 Diana Malaeb1*
Diana Malaeb1* Sara Mansour2
Sara Mansour2 Muna Barakat3Sarah Cherri2Zelal J. Kharaba4
Muna Barakat3Sarah Cherri2Zelal J. Kharaba4 Feras Jirjees4Reem Al Zayer5Eyman M. Eltayib6Zeinab Khidhair7Hala AlObaidi8
Feras Jirjees4Reem Al Zayer5Eyman M. Eltayib6Zeinab Khidhair7Hala AlObaidi8 Sami El Khatib9,10Ruth Alex1
Sami El Khatib9,10Ruth Alex1 Vineetha Menon1Basile Hosseini11Jinane Noureldine12,13Yassen Alfoteih14,15
Vineetha Menon1Basile Hosseini11Jinane Noureldine12,13Yassen Alfoteih14,15 Souheil Hallit16,17†Hassan Hosseini18,19†
Souheil Hallit16,17†Hassan Hosseini18,19†- 1College of Pharmacy, Gulf Medical University, Ajman, United Arab Emirates
- 2Lebanese International University, School of Pharmacy, Beirut, Lebanon
- 3Faculty of Pharmacy, Applied Science Private University, Amman, Jordan
- 4College of Pharmacy, University of Sharjah, Sharjah, United Arab Emirates
- 5Clinical Pharmacy Practice, Mohammed Al-Muna College for Medical Sciences, Dammam, Saudi Arabia
- 6College of Pharmacy, Jouf University, Sakaka, Saudi Arabia
- 7College of Science, University of Baghdad, Baghdad, Iraq
- 8School of Pharmacy, Queens University Belfast, Belfast, United Kingdom
- 9Department of Biomedical Sciences, Lebanese International University, Bekaa, Lebanon
- 10Center for Applied Mathematics and Bioinformatics (CAMB), Gulf University for Science and Technology, Mubarak Al-Abdullah, Kuwait
- 11Hospices Civils de Lyon, Lyon, France
- 12Rammal Hassan Rammal Research Laboratory, PhyToxE Research Group, Nabatieh, Lebanon
- 13Faculty of Sciences, Lebanese University, Nabatieh, Lebanon
- 14College of Dental Surgery, City University Ajman, Ajman, United Arab Emirates
- 15College of General Education, City University Ajman, Ajman, United Arab Emirates
- 16School of Medicine and Medical Sciences, Holy Spirit University of Kaslik, Jounieh, Lebanon
- 17Applied Science Research Center, Applied Science Private University, Amman, Jordan
- 18UPEC-University Paris-Est, Creteil, France
- 19RAMSAY SANTÉ, HPPE, Champigny sur Marne, France
Introduction: While several studies have examined stroke public knowledge and awareness in individual countries within the Middle East and North Africa (MENA) region, none have provided a comprehensive cross-country assessment.
Purpose: To assess public stroke knowledge and awareness among Arabic-speaking adults in seven MENA countries and identify associated factors.
Materials and methods: An online cross-sectional survey was self-administered by the public population in Iraq, Lebanon, Sudan, Jordan, United Arab Emirates, Syria, and Saudi Arabia (April 2021–2023). Associations of stroke risk factors, early symptoms, and consequences with socio-demographics and medical history were analyzed using logistic regression models.
Results: Of 4,090 participants (58.3% females), 42.9% identified four out of five correct answers related to general stroke knowledge. Only 25.2% identified all stroke risk factors, 24.7% recognized all symptoms, and 37.5% knew all possible consequences. Results show consistent pattern of high identification for at least one risk factor and consequences across all countries (96.3 to 99.8% and 86.2 to 100%, respectively), with varying levels of early symptom identification (56.8 to 97.9%). Females were more likely to identify a stroke risk factor, symptom, and consequence compared to males (OR = 2.525, 2.474, and 2.302, respectively, p < 0.001). Employed, urban residents, and those with higher education demonstrated better stroke awareness.
Conclusion: The sample showed variable levels of stroke knowledge among the public, underscoring the pressing need for targeted community initiatives, media campaigns, and educational interventions. These efforts are paramount for improving awareness, early detection, and timely response, especially in countries with lower levels of community stroke awareness.
1 Introduction
Stroke is a significant global health concern and contributes to mortality, morbidity, and disability worldwide (1). Stroke ranks fifth among all causes of death with the highest likelihood occurring within 1 to 5 years after stroke in individuals aged 75 years and older (2). According to the American Health Association 2024, around 795,000 people experience a new or recurrent stroke, with about 610,000 of these as first attacks and 185, 000 as recurrent attacks in the United States (2).
The burden of stroke has decreased in the Middle East and North Africa (MENA) region over the past three decades with large intercountry differences. In 2019, the prevalence and mortality rates of stroke in the MENA region showed a slight decrease of 0.5% in prevalence and a significant 27.8% decline in mortality since 1990 (3).
Despite these improvements, a lack of knowledge and awareness about modifiable and non-modifiable stroke risk factors continues to contribute to the burden of stroke (4). Early warning symptoms of stroke are important for timely management and better treatment outcomes. Rapid thrombolysis therapy during the first 4–6 h from the onset of stroke symptoms lowers the incidence of disabilities and enhances clinical outcomes in patients with ischemic stroke (5). Studies have shown that failure to identify stroke symptoms can delay timely treatment, leading to physical complications, mental disabilities, and increased mortality (4, 6).
There is a consistent trend across studies conducted in countries within the MENA region, including Iraq, Lebanon, Sudan, Jordan, and the United Arab Emirates (UAE), where females demonstrated a higher proficiency in identifying at least one risk factor of stroke (7–11). However, in Saudi Arabia, males showed a significantly higher ability to identify at least one risk factor of stroke compared to females (8). Additionally, in the UAE, Saudi Arabia, Lebanon, Syria, and Jordan, individuals with a university degree, demonstrated greater ability to identify either early stroke symptoms or the consequences of stroke (7–11). In the UAE, individuals with diabetes mellitus were more likely to recognize at least one consequence of stroke compared to patients without diabetes mellitus (7). In Saudi Arabia, individuals with a history of hypertension, dyslipidemia, and obesity were able to identify at least one early stroke symptom (8). However, in Iraq and Jordan, diabetic patients exhibited significantly lower odds of recognizing stroke symptoms compared to non-diabetic patients (9, 11).
Community-based educational initiatives are paramount for stroke prevention by raising patient awareness and knowledge. Adequate knowledge improves quality of life, lowers risk of recurrent strokes, decreases hospitalizations, and reduces healthcare burden and costs (12, 13). Furthermore, increasing public knowledge and awareness of early warning symptoms ensures timely management of stroke, and improves outcomes (7, 8).
While there have been several studies on stroke knowledge and awareness in individual countries within the MENA region, none has provided a comprehensive assessment across countries. Therefore, this study aims to address this gap by assessing public knowledge and awareness of stroke and identifying factors associated with stroke awareness across seven countries in the MENA region. Our study will provide valuable insights to develop targeted educational programs and interventions for stroke prevention and management strategies in the MENA region.
2 Materials and methods
2.1 Study design and participants
This cross-sectional study was conducted using an anonymous online survey in Iraq, Lebanon, Sudan, Jordan, the United Arab Emirates (UAE), Syria, and Saudi Arabia. The snowball sampling method was used from April 2021 to 2023. The data collection sheet was developed on Google form and an electronic link was distributed to the public population in each country through digital platforms such as WhatsApp, LinkedIn, and Facebook. Participation was voluntary. Participants over 18 years of age were eligible; individuals with a history of stroke were excluded.
Participants’ anonymity was guaranteed during the data collection process. At the beginning of the survey, participants were provided with a written informed consent form titled “Your participation in completing this survey is highly appreciated.” Participants provided their electronic consent if they wished to continue with the survey. If not, they selected “disagree to participate” and did not continue the survey. Potential participants who completed the survey were deemed to have provided informed consent to participate in the study.
2.2 Study tool
The survey was written in Arabic, the native language of the included countries, and designed in simple Arabic Language. Pilot was done before study initiation in the involved countries to standardize the data collection form and to ensure it is validity. The data collected for the pilot were not used in the study. The estimated time to complete the questionnaire is 15 min. This investigation was conducted based on previous literature (14, 15). Participants completed without assistance from the investigators to avoid possible influence on answering questions.
The study tool consists of two main parts: the first part of the questionnaire covered sociodemographic and socioeconomic factors, including age, smoking status, marital status, employment status, household income, place of residence, educational level, and medical history (16). The second section assessed common knowledge about stroke. Respondents answered the following statements: Stroke (1) affects the brain, (2) is common in older adults, (3) is contagious, (4) is hereditary, and (5) is preventable. This section also assesses awareness of stroke risk factors, including hypertension, smoking, alcohol consumption, dyslipidemia, diabetes mellitus, physical inactivity, heart disease, obesity, age, and psychosocial stress. Additionally, awareness of early warning signs was examined: (1) Sudden numbness or weakness in the face/arms/legs, especially on one side of the body; (2) Sudden confusion or difficulty speaking/understanding speech; (3) Sudden numbness/weakness in one or both eyes Sudden visual impairment; (4) Sudden difficulty walking, dizziness, or loss of balance or coordination; (5) Sudden severe headache of unknown origin. In line with previous research by Han et al. (15).
Participants received one point for each correct answer to the above statements, but cutoffs to determine acceptable levels of knowledge were lacking. Therefore, our study calculated the total knowledge score by summing up the total number of correct answers.
