
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 08 February 2024
Sec. Neuromuscular Disorders and Peripheral Neuropathies
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1360385
This article is part of the Research TopicDevelopment of the Precision Diagnostics and Treatment for Duchenne/Becker Muscular DystrophyView all 5 articles
 Lenka Juříková1
Lenka Juříková1 Lucia Masárová2*Roman Panovský2,3
Lucia Masárová2*Roman Panovský2,3 Martin Pešl2,3,4
Martin Pešl2,3,4 Kamila Žondra Revendová5,6
Kamila Žondra Revendová5,6 Ondřej Volný2,5,6Věra Feitová2,7Tomaš Holeček2,7,8Vladimír Kincl2,3Pavlína Danhofer1
Ondřej Volný2,5,6Věra Feitová2,7Tomaš Holeček2,7,8Vladimír Kincl2,3Pavlína Danhofer1 Stanislav Voháňka9
Stanislav Voháňka9 Jana Haberlová10Karolína Podolská10
Jana Haberlová10Karolína Podolská10In this prospective study involving 37 Duchenne muscular dystrophy (DMD) patients aged 8–18 years and older, we examined the impact of neurological and cardiac factors on quality of life (QoL). Our findings revealed a negative correlation between upper limb movement and overall mobility, self-service, and usual activities. Ambulatory and non-ambulatory DMD patients showed significant differences in mobility-related parameters. Cardiac evaluations demonstrated associations between mitral annular plane systolic excursion (MAPSE) and mobility-related aspects. The PEDSQL 3.0 neuromuscular model questionnaire further highlighted age-related and movement-related correlations with QoL. The loss of ambulatory status and reduced upper limb movement were negatively associated with QoL, while upper limb movement positively correlated with septal MAPSE. However, no significant associations were found between MAPSE and anxiety/depression. These findings underscore the multifaceted impact of DMD on QoL and emphasize the importance of considering both neurological and cardiac factors in comprehensive patient care.
The most common X-recessive inherited progressive muscular disease is Duchenne muscular dystrophy (DMD). It affects approximately 1:5000 living boys (1). The first symptoms of DMD manifest at the age of two years because of the absence of dystrophin protein, leading to gradual weakness and muscle injury (2).
DMD is still causally incurable (3). Due to the advances in medical care and symptomatic therapy, the life expectancy of DMD patients has been prolonged and their quality of life (QoL) has been improving (4, 5). Today, DMD patients live up to 30 or 40 years (6). It is well-known that DMD influences the QoL not only for patients, but also for their families (7–11).
According to the World Health Organization, QoL is defined as a person’s perception of their position in life including the culture and values in the system in which the person lives, correlating to a person’s goals, expectations, standards, and concerns. It is a complex of physical health, psychological status, level of independence, social relationships, personal beliefs, and a person’s relationship with various features of the environment (12). Published reports about the QoL in DMD patients are not uniform. Some of the previous studies reported a decline only in physical functions compared to healthy controls, while the others show that a whole spectrum of QoL parameters were decreased to age-matched controls (7, 13–15). The results may also have been influenced by self/proxy reports (by the parents/caregivers) (16–22) or by the help of pediatricians (14).
The Pediatric Quality of Life (PEDSQL) 3.0 Neuromuscular Module questionnaire among children/adolescents, EQ-5D, and Individualized Neuromuscular QoL questionnaire for adults are the most commonly used questionnaires in the published studies (23–26).
To date, only one study describing the QoL in DMD patients related to respiratory and cardiac functions including left ventricular ejection fraction (LVEF) evaluated by echocardiography and the presence or absence of electrocardiogram (ECG) abnormalities or cardiomyopathy has been published (27).
To our knowledge, there has been no prospective study describing the QoL of all-aged DMD patients in correlation with a complex evaluation firstly of neurological clinical status and cardiac impairment using cardiac magnetic resonance (CMR), and secondly of the influence of cardiac therapy or corticosteroid therapy, body mass index (BMI), and anxiety/sadness.
The main purpose of this prospective study was to investigate the QoL concerning neurological clinical status and cardiac impairment using CMR, and the influence of actual therapy, BMI, and anxiety/sadness in DMD patients based on a completed questionnaire.
DMD patients 8–18 years and older born in the Czech Republic were consecutively included between 01/2022 to 09/2023 in close cooperation with EndDuchenne (a patient advocacy group). All DMD patients were diagnosed based on their clinical symptoms and/or elevated creatine kinase, and confirmed by genetic testing. The most common genetic mutation was the deletion of 44–63 exons in 65% of our cohort.
This study was performed in accordance with the Declaration of Helsinki (2000) of the World Medical Association and was approved by the Institutional Ethics Committee (University Hospital Brno, reference number 20130410–03). All DMD patients or their parents (for patients younger than 18 years) signed the informed consent.
Every patient was examined by an experienced pediatric neurologist and also an experienced cardiologist including ECG and ECG Holter, and the following pieces of information were collected: demographic data (age, weight, height), current pharmacotherapy (corticosteroid therapy, beta-blockers, angiotensin converting enzyme inhibitors (ACEI), sartan-losartan (generic name of sartan), diuretics), comorbidities (hypertension, diabetes mellitus, chronic renal insufficiency), an actual feeling of dyspnoea and palpitations.
All DMD patients were monitored for respiratory status such as a need of nocturnal non-invasive positive pressure ventilation (NIPPV). Six DMD patients of our cohort use nocturnal NIPPV. Neurological clinical status included the following information - ambulatory/non-ambulatory, self-sitting or sitting requiring help, and the presence of scoliosis including a history of scoliosis surgery. Upper limb movement was assessed in 5 various degrees: preserved mobility, moderately limited mobility, limited mobility, very limited mobility, and work with touchpad/mouse.
DMD patients were divided into three groups based on age: 8–12 years, 13–18 years, and adult patients. All of them were asked to complete questionnaires for muscular dystrophy. The younger patients completed the PEDSQL 3.0 neuromuscular model questionnaire, and the older ones EQ-5D. Due to possible differences between self and proxy reports, we employed a PEDSQL 3.0 neuromuscular model questionnaire completed by DMD patients and their parents. All DMD patients and parents were instructed by an experienced pediatric neurologist how to complete the questionnaire in electronic version. None of the DMD patients were taking any psychotropic medications or opioids when the questionnaire was administered.
PEDSQL is an instrument used to assess Health-Related QoL (HRQoL) in children and adolescents aged 2 to 18. It consists of both generic core and disease-specific modules. The PEDSQL 3.0 Neuromuscular Module questionnaire is a disease-specific module for measuring children’s QoL assessing their neuromuscular disease, communication difficulties, and family resources. This instrument is acknowledged as a validated health outcome measure for patients with neuromuscular diseases (28). It was validated for the Czech Republic (29) for the DMD patient cohort and was translated into the Czech language. Its electronic version can be requested through this web page ePROVIDE™ - Online Support for Clinical Outcome Assessments.1
EQ-5D questionnaire is a standardized measure of HRQoL developed by the EuroQol Group to provide a simple, generic questionnaire for use in clinical and economic appraisal and population health surveys. EQ-5D assesses health status in terms of five dimensions of health and is considered a ‘generic’ questionnaire because these dimensions are not specific to a specific patient group or health condition. EQ-5D can also be referred to as a patient-reported outcome measure (PROM) because patients can complete the questionnaire themselves to provide information about their current health status and how this changes over time (30). It was validated for the Czech population for patients with chronic pain (31) and can be found on the following web page: Available versions – EQ-5D (euroqol.org).
