 Eva Grill1*†
Eva Grill1*† Andreas Zwergal2,3†
Andreas Zwergal2,3† Dorothee Saur4
Dorothee Saur4 Julian Klingbeil4
Julian Klingbeil4 Christopher Fricke4
Christopher Fricke4 Florian Schöberl3Karim Felfela2,3
Florian Schöberl3Karim Felfela2,3 Andrea Zülke5
Andrea Zülke5 Steffi Riedel-Heller5
Steffi Riedel-Heller5 Joseph Classen4
Joseph Classen4- 1Institute for Medical Information Processing, Biometry, and Epidemiology, Faculty of Medicine, Ludwig-Maximilians Universität Munich, Munich, Germany
- 2German Center for Vertigo and Balance Disorders, LMU University Hospital, Munich, Germany
- 3Department of Neurology, LMU University Hospital, Munich, Germany
- 4Department of Neurology, Leipzig University Medical Center, Leipzig, Germany
- 5Institute for Social Medicine, Occupational Health and Public Health, Medical Faculty, University of Leipzig, Leipzig, Germany
Introduction: Modifiable risk factors play an important role in preventing dementia and reducing its progression. Regular physical activity already in midlife, which relies on intact multisensory balance control, can help to decrease the risk of dementia. However, our understanding of the relationship between postural balance and cognitive functions remains limited. The objective of our study was to investigate the association of postural balance during different sensory conditions with specific cognitive domains in older adults.
Methods: Participants were from the population-based prospective “Leipzig Research Center for Civilization Diseases” (LIFE-Adult) cohort in Leipzig, Germany. Executive, memory and processing speed functions were tested by the Consortium to Establish a Registry for Alzheimer’s disease (CERAD) plus battery. Assessment of visuospatial abilities was based on the short form of the Judgment of Line Orientation Test (JLO). Postural sway was recorded on a force plate with eyes open and closed. Romberg’s ratios were calculated for sway path and sway area as a proxy for balance without visual control and tested in generalized linear regression models with the summary scores of executive function, memory, processing speed and visuospatial function as dependent variables. All models were adjusted for sex, age, ApoE status, socioeconomic status, anamnestic stroke, and diabetes.
Results: In total, we analyzed 460 participants with a mean age of 68.6 years, range 60 to 80, 47.6% female. A higher Romberg’s ratio for sway area was a significant indicator for impaired visuospatial abilities as measured by the dichotomized JLO (Odds Ratio = 1.42, 95% confidence interval 1.07 to 1.88). Romberg’s ratios were not significantly associated with executive functions, procedural speed or memory functions.
Discussion: It may be worthwhile to examine in the future whether inclusion of balance testing enhances the value of screening programs for cognitive impairment. Inversely, it may be appropriate to apply routine cognitive tests when balance problems are detected in older patients.
1 Introduction
Dementia is among the major causes for disability and need for care worldwide (1). Over 55 million individuals currently have dementia, with an expected increase of 10 million new cases per year (2). The World Health Organization reported that the costs of caring for the estimated 14.1 million people living with dementia in Europe amounted to US$ 439 billion in 2019 or US$ 32,144 per individual (3), which is close to the mean Gross Domestic Product per capita in Europe [US$ 34,160 in 2022].
Physical inactivity, hypertension, obesity, midlife diabetes, hyperlipidemia, and hearing loss have been identified as major modifiable risk factors for preventing dementia and reducing its progression (4, 5). A healthy lifestyle already in midlife, which critically includes regular physical activity, can help to decrease the risk of dementia (5).
Being physically active relies on an intact balance, which is necessary for upright posture, steady bipedal walking, and a stable representation of the environment. To keep the body in balance, output from visual, proprioceptive, and vestibular systems gets integrated. Decline in vestibular or proprioceptive function can affect posture and gait patterns, increase the risk of falling and as such affect daily functioning, participation and quality of life (6).
The interaction of the multisensory and cognitive function may be at least two-fold. Sensory disorders may affect cognition directly via shared cerebral networks or indirectly via alteration of physical activity. In the last decades, for example, it has been demonstrated that deficits of vestibular function impact several cognitive domains including spatial navigation (7–9), short-term memory and executive function (10), and attention and visuospatial abilities (11). Recent studies linked decreased postural balance (12) and impaired vestibular function (13) to dementia. If this association holds for both postural balance and multisensory vestibular function, early disturbances of sensory balance control need to be identified already in middle-aged and older adults to allow preventive interventions. There is a growing body of evidence that both dedicated balance rehabilitation programs (14) and interventions focusing on vestibular perceptual training improve postural balance (15, 16) possibly also mitigating the risk of dementia. Furthermore, non-invasive vestibular or proprioceptive stimulation devices can improve postural balance (17, 18).
Despite these traces of evidence, our understanding of the relationship between postural balance and cognitive functions remains limited. Little is known about whether certain cognitive domains are disproportionally affected in individuals with impaired postural balance. This question is relevant, because identifying associations with specific cognitive domains could impact diagnostic and therapeutic strategies for patients with combined balance and cognitive disorders. Therefore, the objective of our study was to investigate the association of postural balance during different sensory conditions with specific cognitive domains in older adults.
2 Methods
2.1 Study design and participants
Participants were from the population-based prospective “Leipzig Research Center for Civilization Diseases” (LIFE-Adult) Study in Leipzig, Germany (19). Adult inhabitants of the city of Leipzig were randomly invited via the population registry. Participants underwent structured neuropsychological testing and medical examinations. Medical history and medication were assessed by structured interview. A proportion of participants aged 60 and older underwent specific balance testing. Study design and complete assessment procedures have been described in detail previously (19). Participants were ineligible for inclusion if they had one or more of the following conditions: a stroke within the last 12 months previous to the test date, focal lesions of the brain, delirium, inability to stand safely without support, considerable hearing problems, or any other restriction that would impair or prevent the completion of the testing such as dyslexia, uncorrected visual impairment, visual field impairment, neglect, or alcohol consumption before participation in the study.
