 Qian Yu1,2†
Qian Yu1,2† Yuan Tian
Yuan Tian Furong Zhao
Furong Zhao Zhining Liu
Zhining Liu- 1Huludao Central Hospital Teaching Base of Jinzhou Medical University, Liaoning, China
- 2Liaoning Provincial Key Laboratory of Clinical Oncology Metabonomics, The First Affiliated Hospital of Jinzhou Medical University, Jinzhou, China
- 3Fenyang College of Shanxi Medical University, Fenyang, China
- 4Clinical Research Department, Dalian Boyuan Medical Technology Co., Ltd, Dalian, China
- 5Department of Laboratory Medicine, General Hospital of Fushun Mining Bureau of Liaoning Health Industry Group, Fushun, China
- 6Ultrasound Department, The First Affiliated Hospital of Jinzhou Medical University, Jinzhou, China
Background: Stroke is a leading cause of disability and mortality worldwide, with rising incidence rates among youths and young adults aged 15–39 years. However, comprehensive assessments of stroke burden in this age group at global, regional, and national levels are limited. This study examines trends in stroke incidence, mortality, and disability-adjusted life years (DALYs) from 1990 to 2021 using data from the Global Burden of Disease (GBD) study.
Methods: Data from the GBD study (1990–2021) were analyzed to assess the age-standardized incidence, mortality, and DALYs related to stroke in individuals aged 15–39 years. The relationship between stroke burden and the Socio-Demographic Index (SDI) was explored across 204 countries and 21 regions. Trends were analyzed using the estimated annual percentage change (EAPC) and average annual percentage change (AAPC).
Results: This study reveals global, regional, and national trends in stroke burden among youths and young adults (15–39 years) from 1990 to 2021. In 2021, the global age-standardized stroke incidence was 757,234.61 cases, with 8.72 million DALYs and 122,742 stroke-related deaths. Although global incidence increased by 19.09%, age-standardized rates (ASRs) declined by 0.67% annually. DALYs and mortality rates also decreased globally. Notably, stroke burden increased in low and low-middle SDI regions. South Asia had the highest number of cases, while Oceania reported the highest mortality rate. These findings underscore regional disparities in stroke trends. Globally, metabolic risks (46.2%) and high systolic blood pressure (37.87%) are major contributors to stroke-related mortality.
Introduction
Stroke is a major global health concern, contributing substantially to disability and premature mortality (1, 2). From 1990 to 2019, the age-standardized DALYs rate (ASDR) of stroke decreased by 36.0% globally, yet the absolute DALYs increased by 32.0% (3). While traditionally considered a disease of older populations, stroke among youths and young adults (15–39 years) has gained increasing attention due to its rising incidence, distinct etiologies, and significant socioeconomic burden (4, 5). Young stroke survivors often face long-term disabilities, reduced quality of life, and significant socioeconomic burdens, resulting in substantial societal and economic challenges for both the individuals and their communities (6).
Previous studies have reported regional disparities in stroke burden, with variations driven by factors such as lifestyle changes, healthcare access, and socioeconomic development (7). The Global Burden of Disease (GBD) study provides a valuable framework for assessing these trends by analyzing age-standardized prevalence, mortality, and disability-adjusted life years (DALYs) for stroke (8, 9, 10).Evidence shows regional variations and an increasing prevalence of stroke among young individuals, especially in low- and middle-SDI regions (11). However, the burden of stroke in these areas is aggravated by a lack of targeted interventions, limited healthcare access, and insufficient awareness of stroke risk factors. Understanding these trends is critical for developing effective public health policies and interventions tailored to youths and young adults at risk (12).
This study aims to analyze the global, regional, and national burden of stroke among youths and young adults aged 15–39 years from 1990 to 2021 using GBD data. We seek to identify patterns in incidence, mortality, and DALYs, explore associations with the Socio-Demographic Index, and evaluate temporal trends to inform future strategies for stroke prevention and management in this population.
Methods
Overview and data collection
This cross-sectional study was approved by Jinzhou Medical University. The university’s ethics committee waived the requirement for informed consent, as the study involved only data analysis with no personally identifiable information.
The data on youth and young adult stroke used in this study were derived from the Global Burden of Disease Study 2021 (GBD 2021), which provides comprehensive and up-to-date estimates for 369 diseases, injuries, and conditions across 204 countries and territories, as well as 88 risk factors (7, 13). The GBD 2021 classification system divides the world into 21 geographic regions based on epidemiological similarities and geographical proximity. This regional categorization enables a nuanced understanding of disease burden variations across different parts of the world, thereby facilitating the development of targeted public health policies and interventions (10, 14). The 21 regions considered are as follows: Andean Latin America, Australasia, the Caribbean, Central Asia, Central Europe, Central Latin America, Central Sub-Saharan Africa, East Asia, Eastern Europe, Eastern Sub-Saharan Africa, High-Income Asia Pacific, High-Income North America, North Africa and the Middle East, Oceania, South Asia, Southeast Asia, Southern Latin America, Southern Sub-Saharan Africa, Tropical Latin America, Western Europe, and Western Sub-Saharan Africa. This classification has consistently been utilized in previous GBD iterations and has proven effective in analyzing and comparing health metrics across different geographic and epidemiological regions (7, 10, 14).
For this study, we specifically extracted data on young stroke, focusing on metrics such as incidence, mortality, and disability-adjusted life years (DALYs) to provide a detailed analysis of the burden of stroke among youths and young adults. All data used in this study is publicly accessible through the Global Health Data Exchange platform.1 The study was conducted in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (15).
Sociodemographic index
The Sociodemographic index is a composite measure of a country’s or region’s level of development, incorporating indicators such as fertility rates, educational attainment, and per capita income. SDI values range from 0 to 1, with higher scores reflecting greater socioeconomic development. Previous studies have demonstrated an association between SDI and both disease incidence and mortality rates (16). In this study, we classified countries and regions into five SDI categories (low, low-medium, medium, medium-high, and high) to investigate the relationship between socioeconomic development and the burden of stroke in youths and young adults aged 15–39 years from 1990 to 2021.