After a baseline clinical check-up and collection of all patient information, the DMD patients underwent a neurological examination. On the same day the patients were examined, the questionnaire in the electronic version was completed. After completing the questionnaire, DMD patients were examined by CMR within one week after their clinical examination by a neurologist.
Inclusion criteria for CMR: the absence of CMR contraindications such as an implanted pacemaker/defibrillator, cochlear implant, other ferromagnetic metal parts in the patient’s body, claustrophobia, etc.; the absence of contraindications for using contrast media such as severe renal insufficiency; the patient’s ability to co-operate during CMR examination; no known cardiovascular pathology apart from dystrophin cardiomyopathies.
All DMD patients underwent the CMR according to our previously published protocol (32) using a 1.5 T scanner (Ingenia, Philips Medical Systems, Best, The Netherlands) equipped with 5- and 32-element phased array receiver coils allowing for the use of parallel acquisition techniques in the supine position in repeated breath-hold. Four DMD patients underwent CMR examination without application of contrast agent.
Functional imaging using balanced steady-state free precession cine sequences included four-chamber, two-chamber, and LV outflow tract long axis views, and a short axis stack from the cardiac base to the apex in the perpendicular plane to the LV long axis.
Late gadolinium enhancement (LGE) images in all long-axis views and the short-axis views were acquired 10 min after an intravenous bolus of 0.2 mmol/kg of the gadolinium-based contrast agent gadobutrol (Gadovist, Bayer-Schering Pharma, Germany) using an inversion-recovery turbo field echo sequence and, in case of doubt, also by phase-sensitive inversion recovery turbo field echo. Both 2-dimensional and 3-dimensional data acquisitions were performed in mid-diastole.
The following parameters were evaluated: LVEF, end-diastolic/end-systolic volume (EDV/ESV), septal/lateral/average mitral annular plane systolic excursion (MAPSE), presence/absence of LGE. LV functional and morphological parameters were calculated from the short axis view stack using the summation-of-disc methods in accordance with recommendations for post-processing evaluation from the Society for Cardiovascular Magnetic Resonance (33). Septal and lateral MAPSE was measured as previously described (34, 35) by defining end-diastolic and end-systolic mitral annular planes on a long-axis four-chamber view. The average MAPSE was calculated as the mean of septal and lateral MAPSE.
LGE was defined as an area of visually identified contrast enhancement greater than the mean signal intensity of an adjacent area of the reference myocardium. LGE was not evaluated in four DMD patients who underwent the examination without application of contrast agent.
The data were analyzed using Stata Statistical Software Release 17 (StataCorp, College Station, TX). The continuous variables were reported as means and standard deviations (SDs) or medians and interquartile ranges (IQRs) according to the data distribution. The normality of data was evaluated by the Shapiro–Wilk test. Categorical variables were reported as counts and percentages. The Spearman correlation was used to assess the relationship between the components of the PEDSQL 3.0 neuromuscular model questionnaire and EQ-5D, age, BMI, upper limb movement, and CMR parameters. Similarly, the relationship between upper limb movement and CMR parameters was evaluated using the Spearman correlation. The Spearman’s rank correlation coefficient was interpreted according to Prion and Haerling (36). The Wilcoxon rank-sum (Mann–Whitney) test was used to assess differences in the components of the PEDSQL 3.0 neuromuscular model questionnaire and EQ-5D between the predefined subgroups (heart failure treatment, current corticosteroid therapy, the ability to walk, the ability to sit, the presence of scoliosis, the presence of LGE). The difference between the categories of the PEDSQL 3.0 neuromuscular model questionnaire filled in by the parent or by the patient was evaluated using the Wilcoxon signed-rank test. All tests were two-tailed, and p values <0.05 were considered statistically significant.
A total of 37 DMD patients (median age 16.8 years) were enrolled in the final analysis. The basic demographic data are shown in Table 1. The detailed information about current corticosteroid therapy is shown in Table 2. Results from both questionnaires are shown in Table 3.
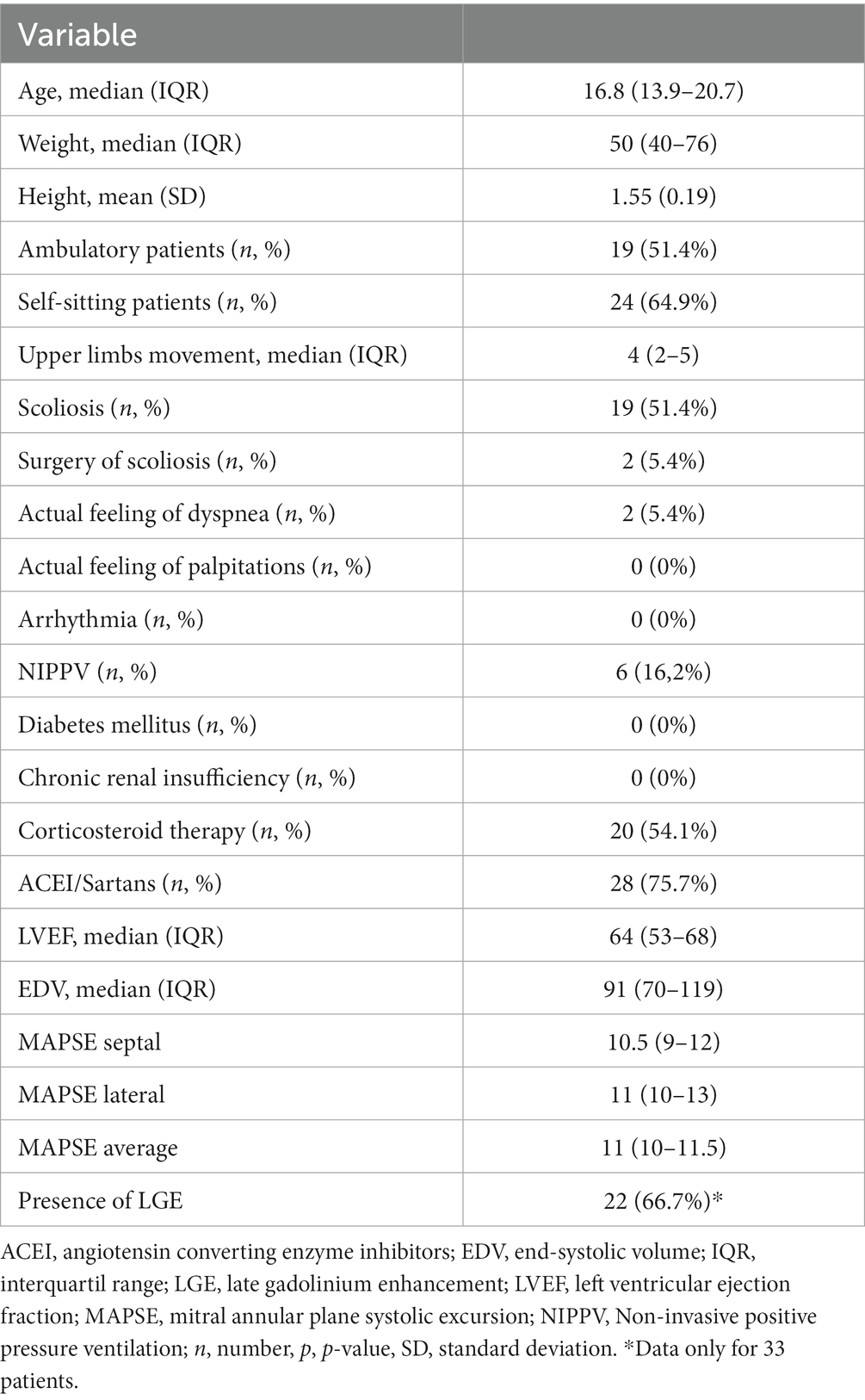
Table 1. Basic demographic data.
