
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol. , 05 March 2025
Sec. Stroke
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1537008
 Luís San Román1
Luís San Román1 Laura Ludovica Gramegna2Sara Pich3
Laura Ludovica Gramegna2Sara Pich3 Laura Domingo-Rodriguez3Marta Duran3Lluís Duocastella3Juan Macho1*
Laura Domingo-Rodriguez3Marta Duran3Lluís Duocastella3Juan Macho1*Rationale: The clinical impact of a novel mechanical thrombectomy strategy, which integrates distal access with flow reversal and flow arrest via a distal balloon, all within a single procedure [Safety and Efficacy of the overall throMbectomy system for sTroke (SEMTiC) strategy], has not been tested.
Aim: The SEMTiC-01 study is the first prospective, multicenter in vivo study evaluating the safety and efficacy of the combined thrombectomy system—iNedit, iNdeep, and iNtercept—in patients with acute ischemic stroke.
Sample size estimates: The study was designed with a sequential structure based on the efficacy endpoint (eTICI ≥2b) reported in the literature [71.1% with a 95% confidence interval of (68.5%, 73.8%)]. An interim analysis was set for 115 patients and a final analysis for 225 patients, ensuring 98% power at a one-sided 0.025 significance level, with a 2.6% non-inferiority margin and a 15% assumed withdrawal rate.
Design: SEMTiC-01 is a prospective, multicenter, single-arm, open-label clinical safety and efficacy investigation.
Outcome: Primary efficacy endpoint: expanded treatment in cerebral infarction score (eTICI) ≥2b revascularization within ≤ 3 stent retriever passes. Primary safety endpoint: monitoring serious adverse events within 24 h post-intervention and all-cause mortality at 90 days.
Mechanical thrombectomy (MT) for large vessel occlusion (LVO) strokes has been the subject of multiple randomized clinical trials, which have invariably demonstrated its overwhelming efficacy (1).
The initial key trials (2–5) focused on MT within 6 h of onset. However, the DEFUSE 3 (6) and DAWN (7) studies extended the therapeutic window to 24 h for selected patients with late-onset or wake-up strokes. Their findings were included in the 2018 American Heart Association (AHA)/American Stroke Association (ASA) stroke guidelines (8). MT can be performed with or without prior rt-PA (2).
Currently, significant research efforts are focused on improving the techniques available for performing MT.
Two main techniques for MT are stent retrievers and direct aspiration catheters, often used in combination. Stent retrievers, the most common (3), can be paired with a balloon guide catheter (BGC) to arrest and reverse blood flow during thrombus removal (9). However, the BGC is usually only advanced to the extracranial carotid artery for balloon inflation. There are no currently available mechanical devices that feature a balloon catheter near the distal tip, which can be inflated in the intracranial portion of the vessel. This could potentially increase the system's stability as the balloon would be surrounded by the petrous segment of the carotid encased in bone.
Direct aspiration catheters, while comparable to stent retrievers in terms of achieved revascularization (10), are less commonly used. They can be operated manually or with an aspiration pump via distal access catheters (DACs), with flexible tips for strong aspiration and efficient clot removal. However, they lack flow arrest and do not feature a balloon to improve the system's stability.
The iVascular (Sant Vicenç dels Horts, Barcelona) neurothrombectomy devices, including the iNedit balloon distal access catheter, iNdeep microcatheter, and iNtercept stent retriever, are designed to leverage the benefits of temporary proximal blood flow restriction via a balloon located 5 cm from the catheter tip, providing enhanced stability during distal aspiration. These devices are compatible with all commonly used stent retrievers.
Preliminary results on using the iNedit balloon DAC in different clinical scenarios indicate that the device achieved a high first-pass effect and final recanalization rate with no safety concerns, resulting in a high percentage of favorable clinical outcomes (11).
This study aims to evaluate the efficacy and safety of this novel MT approach (SEMTiC strategy), which uniquely combines distal access, flow arrest, and flow reversal in a single procedure for acute ischemic stroke (AIS) patients. The non-inferiority of this combination will be compared to existing literature data.