All participants signed informed consent and received a small financial compensation. The study was in accordance with the declaration of Helsinki and received approval by the ethics committee of the University of Leipzig (approval numbers 263–2009-14122009, 263/09-ff, 201/17-ek).
2.2 Measures
2.2.1 Exposure
Postural balance in humans is based on a dynamic coordinative interaction between sensory input from vestibular, visual and proprioceptive systems. The body corrects its posture based on this input. Static posturography objectively assesses postural balance by measuring the extent of body sways (changes in the center of pressure of the feet) under various test conditions, such as with open or closed eyes. The closed eye condition subtracts visual input. Therefore, the ratio of closed-eyed and open-eyed sway is an indicator of how much visual vs. vestibular and proprioceptive input contributes to the individual’s optimal static postural balance performance. Typically, the sway ratio is larger if the individual depends to a great extent on visual clues for postural stability, which may indicate the need to compensate for a lack of vestibular or proprioceptive input. Postural sway can be assessed using a platform that records the center of pressure and its shifts during the test paradigms while the tested individual stands unsupported on the platform (20). In the LIFE Adult Study postural control was assessed using a Zebris FDM-S power plate (zebris Medical GmbH, Isny im Allgäu, Germany) with a sampling rate of 50 Hertz analyzed by WinFDM-S. Sway path and sway area were direct outputs of the software. The Center of Pressure (COP) is calculated by the software from the combined load distribution under the feet. A 95% confidence ellipse is calculated from the time-varying points of the COP. As the COP is a time-varying point that moves as a person sways or adjusts, the ellipse captures the main area of this movement, indicating how much a person is shifting their weight and how stable they are. The sway path is the cumulative distance traveled by the COP as it moves over time. This path shows the trajectory of balance adjustments, with longer paths often indicating more movement or instability in balance. The participants were asked to stand on the force plate without shoes with their eyes open and their feet shoulder-width apart. This position was chosen because it corresponds to a natural posture and provides greater stability than a position in which both feet are close together or a fixed distance that is invariant to individual height. The position of the feet had to correspond to the illustration on the edge of the force plate. A one-minute measurement was carried out with documentation of the parameters area of the confidence ellipse in square millimeters (mm), and length of the sway path in mm. In an analogous manner, the participants were then asked to stand on the force plate with their eyes closed. The examiner had to ensure that the person was standing securely all the time. They remained in the immediate vicinity of the test person during the entire examination. The test was canceled if there was a risk of falling due to an unsteady stance. The examiner stood beside the participant to support them in the event of apparent instability, particularly in the closed-eye condition. There was no formal criterion for assessing postural instability other than the examiner’s judgment.
Romberg’s ratios were calculated by dividing closed-eyed sway path by open-eyed sway path and closed-eyed sway area by open-eyed sway area, respectively. These ratios can indicate a lack of vestibular and proprioceptive input to postural stability.
2.3 Outcome
To test executive, memory and processing speed functions, participants completed the CERAD-plus battery (Consortium to Establish a Registry for Alzheimer’s disease (21)). In accordance with previous studies we constructed summary scores for executive cognitive functions, memory performance and processing speed as follows: Executive function = [z phonemic fluency + z semantic fluency - z Trail Making Test (part B - part A)/part A]/3; memory performance = (z learning + z recall + z recognition)/3; processing speed = −z Trail Making Test part A, where z symbolizes the z score that was calculated to normalize raw scores to enable addition (22). Missing values were not replaced (23).
To test visuospatial function, a short form of the Judgment of Line Orientation Test (JLO, short form Q) was used (24). Participants are asked to match a pair of angled lines to the respective lines contained in a semi-circular fan of 11 lines. The short form Q scores add up to the number of correct items. This score is multiplied by two, one point is added in the 50–64 age group, three points are added in the 65–74 age group; two points are added in all age groups for females. Lower score values indicate higher impairment. JLO is a valid and reproducible test of isolated visuospatial abilities (25).
2.4 Covariates
2.4.1 Age was defined at the first visit to the LIFE study center
An aggregated measure of socioeconomic status (SES) was operationalized from the dimensions education, income and occupation using a method established in large population-based surveys (26). This SES score ranges from 3.0 to 21.0 where lower values indicate lower SES. For the analysis, SES was categorized into low (SES ≤ 9.2), middle (9.2 < SES ≤15.5) and high (SES > 15.5). These thresholds correspond to quintiles where quintile 2 to 4 are aggregated, thus, the middle category comprises 60% of the population. SES was entered as a dummy variable into all multivariable analyses, with the lowest category serving as reference.
Comorbid diabetes was operationally defined as present (yes/no) if the patient reported having diabetes, or receiving antidiabetic medication, or fasting serum glucose was equal or above 7.0 mmoL/L, or HbA1c was equal or above 6.5%, or serum glucose was equal or above 11 mmoL/L measured 2 h after consuming 75 g of glucose solution (Accu-Chek® Dextrose O.G.T. Saft, Roche Diagnostics Deutschland).
APOE e4-allele carriers were identified by isolating genomic DNA from peripheral leukocytes, using an automated protocol on the Qiagen Autopure LS (Qiagen, Hilden, Germany). Genotyping of APOE allele status (e2, e3, e4) was performed using a Roche Lightcycler 480, following established methods (27).
Mild cognitive impairment (MCI) was ascertained using the International Working Group Criteria and expanded Mayo criteria (28, 29).
2.5 Statistical analysis
To examine the association between vestibular/proprioceptive balance control and neuropsychological test results, the Romberg’s ratios for sway path and sway area were tested in generalized linear regression models with the summary scores of, respectively, executive function, memory, and cognitive processing speed as dependent variables and in logistic regression models with the dichotomized score of spatial orientation (JLO) as dependent variable. As recommended (25) we dichotomized the JLO score using a score of 20 as cutoff value to minimize false positives. Visual inspection of the scatter plots of the bivariate associations was conducted to detect any apparent patterns of association such as deviations from the general straight-line assumption of linear regression.
Covariates for the models were chosen based on potential relevance for cognitive status or the association between cognition and postural control, namely sex, age, ApoE status, SES and history of stroke. As diabetes may impair postural stability by virtue of inducing polyneuropathy, we also included diabetes status into the models.
