emotional sensitivity, as evidenced by an AAP effect in the right amygdala, might be explained in large part by their attachment pattern. An alteration of the cognitive control system (RCZ and right DLPFC) is found when unresolved attachment and diagnosis of BDP are present simultaneously. Modulation of BPD patients’ responses in attachment situations during treatment and psychotherapy to patterns similar to those described in the control group might be an important indication of their increasing capacity to regulate attachment distress and to show sufficient cognitive control (Perez et al., 2016). Future studies may examine as to what extent psychotherapy has the potential to change brain activation from a more unresolved to a more resolved pattern.
Author Contributions
The study was conceptualized by HW, AB, SE, CG, HK and MS. The study setup and data collection were organized and conducted by HW, AB, SE, MS, HK and PM. fMRI analyses was performed by HW and SE. Coding of attachment interviews were conducted by AB and CG. SE, HW and DP performed the statistical data analysis and contributed substantially to the result interpretation. HW, AB, SE, CG, and DP provided important intellectual contribution in commenting and revising the manuscript. AB, HW, SE, and CG wrote the manuscript and edited its final version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Edgar Schilly and Marco Jahn, Department of Psychiatry, University of Ulm, for technical assistance in fMRI data analysis, Kathrin Brändle, Department of Psychiatry and retain Department of Diagnostic Radiology, University of Ulm for assistance in fMRI-acquisition, Dipl.-Psych. Claudia Simons and Justice Krampen, Department of Psychosomatic Medicine and Psychotherapy, University of Ulm for translating the German transcripts into English. We thank Dipl.-Psych Dagmar Pape, Munich, for administering the Adult Attachment Interviews in the hospital and Prof. Dr. Fabienne Becker-Stoll, Munich, a certified judge, for classifying the Adult Attachment Interviews.
Abbreviations
AAI, Adult Attachment Interview; ACC, anterior cingulate cortex; AAP, Adult Attachment Projective Picture System; BA, Brodmann area; BPD, Borderline personality disorder; CTR, controls; DLPFC, dorsolateral prefrontal cortex; IPDE, International Personality Disorder Examination; mPFC, medial prefrontal cortex; OFC, orbitofrontal cortex; PAT, patients; PFC, prefrontal cortex; PTSD, posttraumatic stress disorder; RCZ, rostral cingulate zone; SCID-I, Structured Clinical Interview for DSM-IV.
Footnotes
- ^ PM has been trained and certified for reliable diagnosis in the SCID-rating by Prof. Wittchen, Munich, Germany and by A. Loranger MD, New York, NY, USA regarding IPDE. In seven patients an experienced Master’s level psychologist conducted a second SCID interview. Agreement between the raters was κ = 1.0 for both BPD and lifetime depressive episode.
- ^ www.fil.ion.ucl.ac.uk
References
Agrawal, H. R., Gunderson, J., Holmes, B. M., and Lyons-Ruth, K. (2004). Attachment studies with borderline patients: a review. Harv. Rev. Psychiatry 12, 94–104. doi: 10.1080/10673220490447218
Bakermans-Kranenburg, M. J., and van IJzendoorn, M. H. (2009). The first 10,000 adult attachment interviews: distributions of adult attachment representations in clinical and non-clinical groups. Attach. Hum. Dev. 11, 223–263. doi: 10.1080/14616730902814762
Bandelow, B., Krause, J., Wedekind, D., Broocks, A., Hajak, G., and Rüther, E. (2005). Early traumatic life events, parental attitudes, family history and birth risk factors in patients with borderline personality disorder and healthy controls. Psychiatry Res. 134, 169–179. doi: 10.1016/j.psychres.2003.07.008
