
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 12 February 2025
Sec. Headache and Neurogenic Pain
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1556808
This article is part of the Research TopicManagement of migraine in patients with coexistent conditions or comorbidities: from classic to novel therapiesView all 3 articles
 Georgia Kourlaba1*
Georgia Kourlaba1* Michail Vikelis2
Michail Vikelis2 Theodoros Karapanayiotides3
Theodoros Karapanayiotides3 Argyro Solakidi4
Argyro Solakidi4 Dimitrios Trafalis4
Dimitrios Trafalis4 Katerina Lioliou1
Katerina Lioliou1 Panagiotis Andriopoulos1Aspasia Panagiotou1
Panagiotis Andriopoulos1Aspasia Panagiotou1 Dimos-Dimitrios Mitsikostas5
Dimos-Dimitrios Mitsikostas5Introduction: Migraine is a chronic, debilitating neurological disorder affecting billions worldwide. While not life-threatening, migraine patients experience significant unmet needs in diagnosis and management. Addressing these challenges could result in improvement of patient outcomes and reduction of the socioeconomic burden migraine imposes on individuals, healthcare system and the society.
Objective: This survey aimed to capture in Greece the perspective of medical experts (neurologists) specializing in migraine management regarding the socioeconomic burden of migraine and the unmet needs in diagnosis and treatment.
Methods: An online Delphi-based survey was conducted with 13 neurologists, experts in migraine. The survey consisted of 55 statements derived from literature research, regarding the burden of disease, diagnosis, treatment and unmet needs. Participants’ level of agreement for each statement was measured through a 5-point Likert scale (“Strongly Agree,” “Agree,” “Neither Agree nor Disagree,” “Disagree” and “Strongly Disagree”). Three rounds of voting were conducted to achieve consensus. The consensus threshold was set at 70% of responses, focusing on “Strongly Agree”/ “Agree” or “Disagree”/ “Strongly Disagree.”
Results: Most experts agreed on statements emphasizing on financial and social impact of the disease and its epidemiology. However, consensus was not reached on statements concerning patient preferences for treatment administration, treatment adherence, opioid use, and frequency of visits to neurologists. Consensus was reached on the need for better healthcare professional training and the development of effective, safe treatments.
Conclusion: This survey highlighted the challenges of prompt diagnosis and effective management of migraine. Addressing these needs requires patient-centered approaches, enhanced healthcare-provider training, tailored therapeutic interventions, and advanced communication platforms.
Migraine is the most prevalent neurological disorders and one of the foremost causes of disability (1, 2). It is broadly categorized into episodic migraine-EM (less than 15 days per month, with subcategories of 4–8 days as low frequency and 8–14 days as high frequency) and chronic migraine-CM (over 15 headache days per month, of which at least eight are migraine-related or responsive to migraine-specific medication, for a period of over 3 months) (3, 4). Although the International Classification of Headache Disorders the 3rd edition (ICHD-3) formally classifies only CM, we use the terms EM and CM descriptively to reflect differences in migraine frequency and burden as is common in epidemiological research (4). The number of migraine sufferers worldwide has been estimated to 1.1 billion, with the highest prevalence observed in individuals aged 30 to 34 for both males and females (5, 6). Furthermore, migraine is 2–3 times more prevalent in females than males (6). Migraine prevalence in Greek adults up to 70 years-old is estimated at 8.0% (CM: 1.0% and EM: 7.1%) (7).
Untreated migraine usually manifests with recurrent episodes of moderate to severe headaches lasting up to 72 h, as well as nausea, vomiting, sensitivity to light and sound, and depressive symptoms (6). Recent data suggests that headache disorders (including migraine) account for the third highest burden of neurological diseases as measured by disability-adjusted life years (DALYs) in 2019 (8). There is a significant clinical burden associated with migraine because it commonly coexists with other conditions such as depression, anxiety, epilepsy, chronic pain, and cardiovascular events (9). Moreover, migraine causes considerable disruption to daily activities (10–16) and substantial healthcare costs, with indirect costs constituting approximately 90% of its overall economic burden in Europe (14, 17, 18).
Studies conducted in Greece revealed significant impact on job performance and quality of life and emphasized the increased financial burden and psychological impact of migraine on Greek patients (7, 19–26). However, despite advances in migraine treatment, patient-based surveys raise unmet medical needs concerning underdiagnosis, ineffective disease management and lack of awareness (7, 27, 28). However, it is possible that physicians’ perceptions regarding disease burden, treatment management, patient preferences, and unmet medical needs differ from those of patients (29–31). In this context, it is crucial to capture perspectives and beliefs of medical experts regarding migraine. Such information could provide useful insights for decision-makers involved in reimbursement decisions for new treatments. Additionally, it could improve physician-patient interaction, relieve the burden of migraine, and help medical experts adopt a patient-centered approach. The present study aims to document Greek neurologists’ perspectives regarding disease burden, treatment, and unmet needs of migraine.
In this study, the Delphi technique, a widely recognized effective method for achieving maximum consensus among experts, was selected (32–36). Delphi panel, encompassing three voting rounds, was carried out from July 5 to 25, 2023. A hybrid approach was used, combining traditional and modified Delphi techniques, whereby feedback was provided to each panelist between rounds, but without the option to edit or comment on the statements. There were three distinct phases to our research. First, a questionnaire including statements extracted from the literature was developed by a Steering Committee of three neurologists-experts in migraine and an expert of research methodology. During the second phase, the participants engaged in three rounds of voting to reach a consensus. In the third and final phase, data analysis and results were reported.
Eligible to participate in our study were neurologists with expertise on migraine. Expertise was defined as having at least one PubMed publication on migraine disease and working in a headache center. A sample of 20 experts on migraine were selected by the Steering Committee in such a way as to have representation from the private sector, university hospitals and public hospitals. An invitation was sent via email to these neurologists asking them to complete and sign an informed consent form. Thirteen of them responded positively, (65% participation rate) constituting the final sample of our study. Although, there is no specific number of Delphi panel members, these studies typically involve between 10 to 20 participants, therefore the study sample was considered sufficient (35).
The first phase of this study involved the creation of statements based on extensive literature research covering migraine’s epidemiology, comorbidities, guidelines in management and treatment (both national and international), financial, humanistic burden and unmet medical need. The literature search was conducted by the Steering Committee across multiple sources, including clinical guidelines, consensus and research papers, and systematic reviews published in PubMed database as well as in other scientific society websites. A total of 55 statements were included in the final questionnaire divided in six thematic sections: Epidemiology and comorbidities (8 Statements), Burden of migraine (12 Statements), Economic burden of migraine (4 Statements), Diagnosis (7 Statements), Treatment (15 Statements) and Unmet need (9 Statements). In the second phase, the questionnaire was developed in Qualtrics (Provo, United States) and distributed to participants via e-mail. To ensure anonymity, email addresses were not recorded to encourage honest responses. Participants were asked to rate their level of agreement at each statement using a 5-point Likert scale: “Strongly Agree,” “Agree,” “Neither Agree nor Disagree,” “Disagree,” and “Strongly Disagree.” Participants received periodic email reminders to enhance response rates and survey completeness. After the completion of the initial round, the data was processed, and participants received the consolidated results. A second round of voting was conducted, which included the statements that had not achieved consensus in the previous round, considering the results of the first round. After reprocessing the data from the second round, a third and final round was conducted.