Statistical analysis
To assess the burden of stroke in youths and young adults, the primary indicators analyzed were incidence, mortality, and disability-adjusted life years (DALYs). Trends were interpreted based on the estimated annual percent change (EAPC) and its 95% confidence interval (CI): a negative upper limit of the EAPC indicated a decreasing trend, while a positive lower limit suggested an increasing trend (17, 18, 19).
In this study, ASRs for stroke incidence, mortality, and DALYs were calculated using direct standardization, with the GBD 2021 world standard population as the weighting factor. ASRs were reported per 100,000 population, accompanied by 95% uncertainty intervals (UI). To analyze trends in age-specific stroke incidence, mortality, and DALYs at global, regional, and national levels, GBDR analysis was used (20). JD_GBDR software was applied to assess trends from 1990 to 2021. The analysis calculated the average annual percentage change (AAPC) and its 95% CI. Trends were classified as upward (AAPC >0), downward (AAPC <0), or stable (95% CI includes 0). UIs, which differ from CIs by accounting for uncertainties from multiple sources such as sampling error, model estimation, and specification, were also computed (21).
In this study, the R software package (version 4.2.3) and JD_GBDR (V2.22, Jingding Medical Technology Co., Ltd.) were used for the drawing of the figures.
Results
Global trends in stroke incidence, mortality and DALY rate
In 2021, the global age-standardized incidence of stroke was 757,234.61 cases (95% UI: 632,119.62–924,338.12) (Table 1). The age-standardized disability-adjusted life years (DALYs) due to stroke totaled 8,718,567.32 (95% UI: 7,951,154.52–9,472,143.29) (Supplementary Table S1), while age-standardized stroke-related deaths were 122,742.66 (95% UI: 113,243.10–133,292.05) (Table 2). From 1990 to 2021, the global age-standardized incidence of stroke increased by 19.09% (95% UI: 13.56–24.02%). Despite this rise, the incidence rate declined from 29.01 (95% UI: 24.22–35.16) in 1990 to 25.45 (95% UI: 21.25–31.07) in 2021, with an estimated annual percentage change (EAPC) of −0.67 (95% CI: −0.76, −0.58) (Table 1). Over the same period, the age-standardized DALY burden decreased by 5.47%, and age-standardized mortality fell by 8.16%. Additionally, age-standardized mortality rates showed a significant reduction (AAPC = −0.065; 95% CI: −0.068, −0.063), as did age-standardized DALY rates (AAPC = −4.176; 95% CI: −4.301, −4.052) (Table 2; Supplementary Table S1).
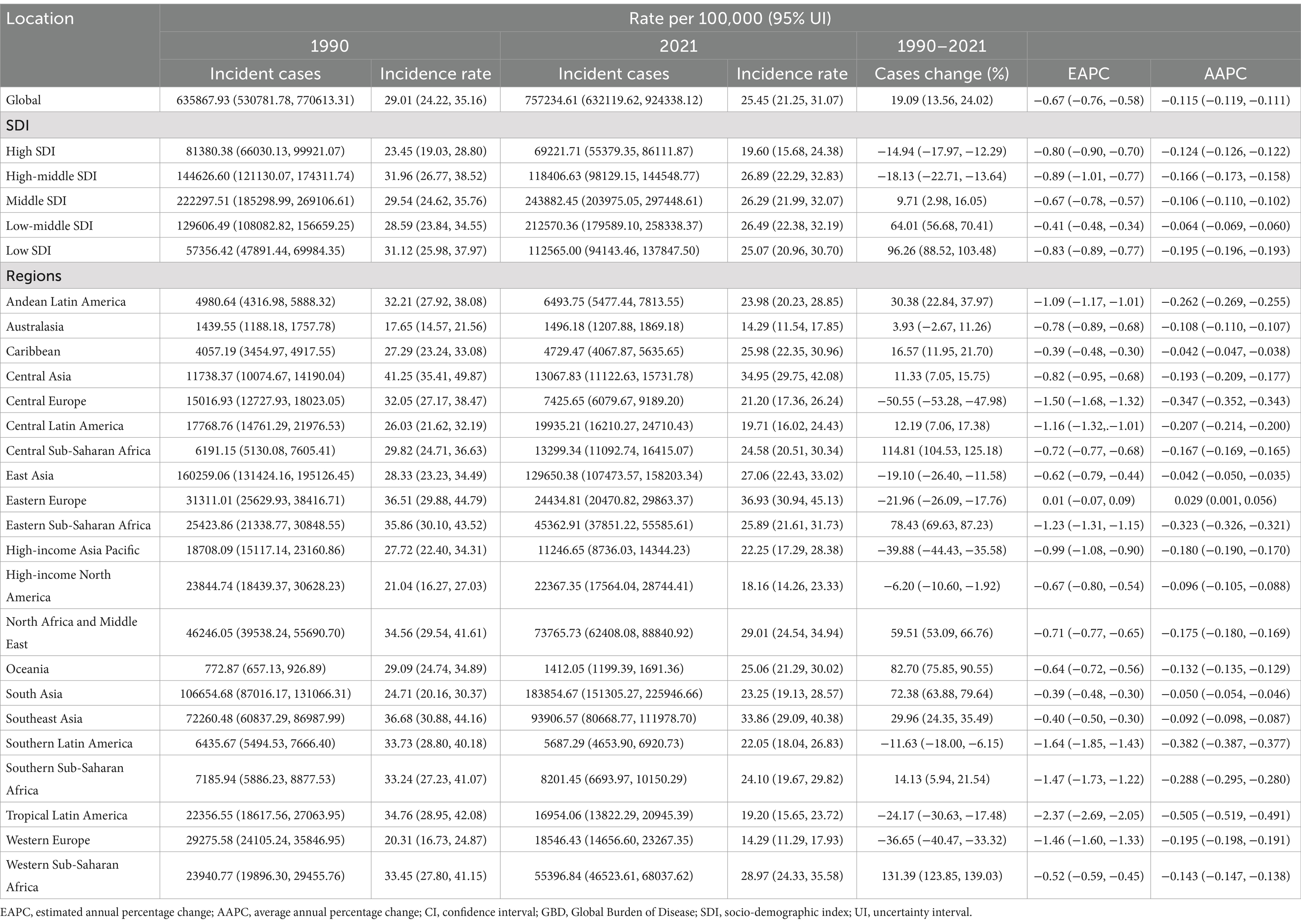
Table 1. Age-standardized incidence and AAPC of stroke in individuals aged 15–39 years at global and regional levels, 1990–2021.