Bartels, A., and Zeki, S. (2000). The neural basis of romantic love. Neuroreport 11, 3829–3834. doi: 10.1097/00001756-200011270-00046
Bartels, A., and Zeki, S. (2004). The neural correlates of maternal and romantic love. Neuroimage 21, 1155–1166. doi: 10.1016/j.neuroimage.2003.11.003
Beblo, T., Driessen, M., Mertens, M., Wingenfeld, K., Piefke, M., Rullkoetter, N., et al. (2006). Functional MRI correlates of the recall of unresolved life events in borderline personality disorder. Psychol. Med. 36, 845–856. doi: 10.1017/S0033291706007227
Botvinick, M. M., Nystrom, L. E., Fissell, K., Carter, C. S., and Cohen, J. D. (1999). Conflict monitoring versus selection for action in anterior cingulate cortex. Nature 402, 179–181. doi: 10.1038/46035
Bruehl, H., Preiβ, S., Heuser, I., Heekeren, H. R., Roepke, S., and Dziobek, I. (2013). Increased prefrontal cortical thickness is associated with enhanced abilities to regulate emotions in PTSD-free women with borderline personality disorder. PLoS One 8:e65584. doi: 10.1371/journal.pone.0065584
Brüne, M., Walden, S., Edel, M. A., and Dimaggio, G. (2016). Mentalization of complex emotions in borderline personality disorder: the impact of parenting and exposure to trauma on the performance in a novel cartoon-based task. Compr. Psychiatry 64, 29–37. doi: 10.1016/j.comppsych.2015.08.003
Buchheim, A., Erk, S., George, C., Kächele, H., Martius, P., Pokorny, D., et al. (2008). Neural correlates of attachment dysregulation in borderline personality disorder using functional magnetic resonance imaging. Psychiatr. Res. 163, 223–235. doi: 10.1016/j.pscychresns.2007.07.001
Buchheim, A., Erk, S., George, C., Kächele, H., Ruchsow, M., Spitzer, M., et al. (2006a). Measuring attachment representation in an fMRI environment: a pilot study. Psychopathology 39, 144–152. doi: 10.1159/000091800
Buchheim, A., George, C., Kächele, H., Erk, S., and Walter, H. (2006b). Measuring adult attachment representation in an fMRI environment: concepts and assessment. Psychopathology 39, 136–143. doi: 10.1159/000091799
Buchheim, A., and George, C. (2011). “Attachment disorganization in borderline personality disorder and anxiety disorder,” in Disorganized Attachment and Caregiving, eds J. Solomon and C. George (New York, NY: Guilford Press), 343–382.
Buchheim, A., Roth, G., Schiepek, G., Pogarell, O., and Karch, S. (2013). Neurobiology of borderline personality disorder (BPD) and antisocial personality disorder (APD). Swiss Arch. Neurol. Psychiatry 164, 115–122.
Buckholtz, J. W., Sust, S., Tan, H. Y., Mattay, V. S., Straub, R. E., Meyer-Lindenberg, A., et al. (2007). fMRI evidence for functional epistasis between COMT and RGS4. Mol. Psychiatry 12, 893–895, 885. doi: 10.1038/sj.mp.4002008
Carter, C. S., Braver, T. S., Barch, D. M., Botvinick, M. M., Noll, D., and Cohen, J. D. (1998). Anterior cingulate cortex, error detection and the online monitoring of performance. Science 280, 747–749. doi: 10.1126/science.280.5364.747
Coan, J. A., Schaefer, H. S., and Davidson, R. J. (2006). Lending a hand: social regulation of the neural response to threat. Psychol. Sci. 17, 1032–1039. doi: 10.1111/j.1467-9280.2006.01832.x
Conklin, C. Z., Bradley, R., and Westen, D. (2006). Affect regulation in borderline personality disorder. J. Nerv. Ment. Dis. 194, 69–77. doi: 10.1097/01.nmd.0000198138.41709.4f
Costafreda, S. G., Brammer, M. J., David, A. S., and Fu, C. H. (2008). Predictors of amygdala activation during the processing of emotional stimuli: a meta-analysis of 385 PET and fMRI studies. Brain Res. Rev. 58, 57–70. doi: 10.1016/j.brainresrev.2007.10.012