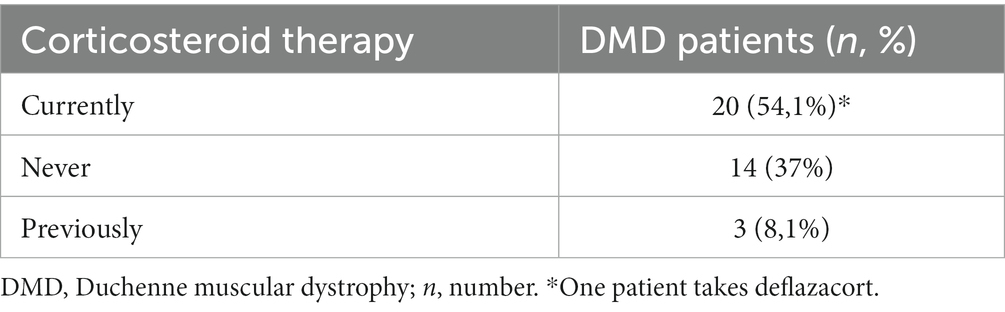
Table 2. Detailed information of corticosteroid therapy.
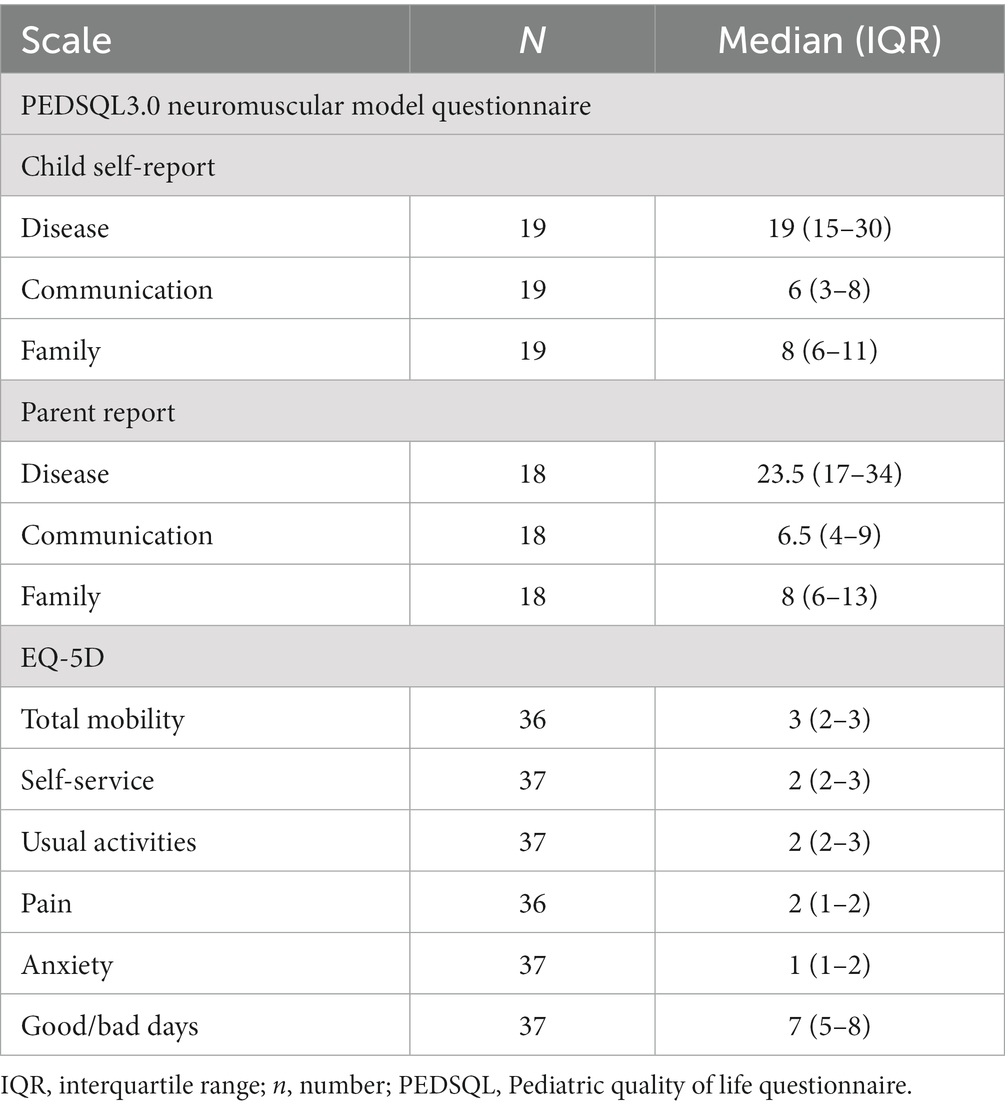
Table 3. PEDSQL 3.0 neuromuscular model and EQ-5D results.
DMD patients taking ACEI/sartans had better total mobility than DMD patients without therapy (p = 0.048).
There was a negative correlation between the movement of the upper limbs and total mobility (rs = −0.619, p = 0.0001), self-service (rs = −0.863, p < 0.001), and usual activities (rs = −0.765, p < 0.001). On the contrary, movement of the upper limbs positively correlated with good/bad days (rs = 0.515, p = 0.001). No correlation was found between the movement of the upper limbs, anxiety, and pain.
There was a statistically significant difference in total mobility (p < 0.001), self-service (p < 0.001), usual activities (p = 0.0001), and good and bad days (p = 0.0095) when comparing the ambulatory/non-ambulatory DMD patients (p < 0.001).
Similar results were found when comparing sitting/non-sitting DMD patients. There was a significant difference in total mobility (p < 0.001), self-service (p < 0.001), usual activities (p < 0.001), and good/bad days (p = 0.039) (see Table 4). No difference was found for anxiety and pain. DMD patients with or without scoliosis showed a statistical difference only on good/bad days (p = 0.011).