SEMTiC-01 is a prospective, multicenter, single-arm, open-label clinical safety and efficacy investigation.
In the SEMTiC-01 trial, eligible participants are AIS patients treated within 24 h of symptom onset, defined as the last time the patient was seen well (LTSW; the start of the procedure is defined as arterial puncture time). Patients will be enrolled at 18 sites, which are in Spain (14 sites: Hospital Clinic Barcelona, Hospital Universitario de Bellvitge, Hospital Universitario Central de Asturias, Hospital Reina Sofía de Córdoba, Hospital Vall d'Hebron, Hospital Clínico San Carlos, Hospital German Trías i Pujol, Hospital Universitario de Cruces, Hospital General Universitario de Alicante, Hospital Universitario la Fe, Hospital Universitario General de Canarias, Hospital General Universitario Gregorio Marañón, Hospital Universitario de Badajoz, and Hospital Clínico Universitario de Valencia), Germany (3 sites: K. München Hospital, K. Nürnberg Hospital, and K. Ludwigsburg Hospital), and Belgium (1 site: AZ Groeninge Hospital) between July 2022 and June 2024.
The detailed inclusion/exclusion criteria are listed in Table 1.
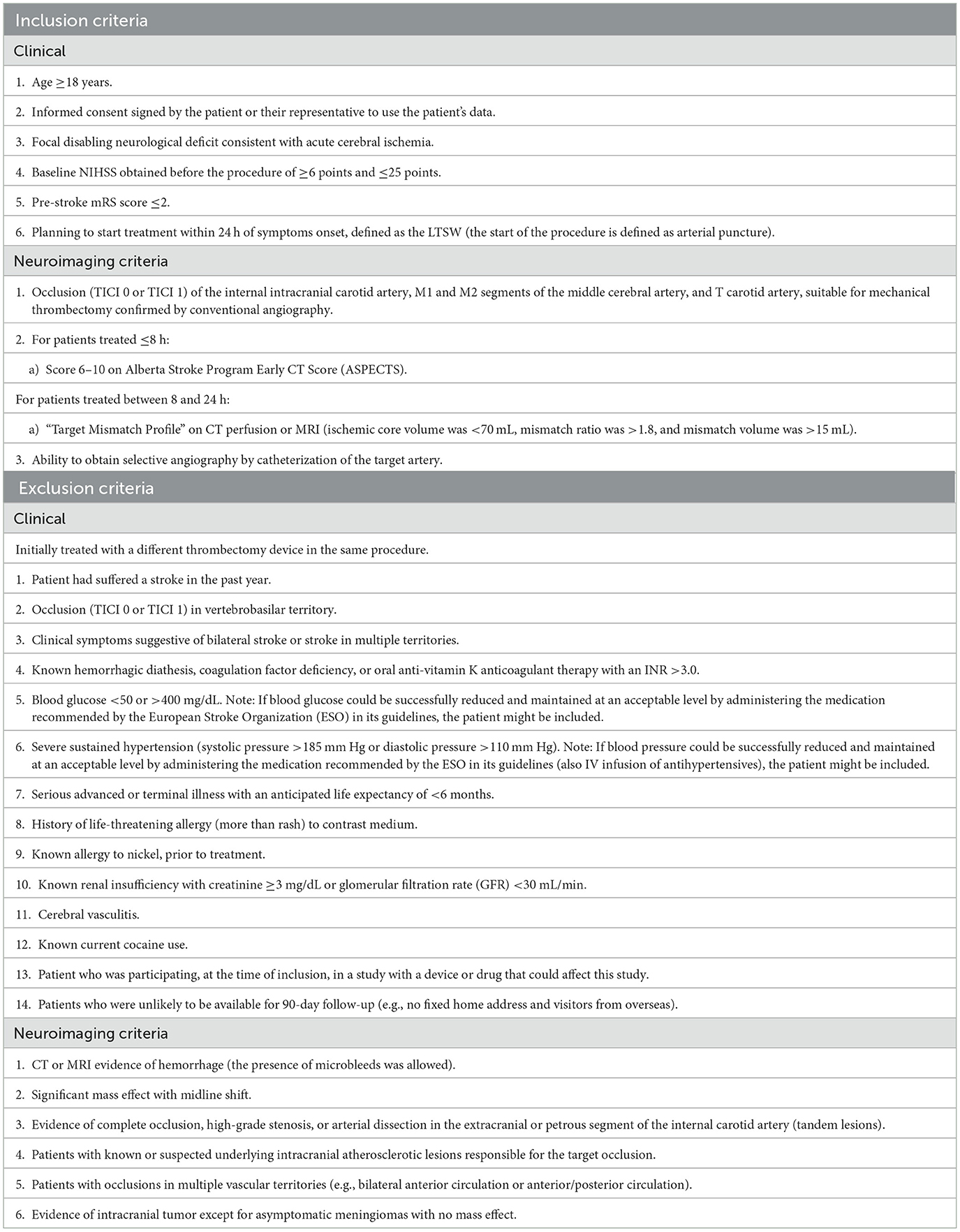
Table 1. Study inclusion and exclusion criteria.
