 Helle Elisabeth Agger-Nielsen
Helle Elisabeth Agger-Nielsen Thomas Stig Grøndberg
Thomas Stig Grøndberg Gabriele Berg-Beckhoff4
Gabriele Berg-Beckhoff4 Therese Ovesen
Therese Ovesen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol., 30 May 2024
Sec. Neuro-Otology
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1396891
This article is part of the Research TopicThe far-reaching impacts of vestibular impairment and novel methods for their assessment and treatmentView all 13 articles
Objective: This study aimed to investigate the impact of early vestibular rehabilitation training combined with corticosteroids initiated within 2 weeks, compared with corticosteroid treatment, after the peripheral acute vestibular syndrome (pAVS) onset.
Data sources: PubMed, CINAHL, EMBASE, and SCOPUS. From inception to January 24, 2024. The International Prospective Register of Systematic Reviews approved this study (CRD42023422308).
Results: Five studies involving 235 patients were included in this systematic review and meta-analysis. The subjective outcome measure Dizziness Handicap Inventory (DHI) was pooled for a meta-analysis and was statistically significantly in favor of early vestibular rehabilitation training (early VRT) plus corticosteroids compared with corticosteroids alone: at one-month follow-up (p = 0.00) and 12 months follow-up (p = 0.01). DHI was a critical outcome for measuring the differences in effect of early VRT. The objective outcome measures of caloric lateralization, cervical vestibular-evoked myogenic potentials, and posturography were gathered for a narrative synthesis.
Conclusion: This meta-analysis showed that early VRT in combination with corticosteroids was more effective for treating pAVS than corticosteroid treatment alone. No adverse effects were reported for early VRT.
Acute vestibular syndrome (AVS) is defined as the acute onset of continuous vertigo lasting >24 h. AVS is often associated with nausea, vomiting, and head motion intolerance (1). In the United States, acute vertigo is estimated to account for 4% of patients admitted to emergency departments (2). Furthermore, vertigo is extremely distressing for patients and may lead to hospitalization.
There are two types of AVS: central AVS (cAVS), which is caused by stroke, and peripheral AVS (pAVS), which is caused by various influences of the vestibular organ in the inner ear and/or vestibular nerve. The pAVS includes several specific diagnoses, including vestibular neuritis, Meniere’s disease, perilymphatic fistulas, and labyrinthitis. The specific cause of AVS may not be evident during an acute diagnostic workup; therefore, the terms p-AVS and c-AVS were introduced to differentiate the two conditions. However, this distinction is extremely important because of the potentially fatal outcome of overlooking stroke (3–6). Accordingly, subdivision into two entities also determines the treatment.
Regarding cAVS, some evidence supports the effectiveness of early rehabilitation (7). In pAVS, early rehabilitation is only sporadically described in available research and guidelines (8, 9). Hypothetically, vestibular rehabilitation, that is, physical exercise developed to stimulate the vestibular system, may have a significant effect on the outcome of pAVS. A Cochrane review in 2015 on unilateral peripheral vestibular dysfunction found that vestibular rehabilitation was more effective than control or sham interventions in improving objective and subjective reports of symptomatology. However, only a few of these studies have focused on acute vestibular dysfunction and mainly covered cases of surgery for vestibular neuromas and BPPV (8). Additionally, the focus was on vestibular rehabilitation in general rather than early-vestibular rehabilitation training (early VRT). To our knowledge, no other systematic review on early VRT for pAVS exists. Other related reviews concern vestibular rehabilitation/vestibular rehabilitation therapy for vestibular neuritis/vestibular neuronitis (9–11). The lack of knowledge regarding early VRT for pAVS, other than iatrogenic dysfunction and BPPV, raises the following question:
What are the effects of early VRT combined with corticosteroid, initiated within 2 weeks, on recovery from pAVS?