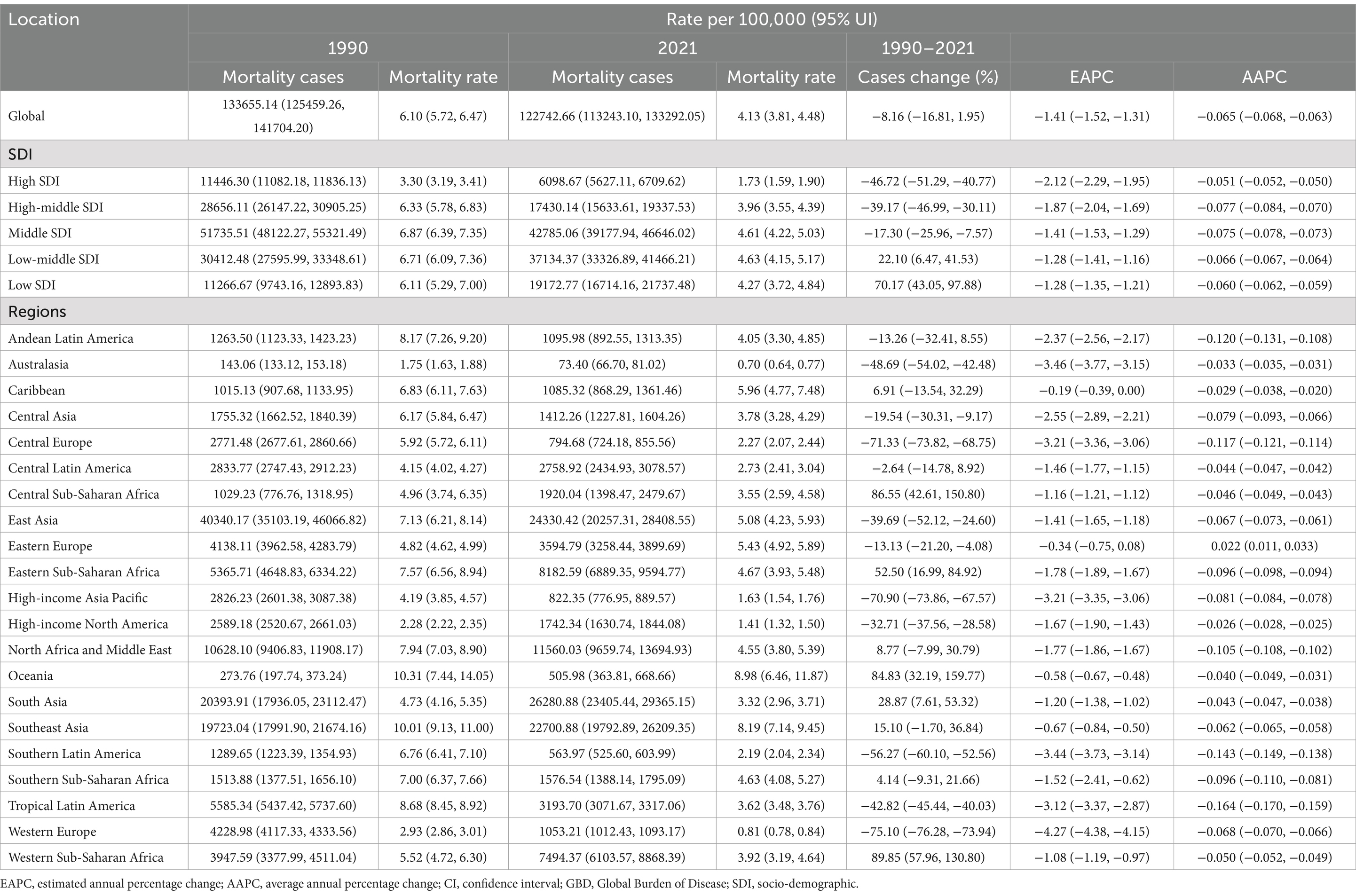
Table 2. Age-standardized morality rate and AAPC of stroke in individuals aged 15–39 years at global and regional levels, 1990–2021.
Regional trend in stroke incidence, mortality and DALY rate in five SDI regions
From 1990 to 2021, both mortality and DALY cases increased in the low-middle and low-SDI regions. In the low-middle SDI group, mortality rose by 22.10% (95% UI: 6.47–41.53%) (Table 2), and DALYs increased by 25.77% (95% UI: 11.05–43.12%) (Supplementary Table S1). In the low SDI group, mortality increased by 70.17% (95% UI: 43.05–97.88%) (Table 2), and DALYs rose by 75.36% (95% UI: 50.23–100.50%) (Supplementary Table S1). Despite these absolute increases, the average annual percentage change (AAPC) for age-standardized mortality and DALY rates was negative across all five SDI regions, indicating a reduction in age-standardized stroke mortality and DALY burdens over this period. In 2021, the middle SDI region had the highest number of stroke cases, with 243,882.45 (95% UI: 203,975.05-297,448.61), while the low SDI region saw a 96.26% increase in incidence (95% UI: 88.52–103.48%) (Table 1). The greatest reduction in stroke incidence among youths was observed in regions with high to mid-SDI (EAPC = −0.89, 95% CI: −1.01 to −0.77) (Table 1).
Regional trend in stroke incidence, mortality and DALY rate in 21 GBD regions
In terms of incidence, South Asia had the highest number of stroke cases in youths and young adults aged 15–39 years in 2021, with 183,854.67 cases (95% UI: 151,305.27–225,946.66), while Oceania had the fewest, with 1,412.05 cases (95% UI: 1,199.39–1,691.36). The highest stroke incidence rate among youths and young adults was observed in Eastern Europe (36.93; 95% UI: 30.94–45.13). In contrast, Australasia and Western Europe had the lowest stroke incidence rates, both at 14.29 (95% UI: 11.54–17.85 and 95% UI: 11.29–17.93, respectively). From 1990 to 2021, the incidence rate of stroke in youths and young adults increased only in Eastern Europe (EAPC: 0.01; 95% CI: −0.07–0.09). The largest decline in stroke incidence was seen in the High-income Asia Pacific region (EAPC: -2.06; 95% CI: −2.17 to −1.94) (Table 1).