This approach leverages an innovative balloon distal design, where a balloon located a few centimeters from the catheter tip blocks blood flow, while the distal tip enables aspiration. This technique uniquely integrates distal access, flow reversal, and flow arrest—via the distal balloon—into a single procedure.
The iNedit balloon distal access catheter is a double-lumen coaxial catheter from the connector to the balloon and a single lumen from the balloon to the tip. It is designed with braid and coil reinforcement. The distal segment has a compliant occlusion balloon located 5 cm from the tip of the catheter, the purpose of which is to occlude the flow at the discretion of the operator, if deemed necessary during the procedure.
The catheter's proximal “Y”-shaped luer-lock connector has a side port for balloon inflation/deflation with diluted contrast and a straight port for device passage or aspiration. The outer diameter of the catheter is compatible with access systems with a minimum internal lumen of 0.088” (2.235 mm). The maximum volume of balloon inflation is 0.2 mL.
The iNdeep microcatheter is a single-lumen catheter from proximal to distal shaft, reinforced with braid and variable stiffness through its entire length to ensure optimal trackability. At the most distal end, there is a radiopaque marker that helps to visualize the device under fluoroscopy.
The catheter's distal body has a durable hydrophilic coating for easier navigation through tortuous arteries and is available in three internal diameters (0.017”, 0.021”, and 0.027”).
The stent retriever consists of a self-expanding nitinol basket with proximal and distal markers for fluoroscopic positioning and gold markers to assess deployment. It is supplied compressed in an introducer sheath for easy insertion via a microcatheter. After full deployment, the device is deployed within or beyond the thrombus and retracted under suction.
The SEMTiC-01 trial is registered on clinicaltrials.gov (NCT05893719). The protocol and data collection of the trial have been approved by the Hospital Clinic, Barcelona, the ethics committee, and all participating sites. Written informed consent will be obtained from patients or representatives before inclusion into the trial.
All patients were consecutively included when the interventional neurologist confirmed that they met all the inclusion criteria and would treat them with the proposed strategy (SEMTiC strategy), including the use of all three devices. In cases where successful reperfusion (defined as eTICI 2b-3) was not achieved after three passes with the iNdeep, iNedit, and iNtercept devices [all with European Conformity (CE) market], rescue therapy—defined as the use of any additional strategies or devices—was permitted.
Deferred informed consent was utilized to prevent delays in treatment initiation. Once a patient is considered eligible for the study, the patient or their representative receives the “Patient Information Sheet” and “Informed Consent Form” (ICF). Written consent will be required from the patient or a family member during the study period to authorize the use of patient data. Investigators will explain the study and deliver a copy of the signed ICF. Each consented patient will be assigned a unique identifier, composed of a site number and a sequential patient number, based on the order of inclusion at each site.