This systematic review aimed to investigate the outcomes of vestibular rehabilitation combined with corticosteroids initiated within 2 weeks of pAVS onset compared with corticosteroids.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used for this systematic review (12). This study was registered with PROSPERO (CRD42023422308). Approval of the study by the institutional review board or the Danish Research Ethics Committee was not required.
Randomized clinical trials (RCTs) involving patients treated with early VRT for pAVS were included (Table 1). Early VRT can be delivered in combination with corticosteroids, as this is regarded standard care. The Covidence data-screening tool (13) was used to screen the references.
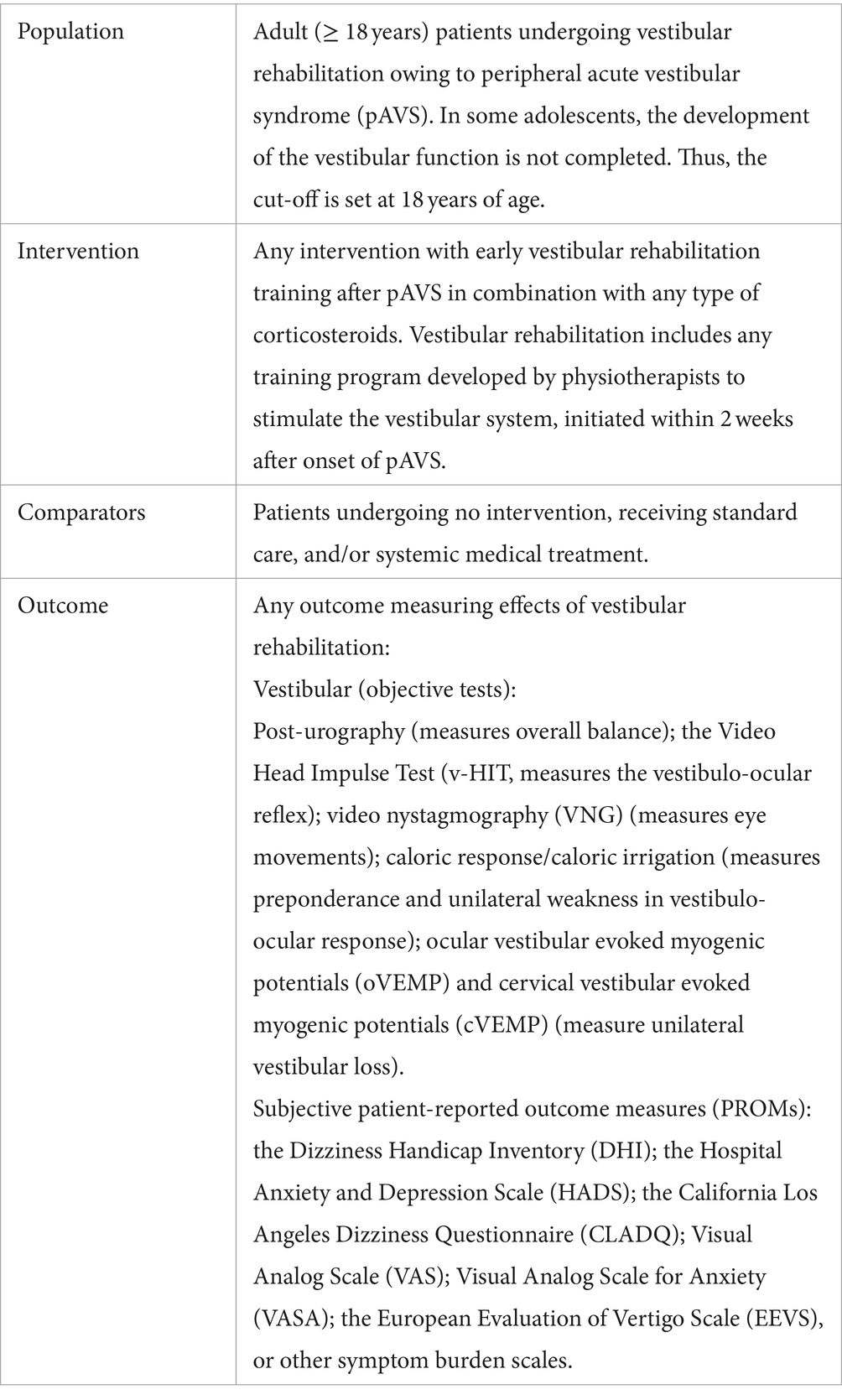
Table 1. Study inclusion criteria according to PICO: population, intervention, comparators, and outcome.
Studies of cAVS, BPPV, or chronic dizziness were excluded. Despite its acute onset, BPPV is considered an episodic syndrome and was excluded from the review because repositioning maneuvers are the treatment of choice. RCTs with less than 30 participants, representing a minimum of 15 participants in each group, were excluded and so was non-RCTs.
On March 7, 2023, we conducted an initial literature search of the PubMed, EMBASE, CINAHL, and SCOPUS electronic bibliographic databases. The search strategy included both MeSH terms and free text searches for acute dizziness, acute vertigo, dizziness, vertigo AND vestibular rehabilitation, therapy, physical therapy, AND randomized controlled trial OR RCT. Further search restrictions included English language and publication years after 1999. The search protocols are presented in Supplementary Table S1.
We searched for relevant RCTs assessing the effect of early VRT in combination and compared with corticosteroids, placebo, or no intervention in patients with pAVS. The last search date was January 24, 2024, and no studies were added to the interval separating the two searches.
Data were extracted from five eligible publications by HAN and TG, and when available, mean differences and standard deviations (SD), 95% confidence intervals, and p values were extracted. The data were pooled for meta-analysis of the Dizziness Handicap Inventory (DHI). For the remaining outcomes, the data could not be numerically synthesized owing to considerable heterogeneity, between-study variations in outcome measures and follow-up times, and differences in the rehabilitation protocols.
The Consensus on Exercise Reporting Template (CERT) (14) was applied to evaluate whether the applied vestibular rehabilitation protocols were completely and explicitly reported (Supplementary Table S2).
The risk of bias was evaluated by the Cochrane Collaboration’s Tool for assessing the Risk Of Bias (ROB-2) (15).
To assess study quality and evidence, we adopted the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) (16) approach. This approach ensures a transparent and structured process for developing and presenting a summary of the evidence.
Consensus on the GRADE quality of evidence and importance of outcomes in the included RCTs was obtained by HAN and TG, and TO made the final decision in the case of discrepancies.
A random-effects model was used for the meta-analysis. Meta-analysis was done on DHI using means and standard deviations, version 18.0 STATA. A random-effects model was chosen to ensure more trustworthy estimates despite large heterogeneity at baseline measurement of DHI. A random effect model takes into account that the standard error of the estimate differs between the studies. For DHI, an analysis on heterogeneity was conducted. A narrative synthesis of the following outcomes was performed for the remaining data: caloric lateralization, vestibular-evoked myogenic potentials (VEMP), posturography, visual analog scale (VAS), and Dynamic Gait Index (DGI).
The preliminary search identified 1,296 publications, of which 35 were excluded, as described in the PRISMA (12) flowchart in Figure 1. Thus, 1,261 publications were screened by title and abstract by HAN and TG using the Covidence software. We excluded 1,215 publications based on the predefined exclusion criteria. Subsequently, 46 publications were read in full by HAN and TG. Thereafter, the reference lists of the publications were screened for relevant studies. In cases of disagreement regarding eligibility, TO made the final decision on whether to include or exclude the study. A total of 41 publications were excluded from the analysis. Thus, five publications conducted by HAN, TG, and TO were included in the final review.