In 2021, East Asia had the highest number of stroke-related deaths among youths and young adults aged 15–39 years, with 24,330.42 deaths (95% UI: 20,257.31–28,408.55). Oceania had the highest stroke-related mortality rate for youths and young adults (8.98; 95% UI: 6.46–11.87). The Caribbean experienced the smallest decrease in stroke-related mortality rate (EAPC: −0.19; 95% CI: −0.39 to 0.00), while Australasia saw the largest reduction (EAPC: −3.46; 95% CI: −3.77 to −3.15) (Table 2).
In 2021, South Asia had the highest number of disability-adjusted life years (DALYs) related to stroke in youths and young adults (1,837,332.75; 95% UI, 1,622,972.92–2,033,261.45), while Australasia had the lowest (7,611.68; 95% UI, 6,516.81–8,696.71). Oceania reported the highest DALY rate (599.51; 95% UI, 452.16–778.14), while Australasia had the lowest DALY rate (72.69; 95% UI, 62.24–83.06) (Table 1). Figure 1 shows a negative correlation between the age-standardized prevalence rate, mortality rate, and disability-adjusted life years (DALY) rate for young stroke in youths and young adults aged 15–39 years and the Socio-Demographic Index (SDI). In 2021, the global SDI was 0.37. Eight regions, including Eastern Europe, Southeast Asia, and High-Income North America, had prevalence rates higher than the global average (Figure 1A), while another eight regions exceeded the global average mortality rate (Figure 1B). Additionally, eight regions reported DALY rates above the global average (Figure 1C).
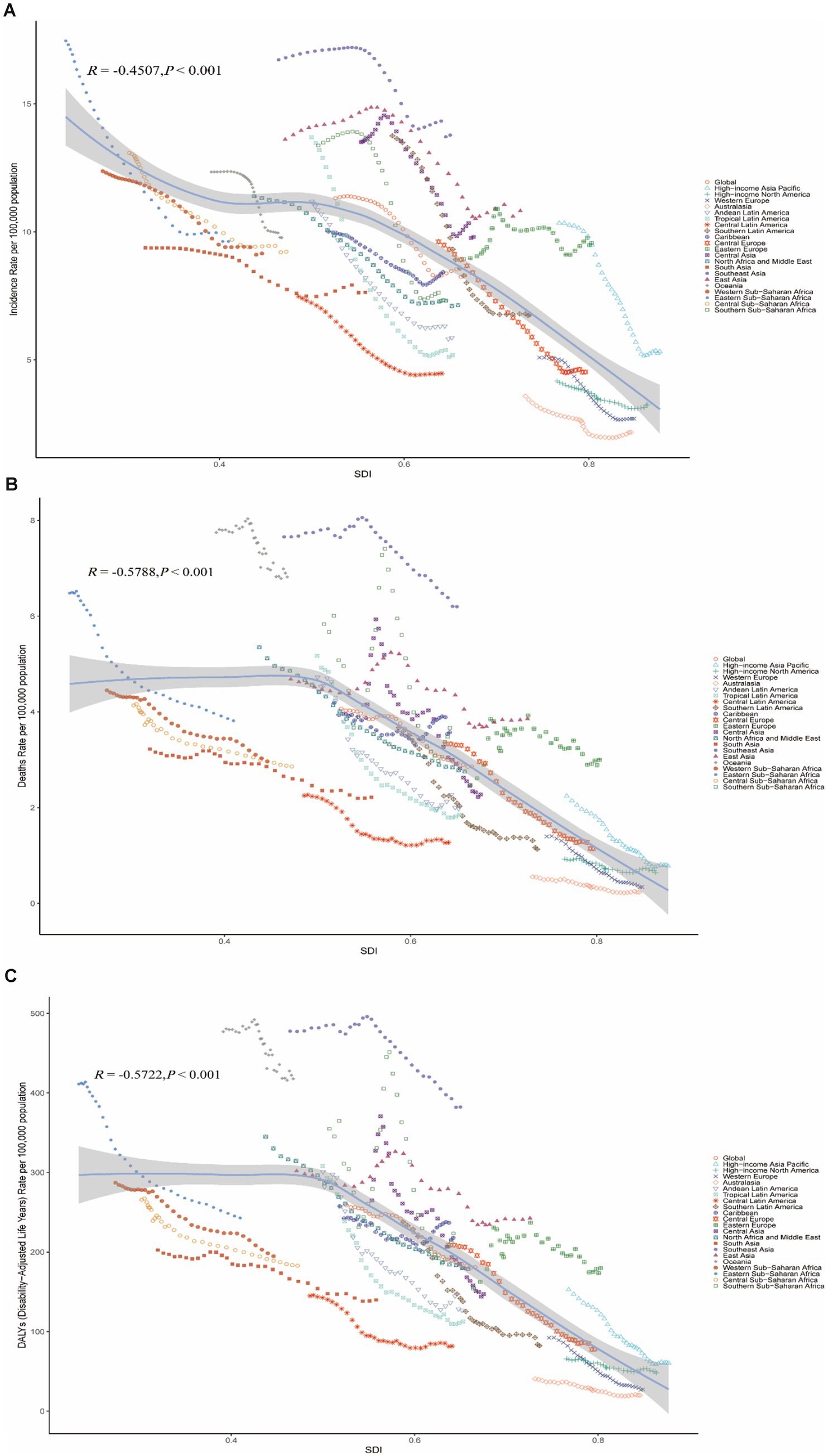
Figure 1. The association between the socio-demographic index and young stroke in youths and young adults aged 15–39 years across 21 GBD regions. (A) The relationship between age-standardized stroke incidence and socio-demographic index. (B) The relationship between age-standardized stroke mortality and socio-demographic index. (C) The relationship between age-standardized stroke disability-adjusted life years and socio-demographic index.