To assess the extent of agreement or disagreement, the mean agreement level for each statement was computed based on the Likert scale in each survey round. The consensus threshold was determined based on the guidelines proposed by Hasson et al. for the Delphi technique, which recommended a level of consensus between 51 and 80% (33). Since the primary objective of this study was to identify unmet medical needs in migraine management, rather than establish guidelines, a consensus threshold of 70% was selected, focusing on borderline options (“Strongly Agree,” “Agree,” “Disagree,” “Strongly Disagree”).
For the study protocol ethical approval was obtained from the Research Ethics Committee of the University of the Peloponnese. Each participant in the study was required to provide written informed consent after being fully informed of the study’s objectives, time commitment, and use of their personal information (33, 37). The Delphi process did not involve any anticipated risks or financial benefits. In order to maintain the confidentiality of participants and their responses in the online survey, all data collected during the study was anonymized (37). In addition, all research data has been managed in accordance with the European and national regulations that govern the protection of personal data in scientific research.
A consensus was reached for all eight statements considered in this section (Table 1). There was consensus (100%) in agreement among the medical experts regarding the annual global prevalence and the annual prevalence of migraine in the adult Greek population (77.8%). Unanimously, the medical experts disagreed that the prevalence has increased in the last 30 years by about 2%, while agreed that migraine is more prevalent in women particularly those under 50 years old (100%), and among individuals aged 20–35 years (100%). Additionally, the medical experts agreed that despite the increased prevalence, migraine remains an underdiagnosed disease (100%). Finally, there was 100% agreement that mood disorders, anxiety and sleep disorders often occur along with migraines, while there was consensus in disagreement regarding the claim that cardiovascular diseases frequently co-exist with migraine (72%).
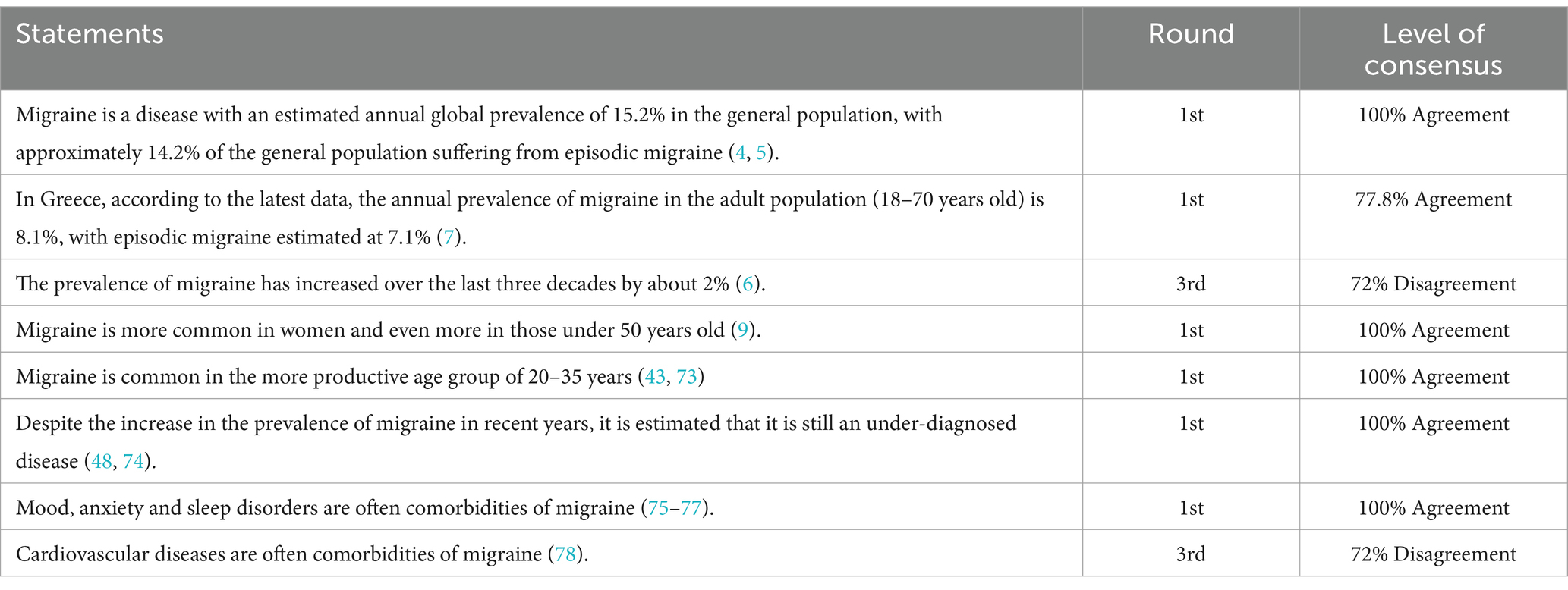
Table 1. Results regarding epidemiology and comorbidities.
On all 12 statements in this section, consensus was reached in agreement (Table 2). According to all medical experts, migraine significantly impacts patients’ quality of life (100%), and patients’ productivity, posing a significant burden on employers, patients, and society (100%). Moreover, medical experts concluded that severe migraine attacks can confine patients to bed, preventing them from performing daily and social activities (100%). Additionally, 77.8% of medical experts concurred that patients are often absent from work during these attacks, and 100% acknowledged that migraines impact not only patients but also their families. In addition, the medical experts agreed that migraine patients under the age of 45 generally suffer from a greater burden in their social and professional lives (88.9%) and that they frequently modify and adapt their lives to avoid future episodes (88.9%). As for stigma, medical experts agreed that this is an underestimated feature experienced by patients (88.9%). Finally, medical experts pointed out that migraine patients often feel that people in their social environment as well as healthcare professionals underestimate the severity of their condition (100%).

Table 2. Results regarding Burden of migraine (Quality of life, social impacts, psychological impacts, Work-related impacts).
Consensus in agreement was reached for all four statements regarding the economic burden of migraine (Table 3). Specifically, medical experts agreed at 77.8% that migraine has a high economic burden comparable to dementia and strokes. This high economic burden is primarily attributed to the substantial loss of productivity among patients (88.9%). Also, there was consensus at 77.8% regarding the extensive use of healthcare resources by migraine patients. This involves frequent visits to doctors of varying specialties and to emergency departments of hospitals. Additionally, there was unanimous agreement that polypharmacy influences the direct costs associated with migraine treatment (77. 8%).
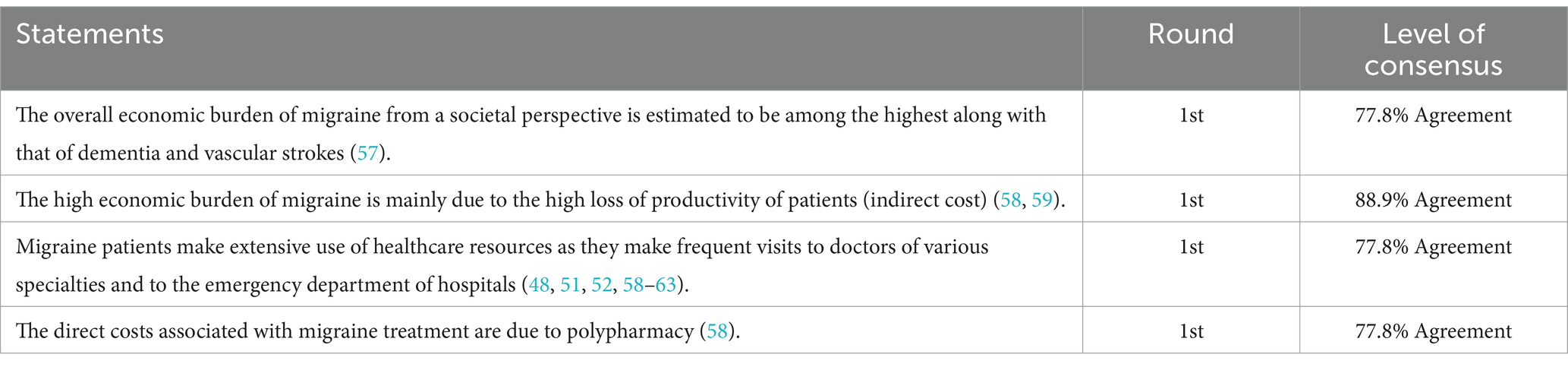
Table 3. Results regarding economic burden of migraine.