Significance level was set at two-sided alpha = 0.05. SAS V9.4 (SAS Institute Inc., Cary, NC, United States) was used for all analyses.
3 Results
In total, we analyzed 460 participants with a mean age of 68.6 years, range 60 to 80, 47.5% female. A total of 6.7% of participants had MCI. Sociodemographic characteristics are shown in Table 1. Cognitive test scores in detail are shown in Supplementary Table S1.
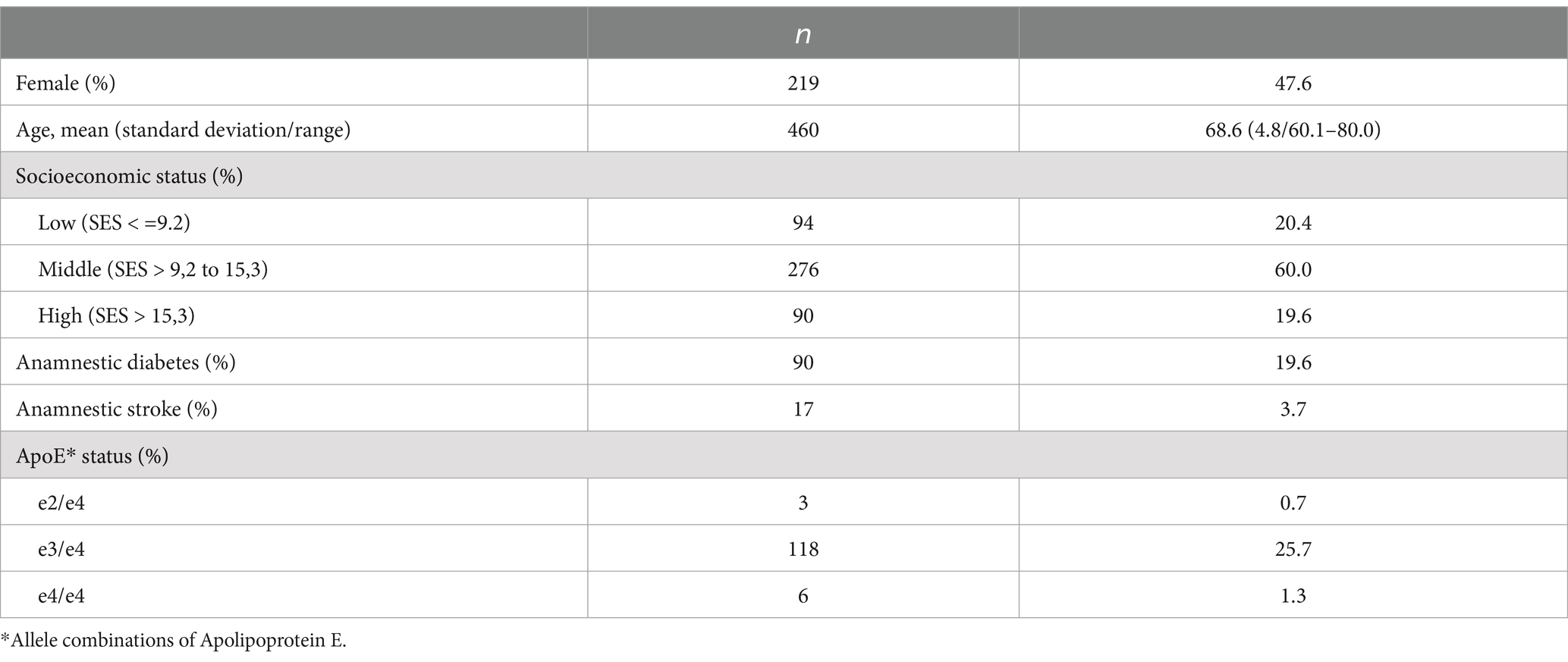
Table 1. Sociodemographic characteristics of participants, n = 460.
Mean sway path was 219.3/519.9 mm for the open eyed/closed eyed condition, mean sway area was 42.0 mm2 for the open-eyed condition and 57.3 mm2 for the closed-eyed condition, resulting in a Romberg’s ratio of 2.4 for sway path and 1.6 for sway area (Table 2).
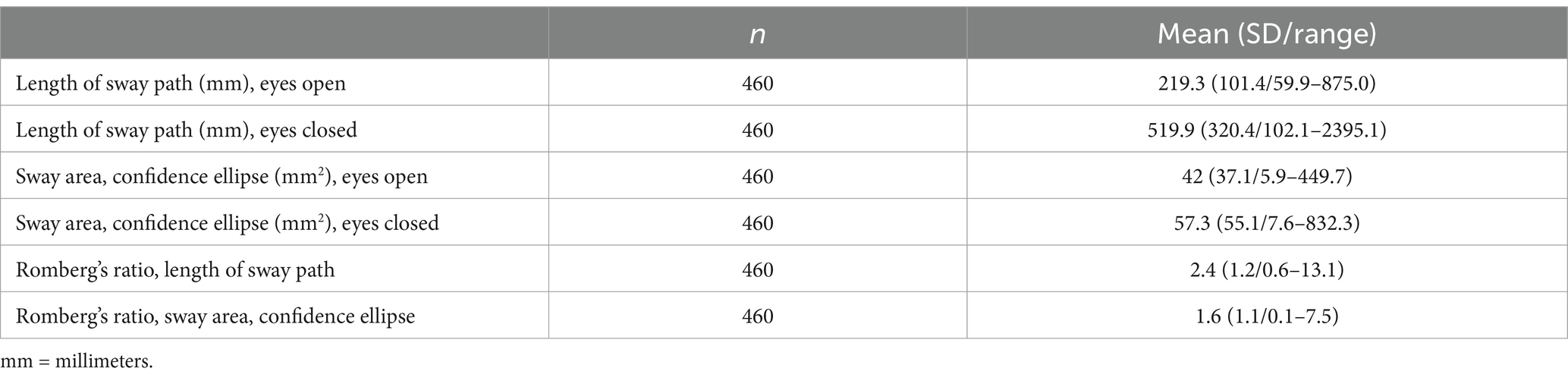
Table 2. Balance test characteristics of participants, mean (Standard deviation/range).