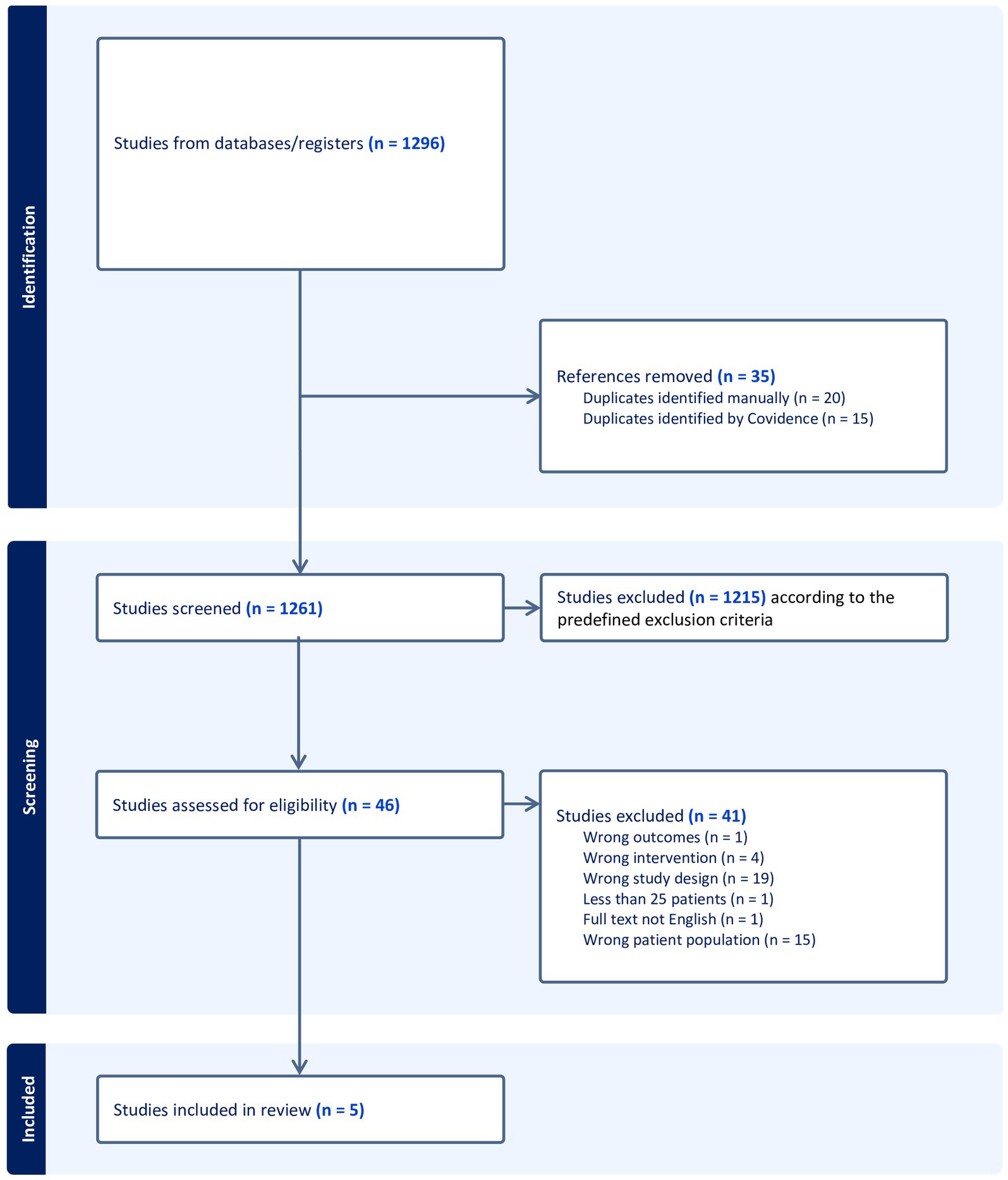
Figure 1. PRISMA flowchart.
Table 2 provides an overview of the five included RCTs (17–21) of early VRT plus corticosteroids initiated within 2 weeks after pAVS onset, with a focus on the intervention arms, outcome measures, and results reported. In Supplementary Table S2 the baseline characteristics of the included studies are described. There are no differences between the groups at baseline, in any of the studies included.
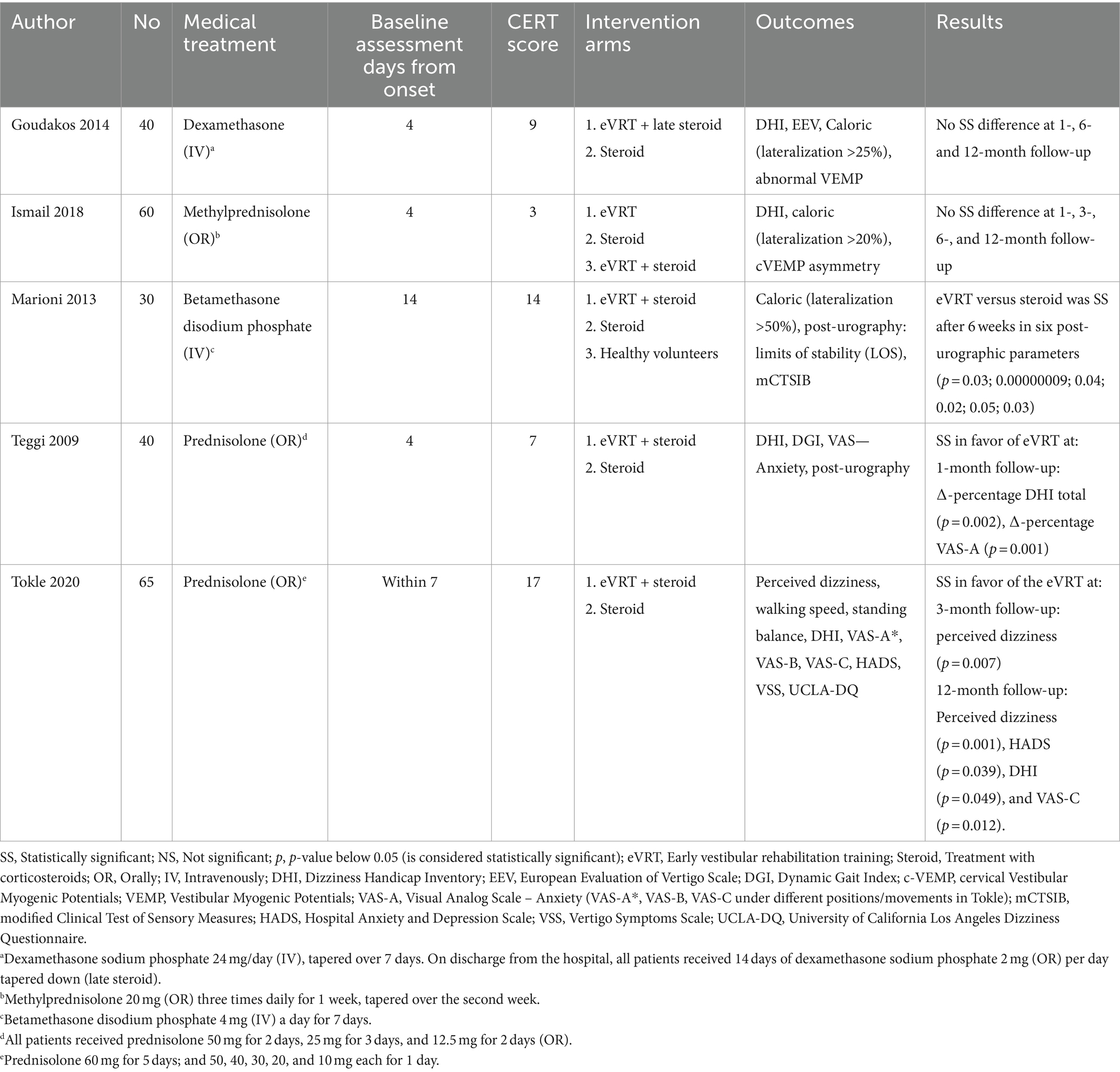
Table 2. Overview of the included randomized controlled trials (RCTs) of the early VRT in case of peripheral acute vestibular syndrome (pAVS).