2.3 Statistical analysis
All study data was extracted from the Google form as Excel spreadsheet and imported to the Statistical Package for Social Sciences version (SPSS) 25.0 for analysis. Categorical variables were presented as frequencies (n) and percentages (%) and continuous variables as means with standard deviation (SD). Bivariate associations between risk factors, early symptoms, and consequences of stroke with socio-demographics and medical history were analyzed using Chi-square test (or Fisher’s exact test if cell count was less than five). Binary logistic regression was performed to determine factors associated with the ability to spontaneously identify at least one or more stroke risk factors, one or more warning signs, one or more consequences, and seeking an emergency room as soon as stroke develops. Variables with a p < 0.2 in the bivariate analysis were included in the logistic regression models. Results were presented as odds ratios (OR) and 95% confidence interval. Statistical tests were reported statistically significant at p < 0.05.
3 Results
3.1 Sample description
Of the total 4,090 participants enrolled in the study, 2,380 (58.3%) were females, 1789 (43.8%) were under 30 years, almost half were single (44.4%), and most of them were residing in urban areas and had university level of education (74.9 and 73.1% respectively). The most common concomitant disease was hypertension (22.6%), followed by dyslipidemia (20.8%) and peptic ulcer (20.0%). The majority of the participants have heard of stroke as a disease (91.3%) and 70.5% knew someone with a stroke. Sociodemographic factors and familiarity with stroke are displayed in Table 1.
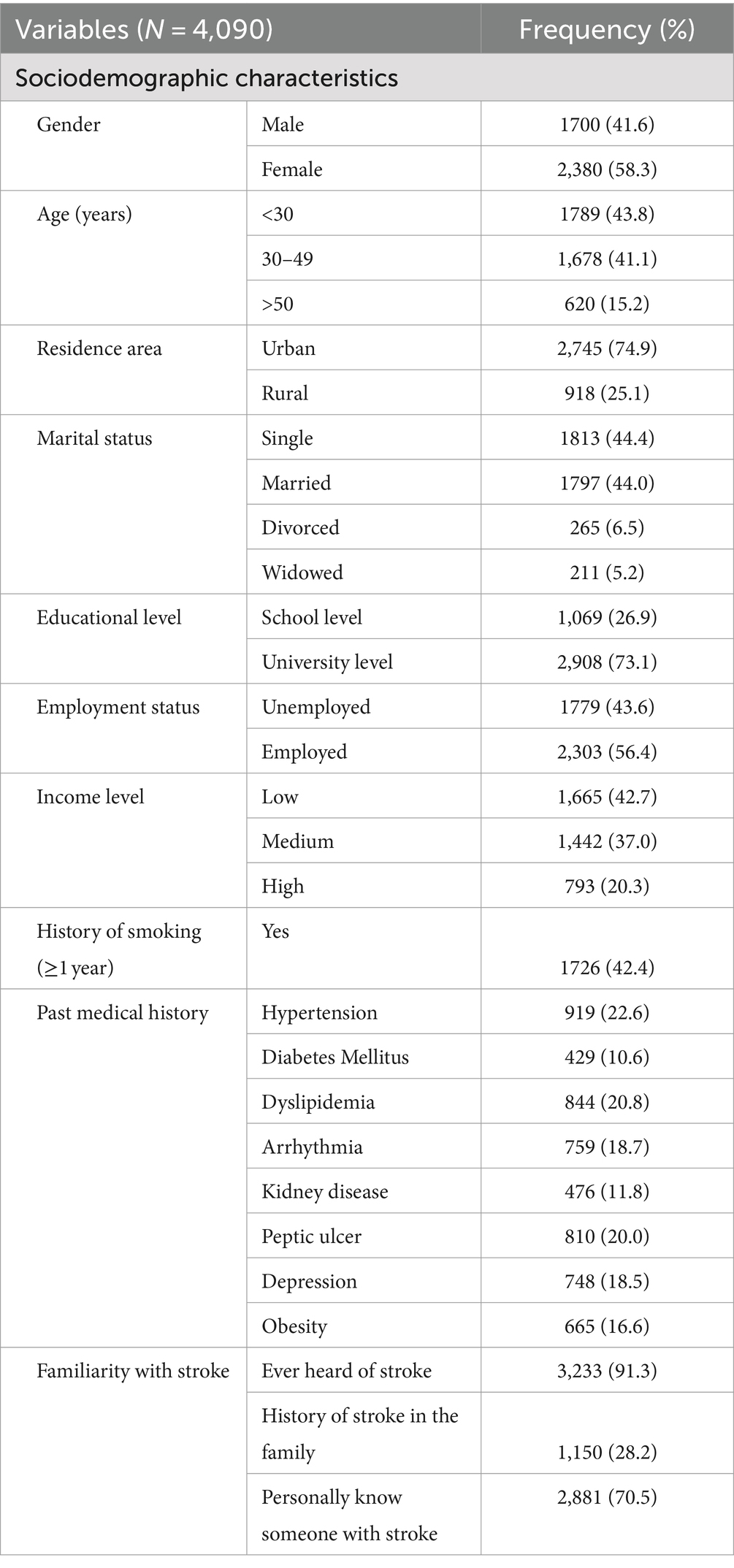
Table 1. Participants’ sociodemographic characteristics, past medical history, and familiarity with stroke.
3.2 Stroke knowledge, risk factors, early symptoms, and consequences
The sample showed a variable level of knowledge about stroke (Figure 1; Table 2). More than half of the participants were aware that stroke is a disease of the brain and that it can be prevented (70.1 and 78.7%, respectively). About 42.9% of the participants could identify four out of five correct answers related to general stroke knowledge. Furthermore, 91.6% believed that hypertension was the most common risk factor, followed by psychosocial stress (84.7%) and high cholesterol (78.1%; Figure 1). The most commonly identified symptoms by participants were “Sudden difficulty in speaking or understanding speech” and “sudden loss of consciousness,” accounting for 89.7 and 86.7%, respectively. Only 25.2% identified all stroke risk factors, 24.7% recognized all stroke early symptoms, and 37.5% knew all possible consequences of stroke (Table 2).
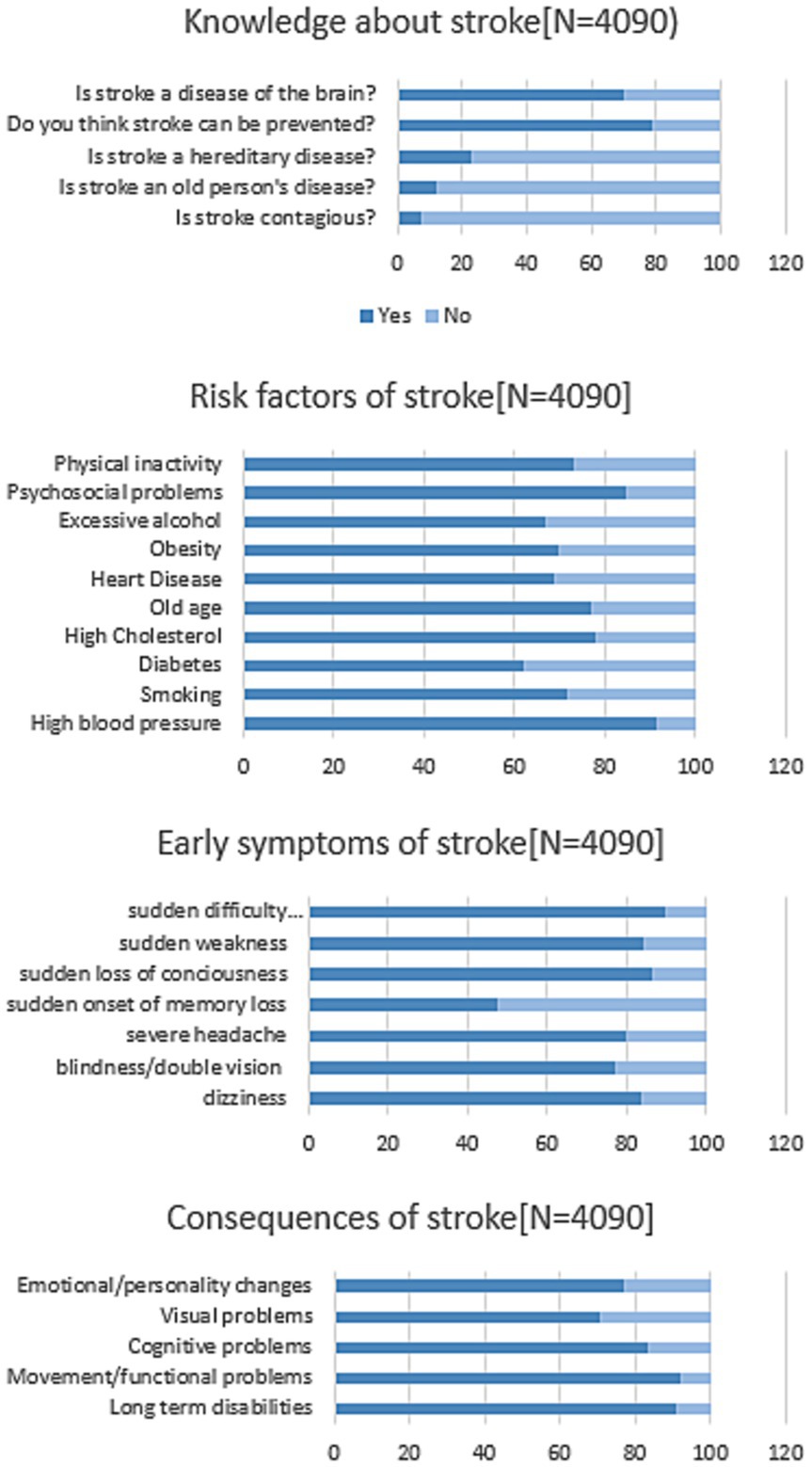
Figure 1. Proportion (%) of responses regarding stroke knowledge, risk factors, and early symptoms.