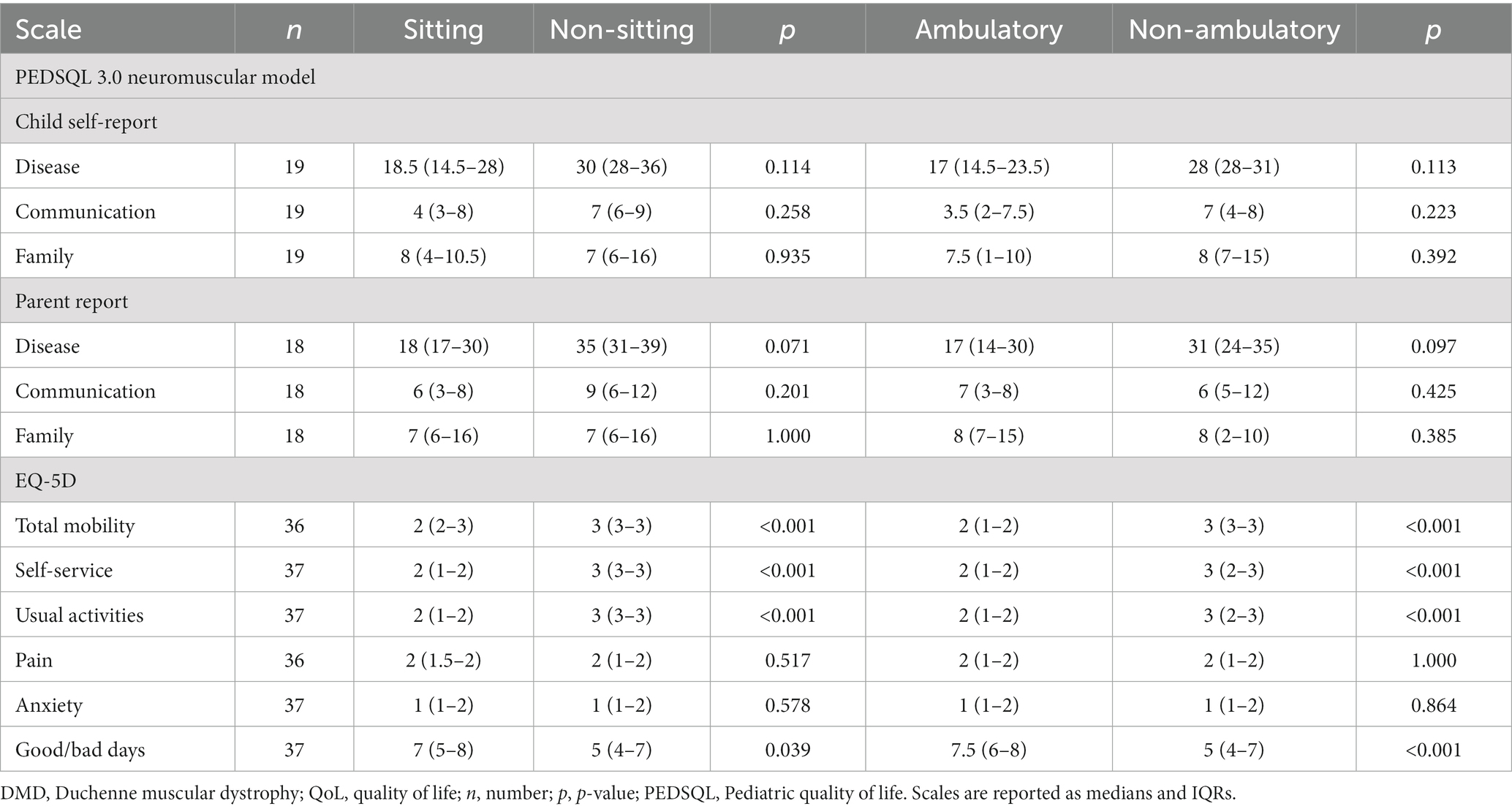
Table 4. QoL and neurological impairment in our DMD cohort.
When evaluating cardiac parameters, the following statistically significant correlations were found: a weak positive correlation between EDV and anxiety (rs = 0.330, p = 0.046), a weak negative correlation between average MAPSE and total mobility (rs = −0.386, p = 0.020), lateral MAPSE and total mobility (rs = −0.344, p = 0.040), septal MAPSE and total mobility (rs = −0.355, p = 0.034), and septal MAPSE and usual activities (rs = −0.342, p = 0.039) (Table 5).
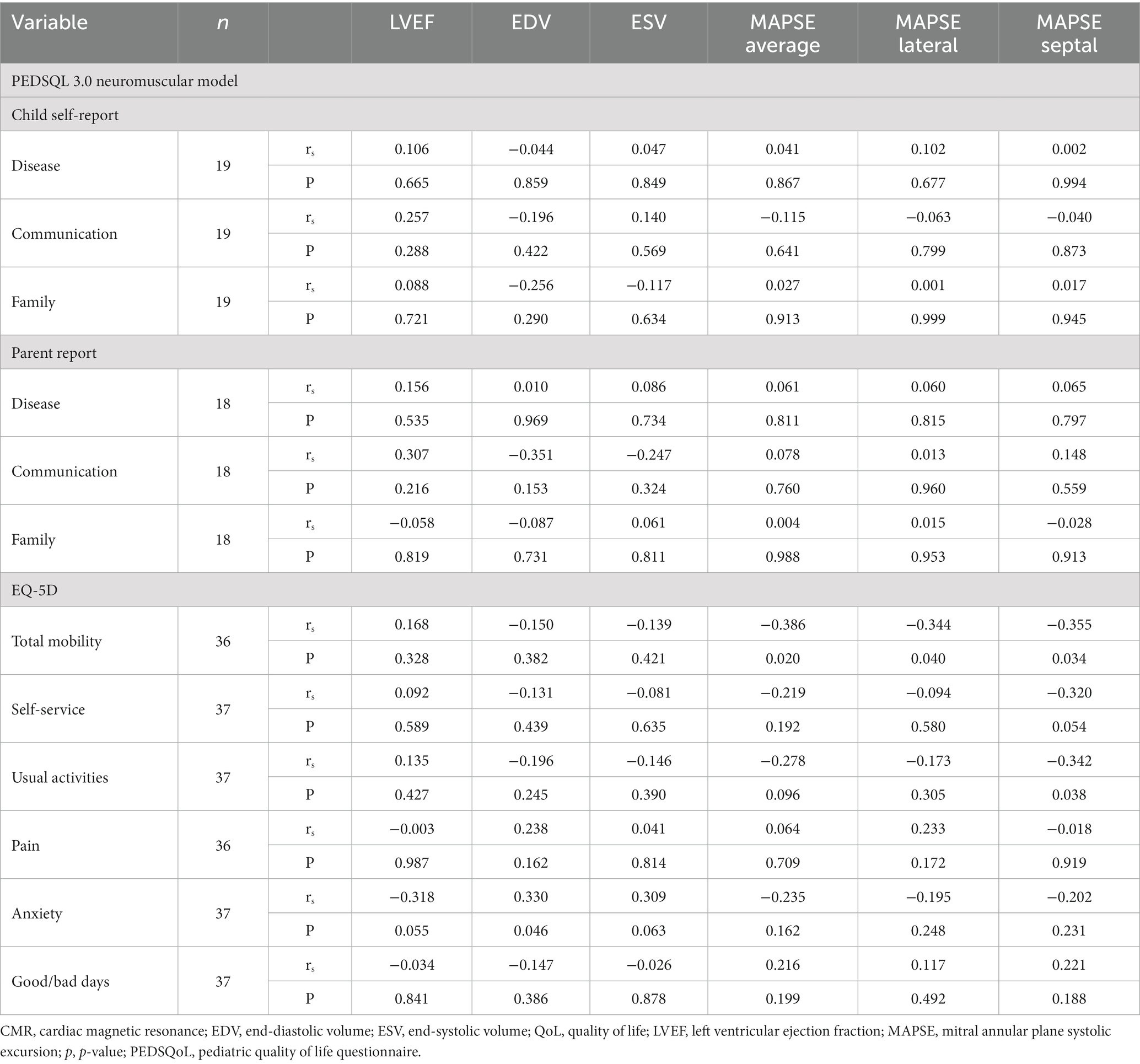
Table 5. Correlation between QoL and cardiac impairment using CMR.
DMD patients aged 8–18 (median 13.9 years, IQR 11.6–15.6) and their parents completed the PEDSQL 3.0 neuromuscular model questionnaire. A statistically significant differences in disease category was found between the PEDSQL 3.0 neuromuscular model questionnaires completed by the DMD patients and their parents (p = 0.008) (see Figure 1).