The specific protocols for vestibular rehabilitation are described in Supplementary Table S3. In Table 2, the total CERT scores are displayed; the results range from 3 to 17. The maximum possible score was 19 points. In the included studies, one intervention arm received corticosteroid treatment, and one arm received early VRT plus corticosteroid treatment. Only one study by Ismail et al. included an intervention arm with early VRT as a stand-alone treatment, and one study by Marioni et al. included an intervention arm with healthy volunteers.
No studies were found that compared early VRT without corticosteroids with no treatment. A study from Yoo et al. compared corticosteroid therapy with no medical treatment, with both groups being instructed to do vestibular exercises plus taking Ginkgo biloba, and found that there was no additional effect of corticosteroids (22). Another study by Kammerlind et al. found no differences in outcome for groups performing home training and one group performing additional physical therapy (23). Yet, another study by Strupp et al. found that corticosteroid was superior to valacyclovir in treating vestibular neuritis (24).
The risk of bias was evaluated using ROB-2, and the domains of the included RCTs were assessed (Table 3). Blinding of patients and personnel was difficult, and four of five studies fail. One in four fail in blinding statistician. Two out of five studies fail in describing if the statistician was blinded. One study is at risk of selective outcome reporting due to missing description of dropouts.
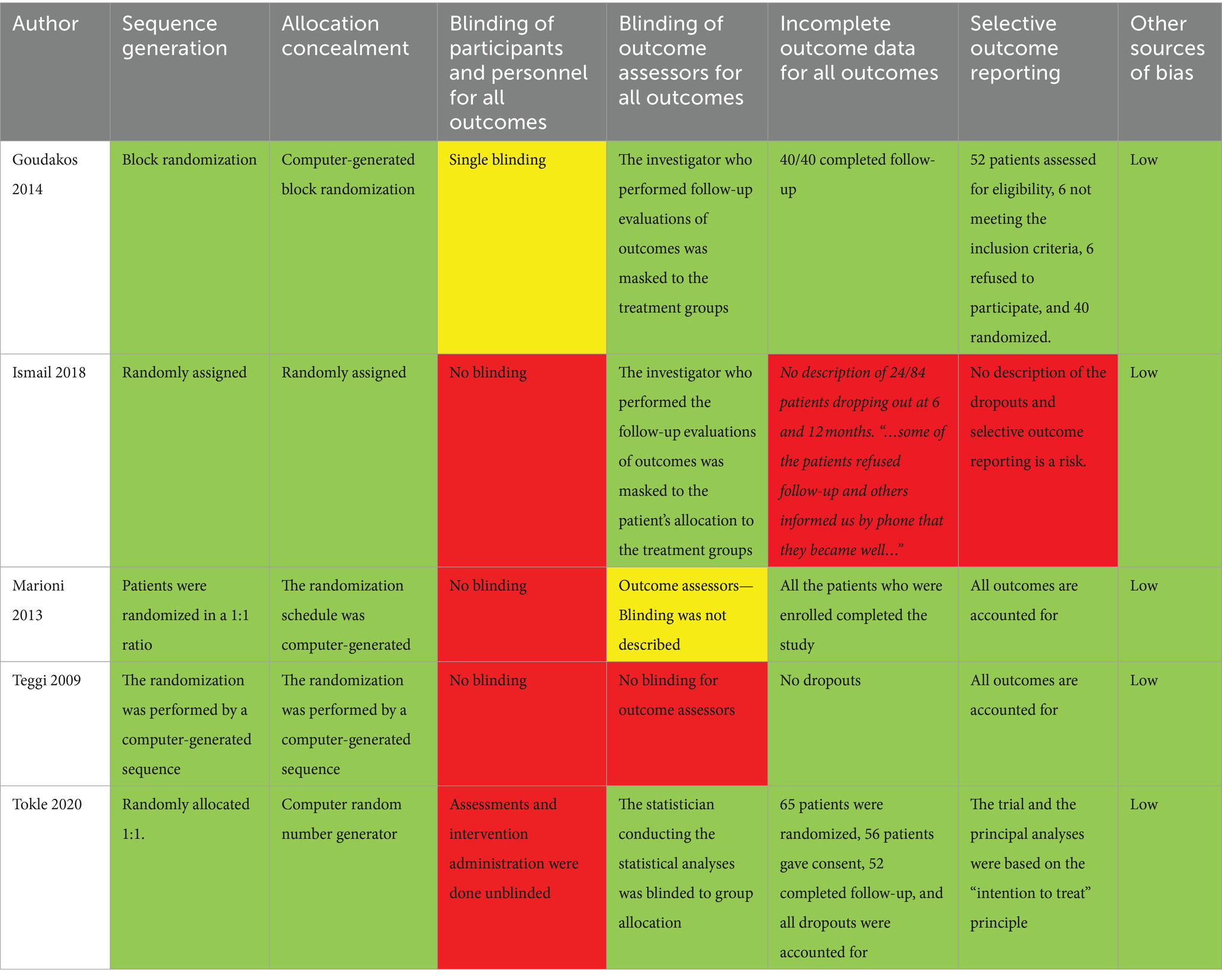
Table 3. Risk of bias of the included studies investigating the early vestibular rehabilitation training (eVRT) in peripheral acute vestibular syndrome (pAVS).
As DHI was included as an outcome measure in four studies, a meta-analysis of the extracted DHI results was performed (Table 4; Figure 2). Table 4 presents the meta-analyses of mean DHI in different time points. In all follow-up periods the means of DHI are very similar, demonstrating homogeneity. However, in the baseline, high heterogeneous results of DHI are given. Heterogeneity was high at baseline 98% in early VRT plus corticosteroid group and corticosteroid group; however, very low at any of the follow-ups.