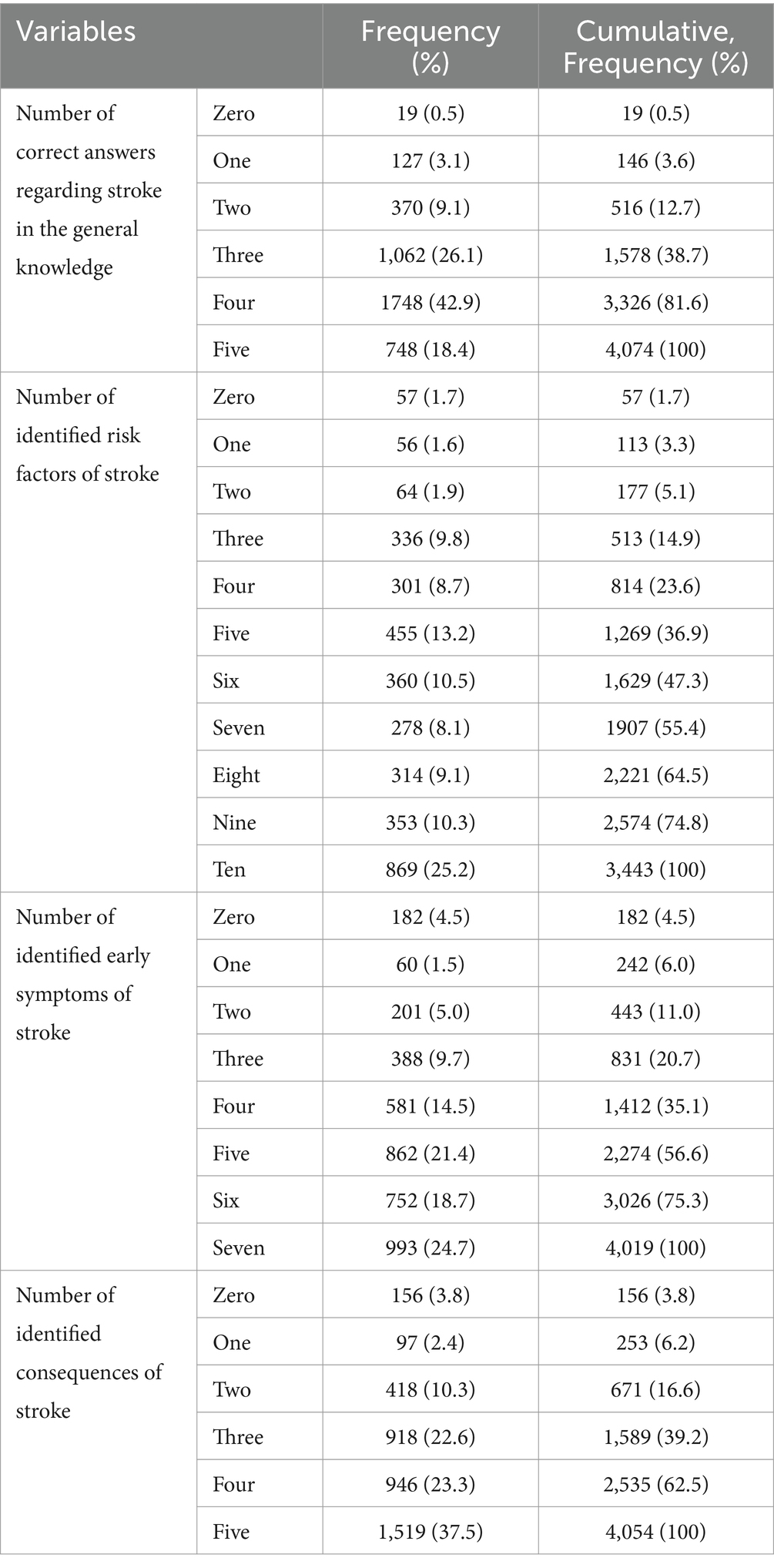
Table 2. Number of stroke risk factors, early symptoms, and consequences that were identified by the participants.
3.3 Cross-country comparison
The study shows a consistent pattern of high identification of at least one stroke risk factor across all seven studied countries, ranging from 96.3 to 99.8% (Table 3).
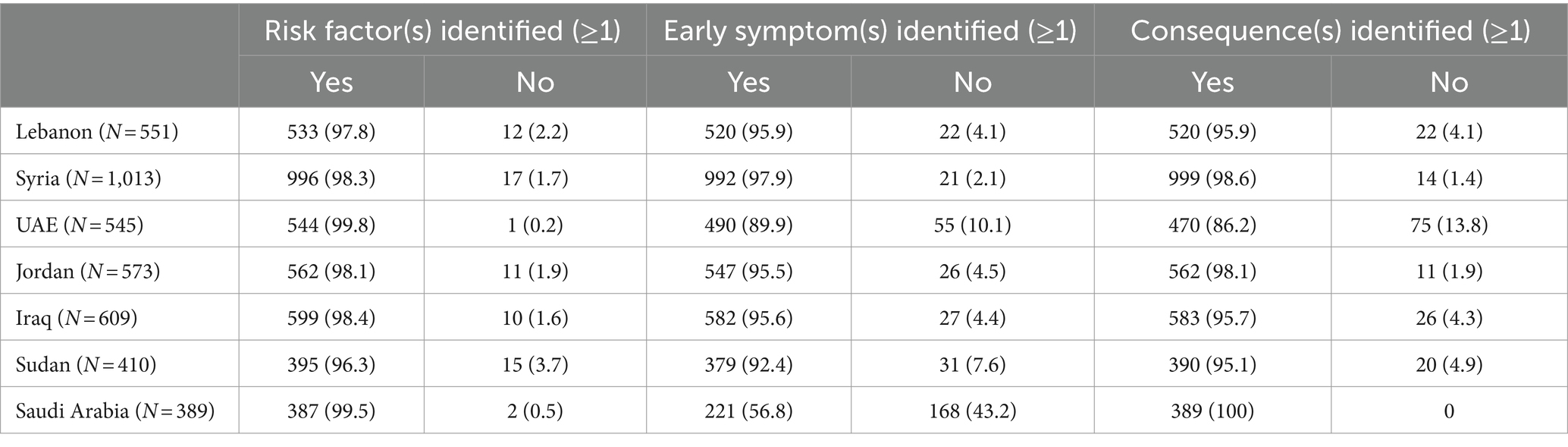
Table 3. Identification of stroke risk factors, early symptoms, and consequences by the participants across the seven countries.
Regarding the identification of at least one early stroke symptom, this study reveals varying patterns across countries. Lebanon, Syria, Jordan, Iraq, and Sudan demonstrate relatively high levels of early symptom identification, ranging from 92.4 to 97.9%. However, the UAE shows a lower level of symptom identification at 89.9%, and Saudi Arabia reports the lowest at 56.8%. Syria, Jordan, and Saudi Arabia show notably high levels of stroke consequence recognition, with percentages ranging from 98.1 to 100%. Lebanon, Iraq, and Sudan also exhibit strong identification exceeding 95%. However, the UAE presents a lower rate at 86.2%.
3.4 Bivariate analysis
A significantly higher proportion of females versus males correctly identified risk factors (58.6% vs. 41.4% p = 0.007), symptoms (95.2% vs. 86.4% p < 0.001), and consequences of stroke (96.8% vs. 95.3% p = 0.016; Table 4). A significantly higher proportion of subjects aged below 30 years versus other age groups (p < 0.001) and who lived in urban versus rural areas (92.5% vs. 88.6%, p < 0.001) correctly identified at least one early symptom of stroke. Furthermore, single and widowed participants and those with higher educational levels exhibited highest percentage of correct responses about early stroke symptoms (p < 0.001). On the other hand, unemployed, those with a high-income level, and with no history of smoking recognized at least one warning symptom of stroke (p < 0.001). Moreover, participants with no history of hypertension (p = 0.007), diabetes mellitus (p < 0.001), arrhythmia (p = 0.001), peptic ulcer (92.1%; p = 0.002), kidney disease (p < 0.001), peptic ulcer (p = 0.002) and depression (p < 0.001) showed the highest percentage of correctly answering at least one question about stroke early symptoms.