Davis, M., and Whalen, P. J. (2001). The amygdala: vigilance and emotion. Mol. Psychiatry 6, 13–34. doi: 10.1038/sj.mp.4000812
De La Fuente, J. M., Goldman, S., Stanus, E., Vizuete, C., Morlán, I., Bobes, J., et al. (1997). Brain glucose metabolism in borderline personality disorder. J. Psychiatr. Res. 31, 531–541. doi: 10.1016/s0022-3956(97)00001-0
Donegan, N. H., Sanislow, C. A., Blumberg, H. P., Fulbright, R. K., Lacadie, C., Skudlarski, P., et al. (2003). Amygdala hyperreactivity in borderline personality disorder: implications for emotional dysregulation. Biol. Psychiatry 54, 1284–1293. doi: 10.1016/s0006-3223(03)00636-x
Driessen, M., Herrmann, J., Stahl, K., Zwaan, M., Meier, S., Hill, A., et al. (2000). Magnetic resonance imaging volumes of the hippocampus and the amygdala in women with borderline personality disorder and early traumatization. Arch. Gen. Psychiatry 57, 1115–1122. doi: 10.1001/archpsyc.57.12.1115
Driessen, M., Wingenfeld, K., Rullkoetter, N., Mensebach, C., Woermann, F. G., Mertens, M., et al. (2009). One-year functional magnetic resonance imaging follow-up study of neural activation during the recall of unresolved negative life events in borderline personality disorder. Psychol. Med. 39, 507–516. doi: 10.1017/s0033291708003358
Duncan, J., and Owen, A. M. (2000). Common regions of the human frontal lobe recruited by diverse cognitive demands. Trends Neurosci. 23, 475–483. doi: 10.1016/s0166-2236(00)01633-7
Enzi, B., Doering, S., Faber, C., Hinrichs, J., Bahmer, J., and Northoff, G. (2013). Reduced deactivation in reward circuitry and midline structures during emotion processing in borderline personality disorder. World J. Biol. Psychiatry 14, 45–56. doi: 10.3109/15622975.2011.579162
Fan, J., Hof, P. R., Guise, K. G., Fossella, J. A., and Posner, M. I. (2008). The functional integration of the anterior cingulate cortex during conflict processing. Cereb. Cortex 18, 796–805. doi: 10.1093/cercor/bhm125
Fearon, R. M., and Mansell, W. (2001). Cognitive perspectives on unresolved loss: insights from the study of PTSD. Bull. Menninger Clin. 65, 380–396. doi: 10.1521/bumc.65.3.380.19845
Fonagy, P., Target, M., and Gergely, G. (2000). Attachment and borderline personality disorder. A theory and some evidence. Psychiatr. Clin. North Am. 23, 103–122, vii–viii. doi: 10.1016/S0193-953X(05)70146-5
Frías, Á., Palma, C., Farriols, N., and González, L. (2016). Sexuality-related issues in borderline personality disorder: a comprehensive review. Personal. Ment. Health doi: 10.1002/pmh.1330 [Epub ahead of print].
George, C., Kaplan, N., and Main, M. (1984/1985/1996). The Adult Attachment Interview (Unpublished Manuscript). Berkeley: University of California.
George, C., and West, M. (2001). The development and preliminary validation of a new measure of adult attachment: the adult attachment projective. Attach. Hum. Dev. 3, 30–61. doi: 10.1080/14616730010024771
George, C., and West, M. (2003). “The adult attachment projective: measuring individual differences in attachment security using projective methodology,” in Comprehensive Handbook of Psychological Assessment, ed. M. Hilsenroth (New Jersey, NJ: Wiley and Sons), 431–448.
George, C., and West, M. L. (2012). The Adult Attachment Projective Picture System: Attachment Theory and Assessment in Adults. New York, NY: Guilford Press.
George, C., West, M., and Pettem, O. (1999). “The adult attachment projective: disorganization of adult attachment at the level of representation,” in Attachment Disorganization, eds J. Solomon and C. George (New York, NY: Guilford), 462–507.