A higher Romberg’s ratio for sway area and female sex were each significant and independent indicators for impaired visuospatial abilities as measured by the dichotomized Judgment of Line Orientation, JLO (Odds Ratio = 1.42 for sway area, Odds Ratio = 2.46 for female sex). Romberg’s ratio for sway path length was not significantly associated with JLO (see Table 3). Age, sociodemographic status, ApoE status, previous stroke and diabetes were not significantly associated with JLO. Sensitivity analyses using the JLO score as a continuous outcome yielded similar results.
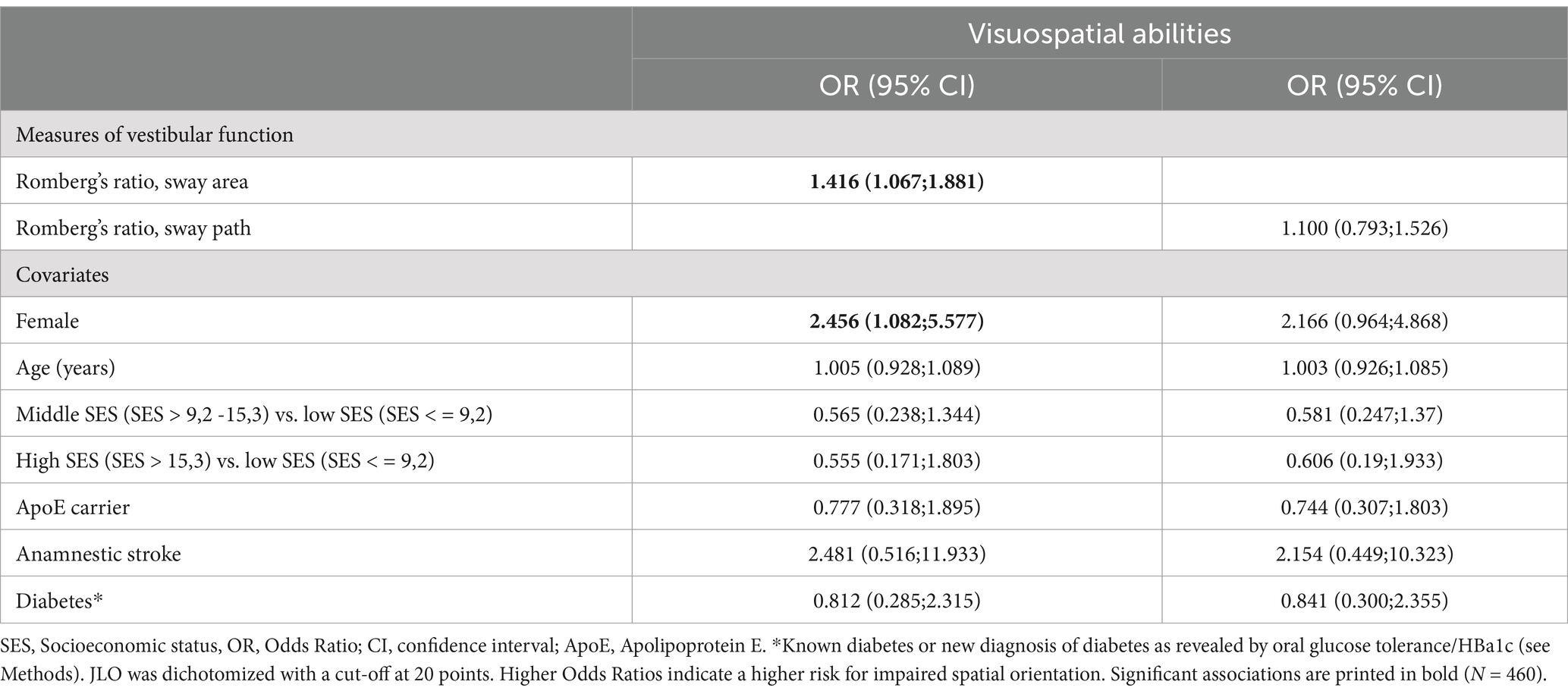
Table 3. Association of two measures of vestibular function with visuospatial abilities (Judgment of Line Orientation, JLO), adjusted for potential confounders in two multiple logistic regression model.
Balance measures were not associated with executive, memory and processing speed functions. More advanced age was an independent significant indicator of worse memory and processing speed functions. Female sex was significantly associated with better memory; middle and high socioeconomic status were both associated with more favorable test results of executive functions and memory. Detailed results are shown in Table 4.