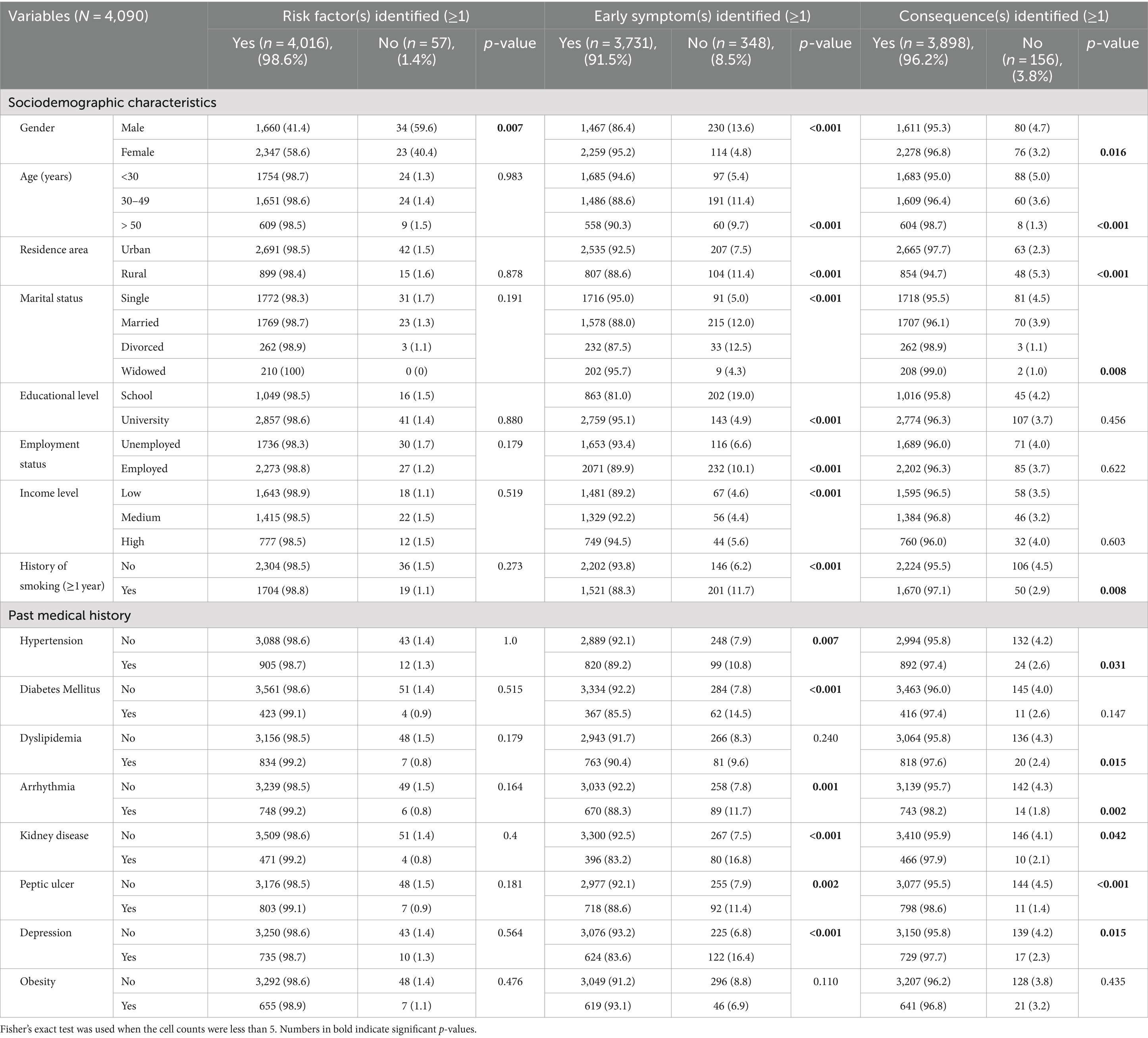
Table 4. Association of risk factors, early symptoms, and consequences of stroke with the sociodemographic characteristics and past medical history.
A significantly higher proportion of subjects aged more than 50 years old (p < 0.001) and those who lived in urban areas vs. rural (97.7% vs. 94.7%; p < 0.001) correctly identified consequences emerging from stroke (Table 4). Moreover, widowed and divorced individuals (p = 0.008) and those with a history of smoking versus no history (97.1% vs. 95.5%; p = 0.008) demonstrated the highest percentage of accurately answering at least one question regarding stroke consequences. A significantly higher number of participants with a history of hypertension (p = 0.031), dyslipidemia (p = 0.015), arrhythmia (p = 0.002), kidney disease (p = 0.042), peptic ulcer disease (p < 0.001) and depression (p = 0.015) identified at least one correct answer about consequences (Table 4).
A significantly higher number of correct answers regarding taking patient to the hospital when there is a stroke symptom was associated with female gender (p < 0.001), younger age (p < 0.001), living in urban areas (80.3% vs. 63.9%, p < 0.001), single status (p < 0.001), university vs. school level of education (79.4% vs. 48.0%, p < 0.001), employed versus unemployed (72.9% vs. 69.3%, p = 0.010), high-income level versus lower income (p < 0.001), and those who had no history of smoking (p < 0.001; Table 5). In addition, those who had no history of hypertension, diabetes mellitus, dyslipidemia, arrhythmia, kidney disease, peptic ulcer, or depression also responded correctly regarding taking patients with symptoms to the hospital (p < 0.001 for all; Table 5).
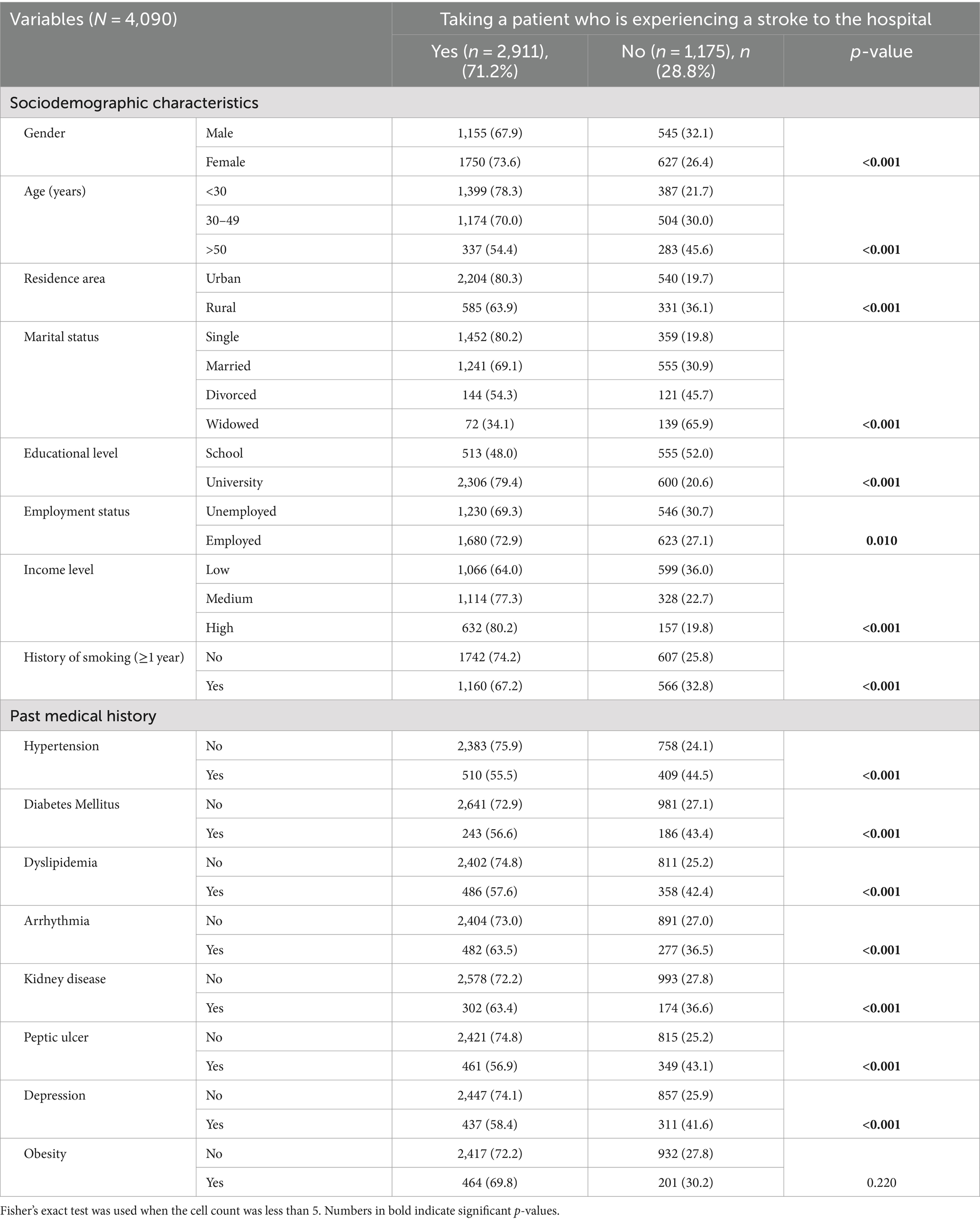
Table 5. Association of taking a patient who is experiencing a stroke to the hospital with sociodemographic characteristics and past medical history.
3.5 Multivariable analysis
Table 6 presents factors associated with the identification of at least one stroke risk factor, early symptom, and consequence. The multivariable analysis showed that females were more likely to identify a risk factor, symptom, and consequence of stroke compared to males (OR = 2.525, 2.474, and 2.302, respectively, p < 0.001; Table 6). Those employed were more likely to identify one stroke risk factor compared to those unemployed (OR = 1.957; 95%CI 1.102; 3.477, p = 0.022).