Table 4. Descriptive results from the dizziness handicap inventory (DHI) in different studies.
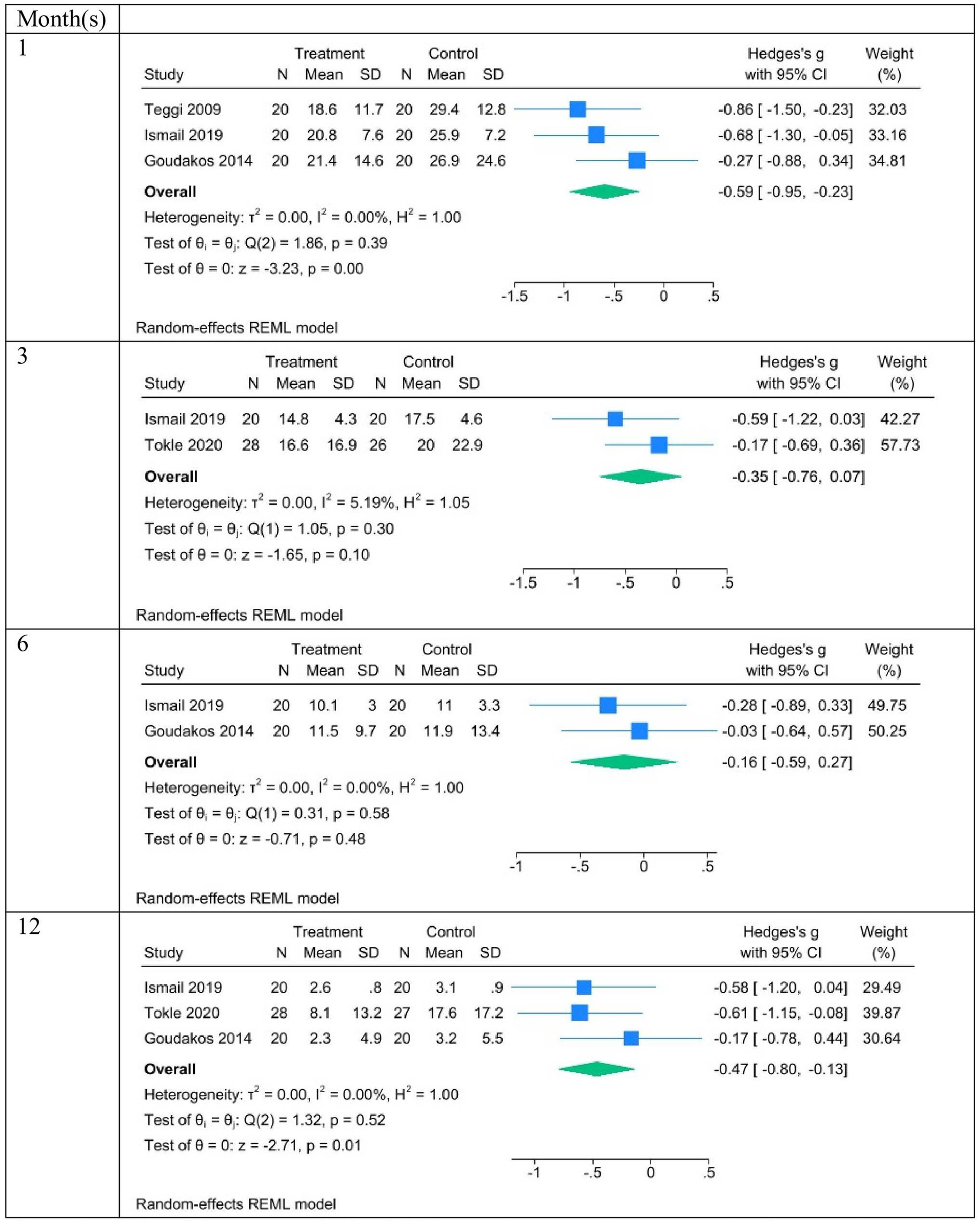
Figure 2. Forest plots of the difference between the treatment (early VRT plus corticosteroid) and control (corticosteroid) groups for all follow-up months.
Figure 2 shows the meta-analyses of DHI differences between the treatment (early VRT plus corticosteroid) and control (corticosteroid) groups at all follow-ups. The estimated effect was a statistically significant reduction of DHI in the early VRT plus corticosteroid group after 1 month −0.59 CI(−0.95, −0.23); I2 = 0.0%; p = 0.00. Moreover, the reduction was also statistically significant after 12 months of follow-up. The estimated effect was −0.47 CI(−0.8, −0.13); I2 = 0.0%; p = 0.01. In the follow-up after three and 6 months, with only two studies included, a reduction was found, but it was not significant. That is, in pAVS, early VRT plus corticosteroids was more effective than corticosteroids, as measured after 1 and 12 months, in improving subjective dizziness measured with DHI.
Table 5 summarizes the relevant outcomes investigated in these studies. The DHI was the only questionnaire used in more than one study (see the DHI meta-analysis) (Figure 2).