There was consensus in agreement for eight out of nine statements regarding the diagnosis of migraine (Table 4). Most of medical experts agreed that patients with migraine symptoms might delay seeking medical advice for several years as they learn to live by partially managing their symptoms with simple analgesics. Furthermore, 88.9% of respondents agreed that the stigma and emotional burden experienced by migraine sufferers from their social environment contributes to their hesitance to seek treatment. It was unanimously agreed by all panelists that patients with migraine symptoms are typically referred to other medical specialties before being referred to a neurologist. Also, a consensus was reached (88.9%) that migraine patients often struggle to effectively communicate their symptoms to treating physicians, resulting in delayed diagnosis. In addition, the panel agreed that delay in diagnosis might be partially attributed to the limited amount of time that physicians spend with patients (88.9%) and that the late diagnosis of ΕΜ might cause CM (100%). However, there was no consensus regarding the statement that most migraine patients who visited a doctor in the past year had consulted a neurologist.
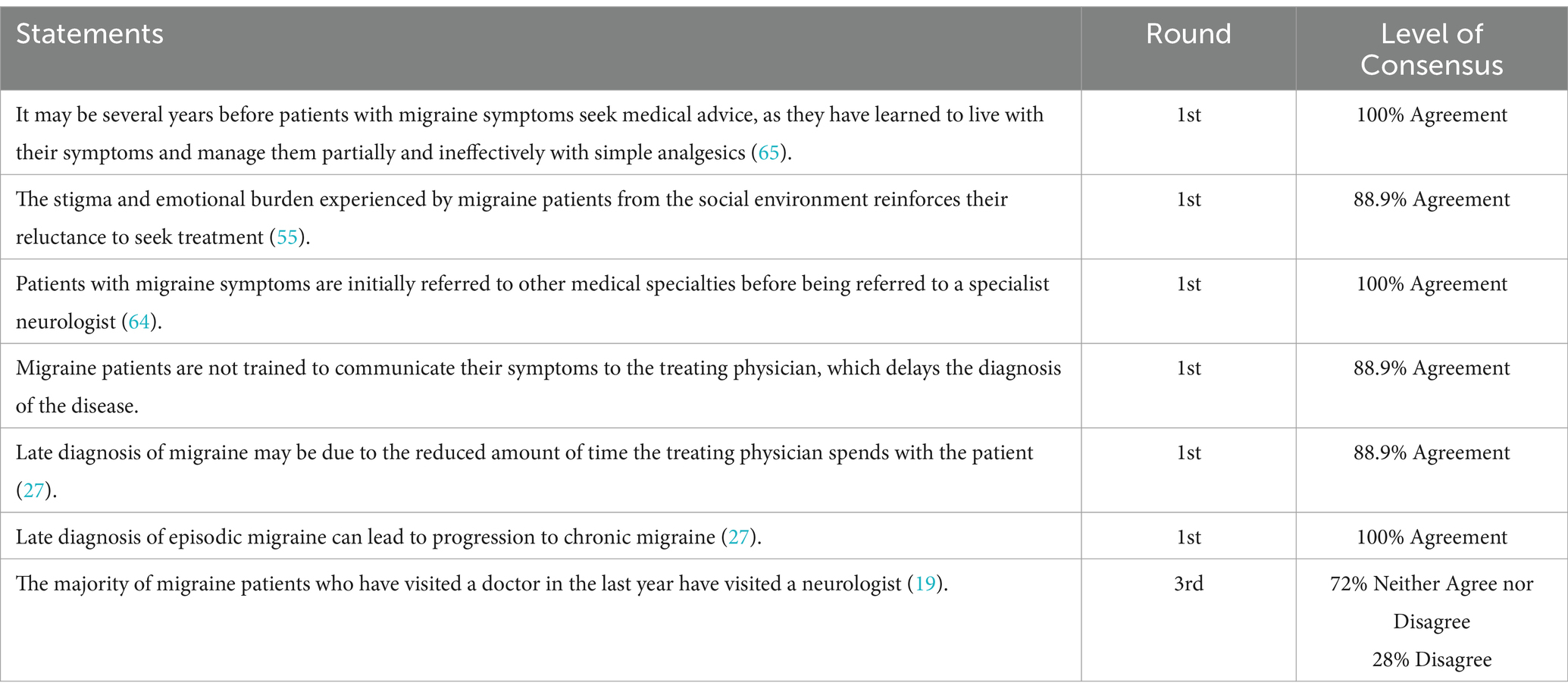
Table 4. Results on diagnosis.
Consensus in agreement was reached for 12 out of 15 statements regarding treatment of migraine (Table 5). According to the medical experts, migraine attacks are typically treated with simple analgesics or anti-inflammatory medications, followed by triptans (100%) and 88.9% of respondents agreed that migraineurs frequently overuse medications. A unanimous consensus was reached by the panel that treatment decisions should be based on a patient’s clinical profile, preferences, lifestyle characteristics, and comorbidities (100%). Moreover, they concurred that many migraine patients fail to respond adequately to available treatments or suffer from intolerable adverse reactions (100%), and that a change in treatment could be made even within the same class of medicines in cases of non-response to treatment or adverse effects (77.8%). A consensus in agreement was also reached regarding the statement that preventive treatment should be initiated if the frequency of migraine attacks exceeds 4 days per month for more than 3 months (77.8%). All members of the panel agreed that preventing EM from progressing to CM is one of the most significant benefits of preventive treatment (100%). A consensus of agreement was reached regarding the statement that most patients using non-prescription analgesic treatments for migraine attacks were dissatisfied with the results (100%). Furthermore, the panel reached agreement that many migraine patients who have tried preventive treatment with antiepileptics, antidepressants, or beta-blockers have discontinued the treatment due to unsatisfactory results. In addition, medical experts agreed that patients’ expectations of immediate improvement in symptoms may lead to preventive medications discontinuation prior to their expected improvement (77.8%). Last but not least, the consensus panel agreed that ineffective patient-physician communication is associated with patients’ dissatisfaction with their treatment and poor treatment adherence (100%). However, consensus was not reached for the statement that migraine patients are more likely to use opioid analgesics than the general population (14% Agree, 72% Neither Agree nor Disagree). Additionally, medical experts have not reached a consensus regarding patients’ preferences for the route of administration when it comes to preventive treatments, whether oral or injectable (57% Agree, 43% Neither Agree nor Disagree). Finally, no consensus was achieved regarding the low adherence of patients receiving preventive treatment (57% Agree, 43% Neither Agree nor Disagree).