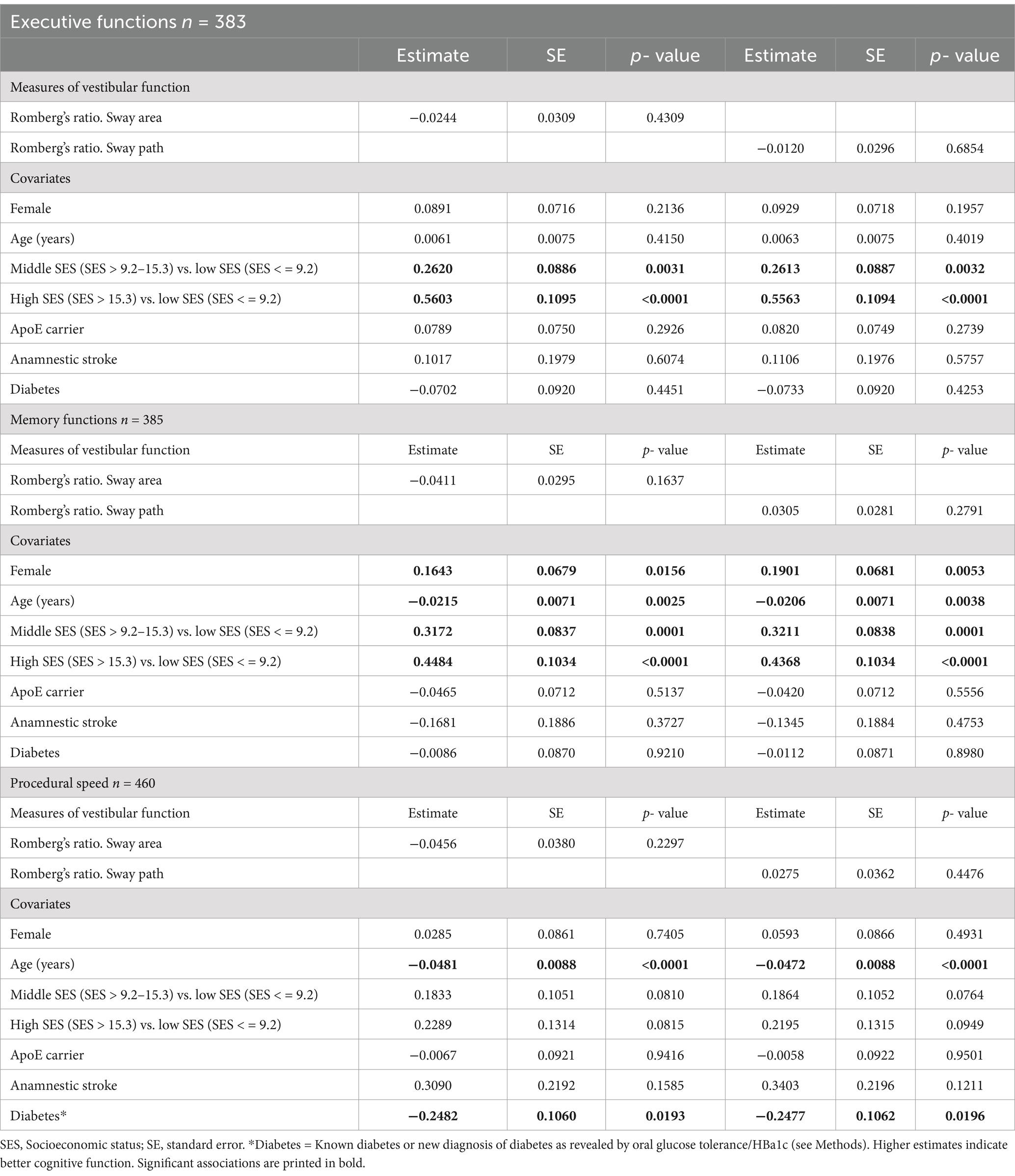
Table 4. Association of Romberg’s ratios with z-standardized a: executive function, b: memory function and c: procedural speed, adjusted for potential confounders in multiple linear regression models.
4 Discussion
The main result of this population-based study in adults aged 60 and older was that poorer postural balance during visual suppression, as indexed by larger sway area ratios during eyes closed relative to eyes open, was significantly and selectively associated with decreased visuospatial abilities as quantified by JLO, but not with functions in other cognitive domains such as memory or execution.
4.1 Non-visually guided postural balance and cognitive domains
In the LIFE Adult Study, postural balance was assessed with and without visual input. Sway parameters, specifically sway area, were calculated, which are sensitive even to subtle changes in postural stability (30). Postural imbalance upon visual suppression is indicative for a deficient vestibular or proprioceptive sensory feedback to central networks of postural control (31) Although dedicated vestibular testing was not performed, the following factors indirectly suggest that postural imbalance with eyes closed in the current study can be overly seen as a surrogate for peripheral vestibular deficits: (1) potential sources of proprioceptive impairment were corrected by adjusting for diabetes and age, (2) the Romberg’s ratio for sway area was associated with performance in the JLO. While the latter is considered a rather pure neuropsychological measure of visuospatial abilities, it has apparent similarities and overlaps with psychophysical testing of verticality perception based on the subjective visual vertical (SVV), which is considered a test of bilateral vestibular graviceptive input (32).
The specific association of postural balance without visual input and visuospatial abilities can be explained by taking a more detailed look at the pathways and networks underlying these functions. JLO engages the superior and posterior parts of the parietal cortex with a right-sided predominance (33). The same parietal areas are activated during mental rotation tasks and spatial updating by the precise estimation of distance and direction (34, 35). Furthermore, perception of verticality guided by graviceptive-vestibular inputs involves parieto-insular cortical areas (36). The superordinate and abstract function of these cortical areas is sensorimotor integration (33). This means that multisensory visual and vestibular afferent inputs are simultaneously processed, analyzed and hierarchically weighted with the major aim to achieve a global egocentric percept of the own body in environmental space. The latter is fundamental for balance control under different sensory conditions and further cognitive processes such as correct estimation of distances and directions in space with regard to the own position in space (37, 38). Thus, there seems to be an obvious link between multisensory, particularly higher-order vestibular processing, in the parietal cortex and visuospatial cognitive abilities. In line with this, vestibular function as tested by vestibular evoked myogenic potentials was predominantly associated with visuospatial abilities in a subcohort of the Baltimore Longitudinal Study of Aging (BLSA) (39).
In the current study, postural control during visual suppression did not show significant associations with executive functions, memory performance and processing speed, i.e., cognitive domains, which are commonly attributed to the frontal and temporal lobes. This finding seems to partially contradict previous reports on neuropsychological deficits in patients with unilateral and bilateral vestibulopathies, who showed mildly reduced performance in short-term memory, executive function, processing speed as well as visuospatial abilities (11) alongside postural imbalance during sensory perturbation. In a representative sample of 1,303 U.S. adults aged ≥60 years, vestibular dysfunction as measured by the modified Romberg’s test, similar to our study, was associated with worse performance in the digital symbol substitution (DSS) test (40). DSS is considered to test multiple cognitive domains including attention, visuospatial skills, associate learning and memory. The discrepancy of these findings to our results may be partially explained by the smaller sample size in the LIFE cohort. Furthermore, recent meta-analyses found heterogeneous associations of balance performance with multi-domain cognitive testing (10, 41). Arguably, more robust analyses are needed to allow a better understanding of the underlying mechanisms related to postural control. Also, the specific effects of the balance system need to be separated from more general effects of aerobic fitness and mobility on cognitive health.