National trend in stroke incidence, mortality and DALY rate
From 1990 to 2021, the global incidence of stroke among individuals aged 15 to 39 varied significantly across countries. In 2021, India reported the highest number of young stroke cases at 131,103.66 (95% UI, 106,504.02–162,808.88) among the 204 countries analyzed, while Tokelau had the lowest incidence, with just 0.19 cases per 100,000 people (95% UI, 0.17–0.22). Kiribati recorded the highest incidence rate of young stroke cases in 2021, at 97.8 per 100,000 people (95% UI, 88.46–107.52), while Portugal had the lowest rate, at 11.39 per 100,000 people (95% UI, 8.65–15.01). The Philippines saw the largest increase in incidence (EAPC, 2.23; 95% CI, 1.92–2.54), while Rwanda experienced the greatest decrease (EAPC, −3.16; 95% CI, −3.50 to −2.81). The global incidence rate for young stroke in 2021 was 25.45 per 100,000 people (95% UI, 21.25–31.07), with 101 countries reporting rates above and 103 countries below the global average (Supplementary Table S2; Figure 2A).
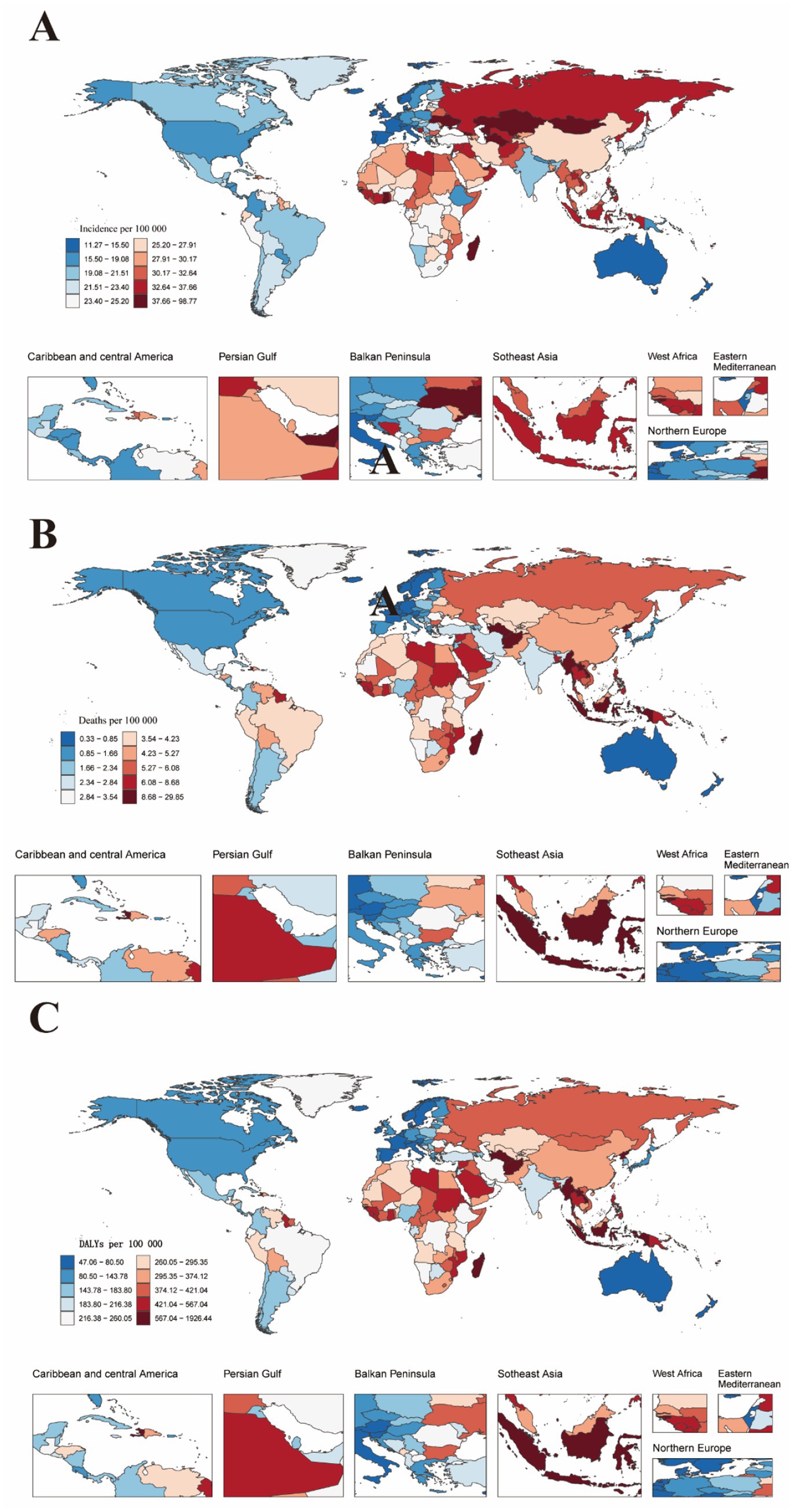
Figure 2. Global maps showing the age-standardized incidence rate, mortality rate, and DALYs rate of stroke in youths and young adults aged 15–39 years for both sexes in 2021. DALYs refer to disability-adjusted life years. (A) Age-standardized incidence rates of stroke in youths and young adults aged 15–39 years for both sexes combined across 204 countries worldwide. (B) Age-standardized mortality rates of stroke in youths and young adults aged 15–39 years for both sexes combined across 204 countries worldwide. (C) Age-standardized disability-adjusted life years rates of stroke in youths and young adults aged 15–39 years for both sexes combined across 204 countries worldwide.
In 2021, China reported the highest number of stroke-related deaths among youths and young adults, with 23,099.87 cases (95% UI, 19,113.48–27,336.47). Nauru had the highest stroke-related mortality rate for this age group, at 29.56 per 100,000 people (95% CI, 21.22–42.56), while Slovenia (SDI 0.84) recorded the lowest rate at 0.33 per 100,000 people (95% CI, 0.27–0.41). Zimbabwe experienced the largest increase in mortality (EAPC, 4.72; 95% CI, 3.56–5.90), while Luxembourg (EAPC, −7.39; 95% CI, −7.73 to −7.06) and Slovenia (EAPC, −6.67; 95% CI, −6.96 to −6.39) showed the greatest decreases. The global stroke-related mortality rate for youths and young adults in 2021 was 4.13 per 100,000 people (95% UI, 3.81–4.48), with 87 countries reporting rates above the global average and 117 countries below it (Supplementary Table S3; Figure 2B).