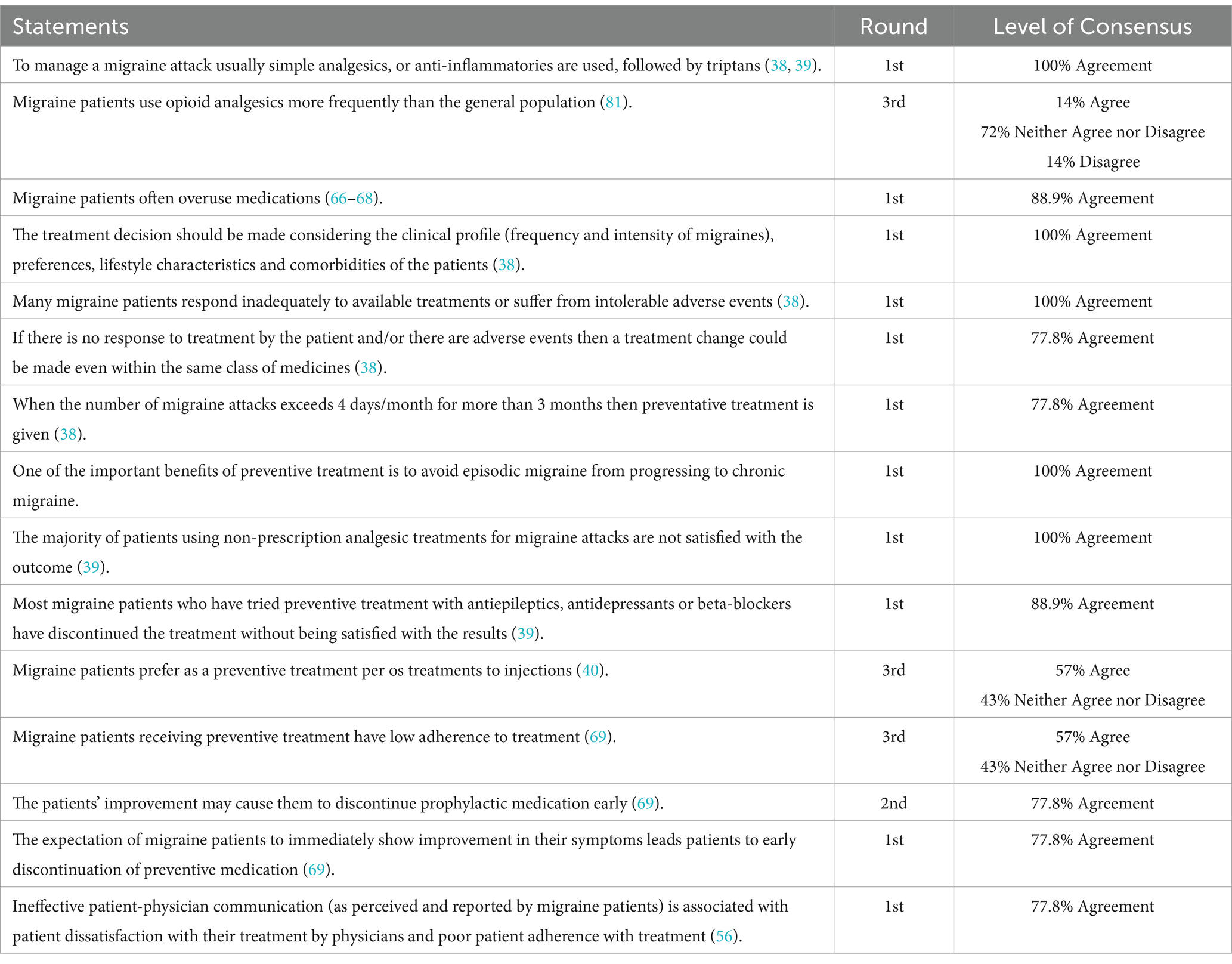
Table 5. Results regarding treatment of migraine.
All statements related to unmet medical needs in migraine management were unanimously accepted (Table 6). It was agreed that healthcare professionals should receive training in the correct diagnosis and treatment of EM to ensure proper disease management (100%). Additionally, consensus was reached regarding the unsatisfactory management of EM despite the wide availability of treatment (88.9%), and that EM should be targeted for prevention, in accordance with its pathophysiology (100%). It was also unanimously agreed that it is imperative to reduce the amount of medication administered to patients suffering from EM during both acute and preventive treatment (100%) and that there is a need for a new treatment for the management of acute migraine without contraindication in patients with cardiovascular problems (100%). Also, the panel noted the importance of simplifying the treatment regimen for EM, suggesting that there is a need for a single medication that could effectively treat migraine attacks and prevent future attacks (88.9%). Finally, the experts agreed that using aids such as apps, patient decision aids, and electronic diaries by migraine patients, enabling them to record crucial information about their migraines and share it with clinicians during their appointments, would enhance patient-physicians communication (88.9%).
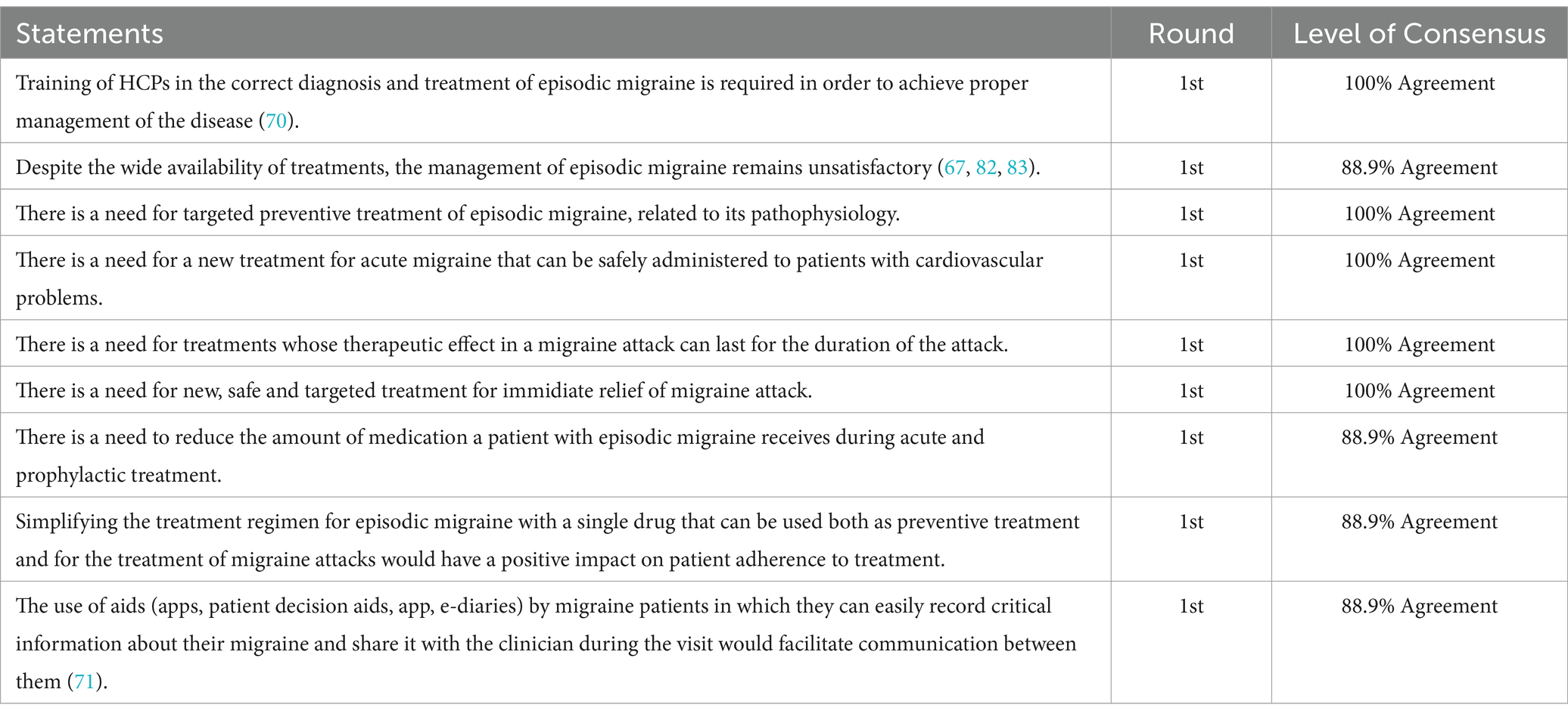
Table 6. Results regarding unmet medical need of migraine.