All patients treated (with the study device or rescue therapy) were evaluated at 24, 72 h, or discharge and 90 days after the index procedure. The patient's study participation is considered complete at the 90-day visit.
The Clinical Events Committee (CEC) reviews all adverse events to determine their severity and seriousness (SAE) and to adjudicate causality related to the procedure or the device. The latter is assessed using the following scale: “possible” (the relationship with the use of the investigational device or the relationship with procedures, is weak but cannot be ruled out completely), “probable” (the relationship with the use of the investigational device or the relationship with procedures, seems relevant and/or the event cannot be reasonably explained by another cause), and “causal relationship” (the serious adverse event is associated with the investigational device or with procedures beyond reasonable doubt).
The primary efficacy endpoint is the achievement of a successful neurothrombectomy, defined as a revascularization of grade ≥2b-3 with ≤3 passes on the eTICI scale (12). The Core Lab used the eTICI scale to assess the performance of the overall system.
For the primary safety endpoint, all serious adverse events (SAEs) within 24 h (−8/+12 h) and mortality at 90 days were considered.
The secondary efficacy endpoint variable includes (I) good functional outcome (mRS 0–2 at 90 days post-treatment); (II) rapid neurological improvement [National Institutes of Health Stroke Scale (NIHSS) reduction >4 points or NIHSS ≤4 within 24 h]; (III) improvement at 72 h (NIHSS reduction ≥8 points or NIHSS 0–1 at 72 h or at discharge); (IV) procedure duration (time from a puncture to achieving eTICI grade ≥2b in fewer than 3 passes or final angiogram); (V) the number of passes required for recanalization; percentage of effective recanalization on the first pass; and (VI) navigability (i.e., the microcatheter and the distal access balloon catheter to reach the occlusion in the main vessel to allow navigation and deployment of the stent retriever to carry out the neurothrombectomy), assessed on a scale as “good”, “standard”, and “deficient”.
Secondary safety endpoint variable includes (I) intracerebral hemorrhage (ICH) assessed by magnetic resonance imaging (MRI)/computed tomography (CT) at 24 h, with symptomatic intracerebral hemorrhage (sICH) defined as ICH causing clinical deterioration (NIHSS worsening by ≥4 points) or death; (II) neurological deterioration (≥4 point increase on the NIHSS scale at 24 h); (III) distal embolization, i.e., any anterograde occlusion in the distal to the target artery injury, in the target ischemic territory; (IV) occurrence of embolization in previously unaffected areas on cerebral angiography; (V) mortality rate (death related to the procedure within 3 days or at discharge); (VI) procedure complications (arterial perforation and dissection—specifically involving the internal carotid artery (ICA), vasospasm, and embolization in new vascular territories); and (VII) infarction rate in previously unaffected areas (evaluated by MRI/CT 24 h post-procedure).
Study evaluations will be conducted at three time points: 24 h, 3 days (or at discharge), and 90 days following MT.
At 24 h post-MT (−8/+12 h), the following assessments will be performed, and relevant data will be collected: NIHSS, control neuroimaging (CT or MRI), recording of any adverse events (AEs) or SAEs, and documentation of concomitant medications.
At 3 days post-MT (±24 h) or at discharge, whichever occurs first, the following assessments will be performed: NIHSS, recording of any relevant AEs or SAEs, and determination of stroke etiology.
At 90 days post-MT, assessments will preferably be conducted through a face-to-face visit, although a telephone visit is also acceptable. Data collected will include the mRS and any SAEs resulting in death.
We anticipated that 82% of patients would achieve eTICI ≥ 2b, compared to 71.1% reported in previous research, to estimate the sample size in a non-inferiority study (13). To ensure 98% statistical power in a Z-test with a one-sided significance level of 0.025 and a non-inferiority margin of −2.6%, an interim analysis with 115 patients is needed (providing 51.1% cumulative information), assuming a 15% withdrawal rate. However, the sample size was increased to N = 225 to gather additional real-world clinical data.