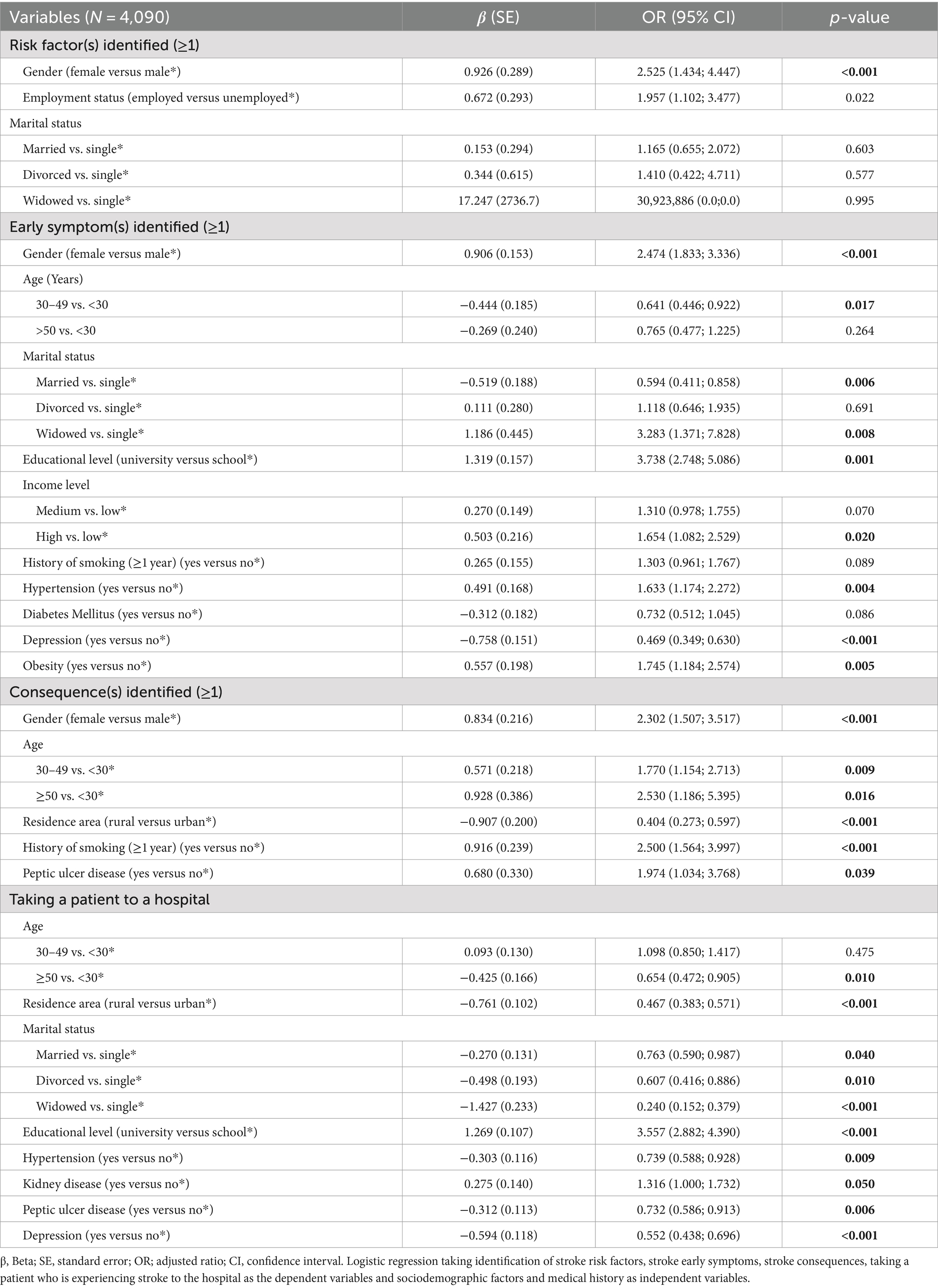
Table 6. Multivariable analysis.
Regarding the identification of at least one early stroke symptom, individuals aged 30–49 years versus <30 years (OR = 0.641; 95%CI 0.446; 0.922, p = 0.017), married versus single (OR = 0.594; 95%CI 0.411; 0.858, p = 0.006) and those with a history of depression versus no history (OR = 0.469; 95%CI 0.349; 0.630, p < 0.001) had significantly lower odds of identifying at least one correct early stroke symptom. Whereas, individuals with higher educational attainment (OR = 3.738, 95%CI 2.748; 5.086, p = 0.001), widowed compared to single (OR = 3.283; 95%CI 1.371; 7.828, p = 0.008), those with high income versus lower income levels (OR = 1.654; 95%CI 1.082; 2.529, p = 0.020) and those with history of hypertension and obesity (OR = 1.633, p = 0.004 and OR = 1.745, p = 0.005, respectively; Table 6) had significantly higher odds identifying at least one stroke symptom.
Concerning the identification of at least one consequence of stroke, older individuals with 30–49 years old and ≥ 50 years compared with <30 years (OR = 1.770; p = 0.009 and OR = 2.530; p = 0.016, respectively), those with a history of smoking (OR = 2.500; p < 0.001), and peptic ulcer disease (OR = 1.974; p = 0.039) had significantly higher odds of identifying a stroke consequence. Individuals living in rural areas had significantly lower odds of identifying a correct stroke consequence compared to those living in urban areas (OR = 0.404; 95% CI 0.273; 0.597, p < 0.001; Table 6).
For the response to stroke symptoms, individuals with a university degree compared to those with lower education (OR = 3.557; 95% CI 2.882; 4.390, p < 0.001; Table 6) were more likely to take a patient experiencing stroke symptoms to a hospital. However, individuals of older age (OR = 0.654), living in rural areas (OR = 0.467), those divorced (OR = 0.607), married (OR = 0.763) or widowed (OR = 0.240) compared to single, and those with chronic disease [i.e., history of hypertension (OR = 0.739), peptic ulcer (OR = 0.732) or depression (OR = 0.552)] had significantly lower odds of responding by taking a patient experiencing stroke symptoms to the hospital.
4 Discussion
4.1 Main findings
This multi-country study assessed public awareness of stroke, focusing on knowledge and identification of stroke risk factors, early warning symptoms, and consequences. Our results showed a variable level of knowledge about stroke and females, employed individuals, urban residents, and those with higher educational attainment demonstrated better knowledge of stroke-related information. Also, 25.2% of individuals identified all stroke risk factors, 24.7% recognized all stroke early symptoms, and 37.5% knew all possible consequences of stroke. Despite this, findings revealed high public awareness of at least one stroke risk factor in all seven countries. However, the identification of at least one early stroke symptom varied: Lebanon, Syria, Jordan, Iraq, and Sudan showed relatively high levels while the UAE and Saudi Arabia had lower levels. Syria, Jordan, and Saudi Arabia reported high recognition of stroke consequences, along with Lebanon, and Iraq, while the UAE had lower rates. Overall, these findings highlight the pressing need for targeted educational interventions and healthcare initiatives to enhance public awareness of stroke, particularly in regions with lower community awareness. Improved knowledge can empower individuals to recognize warning symptoms promptly, seek timely management, and ultimately reduce morbidity and mortality associated with strokes. Addressing these awareness gaps can significantly impact public health outcomes by mitigating stroke burden.
4.2 Stroke general knowledge
The study demonstrated that the majority of the participants were aware of stroke, closely aligning with Dar et al., who reported that 80.5% of patients were informed about the condition (17). This contrasts with several studies that reported lower awareness levels (18–22). The relatively high awareness in our study likely stems from the urban and educated nature of the sample, which promotes greater information exposure and facilitates effective knowledge sharing through close interpersonal and family ties, highlighting the influence of demographic and social factors on public health education aimed at improving stroke awareness within communities. Among those surveyed, 42.9% correctly identified four out of five stroke-related general knowledge, with 18.4% answering all questions, though 0.5% could not provide any correct answers. Notably, 70.1% recognized stroke as a brain disease, and 78.7% acknowledged its preventability. However, several misconceptions about stroke persisted; 23.2% mistakenly considered it hereditary, 12.2% thought it affected only the elderly, and 7.3% incorrectly believed it to be contagious. Similarly, Dar et al. found that 76.0% understood stroke as a brain disease, 85.4% believed in its preventability, but 43.8% considered it hereditary, 32.6% thought it primarily affects elderly, and a concerning 22.9% viewed it as contagious (17).
4.3 Stroke risk factors identification
When asked about potential stroke risk factors, 25.2% of our participants were able to identify all risk factors, while 1.7% could not identify any. Around 91.6% recognized that hypertension is the primary stroke risk factor, followed by psychosocial stress (84.7%), high cholesterol (78.1%), old age (76.9%), and physical inactivity (73.1%). Our results can be interpreted by the fact that the American Heart Association’s 2021 guidelines list hypertension, hyperglycemia, obesity, renal dysfunction, and hyperlipidemia as key stroke risk factors, while also highlighting sedentary lifestyle factors such as smoking and poor diet as significant contributors (23). Recognition of risk factors often varied widely across studies, with 18 to 94% identifying at least one in open-ended questions and 42 to 97% in closed-ended formats (24). For instance, Dar et al. found that most respondents (26.8%) recognized two out of five risk factors, with 19.6% identifying all and 2.3% unable to identify any, consistently pointing to hypertension (93.5%) and diabetes mellitus (45.3%) as primary risk factors (17). Similarly, Sirisha et al. observed that most participants knew fewer than four risk factors, with about 8.85% unaware of any, noting psychological stress (57.6%) and hypertension (57.4%) as top risks (25). Yıldız et al. reported that only 6.5% knew all the risk factors, with hypertension (35.3%) and heart disease (18.5%) as main concerns (26). Lawrence et al. highlighted a concerning trend, with 53.3% of participants unaware of any risk factors, pointing to diabetes mellitus (28.6%) and hypertension (25.7%) as prevalent risks (27). Additionally, a community-based survey across Gulf Cooperation Council (GCC) countries (Qatar, Saudi Arabia, Kuwait, Bahrain, UAE, Oman) emphasized smoking as a significant risk factor (28), underlining the diverse yet overlapping risk factors recognized across different populations and studies.