This study aimed to capture medical experts’ perspective in Greece on burden of migraine and unmet medical needs regarding clinical diagnosis and management. Previous studies have quantified patients’ preferences and satisfaction with treatment as well as the burden of disease in Greece (7, 19, 25, 26, 38–41). To the best of our knowledge, this is the first study to describe Greek medical experts’ point of view through a qualitative analysis. In a recent survey among Greek neurologists on the familiarity and likeability of management and treatment of various neurological disorders, migraine scored high, indicating that physicians like managing migraine and feel confident with its treatment (42).
All statements regarding migraine prevalence, including the higher prevalence in women and among those under 50 years of age, were supported by medical experts, indicating that the existing data are consistent with their clinical experience (5, 7, 9). According to previous studies, migraine is an underdiagnosed disease with various comorbidities occurring in the most productive period of adulthood (5, 43).
In accordance with the literature, it has been agreed that migraine is a burdensome disease for employers, patients, and society in general, as it adversely affects the productivity and social life of patients and their close relatives (10, 11, 38, 44–53). Furthermore, regarding the daily activities of patients our findings are in accordance with a previous Greek study and the international literature (9, 19, 44, 54, 55). In our study, medical experts acknowledged the existence of stigma, as a result of society’s negative perception of the illness and expressed the perception that patients may not feel understood (55, 56).
From an economic perspective, the experts aligned with the international literature and agreed that migraine imposes a substantial financial burden on patients and the healthcare system (57–59). The financial burden is agreed to be attributed to polypharmacy, frequent visits to doctors, and emergency department visits, contributing to increased healthcare resource utilization (48, 51, 52, 58–63).
Our study showed that Greek migraine patients often self-medicate and delay seeking medical help, potentially because of stigma and emotional burden from their environment, in accordance with the literature (55, 64, 65). A major challenge in migraine management is late diagnosis, due to patients’ negligence or to the interference of other physicians before referral to a headache specialist (64). The limited time that physicians dedicate to patients seems to contribute to delayed diagnosis, since migraine is primarily diagnosed clinically (27). As a result, both patients and healthcare providers should become aware of the importance of accelerating the diagnostic process.
The majority of statements related to the clinical management of migraine have been validated by medical experts with their consensus in agreement and were aligned with the available literature (38, 39, 66–68). Furthermore, patients’ expectations of immediate treatment results, ineffective patient-physician communication, and discontinuation of treatment due to symptom improvement seems to lead to patients’ non-adherence. Although it is suggested that oral treatment is more convenient and increases patient adherence, medical experts were not unanimously in agreement about patients’ preference (40). In a recent survey, most Greek migraine patients favored acute medications in tablet form, except CM patients, who preferred subcutaneous treatment due to more severe and prolonged attacks requiring frequent use of subcutaneous sumatriptan as salvage therapy (41). This variability in expert opinion may be attributed to the subjectivity of patients’ preferences. In addition, medical experts have not reached a consensus regarding the issue of low adherence among patients receiving preventive treatment, although the latter is suggested by the literature (69). This may be attributed to the varied clinical scenarios encountered by each physician, making it challenging to generalize conclusions about adherence in preventive treatment. Alternatively, patients may withhold information about their adherence to their physicians.
Targeted training of healthcare professionals (HCPs) in accurate diagnosis and treatment is of paramount importance for the effective management of the disease (70). Considering the prolonged duration of migraine attacks and the associated therapeutic challenges, there is an urgent need for safer and more effective treatments. In addition, streamlining migraine treatment may facilitate adherence to treatment. The use of assistive technologies such as applications, patient decision aids, and electronic diaries facilitates the systematic recording of vital migraine-related information and improves communication between patients and clinicians (71).
Our study’s limitations are primarily related to the Delphi method (72). Firstly, the small number of panelists and secondly, the lack of opportunity to participate in the development of the statements during the Delphi rounds may have limited the comprehension of those statements. As a result of the limited sample size of the Delphi approach, it is difficult to generalize the results to a broader population. In addition, certain statements focused more on the management of episodic migraineurs and our findings apply primarily to EM. However, this is in accordance with the 7-fold prevalence of EM in the Greek population compared to that of CM. This study provides a starting point for designing and conducting future larger and more focused consensus studies in Greece.
In summary, this Delphi survey reveals migraine’s multivariate impact in patients’ lives, its burden in humanistic and economic terms, and the challenges associated with timely and effective diagnosis and tolerable and effective treatment. Moreover, our findings highlight the obstacles associated with prompt diagnosis and successful treatment. To address the unresolved migraine needs of sufferers, patient-centered approaches, enhanced training for healthcare providers, tailored therapeutic interventions, and advanced communication platforms are essential. Relevant data should be registered continuously and incorporated into clinical practice and health policy decisions in a timely manner.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by Research Ethics Committee of the University of the Peloponnese. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
GK: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft. MV: Conceptualization, Methodology, Writing – review & editing. TK: Conceptualization, Writing – review & editing. AS: Writing – review & editing. DT: Writing – review & editing. KL: Formal analysis, Investigation, Methodology, Writing – original draft. PA: Writing – review & editing. AP: Writing – review & editing. D-DM: Conceptualization, Methodology, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was sponsored by Pfizer Hellas S. A. Pfizer was not involved in the management of participants’ personal information, data analysis and results interpretation.
We would like to thank Professor Sofia Zyga, an employee of the University of Peloponnese, for her valuable contribution with the development of this manuscript. We would also like to express our appreciation to all the panelists for their contribution. Listed in alphabetical order, we thank Dr. Athanasia Alexoudi, Dr.Manoli Dermitzakis, Dr. Ermioni Giannouli, Dr. Konstantinos Notas, Dr. Jobst Rudolf, and Dr. Panagiotis Soldatos for their contribution to the survey.
KL, AP, PA, and GK are employees of University of Peloponnese, which received funding from Pfizer in connection with the development of this manuscript. D-DM, MV, and TK, received compensation from Pfizer for their services as members of the Steering Committee for this study. AS and DT are employees of Pfizer Hellas S.A.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CM, Chronic Migraine; DALYs, Disability-Adjusted life years; EM, Episodic Migraine; ICHD-3, International Classification of Headache Disorders, 3rd edition; HCP, Healthcare professional.