In 2021, China had the highest number of stroke-related disability-adjusted life years (DALYs) among youths and young adults, totaling 1,654,368.25 (95% UI, 1,394,426.09–1,906,661.45). Nauru recorded the highest DALY rate for young stroke cases, at 1,907.37 per 100,000 people (95% UI, 1,411.15–2,672.63). Zimbabwe experienced the largest increase in DALY rate (EAPC, 3.97; 95% CI, 2.99–4.96), while Luxembourg (EAPC, −5.64; 95% CI, −5.89 to −5.38) and Rwanda (EAPC, −5.33; 95% CI, −5.94 to −4.72) showed the greatest decreases. In 2021, the global DALY rate for young stroke cases was 293.08 per 100,000 people (95% UI, 267.28–318.41), with 86 countries/regions reporting rates above the global average and 118 countries/regions below it (Supplementary Table S4; Figure 2C).
Factors influencing EAPCs
EAPCs showed significant differences compared to the incidence, mortality, and disability-adjusted life years rates in 2021. Furthermore, there were also notable differences between EAPCs and the 2021 Socio-Demographic Index. Specifically, EAPCs were positively correlated with DALY rates (Pearson r = 0.54; p < 0.001), and they also exhibited positive correlations with incidence rates (Pearson r = 0.51; p < 0.001) and mortality rates (Pearson r = 0.56; p < 0.001). In contrast, the EAPCs for incidence, mortality, and DALYs were negatively correlated with the SDI (Supplementary Figure S1).
Stroke-related deaths attributable to major risk factors by SDI level
The results highlight the proportion of stroke-related deaths in youths and young adults aged 15–39 years for both sexes attributable to various risk factors, both globally and across different Socio-Demographic Index levels: High, High-Middle, Middle, Low-Middle, and Low SDI. The key risk factors analyzed include ambient air pollution, high sodium intake, low fruit intake, tobacco use, and exposure to secondhand smoke. Globally, metabolic risks (46.2%) and high systolic blood pressure (37.87%) are major contributors to stroke-related mortality in youths and young adults aged 15–39 years for both sexes. The impact of these risk factors varies by SDI level: low SDI regions are predominantly affected by environmental and occupational risks as well as metabolic factors, while high SDI regions experience a greater influence from behavioral and metabolic risks. These findings highlight the distinct public health challenges faced by different socio-economic groups and emphasize the need for targeted intervention strategies (Supplementary Figure S2).
Discussion
This study provides a comprehensive analysis of the global, regional, and national trends in stroke incidence, mortality, and disability-adjusted life years among youths and young adults aged 15–39 years from 1990 to 2021. Our findings reveal significant variations in stroke burden across different SDI regions, with notable disparities between high and low SDI regions.
Global trends
During the study period, the global age-standardized incidence of stroke increased by 19.09%, reflecting a growing global burden of stroke. From 1990 to 2021, both the global incidence rate and the prevalence of stroke in the general population rose by over 70%, which aligns with our findings. However, despite this increase, the age-standardized stroke incidence showed a gradual decline, with an estimated annual percentage change of −0.67, indicating a decrease in overall incidence relative to the global population (22). This suggests that while the burden of stroke continues to rise, the rate of incidence has been stabilizing over time. Notably, in 2021, the global stroke incidence continued to increase, further highlighting the ongoing global burden (23).
Regional trends
At the regional level, the low-middle and low SDI regions experienced a significant rise in both mortality and DALYs, with mortality increasing by 22.10 and 70.17%, highlighting the growing health challenge posed by stroke in low-resource settings (24). These increases are likely driven by limited healthcare infrastructure, insufficient stroke prevention programs, delayed access to acute care, and cultural and lifestyle factors such as high-salt and high-fat diets, sedentary lifestyles, and higher rates of smoking and alcohol consumption. These challenges, compounded by inadequate access to healthcare education, significantly exacerbate the risk of stroke and emphasize the urgent need for targeted prevention strategies (25).
In low SDI regions, where the increase in stroke burden is most pronounced, implementing targeted prevention strategies, improving healthcare infrastructure, and enhancing access to treatment are critical to reducing the burden (26, 27). Despite the absolute increase in stroke burden, the negative average annual percentage change for both mortality and DALY rates across all SDI regions reflects a decline in age-standardized rates over time, particularly in high-SDI regions. Addressing these disparities in low-resource settings is essential to prevent further escalation of the stroke burden and improve health outcomes in these populations (28).
National trends
At the national level, India reported the highest number of stroke cases among youths and young adults in 2021, reflecting the country’s high population density and the rising burden of non-communicable diseases. In contrast, countries like Tokelau recorded the lowest incidence rates, likely due to a smaller population and specific regional health factors. The Philippines experienced the largest increase in stroke incidence, while Rwanda saw the greatest decline, potentially reflecting differences in national health policies, healthcare system improvements, and increased awareness of stroke risk factors.
The wide variability in stroke incidence, mortality, and DALYs among countries highlights disparities in healthcare access, quality, and stroke prevention efforts (29). Nations with high stroke incidence and mortality, such as Zimbabwe, could benefit from intensified stroke prevention, early detection, and treatment initiatives. Conversely, countries with significant declines in stroke-related outcomes, like Luxembourg and Rwanda, demonstrate how enhancements in healthcare infrastructure and stroke management can improve outcomes for youths and young adults (1).
Stroke incidence and mortality trends by region
The regional analysis shows that Eastern Europe had the highest stroke incidence rate, indicating a heavy burden of stroke due to factors such as high rates of smoking, unhealthy diets, and limited healthcare access. In contrast, Australasia and Western Europe reported the lowest incidence rates, likely due to better healthcare systems and effective preventive measures. The High-Income Asia Pacific region experienced the largest decline in stroke incidence, reflecting the impact of strong healthcare systems, public health initiatives, and improved stroke care. Significant disparities were also noted in stroke-related mortality and DALY rates, with Oceania recording the highest figures, potentially linked to higher obesity and hypertension rates as well as restricted healthcare access (30, 31).
Implications for public health
The findings of this study have important public health implications. First, targeted stroke prevention programs are essential, particularly in low-middle and low SDI regions where the burden is rising (32). These programs should focus on managing key risk factors such as hypertension, diabetes, and smoking, while also considering the influence of cultural and socioeconomic factors on health behaviors and access to care. Second, improving healthcare infrastructure and access to acute stroke care in low-resource regions is critical to reducing stroke mortality and DALYs (33). Economic disparities limit access to advanced treatments, widening the gap in outcomes. Countries with strong healthcare systems, such as those in Western Europe, have successfully reduced stroke-related mortality and DALY rates through effective policies, early detection, and emergency response systems, providing valuable models for other regions.