4.4 Stroke symptoms identification
As for early stroke symptoms, 24.7% of our participants could recognize all early symptoms of stroke, although 4.5% could not identify any. The most common symptom reported was sudden difficulty in speaking/understanding speech (89.7%), likely due to its immediate and noticeable nature, clearly indicating a serious neurological event. Healthcare providers also often emphasize its importance during routine check-ups and educational sessions, reinforcing its significance. Other warning symptoms reported were sudden loss of consciousness/fainting (86.7%), sudden weakness/numbness (84.2%), sudden dizziness (83.6%), and severe headache (79.9%). Meanwhile, Deepthi et al. reported that about 28.9% of participants were able to identify only one stroke symptom, 3% could not identify any, and only 9% could identify all six symptoms listed, with difficulty in speaking (59.4%) and weakness on one side of face/body (54%) being the most common (29). Similarly, Madae’en et al. found that the majority of their participants (31.6%) recognized two stroke symptoms, while only 2.5% listed all symptoms, and 12.7% could not identify any. Sudden loss of speech (54.7%) followed by sudden weakness of one side of the body (49.1%) were the most recognized symptoms (30). Contrasting these findings, Dar et al. observed that none of their respondents identified all symptoms, with 26.2% unable to identify any, and the most frequently listed symptoms being sudden onset of weakness or numbness of limbs (66.9%) and sudden onset of fainting (37.2%) (17). Lawrence et al. also found only 5.7% identified all warning symptoms, while the majority (42.8%) failed to recognize any, with weakness of the arm/leg (53.3%) and difficulty in balancing (23.8%) being the most frequently reported warning symptoms (27). In GCC countries, Kamran et al. noted that weakness of limbs (23%) and speech problems (21.7%) were the most reported symptoms (28).
4.5 Stroke consequences identification
When inquired about stroke’s potential consequences, a substantial majority of our participants (37.5%) were able to enumerate all possible outcomes, though a small proportion (3.8%) could not identify any. Notably, 91.9% of those surveyed recognized that stroke could result in movement/functional problems, likely due to their immediate and visible impact on daily life. Additionally, 90.9% acknowledged the risk of long-term disabilities, 83.3% believed stroke could lead to cognitive/memory problems, and 77 and 70.5% anticipated visual problems and emotional or personality changes, respectively. Similarly, Madae’en et al. reported that the loss of ability to speak (62%) and walk (52.6%) were the most recognized consequences of stroke (30). In contrast, Alhazzani et al. found that death (63.2%) and paralysis (54.6%) were the most frequently reported outcomes of stroke by participants (31).
4.6 Predictors associated with the identification of stroke risk factors, early symptoms, consequences, and decision-making for hospital visits
In examining the predictors for identifying stroke risk factors, early warning symptoms, consequences, and decision-making for hospital visits, our study identified several key trends. For predictors related to identification of stroke risk factors, females were found to have a higher propensity than males to recognize risk factors, a finding supported by Reeves et al., who noted significantly greater awareness among women (32), probably due to their deeper interest in health issues, spending more time seeking health information than men (33). Employment also emerged as a significant predictor; employed individuals were more likely to identify stroke risk factors than their unemployed peers. This correlation could be due to the financial stability of employed persons, enabling better access to health information and more frequent healthcare consultations, as seen in a similar Spanish study (34).
In analyzing factors that influence the recognition of stroke’s early symptoms, females were significantly better than males at identifying at least one early symptom, confirming literature that associates female gender with greater awareness of stroke symptoms (35–37). In contrast, Wahab et al. found that males had superior knowledge of these symptoms (38). Consistent with the literature (35, 39–43), younger individuals were found to be more capable of recognizing stroke symptoms, likely due to better access to health information through digital platforms and social media. Interestingly, married individuals were less adept at recognizing symptoms, possibly due to distractions of familial obligations and lifestyle changes related to marriage, including diet and exercise habits, which could detract from health awareness. Furthermore, individuals with a university education were more capable of identifying symptoms compared to those with only a school education, a trend supported by other studies (20, 22, 35, 38, 44–47), probably due to higher health literacy. Individuals with a high income were significantly more likely to identify early stroke symptoms, possibly because higher income levels often correlate with better access to healthcare resources and information, allowing these individuals to receive regular medical check-ups and education. These results were also corroborated in studies by Yoon et al. (40) and Reeves et al. (32). People with chronic diseases like hypertension and obesity were more likely to identify early stroke symptoms, probably because they were more informed about health due to regular medical visits (48, 49) and actively seeking health information online (50). Hypertension was demonstrated to be a significant predictor of increased knowledge of stroke symptoms in research by Pancioli et al. (35), Schneider et al. (43), and Reeves et al. (32). Conversely, individuals with depression were found to be significantly less likely to identify early stroke symptoms compared to those without depression. Depression impairs cognitive function, reducing the ability to process and retain health information (51). It also lowers motivation to seek and engage with health education resources. Additionally, individuals with depression may interact less frequently with healthcare providers due to hopelessness or lack of energy, resulting in reduced exposure to health information (52).
In identifying stroke consequences, females were more capable than males, demonstrating a gender disparity in health awareness, despite inconsistent findings in previous gender-specific studies (53–55). Age was a crucial factor, with those aged 50 and above more likely to identify consequences than younger individuals, contradicting findings by Ramirez-Moreno et al. that older patients were less knowledgeable (34). Older adults are usually more aware of their higher risk for stroke and other health conditions and are more likely to have had personal or family experiences with stroke, making them more attentive to information about stroke consequences. Geographical differences also impacted awareness, with urban residents more likely to identify stroke consequences than rural ones. Alluqmani et al. found that urban residents were more likely to recognize consequences, likely due to better access to resources and health services in urban areas (56). Lifestyle choices and chronic conditions such as smoking and peptic ulcer disease positively enhanced awareness, likely because affected individuals were more attuned to their healthcare needs and the importance of understanding potential health risks, motivating them to educate themselves about conditions like stroke. Nonetheless, further research is needed to fully explore these aspects.
Regarding the decision to transport a patient experiencing stroke symptoms to hospital, our research identified several key determinants. Previously, limited research has focused on witness factors rather than patient factors affecting response behaviors to stroke, highlighting how environmental context and resources, social influences (e.g., prompts from patients), and beliefs about consequences shape witness behavior (57–59). Our study builds on this by identifying additional factors impacting behavior in response to stroke. Age was a significant factor; individuals aged 50 and above were less likely to transport patients to hospital compared to under 30, possibly due to generational differences in health education, leading older adults to underestimate stroke symptoms or delay seeking immediate medical intervention. Additionally, mobility and transportation challenges that worsen with age, along with potential skepticism toward the healthcare system, may also contribute to this reluctance. Geographical disparities also influenced decisions, with rural residents less likely to seek hospital care for a patient possibly due to limited healthcare access, transportation challenges, and lower stroke awareness. Marital status also impacted the decision-making process, with divorced and widowed individuals less likely to transport patients to hospital than singles, potentially due to the emotional and psychological impacts of their situations affecting their emergency response capabilities. Educational attainment seemed to positively influence decisions, with university educated individuals more inclined to take patients to the hospital compared to those with only school education. This trend was also noted by Dar et al., who observed that higher education was linked to a greater likelihood of taking a stroke patient to a hospital (17). Additionally, caregivers with chronic conditions like hypertension, peptic ulcer disease, and depression were less likely to transport patients, possibly due to physical or emotional barriers these conditions create, which could limit their physical ability to assist others in emergencies.
This study had several limitations. Firstly, the use of an anonymous online survey and the snowball sampling method may introduce selection bias, as it primarily reaches individuals with internet access and those active on social media platforms. This can skew the sample toward younger, more educated, and urban populations, potentially underrepresenting older adults, those with lower educational levels, and rural residents. Secondly, the cross-sectional design limits the ability to establish causality between observed factors and stroke awareness. Thirdly, self-reported data are subject to recall bias and social desirability bias, where participants might overreport their knowledge to present themselves in a better light. Lastly, the exclusion of individuals with a history of stroke may overlook insights from those who have firsthand experience with the condition, potentially missing valuable perspectives on stroke awareness and knowledge.