1. Amiri, P, Kazeminasab, S, Nejadghaderi, SA, Mohammadinasab, R, Pourfathi, H, Araj-Khodaei, M, et al. Migraine: A review on its history, global epidemiology, risk factors, and comorbidities. Front Neurol. (2021) 12:800605. doi: 10.3389/fneur.2021.800605
2. Steiner, TJ, Stovner, LJ, Jensen, R, Uluduz, D, and Katsarava, Z. On behalf of lifting the burden: the global campaign against H. Migraine remains second among the world’s causes of disability, and first among young women: findings from GBD 2019. J Headache Pain. (2020) 21:137. doi: 10.1186/s10194-020-01208-0
3. Buse, DC, Greisman, JD, Baigi, K, and Lipton, RB. Migraine progression: A systematic review. Headache. (2019) 59:306–38. doi: 10.1111/head.13459
4. IHS. International headache society. Headache classification Committee of the International Headache Society (IHS) the international classification of headache disorders, 3rd edition. Cephalalgia. (2018) 38:1–211. doi: 10.1177/0333102417738202
5. Steiner, TJ, and Stovner, LJ. Global epidemiology of migraine and its implications for public health and health policy. Nat Rev Neurol. (2023) 19:109–17. doi: 10.1038/s41582-022-00763-1
6. Safiri, S, Pourfathi, H, Eagan, A, Mansournia, MA, Khodayari, MT, Sullman, MJM, et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain. (2022) 163:e293–309. doi: 10.1097/j.pain.0000000000002275
7. Constantinidis, TS, Arvaniti, C, Fakas, N, Rudolf, J, Kouremenos, E, Giannouli, E, et al. A population-based survey for disabling headaches in Greece: prevalence, burden and treatment preferences. Cephalalgia. (2021) 41:810–20. doi: 10.1177/0333102421989630
8. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet Neurol. (2024) 23:344–81. doi: 10.1016/S1474-4422(24)00038-3
9. Ashina, M, Katsarava, Z, Do, TP, Buse, DC, Pozo-Rosich, P, Ozge, A, et al. Migraine: epidemiology and systems of care. Lancet (London, England). (2021) 397:1485–95. doi: 10.1016/S0140-6736(20)32160-7
10. Blumenfeld, AM, Varon, SF, Wilcox, TK, Buse, DC, Kawata, AK, Manack, A, et al. Disability, HRQoL and resource use among chronic and episodic migraineurs: results from the international burden of migraine study (IBMS). Cephalalgia. (2011) 31:301–15. doi: 10.1177/0333102410381145
11. Martelletti, P, Schwedt, TJ, Lanteri-Minet, M, Quintana, R, Carboni, V, Diener, HC, et al. My migraine voice survey: a global study of disease burden among individuals with migraine for whom preventive treatments have failed. J Headache Pain. (2018) 19:115. doi: 10.1186/s10194-018-0946-z
12. Buse, D, Manack, A, Serrano, D, Reed, M, Varon, S, Turkel, C, et al. Headache impact of chronic and episodic migraine: results from the American migraine prevalence and prevention study. Headache. (2011) 52:3–17. doi: 10.1111/j.1526-4610.2011.02046.x
13. Ford, JH, Jackson, J, Milligan, G, Cotton, S, Ahl, J, and Aurora, SK. A real-world analysis of migraine: A cross-sectional study of disease burden and treatment patterns. Headache. (2017) 57:1532–44. doi: 10.1111/head.13202
14. Buse, DC, Reed, ML, Fanning, KM, Bostic, RC, and Lipton, RB. Demographics, headache features, and comorbidity profiles in relation to headache frequency in people with migraine: results of the American migraine prevalence and prevention (AMPP) study. Headache. (2020) 60:2340–56. doi: 10.1111/head.13966
15. Doane, MJ, Gupta, S, Fang, J, Laflamme, AK, and Vo, P. The humanistic and economic burden of migraine in Europe: A cross-sectional survey in five countries. Neurol Ther. (2020) 9:535–49. doi: 10.1007/s40120-020-00196-2
16. Ford, JH, Foster, SA, Nichols, RM, Tockhorn-Heidenreich, A, Ye, W, Jackson, J, et al. A real-world analysis of patient-reported outcomes in patients with migraine by preventive treatment eligibility status in the US and Europe. J Patient Rep Outcomes. (2020) 4:53. doi: 10.1186/s41687-020-00221-w
17. Linde, M, Gustavsson, A, Stovner, LJ, Steiner, TJ, Barré, J, Katsarava, Z, et al. The cost of headache disorders in Europe: the Eurolight project. Eur J Neurol. (2012) 19:703–11. doi: 10.1111/j.1468-1331.2011.03612.x
18. Jellestad, PL, Carlsen, LN, Westergaard, ML, Munksgaard, SB, Bendtsen, L, Lainez, M, et al. Economic benefits of treating medication-overuse headache - results from the multicenter COMOESTAS project. Cephalalgia. (2019) 39:274–85. doi: 10.1177/0333102418786265
19. Dermitzakis, EV, Kouroudi, A, Argyriou, AA, Spingos, KC, Bilias, K, and Vikelis, M. Results of a web-based survey of 2105 Greek migraine patients in 2020: demographics, clinical characteristics, burden and the effects of the COVID-19 pandemic on the course of migraine. BMC Neurol. (2022) 22:440. doi: 10.1186/s12883-022-02968-9
20. Dermitzakis, EV, Argyriou, AA, Bilias, K, Barmpa, E, Liapi, S, Rikos, D, et al. Results of a web-based survey on 2565 Greek migraine patients in 2023: demographic data, imposed burden and satisfaction to acute and prophylactic treatments in the era of new treatment options. J Clin Med. (2024) 13:13. doi: 10.3390/jcm13102768
21. Mitsikostas, DD, Tsaklakidou, D, Athanasiadis, N, and Thomas, A. The prevalence of headache in Greece: correlations to latitude and climatological factors. Headache. (1996) 36:168–73. doi: 10.1046/j.1526-4610.1996.3603168.x
22. Constantinidis, TS, Arvaniti, C, Fakas, N, Rudolf, J, Kouremenos, E, Giannouli, E, et al. The prevalence and burden of medication overuse headache in Greece. Cephalalgia. (2023) 43:3331024231184909. doi: 10.1177/03331024231184909
23. Mitsikostas, DD, Gatzonis, S, Thomas, A, Kalfakis, N, IIias, A, and Papageoergiou, C. An epidemiological study of headaches among medical students in Athens. Headache. (1996) 36:561–4. doi: 10.1046/j.1526-4610.1996.3609561.x
24. Mitsikostas, DD, Thomas, A, Gatzonis, S, Ilias, A, and Papageorgiou, C. An epidemiological study of headache among the monks of Athos (Greece). Headache. (1994) 34:539–41. doi: 10.1111/j.1526-4610.1994.hed3409539.x
25. Mantonakis, L, Belesioti, I, Deligianni, CI, Natsis, V, Mitropoulou, E, Kasioti, E, et al. Depression and anxiety symptoms in headache disorders: an observational, cross-sectional study. Neurol Int. (2024) 16:356–69. doi: 10.3390/neurolint16020026
26. Mitsikostas, DD, Alexoudi, A, Arvaniti, C, Giannouli, E, Kouremenos, Ε, Constantinidis, TS, et al. Hellenic headache society recommendations for the use of monoclonal antibodies targeting the calcitonin gene-related peptide pathway for the prevention of migraine and cluster headache—2023 update. SN Compr Clin Med. (2023) 5:118. doi: 10.1007/s42399-023-01452-w