Gillath, O., Bunge, S. A., Shaver, P. R., Wendelken, C., and Mikulincer, M. (2005). Attachment-style differences in the ability to suppress negative thoughts: exploring the neural correlates. Neuroimage 28, 835–847. doi: 10.1016/j.neuroimage.2005.06.048
Gunderson, J. G., Daversa, M. T., Grilo, C. M., McGlashan, T. H., Zanarini, M. C., Shea, M. T., et al. (2006). Predictors of 2-year outcome for patients with borderline personality disorder. Am. J. Psychiatry 163, 822–826. doi: 10.1176/appi.ajp.163.5.822
Gunderson, J. G., and Lyons-Ruth, K. (2008). BPD’s interpersonal hypersensitivity phenotype: a gene-environment-developmental model. J. Pers. Disord. 22, 22–41. doi: 10.1521/pedi.2008.22.1.22
Hazlett, E. A., Zhang, J., New, A. S., Zelmanova, Y., Goldstein, K. E., Haznedar, M. M., et al. (2012). Potentiated amygdala response to repeated emotional pictures in borderline personality disorder. Biol. Psychiatry 72, 448–456. doi: 10.1016/j.biopsych.2012.03.027
Herpertz, S. C., and Bertsch, K. (2015). A new perspective on the pathophysiology of borderline personality disorder: a model of the role of oxytocin. Am. J. Psychiatry 172, 840–851. doi: 10.1176/appi.ajp.2015.15020216
Herpertz, S. C., Dietrich, T. M., Wenning, B., Krings, T., Erberich, S. G., Willmes, K., et al. (2001). Evidence of abnormal amygdala functioning in borderline personality disorder: a functional MRI study. Biol. Psychiatry 50, 292–298. doi: 10.1016/s0006-3223(01)01075-7
Hoerst, M., Weber-Fahr, W., Tunc-Skarka, N., Ruf, M., Bohus, M., Schmahl, C., et al. (2010). Metabolic alterations in the amygdala in borderline personality disorder: a proton magnetic resonance spectroscopy study. Biol. Psychiatry 67, 399–405. doi: 10.1016/j.biopsych.2009.09.030
Irle, E., Lange, C., and Sachsse, U. (2005). Reduced size and abnormal asymmetry of parietal cortex in women with borderline personality disorder. Biol. Psychiatry 57, 173–182. doi: 10.1016/j.biopsych.2004.10.004
Joubert, D., Webster, L., and Hackett, R. K. (2012). Unresolved attachment status and trauma-related symptomatology in maltreated adolescents: an examination of cognitive mediators. Child Psychiatry Hum. Dev. 43, 471–483. doi: 10.1007/s10578-011-0276-8
Kamphausen, S., Schröder, P., Maier, S., Bader, K., Feige, B., Kaller, C. P., et al. (2013). Medial prefrontal dysfunction and prolonged amygdala response during instructed fear processing in borderline personality disorder. World J. Biol. Psychiatry 14, 307–318, S301–304. doi: 10.3109/15622975.2012.665174
Keinänen, M. T., Johnson, J. G., Richards, E. S., and Courtney, E. A. (2012). A systematic review of the evidence based psychosocial risk factors for understanding of borderline personality disorder. Psychoanal. Psychother. 26, 65–91. doi: 10.1080/02668734.2011.652659
Labek, K., Viviani, R., Gizewski, E. R., Verius, M., and Buchheim, A. (2016). Neural correlates of the appraisal of attachment scenes in healthy controls and social cognition—an fMRI study. Front. Hum. Neurosci. 10:345. doi: 10.3389/fnhum.2016.00345
Landis, J. R., and Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics 33, 159–174. doi: 10.2307/2529310
Lang, S., Kotchoubey, B., Frick, C., Spitzer, C., Grabe, H. J., and Barnow, S. (2012). Cognitive reappraisal in trauma-exposed women with borderline personality disorder. Neuroimage 59, 1727–1734. doi: 10.1016/j.neuroimage.2011.08.061
Leibenluft, E., Gobbini, M. I., Harrison, T., and Haxby, J. V. (2004). Mothers’ neural activation in response to pictures of their children and other children. Biol. Psychiatry 56, 225–232. doi: 10.1016/j.biopsych.2004.05.017
Leichsenring, F., Leibing, E., Kruse, J., New, A. S., and Leweke, F. (2011). Borderline personality disorder. Lancet 377, 74–84. doi: 10.1016/S0140-6736(10)61422-5
Lenzi, D., Trentini, C., Pantano, P., Macaluso, E., Iacoboni, M., Lenzi, G. L., et al. (2009). Neural basis of maternal communication and emotional expression processing during infant preverbal stage. Cereb. Cortex 19, 1124–1133. doi: 10.1093/cercor/bhn153
Lieb, K., Zanarini, M. C., Schmahl, C., Linehan, M. M., and Bohus, M. (2004). Borderline personality disorder. Lancet 364, 453–461. doi: 10.1016/S0140-6736(04)16770-6
Linehan, M. M., Tutek, D. A., Heard, H. L., and Armstrong, H. E. (1994). Interpersonal outcome of cognitive behavioral treatment for chronically suicidal borderline patients. Am. J. Psychiatry 151, 1771–1776. doi: 10.1176/ajp.151.12.1771
Lyons-Ruth, K., and Jacobvitz, D. (2008). “Attachment disorganization: unresolved loss, relational violence and lapses in behavioral and attentional strategies,” in Handbook of Attachment: Theory, Research and Clinical Applications, 2nd Edn. eds J. Cassidy and P. R. Shaver (New York, NY: Guilford Press), 666–697.