4.2 Non-visually guided postural balance and cognitive decline
The predominant association of postural balance during visual suppression with neuropsychological deficits in the JLO may have interesting implications for the early diagnostic screening of cognitive decline and dementia. Previous studies show that in patients with Mild Cognitive Impairment (MCI), Alzheimer’s dementia (AD) and Parkinson’s Disease (PD) visuospatial abilities as quantified by JLO are inferior than in healthy controls and associated with a concomitant decrease in parietal gray matter volume (42, 43). In general, tests of visuospatial abilities such as the 4 Mountains Test for visual perception and mental rotation, the Rey-Osterrieth Complex Figure (ROCF test) for visuo-constructive abilities and complex visual memory as well as paradigms for spatial navigation, i.e., correct and efficient wayfinding and route execution, have been proven as highly sensitive screening tests for the early detection of MCI and also the differentiation of amyloid-positive and -negative MCI (44–46). Thus, postural imbalance as a marker associated with impaired spatial orientation could be an early sign of progressive dementia, thus, allowing early screening and intervention (47).
5 Strengths and limitations
In contrast to many of the previous studies, our analyses were carried out in a large, representative sample of a population-based study. This may make it less prone to bias from cohorts enriched in people with more comorbidities. The magnitude of the sway path and area found in our study lie within the expected range for an older, non-clinical population (48, 49). Other strengths of the study include the use of validated testing procedures along with deep phenotyping of participants. Also, participants with hearing impairment were excluded, confirming the postulated independent association between vestibular and cognitive functions (50), specifically regarding visuospatial abilities (51). One obvious limitation is the cross-sectional nature of the data which precludes the analysis of causal association and independent effects.
6 Conclusion
In our study of older adults, a population-based approach with a rigorous assessment routine aligns with previous studies investigating the association of vestibular with cognitive impairment conducted in clinical settings. We found that poorer postural balance during visual suppression was significantly and selectively associated with decreased visuospatial abilities. While a test for postural balance can only be viewed as a surrogate of vestibular function, it may be worthwhile to examine in the future whether inclusion of balance testing enhances the value of screening programs for early detection of cognitive impairment. Also, it may be appropriate to apply routine cognitive tests when balance problems are detected.
Balance functions and specifically vestibular functions are amenable to interventions. There is also evidence that cognitive training in MCI or early dementia helps to decelerate or even prevent cognitive deterioration (52, 53). Further research should investigate if balance is only an indicator, or if interventions targeted on balance are a necessary component to preserve brain health in aging.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the University of Leipzig (Approval numbers: 263–2009-14122009, 263/09-ff, 201/17-ek). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EG: Conceptualization, Formal analysis, Writing – original draft. AZw: Conceptualization, Methodology, Writing – review & editing. SD: Methodology, Writing – review & editing. JK: Methodology, Writing – review & editing. CF: Methodology, Writing – review & editing. FS: Writing – review & editing. KF: Writing – review & editing. AZü: Data curation, Methodology, Project administration, Writing – review & editing. SR-H: Methodology, Supervision, Writing – review & editing. JC: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was funded by the German Federal Ministry of Education and Research (BMBF) in the context of the German Center for Vertigo and Balance Disorders (DSGZ) (grant no. 01 EO 1401). LIFE is funded by means of the European Union, by the European Regional Development Fund (ERDF) and by funds of the Free State of Saxony within the framework of the excellence initiative (project nos. 713–241202, 713–241202, 14505/2470, and 14575/2470).
Acknowledgments
We acknowledge the contribution of all participants of the LIFE Adult Study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1452150/full#supplementary-material
References
1. World Health Organization. First WHO ministerial conference on global action against dementia. Geneva: World Health Organization (2015).
3. World Health Organization. Global status report on the public health response to dementia. Geneva: World Health Organization (2021).
4. Deckers, K, van Boxtel, MP, Schiepers, OJ, de Vugt, M, Munoz Sanchez, JL, Anstey, KJ, et al. Target risk factors for dementia prevention: a systematic review and Delphi consensus study on the evidence from observational studies. Int J Geriatr Psychiatry. (2015) 30:234–46. doi: 10.1002/gps.4245
5. Livingston, G, Huntley, J, Sommerlad, A, Ames, D, Ballard, C, Banerjee, S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/S0140-6736(20)30367-6
6. Mueller, M, Strobl, R, Jahn, K, Linkohr, B, Ladwig, KH, Mielck, A, et al. Impact of vertigo and dizziness on self-perceived participation and autonomy in older adults: results from the KORA-age study. Qual Life Res. (2014) 23:2301–8. doi: 10.1007/s11136-014-0684-x