5 Conclusion
This study provides a comprehensive assessment of stroke knowledge and awareness among Arabic-speaking adults across seven countries in the MENA region. The findings reveal high levels of awareness regarding stroke risk factors and consequences, with notable variability in the identification of early symptoms across countries. Females, employed individuals, urban residents, and those with higher educational attainment demonstrated better knowledge of stroke-related information. The study underscores the importance of community-based educational initiatives to improve stroke awareness, early detection, and timely response. Enhancing public knowledge through mass media campaigns, educational programs, and healthcare initiatives is crucial for reducing the burden of stroke-related morbidity and mortality in the MENA region. Future research should address the identified limitations and explore strategies to reach underrepresented populations, ensuring a more inclusive approach to stroke education and prevention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study was conducted based on the declaration of Helsinki and was approved by the following ethics committee at: School of Pharmacy of the Lebanese International University (202ORC-035-LIUSOP), Applied Science Private University, Amman, Jordan (2021-PHA-9), The University of Sharjah, UAE (REC-21-03-20-01), The University of Baghdad, Iraq (SA 3/6502), The Scientific Research Unit at Almana College for Medical Sciences, Dammam, Saudi Arabia (SR/RP/82), The research ethics committee of the Faculty of Pharmacy, Al Neelain University, Khartoum, Sudan (NPH1021), and Al Furat University in Syria (IRB: FU- 27412: 2022). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
DM: Conceptualization, Project administration, Supervision, Writing – review & editing. SM: Formal analysis, Writing – original draft, Writing – review & editing. MB: Writing – original draft, Writing – review & editing. SC: Formal analysis, Writing – review & editing. ZJK: Data curation, Writing – review & editing. FJ: Data curation, Writing – review & editing. RAZ: Data curation, Writing – review & editing. EE: Data curation, Writing – review & editing. ZK: Writing – review & editing. HA: Data curation, Writing – review & editing. SE: Data curation, Writing – review & editing. RA: Writing – original draft, Writing – review & editing. VM: Writing – original draft, Writing – review & editing. BH: Writing – review & editing. JN: Formal analysis, Writing – review & editing. YA: Data curation, Writing – review & editing. SH: Formal analysis, Writing – review & editing. HH: Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank the participants for their contribution to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Katan, M, and Luft, A. Global burden of stroke. Semin Neurol. (2018) 38:208–11. doi: 10.1055/s-0038-1649503
2. Martin, SS, Aday, AW, Almarzooq, ZI, Anderson, CAM, Arora, P, Avery, CL, et al. 2024 heart disease and stroke statistics: a report of us and global data from the American Heart Association. Circulation. (2024) 149:e347–913. doi: 10.1161/cir.0000000000001209
3. Jaberinezhad, M, Farhoudi, M, Nejadghaderi, SA, Alizadeh, M, Sullman, MJM, Carson-Chahhoud, K, et al. The burden of stroke and its attributable risk factors in the Middle East and North Africa region, 1990-2019. Sci Rep. (2022) 12:2700. doi: 10.1038/s41598-022-06418-x
4. Donkor, ES. Stroke in the 21(St) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. (2018) 2018:3238165. doi: 10.1155/2018/3238165
5. Wardlaw, JM, Murray, V, Berge, E, and del Zoppo, GJ. Thrombolysis for acute Ischaemic stroke. Cochrane Database Syst Rev. (2014) 2014:CD000213. doi: 10.1002/14651858.CD000213.pub3
6. Basri, R, Issrani, R, Hua Gan, S, Prabhu, N, and Khursheed, AM. Burden of stroke in the Kingdom of Saudi Arabia: a soaring epidemic. Saudi Pharm J. (2021) 29:264–8. doi: 10.1016/j.jsps.2021.02.002
7. Jirjees, F, Al-Obaidi, H, Barakat, M, Kharaba, Z, AlSalamat, H, Khidhair, Z, et al. Knowledge and awareness of stroke in the United Arab Emirates: a cross-sectional study of the general population. F1000Res. (2023) 12:1112. doi: 10.12688/f1000research.134328.2
8. Alzayer, R, Barakat, M, Jirjees, F, Alhamdan, A, Aloraifej, S, Cherri, S, et al. Knowledge and awareness of stroke and associated factors in the Saudi general population: a cross-sectional study. Front Neurol. (2023) 14:1225980. doi: 10.3389/fneur.2023.1225980
9. Al-Obaidi, H, Khidhair, Z, Jirjees, F, Barakat, M, AlSalamat, H, Kharaba, Z, et al. Factors associated with knowledge and awareness of stroke in the Iraqi population: a cross-sectional study. Front Neurol. (2023) 14:1144481. doi: 10.3389/fneur.2023.1144481
10. Malaeb, D, Dia, N, Haddad, C, Hallit, S, Sacre, H, Barakat, M, et al. Factors associated with knowledge and awareness of stroke among the Lebanese population: a cross-sectional study. F1000Res. (2022) 11:425. doi: 10.12688/f1000research.108734.2
11. Barakat, M, AA, H, Jirjees, F, Al-Obaidi, H, KH, Z, El Hadidi, S, et al. Factors associated with knowledge and awareness of stroke among the Jordanian population: a cross-sectional study. F1000Res. (2021) 10:1242. doi: 10.12688/f1000research.74492.2
12. Awad, A, and Al-Nafisi, H. Public knowledge of cardiovascular disease and its risk factors in Kuwait: a cross-sectional survey. BMC Public Health. (2014) 14:1131. doi: 10.1186/1471-2458-14-1131
13. Vincent-Onabajo, G, Mshelia, JY, Abubakar, U, Majidadi, RW, Aliyu, HN, Gujba, FK, et al. Knowledge of stroke risk factors among individuals diagnosed with hypertension and diabetes: a hospital-based survey. Br J Med Res. (2015) 10:1–8. doi: 10.9734/BJMMR/2015/19865
14. Sadighi, A, Groody, A, Wasko, L, Hornak, J, and Zand, R. Recognition of stroke warning signs and risk factors among rural population in Central Pennsylvania. J Vasc Interv Neurol. (2018) 10:4–10.
15. Han, CH, Kim, H, Lee, S, and Chung, JH. Knowledge and poor understanding factors of stroke and heart attack symptoms. Int J Environ Res Public Health. (2019) 16:665. doi: 10.3390/ijerph16193665
16. Ahmed, AAA, Al-Shami, AM, Jamshed, S, and Fata Nahas, AR. Development of questionnaire on awareness and action towards symptoms and risk factors of heart attack and stroke among a Malaysian population. BMC Public Health. (2019) 19:1300. doi: 10.1186/s12889-019-7596-1
17. Dar, NZ, Khan, SA, Ahmad, A, and Maqsood, S. Awareness of stroke and health-seeking practices among hypertensive patients in a tertiary care hospital: a cross-sectional survey. Cureus. (2019) 11:e4774. doi: 10.7759/cureus.4774
18. Hickey, A, Holly, D, McGee, H, Conroy, R, and Shelley, E. Knowledge of stroke risk factors and warning signs in Ireland: development and application of the stroke awareness questionnaire (Saq). Int J Stroke. (2012) 7:298–306. doi: 10.1111/j.1747-4949.2011.00698.x
19. Das, S, and Das, SK. Knowledge, attitude and practice of stroke in India versus other developed and developing countries. Ann Indian Acad Neurol. (2013) 16:488–93. doi: 10.4103/0972-2327.120431
20. Menon, B, Swaroop, JJ, Deepika, HKR, Conjeevaram, J, and Munisusmitha, K. Poor awareness of stroke--a hospital-based study from South India: an urgent need for awareness programs. J Stroke Cerebrovasc Dis. (2014) 23:2091–8. doi: 10.1016/j.jstrokecerebrovasdis.2014.03.017
21. Kaddumukasa, M, Kayima, J, Kaddumukasa, MN, Ddumba, E, Mugenyi, L, Pundik, S, et al. Knowledge, attitudes and perceptions of stroke: a cross-sectional survey in rural and urban Uganda. BMC Res Notes. (2015) 8:819. doi: 10.1186/s13104-015-1820-6
22. Sadeghi-Hokmabadi, E, Vahdati, SS, Rikhtegar, R, Ghasempour, K, and Rezabakhsh, A. Public knowledge of people visiting imam Reza hospital regarding stroke symptoms and risk factors. BMC Emerg Med. (2019) 19:36. doi: 10.1186/s12873-019-0250-5
23. Virani, SS, Alonso, A, Aparicio, HJ, Benjamin, EJ, Bittencourt, MS, Callaway, CW, et al. Heart disease and stroke Statistics-2021 update: a report from the American Heart Association. Circulation. (2021) 143:e254–743. doi: 10.1161/cir.0000000000000950
24. Jones, SP, Jenkinson, AJ, Leathley, MJ, and Watkins, CL. Stroke knowledge and awareness: an integrative review of the evidence. Age Ageing. (2010) 39:11–22. doi: 10.1093/ageing/afp196
25. Sirisha, S, Jala, S, Vooturi, S, Yada, PK, and Kaul, S. Awareness, recognition, and response to stroke among the general public-an observational study. J Neurosci Rural Pract. (2021) 12:704–10. doi: 10.1055/s-0041-1735822