All data will be analyzed with SPSS 27.0 Software. The mean ± standard deviation (SD) will be used if the data are normally distributed, and the median and interquartile range (IQR) will be used if the data are non-normally distributed.
The proportion of patients with eTICI ≥ 2b will be obtained, and the significance level for non-inferiority will be determined using the Z statistic for comparing two proportions with a non-inferiority margin of −0.026.
All values will be estimated using the 95% confidence interval (recommended Wilson's or Agresti methods). The following study populations will be defined for statistical analysis:
• Intention to treat (ITT) is defined as all patients included in the study who have been treated with at least one of the study devices. The primary efficacy analysis in relation to non-inferiority will be performed on this population.
• Population by protocol (PP) is defined as ITT subset with no major deviations from the clinical investigational plan. The primary efficacy analysis in relation to non-inferiority will also be performed with this population.
• Modified population by protocol (PP) is defined as PP subset excluding patients treated with rescue therapy.
All outcomes will be evaluated across all study populations. The proportion of patients undergoing rescue therapy will also be measured. The impact of rescue therapy on both angiographic and clinical outcomes will be assessed using adjusted logistic regression models. A subgroup analysis will compare the results achieved in cases with the occlusion of the M2 vs. the M1/T carotid segments.
The analysis after 115 patients showed non-inferiority of the SEMTiC strategy using iVascular devices in achieving the primary efficacy endpoint (80% in ITT and 89% in PP populations). These 115 patients had enough statistical power to finish recruitment at that point. However, the increase in the sample size to N = 225 was designed to obtain additional real-life clinical data. The study completed recruitment on June 30, 2024.
The primary efficacy endpoint of this study is to evaluate the non-inferiority of the iNedit, iNdeep, and iNtercept thrombectomy system in treating acute ischemic stroke in terms of successful recanalization, compared to existing literature. The key efficacy measure (eTICI ≥2b) is a well-established predictor of functional outcomes after mechanical thrombectomy (8). Literature reports successful recanalization rates ranging from 59 to 88% (14, 15).
For the primary safety outcome, we will analyze 90-day mortality, which has been reported to range from 7.9 to 14% in prior studies (3, 9, 15–17), along with any possible serious adverse event as evaluated by an external safety committee.
The secondary prespecified outcome will include eTICI ≥2c following MT, considering that the current goal is to achieve the highest possible percentage of complete or near-complete recanalization (2c or 3). ARISE II trial reported a rate of 64.8% for eTICI ≥2c (3). Favorable clinical outcomes, as measured by mRS of 0–2 at 90 days, will still be evaluated. In previous trials, ~50% of patients achieved this outcome 90 days post-MT (3, 9, 10, 16, 18).
In analyzing secondary outcomes (secondary efficacy outcome V), particular emphasis will be placed on evaluating the TICI score and the degree of recanalization achieved at each pass with the three devices. In addition, a comparative assessment of outcomes with and without rescue therapy will be conducted to understand its impact on procedural success.
Moreover, given the innovative nature of the devices (secondary efficacy outcome VI), thorough attention will be dedicated to evaluating procedure-related complications, including arterial perforation, dissection (particularly involving the ICA), vasospasm, and embolization in new vascular territories. In particular, the risk of balloon rupture will be considered a specific complication associated with using iNedit catheters. It will be recorded and reported during the trial as a post-hoc analysis, even if it is expected to have no clinical relevance.
These complications will be systematically assessed by the local investigators, independently reviewed through imaging analysis by the external core lab, and adjudicated by an independent Clinical Events Committee (CEC) to ensure objective evaluation and accuracy.
Special attention will be given to outcomes related to the navigability of the devices as the balloon catheter has been specifically developed to improve the navigability compared to currently available balloon guide catheters. Previous studies of preliminary experiences with this device have reported high scores in terms of navigability (11).
In addition, we expect a lower incidence of vasospasm, as balloon inflation occurs at the petrous segment of the carotid artery, where the periosteal layer provides stability by attaching to both the vessel and the surrounding bone. This contrasts with the cervical ICA, which is more prone to collapse due to being surrounded by the neck's soft tissues (19).