7. Dobbels, B, Peetermans, O, Boon, B, Mertens, G, Van de Heyning, P, and Van Rompaey, V. Impact of bilateral Vestibulopathy on spatial and nonspatial cognition: a systematic review. Ear Hear. (2019) 40:757–65. doi: 10.1097/aud.0000000000000679
8. Schoberl, F, Pradhan, C, Grosch, M, Brendel, M, Jostes, F, Obermaier, K, et al. Bilateral vestibulopathy causes selective deficits in recombining novel routes in real space. Sci Rep. (2021) 11:2695. doi: 10.1038/s41598-021-82427-6
9. Zwergal, A, Grabova, D, and Schoberl, F. Vestibular contribution to spatial orientation and navigation. Curr Opin Neurol. (2024) 37:52–8. doi: 10.1097/WCO.0000000000001230
10. Demnitz, N, Esser, P, Dawes, H, Valkanova, V, Johansen-Berg, H, Ebmeier, KP, et al. A systematic review and meta-analysis of cross-sectional studies examining the relationship between mobility and cognition in healthy older adults. Gait Posture. (2016) 50:164–74. doi: 10.1016/j.gaitpost.2016.08.028
11. Popp, P, Wulff, M, Finke, K, Ruhl, M, Brandt, T, and Dieterich, M. Cognitive deficits in patients with a chronic vestibular failure. J Neurol. (2017) 264:554–63. doi: 10.1007/s00415-016-8386-7
12. Blodgett, JM, Cooper, R, Davis, DHJ, Kuh, D, and Hardy, R. Associations of word memory, verbal fluency, processing speed, and crystallized cognitive ability with one-legged balance performance in mid- and later life. J Gerontol A Biol Sci Med Sci. (2022) 77:807–16. doi: 10.1093/gerona/glab168
13. Smith, PF. The vestibular system and cognition. Curr Opin Neurol. (2017) 30:84–9. doi: 10.1097/WCO.0000000000000403
14. Van Vugt, VA, van der Wouden, JC, Essery, R, Yardley, L, Twisk, JWR, van der Horst, HE, et al. Internet based vestibular rehabilitation with and without physiotherapy support for adults aged 50 and older with a chronic vestibular syndrome in general practice: three armed randomised controlled trial. BMJ. (2019) 367:l5922. doi: 10.1136/bmj.l5922
15. Klaus, MP, Schone, CG, Hartmann, M, Merfeld, DM, Schubert, MC, and Mast, FW. Roll tilt self-motion direction discrimination training: first evidence for perceptual learning. Atten Percept Psychophys. (2020) 82:1987–99. doi: 10.3758/s13414-019-01967-2
16. Wagner, AR, Kobel, MJ, Tajino, J, and Merfeld, DM. Improving self-motion perception and balance through roll tilt perceptual training. J Neurophysiol. (2022) 128:619–33. doi: 10.1152/jn.00092.2022
17. Kingma, H, Felipe, L, Gerards, MC, Gerits, P, Guinand, N, Perez-Fornos, A, et al. Vibrotactile feedback improves balance and mobility in patients with severe bilateral vestibular loss. J Neurol. (2019) 266:19–26. doi: 10.1007/s00415-018-9133-z
18. Wuehr, M, Eder, J, Kellerer, S, Amberger, T, and Jahn, K. Mechanisms underlying treatment effects of vestibular noise stimulation on postural instability in patients with bilateral vestibulopathy. J Neurol. (2024) 271:1408–15. doi: 10.1007/s00415-023-12085-3
19. Loeffler, M, Engel, C, Ahnert, P, Alfermann, D, Arelin, K, Baber, R, et al. The LIFE-adult-study: objectives and design of a population-based cohort study with 10,000 deeply phenotyped adults in Germany. BMC Public Health. (2015) 15:691. doi: 10.1186/s12889-015-1983-z
20. Prieto, TE, Myklebust, JB, Hoffmann, RG, Lovett, EG, and Myklebust, BM. Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans Biomed Eng. (1996) 43:956–66. doi: 10.1109/10.532130
21. Morris, JC, Heyman, A, Mohs, RC, Hughes, JP, van Belle, G, Fillenbaum, G, et al. The consortium to establish a registry for alzheimer’s disease (CERAD). Part I. Clinical and neuropsychological assessment of alzheimer’s disease. Neurology. (1989) 39:1159–65. doi: 10.1212/wnl.39.9.1159
22. Kharabian Masouleh, S, Arélin, K, Horstmann, A, Lampe, L, Kipping, JA, Luck, T, et al. Higher body mass index in older adults is associated with lower gray matter volume: implications for memory performance. Neurobiol Aging. (2016) 40:1–10. doi: 10.1016/j.neurobiolaging.2015.12.020
23. van de Rest, O, Geleijnse, JM, Kok, FJ, van Staveren, WA, Dullemeijer, C, OldeRikkert, MGM, et al. Effect of fish oil on cognitive performance in older subjects: a randomized, controlled trial. Neurology. (2008) 71:430–8. doi: 10.1212/01.wnl.0000324268.45138.86
24. Benton, AL, Sivan, AB, Hamsher, KD, Varney, NR, and Spreen, O. Contributions to neuropsychological assessment. A clinical manual. New York, Oxford: Oxford University Press (1994).
25. Qualls, CE, Bliwise, NG, and Stringer, AY. Short forms of the Benton judgment of line orientation test: development and psychometric properties. Arch Clin Neuropsychol. (2000) 15:159–63. doi: 10.1016/S0887-6177(98)00043-2
26. Lampert, T, Kroll, LE, Muters, S, and Stolzenberg, H. Measurement of the socioeconomic status within the German health update 2009 (GEDA). Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. (2013) 56:131–43. doi: 10.1007/s00103-012-1583-3
27. Aslanidis, C, and Schmitz, G. High-speed apolipoprotein E genotyping and apolipoprotein B3500 mutation detection using real-time fluorescence PCR and melting curves. Clin Chem. (1999) 45:1094–7. doi: 10.1093/clinchem/45.7.1094
28. Petersen, RC. Mild cognitive impairment as a diagnostic entity. J Intern Med. (2004) 256:183–94. doi: 10.1111/j.1365-2796.2004.01388.x
29. Winblad, B, Palmer, K, Kivipelto, M, Jelic, V, Fratiglioni, L, Wahlund, LO, et al. Mild cognitive impairment--beyond controversies, towards a consensus: report of the international working group on mild cognitive impairment. J Intern Med. (2004) 256:240–6. doi: 10.1111/j.1365-2796.2004.01380.x
30. Sun, R, Hsieh, KL, and Sosnoff, JJ. Fall risk prediction in multiple sclerosis using postural sway measures: a machine learning approach. Sci Rep. (2019) 9:16154. doi: 10.1038/s41598-019-52697-2