27. Piccinni, C, Cevoli, S, Ronconi, G, Dondi, L, Calabria, S, Pedrini, A, et al. A real-world study on unmet medical needs in triptan-treated migraine: prevalence, preventive therapies and triptan use modification from a large Italian population along two years. J Headache Pain. (2019) 20:74. doi: 10.1186/s10194-019-1027-7
28. Kim, BK, Chu, MK, Yu, SJ, Dell'Agnello, G, Han, JH, and Cho, SJ. Burden of migraine and unmet needs from the patients' perspective: a survey across 11 specialized headache clinics in Korea. J Headache Pain. (2021) 22:45. doi: 10.1186/s10194-021-01250-6
29. Kennedy, BM, Rehman, M, Johnson, WD, Magee, MB, Leonard, R, and Katzmarzyk, PT. Healthcare providers versus Patients' understanding of health beliefs and values. Patient Exp J. (2017) 4:29–37. doi: 10.35680/2372-0247.1237
30. Natafgi, N, Ladeji, O, Blackwell, S, Hong, YD, Graham, G, Cort, M, et al. Similar values, different expectations: how do patients and providers view 'health' and perceive the healthcare experience? Health Expect. (2022) 25:1517–28. doi: 10.1111/hex.13493
31. van Dulmen, AM. Different perspectives of doctor and patient in communication. Int Congr Ser. (2002) 1241:243–8. doi: 10.1016/S0531-5131(02)00691-X
32. Black, N, Murphy, M, Lamping, D, McKee, M, Sanderson, C, Askham, J, et al. Consensus development methods: a review of best practice in creating clinical guidelines. J Health Serv Res Policy. (1999) 4:236–48. doi: 10.1177/135581969900400410
33. Hasson, F, Keeney, S, and RC, MK. Research guidelines for the Delphi survey technique. Leading Glob Nurs Res. (2000) 32:1008–15. doi: 10.1046/j.1365-2648.2000.t01-1-01567.x
34. Nair, R, Aggarwal, R, and Khanna, D. Methods of formal consensus in classification/diagnostic criteria and guideline development. Seminars in arthritis and rheumatism. Semin Arthritis Rheum. (2011) 41:95–105. doi: 10.1016/j.semarthrit.2010.12.001
35. Nasa, P, Jain, R, and Juneja, D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. (2021) 11:116–29. doi: 10.5662/wjm.v11.i4.116
36. Vogel, C, Zwolinsky, S, Griffiths, C, Hobbs, M, Henderson, E, and Wilkins, E. A Delphi study to build consensus on the definition and use of big data in obesity research. Int J Obes. (2005) 43:2573–86. doi: 10.1038/s41366-018-0313-9
37. Slade, SC, Dionne, CE, Underwood, M, and Buchbinder, R. Standardised method for reporting exercise programmes: protocol for a modified Delphi study. BMJ Open. (2014) 4:e006682. doi: 10.1136/bmjopen-2014-006682
38. Kouremenos, E, Arvaniti, C, Constantinidis, TS, Giannouli, E, Fakas, N, Kalamatas, T, et al. Consensus statement of the hellenic headache society on the diagnosis and treatment of migraine. J Headache Pain. (2020) 20:113. doi: 10.1186/s10194-019-1060-6
39. Dermitzakis, EV, Kouroudi, A, Argyriou, AA, Spingos, KC, Bilias, K, and Vikelis, M. Results of a web-based survey on 2105 Greek migraine patients-second part: Efficacy of acute and prophylactic migraine treatments and corresponding Patients' reported satisfaction. Medicina (Kaunas, Lithuania). (2022) 59:59. doi: 10.3390/medicina59010031
40. Mitsikostas, DD, Belesioti, I, Arvaniti, C, Mitropoulou, E, Deligianni, C, Kasioti, E, et al. Patients’ preferences for headache acute and preventive treatment. J Headache Pain. (2017) 18:102. doi: 10.1186/s10194-017-0813-3
41. Vikelis, M, Rikos, D, Argyriou, AA, Papachristou, P, Rallis, D, Karapanayiotides, T, et al. Preferences and perceptions of 617 migraine patients on acute and preventive migraine treatment attributes and clinical trial endpoints. Expert Rev Neurother. (2024) 24:815–26. doi: 10.1080/14737175.2024.2365312
42. Vikelis, MRD, Vlachos, GS, Argyriou, AA, Dermitzakis, EV, Xiromerisiou, G, Soldatos, P, et al. A survey of Greek neurologists on the likeability of headaches and other common neurological disorders and the familiarity to treat them. Arch Clin Neurol. (2023) 32:18–26.
43. Gupta, J, and Gaurkar, SS. Migraine: an underestimated neurological condition affecting billions. Cureus. (2022) 14:e28347. doi: 10.7759/cureus.28347
44. Al Ghadeer, HA, AlSalman, SA, Albaqshi, FM, Alsuliman, SR, Alsowailem, FA, Albusror, HA, et al. Quality of life and disability among migraine patients: A single-center study in AlAhsa, Saudi Arabia. Cureus. (2021) 13:e19210. doi: 10.7759/cureus.19210
45. Steiner, TJ, Stovner, LJ, and Vos, T. GBD 2015: migraine is the third cause of disability in under 50s. J Headache Pain. (2016) 17:104. doi: 10.1186/s10194-016-0699-5
46. Ailani, J, Burch, RC, and Robbins, MS. Board of Directors of the American headache S. The American headache society consensus statement: update on integrating new migraine treatments into clinical practice. Headache. (2021) 61:1021–39. doi: 10.1111/head.14153
47. Burton, WN, Schultz, AB, Shepherd, ME, and Hines, D. Migraine headache in an employed population: demographics, health risks, pharmaceutical utilization, and productivity loss. J Occup Environ Med. (2022) 64:679–85. doi: 10.1097/JOM.0000000000002564
48. Hazard, E, Munakata, J, Bigal, ME, Rupnow, MF, and Lipton, RB. The burden of migraine in the United States: current and emerging perspectives on disease management and economic analysis. Value Health. (2009) 12:55–64. doi: 10.1111/j.1524-4733.2008.00404.x
49. Paris, N, Vo, P, Valena, T, Bilitou, A, De Vulpillieres, FR, Fang, J, et al. Understanding the impact of migraine on work productivity using self-reported migraine diary data using the migraine-buddy© application in Europe. J Pain. (2017) 9:10. doi: 10.1007/s40120-018-0113-0
50. Pozo-Rosich, P, Lucas, C, Watson, DPB, Gaul, C, Ramsden, E, Ritter, S, et al. Burden of migraine in patients with preventive treatment failure attending European headache specialist centers: real-world evidence from the BECOME study. Pain Ther. (2021) 10:1691–708. doi: 10.1007/s40122-021-00331-3
51. Saylor, D, and Steiner, TJ. The global burden of headache. Semin Neurol. (2018) 38:182–90. doi: 10.1055/s-0038-1646946
52. Sumelahti, ML, Sumanen, M, Sumanen, MS, Tuominen, S, Vikkula, J, Honkala, SM, et al. My migraine voice survey: disease impact on healthcare resource utilization, personal and working life in Finland. J Headache Pain. (2020) 21:118. doi: 10.1186/s10194-020-01185-4
53. Tepper, SJ, Silberstein, SD, Rosen, NL, Lipton, RB, Dennehy, EB, Dowsett, SA, et al. The influence of migraine on driving: current understanding, future directions, and potential implications of findings. Headache. (2020) 60:178–89. doi: 10.1111/head.13716
54. Lo, SH, Gallop, K, Smith, T, Powell, L, Johnston, K, Hubig, LT, et al. Real-world experience of interictal burden and treatment in migraine: a qualitative interview study. J Headache Pain. (2022) 23:65. doi: 10.1186/s10194-022-01429-5