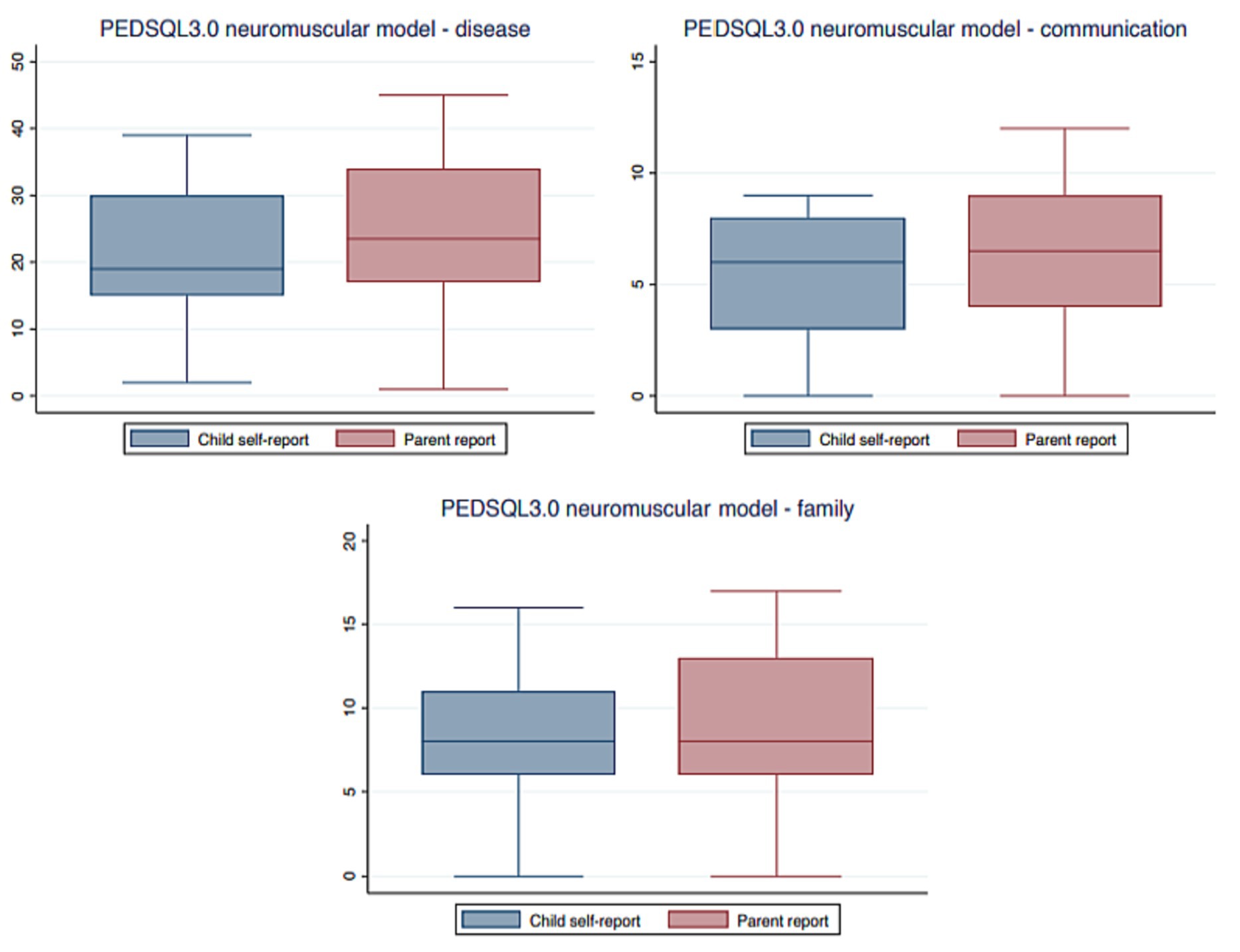
Figure 1. PEDSQL 3.0 neuromuscular model questionnaire completed by DMD patients and their parents. DMD, Duchenne muscular dystrophy; PEDSQL, pediatric quality of life questionnaire.
There was no significant difference in the PEDSQL 3.0 neuromuscular model questionnaire for DMD patients taking or not taking ACEI/sartans, nor for those taking or not taking corticosteroids.
BMI did not correlate with any of the evaluated parameters in the PEDSQL 3.0 neuromuscular model questionnaire.
QoL negatively correlated with movement of the upper limbs using PEDSQL 3.0 neuromuscular model questionnaire in the disease category completed by the DMD patients (rs = −0.748, p = 0.0002) and by the parents (rs = −0.742, p = 0.0004).
Movement of upper limbs positively correlated with septal MAPSE (rs = 0.3422, p = 0.038).
This was the first prospective study describing a detailed evaluation of the QoL in DMD patients of various ages and degrees of disability in relation to functional neurological and cardiac impairment. The most important results of our prospective study were the relation/association between:
1. Better movement of the upper limbs and total mobility, self-service, and good/bad days, but not usual activities.
2. Decreased QoL and movement of the upper limbs using the PEDSQL 3.0 neuromuscular model questionnaire in disease category completed both by DMD patients and their parents.
3. Movement of the upper limbs and septal MAPSE also trended toward average MAPSE.
4. Scoliosis and good/bad days.
5. EDV and anxiety/depression, but not average MAPSE and overall mobility or lateral MAPSE and total mobility.
6. Septal MAPSE and total mobility or usual activities.
7. DMD patients taking ACEI/sartans had better overall mobility than DMD patients without therapy for heart failure.
Compared to the previously published studies focused on QoL in DMD patients (7, 8, 10, 11, 13–25, 27, 29, 37–39), we included all-aged DMD patients, we used the common questionnaires such as EQ-5D and PEDSQL 3.0 neuromuscular model questionnaire, and the results were not under/overestimated due to proxy reports as the PEDSQL 3.0 neuromuscular model questionnaire was completed both by DMD patients and their parents in our study. Possible reasons why DMD patients perceive their QoL as higher compared to their parents include fears about their child’s disorder, the adaptation of DMD patients to their disease, an inexact perception of a child’s status by their parents, limitations of the child, and the influence of environmental factors (13–15, 40). The results of our study were consistent with the previous studies, as the PEDSQL 3.0 neuromuscular model questionnaire completed by the parents showed more decreased QoL of DMD patients in the disease category compared to those who self-reported.
According to Powell et al., a comprehensive and reliable PROM of QoL including physical and social domain (41, 42) that is typically used for DMD patients (43–47) has a significant positive correlation with the PEDSQL 3.0 neuromuscular model questionnaire and the EQ-5D questionnaires used in our study (46). Moreover, we analyzed the most functional parameters related to the QoL for DMD patients that have ever been published.
When assessing the respiratory functions and QoL, the aspects of daily living and disability were highlighted in DMD patients on NIPPV compared to DMD patients without NIPPV. Regardless of the reduction in pulmonary function and daily living activities, DMD patients on NIPPV showed similar HRQoL to patients without NIPPV (27). The relationship between the physical and mental domains contrary to forced vital capacity did not show any statistically significant results (27). It is consistent with cardiomyopathy where DMD patients with or without cardiomyopathy reported similar disability scores (27). In our investigation, a minority of DMD patients necessitated nocturnal NIPPV; hence, we refrained from correlating its influence with the evaluated parameters.
In our study, we focused on cardiac function using CMR and QoL in DMD patients. Based on our previous study, Panovský et al. (48), DMD patients had impaired LV systolic function measured by MAPSE and global LV strain regardless of normal LVEF and the absence of LGE (48). The higher the EDV the higher anxiety/depression in DMD patients, whereas average MAPSE and total mobility or lateral MAPSE and total mobility were associated negatively. Similarly, decreasing septal MAPSE introduced reduced total mobility and usual activities. The better movement of the upper limbs the higher the septal MAPSE value. No arrhythmia was detected based on ECG Holter monitoring in our cohort. When evaluating the presence or absence of LGE and LVEF, there were no statistically significant differences observed in relation to any of the assessed parameters.