Main, M., and Goldwyn, R. (1995). Adult Attachment Classification System (Unpublished Manuscript). Berkeley, CA: University of California.
Mensebach, C., Beblo, T., Driessen, M., Wingenfeld, K., Mertens, M., Rullkoetter, N., et al. (2009). Neural correlates of episodic and semantic memory retrieval in borderline personality disorder: an fMRI study. Psychiatry Res. 171, 94–105. doi: 10.1016/j.pscychresns.2008.02.006
Meyer-Lindenberg, A., Kohn, P. D., Kolachana, B., Kippenhan, S., Mcinerney-Leo, A., Nussbaum, R., et al. (2005). Midbrain dopamine and prefrontal function in humans: interaction and modulation by COMT genotype. Nat. Neurosci. 8, 594–596. doi: 10.1038/nn1438
Milrod, B., Markowitz, J. C., Gerber, A. J., Cyranowski, J., Altemus, M., Shapiro, T., et al. (2014). Childhood separation anxiety and the pathogenesis and treatment of adult anxiety. Am. J. Psychiatry 171, 34–43. doi: 10.1176/appi.ajp.2013.13060781
Minzenberg, M. J., Fan, J., New, A. S., Tang, C. Y., and Siever, L. J. (2007). Fronto-limbic dysfunction in response to facial emotion in borderline personality disorder: an event-related fMRI study. Psychiatry Res. 155, 231–243. doi: 10.1016/j.pscychresns.2007.03.006
Mitchell, A. E., Dickens, G. L., and Picchioni, M. M. (2014). Facial emotion processing in borderline personality disorder: a systematic review and meta-analysis. Neuropsychol. Rev. 24, 166–184. doi: 10.1007/s11065-014-9254-9
Mosquera, D., Gonzalez, A., and Leeds, A. M. (2014). Early experience, structural dissociation and emotional dysregulation in borderline personality disorder: the role of insecure and disorganized attachment. Borderline Personal. Disord. Emot. Dysregul. 1:15. doi: 10.1186/2051-6673-1-15
Nakash-Eisikovits, O., Dutra, L., and Westen, D. (2002). Relationship between attachment patterns and personality pathology in adolescents. J. Am. Acad. Child Adolesc. Psychiatry 41, 1111–1123. doi: 10.1097/00004583-200209000-00012
Nee, D. E., Kastner, S., and Brown, J. W. (2011). Functional heterogeneity of conflict, error, task-switching and unexpectedness effects within medial prefrontal cortex. Neuroimage 54, 528–540. doi: 10.1016/j.neuroimage.2010.08.027
Nitschke, J. B., Nelson, E. E., Rusch, B. D., Fox, A. S., Oakes, T. R., and Davidson, R. J. (2004). Orbitofrontal cortex tracks positive mood in mothers viewing pictures of their newborn infants. Neuroimage 21, 583–592. doi: 10.1016/j.neuroimage.2003.10.005
Ochsner, K. N., and Gross, J. J. (2005). The cognitive control of emotion. Trends. Cogn. Sci. 9, 242–249. doi: 10.1016/j.tics.2005.03.010
O’Neill, A., D’Souza, A., Carballedo, A., Joseph, S., Kerskens, C., and Frodl, T. (2013). Magnetic resonance imaging in patients with borderline personality disorder: a study of volumetric abnormalities. Psychiatry Res. 213, 1–10. doi: 10.1016/j.pscychresns.2013.02.006
O’Neill, A., and Frodl, T. (2012). Brain structure and function in borderline personality disorder. Brain Struct. Funct. 217, 767–782. doi: 10.1007/s00429-012-0379-4
Perez, D. L., Vago, D. R., Pan, H., Root, J., Tuescher, O., Fuchs, B. H., et al. (2016). Frontolimbic neural circuit changes in emotional processing and inhibitory control associated with clinical improvement following transference-focused psychotherapy in borderline personality disorder. Psychiatry Clin. Neurosci. 70, 51–61. doi: 10.1111/pcn.12357
Putnam, K. M., and Silk, K. R. (2005). Emotion dysregulation and the development of borderline personality disorder. Dev. Psychopathol. 17, 899–925. doi: 10.1017/s0954579405050431
Ridderinkhof, K. R., van den Wildenberg, W. P., Segalowitz, S. J., and Carter, C. S. (2004). Neurocognitive mechanisms of cognitive control: the role of prefrontal cortex in action selection, response inhibition, performance monitoring and reward-based learning. Brain Cogn. 56, 129–140. doi: 10.1016/j.bandc.2004.09.016
Riem, M. M., Bakermans-Kranenburg, M. J., van IJzendoorn, M. H., Out, D., and Rombouts, S. A. (2012). Attachment in the brain: adult attachment representations predict amygdala and behavioral responses to infant crying. Attach. Hum. Dev. 14, 533–551. doi: 10.1080/14616734.2012.727252