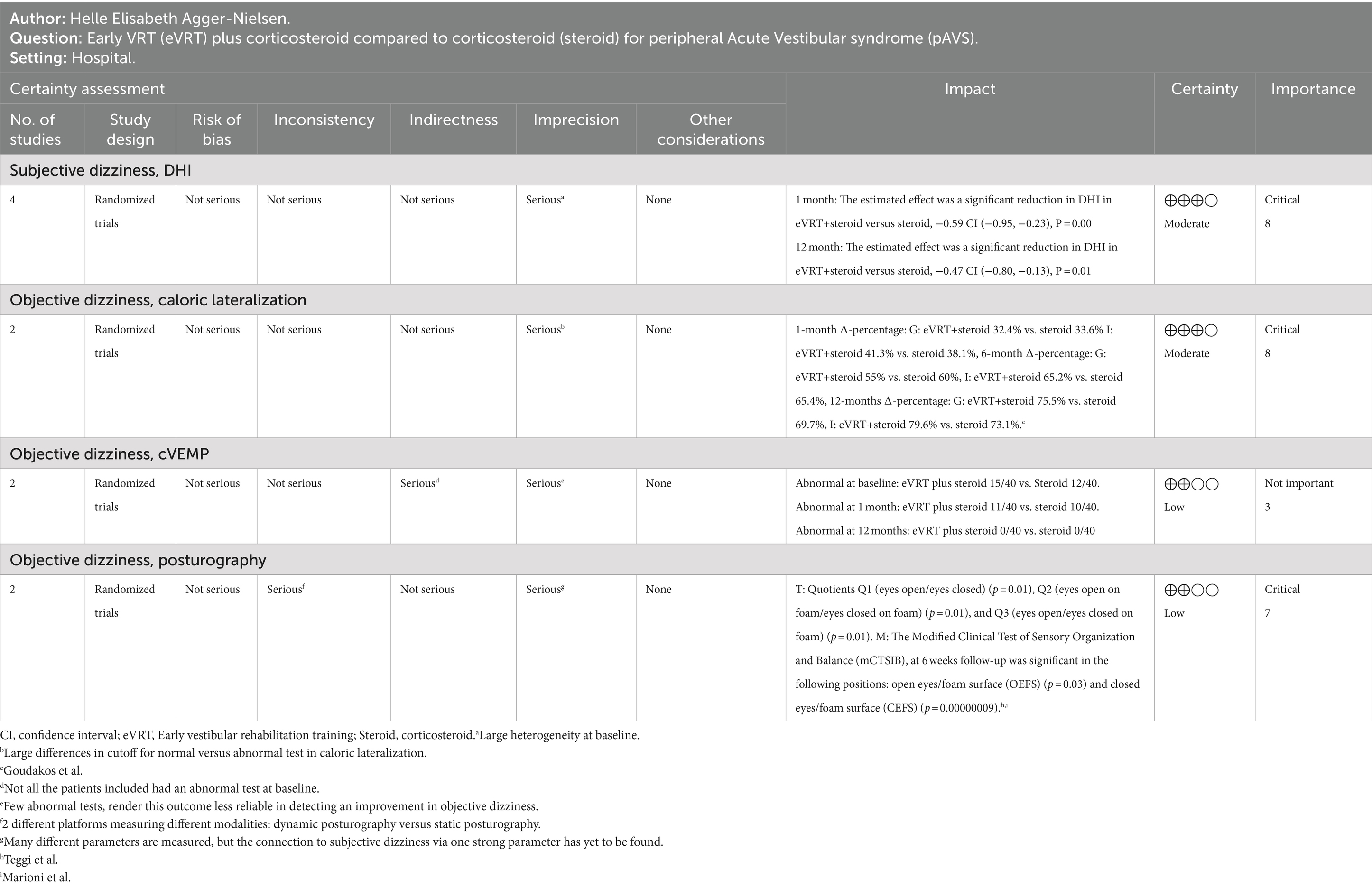
Table 5. Summary of findings: GRADE on patient-important outcomes.
The subjective outcome measures were addressed for the GRADE evaluation:
DHI was downgraded due to large heterogeneity at baseline. The certainty of evidence was moderate, and the importance of the outcome was critical.
The other outcome measures investigated in these studies have not been described in further detail. Subjective dizziness outcome measures, including the Hospital Anxiety and Depression Scale, Los Angeles Dizziness Questionnaire, VAS, VAS for Anxiety, and European Evaluation of Vertigo Scale questionnaires, were applied only in one study, and data pooling was therefore impossible. The Perceived Dizziness Test was used in only one study; therefore, pooling was irrelevant.
The objective outcome measures were addressed for the GRADE evaluation:
Caloric lateralization was downgraded due to imprecision in different cutoff values. The certainty of evidence was moderate, and the importance of the evidence was critical. In caloric lateralization, the data from two studies are presented as ∆-percentages from baseline to 1, 6, and 12 months. The ∆-percentage may seem significant at 12 months (75.5% vs. 69.7%); however, the different cut-off values and limited data from only these two studies did enable further analysis. Goudakos et al. considered caloric lateralization abnormal if it was >25%, and Ismail et al. considered a 20% lateralization or higher abnormality. Marioni et al. reported that more than 50% of the cases of vestibular weakness were abnormal. Owing to these large differences in cut-off values, a meta-analysis could not be conducted.
Cervical vestibular evoked myogenic potential (cVEMP) was downgraded due to indirectness and imprecision. The large number of normal tests in the affected patients renders this outcome useless for detecting of change in dizziness. The certainty of the evidence was low, and the outcome was not important. The cVEMP data of 80 patients with pAVS are reported in Supplementary Table S3.
Posturography was downgraded due to different ways of measuring, with two different platforms. This measure was further downgraded due to imprecisions as multiple parameters instead of one solid parameter are at play. The certainty of the evidence is low, and the importance of the evidence was critical. The posturographic outcome measures were significant and in favor of the early VRT group for several parameters in both studies. However, between-study differences in the outcomes obtained from posturography rendered further analysis impossible.
DGI was used in only one study; therefore, data pooling was not possible.
According to the meta-analysis of differences, early VRT plus corticosteroids reduced DHI compared with corticosteroid in pAVS. This effect was significant at 1 and 12 months. Due to the small number of studies (reduced power), the meta-analyses revealed no significant reduction in the follow-up of at 3 and 6 months. The essence of the present systematic review was that the GRADE evaluation suggested that early VRT and corticosteroids affect objective outcome measures. The GRADE evaluation process underlines the importance of remaining attentive to minor potential effects and considering all results that could contribute to the evaluation. However, none of these effects were significant except for DHI.
The number of included studies was consistent with that of other studies on related topics. Hidayati et al. (10) included four RCTs in a systematic review on vestibular rehabilitation and corticosteroids for vestibular neuritis, and García-Mûnoz et al. included five RCTs in a systematic review on vestibular training for patients with multiple sclerosis (25). In a systematic review by Chen et al. (9) on vestibular rehabilitation training combined with anti-vertigo drugs for vertigo and balance function in patients with vestibular neuritis, 18 of the 21 studies originated from China and could be found only via searches of Chinese literature databases. Some relevant studies may have been missed in the present review because they were Chinese.
The five RCTs reported homogeneous intervention groups. Geographically, the five studies were conducted in various countries, from Norway to Egypt, which might have posed a risk of cultural bias. Thus, the review by Chen et al. mentioned above had results that were in line with ours in terms of DHI meta-analyses.