55. Parikh, SK, and Young, WB. Migraine: stigma in society. Curr Pain Headache Rep. (2019) 23:8. doi: 10.1007/s11916-019-0743-7
56. Patwardhan, M, Coeytaux, RR, Deshmukh, R, and Samsa, G. What is the impact of physician communication and patient understanding in the management of headache? Neuropsychiatr Dis Treat. (2007) 3:893–7. doi: 10.2147/NDT.S493
57. DiLuca, M, and Olesen, J. The cost of brain diseases: a burden or a challenge? Neuron. (2014) 82:1205–8. doi: 10.1016/j.neuron.2014.05.044
58. Bonafede, M, Sapra, S, Shah, N, Tepper, S, Cappell, K, and Desai, P. Direct and indirect healthcare resource utilization and costs among migraine patients in the United States. Headache. (2018) 58:700–14. doi: 10.1111/head.13275
59. Gilligan, AM, Foster, SA, Sainski-Nguyen, A, Sedgley, R, Smith, D, and Morrow, P. Direct and indirect costs among United States commercially insured employees with migraine. J Occup Environ Med. (2018) 60:1120–7. doi: 10.1097/JOM.0000000000001450
60. Kikui, S, Chen, Y, Todaka, H, Asao, K, Adachi, K, and Takeshima, T. Burden of migraine among Japanese patients: a cross-sectional National Health and wellness survey. J Headache Pain. (2020) 21:110. doi: 10.1186/s10194-020-01180-9
61. Bonafede, M, Cai, Q, Cappell, K, Kim, G, Sapra, SJ, Shah, N, et al. Factors associated with direct health care costs among patients with migraine. J Manag Care Spec Pharm. (2017) 23:1169–76. doi: 10.18553/jmcp.2017.23.11.1169
62. Deighton, AM, Harris, LA, Johnston, K, Hogan, S, Quaranta, LA, L’Italien, G, et al. The burden of medication overuse headache and patterns of switching and discontinuation among triptan users: A systematic literature review. BMC Neurol. (2021) 21:1–13. doi: 10.1186/s12883-021-02451-x
63. Deuschl, G, Beghi, E, Fazekas, F, Varga, T, Christoforidi, KA, Sipido, E, et al. The burden of neurological diseases in Europe: an analysis for the global burden of disease study 2017. Lancet Public Health. (2020) 5:e551–67. doi: 10.1016/S2468-2667(20)30190-0
64. Rai, NK, Bitswa, R, Singh, R, Pakhre, AP, and Parauha, DS. Factors associated with delayed diagnosis of migraine: A hospital-based cross-sectional study. J Family Med Prim Care. (2019) 8:1925–30. doi: 10.4103/jfmpc.jfmpc_376_19
65. Davies, PTG, Lane, RJM, Astbury, T, Fontebasso, M, Murphy, J, and Matharu, M. The long and winding road: the journey taken by headache sufferers in search of help. Prim Health Care Res Dev. (2019) 20:e4. doi: 10.1017/S1463423618000324
66. Elkind, AH. Drug abuse and headache. Med Clin North Am. (1991) 75:717–32. doi: 10.1016/S0025-7125(16)30445-X
67. Silberstein, SD, and Rosenberg, J. Multispecialty consensus on diagnosis and treatment of headache. Neurology. (2000) 54:1553. doi: 10.1212/WNL.54.8.1553
68. Takahashi, TT, Ornello, R, Quatrosi, G, Torrente, A, Albanese, M, Vigneri, S, et al. Medication overuse and drug addiction: a narrative review from addiction perspective. J Headache Pain. (2021) 22:32. doi: 10.1186/s10194-021-01224-8
69. Sevivas, H, and Fresco, P. Treatment of resistant chronic migraine with anti-CGRP monoclonal antibodies: a systematic review. Eur J Med Res. (2022) 27:86. doi: 10.1186/s40001-022-00716-w
70. Martelletti, P, and Curto, M. Unmet needs for migraine. Curr Med Res Opin. (2021) 37:1957–9. doi: 10.1080/03007995.2021.1976738
71. Dodick, DW, Tepper, SJ, Lipton, RB, Buse, DC, Stewart, WF, Bayliss, M, et al. Improving medical communication in migraine management: A modified Delphi study to develop a digital migraine tracker. Headache. (2018) 58:1358–72. doi: 10.1111/head.13426
72. Fink-Hafner, D, Dagen, T, Doušak, M, Novak, M, and Hafner-Fink, MJ. Delphi method: strengths and weaknesses. J Adv Methodol Stat. (2019) 16:1–19. doi: 10.51936/fcfm6982
73. Stewart, WF, Wood, C, Reed, ML, Roy, J, and Lipton, RB. Cumulative lifetime migraine incidence in women and men. Cephalalgia. (2008) 28:1170–8. doi: 10.1111/j.1468-2982.2008.01666.x
74. Ryvlin, P, Skorobogatykh, K, Negro, A, Sanchez-De La Rosa, R, Israel-Willner, H, Sundal, C, et al. Current clinical practice in disabling and chronic migraine in the primary care setting: results from the European my-LIFE anamnesis survey. BMC Neurol. (2021) 21:1. doi: 10.1186/s12883-020-02014-6
75. Silberstein, SD, and Lipton, RB. Epidemiology of migraine. Neuroepidemiology. (1993) 12:179–94. doi: 10.1159/000110317
76. Minen, MT, Begasse De Dhaem, O, Kroon Van Diest, A, Powers, S, Schwedt, TJ, Lipton, R, et al. Migraine and its psychiatric comorbidities. J Neurol Neurosurg Psychiatry. (2016) 87:741–9. doi: 10.1136/jnnp-2015-312233
77. Morgan, I, Eguia, F, Gelaye, B, Peterlin, BL, Tadesse, MG, Lemma, S, et al. Sleep disturbances and quality of life in sub-Saharan African migraineurs. J Headache Pain. (2015) 16:18. doi: 10.1186/s10194-015-0504-x
78. Burch, RC, Buse, DC, and Lipton, RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin. (2019) 37:631–49. doi: 10.1016/j.ncl.2019.06.001
79. Mac Gregor, EA, Brandes, J, Eikermann, A, and Giammarco, R. Impact of migraine on patients and their families: the migraine and Zolmitriptan evaluation (MAZE) survey--phase III. Curr Med Res Opin. (2004) 20:1143–50. doi: 10.1185/030079904125004178
80. Fofi, L, Altamura, C, Fiorentini, G, Brunelli, N, Marcosano, M, Barbanti, P, et al. Improving distress perception and mutuality in migraine caregivers after 6 months of galcanezumab treatment. Headache. (2022) 62:1143–7. doi: 10.1111/head.14400
81. Stone, MT, Weed, V, and Kulich, RJ. Opioid treatment of migraine: risk factors and behavioral issues. Curr Pain Headache Rep. (2016) 20:51. doi: 10.1007/s11916-016-0581-9
82. Lipton, RB, Diamond, S, Reed, M, Diamond, ML, and Stewart, WF. Migraine diagnosis and treatment: results from the American migraine study II. Headache. (2001) 41:638–45. doi: 10.1046/j.1526-4610.2001.041007638.x
Keywords: migraine, Delphi consensus, neurologists, burden, unmet needs, Greece
Citation: Kourlaba G, Vikelis M, Karapanayiotides T, Solakidi A, Trafalis D, Lioliou K, Andriopoulos P, Panagiotou A and Mitsikostas D-D (2025) Unmet needs in the management of migraine in Greece from the perspective of medical experts: a Delphi consensus. Front. Neurol. 16:1556808. doi: 10.3389/fneur.2025.1556808
Edited by:
Antonio Russo, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Florian Rimmele, University Hospital Rostock, GermanyCopyright © 2025 Kourlaba, Vikelis, Karapanayiotides, Solakidi, Trafalis, Lioliou, Andriopoulos, Panagiotou and Mitsikostas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georgia Kourlaba, Zy5rb3VybGFiYUB1b3AuZ3I=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.