Rossi, R., Lanfredi, M., Pievani, M., Boccardi, M., Beneduce, R., Rillosi, L., et al. (2012). Volumetric and topographic differences in hippocampal subdivisions in borderline personality and bipolar disorders. Psychiatry Res. 203, 132–138. doi: 10.1016/j.pscychresns.2011.12.004
Ruocco, A. C., Amirthavasagam, S., Choi-Kain, L. W., and McMain, S. F. (2013). Neural correlates of negative emotionality in borderline personality disorder: an activation-likelihood-estimation meta-analysis. Biol. Psychiatry 73, 153–160. doi: 10.1016/j.biopsych.2012.07.014
Scherpiet, S., Brühl, A. B., Opialla, S., Roth, L., Jäncke, L., and Herwig, U. (2014). Altered emotion processing circuits during the anticipation of emotional stimuli in women with borderline personality disorder. Eur. Arch. Psychiatry Clin. Neurosci. 264, 45–60. doi: 10.1007/s00406-013-0444-x
Schmahl, C. G., Berne, K., Krause, A., Kleindienst, N., Valerius, G., Vermetten, E., et al. (2009). Hippocampus and amygdala volumes in patients with borderline personality disorder with or without posttraumatic stress disorder. J. Psychiatry Neurosci. 34, 289–295.
Schmahl, C. G., Elzinga, B. M., Vermetten, E., Sanislow, C., McGlashan, T. H., and Bremner, J. D. (2003). Neural correlates of memories of abandonment in women with and without borderline personality disorder. Biol. Psychiatry 54, 142–151. doi: 10.1016/s0006-3223(02)01720-1
Schmahl, C. G., Herpertz, S. C., Bertsch, K., Ende, G., Flor, H., Kirsch, P., et al. (2014). Mechanisms of disturbed emotion processing and social interaction in borderline personality disorder: state of knowledge and research agenda of the German clinical research unit. Borderline Personal. Disord. Emot. Dysregul. 1:12. doi: 10.1186/2051-6673-1-12
Schmahl, C. G., Vermetten, E., Elzinga, B. M., and Bremner, J. D. (2004). A positron emission tomography study of memories of childhood abuse in borderline personality disorder. Biol. Psychiatry 55, 759–765. doi: 10.1016/j.biopsych.2003.11.007
Schulze, L., Domes, G., Krüger, A., Berger, C., Fleischer, M., Prehn, K., et al. (2011). Neuronal correlates of cognitive reappraisal in borderline patients with affective instability. Biol. Psychiatry 69, 564–573. doi: 10.1016/j.biopsych.2010.10.025
Schulze, L., Schmahl, C., and Niedtfeld, I. (2016). Neural correlates of disturbed emotion processing in borderline personality disorder: a multimodal meta-analysis. Biol. Psychiatry 79, 97–106. doi: 10.1016/j.biopsych.2015.03.027
Scott, L. N., Levy, K. N., and Pincus, A. L. (2009). Adult attachment, personality traits and borderline personality disorder features in young adults. J. Pers. Disord. 23, 258–280. doi: 10.1521/pedi.2009.23.3.258
Shenhav, A., Botvinick, M. M., and Cohen, J. D. (2013). The expected value of control: an integrative theory of anterior cingulate cortex function. Neuron 79, 217–240. doi: 10.1016/j.neuron.2013.07.007
Silbersweig, D., Clarkin, J. F., Goldstein, M., Kernberg, O. F., Tuescher, O., Levy, K. N., et al. (2007). Failure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder. Am. J. Psychiatry 164, 1832–1841. doi: 10.1176/appi.ajp.2007.06010126
Skodol, A. E., Siever, L. J., Livesley, W. J., Gunderson, J. G., Pfohl, B., and Widiger, T. A. (2002). The borderline diagnosis II: biology, genetics and clinical course. Biol. Psychiatry 51, 951–963. doi: 10.1016/s0006-3223(02)01325-2
Soloff, P. H., Meltzer, C. C., Greer, P. J., Constantine, D., and Kelly, T. M. (2000). A fenfluramine-activated FDG-PET study of borderline personality disorder. Biol. Psychiatry 47, 540–547. doi: 10.1016/s0006-3223(99)00202-4
Soloff, P. H., White, R., Omari, A., Ramaseshan, K., and Diwadkar, V. A. (2015). Affective context interferes with brain responses during cognitive processing in borderline personality disorder: fMRI evidence. Psychiatry Res. 233, 23–35. doi: 10.1016/j.pscychresns.2015.04.006
Talairach, J., and Tournoux, P. (1988). Co-Planar Stereotactic Atlas of the Human Brain. Stuttgart: Thieme.