Integrating distal access, flow reversal, and flow arrest in mechanical thrombectomy potentially enhances clot retrieval efficiency, reduces embolization risk, and improves procedural safety. DACs allow closer proximity to the thrombus, providing stable support for thrombectomy devices, improving clot retrieval, and facilitating direct aspiration. Flow reversal helps prevent clot fragmentation and distal migration during retrieval, while flow arrest enables safer retrieval of large thrombi and enhances overall procedural control.
A potential limitation of the strategy proposed by the current study is that the distal aspiration balloon catheter has an inner diameter of 0.058”, which refers to the width of the hollow tube that runs through the center of the device. This may not be considered large enough to perform aspiration in certain cases with large clots, such as in the carotid T, according to some operators. However, this inner dimension may be advantageous for aspiration in distal vessels (20). A subgroup analysis comparing outcomes in M2 occlusions vs. the carotid T and M1 segments could support the future use of this catheter specifically for M2 occlusions, especially by inflating the distal balloon to achieve more effective flow arrest.
The main objective of this study is to demonstrate the feasibility and safety of the combined use of the three iVascular devices. The results of this study should be interpreted with caution due to its single-arm design, which may limit the ability to determine whether an alternative method would have yielded superior outcomes. However, a multicenter international study design has been implemented to reduce center-specific biases and enhance the generalizability of the findings. Furthermore, a secondary propensity score matching analysis will account for potential confounding factors by comparing similar patients treated with alternative methods.
The results of the SEMTiC studies, expected to be available in 2025, will answer whether combining flow arrest, flow reversal, and distal access (SEMTiC strategy) is an effective and safe strategy for performing mechanical thrombectomy.
The studies involving humans were approved by Hospital Clinic, Barcelona Ethic Commitee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LS: Conceptualization, Writing – original draft, Writing – review & editing. LG: Writing – original draft, Writing – review & editing. SP: Writing – original draft, Writing – review & editing. LD-R: Writing – original draft, Writing – review & editing. MD: Writing – original draft, Writing – review & editing. LD: Writing – original draft, Writing – review & editing. JM: Conceptualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work has been sponsored by iVascular S.L.U., Sant Vicenç dels Horts, Spain.
SP, LD-R, MD, and LD are all employees at iVascular S.L.U., Sant Vicenç dels Horts, Spain.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
2. Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, Yoo AJ, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. (2015) 372:11–20. doi: 10.1056/NEJMoa1411587
3. Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. (2015) 372:1019–30. doi: 10.1056/NEJMoa1414905
4. Campbell BC, Mitchell PJ, Kleinig TJ, Dewey HM, Churilov L, Yassi N, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. (2015) 372:1009–18. doi: 10.1056/NEJMoa1414792
5. Saver JL, Goyal M, Bonafe A, Diener HC, Levy EI, Pereira VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. (2015) 372:2285–95. doi: 10.1056/NEJMoa1415061
6. Albers GW, Marks MP, Kemp S, Christensen S, Tsai JP, Ortega-Gutierrez S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. (2018) 378:708–18. doi: 10.1056/NEJMoa1713973
7. Nogueira RG, Jadhav AP, Haussen DC, Bonafe A, Budzik RF, Bhuva P, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. (2018) 378:11–21. doi: 10.1056/NEJMoa1706442
8. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2018) 49:e46–e110. doi: 10.1161/STR.0000000000000158
9. Zaidat OO, Mueller-Kronast NH, Hassan AE, Haussen DC, Jadhav AP, Froehler MT, et al. Impact of balloon guide catheter use on clinical and angiographic outcomes in the STRATIS stroke thrombectomy registry. Stroke. (2019) 50:697–704. doi: 10.1161/STROKEAHA.118.022987
10. Lapergue B, Blanc R, Guedin P, Decroix JP, Labreuche J, Preda C, et al. A direct aspiration, first pass technique (ADAPT) versus stent retrievers for acute stroke therapy: an observational comparative study. AJNR. (2016) 37:1860–5. doi: 10.3174/ajnr.A4840
11. Tomasello A, Gramegna LL, Vega P, Castano C, Moreu M, Dominguez C, et al. Mechanical thrombectomy with a new intermediate balloon catheter combining the BGC and DAC features: Initial clinical experience with the iNedit device. Interv Neuroradiol. (2023) 15910199231207407. doi: 10.1177/15910199231207407
12. Liebeskind DS, Bracard S, Guillemin F, Jahan R, Jovin TG, Majoie CB, et al. eTICI reperfusion: defining success in endovascular stroke therapy. J Neurointerv Surg. (2019) 11:433–8. doi: 10.1136/neurintsurg-2018-014127
13. Garcia-Tornel A, Requena M, Rubiera M, Muchada M, Pagola J, Rodriguez-Luna D, et al. When to stop. Stroke. (2019) 50:1781–8. doi: 10.1161/STROKEAHA.119.025088
14. Rodriguez-Calienes A, Siddiqui FM, Galecio-Castillo M, Mohammaden MH, Dolia JN, Grossberg JA, et al. Rescue therapy for failed mechanical thrombectomy in acute ischemic stroke: a pooled analysis of the society of vascular and interventional neurology registry. Ann Neurol. (2024) 96:343–55. doi: 10.1002/ana.26967
15. Zaidat OO, Bozorgchami H, Ribo M, Saver JL, Mattle HP, Chapot R, et al. Primary results of the multicenter ARISE II study (analysis of revascularization in ischemic stroke with EmboTrap). Stroke. (2018) 49:1107–15. doi: 10.1161/STROKEAHA.117.020125
16. Ospel JM, McTaggart R, Kashani N, Psychogios M, Almekhlafi M, Goyal M. Evolution of stroke thrombectomy techniques to optimize first-pass complete reperfusion. Semin Intervent Radiol. (2020) 37:119–31. doi: 10.1055/s-0040-1709153
17. Mohammaden MH, Haussen DC, Al-Bayati AR, Hassan A, Tekle W, Fifi J, et al. Stenting and angioplasty in neurothrombectomy: matched analysis of rescue intracranial stenting versus failed thrombectomy. Stroke. (2022) 53:2779–88. doi: 10.1161/STROKEAHA.121.038248
18. Nogueira RG, Frei D, Kirmani JF, Zaidat O, Lopes D, Turk AS III, et al. Safety and efficacy of a 3-dimensional stent retriever with aspiration-based thrombectomy vs aspiration-based thrombectomy alone in acute ischemic stroke intervention: a randomized clinical trial. JAMA Neurol. (2018) 75:304–11. doi: 10.1001/jamaneurol.2017.3967
19. Sekhar LN, Schramm VL Jr, Jones NF, Yonas H, Horton J, Latchaw RE, et al. Operative exposure and management of the petrous and upper cervical internal carotid artery. Neurosurgery. (1986) 19:967–82. doi: 10.1227/00006123-198612000-00012
Keywords: mechanical thrombectomy, acute ischemic stroke, balloon guide catheter, distal aspiration catheter, endovascular stroke treatment
Citation: San Román L, Gramegna LL, Pich S, Domingo-Rodriguez L, Duran M, Duocastella L and Macho J (2025) First prospective, single-arm, multicenter study to evaluate safety and efficacy of the overall thrombectomy system -iNedit, iNdeep, and iNtercept- for acute ischemic stroke. Rationale beyond the study. Front. Neurol. 16:1537008. doi: 10.3389/fneur.2025.1537008
Received: 29 November 2024; Accepted: 17 February 2025;
Published: 05 March 2025.
Edited by:
Patricia Martínez Sánchez, Torrecárdenas University Hospital, SpainReviewed by:
Jacopo Scaggiante, Gemelli Hospital, ItalyCopyright © 2025 San Román, Gramegna, Pich, Domingo-Rodriguez, Duran, Duocastella and Macho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juan Macho, anVhbm1hY2hvQHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.