31. Horlings, CG, Kung, UM, Bloem, BR, Honegger, F, Van Alfen, N, Van Engelen, BG, et al. Identifying deficits in balance control following vestibular or proprioceptive loss using posturographic analysis of stance tasks. Clin Neurophysiol. (2008) 119:2338–46. doi: 10.1016/j.clinph.2008.07.221
32. Dieterich, M, and Brandt, T. Perception of verticality and vestibular disorders of balance and falls. Front Neurol. (2019) 10:172. doi: 10.3389/fneur.2019.00172
33. Isaacs, EB, Edmonds, CJ, Chong, WK, Lucas, A, and Gadian, DG. Cortical anomalies associated with visuospatial processing deficits. Ann Neurol. (2003) 53:768–73. doi: 10.1002/ana.10546
34. Anomal, RF, Brandão, DS, Porto, SB, de Oliveira, SS, de Souza, RFL, Fiel, JS, et al. The role of frontal and parietal cortex in the performance of gifted and average adolescents in a mental rotation task. PLoS One. (2020) 15:e0232660. doi: 10.1371/journal.pone.0232660
35. Blouin, J, Pialasse, J-P, Mouchnino, L, and Simoneau, M. On the dynamics of spatial updating. Front Neurosci. (2022) 16:27. doi: 10.3389/fnins.2022.780027
36. Conrad, J, Baier, B, Eberle, L, Ruehl, RM, Boegle, R, Zwergal, A, et al. Network architecture of verticality processing in the human thalamus. Ann Neurol. (2023) 94:133–45. doi: 10.1002/ana.26652
37. Dieterich, M, and Brandt, T. The parietal lobe and the vestibular system. Handb Clin Neurol. (2018) 151:119–40. doi: 10.1016/B978-0-444-63622-5.00006-1
38. Medendorp, WP, and Selen, LJP. Vestibular contributions to high-level sensorimotor functions. Neuropsychologia. (2017) 105:144–52. doi: 10.1016/j.neuropsychologia.2017.02.004
39. Bigelow, RT, Semenov, YR, Trevino, C, Ferrucci, L, Resnick, SM, Simonsick, EM, et al. Association between visuospatial ability and vestibular function in the Baltimore longitudinal study of aging. J Am Geriatr Soc. (2015) 63:1837–44. doi: 10.1111/jgs.13609
40. Semenov, YR, Bigelow, RT, Xue, QL, du Lac, S, and Agrawal, Y. Association between vestibular and cognitive function in U.S. adults: data from the National Health and nutrition examination survey. J Gerontol A Biol Sci Med Sci. (2016) 71:243–50. doi: 10.1093/gerona/glv069
41. Divandari, N, Bird, M-L, Vakili, M, and Jaberzadeh, S. The association between cognitive domains and postural balance among healthy older adults: a systematic review of literature and Meta-analysis. Curr Neurol Neurosci Rep. (2023) 23:681–93. doi: 10.1007/s11910-023-01305-y
42. Finton, MJ, Lucas, JA, Graff-Radford, NR, and Uitti, RJ. Analysis of visuospatial errors in patients with Alzheimer's disease or Parkinson's disease. J Clin Exp Neuropsychol. (1998) 20:186–93. doi: 10.1076/jcen.20.2.186.1167
43. Wasserman, V, Emrani, S, Matusz, EF, Peven, J, Cleary, S, Price, CC, et al. Visuospatial performance in patients with statistically-defined mild cognitive impairment. J Clin Exp Neuropsychol. (2020) 42:319–28. doi: 10.1080/13803395.2020.1714550
44. Coughlan, G, Laczó, J, Hort, J, Minihane, A-M, and Hornberger, M. Spatial navigation deficits — overlooked cognitive marker for preclinical Alzheimer disease? Nat Rev Neurol. (2018) 14:496–506. doi: 10.1038/s41582-018-0031-x
45. Schöberl, F, Pradhan, C, Irving, S, Buerger, K, Xiong, G, Kugler, G, et al. Real-space navigation testing differentiates between amyloid-positive and -negative aMCI. Neurology. (2020) 94:e861–73. doi: 10.1212/wnl.0000000000008758
46. Schoberl, F, Zwergal, A, and Brandt, T. Testing navigation in real space: contributions to understanding the physiology and pathology of human navigation control. Front Neural Circuits. (2020) 14:6. doi: 10.3389/fncir.2020.00006
47. Cammisuli, DM, Isella, V, Verde, F, Silani, V, Ticozzi, N, Pomati, S, et al. Behavioral disorders of spatial cognition in patients with mild cognitive impairment due to Alzheimer’s disease: preliminary findings from the BDSC-MCI project. J Clin Med. (2024) 13:1178. doi: 10.3390/jcm13041178
48. Johansson, J, Nordström, A, Gustafson, Y, Westling, G, and Nordström, P. Increased postural sway during quiet stance as a risk factor for prospective falls in community-dwelling elderly individuals. Age Ageing. (2017) 46:964–70. doi: 10.1093/ageing/afx083
49. König, N, Taylor, WR, Baumann, CR, Wenderoth, N, and Singh, NB. Revealing the quality of movement: a meta-analysis review to quantify the thresholds to pathological variability during standing and walking. Neurosci Biobehav Rev. (2016) 68:111–9. doi: 10.1016/j.neubiorev.2016.03.035
50. Smith, PF. Hearing loss versus vestibular loss as contributors to cognitive dysfunction. J Neurol. (2022) 269:87–99. doi: 10.1007/s00415-020-10343-2
51. Bosmans, J, Gommeren, H, Mertens, G, Cras, P, Engelborghs, S, Van Ombergen, A, et al. Associations of bilateral Vestibulopathy with cognition in older adults matched with healthy controls for hearing status. JAMA Otolaryngol Head Neck Surg. (2022) 148:731–9. doi: 10.1001/jamaoto.2022.1303
52. Belleville, S. Cognitive training for persons with mild cognitive impairment. Int Psychogeriatr. (2008) 20:57–66. doi: 10.1017/S104161020700631X
Keywords: Hans Straka’s memory, the vestibular system, mild cognitive impairment, cognition, postural balance
Citation: Grill E, Zwergal A, Saur D, Klingbeil J, Fricke C, Schöberl F, Felfela K, Zülke A, Riedel-Heller S and Classen J (2024) Postural imbalance without visual input is associated with specific neuropsychological deficits in older adults – results from the LIFE-adult study. Front. Neurol. 15:1452150. doi: 10.3389/fneur.2024.1452150
Edited by:
Dominik Straumann, University of Zurich, SwitzerlandCopyright © 2024 Grill, Zwergal, Saur, Klingbeil, Fricke, Schöberl, Felfela, Zülke, Riedel-Heller, Classen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eva Grill, ZXZhLmdyaWxsQG1lZC51bmktbXVlbmNoZW4uZGU=
†These authors have contributed equally to this work and share first authorship