According to Porcher et al., DMD patients who take ACEI therapy prophylactically had significantly higher overall survival and lower rates of hospitalization for heart failure (49). This correlates with the results of our study that found DMD patients on ACEI/sartans had better overall mobility than DMD patients without therapy. Contrary to it, there was no significant difference for those taking ACEI/sartans according to the PEDSQL 3.0 neuromuscular model questionnaire.
It is well-known that corticosteroid therapy can improve physical functioning and prolong estimated life expectancy and HRQoL in muscular dystrophy patients (11, 39, 50). We concentrated on influence of current corticosteroid therapy in our cohort. The average age at which corticosteroid therapy was initiated in our cohort is 5 years. All patients receive prednisone at a dose of 0.75 mg/kg/day, with the exception of one patient who takes deflazacort at a dose of 0.9 mg/kg/day. Some patients chose not to undergo corticosteroid therapy due to the gradual progression of the disease or concerns about potential side effects. Additionally, DMD patients discontinued corticosteroid therapy when they were no longer ambulatory, despite some guidelines recommending its use for preventing heart or respiratory failure.
Concerning the QoL, DMD patients taking or not taking corticosteroid therapy did not show any differences in their PEDSQL 3.0 neuromuscular model questionnaire.
It was well-recognized that the administration of steroids can result in weight gain and short stature (51). In the case of our study, BMI did not correlate with any of the evaluated parameters in the PEDSQL 3.0 neuromuscular model questionnaire.
DMD patients usually do not complain of pain although their ability to manage pain is limited (52, 53). It was not the subject of our study.
Overall mobility in DMD is a crucial item of QoL (46). Younger DMD patients are usually more tired due to the extra work/effort required for movement, whereas older DMD patients move less (46). Focusing on the movement of the upper limbs, we found a positive association with total mobility, self-service, and good/bad days in DMD patients, but it correlated negatively with usual activities. QoL negatively correlated with movement of the upper limbs using the PEDSQL 3.0 neuromuscular model questionnaire in disease category completed both by the DMD patients and their parents. Moreover, movement of the upper limbs positively correlated with septal MAPSE.
When assessing the ambulatory/non-ambulatory and sitting/non-sitting DMD patients, statistically significant difference in total mobility was found. Ambulatory/non-ambulatory and sitting/non-sitting DMD patients showed significant differences in self-service, usual activities, and good/bad days.
DMD patients with/without scoliosis showed a statistically significant difference in good/bad days.
The QoL focused on physical activities, health, and friends in DMD patients was reduced (13). Pangalila et al. reported that social issues of QoL were affected/impaired in DMD patients compared to the control group (54). Based on previous studies, it is known that the general mood and feelings assessed for parents were decreased than that for DMD patients (11, 55). From the children’s perspective, physical activities and health and friends were lower (13).
This is consistent with the results in our study in which EDV was positively associated with anxiety/depression, but was negatively associated with average MAPSE and total mobility, as were lateral MAPSE and total mobility.
It was a small sample because of the rare occurrence of DMD and it was a single-centre study. The questionnaire was completed in electronic version. The results of our study cannot be generalized to the worldwide population due to various levels of health care and social possibilities (56–58). In our study, our emphasis was on categorizing DMD patients into two primary groups: ambulatory and non-ambulatory. Specifically, detailed information on five subcategories of upper limb movement was collected exclusively from the “non-ambulatory DMD patients,” with the corresponding data absent for ambulatory DMD patients. Regarding the evaluation of corticosteroid therapy’s influence, our focus was solely on the ongoing pharmacotherapy. Future studies focused on QoL in DMD are needed to confirm our results.
This study delved into various dimensions of QoL in DMD patients, considering neurological, cardiac, therapeutic, and emotional aspects. Key findings revealed significant correlations: improved upper limb movement positively related to overall mobility and emotional well-being, while QoL displayed negative associations with upper limb movement. Cardiac parameters, especially septal MAPSE, were interlinked with motor function. QoL distinctions were apparent among ambulatory/non-ambulatory and sitting/non-sitting DMD patients. Anxiety/depression correlated with cardiac parameters, highlighting the intricate connection between emotional and cardiac well-being. Treatment with ACEI/sartans positively impacted overall mobility. Despite study limitations, these insights underscore the imperative for personalized care strategies in DMD patient management.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Institutional Ethics Committee (University Hospital Brno, reference number 20130410-03). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
LJ: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. LM: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization. RP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. MP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. KR: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. OV: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. VF: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. TH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. VK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. PD: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. SV: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. JH: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. KP: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The five of the authors of this publication are members of the European Reference Network for Neuromuscular Diseases – Project ID N°870177. This publication was supported by specific research grant of Masaryk university (MUNI/A/1624/2023).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^ mapi-trust.org
1. Stark, AE. Determinants of the incidence of Duchenne muscular dystrophy. Ann Transl Med. (2015) 3:287. doi: 10.3978/j.issn.2305-5839.2015.10.45
2. Wong, SH, McClaren, BJ, Archibald, AD, Weeks, A, Langmaid, T, Ryan, MM, et al. A mixed methods study of age at diagnosis and diagnostic odyssey for Duchenne muscular dystrophy. Eur J Hum Genet EJHG. (2015) 23:1294–300. doi: 10.1038/ejhg.2014.301
3. Birnkrant, DJ, Bushby, K, Bann, CM, Apkon, SD, Blackwell, A, Brumbaugh, D, et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. (2018) 17:251–67. doi: 10.1016/S1474-4422(18)30024-3
4. Eagle, M, Baudouin, SV, Chandler, C, Giddings, DR, Bullock, R, and Bushby, K. Survival in Duchenne muscular dystrophy: improvements in life expectancy since 1967 and the impact of home nocturnal ventilation. Neuromuscul Disord NMD. (2002) 12:926–9. doi: 10.1016/S0960-8966(02)00140-2
5. Passamano, L, Taglia, A, Palladino, A, Viggiano, E, D’Ambrosio, P, Scutifero, M, et al. Improvement of survival in Duchenne muscular dystrophy: retrospective analysis of 835 patients. Acta Myol. (2012) 31:121–5.
6. Landfeldt, E, Thompson, R, Sejersen, T, McMillan, HJ, Kirschner, J, and Lochmüller, H. Life expectancy at birth in Duchenne muscular dystrophy: a systematic review and meta-analysis. Eur J Epidemiol. (2020) 35:643–53. doi: 10.1007/s10654-020-00613-8
7. Baiardini, I, Minetti, C, Bonifacino, S, Porcu, A, Klersy, C, Petralia, P, et al. Quality of life in Duchenne muscular dystrophy: the subjective impact on children and parents. J Child Neurol. (2011) 26:707–13. doi: 10.1177/0883073810389043
8. Witte, RA. The psychosocial impact of a progressive physical handicap and terminal illness (Duchenne muscular dystrophy) on adolescents and their families. Br J Med Psychol. (1985) 58:179–87. doi: 10.1111/j.2044-8341.1985.tb02632.x
9. Gagliardi, BA. The impact of Duchenne muscular dystrophy on families. Orthop Nurs. (1991) 10:41–9. doi: 10.1097/00006416-199109000-00009
10. Grootenhuis, MA, de Boone, J, and van der Kooi, AJ. Living with muscular dystrophy: health related quality of life consequences for children and adults. Health Qual Life Outcomes. (2007) 5:31. doi: 10.1186/1477-7525-5-31
11. Bray, P, Bundy, AC, Ryan, MM, North, KN, and Everett, A. Health-related quality of life in boys with Duchenne muscular dystrophy: agreement between parents and their sons. J Child Neurol. (2010) 25:1188–94. doi: 10.1177/0883073809357624
12. Vahedi, S. World Health Organization quality-of-life scale (WHOQOL-BREF): analyses of their item response theory properties based on the graded responses model. Iran J Psychiatry. (2010) 5:140–53.