Generally, the risk of bias was low in the included studies. The lack of blinding of the intervention was considered a bias. However, blinding of physical exercise is almost impossible. None of the included studies reported how and by whom the patients were screened for inclusion. The studies only included patients who had spontaneous nystagmus for several days, with a baseline assessment on day 4–14. Thus, milder and less grave cases of pAVS were missed because of the disappearance of nystagmus. Remission of spontaneous nystagmus associated with vestibular neuritis often occurs within days; however, patients continue to complain of vertigo (26). Dynamic visual acuity (DVA) has been proposed as an outcome measure for testing and rehabilitating the vestibular ocular reflex in acute peripheral hypofunction (27). In the study by Michel et al., the largest improvement in DVA score was found in the early rehabilitation group (p < 0.001) rather than in the late rehabilitation group. Both groups showed a statistically significant improvement. However, owing to the lack of randomization, spontaneous remission was not considered.
The DHI questionnaire might introduce a source of bias because translation, interpretation, and cultural adaptation may differ according to country and language. The DHI was translated and cross-culturally adapted to the languages of the RCTs included in the review.
This meta-analysis demonstrated a statistically significant effect of early VRT plus corticosteroids compared with corticosteroids at 1 and 12 months of follow-up.
In this review, VEMP as a parameter of recovery was not a useful outcome measure because only 27/80 patients had abnormal test results at baseline. Ocular VEMPs and cervical VEMPs offer insight into the location of the lesion in pAVS and may provide information on recovery in patients with abnormal test results (28). Other studies found insignificant differences in VEMP between the corticosteroid and vestibular rehabilitation groups (10).
The included studies were characterized by considerable differences in how well the early VRT intervention was described. This is presented in Supplementary Table S2, which was evaluated using the CERT. The scores range from 3 to 17 out of 19 points. In some RCTs, the type of intervention and the specific type of exercise chosen were barely described. The dosage of medication and type and dosage of intervention with early VRT were crucial to the outcome. None of the studies reported compliance or adherence to the interventions, whereas some reported adverse events. The study by Goudakos et al. was the only one to report the occurrence of adverse events.
One study reported an adverse event in the form of hyperglycemia, after which corticosteroid treatment was discontinued. None of the included RCTs provided compliance data and only one mentioned compliance.
Meta-analyses of RCTs generally provide reliable results on effective outcome measures and their implications for interventions.
Marioni et al. (18) entitled their publication a “randomized investigation” as they used a computer-generated randomization schedule and as such met the criterion to be considered an RCT. We chose to include their RCT in this systematic review because the data could potentially be used for meta-analysis; however, raw data from their study were not included in the meta-analysis.
Only patients with vestibular neuritis participated in four of the included RCTs. One RCT investigated unilateral peripheral vestibular disorders; however, the diagnostic criteria were set to primarily include vestibular neuritis because normal audiometry was required. Vestibular neuritis often improves spontaneously over time. Because of the self-limiting behavior of this condition, it is challenging to demonstrate a significant effect of early VRT. The solution would be large-scale, well-performed RCTs on vestibular rehabilitation.
Further studies should include a precise description of the applied vestibular rehabilitation program. A consensus on the program is important because it may considerably affect outcomes. As in other medical trials, a lack of research description may disqualify it. Subjective and objective measures of dizziness improvement should include validated questionnaires such as the DHI (at 1 week, 4–6 weeks; and 3, 6, and 12 months). The DHI should be combined with a simple VAS score (0–100) or other simple questions in the acute phase. The objective outcome measures should preferably be video-head impulse testing (v-HIT), caloric lateralization, posturography, or VNG.
The research questions were then answered; early VRT plus corticosteroids is statistically significant in improving subjective dizziness in pAVS, as illustrated via the meta-analysis of DHI. Early VRT is safe and no serious adverse events have been reported in any RCTs. Caloric lateralization and posturography suggested that early VRT plus corticosteroid was more effective than corticosteroid treatment. However, the studies are inhomogeneous in many respects, which impedes meta-analyses.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
HAN: Writing – original draft, Writing – review & editing. TG: Writing – review & editing. GB-B: Writing – review & editing. TO: Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Morten Pilegaard (www.vidkom.dk) and Editage (www.editage.com) for English language editing. We would like to thank Christian Mirian Larsen for his comments in the early stages of the review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1396891/full#supplementary-material
1. Hotson, JR, and Baloh, RW. Acute vestibular syndrome. N Engl J Med. (1998) 339:680–5. doi: 10.1056/NEJM199809033391007
2. Saber Tehrani, AS, Kattah, JC, Kerber, KA, Gold, DR, Zee, DS, Urrutia, VC, et al. Diagnosing stroke in acute dizziness and vertigo: pitfalls and pearls. Stroke. (2018) 49:788–95. doi: 10.1161/STROKEAHA.117.016979
3. Strupp, M, Hüfner, K, Sandmann, R, Zwergal, A, Dieterich, M, Jahn, K, et al. Central oculomotor disturbances and nystagmus: a window into the brainstem and cerebellum. Dtsch Arztebl Int. (2011) 108:197–204. doi: 10.3238/arztebl.2011.0197
4. Kattah, JC . Use of HINTS in the acute vestibular syndrome. An overview. Stroke Vasc Neurol. (2018) 3:190–6. doi: 10.1136/svn-2018-000160
5. Newman-Toker, DE . Missed stroke in acute vertigo and dizziness: it is time for action, not debate. Ann Neurol. (2016) 79:27–31. doi: 10.1002/ana.24532
6. Edlow, JA, Carpenter, C, Akhter, M, Khoujah, D, Marcolini, E, Meurer, WJ, et al. Guidelines for reasonable and appropriate care in the emergency department 3 (GRACE-3): acute dizziness and vertigo in the emergency department. Acad Emerg Med Off J Soc Acad Emerg Med. (2023) 30:442–86. doi: 10.1111/acem.14728
7. Meng, L, Liang, Q, Yuan, J, Li, S, Ge, Y, Yang, J, et al. Vestibular rehabilitation therapy on balance and gait in patients after stroke: a systematic review and meta-analysis. BMC Med. (2023) 21:322. doi: 10.1186/s12916-023-03029-9
8. McDonnell, MN, and Hillier, SL. Vestibular rehabilitation for unilateral peripheral vestibular dysfunction. Cochrane Database Syst Rev. (2015) 1:CD005397. doi: 10.1002/14651858.CD005397.pub4
9. Chen, J, Liu, Z, Xie, Y, and Jin, S. Effects of vestibular rehabilitation training combined with anti-vertigo drugs on vertigo and balance function in patients with vestibular neuronitis: a systematic review and meta-analysis. Front Neurol. (2023) 14:1278307. doi: 10.3389/fneur.2023.1278307
10. Hidayati, HB, Imania, HAN, Octaviana, DS, Kurniawan, RB, Wungu, CDK, Rida Ariarini, NN, et al. Vestibular rehabilitation therapy and corticosteroids for vestibular neuritis: a systematic review and Meta-analysis of randomized controlled trials. Medicina (Kaunas). (2022) 58. doi: 10.3390/medicina58091221
11. Huang, HH, Chen, CC, Lee, HH, Chen, HC, Lee, TY, Tam, KW, et al. Efficacy of vestibular rehabilitation in vestibular neuritis: a systematic review and Meta-analysis. Am J Phys Med Rehabil. (2024) 103:38–46. doi: 10.1097/PHM.0000000000002301
12. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clin Res ed). (2021) 372:n71. doi: 10.1136/bmj.n71
13. Covidence VHI . Covidence systematic review software. Available at: www.covidence.org: Veritas Health Innovation; (2023).