Finally, ongoing research and surveillance are needed to track stroke trends and assess intervention effectiveness. Policy measures, including tobacco control, dietary regulations, and expanded healthcare coverage, can help mitigate regional disparities. Further studies should examine the interplay of economic development, healthcare policies, and cultural factors to inform tailored strategies (34, 35).
Limitations
This study has several limitations. First, the analysis relies on data from the GBD study, which may be affected by reporting inconsistencies and data quality issues, especially in regions with limited healthcare infrastructure. Second, while the study includes ASRs, it does not fully account for potential confounders such as socioeconomic status, healthcare access, and lifestyle factors, which could influence stroke incidence and outcomes. Additionally, the use of estimated data and uncertainty intervals may introduce variability in the results, particularly in regions with sparse data. Finally, the study does not explore underlying causes or specific risk factors for stroke, limiting the understanding of its etiology in different populations.
Conclusion
In conclusion, this study provides a detailed assessment of the burden of stroke among youths and young adults globally, regionally, and nationally. While the global trend shows a decline in age-standardized stroke incidence, mortality, and DALYs, significant disparities persist across SDI regions and countries. Addressing these disparities through targeted prevention, improved healthcare access and better stroke management is essential to reducing the stroke burden, particularly in low and middle-income countries. Further research and policy interventions are needed to sustain these improvements and tackle the rising stroke burden in certain regions.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Jinzhou Medical University. The study was conducted in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
QY: Formal analysis, Writing – original draft, Writing – review & editing. YT: Data curation, Investigation, Methodology, Writing – original draft. NJ: Conceptualization, Writing – original draft. FZ: Conceptualization, Writing – review & editing. SW: Investigation, Methodology, Writing – review & editing. MS: Conceptualization, Writing – review & editing. ZL: Conceptualization, Project administration, Writing – original draft. XL: Conceptualization, Data curation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Nature Science Foundation of Liaoning (grant number 2022-MS-460).
Conflict of interest
SW was employed by Clinical Research Department, Dalian Boyuan Medical Technology Co., Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1535278/full#supplementary-material
Footnotes
References
1. Luo, Z, Shan, S, Cao, J, Zhou, J, Zhou, L, Jiang, D, et al. Temporal trends in cross-country inequalities of stroke and subtypes burden from 1990 to 2021: a secondary analysis of the global burden of disease study 2021. EClinicalMedicine. (2024) 76:102829. doi: 10.1016/j.eclinm.2024.102829
2. Mead, GE, Sposato, LA, Sampaio Silva, G, Yperzeele, L, Wu, S, Kutlubaev, M, et al. A systematic review and synthesis of global stroke guidelines on behalf of the world stroke organization. Int J Stroke. (2023) 18:499–531. doi: 10.1177/17474930231156753
3. Feigin, VL, Brainin, M, Norrving, B, Martins, S, Sacco, RL, Hacke, W, et al.Corrigendum to: world stroke organization (WSO): global stroke fact sheet 2022. Int J Stroke. (2022) 17:478. doi: 10.1177/17474930221080343
4. Fraser, S, Pabst, L, and Smith, F. Stroke in the young. Curr Opin Neurol. (2023) 36:131–9. doi: 10.1097/WCO.0000000000001145
5. Perera, KS, de Sa Boasquevisque, D, Rao-Melacini, P, Taylor, A, Cheng, A, Hankey, GJ, et al. Evaluating rates of recurrent ischemic stroke among young adults with embolic stroke of undetermined source: the young ESUS longitudinal cohort study. JAMA Neurol. (2022) 79:450–8. doi: 10.1001/jamaneurol.2022.0048
6. Du, M, Mi, D, Liu, M, and Liu, J. Global trends and regional differences in disease burden of stroke among children: a trend analysis based on the global burden of disease study 2019. BMC Public Health. (2023) 23:2120. doi: 10.1186/s12889-023-17046-z
7. Tuo, Y, Li, Y, Li, Y, Ma, J, Yang, X, Wu, S, et al. Global, regional, and national burden of thalassemia, 1990-2021: a systematic analysis for the global burden of disease study 2021. EClinicalMedicine. (2024) 72:102619. doi: 10.1016/j.eclinm.2024.102619
8. Roth, GA, Mensah, GA, Johnson, CO, Addolorato, G, Ammirati, E, Baddour, LM, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 76:2982–3021. doi: 10.1016/j.jacc.2020.11.010
9. Krishnamurthi, RV, Ikeda, T, and Feigin, VL. Global, regional and country-specific burden of Ischaemic stroke, intracerebral Haemorrhage and subarachnoid Haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. (2020) 54:171–9. doi: 10.1159/000506396
10. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet (London, England). (2020) 396:1204–22. doi: 10.1016/S0140-6736(20)30925-9
11. Wang, Y, Liang, J, Fang, Y, Yao, D, Zhang, L, Zhou, Y, et al. Burden of common neurologic diseases in Asian countries, 1990-2019: an analysis for the global burden of disease study 2019. Neurology. (2023) 100:e2141–54. doi: 10.1212/WNL.0000000000207218
12. Singhal, AB, Biller, J, Elkind, MS, Fullerton, HJ, Jauch, EC, Kittner, SJ, et al. Recognition and management of stroke in young adults and adolescents. Neurology. (2013) 81:1089–97. doi: 10.1212/WNL.0b013e3182a4a451
13. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet (London, England). (2020) 396:1223–49. doi: 10.1016/S0140-6736(20)30752-2