13. Zamani, G, Heidari, M, Azizi Malamiri, R, Ashrafi, MR, Mohammadi, M, Shervin Badv, R, et al. The quality of life in boys with Duchenne muscular dystrophy. Neuromuscul Disord NMD. (2016) 26:423–7. doi: 10.1016/j.nmd.2016.05.004
14. Elsenbruch, S, Schmid, J, Lutz, S, Geers, B, and Schara, U. Self-reported quality of life and depressive symptoms in children, adolescents, and adults with Duchenne muscular dystrophy: a cross-sectional survey study. Neuropediatrics. (2013) 44:257–64. doi: 10.1055/s-0033-1347935
15. Bendixen, RM, Senesac, C, Lott, DJ, and Vandenborne, K. Participation and quality of life in children with Duchenne muscular dystrophy using the international classification of functioning, disability, and health. Health Qual Life Outcomes. (2012) 10:43. doi: 10.1186/1477-7525-10-43
16. Riley, AW. Evidence that school-age children can self-report on their health. Ambul Pediatr. (2004) 4:371–6. doi: 10.1367/A03-178R.1
17. Raat, H, Bonsel, GJ, Essink-Bot, ML, Landgraf, JM, and Gemke, RJBJ. Reliability and validity of comprehensive health status measures in children: the child health questionnaire in relation to the health utilities index. J Clin Epidemiol. (2002) 55:67–76. doi: 10.1016/S0895-4356(01)00411-5
18. Ravens-Sieberer, U, Gosch, A, Abel, T, Auquier, P, Bellach, BM, Bruil, J, et al. Quality of life in children and adolescents: a European public health perspective. Soz Praventivmed. (2001) 46:294–302. doi: 10.1007/BF01321080
19. McPhail, S, Beller, E, and Haines, T. Two perspectives of proxy reporting of health-related quality of life using the Euroqol-5D, an investigation of agreement. Med Care. (2008) 46:1140–8. doi: 10.1097/MLR.0b013e31817d69a6
20. Marques, JCB, Oliveira, JA, Goulardins, JB, Nascimento, RO, Lima, AMV, and Casella, EB. Comparison of child self-reports and parent proxy-reports on quality of life of children with attention deficit hyperactivity disorder. Health Qual Life Outcomes. (2013) 11:186. doi: 10.1186/1477-7525-11-186
21. Grimaldi Capitello, T, Fiorilli, C, Placidi, S, Vallone, R, Drago, F, and Gentile, S. What factors influence parents’ perception of the quality of life of children and adolescents with neurocardiogenic syncope? Health Qual Life Outcomes. (2016) 14:79. doi: 10.1186/s12955-016-0476-9
22. Nolan, LB. An exploration of proxy- and self-reported adolescent health in low-resource settings. Surv Res Methods. (2016) 10:65–83. doi: 10.18148/srm/2016.v10i2.6711
23. Connolly, MA, and Johnson, JA. Measuring quality of life in paediatric patients. PharmacoEconomics. (1999) 16:605–25. doi: 10.2165/00019053-199916060-00002
24. Hullmann, SE, Ryan, JL, Ramsey, RR, Chaney, JM, and Mullins, LL. Measures of general pediatric quality of life: child health questionnaire (CHQ), DISABKIDS chronic generic measure (DCGM), KINDL-R, pediatric quality of life inventory (PedsQL) 4.0 generic Core scales, and quality of my life questionnaire (QoML). Arthritis Care Res. (2011) 63:S420–30. doi: 10.1002/acr.20637
25. Vincent, KA, Carr, AJ, Walburn, J, Scott, DL, and Rose, MR. Construction and validation of a quality of life questionnaire for neuromuscular disease (INQoL). Neurology. (2007) 68:1051–7. doi: 10.1212/01.wnl.0000257819.47628.41
26. Crossnohere, NL, Fischer, R, Lloyd, A, Prosser, LA, and Bridges, JFP. Assessing the appropriateness of the EQ-5D for Duchenne muscular dystrophy: a patient-centered study. Med Decis Mak Int J Soc Med Decis Mak. (2021) 41:209–21. doi: 10.1177/0272989X20978390
27. Kohler, M, Clarenbach, CF, Böni, L, Brack, T, Russi, EW, and Bloch, KE. Quality of life, physical disability, and respiratory impairment in Duchenne muscular dystrophy. Am J Respir Crit Care Med. (2005) 172:1032–6. doi: 10.1164/rccm.200503-322OC
28. Wiwaha, G, Sari, DM, Biben, V, Sunjaya, DK, and Hilmanto, D. Translation and validation of Indonesian version of pediatric quality of life inventory™ (PedsQL™) neuromuscular module. Health Qual Life Outcomes. (2022) 20:33. doi: 10.1186/s12955-022-01933-x
29. Landfeldt, E, Lindgren, P, Bell, CF, Guglieri, M, Straub, V, Lochmüller, H, et al. Health-related quality of life in patients with Duchenne muscular dystrophy: a multinational, cross-sectional study. Dev Med Child Neurol. (2016) 58:508–15. doi: 10.1111/dmcn.12938