van Elst, L. T., Hesslinger, B., Thiel, T., Geiger, E., Haegele, K., Lemieux, L., et al. (2003). Frontolimbic brain abnormalities in patients with borderline personality disorder: a volumetric magnetic resonance imaging study. Biol. Psychiatry 54, 163–171. doi: 10.1016/s0006-3223(02)01743-2
van Elst, L. T., Thiel, T., Hesslinger, B., Lieb, K., Bohus, M., Hennings, J., et al. (2001). Subtle prefrontal neuropathology in a pilot magnetic resonance spectroscopy study in patients with borderline personality disorder. J. Neuropsychiatry Clin. Neurosci. 13, 511–514. doi: 10.1176/appi.neuropsych.13.4.511
van Dijke, A., Ford, J. D., van der Hart, O., Van Son, M. J. M., van der Heijden, P. G. M., and Bühring, M. (2011). Childhood traumatization by primary caretaker and affect dysregulation in patients with borderline personality disorder and somatoform disorder. Eur. J. Psychotraumatol. 2:5628. doi: 10.3402/ejpt.v2i0.5628
van Zutphen, L., Siep, N., Jacob, G. A., Goebel, R., and Arntz, A. (2015). Emotional sensitivity, emotion regulation and impulsivity in borderline personality disorder: a critical review of fMRI studies. Neurosci. Biobehav. Rev. 51, 64–76. doi: 10.1016/j.neubiorev.2015.01.001
Viviani, R., Kächele, H., and Buchheim, A. (2011). Models of change in the psychotherapy of borderline personality disorders. Neuropsychoanalysis 13, 147–160. doi: 10.1080/15294145.2011.10773671
Westen, D., Nakash, O., Thomas, C., and Bradley, R. (2006). Clinical assessment of attachment patterns and personality disorder in adolescents and adults. J. Consult. Clin. Psychol. 74, 1065–1085. doi: 10.1037/0022-006x.74.6.1065
White, S. F., Adalio, C., Nolan, Z. T., Yang, J., Martin, A., and Blair, J. R. (2014). The amygdala’s response to face and emotional information and potential category-specific modulation of temporal cortex as a function of emotion. Front. Hum. Neurosci. 8:14. doi: 10.3389/fnhum.2014.00714
Wittfoth-Schardt, D., Gründing, J., Wittfoth, M., Lanfermann, H., Heinrichs, M., Domes, G., et al. (2012). Oxytocin modulates neural reactivity to children’s faces as a function of social salience. Neuropsychopharmacology 37, 1799–1807. doi: 10.1038/npp.2012.47
Keywords: borderline personality disorder, emotional regulation, attachment system, amygdala, functional MRI
Citation: Buchheim A, Erk S, George C, Kächele H, Martius P, Pokorny D, Spitzer M and Walter H (2016) Neural Response during the Activation of the Attachment System in Patients with Borderline Personality Disorder: An fMRI Study. Front. Hum. Neurosci. 10:389. doi: 10.3389/fnhum.2016.00389
Received: 10 March 2016; Accepted: 19 July 2016;
Published: 02 August 2016.
Edited by:
Tetsuo Kida, National Institute for Physiological Sciences (NIPS), JapanReviewed by:
Shane McKie, University of Manchester, UKMartin Driessen, Ev. Hospital Bielefeld, Germany
Copyright © 2016 Buchheim, Erk, George, Kächele, Martius, Pokorny, Spitzer and Walter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution and reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Buchheim, YW5uYS5idWNoaGVpbUB1aWJrLmFjLmF0