14. Safiri, S, Nejadghaderi, SA, Karamzad, N, Carson-Chahhoud, K, Bragazzi, NL, Sullman, MJM, et al. Global, regional, and national cancer deaths and disability-adjusted life-years (DALYs) attributable to alcohol consumption in 204 countries and territories, 1990-2019. Cancer. (2022) 128:1840–52. doi: 10.1002/cncr.34111
15. Mathew, G, Agha, R, Albrecht, J, Goel, P, Mukherjee, I, Pai, P, et al. STROCSS 2021: strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg. (2021) 96:106165. doi: 10.1016/j.ijsu.2021.106165
16. GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study, 2021. Lancet Rheumatol. (2023) 5:e316–29. doi: 10.1016/S2665-9913(23)00098-X
17. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet (London, England). (2015) 385:117–71. doi: 10.1016/S0140-6736(14)61682-2
18. Zhang, J, Zhu, S, Liu, C, Hu, Y, Yang, A, Zhang, Y, et al. Global, regional and national burden of ischemic stroke attributed to high low-density lipoprotein cholesterol, 1990-2019:a decomposition analysis and age-period-cohort analysis. J Cereb Blood Flow Metab. (2024) 44:527–41. doi: 10.1177/0271678X231211448
19. Yang, Y, Fu, WJ, and Land, KC. A methodological comparison of age-period-cohort models: the intrinsic estimator and conventional generalized linear models. Sociol Methodol. (2004) 34:75–110. doi: 10.1111/j.0081-1750.2004.00148.x
20. Kim, HJ, Fay, MP, Feuer, EJ, and Midthune, DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. (2000) 19:335–51. doi: 10.1002/(SICI)1097-0258(20000215)19:3<335::AID-SIM336>3.0.CO;2-Z
21. GBD 2015 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet (London, England). (2016) 388:1603–58. doi: 10.1016/S0140-6736(16)31460-X
22. GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. (2021) 20:795–820. doi: 10.1016/S1474-4422(21)00252-0
23. Li, XY, Kong, XM, Yang, CH, Cheng, ZF, Lv, JJ, Guo, H, et al. Global, regional, and national burden of ischemic stroke, 1990-2021: an analysis of data from the global burden of disease study 2021. EClinicalMedicine. (2024) 75:102758. doi: 10.1016/j.eclinm.2024.102758
24. Marshall, IJ, Wang, Y, Crichton, S, McKevitt, C, Rudd, AG, and Wolfe, CD. The effects of socioeconomic status on stroke risk and outcomes. Lancet. Neurol. (2015) 14:1206–18. doi: 10.1016/S1474-4422(15)00200-8
25. Park, WB, Cho, JS, Shin, SD, Kong, SY, Kim, JJ, Lim, YS, et al. Comparison of epidemiology, emergency care, and outcomes of acute ischemic stroke between young adults and elderly in Korean population: a multicenter observational study. J Korean Med Sci. (2014) 29:985–91. doi: 10.3346/jkms.2014.29.7.985
26. Langhorne, P, O'Donnell, MJ, Chin, SL, Zhang, H, Xavier, D, Avezum, A, et al. Practice patterns and outcomes after stroke across countries at different economic levels (INTERSTROKE): an international observational study. Lancet (London, England). (2018) 391:2019–27. doi: 10.1016/S0140-6736(18)30802-X
27. Jayatilleke, K. Challenges in implementing surveillance tools of high-income countries (HICs) in low middle income countries (LMICs). Curr Treat Options Infect Dis. (2020) 12:191–201. doi: 10.1007/s40506-020-00229-2
28. Khatib, R, Jawaada, AM, Arevalo, YA, Hamed, HK, Mohammed, SH, and Huffman, MD. Implementing evidence-based practices for acute stroke Care in low- and Middle-Income Countries. Curr Atheroscler Rep. (2017) 19:61. doi: 10.1007/s11883-017-0694-6
29. Thayabaranathan, T, Kim, J, Cadilhac, DA, Thrift, AG, Donnan, GA, Howard, G, et al. Global stroke statistics 2022. Int J Stroke. (2022) 17:946–56. doi: 10.1177/17474930221123175
30. O'Donnell, MJ, Chin, SL, Rangarajan, S, Xavier, D, Liu, L, Zhang, H, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet (London, England). (2016) 388:761–75. doi: 10.1016/S0140-6736(16)30506-2
31. Lynch, EA, Bulto, LN, Cheng, H, Craig, L, Luker, JA, Bagot, KL, et al. Interventions for the uptake of evidence-based recommendations in acute stroke settings. Cochrane Database Syst Rev. (2023) 8:CD012520. doi: 10.1002/14651858.CD012520.pub2
32. Bhattacharya, P, Sarmah, D, Dave, KR, Goswami, A, Watanabe, M, Wang, X, et al. Stroke and stroke prevention in sickle cell anemia in developed and selected developing countries. J Neurol Sci. (2021) 427:117510. doi: 10.1016/j.jns.2021.117510
33. Krishnamurthi, RV, deVeber, G, Feigin, VL, Barker-Collo, S, Fullerton, H, Mackay, MT, et al. Stroke prevalence, mortality and disability-adjusted life years in children and youth aged 0-19 years: data from the global and regional burden of stroke 2013. Neuroepidemiology. (2015) 45:177–89. doi: 10.1159/000441087
34. Feigin, VL, and Owolabi, MO. Pragmatic solutions to reduce the global burden of stroke: a world stroke organization-lancet neurology commission. Lancet Neurol. (2023) 22:1160–206. doi: 10.1016/S1474-4422(23)00277-6
Keywords: stroke, risk factors, incidence, mortality, disability-adjusted life years
Citation: Yu Q, Tian Y, Jiang N, Zhao F, Wang S, Sun M, Liu Z and Liu X (2025) Global, regional, and national burden and trends of stroke among youths and young adults aged 15–39 years from 1990 to 2021: findings from the Global Burden of Disease study 2021. Front. Neurol. 16:1535278. doi: 10.3389/fneur.2025.1535278
Edited by:
Yannick Béjot, Centre Hospitalier Regional Universitaire De Dijon, FranceReviewed by:
Laura Amaya Pascasio, Complejo Hospitalario Torrecárdenas, SpainHongjing Yan, Handan First Hospital, China
Jinxin Zheng, Ruijin Hospital North, China
Khuzeima Khanbhai, Jakaya Kikwete Cardiac Institute (JKCI), Tanzania
Copyright © 2025 Yu, Tian, Jiang, Zhao, Wang, Sun, Liu and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Liu, bHl5NjYxMTJAMTYzLmNvbQ==; Zhining Liu, bGl1emhpbmluZ2Z1eWlAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
‡ORCID: Zhining Liu, orcid.org/0000-0002-2723-5999