30. Devlin, N, Parkin, D, and Janssen, B. Methods for Analysing and reporting EQ-5D data. Cham: Springer Nature (2020).
31. Obradovic, M, Lal, A, and Liedgens, H. Validity and responsiveness of EuroQol-5 dimension (EQ-5D) versus short Form-6 dimension (SF-6D) questionnaire in chronic pain. Health Qual Life Outcomes. (2013) 11:110. doi: 10.1186/1477-7525-11-110
32. Panovský, R, Pešl, M, Holeček, T, Máchal, J, Feitová, V, Mrázová, L, et al. Cardiac profile of the Czech population of Duchenne muscular dystrophy patients: a cardiovascular magnetic resonance study with T1 mapping. Orphanet J Rare Dis. (2019) 14:10. doi: 10.1186/s13023-018-0986-0
33. Schulz-Menger, J, Bluemke, DA, Bremerich, J, Flamm, SD, Fogel, MA, Friedrich, MG, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) board of trustees task force on standardized post processing. J Cardiovasc Magn Reson. (2013) 15:35. doi: 10.1186/1532-429X-15-35
34. Puchalski, MD, Williams, RV, Askovich, B, Sower, CT, Hor, KH, Su, JT, et al. Late gadolinium enhancement: precursor to cardiomyopathy in Duchenne muscular dystrophy? Int J Cardiovasc Imaging. (2009) 25:57–63. doi: 10.1007/s10554-008-9352-y
35. Florian, A, Ludwig, A, Engelen, M, Waltenberger, J, Rösch, S, Sechtem, U, et al. Left ventricular systolic function and the pattern of late-gadolinium-enhancement independently and additively predict adverse cardiac events in muscular dystrophy patients. J Cardiovasc Magn Reson. (2014) 16:81. doi: 10.1186/s12968-014-0081-1
36. Prion, SK, and Haerling, KA. Making sense of methods and measurement: spearman-rho ranked-order correlation coefficient. Clin Simul Nurs. (2014) 10:535–6. doi: 10.1016/j.ecns.2014.07.005
37. Wei, Y, Speechley, KN, Zou, G, and Campbell, C. Factors associated with health-related quality of life in children with Duchenne muscular dystrophy. J Child Neurol. (2016) 31:879–86. doi: 10.1177/0883073815627879
38. Houwen-van Opstal, SLS, Jansen, M, van Alfen, N, and de Groot, IJM. Health-related quality of life and its relation to disease severity in boys with Duchenne muscular dystrophy: satisfied boys, worrying parents--a case-control study. J Child Neurol. (2014) 29:1486–95. doi: 10.1177/0883073813506490
39. Uzark, K, King, E, Cripe, L, Spicer, R, Sage, J, Kinnett, K, et al. Health-related quality of life in children and adolescents with Duchenne muscular dystrophy. Pediatrics. (2012) 130:e1559–66. doi: 10.1542/peds.2012-0858
40. Liang, R, Chan, SHS, Ho, FKW, Tang, OC, Cherk, SWW, Ip, P, et al. Health-related quality of life in Chinese boys with Duchenne muscular dystrophy and their families. J Child Health Care. (2019) 23:495–506. doi: 10.1177/1367493519857423
41. Uttley, L, Carlton, J, Woods, HB, and Brazier, J. A review of quality of life themes in Duchenne muscular dystrophy for patients and carers. Health Qual Life Outcomes. (2018) 16:237. doi: 10.1186/s12955-018-1062-0
42. Lue, YJ, Chen, SS, and Lu, YM. Quality of life of patients with Duchenne muscular dystrophy: from adolescence to young men. Disabil Rehabil. (2017) 39:1408–13. doi: 10.1080/09638288.2016.1196398
43. Bann, CM, Abresch, RT, Biesecker, B, Conway, KC, Heatwole, C, Peay, H, et al. Measuring quality of life in muscular dystrophy. Neurology. (2015) 84:1034–42. doi: 10.1212/WNL.0000000000001336
44. Straub, V, and Mercuri, E. Report on the workshop: meaningful outcome measures for Duchenne muscular dystrophy, London, UK, 30-31 January 2017. Neuromuscul Disord NMD. (2018) 28:690–701. doi: 10.1016/j.nmd.2018.05.013
45. Mokkink, LB, Terwee, CB, Patrick, DL, Alonso, J, Stratford, PW, Knol, DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res Int J Qual Life Asp Treat Care Rehabil. (2010) 19:539–49. doi: 10.1007/s11136-010-9606-8
46. Powell, PA, Carlton, J, Rowen, D, Chandler, F, Guglieri, M, and Brazier, JE. Development of a new quality of life measure for Duchenne muscular dystrophy using mixed methods: the DMD-QoL. Neurology. (2021) 96:e2438–50. doi: 10.1212/WNL.0000000000011896
47. Rowen, D, Powell, P, Mukuria, C, Carlton, J, Norman, R, and Brazier, J. Deriving a preference-based measure for people with Duchenne muscular dystrophy from the DMD-QoL. Value Health J Int Soc Pharmacoeconomics Outcomes Res. (2021) 24:1499–510. doi: 10.1016/j.jval.2021.03.007
48. Panovský, R, Pešl, M, Máchal, J, Holeček, T, Feitová, V, Juříková, L, et al. Quantitative assessment of left ventricular longitudinal function and myocardial deformation in Duchenne muscular dystrophy patients. Orphanet J Rare Dis. (2021) 16:57. doi: 10.1186/s13023-021-01704-9
49. Porcher, R, Desguerre, I, Amthor, H, Chabrol, B, Audic, F, Rivier, F, et al. Association between prophylactic angiotensin-converting enzyme inhibitors and overall survival in Duchenne muscular dystrophy—analysis of registry data. Eur Heart J. (2021) 42:1976–84. doi: 10.1093/eurheartj/ehab054
50. Hendriksen, JGM, Poysky, JT, Schrans, DGM, Schouten, EGW, Aldenkamp, AP, and Vles, JSH. Psychosocial adjustment in males with Duchenne muscular dystrophy: psychometric properties and clinical utility of a parent-report questionnaire. J Pediatr Psychol. (2009) 34:69–78. doi: 10.1093/jpepsy/jsn067
51. Lamb, MM, West, NA, Ouyang, L, Yang, M, Weitzenkamp, D, James, K, et al. Corticosteroid treatment and growth patterns in ambulatory males with Duchenne muscular dystrophy. J Pediatr. (2016) 173:207–213.e3. doi: 10.1016/j.jpeds.2016.02.067
52. Pangalila, RF, van den Bos, GA, Bartels, B, Bergen, M, Stam, HJ, and Roebroeck, ME. Prevalence of fatigue, pain, and affective disorders in adults with duchenne muscular dystrophy and their associations with quality of life. Arch Phys Med Rehabil. (2015) 96:1242–7. doi: 10.1016/j.apmr.2015.02.012
53. Hunt, A, Carter, B, Abbott, J, Parker, A, Spinty, S, and deGoede, C. Pain experience, expression and coping in boys and young men with Duchenne muscular dystrophy - a pilot study using mixed methods. Eur J Paediatr Neurol EJPN. (2016) 20:630–8. doi: 10.1016/j.ejpn.2016.03.002
54. Pangalila, RF, van den Bos, GAM, Bartels, B, Bergen, MP, Kampelmacher, MJ, Stam, HJ, et al. Quality of life of adult men with Duchenne muscular dystrophy in the Netherlands: implications for care. J Rehabil Med. (2015) 47:161–6. doi: 10.2340/16501977-1898
55. Davis, SE, Hynan, LS, Limbers, CA, Andersen, CM, Greene, MC, Varni, JW, et al. The PedsQL in pediatric patients with Duchenne muscular dystrophy: feasibility, reliability, and validity of the pediatric quality of life inventory neuromuscular module and generic Core scales. J Clin Neuromuscul Dis. (2010) 11:97–109. doi: 10.1097/CND.0b013e3181c5053b
56. Cavazza, M, Kodra, Y, Armeni, P, De Santis, M, López-Bastida, J, Linertová, R, et al. Social/economic costs and health-related quality of life in patients with Duchenne muscular dystrophy in Europe. Eur J Health Econ HEPAC. (2016) 17:19–29. doi: 10.1007/s10198-016-0782-5
57. Steffensen, B, Otto, C, Werlauff, U, Rahbek, J, Hoejberg, A, Kirschner, J, et al. G.P.388 - health related quality of life in European adults with DMD: results from the care-NMD-project. Neuromuscul Disord. (2015) 25:S302. doi: 10.1016/j.nmd.2015.06.412
Keywords: quality of life, Duchenne muscular dystrophy, cardiac magnetic resonance, neurological status, cardiac impairment
Citation: Juříková L, Masárová L, Panovský R, Pešl M, Revendová KŽ, Volný O, Feitová V, Holeček T, Kincl V, Danhofer P, Voháňka S, Haberlová J and Podolská K (2024) Decreased quality of life in Duchenne muscular disease patients related to functional neurological and cardiac impairment. Front. Neurol. 15:1360385. doi: 10.3389/fneur.2024.1360385
Edited by:
Liang Wang, Sun Yat-sen University, ChinaReviewed by:
Hoi Shan Sophelia Chan, The University of Hong Kong, Hong Kong SAR, ChinaCopyright © 2024 Juříková, Masárová, Panovský, Pešl, Revendová, Volný, Feitová, Holeček, Kincl, Danhofer, Voháňka, Haberlová and Podolská. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lucia Masárová, bHVjaWEubWFzYXJvdmFAZm51c2EuY3o=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.