14. Slade, SC, Dionne, CE, Underwood, M, and Buchbinder, R. Consensus on exercise reporting template (CERT): explanation and elaboration statement. Br J Sports Med. (2016) 50:1428–37. doi: 10.1136/bjsports-2016-096651
15. Higgins, JPT TJ, Chandler, J, Cumpston, M, Li, T, Page, MJ, and Welch, VA, editors. Risk of Bias (ROB-2)—Cochrane handbook for systematic reviews of interventions version 6.4. Available at: www.training.cochrane.org/handbook; Cochrane; (2023)
16. Guyatt, GH, Oxman, AD, Vist, GE, Kunz, R, Falck-Ytter, Y, Alonso-Coello, P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. (2008) 336:924–6. doi: 10.1136/bmj.39489.470347.AD
17. Goudakos, JK, Markou, KD, Psillas, G, Vital, V, and Tsaligopoulos, M. Corticosteroids and vestibular exercises in vestibular neuritis. Single-blind randomized clinical trial. JAMA Otolaryngol Head Neck Surg. (2014) 140:434–40. doi: 10.1001/jamaoto.2014.48
18. Marioni, G, Fermo, S, Zanon, D, Broi, N, and Staffieri, A. Early rehabilitation for unilateral peripheral vestibular disorders: a prospective, randomized investigation using computerized posturography. Eur Arch Otorrinolaringol. (2013) 270:425–35. doi: 10.1007/s00405-012-1944-4
19. Ismail, EI, Morgan, AE, and Abdel Rahman, AM. Corticosteroids versus vestibular rehabilitation in long-term outcomes in vestibular neuritis. J Vestib Res. (2018) 28:417–24. doi: 10.3233/VES-180645
20. Teggi, R, Caldirola, D, Fabiano, B, Recanati, P, and Bussi, M. Rehabilitation after acute vestibular disorders. J Laryngol Otol. (2009) 123:397–402. doi: 10.1017/S0022215108002983
21. Tokle, G, Mørkved, S, Bråthen, G, Goplen, FK, Salvesen, Ø, Arnesen, H, et al. Efficacy of vestibular rehabilitation following acute vestibular neuritis: a randomized controlled trial. Otol Neurotol. (2020) 41:78–85. doi: 10.1097/MAO.0000000000002443
22. Yoo, MH, Yang, CJ, Kim, SA, Park, MJ, Ahn, JH, Chung, JW, et al. Efficacy of steroid therapy based on symptomatic and functional improvement in patients with vestibular neuritis: a prospective randomized controlled trial. Eur Arch Otorhinolaryngol. (2017) 274:2443–51. doi: 10.1007/s00405-017-4556-1
23. Kammerlind, AS, Ledin, TE, Odkvist, LM, and Skargren, EI. Effects of home training and additional physical therapy on recovery after acute unilateral vestibular loss – a randomized study. Clin Rehabil. (2005) 19:54–62. doi: 10.1191/0269215505cr830oa
24. Strupp, M, Zingler, VC, Arbusow, V, Niklas, D, Maag, KP, Dieterich, M, et al. Methylprednisolone, valacyclovir, or the combination for vestibular neuritis. N Engl J Med. (2004) 351:354–61. doi: 10.1056/NEJMoa033280
25. García-Muñoz, C, Cortés-Vega, MD, Heredia-Rizo, AM, Martín-Valero, R, García-Bernal, MI, and Casuso-Holgado, MJ. Effectiveness of vestibular training for balance and dizziness rehabilitation in people with multiple sclerosis: a systematic review and meta-analysis. J Clin Med. (2020) 9:590. doi: 10.3390/jcm9020590
26. Curthoys, IS . Vestibular compensation and substitution. Curr Opin Neurol. (2000) 13:27–30. doi: 10.1097/00019052-200002000-00006
27. Michel, L, Laurent, T, and Alain, T. Rehabilitation of dynamic visual acuity in patients with unilateral vestibular hypofunction: earlier is better. Eur Arch Otorrinolaringol. (2020) 277:103–13. doi: 10.1007/s00405-019-05690-4
Keywords: acute vestibular syndrome, acute dizziness, vestibular rehabilitation, acute unilateral vestibular loss, vestibular neuritis, systematic review, meta-analysis, corticosteroid
Citation: Agger-Nielsen HE, Grøndberg TS, Berg-Beckhoff G and Ovesen T (2024) Early vestibular rehabilitation training of peripheral acute vestibular syndrome—a systematic review and meta-analysis. Front. Neurol. 15:1396891. doi: 10.3389/fneur.2024.1396891
Edited by:
Diego Kaski, University College London, United KingdomReviewed by:
David Herdman, St George’s University Hospitals NHS Foundation Trust, United KingdomCopyright © 2024 Agger-Nielsen, Grøndberg, Berg-Beckhoff and Ovesen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helle Elisabeth Agger-Nielsen, aGFnZ2VybmllbHNlbkBoZWFsdGguc2R1LmRr
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.