26. Yıldız, BTGM, and Şahin, H. Awareness of stroke in the population presenting to outpatient clinics at a tertiary health institution. Turk J Neurol. (2020) 26:149–52. doi: 10.4274/tnd.2020.47887
27. Lawrence, MR, and Wilson, R. Awareness of stroke warning signs, risk factors and response to stroke: a hospital based survey. Int J Res Med Sci. (2023) 11:2550–3. doi: 10.18203/2320-6012.ijrms20232098
28. Kamran, S, Bener, AB, Deleu, D, Khoja, W, Jumma, M, Al Shubali, A, et al. The level of awareness of stroke risk factors and symptoms in the Gulf cooperation council countries: gulf cooperation council stroke awareness study. Neuroepidemiology. (2007) 29:235–42. doi: 10.1159/000112856
29. Deepthi, S, Anoop, KK, Rammohan, K, and Srikumar, B. Public awareness of stroke recognition, risk factors and access to appropriate treatment: a hospital-based cross-sectional survey from a tertiary referral Centre in Southern India. J Clin Diagn Res. (2022). doi: 10.7860/JCDR/2022/51505.16599
30. SSM, E, Bulatova, NR, Al-Qhewii, TA, El-Zayyat, HH, Kamar, MA, Al-Haqeesh, H, et al. Stroke awareness in the general population: a study from Jordan. Trop J Pharm Res. (2014) 12:1071–6. doi: 10.4314/tjpr.v12i6.31
31. Alhazzani, AA, Mahfouz, AA, Abolyazid, AY, Awadalla, NJ, Ahmed, RA, Siddiqui, AF, et al. Awareness of stroke among patients attending primary healthcare services in Abha, southwestern Saudi Arabia. Neurosciences. (2019) 24:214–20. doi: 10.17712/nsj.2019.3.20180041
32. Reeves, MJ, Hogan, JG, and Rafferty, AP. Knowledge of stroke risk factors and warning signs among Michigan adults. Neurology. (2002) 59:1547–52. doi: 10.1212/01.wnl.0000031796.52748.a5
33. Horch, K, and Wirz, J. Nutzung Von Gesundheitsinformationen. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz. (2005) 48:1250–5. doi: 10.1007/s00103-005-1153-z
34. Ramírez-Moreno, JM, Alonso-González, R, Peral Pacheco, D, Millán-Nuñez, MV, Roa-Montero, A, Constantino-Silva, AB, et al. Effect of socioeconomic level on knowledge of stroke in the general population: a social inequality gradient. Neurologia. (2016) 31:24–32. doi: 10.1016/j.nrl.2014.06.004
35. Pancioli, AM, Broderick, J, Kothari, R, Brott, T, Tuchfarber, A, Miller, R, et al. Public perception of stroke warning signs and knowledge of potential risk factors. JAMA. (1998) 279:1288–92. doi: 10.1001/jama.279.16.1288
36. Stroebele, N, Müller-Riemenschneider, F, Nolte, CH, Müller-Nordhorn, J, Bockelbrink, A, and Willich, SN. Knowledge of risk factors, and warning signs of stroke: a systematic review from a gender perspective. Int J Stroke. (2011) 6:60–6. doi: 10.1111/j.1747-4949.2010.00540.x
37. Truelsen, T, and Krarup, LH. Stroke Awareness in Denmark. Neuroepidemiology. (2010) 35:165–70. doi: 10.1159/000314344
38. Wahab, KW, Okokhere, PO, Ugheoke, AJ, Oziegbe, O, Asalu, AF, and Salami, TA. Awareness of warning signs among suburban Nigerians at high risk for stroke is poor: a cross-sectional study. BMC Neurol. (2008) 8:18. doi: 10.1186/1471-2377-8-18
39. Kothari, R, Sauerbeck, L, Jauch, E, Broderick, J, Brott, T, Khoury, J, et al. Patients' awareness of stroke signs, symptoms, and risk factors. Stroke. (1997) 28:1871–5. doi: 10.1161/01.str.28.10.1871
40. Sug Yoon, S, Heller, RF, Levi, C, Wiggers, J, and Fitzgerald, PE. Knowledge of stroke risk factors, warning symptoms, and treatment among an Australian urban population. Stroke. (2001) 32:1926–30. doi: 10.1161/01.str.32.8.1926
41. Greenlund, KJ, Neff, LJ, Zheng, ZJ, Keenan, NL, Giles, WH, Ayala, CA, et al. Low public recognition of major stroke symptoms. Am J Prev Med. (2003) 25:315–9. doi: 10.1016/s0749-3797(03)00206-x
42. Rowe, AK, Frankel, MR, and Sanders, KA. Stroke awareness among Georgia adults: epidemiology and considerations regarding measurement. South Med J. (2001) 94:613–8. doi: 10.1097/00007611-200106000-00015
43. Schneider, AT, Pancioli, AM, Khoury, JC, Rademacher, E, Tuchfarber, A, Miller, R, et al. Trends in community knowledge of the warning signs and risk factors for stroke. JAMA. (2003) 289:343–6. doi: 10.1001/jama.289.3.343
44. Al Shafaee, MA, Ganguly, SS, and Al Asmi, AR. Perception of stroke and knowledge of potential risk factors among Omani patients at increased risk for stroke. BMC Neurol. (2006) 6:38. doi: 10.1186/1471-2377-6-38
45. Kim, YS, Park, SS, Bae, HJ, Heo, JH, Kwon, SU, Lee, BC, et al. Public awareness of stroke in Korea: a population-based National Survey. Stroke. (2012) 43:1146–9. doi: 10.1161/strokeaha.111.638460
46. Sundseth, A, Faiz, KW, Rønning, OM, and Thommessen, B. Factors related to knowledge of stroke symptoms and risk factors in a Norwegian stroke population. J Stroke Cerebrovasc Dis. (2014) 23:1849–55. doi: 10.1016/j.jstrokecerebrovasdis.2014.02.026
47. Arisegi, SA, Awosan, KJ, Oche, MO, Sabir, AA, and Ibrahim, MT. Knowledge and practices related to stroke prevention among hypertensive and diabetic patients attending specialist hospital, Sokoto, Nigeria. Nigeria Pan Afr Med J. (2018) 29:63. doi: 10.11604/pamj.2018.29.63.13252
48. NigeriaChukwuocha, IK, Anyanwu, AC, and Nwazor, EO. Awareness of stroke among subjects with diabetes mellitus attending a tertiary diabetes outpatient Clinic in South-East Nigeria. Medicine. (2018) 4:148. doi: 10.16966/2380-548X.148
49. Baragwanath, CH. Knowledge of stroke risk factors amongst black diabetic, Hypertensive and Stroke Patients. South African J. Physiother. (2014) 59:210. doi: 10.4102/sajp.v59i4.210
50. Ayers, SL, and Kronenfeld, JJ. Chronic illness and health-seeking information on the internet. Health. (2007) 11:327–47. doi: 10.1177/1363459307077547
51. Hammar, A, and Ardal, G. Cognitive functioning in major depression--a summary. Front Hum Neurosci. (2009) 3:26. doi: 10.3389/neuro.09.026.2009
52. Beazley, P, and Gudjonsson, G. Motivating inpatients to engage with treatment: the role of depression and Ward atmosphere. Nord J Psychiatry. (2011) 65:95–100. doi: 10.3109/08039488.2010.502244
53. Park, MH, Jo, SA, Jo, I, Kim, E, Eun, SY, Han, C, et al. No difference in stroke knowledge between Korean adherents to traditional and Western medicine – the age study: an epidemiological study. BMC Public Health. (2006) 6:153. doi: 10.1186/1471-2458-6-153
54. Koçer, A, Ince, N, Koçer, E, and Taşçi, A. Factors influencing treatment compliance among Turkish people at risk for stroke. J Prim Prev. (2006) 27:81–9. doi: 10.1007/s10935-005-0020-x
55. Pontes-Neto, OM, Silva, GS, Feitosa, MR, de Figueiredo, NL, Fiorot, JA Jr, Rocha, TN, et al. Stroke awareness in Brazil: alarming results in a community-based study. Stroke. (2008) 39:292–6. doi: 10.1161/strokeaha.107.493908
56. Alluqmani, MM, Almshhen, NR, Alotaibi, RA, Aljardi, OY, and Zahid, HM. Public awareness of ischemic stroke in Medina city, Kingdom of Saudi Arabia. Neurosciences. (2021) 26:134–40. doi: 10.17712/nsj.2021.2.20200105
57. Dombrowski, SU, Sniehotta, FF, Mackintosh, J, White, M, Rodgers, H, Thomson, RG, et al. Witness response at acute onset of stroke: a qualitative theory-guided study. PLoS One. (2012) 7:e39852. doi: 10.1371/journal.pone.0039852
58. Iversen, AB, Blauenfeldt, RA, Johnsen, SP, Sandal, BF, Christensen, B, Andersen, G, et al. Understanding the seriousness of a stroke is essential for appropriate help-seeking and early arrival at a stroke Centre: a cross-sectional study of stroke patients and their bystanders. Eur Stroke J. (2020) 5:351–61. doi: 10.1177/2396987320945834
Keywords: stroke, knowledge, awareness, community, risk factors, MENA region stroke, MENA region, symptom identification
Citation: Malaeb D, Mansour S, Barakat M, Cherri S, Kharaba ZJ, Jirjees F, Al Zayer R, Eltayib EM, Khidhair Z, AlObaidi H, El Khatib S, Alex R, Menon V, Hosseini B, Noureldine J, Alfoteih Y, Hallit S and Hosseini H (2024) Assessment of knowledge and awareness of stroke among Arabic speaking adults: unveiling the current landscape in seven countries through the first international representative study. Front. Neurol. 15:1492756. doi: 10.3389/fneur.2024.1492756
Edited by:
Majaz Moonis, UMass Memorial Medical Center, United StatesCopyright © 2024 Malaeb, Mansour, Barakat, Cherri, Kharaba, Jirjees, Al Zayer, Eltayib, Khidhair, AlObaidi, El Khatib, Alex, Menon, Hosseini, Noureldine, Alfoteih, Hallit and Hosseini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana Malaeb, ZHIuZGlhbmFAZ211LmFjLmFl
†These authors share last authorship